Embed Size (px)
Citation preview
EQUITY PROFILES OF THREE SOCIAL FRANCHISE NETWORKS IN WEST AFRICA
Nirali Chakraborty, Ph.DResearch Advisor for Reproductive Health
9th World Congress on Health Economics, Sydney, Australia
10 July 2013

Background– Franchising– Study sites
Equity calculation methodology Results
– Benin– Democratic Republic of Congo (DRC)– Mali
Implications
Outline
PAGE 2

24 FRANCHISES IN 23 COUNTRIES
SOCIAL FRANCHISING AT PSI
+10,000 FRANCHISEES 10 MILLION CLIENTS PER YEAR

+ Health Impact
✓ Quality
$ Cost-Effectiveness
Equity
Market Expansion
Improving population health
Ensuring adherence to clinical standards for client care
Providing services at equal or lower cost to alternatives
Enabling the poorest to access services
Delivering services that would not otherwise be provided
Goals of Social Franchising

Pilot equity measurement at franchises Justify use of national or sub-national reference
population, for program decision making
Study objectives
page 5

Client exit interviews Equity benchmarked
to reference population
Franchises primarily urban and peri-urban
Study context
page 6

Benin
page 7
Indicator Total Urban Rural
CPR among married women
6.1 9.0 4.5
Unmet need among married women
27.3 26.3 27.9
Under 5 mortality 136 116 145
Has electricity 27.9 56.6 8.5
Urban residence 41.4
Private Health Expenditure/THE
46.7
Out of Pocket/PHE 91.2
Source: DHS 2006 and WHO Global Health Observatory 2011 data

Offers Family Planning, SRH/HIV and MNCH services
185 clinic outlets ~33% of providers are
MDs ~100,000 clinic visits
recorded in 2012
Benin – ProFam franchise
page 8
Source: 2013 Social Franchising Compendium, www.sf4health.org

Democratic Republic of Congo
page 9
Indicator Total Urban Rural
CPR among married women
5.8 9.5 3.3
Unmet need among married women
26.9 28.1 26.1
Under 5 mortality 155 122 177
Has electricity 15.2 36.6 1.1
Urban residence 45.4
Private Health Expenditure/THE
66.3
Out of Pocket/PHE 65.7
Source: DHS 2007 and WHO Global Health Observatory 2011 data

Offers Family Planning, MNCH and Water Purification services
138 clinic outlets ~15% of providers are
MDs ~192,000 clinic visits
recorded in 2012
DRC – Réseau Confiance
page 10
Source: 2013 Social Franchising Compendium, www.sf4health.org

Mali
page 11
Indicator Total Urban Rural
CPR among married women
6.9 13 4.2
Unmet need among married women
27.6 28.4 27.2
Under 5 mortality 215 158 234
Has electricity 16.6 47.4 3.2
Urban residence 33.7
Private Health Expenditure/THE
54.9
Out of Pocket/PHE 99.6
Source: DHS 2006 and WHO Global Health Observatory 2011 data

Offers Family Planning, SRH/HIV and MNCH services
71 clinic outlets ~42% of providers are
MDs ~43,000 clinic visits
recorded in 2012
Mali – ProFam franchise
page 12
Source: 2013 Social Franchising Compendium, www.sf4health.org

Equity measurement methodology
PAGE 13
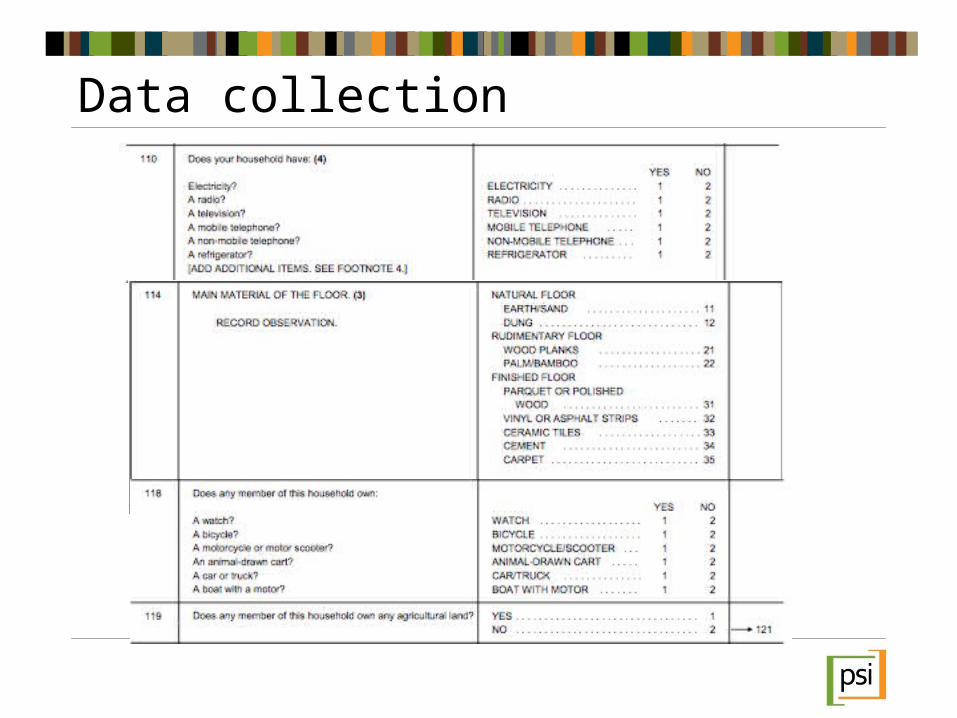
Data collection
1. Principal Components Analysis on weighted DHS asset ownership data
2. Capture eigenvector from first principal component for each asset, and quintile cut-points from asset index
3. Standardize Client data to DHS data
4. Multiply each asset by eigenvector
5. Sum (Std value*eigenvector) for each client
6. Place clients within DHS quintiles
Placing clients within reference population
Calculation done twice:National populationUrban only

Let Ai1=Asset score for each household i in DHS
Let =standardized value of each asset for household i in DHS
Let v = Value of eigenvector from first component for variable v
Let Ai2=Asset score for each client i sampled
Mathematically speaking…
page 16
ˆ v i
DHS data Client data
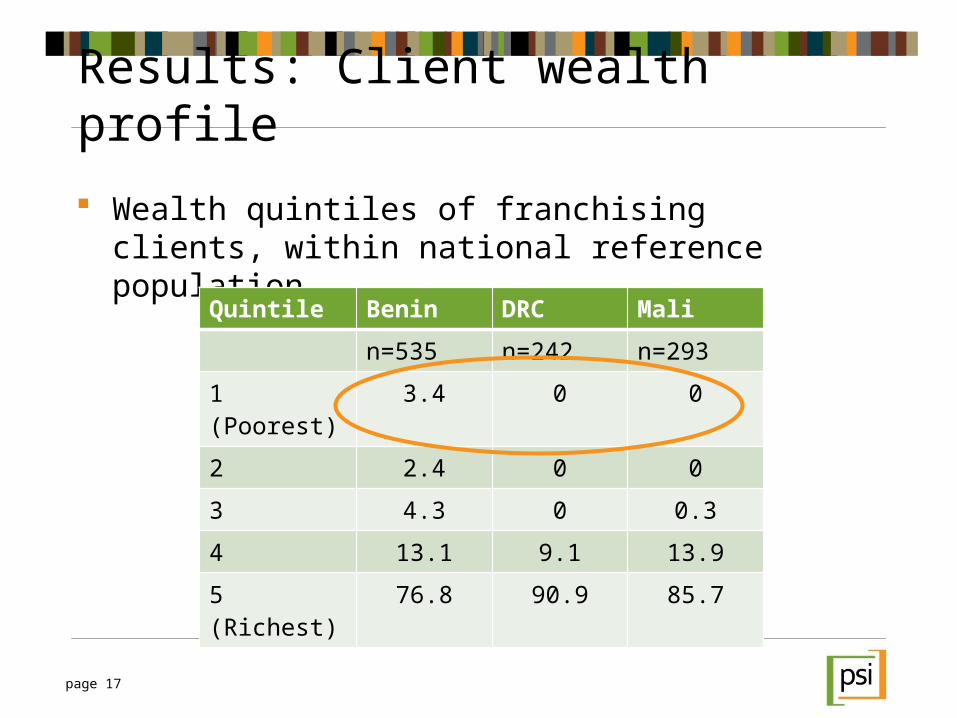
Wealth quintiles of franchising clients, within national reference population
Results: Client wealth profile
page 17
Quintile Benin DRC Mali
n=535 n=242 n=293
1 (Poorest) 3.4 0 0
2 2.4 0 0
3 4.3 0 0.3
4 13.1 9.1 13.9
5 (Richest) 76.8 90.9 85.7

Quintile National Urban
Poorest 3.4 6.7
Quintile 2 2.4 8.8
Quintile 3 4.3 11.4
Quintile 4 13.1 33.3
Richest 76.8 39.8
Poore
st Q2
Q3
Q4
Riches
t0
10
20
30
40
50
60
70
80
90
NationalUrban
Results: Client wealth profiles in context
page 18
Benin – ProFam Franchise

Quintile National Urban
Poorest 0 0
Quintile 2 0 4.6
Quintile 3 0 12.8
Quintile 4 9.1 40.9
Richest 90.9 41.7
Poore
st Q2
Q3
Q4
Riches
t0
102030405060708090
100
NationalUrban
Results: Client wealth profiles in context
page 19
DRC – Réseau Confiance

Quintile National Urban
Poorest 0 0.3
Quintile 2 0 2.1
Quintile 3 0.3 4.1
Quintile 4 14.0 15.0
Richest 85.7 78.5
Poore
st Q2
Q3
Q4
Riches
t0
10
20
30
40
50
60
70
80
90
NationalUrban
Results: Client wealth profiles in context
page 20
Mali – ProFam Franchise

Social Franchise community of practice is recommending client equity to be benchmarked against national reference population
For program decision making, sub-national reference population may be more informative
In these 3 countries, franchises appear to serve a wealthy population segment
Do social franchises serve the poor? Should social franchises aim to serve the poor(est)?
Implications
page 21
Acknowledgements: I gratefully acknowledge the PSI research managers from the three countries where this data was collected: Cyprien Zinsou (Benin), Willy Onema (DRC), and Mamadou Bah (Mali).
page 22
Questions?
1 1 2 0 1 9 T H S T R E E T , N W | S U I T E 6 0 0
W A S H I N G T O N , D C 2 0 0 3 6
P S I . O R G | T W I T T E R : @ P S I H E A LT H Y L I V E S | B L O G : P S I H E A LT H Y L I V E S . C O M
PSI


![BAWS SMALL PRINT CIRCUIT-2020 [MONOCHROME] PRINT ACCEPTANCE 2020-M2.pdfmanas chakraborty india care * manas chakraborty india traditional passage * * manas chakraborty india valencia](https://img.pdfslide.net/doc/110x75/5f5efd9c741aa6101f1839dc/baws-small-print-circuit-2020-monochrome-print-acceptance-2020-m2pdf-manas-chakraborty.jpg)
![· XLS file · Web view2016-07-27 · 00000_nayan_sam[0087] nimai bagdi[0063] marubala bagdi shanka chakraborty[0026] santosh chakraborty parbati chakraborty ... aditya ruidas[9946]](https://img.pdfslide.net/doc/110x75/5b2272847f8b9acb1d8b45e1/-xls-file-web-view2016-07-27-00000nayansam0087-nimai-bagdi0063.jpg)