Embed Size (px)
Citation preview

Erectile dysfunction
Introduction • Definition: erectile dysfunction (ED) is defined as the persistent inability to achieve and maintain an erection sufficient for satisfactory sexual intercourse.
• Epidemiology: the overall prevalence of ED is 19%. It occurs in 2% of the population up to 30 years of age and increases to 52% in men in their 80s.
• Pathophysiology: an erection is a neurovascular phenomenon that occurs under hormonal trol and a certain psychological environment. The origin of ED can thus be vascular (arte‐
ial or venous), neurogenic, hormonal or psychogenic. conr Anamnesis • Medical history identifi:
- Vasccation of possible causes of ED.
ular ED: Arterial causes: hypertension, diabetes, cholesterol, smoking, sedentary lifestyle, radical prostatectomy or other pelvic surgery, pelvic radiotherapy, vasculopathy.
Venous causes: failure of the corporal veno‐occlusive mechanism that impedes ve‐nous leak ge when an erection has been triggered. This typically occurs in young men who itia detumesce
ain
- Neurlly achieve good rigidity, but with rapid nce.
ogenic ED: Central causes: m ultiple sclerosis, multiple atrophy, Parkinson’s disease, tumors,stroke, disc disease, spinal cord injury.
Peripheral causes: DM, alcoholism, uremia, polyneuropathy, retroperitoneal or pel‐vic surgery (radical prostatectomy or other pelvic surgery).
- ED due to anatomical or structural causes: Peyroni c re injury of ar
e’s disease, ongenital curvatu of the penis, micropenis, hypspadias, epispadias, the penile tery or CC.
- ED due to per‐prolactinemia,
hormonal causes: testosterone deficiency (hypogonadism), hyh per‐ or hypothyroidism se.
- Psychogenic E : tress, relationship prob ms fear (performance anxiety). y , Cushing’s disea
D s le , of failure - Drugrelated ED: antihypertensive drugs (diuretics and βblockers), antidepressants and
antipsychotics, antihistamines, antiandrogens, drug abuse. Antihypertensive αblockers (doxazosin), ACE inhibitors, ARBs, and Ca++antagonists do not cause ED.
Substances which may cause Erectile Dysfunction
Alcohol Cannabis Phenothiazine MetoclopramideAmitriptyline Cimetidine Haloperidol NaproxenLHRH analogs Clofibrate Heroine NicotineAmphetamines Cocaine Hydralazine OmeprazoleAntiandrogens Digoxin Indomethacin OpioidAntidepressants Spironolactone MAO inhibitors ThiazideAtenolol Steroids Lithium VerapamilBarbiturates Famotidine Methadone βblockers Phenytoin Methyldopa
• Sexual anamnesis: - Start of ED: duration, circumstances in which it occurs, evolution. - Degree of impotence: an erna‐tion with normal erec
erection, 1‐10/10 swelling, premature detumescence, alt
- Circumstances ED occu rs. tions, time changes, ability to penetrate. rs: visua e
- Spontaneous erectionl/tactile stimulus, masturbation, different partn
ions. - Othe pects of sexu
s: presence or absence of morning or nocturnal erectal function: assessment of
- r as libido, ejaculation, and orgasm.
Associated symptoms: presence of pain with erection or penile curvature. - IIEF (International Index of Erectile Function): validated questionnaire with multiple domains of sexual function, useful for recording changes after treatment.

IIEF (Inter a f e Fun nnation l Index o Erectil ctio ) Over the past 4 weeks: No sexual
activity
Almost never /never
< half of the time
About half the time
> half of the time
Al s most alwayor al ays w
1. How often were you able to get an erection during sexual activity? 0 1 2 3 4 5
2. When you had erections with sexual sti s mulation, how often were your erectionhard enough for penetration?
0 1 2 3 4 5
3. When you attempted intercourse, how often were you able to penetrate? 0 1 2 3 4 5
4. After penetration, how often were you able to maintain your erection? 0 1 2 3 4 5
Did not attempt
interc urseo
Extremely difficult Very difficult Difficult Slightly
difficult Not difficult
5. During sexual intercourse, how difficult was it to maintain your erection to completion of intercourse?
0 1 2 3 4 5
No att mptse 1‐2 at mpts te 3‐4 at mptste 5‐6 at mpts te 7‐10 attempts
11 or more attempts
6. How many times have you attempted sexual intercourse?
0 1 2 3 4 5
Did not attempt
interc urseo
Alm erost nev/never
< half of the time
About half the time
> half of the time
Almost always or al ays w
7. When you attempted sexual intercourse, how often was it satisfactory for you? 0 1 2 3 4 5
No interc urseo
No enjoyment at ll a
Not very enjo ble ya
Fairly enjo ble ya
Highly enjo ble ya
Very highly enjo ble ya
8. How much have you enjoyed sexual intercourse? 0 1 2 3 4 5
No arousal interc urseo
Almost never or er nev
< half of the ti e m
About half the me ti
> half of the ti e m
Almost always or al ays w
9. When you had sexual stimulation or int ercourse, how often did you ejaculate? 0 1 2 3 4 5
10. When you had sexual stimulation or intercourse, how often did you have the feeling of orgasm or climax?
0 1 2 3 4 5
Almost never or er nev
< half of the ti ) me
About half of the me ti
> half of the ti e m
Almost always or al ays w
11. How often have you felt sexual desire? 1 2 3 4 5
Very low or none t all a L ow Mod ate er H igh Very igh h
12. How would you rate your level of sexual desire? 1 2 3 4 5
Very dissatisfied
Moderately dissa fied tis
Neutral
Moderately sati ied sf
Very s tisfied a
13. How satisfied have you been with your overall sex life? 1 2 3 4 5
14. How satisfied are you with your sexual relationship with your partner? 1 2 3 4 5
Ver ow y l L ow Mod ate er H igh Very igh h
15. How do you rate your confidence that you could get and keep an erection? 1 2 3 4 5
Results Domains Score Severity of erectile dysfunction
(Score on the erectile function domain) Erectile function (Q1‐5 and Q15) Satisfaction with sexual relationship (Q6‐8) Severe
Moderate Mild Without erectile dysfunction
6‐10 11‐16 17‐25 26‐30
Orgasmic function (Q9‐10) Sexual desire (Q11‐12) Overall satisfaction (Q13‐14)

• Psychosocial history: xual relati
- acto s. - onships (stable partner or not, frequency of intercourse, etc.). Evaluation of seFamily and work f r
- Socio‐economic status.
Physical examination • General ecomastia, degree of androge
: weight, height, phenotype, secondary sex characteristics, gynnizatio
• Genital: penis n, peripheral pulses. (abnormalities, fibrosis of CC), testes, scrotum, prostate.
• Neurological: sensitivity (perineogenital), reflexes (bulbocavernosus/scrotal/cremasteric). Analyses CBC and general b emistry: glycemia, rea, liver enzymes.
• Lipids: total chole terol, HDL, LDL, VHDL, triglycerides. Changes in any of these parameters require treatment.
• ioch creatinine, us
• Hormonal study: - Total, free, and SHB ypogonadis ter on L
onse 8‐10 a.m. (m k). G testosterone: to rule out h m (see chap ate
t Hypogonadism). Should be measured between orning pea Free testosterone: can be calculated from total testosterone, SHBG and albumin val‐ues. A calculator is available at: http://www.issam.ch/freetesto.htm
Normal ranges: if >upper limits, no replacement therapy is needed; if <lower limits replacement therapy is hin the normal range, treat‐ment depends on sym
recommended. For values witptoms.
‐ ol/L (231‐3- Total testosterone: 8 12 nm 46 ng/dL). - Free testosterone: 180‐250 pmol/L (52‐72 pg/mL).
es may show o30% of cas ↓ free testosterone with n rmal total testosterone due to ↑ SHBG. These patients are candidates for treatment. When free testosterone is near the lower limit, a 2nd measurement with LH and PRL is re
- LH: commended.
High: indicates androgen deficiency even with normal total testosterone. Androgen replacement therapy is indicated.
Decr tropic hypogoneased: indicates hypogonado adism. Likewise requires treat‐ment with testosterone, but only after an endocrinological study (LHRH test).
- Prolactin: if there is al or olfacto
a history of taking dopaminergic medications or symptoms of visuaches or l
- els are abnory disturbances, frequent head oss of libido.
FSH, TSH, ACTH, GH: to complete the pituitary study if LH or PRL lev rmal. - Estradiol: if gynecomastia or possible androgen resistance (high testosterone and LH levels with submasculinization) is present.
Cardiovascular risk assessment • Low risk: asymptomatic patient with <3 vascular risk factors, with mild angina that has been assessed and treated, previous uncomplicated infarct, mild ventricular dysfunction, success‐ful coronary revasc dularization, controlled hypertension, or mild valve efect. These patients may have sex without risk and be treated with PDE5 without prior cardiac evaluation.
• Intermediate risk: patients with ≥3 vascular risk factors, moderate stable angina, recent infarction (2‐6 weeks), moderate ventricular dysfunction, stroke, or peripheral vascular disease. Before starting ED treatment, these patients should be evaluated by a cardiologist to be classified as high or low risk patients.
• High risk: high‐risk arrhythmias, unstable or refractory angina, recent infarct (<2 weeks), severe ventricular dysfunction, hypertrophic obstructive cardiomyopathy, or other cardio‐myopathies, uncontrolled hypertension, moderate/severe valve defects. These patients should be discouraged from engaging in sexual activity until their heart function is stabilized.

Erectile dysfunction Complementary explorations In men aged 60 or over, if the clinical history, physical examination, and analysis are normal, empirical treatment with oral drugs can be started as long as the patient concurs and does not desire further study of the causal factors of his ED. In patients u h to study the causes of their ED further, the following tests can
nder 60 or for those who wis
• be performed:
Nocturnal penile tumescence and rigidity test (Rigiscan®): should last at least 2 nights. • Intracavernous injection of vasoactive drugs (IIVD test): considered to be positive if after 10 min a rigid and to initiate an IIVD
erection lasting 30 min is achieved. Useful for assessing responsiveness program, but with questionable diagnostic value.
- Procedure: involves the intracavernous administration of a vasoactive drug like prostaglandin E1 or alprosan erection is achiev
tadil (CAVERJECT®) at a dose of 20 µg, then waiting 10‐15 min until e
- d. Visual or tactile stimulus is sometimes necessary.
If an erection occurs: moderate vascular, neurogenic, psychogenic, or hormonal etiology. - If there is no erection: injection should be repeated under more favorable conditions. If that fails to elicit an be performed (Doppler ultrasound, neu‐rophysiological s
erection, other tests should
Severe vascutudy, cavernosometry). The etiology is: lar: arterial, venous, or mixed.
Psychogenic: anxiety caused by the test may inhibit erection. • Doppler ultrasound of the penis: evaluates a possible vasculogenic origin of ED. A peak systolic flow >30 cm/s and a resistance index >0.8 are considered normal.
• Arteriography of the pudendal artery and cavernosometry/cavernosography: should only be performed if reconstructive vascular surgery is being considered (arterial revascu‐larization).
• Neurophysiological study: to determine a neurogenic origin. Possible tests include: elec‐tromyography (EMG) of ve somatosensory evoked potentials, condu oked potentials.
the bulbocavernosus reflex (BCR), pudendal nerction al ev
• Psychiatric evaluation: in cas ers. time of the dorsal penile nerve, and sacres of psychiatric or psychosexual disord
• Endocrinological evaluation: in cases of complex endocrinopathies.
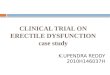
• Medical Sexual
• Psychosocial •
Anamnesis Physical examination Analyses
Erectile dysfunction diagnosis
• General • Genital • Neurological
• CBC • Biochemistry • Lipids • Hormonal study

Treatment tyle changes and risk factor modification:
- hanisms of • Lifes
Elimination of tobacco, drugs, alcohol, or medications that can alter the mecerection, such as ßblock
en diabetes, hers or psychotropic drugs.
- Treatm t of yperlipidemia, hypertension, sedentary lifestyle, etc. • Testosterone: if testosterone deficiency syndrome is detected, replacement therapy should be started (see chapter on Lateonset Hypogonadism). If ED persists, an oral drug can be add‐ed. Occasionally patients who initially do not respond to oral drugs do so after initiating treatment with androgens.
- Transdermal gels:
Generic name Brand name® Dose
Testosterone TESTOGEL gel 50 mg/5 g
Initial: 50 mg/d.* Maintenance: adjust dose according to levels of testos‐terone. Max 100 mg / d.
* Applied to the abdomen, sh ulders or inner thigh region. Requires monitoring of levels and dose adjustment. o
- Transdermal patches:
Generic name Brand names® Dose
Testosterone INTRINSA transdermal patch 300μ/24h 300μ/24h
- Intramuscular preparations :
Generic name Brand names® Dose
Testosterone NEBIDO 1 g solution injections
Initial: 1gr im, 2nd dose at 6 weeks and then eve 12 ryweeks. After gel or patch: 2nd dose at 8 weeks and then ever 12 yweeks.
• Phosphodiesterase 5 (PDE5) inhibitors: can be stawhen
rted empirically as a 1st line treatment other treatable causes of ED (e.g. LOH) have been ruled out.
- If a drug fails when taken at the maximum dose: first confirm that it was administered correctly, then eplace it r with another before attempting intracavernous injection or a vacuum device.
- Characteristics: Tadalafil may be administered on demand or daily. Its absorption is not affected by lipids minis‐tered in the for
(in contrast to that of Sildenafil and Vardenafil, except when adm o aster ac
- ngf orodispersible pills). Vardenafil is f ting.
Adverse effects: headache, facial flushing, dyspepsia, nasal co estion, blue vision. - Contraindications: ischemic heart disease treated with Nitrates, pigmentary retinopathy, CRF, liver disease. Should not be taken with Terazosin and Doxazosin (but can be taken with other αblockers).
Generic name Brand name® Dose Vardenafil LEVITRA 5, 10, and 20 mg
tablets 1 e tablet ½‐1 h before intercours
Sildenafil VIAGRA 25, 50, and 100 mg tablets
1 tablet 1 h before intercourse
Tadalafil CIALIS 10 and 20 mg tablets CIALIS 5 mg tablets
1 tablet 2 h before intercourse ½‐1 tablet/24 h
• Intracavernous drugs: 2nd line treatment after failure of oral drugs. Repeated administra‐tion of IIVDs leads to fibrosis and penile curvature in 5‐6% of cases. Contraindicated in pa‐tients with clotting disorders or taking oral anticoagulants. In neurogenic ED, ↓ doses should be used due to risk of priapism. After long periods of IIVD use, some patients respond to oral drugs. In refractory cases, an oral drug can be added, which helps 1/3 of patients.

Generic name Brand name® Dose
Alprostadil (PGE1) CAVE mcg RJECT 10 and 20
injections 5‐40 m ourse cg before interc
Papaverine + Phentolamine + PGE1
TRIMIX 4.25 mL multi‐dose solution *
Initial 0.1 mL. Can be incr d to 0. mL ease 5
* 2.5 mL Papaverine (30 m + L Phentolamine (5 mg/mL) + 0.05 mL PGE1 (501.2 mL of NSS. Prepared i a cy under sterile conditions and stored at 4° C.
g/mL) 0.5 m 0 μg/mL) + n the ph rma
• Intraurethral drugs: MUSE® (Medicated Urethral System
for Erection) is a small intraurethral rod that releases PGE1. Very poor results.
• Psychological support and sexual reeducation techniques: especially in psychogenic ED, although all types of ED may have a psychological component.
• Vacuum devices: produce passive tumescence of the CC which is maintained by applying a constrictive ring at the base of the penis. The efficacy is 90%, but with a high dropout rate due to penile pain, petechiae, etc. Contraindicated in patients with clotting disorders or tak‐ing oral ti , POS‐T‐VAC®, RAPPORT
an coagulants. There are several on the market: OSBON ERECAID® PREMIER/
• Surgery: 3rd line treaCLASSIC®, ERECTEASE®, NOOGLEBERRY®, VET‐CO®. t
- ment after failure of oral drugs, IIVD, or vacuum devices.
Penile prosthesis: malleable (semi‐rigid) or inflatable (2 or 3 components). - Revascularization: in selected cases with limited circumscribed arterial injury but no failure of the corporal veno‐occlusive mechanism. The injury must be identified with a Doppler ultraso y; venous leakage must be ruled out with cavern
und and confirmed with arteriographosography.
- Venous ligation: gives poor results; not recommended.
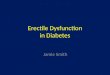
Erectile dysfunction treatment
• Psychological Hypogonadism
• Vascular lesion •
Identification of treatable causes
Other causes
• Lifestyle changes • Risk factor modification • Psychological support
1º PDE5 inhibitors 2º Intracavernous drugs / Vacuum 3º Penile prothesis

Penile rehabilitation after radical prostatectomy • Definition: scheduled administration of pro‐erection drugs after radical prostatectomy. Several studies have shown higher recovery rates of erectile function in patients receiving drugs for ED; the earlier treatment is started (within 4‐6 weeks), the better the results.
• Scientific basis: the benefit has been demonstrated in animal trials. Human trials have also shown good esults, but with short follow‐up periods and without establishing clear guide‐lines.
r
• Guidelines: - PDE5 inhibitors: the drugs of choice. They have been shown to prevent atrophy of the CC smooth muscle after radical prostatectomy. Much more effective if the neurovascular bundles have d bilaterally (35‐75% response) than if the bundles have not been pres dations:
been preserve
Sildenafil erved (0‐15% response). Dosage recommen1
Tadalafil m 3 times/w00 mg/night.
y or 20 Vardenaf
5 mg/da g taken 2‐ eek. il 20 mg
ldenafil 100 m/night.
Si g, Tadalafil 20 mg, or Vardenafil 20 mg on demand. - Intracave o response to PDE5 inhibitors. Dosage recommenda‐tions:
rnous drugs: if there is n
PGE1 20 μg/1‐3 times/week. - Vacuum devices: if there is no response to PDE5 inhibitors. Can improve erectile func‐tion a ile shorteningtions
nd prevent pen after radical prostatectomy. Dosage recommenda‐:
Daily use of the vacuum device without constricting ring (to avoid accumulation of non‐oxygenated venous blood).
Generic name Brand name® Dose Vardenafil L EVITRA 20 mg 1 tablet/night or on demand Sildenafil V I gAGRA 100 m 1 tablets/n n demand ight or o
Tadalafil CIALIS 20 mg CIALIS 5 mg
2‐3 tabl emand ets/week or on d5 mg/d
PGE1 CAVERJECT 20 μg 1‐3 times/week
Vacuum devices ERECAID®, POS‐T‐VAC , ®ERECTEASE®, VET‐CO®
Daily use without constricting ring