Embed Size (px)
Citation preview

ESC ACCAHA and Malaysian CPG Guidelines on lipids Statins Introduction to non-statins Guideline recommendations for non-statins Clinical trials of non-statin drugs
Non-statin vs placebo
Non-statin vs placebo (on background of statin-based lipid-lowering therapy)
Non-statin + statin vs placebo Non-statins on the horizon Conclusions
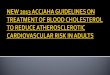
25-year-old lady presented at 12 weeks of pregnancy with NSTEMI in Feb 2015She declined termination of pregnancy despite being advised by the feto-maternal specialist
Past historyCoronary Angiogram (Jan 2014) severe ostial LMS and severe RCA stenosisECHO EF 69 Supravalvular AS calcified aortic cusps (AVA 10cm2)Planned for CABG in Feb 2014 but patient defaulted
Premorbid medical history Homozygous Familial Hypercholesterolemia - (Total chol 177 LDL 153)Hypertension
Family history Father - CABG 48yr and sister- PCI RCA 31yr
Tight LMSTight ostial RCA
More emphasise on diet and healthy lifestyle Statin remains the mainstay treatment then combination
therapy with ezetimibe and as a third line the new PCSK9 inhibitors
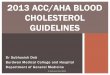
Focus on ASCVD risk reduction 4 statin benefit groups
Clinical ASCVD
Diabetes aged 40-75 years with LDL-C 70-189 mgdL
LDL-C level gt190mgdl
Estimated 10-year risk of ASCVD of gt75aged 40-75 years with
LDL-C 70-189 mgdL
Stone NJ Robinson J Lichtenstein AH et al 2013 ACCAHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults A Report of the American College of CardiologyAmerican Heart Association Task Force on Practice Guidelines J Am Coll Cardiol 2013
ASCVD atherosclerotic cardiovascular disease LDL-C Low-density lipoprotein cholesterol
Stone NJ et al J Am Coll Cardiol 2013 doi101016jjacc201311002 Available at httpcontentonlinejaccorgarticleaspxarticleid=1770217 Accessed November 13 2013
11
ASCVD Statin Benefit GroupsHeart healthy lifestyle habits are the foundation of ASCVD prevention
ASCVD prevention benefit of statin therapy may be less clear in other groups Consider additional factors influencing ASCVD risk potential ASCVD risk benefits and adverse effects drug-drug interactions and patient preferences for statin treatment
With LDL-C of 70-189 mgdLdagger Estimated using the Pooled Cohort Risk Assessment Equations
Clinical ASCVD
bull High-Intensity statin (age le75 years)
bull Moderate-intensity statin if gt75 years or not a candidate for high-intensity statin
LDL-C ge49 mmolL
bull High-intensity statin
bull Moderate-intensity statin if not a candidate for high-intensity statin
Diabetes age 40-75 years
bull Moderate-intensity statin
bull High-intensity statin if estimated 10 year ASCVD risk ge75
Estimated 10-yr ASCVD risk ge75dagger
age 40-75 years
bull Moderate- to high-intensity statin
Look at1 Family history of premature ASCVD2 LDL-C gt160 mgdl (42mmolL)3 hsCRP ge2 mgdl4 Calcium score ge300 Agatston units or ge75th 5 Sex6 Ethnicity7 Ankle-brachial index lt098 Elevated lifetime risk of ASCVD
Stone NJ Robinson J Lichtenstein AH et al 2013 ACCAHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults A Report of the American College of CardiologyAmerican Heart Association Task Force on Practice Guidelines J Am Coll Cardiol 2013
daggerEvidence from 1 RCT only down-titration if unable to tolerate atorvastatin 80 mg in IDEAL (47)DaggerAlthough simvastatin 80 mg was evaluated in RCTs initiation of simvastatin 80 mg or titration to 80 mg is not recommended by the FDA due to the increased risk of myopathy including rhabdomyolysis
High Moderate and Low-Intensity Statin Therapy (Used in the RCTs reviewed by the Expert Panel)
High-Intensity StatinTherapy
Moderate-Intensity StatinTherapy
Low-Intensity StatinTherapy
Daily dose lowers LDLndashC by approximately ge50
Daily dose lowers LDLndashC by approximately 30 to lt50
Daily dose lowers LDLndashC by lt30
Atorvastatin (40dagger)ndash80 mg Rosuvastatin 20 (40) mg
Atorvastatin 10 (20) mg Rosuvastatin (5) 10 mg Simvastatin 20ndash40 mgDagger Pravastatin 40 (80) mg Lovastatin 40 mg Fluvastatin XL 80 mg Fluvastatin 40 mg bid Pitavastatin 2ndash4 mg
Simvastatin 10 mg Pravastatin 10ndash20 mg Lovastatin 20 mg Fluvastatin 20ndash40 mg Pitavastatin 1 mg
Treat patients aggressively with the right statin dose and intensity for the patients thatrsquos been proven to benefit most from statin treatment
LDL-C targets should NOT be the ONLY determination factor to initiate statin treatment Treat to reduce the CV risk and not just the LDL-C numbers alone
Jones P et al Comparison of the efficacy and safety of rosuvastatin versus atorvastatin simvastatin and pravastatin across doses (STELLAR Trial) Am J Cardiol 200392152-160
The STELLAR study
Rosuvastatin
Atorvastatin
Simvastatin
Pravastatin
X
X
X
ndash60
ndash50
ndash40
ndash30
ndash20
ndash10
0
Dose mg (log scale)10 20 40 80
X
n = 648
n = 473n = 634
n = 485
daggerDagger
Cha
nge
in L
DL-
C fr
om
base
line
() X
Plt002 vs atorvastatin 10 mg simvastatin 10 20 40 mg pravastatin 10 20 40 mgdaggerPlt002 vs atorvastatin 20 40 mg simvastatin 20 40 80 mg pravastatin 20 40 mgDaggerPlt002 vs atorvastatin 40 mg simvastatin 40 80 mg pravastatin 40 mg
dagger
Dagger
Scandinavian Simvastatin Survival Study Group Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease the Scandinavian Simvastatin Survival Study (4S) Lancet 19943441383-1389
085
080
000
00
100
095
090
Pro
porti
on a
live
Years since randomisation
Placebo
Simvastatin
64321 5
Log rank P = 0003
Non-statins have been investigated for potential benefit in atherosclerotic cardiovascular disease (ASCVD)
This presentation surveys the clinical evidence to date
bull Cholesterol absorption inhibitors (ezetimibe)
bull Fibrates
bull Omega-3 polyunsaturated fatty acids (PUFAs)
bull Niacin
bull Emerging products
bull PCSK9 inhibitors
bull Cholesterylester transfer protein (CETP) inhibitors
ACCAHA guidelines (2014) do not support routine use of non-statins alone or in combination with statins1
Benefits not acceptable relative to potential adverse effects NICE lipid guidelines (2014) recommend against
non-statins23
No evidence of benefit ESCEAS guidelines (2012) recommend non-statins in limited
situations4
Lipid target not reached with maximally tolerated statin
Statin not tolerated 1 Stone NJ et al J Am Coll Cardiol 2014632889ndash29342 Rabar S et al BMJ 2014349g4356 doi101136bmjg4356
3 National Institute for Health and Care ExcellenceLipid modification July 2014 httpwwwniceorgukGuidanceCG181
4 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash1701
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
FIELD Fenofibrate did not reduce primary outcome (CHD death or nonfatal
MI) in patients with diabetes
FIELD fenofibrate 200 mgd vs placebo in 9795 patients with type 2 diabetesMedian follow-up 5 years
307
11
193
31
11
20
26
112
187
243
113147
00
05
10
15
20
25
30
35
LDL-C HDL-C TGs
Placebo baseline Fenofibrate baseline
Placebo study end Fenofibrate study end
Mea
n lip
id le
vel (
mm
olL
)R
ate
1000
per
son-
year
s
104
44
64 64
142
119117
37
8471
129
150
02468
10121416
Primary outcome CHD mortality Nonfatal MI Stroke All-cause mortality Coronary revascularization
Fenofibrate PlaceboHR 089
95 CI 075 to 105p=016dagger
p=022
p=036
p=018
HR 07695 CI 062 to 094
p=001
HR 07995 CI 068 to 093
p=0003
Keech A et al Lancet 20053661849ndash1861
CHD mortality or nonfatal MIdaggerARR over course of study=07 NNT=143NNT number needed to treat
Keech p7 ndash 1E
Meta-analysis Fibrates may reduce CV events
but not all-cause mortality
151005
090 (082 to 100) p=0048I2=470 p for heterogeneity=0110
087 (081 to 093) plt00001I2=221 p for heterogeneity=0202
081 (075 to 089) plt00001I2=145 p for heterogeneity=0310
100 (093 to 108) p=0918I2=194 p for heterogeneity=0237
Relative risk (95 CI)
5Major CV events
16Coronary event
10Nonfatal coronary events
16All-cause mortality
Number of studies included
Favors placeboFavors fibrateRelative risk (95 CI)
Jun M et al Lancet 20103621563ndash1574Reprinted from The Lancet Volume 362 Jun M et al Effects of fibrates on cardiovascular outcomes
a systematic review and meta-analysis 1563ndash1574 Copyright 2010 with permission from ElsevierMI and stroke
Meta-analysis of 18 placebo-controlled fibrate trials (45 058 patients)
Docosahexenoic acid (DHA)
Eicosapentenoic acid (EPA)
PUFAs Found in fish oil and Mediterranean diet1
Have been used to lower TG1
Omega-3 fatty acids
EPA1
Marketed omega-3 fatty acids include Vascepa (ethyl-EPA)2
Lovaza (mixture of ethyl-esterified EPA DHA and other fish oils)3
1 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash17012 Vascepa Prescribing Information httpwwwdrugscomprovascepahtml
3 Lovaza Prescribing Information httpswwwgsksourcecomgskprmhtdocsdocumentsLOVAZA-PI-PILPDF
Placebo-controlled trials of omega-3 fatty acids
have reported beneficial effects on CV outcomes
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin vs placebo
DART1Men previous MI(n=2033)
Dietary fish intakeMean 2 years
No significant change in total-C over 2 years
All-cause mortality darr29 (plt005)
GISSI-P2 Recent MI (n=11 324)
Omega-3 PUFA1 gd vs control Mean 35 years
LDL-C uarr99 (p=0002) HDL-C uarr88 (p=NS)TGs darr34 (p=0001)
Death nonfatal MI or nonfatal stroke darr10 (p=0048)
GISSI-HF3 Chronic HF(n=6975)
Omega-3 PUFA1 gd vs placebo Median 39 years
TGs darr from 142 to 134 mmolL over 3 years with PUFA (plt00001 vs placebo)
All-cause death darr9 (p=0041)All-cause death or CV hospitalization darr8 (p=0009)
1 Burr ML et al Lancet 19892757ndash7612 GISSI-Prevenzione Investigators Lancet 1999354447ndash455
3 GISSI-HF Investigators Lancet 20083721223ndash1230
Statin use was 5 at study baseline rising to 46 after 42 monthsrsquo follow-upPatients were also randomized to rosuvastatin or placebo no interaction was recorded between PUFA and statin
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Cholesterol absorption inhibitor
Ezetimibe
ENHANCE Simvastatin + ezetimibe did not significantly reduce intima-medial
thickness vs simvastatin alone
00111
00058
0000
0005
0010
0015
Simvastatin + ezetimibe Simvastatin + placebo
Diff
eren
ce fr
om b
asel
ine
at M
onth
24
(mm
)
p=029
44
46
48
50
52
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Mea
n H
DL-
C (m
gdL
)
100
120
140
160
180
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Med
ian
TGs
(mg
dL)
0
100
200
300
400
Baseline Month 24
Simvastatin + placebo
Simvastatin + ezetimibe
Mea
n LD
L-C
(mg
dL)
plt001
p=078
plt001
Primary endpointChange in carotid intima-medial thickness at
Month 24
ENHANCE ezetimibe 10 mgd vs placebo (added to simvastatin 80 mgd) in 720 patients with familial hypercholesterolemia (follow-up 24 months)1
1 Kastelein JJP et al N Engl J Med 20083581431ndash14432 Zocor (simvastatin calcium) Prescribing Information Merck Sharp amp Dohme Ltd October 2012No longer a recommended dose of simvastatin2
Fibrates
ACCORD Fenofibrate had no significant effect on CV endpoints when added to a
statin in patients with diabetes
36
37
38
39
40
41
42
Baseline Study end
Placebo Fenofibrate
Mea
n H
DL-
C
chol
este
rol (
mg
dL)
100
120
140
160
180
Baseline Study end
Placebo Fenofibrate
Mea
n TG
s (m
gdL
)
224
258
132
038
147
241
270
144
036
161
00
05
10
15
20
25
30
Primary outcome Major coronary eventdagger Nonfatal MI Stroke All-cause mortality
Fenofibrate Placebo
Out
com
e ra
tey
r(
) p=NS for all endpoints(Primary outcome HR 092 95 CI 079 to 108 p=032 ARR 017 per year NNT 588 to avoid one event over 1 year)
p=001
plt0001
ACCORD fenofibrate (starting dose 160 mgd) vs placebo in 5518 patients with type 2 diabetes treated with open-label simvastatin (mean follow-up 47 years)
Ginsberg HN et al N Engl J Med 20103621563ndash1574Nonfatal MI nonfatal stroke or CV deathdaggerFatal coronary event nonfatal MI or unstable angina
Niacin
55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

25-year-old lady presented at 12 weeks of pregnancy with NSTEMI in Feb 2015She declined termination of pregnancy despite being advised by the feto-maternal specialist
Past historyCoronary Angiogram (Jan 2014) severe ostial LMS and severe RCA stenosisECHO EF 69 Supravalvular AS calcified aortic cusps (AVA 10cm2)Planned for CABG in Feb 2014 but patient defaulted
Premorbid medical history Homozygous Familial Hypercholesterolemia - (Total chol 177 LDL 153)Hypertension
Family history Father - CABG 48yr and sister- PCI RCA 31yr
Tight LMSTight ostial RCA
More emphasise on diet and healthy lifestyle Statin remains the mainstay treatment then combination
therapy with ezetimibe and as a third line the new PCSK9 inhibitors
Focus on ASCVD risk reduction 4 statin benefit groups
Clinical ASCVD
Diabetes aged 40-75 years with LDL-C 70-189 mgdL
LDL-C level gt190mgdl
Estimated 10-year risk of ASCVD of gt75aged 40-75 years with
LDL-C 70-189 mgdL
Stone NJ Robinson J Lichtenstein AH et al 2013 ACCAHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults A Report of the American College of CardiologyAmerican Heart Association Task Force on Practice Guidelines J Am Coll Cardiol 2013
ASCVD atherosclerotic cardiovascular disease LDL-C Low-density lipoprotein cholesterol
Stone NJ et al J Am Coll Cardiol 2013 doi101016jjacc201311002 Available at httpcontentonlinejaccorgarticleaspxarticleid=1770217 Accessed November 13 2013
11
ASCVD Statin Benefit GroupsHeart healthy lifestyle habits are the foundation of ASCVD prevention
ASCVD prevention benefit of statin therapy may be less clear in other groups Consider additional factors influencing ASCVD risk potential ASCVD risk benefits and adverse effects drug-drug interactions and patient preferences for statin treatment
With LDL-C of 70-189 mgdLdagger Estimated using the Pooled Cohort Risk Assessment Equations
Clinical ASCVD
bull High-Intensity statin (age le75 years)
bull Moderate-intensity statin if gt75 years or not a candidate for high-intensity statin
LDL-C ge49 mmolL
bull High-intensity statin
bull Moderate-intensity statin if not a candidate for high-intensity statin
Diabetes age 40-75 years
bull Moderate-intensity statin
bull High-intensity statin if estimated 10 year ASCVD risk ge75
Estimated 10-yr ASCVD risk ge75dagger
age 40-75 years
bull Moderate- to high-intensity statin
Look at1 Family history of premature ASCVD2 LDL-C gt160 mgdl (42mmolL)3 hsCRP ge2 mgdl4 Calcium score ge300 Agatston units or ge75th 5 Sex6 Ethnicity7 Ankle-brachial index lt098 Elevated lifetime risk of ASCVD
Stone NJ Robinson J Lichtenstein AH et al 2013 ACCAHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults A Report of the American College of CardiologyAmerican Heart Association Task Force on Practice Guidelines J Am Coll Cardiol 2013
daggerEvidence from 1 RCT only down-titration if unable to tolerate atorvastatin 80 mg in IDEAL (47)DaggerAlthough simvastatin 80 mg was evaluated in RCTs initiation of simvastatin 80 mg or titration to 80 mg is not recommended by the FDA due to the increased risk of myopathy including rhabdomyolysis
High Moderate and Low-Intensity Statin Therapy (Used in the RCTs reviewed by the Expert Panel)
High-Intensity StatinTherapy
Moderate-Intensity StatinTherapy
Low-Intensity StatinTherapy
Daily dose lowers LDLndashC by approximately ge50
Daily dose lowers LDLndashC by approximately 30 to lt50
Daily dose lowers LDLndashC by lt30
Atorvastatin (40dagger)ndash80 mg Rosuvastatin 20 (40) mg
Atorvastatin 10 (20) mg Rosuvastatin (5) 10 mg Simvastatin 20ndash40 mgDagger Pravastatin 40 (80) mg Lovastatin 40 mg Fluvastatin XL 80 mg Fluvastatin 40 mg bid Pitavastatin 2ndash4 mg
Simvastatin 10 mg Pravastatin 10ndash20 mg Lovastatin 20 mg Fluvastatin 20ndash40 mg Pitavastatin 1 mg
Treat patients aggressively with the right statin dose and intensity for the patients thatrsquos been proven to benefit most from statin treatment
LDL-C targets should NOT be the ONLY determination factor to initiate statin treatment Treat to reduce the CV risk and not just the LDL-C numbers alone
Jones P et al Comparison of the efficacy and safety of rosuvastatin versus atorvastatin simvastatin and pravastatin across doses (STELLAR Trial) Am J Cardiol 200392152-160
The STELLAR study
Rosuvastatin
Atorvastatin
Simvastatin
Pravastatin
X
X
X
ndash60
ndash50
ndash40
ndash30
ndash20
ndash10
0
Dose mg (log scale)10 20 40 80
X
n = 648
n = 473n = 634
n = 485
daggerDagger
Cha
nge
in L
DL-
C fr
om
base
line
() X
Plt002 vs atorvastatin 10 mg simvastatin 10 20 40 mg pravastatin 10 20 40 mgdaggerPlt002 vs atorvastatin 20 40 mg simvastatin 20 40 80 mg pravastatin 20 40 mgDaggerPlt002 vs atorvastatin 40 mg simvastatin 40 80 mg pravastatin 40 mg
dagger
Dagger
Scandinavian Simvastatin Survival Study Group Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease the Scandinavian Simvastatin Survival Study (4S) Lancet 19943441383-1389
085
080
000
00
100
095
090
Pro
porti
on a
live
Years since randomisation
Placebo
Simvastatin
64321 5
Log rank P = 0003
Non-statins have been investigated for potential benefit in atherosclerotic cardiovascular disease (ASCVD)
This presentation surveys the clinical evidence to date
bull Cholesterol absorption inhibitors (ezetimibe)
bull Fibrates
bull Omega-3 polyunsaturated fatty acids (PUFAs)
bull Niacin
bull Emerging products
bull PCSK9 inhibitors
bull Cholesterylester transfer protein (CETP) inhibitors
ACCAHA guidelines (2014) do not support routine use of non-statins alone or in combination with statins1
Benefits not acceptable relative to potential adverse effects NICE lipid guidelines (2014) recommend against
non-statins23
No evidence of benefit ESCEAS guidelines (2012) recommend non-statins in limited
situations4
Lipid target not reached with maximally tolerated statin
Statin not tolerated 1 Stone NJ et al J Am Coll Cardiol 2014632889ndash29342 Rabar S et al BMJ 2014349g4356 doi101136bmjg4356
3 National Institute for Health and Care ExcellenceLipid modification July 2014 httpwwwniceorgukGuidanceCG181
4 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash1701
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
FIELD Fenofibrate did not reduce primary outcome (CHD death or nonfatal
MI) in patients with diabetes
FIELD fenofibrate 200 mgd vs placebo in 9795 patients with type 2 diabetesMedian follow-up 5 years
307
11
193
31
11
20
26
112
187
243
113147
00
05
10
15
20
25
30
35
LDL-C HDL-C TGs
Placebo baseline Fenofibrate baseline
Placebo study end Fenofibrate study end
Mea
n lip
id le
vel (
mm
olL
)R
ate
1000
per
son-
year
s
104
44
64 64
142
119117
37
8471
129
150
02468
10121416
Primary outcome CHD mortality Nonfatal MI Stroke All-cause mortality Coronary revascularization
Fenofibrate PlaceboHR 089
95 CI 075 to 105p=016dagger
p=022
p=036
p=018
HR 07695 CI 062 to 094
p=001
HR 07995 CI 068 to 093
p=0003
Keech A et al Lancet 20053661849ndash1861
CHD mortality or nonfatal MIdaggerARR over course of study=07 NNT=143NNT number needed to treat
Keech p7 ndash 1E
Meta-analysis Fibrates may reduce CV events
but not all-cause mortality
151005
090 (082 to 100) p=0048I2=470 p for heterogeneity=0110
087 (081 to 093) plt00001I2=221 p for heterogeneity=0202
081 (075 to 089) plt00001I2=145 p for heterogeneity=0310
100 (093 to 108) p=0918I2=194 p for heterogeneity=0237
Relative risk (95 CI)
5Major CV events
16Coronary event
10Nonfatal coronary events
16All-cause mortality
Number of studies included
Favors placeboFavors fibrateRelative risk (95 CI)
Jun M et al Lancet 20103621563ndash1574Reprinted from The Lancet Volume 362 Jun M et al Effects of fibrates on cardiovascular outcomes
a systematic review and meta-analysis 1563ndash1574 Copyright 2010 with permission from ElsevierMI and stroke
Meta-analysis of 18 placebo-controlled fibrate trials (45 058 patients)
Docosahexenoic acid (DHA)
Eicosapentenoic acid (EPA)
PUFAs Found in fish oil and Mediterranean diet1
Have been used to lower TG1
Omega-3 fatty acids
EPA1
Marketed omega-3 fatty acids include Vascepa (ethyl-EPA)2
Lovaza (mixture of ethyl-esterified EPA DHA and other fish oils)3
1 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash17012 Vascepa Prescribing Information httpwwwdrugscomprovascepahtml
3 Lovaza Prescribing Information httpswwwgsksourcecomgskprmhtdocsdocumentsLOVAZA-PI-PILPDF
Placebo-controlled trials of omega-3 fatty acids
have reported beneficial effects on CV outcomes
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin vs placebo
DART1Men previous MI(n=2033)
Dietary fish intakeMean 2 years
No significant change in total-C over 2 years
All-cause mortality darr29 (plt005)
GISSI-P2 Recent MI (n=11 324)
Omega-3 PUFA1 gd vs control Mean 35 years
LDL-C uarr99 (p=0002) HDL-C uarr88 (p=NS)TGs darr34 (p=0001)
Death nonfatal MI or nonfatal stroke darr10 (p=0048)
GISSI-HF3 Chronic HF(n=6975)
Omega-3 PUFA1 gd vs placebo Median 39 years
TGs darr from 142 to 134 mmolL over 3 years with PUFA (plt00001 vs placebo)
All-cause death darr9 (p=0041)All-cause death or CV hospitalization darr8 (p=0009)
1 Burr ML et al Lancet 19892757ndash7612 GISSI-Prevenzione Investigators Lancet 1999354447ndash455
3 GISSI-HF Investigators Lancet 20083721223ndash1230
Statin use was 5 at study baseline rising to 46 after 42 monthsrsquo follow-upPatients were also randomized to rosuvastatin or placebo no interaction was recorded between PUFA and statin
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Cholesterol absorption inhibitor
Ezetimibe
ENHANCE Simvastatin + ezetimibe did not significantly reduce intima-medial
thickness vs simvastatin alone
00111
00058
0000
0005
0010
0015
Simvastatin + ezetimibe Simvastatin + placebo
Diff
eren
ce fr
om b
asel
ine
at M
onth
24
(mm
)
p=029
44
46
48
50
52
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Mea
n H
DL-
C (m
gdL
)
100
120
140
160
180
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Med
ian
TGs
(mg
dL)
0
100
200
300
400
Baseline Month 24
Simvastatin + placebo
Simvastatin + ezetimibe
Mea
n LD
L-C
(mg
dL)
plt001
p=078
plt001
Primary endpointChange in carotid intima-medial thickness at
Month 24
ENHANCE ezetimibe 10 mgd vs placebo (added to simvastatin 80 mgd) in 720 patients with familial hypercholesterolemia (follow-up 24 months)1
1 Kastelein JJP et al N Engl J Med 20083581431ndash14432 Zocor (simvastatin calcium) Prescribing Information Merck Sharp amp Dohme Ltd October 2012No longer a recommended dose of simvastatin2
Fibrates
ACCORD Fenofibrate had no significant effect on CV endpoints when added to a
statin in patients with diabetes
36
37
38
39
40
41
42
Baseline Study end
Placebo Fenofibrate
Mea
n H
DL-
C
chol
este
rol (
mg
dL)
100
120
140
160
180
Baseline Study end
Placebo Fenofibrate
Mea
n TG
s (m
gdL
)
224
258
132
038
147
241
270
144
036
161
00
05
10
15
20
25
30
Primary outcome Major coronary eventdagger Nonfatal MI Stroke All-cause mortality
Fenofibrate Placebo
Out
com
e ra
tey
r(
) p=NS for all endpoints(Primary outcome HR 092 95 CI 079 to 108 p=032 ARR 017 per year NNT 588 to avoid one event over 1 year)
p=001
plt0001
ACCORD fenofibrate (starting dose 160 mgd) vs placebo in 5518 patients with type 2 diabetes treated with open-label simvastatin (mean follow-up 47 years)
Ginsberg HN et al N Engl J Med 20103621563ndash1574Nonfatal MI nonfatal stroke or CV deathdaggerFatal coronary event nonfatal MI or unstable angina
Niacin
55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Tight LMSTight ostial RCA
More emphasise on diet and healthy lifestyle Statin remains the mainstay treatment then combination
therapy with ezetimibe and as a third line the new PCSK9 inhibitors
Focus on ASCVD risk reduction 4 statin benefit groups
Clinical ASCVD
Diabetes aged 40-75 years with LDL-C 70-189 mgdL
LDL-C level gt190mgdl
Estimated 10-year risk of ASCVD of gt75aged 40-75 years with
LDL-C 70-189 mgdL
Stone NJ Robinson J Lichtenstein AH et al 2013 ACCAHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults A Report of the American College of CardiologyAmerican Heart Association Task Force on Practice Guidelines J Am Coll Cardiol 2013
ASCVD atherosclerotic cardiovascular disease LDL-C Low-density lipoprotein cholesterol
Stone NJ et al J Am Coll Cardiol 2013 doi101016jjacc201311002 Available at httpcontentonlinejaccorgarticleaspxarticleid=1770217 Accessed November 13 2013
11
ASCVD Statin Benefit GroupsHeart healthy lifestyle habits are the foundation of ASCVD prevention
ASCVD prevention benefit of statin therapy may be less clear in other groups Consider additional factors influencing ASCVD risk potential ASCVD risk benefits and adverse effects drug-drug interactions and patient preferences for statin treatment
With LDL-C of 70-189 mgdLdagger Estimated using the Pooled Cohort Risk Assessment Equations
Clinical ASCVD
bull High-Intensity statin (age le75 years)
bull Moderate-intensity statin if gt75 years or not a candidate for high-intensity statin
LDL-C ge49 mmolL
bull High-intensity statin
bull Moderate-intensity statin if not a candidate for high-intensity statin
Diabetes age 40-75 years
bull Moderate-intensity statin
bull High-intensity statin if estimated 10 year ASCVD risk ge75
Estimated 10-yr ASCVD risk ge75dagger
age 40-75 years
bull Moderate- to high-intensity statin
Look at1 Family history of premature ASCVD2 LDL-C gt160 mgdl (42mmolL)3 hsCRP ge2 mgdl4 Calcium score ge300 Agatston units or ge75th 5 Sex6 Ethnicity7 Ankle-brachial index lt098 Elevated lifetime risk of ASCVD
Stone NJ Robinson J Lichtenstein AH et al 2013 ACCAHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults A Report of the American College of CardiologyAmerican Heart Association Task Force on Practice Guidelines J Am Coll Cardiol 2013
daggerEvidence from 1 RCT only down-titration if unable to tolerate atorvastatin 80 mg in IDEAL (47)DaggerAlthough simvastatin 80 mg was evaluated in RCTs initiation of simvastatin 80 mg or titration to 80 mg is not recommended by the FDA due to the increased risk of myopathy including rhabdomyolysis
High Moderate and Low-Intensity Statin Therapy (Used in the RCTs reviewed by the Expert Panel)
High-Intensity StatinTherapy
Moderate-Intensity StatinTherapy
Low-Intensity StatinTherapy
Daily dose lowers LDLndashC by approximately ge50
Daily dose lowers LDLndashC by approximately 30 to lt50
Daily dose lowers LDLndashC by lt30
Atorvastatin (40dagger)ndash80 mg Rosuvastatin 20 (40) mg
Atorvastatin 10 (20) mg Rosuvastatin (5) 10 mg Simvastatin 20ndash40 mgDagger Pravastatin 40 (80) mg Lovastatin 40 mg Fluvastatin XL 80 mg Fluvastatin 40 mg bid Pitavastatin 2ndash4 mg
Simvastatin 10 mg Pravastatin 10ndash20 mg Lovastatin 20 mg Fluvastatin 20ndash40 mg Pitavastatin 1 mg
Treat patients aggressively with the right statin dose and intensity for the patients thatrsquos been proven to benefit most from statin treatment
LDL-C targets should NOT be the ONLY determination factor to initiate statin treatment Treat to reduce the CV risk and not just the LDL-C numbers alone
Jones P et al Comparison of the efficacy and safety of rosuvastatin versus atorvastatin simvastatin and pravastatin across doses (STELLAR Trial) Am J Cardiol 200392152-160
The STELLAR study
Rosuvastatin
Atorvastatin
Simvastatin
Pravastatin
X
X
X
ndash60
ndash50
ndash40
ndash30
ndash20
ndash10
0
Dose mg (log scale)10 20 40 80
X
n = 648
n = 473n = 634
n = 485
daggerDagger
Cha
nge
in L
DL-
C fr
om
base
line
() X
Plt002 vs atorvastatin 10 mg simvastatin 10 20 40 mg pravastatin 10 20 40 mgdaggerPlt002 vs atorvastatin 20 40 mg simvastatin 20 40 80 mg pravastatin 20 40 mgDaggerPlt002 vs atorvastatin 40 mg simvastatin 40 80 mg pravastatin 40 mg
dagger
Dagger
Scandinavian Simvastatin Survival Study Group Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease the Scandinavian Simvastatin Survival Study (4S) Lancet 19943441383-1389
085
080
000
00
100
095
090
Pro
porti
on a
live
Years since randomisation
Placebo
Simvastatin
64321 5
Log rank P = 0003
Non-statins have been investigated for potential benefit in atherosclerotic cardiovascular disease (ASCVD)
This presentation surveys the clinical evidence to date
bull Cholesterol absorption inhibitors (ezetimibe)
bull Fibrates
bull Omega-3 polyunsaturated fatty acids (PUFAs)
bull Niacin
bull Emerging products
bull PCSK9 inhibitors
bull Cholesterylester transfer protein (CETP) inhibitors
ACCAHA guidelines (2014) do not support routine use of non-statins alone or in combination with statins1
Benefits not acceptable relative to potential adverse effects NICE lipid guidelines (2014) recommend against
non-statins23
No evidence of benefit ESCEAS guidelines (2012) recommend non-statins in limited
situations4
Lipid target not reached with maximally tolerated statin
Statin not tolerated 1 Stone NJ et al J Am Coll Cardiol 2014632889ndash29342 Rabar S et al BMJ 2014349g4356 doi101136bmjg4356
3 National Institute for Health and Care ExcellenceLipid modification July 2014 httpwwwniceorgukGuidanceCG181
4 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash1701
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
FIELD Fenofibrate did not reduce primary outcome (CHD death or nonfatal
MI) in patients with diabetes
FIELD fenofibrate 200 mgd vs placebo in 9795 patients with type 2 diabetesMedian follow-up 5 years
307
11
193
31
11
20
26
112
187
243
113147
00
05
10
15
20
25
30
35
LDL-C HDL-C TGs
Placebo baseline Fenofibrate baseline
Placebo study end Fenofibrate study end
Mea
n lip
id le
vel (
mm
olL
)R
ate
1000
per
son-
year
s
104
44
64 64
142
119117
37
8471
129
150
02468
10121416
Primary outcome CHD mortality Nonfatal MI Stroke All-cause mortality Coronary revascularization
Fenofibrate PlaceboHR 089
95 CI 075 to 105p=016dagger
p=022
p=036
p=018
HR 07695 CI 062 to 094
p=001
HR 07995 CI 068 to 093
p=0003
Keech A et al Lancet 20053661849ndash1861
CHD mortality or nonfatal MIdaggerARR over course of study=07 NNT=143NNT number needed to treat
Keech p7 ndash 1E
Meta-analysis Fibrates may reduce CV events
but not all-cause mortality
151005
090 (082 to 100) p=0048I2=470 p for heterogeneity=0110
087 (081 to 093) plt00001I2=221 p for heterogeneity=0202
081 (075 to 089) plt00001I2=145 p for heterogeneity=0310
100 (093 to 108) p=0918I2=194 p for heterogeneity=0237
Relative risk (95 CI)
5Major CV events
16Coronary event
10Nonfatal coronary events
16All-cause mortality
Number of studies included
Favors placeboFavors fibrateRelative risk (95 CI)
Jun M et al Lancet 20103621563ndash1574Reprinted from The Lancet Volume 362 Jun M et al Effects of fibrates on cardiovascular outcomes
a systematic review and meta-analysis 1563ndash1574 Copyright 2010 with permission from ElsevierMI and stroke
Meta-analysis of 18 placebo-controlled fibrate trials (45 058 patients)
Docosahexenoic acid (DHA)
Eicosapentenoic acid (EPA)
PUFAs Found in fish oil and Mediterranean diet1
Have been used to lower TG1
Omega-3 fatty acids
EPA1
Marketed omega-3 fatty acids include Vascepa (ethyl-EPA)2
Lovaza (mixture of ethyl-esterified EPA DHA and other fish oils)3
1 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash17012 Vascepa Prescribing Information httpwwwdrugscomprovascepahtml
3 Lovaza Prescribing Information httpswwwgsksourcecomgskprmhtdocsdocumentsLOVAZA-PI-PILPDF
Placebo-controlled trials of omega-3 fatty acids
have reported beneficial effects on CV outcomes
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin vs placebo
DART1Men previous MI(n=2033)
Dietary fish intakeMean 2 years
No significant change in total-C over 2 years
All-cause mortality darr29 (plt005)
GISSI-P2 Recent MI (n=11 324)
Omega-3 PUFA1 gd vs control Mean 35 years
LDL-C uarr99 (p=0002) HDL-C uarr88 (p=NS)TGs darr34 (p=0001)
Death nonfatal MI or nonfatal stroke darr10 (p=0048)
GISSI-HF3 Chronic HF(n=6975)
Omega-3 PUFA1 gd vs placebo Median 39 years
TGs darr from 142 to 134 mmolL over 3 years with PUFA (plt00001 vs placebo)
All-cause death darr9 (p=0041)All-cause death or CV hospitalization darr8 (p=0009)
1 Burr ML et al Lancet 19892757ndash7612 GISSI-Prevenzione Investigators Lancet 1999354447ndash455
3 GISSI-HF Investigators Lancet 20083721223ndash1230
Statin use was 5 at study baseline rising to 46 after 42 monthsrsquo follow-upPatients were also randomized to rosuvastatin or placebo no interaction was recorded between PUFA and statin
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Cholesterol absorption inhibitor
Ezetimibe
ENHANCE Simvastatin + ezetimibe did not significantly reduce intima-medial
thickness vs simvastatin alone
00111
00058
0000
0005
0010
0015
Simvastatin + ezetimibe Simvastatin + placebo
Diff
eren
ce fr
om b
asel
ine
at M
onth
24
(mm
)
p=029
44
46
48
50
52
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Mea
n H
DL-
C (m
gdL
)
100
120
140
160
180
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Med
ian
TGs
(mg
dL)
0
100
200
300
400
Baseline Month 24
Simvastatin + placebo
Simvastatin + ezetimibe
Mea
n LD
L-C
(mg
dL)
plt001
p=078
plt001
Primary endpointChange in carotid intima-medial thickness at
Month 24
ENHANCE ezetimibe 10 mgd vs placebo (added to simvastatin 80 mgd) in 720 patients with familial hypercholesterolemia (follow-up 24 months)1
1 Kastelein JJP et al N Engl J Med 20083581431ndash14432 Zocor (simvastatin calcium) Prescribing Information Merck Sharp amp Dohme Ltd October 2012No longer a recommended dose of simvastatin2
Fibrates
ACCORD Fenofibrate had no significant effect on CV endpoints when added to a
statin in patients with diabetes
36
37
38
39
40
41
42
Baseline Study end
Placebo Fenofibrate
Mea
n H
DL-
C
chol
este
rol (
mg
dL)
100
120
140
160
180
Baseline Study end
Placebo Fenofibrate
Mea
n TG
s (m
gdL
)
224
258
132
038
147
241
270
144
036
161
00
05
10
15
20
25
30
Primary outcome Major coronary eventdagger Nonfatal MI Stroke All-cause mortality
Fenofibrate Placebo
Out
com
e ra
tey
r(
) p=NS for all endpoints(Primary outcome HR 092 95 CI 079 to 108 p=032 ARR 017 per year NNT 588 to avoid one event over 1 year)
p=001
plt0001
ACCORD fenofibrate (starting dose 160 mgd) vs placebo in 5518 patients with type 2 diabetes treated with open-label simvastatin (mean follow-up 47 years)
Ginsberg HN et al N Engl J Med 20103621563ndash1574Nonfatal MI nonfatal stroke or CV deathdaggerFatal coronary event nonfatal MI or unstable angina
Niacin
55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

More emphasise on diet and healthy lifestyle Statin remains the mainstay treatment then combination
therapy with ezetimibe and as a third line the new PCSK9 inhibitors
Focus on ASCVD risk reduction 4 statin benefit groups
Clinical ASCVD
Diabetes aged 40-75 years with LDL-C 70-189 mgdL
LDL-C level gt190mgdl
Estimated 10-year risk of ASCVD of gt75aged 40-75 years with
LDL-C 70-189 mgdL
Stone NJ Robinson J Lichtenstein AH et al 2013 ACCAHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults A Report of the American College of CardiologyAmerican Heart Association Task Force on Practice Guidelines J Am Coll Cardiol 2013
ASCVD atherosclerotic cardiovascular disease LDL-C Low-density lipoprotein cholesterol
Stone NJ et al J Am Coll Cardiol 2013 doi101016jjacc201311002 Available at httpcontentonlinejaccorgarticleaspxarticleid=1770217 Accessed November 13 2013
11
ASCVD Statin Benefit GroupsHeart healthy lifestyle habits are the foundation of ASCVD prevention
ASCVD prevention benefit of statin therapy may be less clear in other groups Consider additional factors influencing ASCVD risk potential ASCVD risk benefits and adverse effects drug-drug interactions and patient preferences for statin treatment
With LDL-C of 70-189 mgdLdagger Estimated using the Pooled Cohort Risk Assessment Equations
Clinical ASCVD
bull High-Intensity statin (age le75 years)
bull Moderate-intensity statin if gt75 years or not a candidate for high-intensity statin
LDL-C ge49 mmolL
bull High-intensity statin
bull Moderate-intensity statin if not a candidate for high-intensity statin
Diabetes age 40-75 years
bull Moderate-intensity statin
bull High-intensity statin if estimated 10 year ASCVD risk ge75
Estimated 10-yr ASCVD risk ge75dagger
age 40-75 years
bull Moderate- to high-intensity statin
Look at1 Family history of premature ASCVD2 LDL-C gt160 mgdl (42mmolL)3 hsCRP ge2 mgdl4 Calcium score ge300 Agatston units or ge75th 5 Sex6 Ethnicity7 Ankle-brachial index lt098 Elevated lifetime risk of ASCVD
Stone NJ Robinson J Lichtenstein AH et al 2013 ACCAHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults A Report of the American College of CardiologyAmerican Heart Association Task Force on Practice Guidelines J Am Coll Cardiol 2013
daggerEvidence from 1 RCT only down-titration if unable to tolerate atorvastatin 80 mg in IDEAL (47)DaggerAlthough simvastatin 80 mg was evaluated in RCTs initiation of simvastatin 80 mg or titration to 80 mg is not recommended by the FDA due to the increased risk of myopathy including rhabdomyolysis
High Moderate and Low-Intensity Statin Therapy (Used in the RCTs reviewed by the Expert Panel)
High-Intensity StatinTherapy
Moderate-Intensity StatinTherapy
Low-Intensity StatinTherapy
Daily dose lowers LDLndashC by approximately ge50
Daily dose lowers LDLndashC by approximately 30 to lt50
Daily dose lowers LDLndashC by lt30
Atorvastatin (40dagger)ndash80 mg Rosuvastatin 20 (40) mg
Atorvastatin 10 (20) mg Rosuvastatin (5) 10 mg Simvastatin 20ndash40 mgDagger Pravastatin 40 (80) mg Lovastatin 40 mg Fluvastatin XL 80 mg Fluvastatin 40 mg bid Pitavastatin 2ndash4 mg
Simvastatin 10 mg Pravastatin 10ndash20 mg Lovastatin 20 mg Fluvastatin 20ndash40 mg Pitavastatin 1 mg
Treat patients aggressively with the right statin dose and intensity for the patients thatrsquos been proven to benefit most from statin treatment
LDL-C targets should NOT be the ONLY determination factor to initiate statin treatment Treat to reduce the CV risk and not just the LDL-C numbers alone
Jones P et al Comparison of the efficacy and safety of rosuvastatin versus atorvastatin simvastatin and pravastatin across doses (STELLAR Trial) Am J Cardiol 200392152-160
The STELLAR study
Rosuvastatin
Atorvastatin
Simvastatin
Pravastatin
X
X
X
ndash60
ndash50
ndash40
ndash30
ndash20
ndash10
0
Dose mg (log scale)10 20 40 80
X
n = 648
n = 473n = 634
n = 485
daggerDagger
Cha
nge
in L
DL-
C fr
om
base
line
() X
Plt002 vs atorvastatin 10 mg simvastatin 10 20 40 mg pravastatin 10 20 40 mgdaggerPlt002 vs atorvastatin 20 40 mg simvastatin 20 40 80 mg pravastatin 20 40 mgDaggerPlt002 vs atorvastatin 40 mg simvastatin 40 80 mg pravastatin 40 mg
dagger
Dagger
Scandinavian Simvastatin Survival Study Group Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease the Scandinavian Simvastatin Survival Study (4S) Lancet 19943441383-1389
085
080
000
00
100
095
090
Pro
porti
on a
live
Years since randomisation
Placebo
Simvastatin
64321 5
Log rank P = 0003
Non-statins have been investigated for potential benefit in atherosclerotic cardiovascular disease (ASCVD)
This presentation surveys the clinical evidence to date
bull Cholesterol absorption inhibitors (ezetimibe)
bull Fibrates
bull Omega-3 polyunsaturated fatty acids (PUFAs)
bull Niacin
bull Emerging products
bull PCSK9 inhibitors
bull Cholesterylester transfer protein (CETP) inhibitors
ACCAHA guidelines (2014) do not support routine use of non-statins alone or in combination with statins1
Benefits not acceptable relative to potential adverse effects NICE lipid guidelines (2014) recommend against
non-statins23
No evidence of benefit ESCEAS guidelines (2012) recommend non-statins in limited
situations4
Lipid target not reached with maximally tolerated statin
Statin not tolerated 1 Stone NJ et al J Am Coll Cardiol 2014632889ndash29342 Rabar S et al BMJ 2014349g4356 doi101136bmjg4356
3 National Institute for Health and Care ExcellenceLipid modification July 2014 httpwwwniceorgukGuidanceCG181
4 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash1701
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
FIELD Fenofibrate did not reduce primary outcome (CHD death or nonfatal
MI) in patients with diabetes
FIELD fenofibrate 200 mgd vs placebo in 9795 patients with type 2 diabetesMedian follow-up 5 years
307
11
193
31
11
20
26
112
187
243
113147
00
05
10
15
20
25
30
35
LDL-C HDL-C TGs
Placebo baseline Fenofibrate baseline
Placebo study end Fenofibrate study end
Mea
n lip
id le
vel (
mm
olL
)R
ate
1000
per
son-
year
s
104
44
64 64
142
119117
37
8471
129
150
02468
10121416
Primary outcome CHD mortality Nonfatal MI Stroke All-cause mortality Coronary revascularization
Fenofibrate PlaceboHR 089
95 CI 075 to 105p=016dagger
p=022
p=036
p=018
HR 07695 CI 062 to 094
p=001
HR 07995 CI 068 to 093
p=0003
Keech A et al Lancet 20053661849ndash1861
CHD mortality or nonfatal MIdaggerARR over course of study=07 NNT=143NNT number needed to treat
Keech p7 ndash 1E
Meta-analysis Fibrates may reduce CV events
but not all-cause mortality
151005
090 (082 to 100) p=0048I2=470 p for heterogeneity=0110
087 (081 to 093) plt00001I2=221 p for heterogeneity=0202
081 (075 to 089) plt00001I2=145 p for heterogeneity=0310
100 (093 to 108) p=0918I2=194 p for heterogeneity=0237
Relative risk (95 CI)
5Major CV events
16Coronary event
10Nonfatal coronary events
16All-cause mortality
Number of studies included
Favors placeboFavors fibrateRelative risk (95 CI)
Jun M et al Lancet 20103621563ndash1574Reprinted from The Lancet Volume 362 Jun M et al Effects of fibrates on cardiovascular outcomes
a systematic review and meta-analysis 1563ndash1574 Copyright 2010 with permission from ElsevierMI and stroke
Meta-analysis of 18 placebo-controlled fibrate trials (45 058 patients)
Docosahexenoic acid (DHA)
Eicosapentenoic acid (EPA)
PUFAs Found in fish oil and Mediterranean diet1
Have been used to lower TG1
Omega-3 fatty acids
EPA1
Marketed omega-3 fatty acids include Vascepa (ethyl-EPA)2
Lovaza (mixture of ethyl-esterified EPA DHA and other fish oils)3
1 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash17012 Vascepa Prescribing Information httpwwwdrugscomprovascepahtml
3 Lovaza Prescribing Information httpswwwgsksourcecomgskprmhtdocsdocumentsLOVAZA-PI-PILPDF
Placebo-controlled trials of omega-3 fatty acids
have reported beneficial effects on CV outcomes
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin vs placebo
DART1Men previous MI(n=2033)
Dietary fish intakeMean 2 years
No significant change in total-C over 2 years
All-cause mortality darr29 (plt005)
GISSI-P2 Recent MI (n=11 324)
Omega-3 PUFA1 gd vs control Mean 35 years
LDL-C uarr99 (p=0002) HDL-C uarr88 (p=NS)TGs darr34 (p=0001)
Death nonfatal MI or nonfatal stroke darr10 (p=0048)
GISSI-HF3 Chronic HF(n=6975)
Omega-3 PUFA1 gd vs placebo Median 39 years
TGs darr from 142 to 134 mmolL over 3 years with PUFA (plt00001 vs placebo)
All-cause death darr9 (p=0041)All-cause death or CV hospitalization darr8 (p=0009)
1 Burr ML et al Lancet 19892757ndash7612 GISSI-Prevenzione Investigators Lancet 1999354447ndash455
3 GISSI-HF Investigators Lancet 20083721223ndash1230
Statin use was 5 at study baseline rising to 46 after 42 monthsrsquo follow-upPatients were also randomized to rosuvastatin or placebo no interaction was recorded between PUFA and statin
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Cholesterol absorption inhibitor
Ezetimibe
ENHANCE Simvastatin + ezetimibe did not significantly reduce intima-medial
thickness vs simvastatin alone
00111
00058
0000
0005
0010
0015
Simvastatin + ezetimibe Simvastatin + placebo
Diff
eren
ce fr
om b
asel
ine
at M
onth
24
(mm
)
p=029
44
46
48
50
52
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Mea
n H
DL-
C (m
gdL
)
100
120
140
160
180
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Med
ian
TGs
(mg
dL)
0
100
200
300
400
Baseline Month 24
Simvastatin + placebo
Simvastatin + ezetimibe
Mea
n LD
L-C
(mg
dL)
plt001
p=078
plt001
Primary endpointChange in carotid intima-medial thickness at
Month 24
ENHANCE ezetimibe 10 mgd vs placebo (added to simvastatin 80 mgd) in 720 patients with familial hypercholesterolemia (follow-up 24 months)1
1 Kastelein JJP et al N Engl J Med 20083581431ndash14432 Zocor (simvastatin calcium) Prescribing Information Merck Sharp amp Dohme Ltd October 2012No longer a recommended dose of simvastatin2
Fibrates
ACCORD Fenofibrate had no significant effect on CV endpoints when added to a
statin in patients with diabetes
36
37
38
39
40
41
42
Baseline Study end
Placebo Fenofibrate
Mea
n H
DL-
C
chol
este
rol (
mg
dL)
100
120
140
160
180
Baseline Study end
Placebo Fenofibrate
Mea
n TG
s (m
gdL
)
224
258
132
038
147
241
270
144
036
161
00
05
10
15
20
25
30
Primary outcome Major coronary eventdagger Nonfatal MI Stroke All-cause mortality
Fenofibrate Placebo
Out
com
e ra
tey
r(
) p=NS for all endpoints(Primary outcome HR 092 95 CI 079 to 108 p=032 ARR 017 per year NNT 588 to avoid one event over 1 year)
p=001
plt0001
ACCORD fenofibrate (starting dose 160 mgd) vs placebo in 5518 patients with type 2 diabetes treated with open-label simvastatin (mean follow-up 47 years)
Ginsberg HN et al N Engl J Med 20103621563ndash1574Nonfatal MI nonfatal stroke or CV deathdaggerFatal coronary event nonfatal MI or unstable angina
Niacin
55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Focus on ASCVD risk reduction 4 statin benefit groups
Clinical ASCVD
Diabetes aged 40-75 years with LDL-C 70-189 mgdL
LDL-C level gt190mgdl
Estimated 10-year risk of ASCVD of gt75aged 40-75 years with
LDL-C 70-189 mgdL
Stone NJ Robinson J Lichtenstein AH et al 2013 ACCAHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults A Report of the American College of CardiologyAmerican Heart Association Task Force on Practice Guidelines J Am Coll Cardiol 2013
ASCVD atherosclerotic cardiovascular disease LDL-C Low-density lipoprotein cholesterol
Stone NJ et al J Am Coll Cardiol 2013 doi101016jjacc201311002 Available at httpcontentonlinejaccorgarticleaspxarticleid=1770217 Accessed November 13 2013
11
ASCVD Statin Benefit GroupsHeart healthy lifestyle habits are the foundation of ASCVD prevention
ASCVD prevention benefit of statin therapy may be less clear in other groups Consider additional factors influencing ASCVD risk potential ASCVD risk benefits and adverse effects drug-drug interactions and patient preferences for statin treatment
With LDL-C of 70-189 mgdLdagger Estimated using the Pooled Cohort Risk Assessment Equations
Clinical ASCVD
bull High-Intensity statin (age le75 years)
bull Moderate-intensity statin if gt75 years or not a candidate for high-intensity statin
LDL-C ge49 mmolL
bull High-intensity statin
bull Moderate-intensity statin if not a candidate for high-intensity statin
Diabetes age 40-75 years
bull Moderate-intensity statin
bull High-intensity statin if estimated 10 year ASCVD risk ge75
Estimated 10-yr ASCVD risk ge75dagger
age 40-75 years
bull Moderate- to high-intensity statin
Look at1 Family history of premature ASCVD2 LDL-C gt160 mgdl (42mmolL)3 hsCRP ge2 mgdl4 Calcium score ge300 Agatston units or ge75th 5 Sex6 Ethnicity7 Ankle-brachial index lt098 Elevated lifetime risk of ASCVD
Stone NJ Robinson J Lichtenstein AH et al 2013 ACCAHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults A Report of the American College of CardiologyAmerican Heart Association Task Force on Practice Guidelines J Am Coll Cardiol 2013
daggerEvidence from 1 RCT only down-titration if unable to tolerate atorvastatin 80 mg in IDEAL (47)DaggerAlthough simvastatin 80 mg was evaluated in RCTs initiation of simvastatin 80 mg or titration to 80 mg is not recommended by the FDA due to the increased risk of myopathy including rhabdomyolysis
High Moderate and Low-Intensity Statin Therapy (Used in the RCTs reviewed by the Expert Panel)
High-Intensity StatinTherapy
Moderate-Intensity StatinTherapy
Low-Intensity StatinTherapy
Daily dose lowers LDLndashC by approximately ge50
Daily dose lowers LDLndashC by approximately 30 to lt50
Daily dose lowers LDLndashC by lt30
Atorvastatin (40dagger)ndash80 mg Rosuvastatin 20 (40) mg
Atorvastatin 10 (20) mg Rosuvastatin (5) 10 mg Simvastatin 20ndash40 mgDagger Pravastatin 40 (80) mg Lovastatin 40 mg Fluvastatin XL 80 mg Fluvastatin 40 mg bid Pitavastatin 2ndash4 mg
Simvastatin 10 mg Pravastatin 10ndash20 mg Lovastatin 20 mg Fluvastatin 20ndash40 mg Pitavastatin 1 mg
Treat patients aggressively with the right statin dose and intensity for the patients thatrsquos been proven to benefit most from statin treatment
LDL-C targets should NOT be the ONLY determination factor to initiate statin treatment Treat to reduce the CV risk and not just the LDL-C numbers alone
Jones P et al Comparison of the efficacy and safety of rosuvastatin versus atorvastatin simvastatin and pravastatin across doses (STELLAR Trial) Am J Cardiol 200392152-160
The STELLAR study
Rosuvastatin
Atorvastatin
Simvastatin
Pravastatin
X
X
X
ndash60
ndash50
ndash40
ndash30
ndash20
ndash10
0
Dose mg (log scale)10 20 40 80
X
n = 648
n = 473n = 634
n = 485
daggerDagger
Cha
nge
in L
DL-
C fr
om
base
line
() X
Plt002 vs atorvastatin 10 mg simvastatin 10 20 40 mg pravastatin 10 20 40 mgdaggerPlt002 vs atorvastatin 20 40 mg simvastatin 20 40 80 mg pravastatin 20 40 mgDaggerPlt002 vs atorvastatin 40 mg simvastatin 40 80 mg pravastatin 40 mg
dagger
Dagger
Scandinavian Simvastatin Survival Study Group Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease the Scandinavian Simvastatin Survival Study (4S) Lancet 19943441383-1389
085
080
000
00
100
095
090
Pro
porti
on a
live
Years since randomisation
Placebo
Simvastatin
64321 5
Log rank P = 0003
Non-statins have been investigated for potential benefit in atherosclerotic cardiovascular disease (ASCVD)
This presentation surveys the clinical evidence to date
bull Cholesterol absorption inhibitors (ezetimibe)
bull Fibrates
bull Omega-3 polyunsaturated fatty acids (PUFAs)
bull Niacin
bull Emerging products
bull PCSK9 inhibitors
bull Cholesterylester transfer protein (CETP) inhibitors
ACCAHA guidelines (2014) do not support routine use of non-statins alone or in combination with statins1
Benefits not acceptable relative to potential adverse effects NICE lipid guidelines (2014) recommend against
non-statins23
No evidence of benefit ESCEAS guidelines (2012) recommend non-statins in limited
situations4
Lipid target not reached with maximally tolerated statin
Statin not tolerated 1 Stone NJ et al J Am Coll Cardiol 2014632889ndash29342 Rabar S et al BMJ 2014349g4356 doi101136bmjg4356
3 National Institute for Health and Care ExcellenceLipid modification July 2014 httpwwwniceorgukGuidanceCG181
4 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash1701
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
FIELD Fenofibrate did not reduce primary outcome (CHD death or nonfatal
MI) in patients with diabetes
FIELD fenofibrate 200 mgd vs placebo in 9795 patients with type 2 diabetesMedian follow-up 5 years
307
11
193
31
11
20
26
112
187
243
113147
00
05
10
15
20
25
30
35
LDL-C HDL-C TGs
Placebo baseline Fenofibrate baseline
Placebo study end Fenofibrate study end
Mea
n lip
id le
vel (
mm
olL
)R
ate
1000
per
son-
year
s
104
44
64 64
142
119117
37
8471
129
150
02468
10121416
Primary outcome CHD mortality Nonfatal MI Stroke All-cause mortality Coronary revascularization
Fenofibrate PlaceboHR 089
95 CI 075 to 105p=016dagger
p=022
p=036
p=018
HR 07695 CI 062 to 094
p=001
HR 07995 CI 068 to 093
p=0003
Keech A et al Lancet 20053661849ndash1861
CHD mortality or nonfatal MIdaggerARR over course of study=07 NNT=143NNT number needed to treat
Keech p7 ndash 1E
Meta-analysis Fibrates may reduce CV events
but not all-cause mortality
151005
090 (082 to 100) p=0048I2=470 p for heterogeneity=0110
087 (081 to 093) plt00001I2=221 p for heterogeneity=0202
081 (075 to 089) plt00001I2=145 p for heterogeneity=0310
100 (093 to 108) p=0918I2=194 p for heterogeneity=0237
Relative risk (95 CI)
5Major CV events
16Coronary event
10Nonfatal coronary events
16All-cause mortality
Number of studies included
Favors placeboFavors fibrateRelative risk (95 CI)
Jun M et al Lancet 20103621563ndash1574Reprinted from The Lancet Volume 362 Jun M et al Effects of fibrates on cardiovascular outcomes
a systematic review and meta-analysis 1563ndash1574 Copyright 2010 with permission from ElsevierMI and stroke
Meta-analysis of 18 placebo-controlled fibrate trials (45 058 patients)
Docosahexenoic acid (DHA)
Eicosapentenoic acid (EPA)
PUFAs Found in fish oil and Mediterranean diet1
Have been used to lower TG1
Omega-3 fatty acids
EPA1
Marketed omega-3 fatty acids include Vascepa (ethyl-EPA)2
Lovaza (mixture of ethyl-esterified EPA DHA and other fish oils)3
1 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash17012 Vascepa Prescribing Information httpwwwdrugscomprovascepahtml
3 Lovaza Prescribing Information httpswwwgsksourcecomgskprmhtdocsdocumentsLOVAZA-PI-PILPDF
Placebo-controlled trials of omega-3 fatty acids
have reported beneficial effects on CV outcomes
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin vs placebo
DART1Men previous MI(n=2033)
Dietary fish intakeMean 2 years
No significant change in total-C over 2 years
All-cause mortality darr29 (plt005)
GISSI-P2 Recent MI (n=11 324)
Omega-3 PUFA1 gd vs control Mean 35 years
LDL-C uarr99 (p=0002) HDL-C uarr88 (p=NS)TGs darr34 (p=0001)
Death nonfatal MI or nonfatal stroke darr10 (p=0048)
GISSI-HF3 Chronic HF(n=6975)
Omega-3 PUFA1 gd vs placebo Median 39 years
TGs darr from 142 to 134 mmolL over 3 years with PUFA (plt00001 vs placebo)
All-cause death darr9 (p=0041)All-cause death or CV hospitalization darr8 (p=0009)
1 Burr ML et al Lancet 19892757ndash7612 GISSI-Prevenzione Investigators Lancet 1999354447ndash455
3 GISSI-HF Investigators Lancet 20083721223ndash1230
Statin use was 5 at study baseline rising to 46 after 42 monthsrsquo follow-upPatients were also randomized to rosuvastatin or placebo no interaction was recorded between PUFA and statin
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Cholesterol absorption inhibitor
Ezetimibe
ENHANCE Simvastatin + ezetimibe did not significantly reduce intima-medial
thickness vs simvastatin alone
00111
00058
0000
0005
0010
0015
Simvastatin + ezetimibe Simvastatin + placebo
Diff
eren
ce fr
om b
asel
ine
at M
onth
24
(mm
)
p=029
44
46
48
50
52
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Mea
n H
DL-
C (m
gdL
)
100
120
140
160
180
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Med
ian
TGs
(mg
dL)
0
100
200
300
400
Baseline Month 24
Simvastatin + placebo
Simvastatin + ezetimibe
Mea
n LD
L-C
(mg
dL)
plt001
p=078
plt001
Primary endpointChange in carotid intima-medial thickness at
Month 24
ENHANCE ezetimibe 10 mgd vs placebo (added to simvastatin 80 mgd) in 720 patients with familial hypercholesterolemia (follow-up 24 months)1
1 Kastelein JJP et al N Engl J Med 20083581431ndash14432 Zocor (simvastatin calcium) Prescribing Information Merck Sharp amp Dohme Ltd October 2012No longer a recommended dose of simvastatin2
Fibrates
ACCORD Fenofibrate had no significant effect on CV endpoints when added to a
statin in patients with diabetes
36
37
38
39
40
41
42
Baseline Study end
Placebo Fenofibrate
Mea
n H
DL-
C
chol
este
rol (
mg
dL)
100
120
140
160
180
Baseline Study end
Placebo Fenofibrate
Mea
n TG
s (m
gdL
)
224
258
132
038
147
241
270
144
036
161
00
05
10
15
20
25
30
Primary outcome Major coronary eventdagger Nonfatal MI Stroke All-cause mortality
Fenofibrate Placebo
Out
com
e ra
tey
r(
) p=NS for all endpoints(Primary outcome HR 092 95 CI 079 to 108 p=032 ARR 017 per year NNT 588 to avoid one event over 1 year)
p=001
plt0001
ACCORD fenofibrate (starting dose 160 mgd) vs placebo in 5518 patients with type 2 diabetes treated with open-label simvastatin (mean follow-up 47 years)
Ginsberg HN et al N Engl J Med 20103621563ndash1574Nonfatal MI nonfatal stroke or CV deathdaggerFatal coronary event nonfatal MI or unstable angina
Niacin
55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Stone NJ et al J Am Coll Cardiol 2013 doi101016jjacc201311002 Available at httpcontentonlinejaccorgarticleaspxarticleid=1770217 Accessed November 13 2013
11
ASCVD Statin Benefit GroupsHeart healthy lifestyle habits are the foundation of ASCVD prevention
ASCVD prevention benefit of statin therapy may be less clear in other groups Consider additional factors influencing ASCVD risk potential ASCVD risk benefits and adverse effects drug-drug interactions and patient preferences for statin treatment
With LDL-C of 70-189 mgdLdagger Estimated using the Pooled Cohort Risk Assessment Equations
Clinical ASCVD
bull High-Intensity statin (age le75 years)
bull Moderate-intensity statin if gt75 years or not a candidate for high-intensity statin
LDL-C ge49 mmolL
bull High-intensity statin
bull Moderate-intensity statin if not a candidate for high-intensity statin
Diabetes age 40-75 years
bull Moderate-intensity statin
bull High-intensity statin if estimated 10 year ASCVD risk ge75
Estimated 10-yr ASCVD risk ge75dagger
age 40-75 years
bull Moderate- to high-intensity statin
Look at1 Family history of premature ASCVD2 LDL-C gt160 mgdl (42mmolL)3 hsCRP ge2 mgdl4 Calcium score ge300 Agatston units or ge75th 5 Sex6 Ethnicity7 Ankle-brachial index lt098 Elevated lifetime risk of ASCVD
Stone NJ Robinson J Lichtenstein AH et al 2013 ACCAHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults A Report of the American College of CardiologyAmerican Heart Association Task Force on Practice Guidelines J Am Coll Cardiol 2013
daggerEvidence from 1 RCT only down-titration if unable to tolerate atorvastatin 80 mg in IDEAL (47)DaggerAlthough simvastatin 80 mg was evaluated in RCTs initiation of simvastatin 80 mg or titration to 80 mg is not recommended by the FDA due to the increased risk of myopathy including rhabdomyolysis
High Moderate and Low-Intensity Statin Therapy (Used in the RCTs reviewed by the Expert Panel)
High-Intensity StatinTherapy
Moderate-Intensity StatinTherapy
Low-Intensity StatinTherapy
Daily dose lowers LDLndashC by approximately ge50
Daily dose lowers LDLndashC by approximately 30 to lt50
Daily dose lowers LDLndashC by lt30
Atorvastatin (40dagger)ndash80 mg Rosuvastatin 20 (40) mg
Atorvastatin 10 (20) mg Rosuvastatin (5) 10 mg Simvastatin 20ndash40 mgDagger Pravastatin 40 (80) mg Lovastatin 40 mg Fluvastatin XL 80 mg Fluvastatin 40 mg bid Pitavastatin 2ndash4 mg
Simvastatin 10 mg Pravastatin 10ndash20 mg Lovastatin 20 mg Fluvastatin 20ndash40 mg Pitavastatin 1 mg
Treat patients aggressively with the right statin dose and intensity for the patients thatrsquos been proven to benefit most from statin treatment
LDL-C targets should NOT be the ONLY determination factor to initiate statin treatment Treat to reduce the CV risk and not just the LDL-C numbers alone
Jones P et al Comparison of the efficacy and safety of rosuvastatin versus atorvastatin simvastatin and pravastatin across doses (STELLAR Trial) Am J Cardiol 200392152-160
The STELLAR study
Rosuvastatin
Atorvastatin
Simvastatin
Pravastatin
X
X
X
ndash60
ndash50
ndash40
ndash30
ndash20
ndash10
0
Dose mg (log scale)10 20 40 80
X
n = 648
n = 473n = 634
n = 485
daggerDagger
Cha
nge
in L
DL-
C fr
om
base
line
() X
Plt002 vs atorvastatin 10 mg simvastatin 10 20 40 mg pravastatin 10 20 40 mgdaggerPlt002 vs atorvastatin 20 40 mg simvastatin 20 40 80 mg pravastatin 20 40 mgDaggerPlt002 vs atorvastatin 40 mg simvastatin 40 80 mg pravastatin 40 mg
dagger
Dagger
Scandinavian Simvastatin Survival Study Group Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease the Scandinavian Simvastatin Survival Study (4S) Lancet 19943441383-1389
085
080
000
00
100
095
090
Pro
porti
on a
live
Years since randomisation
Placebo
Simvastatin
64321 5
Log rank P = 0003
Non-statins have been investigated for potential benefit in atherosclerotic cardiovascular disease (ASCVD)
This presentation surveys the clinical evidence to date
bull Cholesterol absorption inhibitors (ezetimibe)
bull Fibrates
bull Omega-3 polyunsaturated fatty acids (PUFAs)
bull Niacin
bull Emerging products
bull PCSK9 inhibitors
bull Cholesterylester transfer protein (CETP) inhibitors
ACCAHA guidelines (2014) do not support routine use of non-statins alone or in combination with statins1
Benefits not acceptable relative to potential adverse effects NICE lipid guidelines (2014) recommend against
non-statins23
No evidence of benefit ESCEAS guidelines (2012) recommend non-statins in limited
situations4
Lipid target not reached with maximally tolerated statin
Statin not tolerated 1 Stone NJ et al J Am Coll Cardiol 2014632889ndash29342 Rabar S et al BMJ 2014349g4356 doi101136bmjg4356
3 National Institute for Health and Care ExcellenceLipid modification July 2014 httpwwwniceorgukGuidanceCG181
4 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash1701
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
FIELD Fenofibrate did not reduce primary outcome (CHD death or nonfatal
MI) in patients with diabetes
FIELD fenofibrate 200 mgd vs placebo in 9795 patients with type 2 diabetesMedian follow-up 5 years
307
11
193
31
11
20
26
112
187
243
113147
00
05
10
15
20
25
30
35
LDL-C HDL-C TGs
Placebo baseline Fenofibrate baseline
Placebo study end Fenofibrate study end
Mea
n lip
id le
vel (
mm
olL
)R
ate
1000
per
son-
year
s
104
44
64 64
142
119117
37
8471
129
150
02468
10121416
Primary outcome CHD mortality Nonfatal MI Stroke All-cause mortality Coronary revascularization
Fenofibrate PlaceboHR 089
95 CI 075 to 105p=016dagger
p=022
p=036
p=018
HR 07695 CI 062 to 094
p=001
HR 07995 CI 068 to 093
p=0003
Keech A et al Lancet 20053661849ndash1861
CHD mortality or nonfatal MIdaggerARR over course of study=07 NNT=143NNT number needed to treat
Keech p7 ndash 1E
Meta-analysis Fibrates may reduce CV events
but not all-cause mortality
151005
090 (082 to 100) p=0048I2=470 p for heterogeneity=0110
087 (081 to 093) plt00001I2=221 p for heterogeneity=0202
081 (075 to 089) plt00001I2=145 p for heterogeneity=0310
100 (093 to 108) p=0918I2=194 p for heterogeneity=0237
Relative risk (95 CI)
5Major CV events
16Coronary event
10Nonfatal coronary events
16All-cause mortality
Number of studies included
Favors placeboFavors fibrateRelative risk (95 CI)
Jun M et al Lancet 20103621563ndash1574Reprinted from The Lancet Volume 362 Jun M et al Effects of fibrates on cardiovascular outcomes
a systematic review and meta-analysis 1563ndash1574 Copyright 2010 with permission from ElsevierMI and stroke
Meta-analysis of 18 placebo-controlled fibrate trials (45 058 patients)
Docosahexenoic acid (DHA)
Eicosapentenoic acid (EPA)
PUFAs Found in fish oil and Mediterranean diet1
Have been used to lower TG1
Omega-3 fatty acids
EPA1
Marketed omega-3 fatty acids include Vascepa (ethyl-EPA)2
Lovaza (mixture of ethyl-esterified EPA DHA and other fish oils)3
1 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash17012 Vascepa Prescribing Information httpwwwdrugscomprovascepahtml
3 Lovaza Prescribing Information httpswwwgsksourcecomgskprmhtdocsdocumentsLOVAZA-PI-PILPDF
Placebo-controlled trials of omega-3 fatty acids
have reported beneficial effects on CV outcomes
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin vs placebo
DART1Men previous MI(n=2033)
Dietary fish intakeMean 2 years
No significant change in total-C over 2 years
All-cause mortality darr29 (plt005)
GISSI-P2 Recent MI (n=11 324)
Omega-3 PUFA1 gd vs control Mean 35 years
LDL-C uarr99 (p=0002) HDL-C uarr88 (p=NS)TGs darr34 (p=0001)
Death nonfatal MI or nonfatal stroke darr10 (p=0048)
GISSI-HF3 Chronic HF(n=6975)
Omega-3 PUFA1 gd vs placebo Median 39 years
TGs darr from 142 to 134 mmolL over 3 years with PUFA (plt00001 vs placebo)
All-cause death darr9 (p=0041)All-cause death or CV hospitalization darr8 (p=0009)
1 Burr ML et al Lancet 19892757ndash7612 GISSI-Prevenzione Investigators Lancet 1999354447ndash455
3 GISSI-HF Investigators Lancet 20083721223ndash1230
Statin use was 5 at study baseline rising to 46 after 42 monthsrsquo follow-upPatients were also randomized to rosuvastatin or placebo no interaction was recorded between PUFA and statin
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Cholesterol absorption inhibitor
Ezetimibe
ENHANCE Simvastatin + ezetimibe did not significantly reduce intima-medial
thickness vs simvastatin alone
00111
00058
0000
0005
0010
0015
Simvastatin + ezetimibe Simvastatin + placebo
Diff
eren
ce fr
om b
asel
ine
at M
onth
24
(mm
)
p=029
44
46
48
50
52
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Mea
n H
DL-
C (m
gdL
)
100
120
140
160
180
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Med
ian
TGs
(mg
dL)
0
100
200
300
400
Baseline Month 24
Simvastatin + placebo
Simvastatin + ezetimibe
Mea
n LD
L-C
(mg
dL)
plt001
p=078
plt001
Primary endpointChange in carotid intima-medial thickness at
Month 24
ENHANCE ezetimibe 10 mgd vs placebo (added to simvastatin 80 mgd) in 720 patients with familial hypercholesterolemia (follow-up 24 months)1
1 Kastelein JJP et al N Engl J Med 20083581431ndash14432 Zocor (simvastatin calcium) Prescribing Information Merck Sharp amp Dohme Ltd October 2012No longer a recommended dose of simvastatin2
Fibrates
ACCORD Fenofibrate had no significant effect on CV endpoints when added to a
statin in patients with diabetes
36
37
38
39
40
41
42
Baseline Study end
Placebo Fenofibrate
Mea
n H
DL-
C
chol
este
rol (
mg
dL)
100
120
140
160
180
Baseline Study end
Placebo Fenofibrate
Mea
n TG
s (m
gdL
)
224
258
132
038
147
241
270
144
036
161
00
05
10
15
20
25
30
Primary outcome Major coronary eventdagger Nonfatal MI Stroke All-cause mortality
Fenofibrate Placebo
Out
com
e ra
tey
r(
) p=NS for all endpoints(Primary outcome HR 092 95 CI 079 to 108 p=032 ARR 017 per year NNT 588 to avoid one event over 1 year)
p=001
plt0001
ACCORD fenofibrate (starting dose 160 mgd) vs placebo in 5518 patients with type 2 diabetes treated with open-label simvastatin (mean follow-up 47 years)
Ginsberg HN et al N Engl J Med 20103621563ndash1574Nonfatal MI nonfatal stroke or CV deathdaggerFatal coronary event nonfatal MI or unstable angina
Niacin
55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Look at1 Family history of premature ASCVD2 LDL-C gt160 mgdl (42mmolL)3 hsCRP ge2 mgdl4 Calcium score ge300 Agatston units or ge75th 5 Sex6 Ethnicity7 Ankle-brachial index lt098 Elevated lifetime risk of ASCVD
Stone NJ Robinson J Lichtenstein AH et al 2013 ACCAHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults A Report of the American College of CardiologyAmerican Heart Association Task Force on Practice Guidelines J Am Coll Cardiol 2013
daggerEvidence from 1 RCT only down-titration if unable to tolerate atorvastatin 80 mg in IDEAL (47)DaggerAlthough simvastatin 80 mg was evaluated in RCTs initiation of simvastatin 80 mg or titration to 80 mg is not recommended by the FDA due to the increased risk of myopathy including rhabdomyolysis
High Moderate and Low-Intensity Statin Therapy (Used in the RCTs reviewed by the Expert Panel)
High-Intensity StatinTherapy
Moderate-Intensity StatinTherapy
Low-Intensity StatinTherapy
Daily dose lowers LDLndashC by approximately ge50
Daily dose lowers LDLndashC by approximately 30 to lt50
Daily dose lowers LDLndashC by lt30
Atorvastatin (40dagger)ndash80 mg Rosuvastatin 20 (40) mg
Atorvastatin 10 (20) mg Rosuvastatin (5) 10 mg Simvastatin 20ndash40 mgDagger Pravastatin 40 (80) mg Lovastatin 40 mg Fluvastatin XL 80 mg Fluvastatin 40 mg bid Pitavastatin 2ndash4 mg
Simvastatin 10 mg Pravastatin 10ndash20 mg Lovastatin 20 mg Fluvastatin 20ndash40 mg Pitavastatin 1 mg
Treat patients aggressively with the right statin dose and intensity for the patients thatrsquos been proven to benefit most from statin treatment
LDL-C targets should NOT be the ONLY determination factor to initiate statin treatment Treat to reduce the CV risk and not just the LDL-C numbers alone
Jones P et al Comparison of the efficacy and safety of rosuvastatin versus atorvastatin simvastatin and pravastatin across doses (STELLAR Trial) Am J Cardiol 200392152-160
The STELLAR study
Rosuvastatin
Atorvastatin
Simvastatin
Pravastatin
X
X
X
ndash60
ndash50
ndash40
ndash30
ndash20
ndash10
0
Dose mg (log scale)10 20 40 80
X
n = 648
n = 473n = 634
n = 485
daggerDagger
Cha
nge
in L
DL-
C fr
om
base
line
() X
Plt002 vs atorvastatin 10 mg simvastatin 10 20 40 mg pravastatin 10 20 40 mgdaggerPlt002 vs atorvastatin 20 40 mg simvastatin 20 40 80 mg pravastatin 20 40 mgDaggerPlt002 vs atorvastatin 40 mg simvastatin 40 80 mg pravastatin 40 mg
dagger
Dagger
Scandinavian Simvastatin Survival Study Group Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease the Scandinavian Simvastatin Survival Study (4S) Lancet 19943441383-1389
085
080
000
00
100
095
090
Pro
porti
on a
live
Years since randomisation
Placebo
Simvastatin
64321 5
Log rank P = 0003
Non-statins have been investigated for potential benefit in atherosclerotic cardiovascular disease (ASCVD)
This presentation surveys the clinical evidence to date
bull Cholesterol absorption inhibitors (ezetimibe)
bull Fibrates
bull Omega-3 polyunsaturated fatty acids (PUFAs)
bull Niacin
bull Emerging products
bull PCSK9 inhibitors
bull Cholesterylester transfer protein (CETP) inhibitors
ACCAHA guidelines (2014) do not support routine use of non-statins alone or in combination with statins1
Benefits not acceptable relative to potential adverse effects NICE lipid guidelines (2014) recommend against
non-statins23
No evidence of benefit ESCEAS guidelines (2012) recommend non-statins in limited
situations4
Lipid target not reached with maximally tolerated statin
Statin not tolerated 1 Stone NJ et al J Am Coll Cardiol 2014632889ndash29342 Rabar S et al BMJ 2014349g4356 doi101136bmjg4356
3 National Institute for Health and Care ExcellenceLipid modification July 2014 httpwwwniceorgukGuidanceCG181
4 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash1701
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
FIELD Fenofibrate did not reduce primary outcome (CHD death or nonfatal
MI) in patients with diabetes
FIELD fenofibrate 200 mgd vs placebo in 9795 patients with type 2 diabetesMedian follow-up 5 years
307
11
193
31
11
20
26
112
187
243
113147
00
05
10
15
20
25
30
35
LDL-C HDL-C TGs
Placebo baseline Fenofibrate baseline
Placebo study end Fenofibrate study end
Mea
n lip
id le
vel (
mm
olL
)R
ate
1000
per
son-
year
s
104
44
64 64
142
119117
37
8471
129
150
02468
10121416
Primary outcome CHD mortality Nonfatal MI Stroke All-cause mortality Coronary revascularization
Fenofibrate PlaceboHR 089
95 CI 075 to 105p=016dagger
p=022
p=036
p=018
HR 07695 CI 062 to 094
p=001
HR 07995 CI 068 to 093
p=0003
Keech A et al Lancet 20053661849ndash1861
CHD mortality or nonfatal MIdaggerARR over course of study=07 NNT=143NNT number needed to treat
Keech p7 ndash 1E
Meta-analysis Fibrates may reduce CV events
but not all-cause mortality
151005
090 (082 to 100) p=0048I2=470 p for heterogeneity=0110
087 (081 to 093) plt00001I2=221 p for heterogeneity=0202
081 (075 to 089) plt00001I2=145 p for heterogeneity=0310
100 (093 to 108) p=0918I2=194 p for heterogeneity=0237
Relative risk (95 CI)
5Major CV events
16Coronary event
10Nonfatal coronary events
16All-cause mortality
Number of studies included
Favors placeboFavors fibrateRelative risk (95 CI)
Jun M et al Lancet 20103621563ndash1574Reprinted from The Lancet Volume 362 Jun M et al Effects of fibrates on cardiovascular outcomes
a systematic review and meta-analysis 1563ndash1574 Copyright 2010 with permission from ElsevierMI and stroke
Meta-analysis of 18 placebo-controlled fibrate trials (45 058 patients)
Docosahexenoic acid (DHA)
Eicosapentenoic acid (EPA)
PUFAs Found in fish oil and Mediterranean diet1
Have been used to lower TG1
Omega-3 fatty acids
EPA1
Marketed omega-3 fatty acids include Vascepa (ethyl-EPA)2
Lovaza (mixture of ethyl-esterified EPA DHA and other fish oils)3
1 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash17012 Vascepa Prescribing Information httpwwwdrugscomprovascepahtml
3 Lovaza Prescribing Information httpswwwgsksourcecomgskprmhtdocsdocumentsLOVAZA-PI-PILPDF
Placebo-controlled trials of omega-3 fatty acids
have reported beneficial effects on CV outcomes
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin vs placebo
DART1Men previous MI(n=2033)
Dietary fish intakeMean 2 years
No significant change in total-C over 2 years
All-cause mortality darr29 (plt005)
GISSI-P2 Recent MI (n=11 324)
Omega-3 PUFA1 gd vs control Mean 35 years
LDL-C uarr99 (p=0002) HDL-C uarr88 (p=NS)TGs darr34 (p=0001)
Death nonfatal MI or nonfatal stroke darr10 (p=0048)
GISSI-HF3 Chronic HF(n=6975)
Omega-3 PUFA1 gd vs placebo Median 39 years
TGs darr from 142 to 134 mmolL over 3 years with PUFA (plt00001 vs placebo)
All-cause death darr9 (p=0041)All-cause death or CV hospitalization darr8 (p=0009)
1 Burr ML et al Lancet 19892757ndash7612 GISSI-Prevenzione Investigators Lancet 1999354447ndash455
3 GISSI-HF Investigators Lancet 20083721223ndash1230
Statin use was 5 at study baseline rising to 46 after 42 monthsrsquo follow-upPatients were also randomized to rosuvastatin or placebo no interaction was recorded between PUFA and statin
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Cholesterol absorption inhibitor
Ezetimibe
ENHANCE Simvastatin + ezetimibe did not significantly reduce intima-medial
thickness vs simvastatin alone
00111
00058
0000
0005
0010
0015
Simvastatin + ezetimibe Simvastatin + placebo
Diff
eren
ce fr
om b
asel
ine
at M
onth
24
(mm
)
p=029
44
46
48
50
52
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Mea
n H
DL-
C (m
gdL
)
100
120
140
160
180
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Med
ian
TGs
(mg
dL)
0
100
200
300
400
Baseline Month 24
Simvastatin + placebo
Simvastatin + ezetimibe
Mea
n LD
L-C
(mg
dL)
plt001
p=078
plt001
Primary endpointChange in carotid intima-medial thickness at
Month 24
ENHANCE ezetimibe 10 mgd vs placebo (added to simvastatin 80 mgd) in 720 patients with familial hypercholesterolemia (follow-up 24 months)1
1 Kastelein JJP et al N Engl J Med 20083581431ndash14432 Zocor (simvastatin calcium) Prescribing Information Merck Sharp amp Dohme Ltd October 2012No longer a recommended dose of simvastatin2
Fibrates
ACCORD Fenofibrate had no significant effect on CV endpoints when added to a
statin in patients with diabetes
36
37
38
39
40
41
42
Baseline Study end
Placebo Fenofibrate
Mea
n H
DL-
C
chol
este
rol (
mg
dL)
100
120
140
160
180
Baseline Study end
Placebo Fenofibrate
Mea
n TG
s (m
gdL
)
224
258
132
038
147
241
270
144
036
161
00
05
10
15
20
25
30
Primary outcome Major coronary eventdagger Nonfatal MI Stroke All-cause mortality
Fenofibrate Placebo
Out
com
e ra
tey
r(
) p=NS for all endpoints(Primary outcome HR 092 95 CI 079 to 108 p=032 ARR 017 per year NNT 588 to avoid one event over 1 year)
p=001
plt0001
ACCORD fenofibrate (starting dose 160 mgd) vs placebo in 5518 patients with type 2 diabetes treated with open-label simvastatin (mean follow-up 47 years)
Ginsberg HN et al N Engl J Med 20103621563ndash1574Nonfatal MI nonfatal stroke or CV deathdaggerFatal coronary event nonfatal MI or unstable angina
Niacin
55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Stone NJ Robinson J Lichtenstein AH et al 2013 ACCAHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults A Report of the American College of CardiologyAmerican Heart Association Task Force on Practice Guidelines J Am Coll Cardiol 2013
daggerEvidence from 1 RCT only down-titration if unable to tolerate atorvastatin 80 mg in IDEAL (47)DaggerAlthough simvastatin 80 mg was evaluated in RCTs initiation of simvastatin 80 mg or titration to 80 mg is not recommended by the FDA due to the increased risk of myopathy including rhabdomyolysis
High Moderate and Low-Intensity Statin Therapy (Used in the RCTs reviewed by the Expert Panel)
High-Intensity StatinTherapy
Moderate-Intensity StatinTherapy
Low-Intensity StatinTherapy
Daily dose lowers LDLndashC by approximately ge50
Daily dose lowers LDLndashC by approximately 30 to lt50
Daily dose lowers LDLndashC by lt30
Atorvastatin (40dagger)ndash80 mg Rosuvastatin 20 (40) mg
Atorvastatin 10 (20) mg Rosuvastatin (5) 10 mg Simvastatin 20ndash40 mgDagger Pravastatin 40 (80) mg Lovastatin 40 mg Fluvastatin XL 80 mg Fluvastatin 40 mg bid Pitavastatin 2ndash4 mg
Simvastatin 10 mg Pravastatin 10ndash20 mg Lovastatin 20 mg Fluvastatin 20ndash40 mg Pitavastatin 1 mg
Treat patients aggressively with the right statin dose and intensity for the patients thatrsquos been proven to benefit most from statin treatment
LDL-C targets should NOT be the ONLY determination factor to initiate statin treatment Treat to reduce the CV risk and not just the LDL-C numbers alone
Jones P et al Comparison of the efficacy and safety of rosuvastatin versus atorvastatin simvastatin and pravastatin across doses (STELLAR Trial) Am J Cardiol 200392152-160
The STELLAR study
Rosuvastatin
Atorvastatin
Simvastatin
Pravastatin
X
X
X
ndash60
ndash50
ndash40
ndash30
ndash20
ndash10
0
Dose mg (log scale)10 20 40 80
X
n = 648
n = 473n = 634
n = 485
daggerDagger
Cha
nge
in L
DL-
C fr
om
base
line
() X
Plt002 vs atorvastatin 10 mg simvastatin 10 20 40 mg pravastatin 10 20 40 mgdaggerPlt002 vs atorvastatin 20 40 mg simvastatin 20 40 80 mg pravastatin 20 40 mgDaggerPlt002 vs atorvastatin 40 mg simvastatin 40 80 mg pravastatin 40 mg
dagger
Dagger
Scandinavian Simvastatin Survival Study Group Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease the Scandinavian Simvastatin Survival Study (4S) Lancet 19943441383-1389
085
080
000
00
100
095
090
Pro
porti
on a
live
Years since randomisation
Placebo
Simvastatin
64321 5
Log rank P = 0003
Non-statins have been investigated for potential benefit in atherosclerotic cardiovascular disease (ASCVD)
This presentation surveys the clinical evidence to date
bull Cholesterol absorption inhibitors (ezetimibe)
bull Fibrates
bull Omega-3 polyunsaturated fatty acids (PUFAs)
bull Niacin
bull Emerging products
bull PCSK9 inhibitors
bull Cholesterylester transfer protein (CETP) inhibitors
ACCAHA guidelines (2014) do not support routine use of non-statins alone or in combination with statins1
Benefits not acceptable relative to potential adverse effects NICE lipid guidelines (2014) recommend against
non-statins23
No evidence of benefit ESCEAS guidelines (2012) recommend non-statins in limited
situations4
Lipid target not reached with maximally tolerated statin
Statin not tolerated 1 Stone NJ et al J Am Coll Cardiol 2014632889ndash29342 Rabar S et al BMJ 2014349g4356 doi101136bmjg4356
3 National Institute for Health and Care ExcellenceLipid modification July 2014 httpwwwniceorgukGuidanceCG181
4 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash1701
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
FIELD Fenofibrate did not reduce primary outcome (CHD death or nonfatal
MI) in patients with diabetes
FIELD fenofibrate 200 mgd vs placebo in 9795 patients with type 2 diabetesMedian follow-up 5 years
307
11
193
31
11
20
26
112
187
243
113147
00
05
10
15
20
25
30
35
LDL-C HDL-C TGs
Placebo baseline Fenofibrate baseline
Placebo study end Fenofibrate study end
Mea
n lip
id le
vel (
mm
olL
)R
ate
1000
per
son-
year
s
104
44
64 64
142
119117
37
8471
129
150
02468
10121416
Primary outcome CHD mortality Nonfatal MI Stroke All-cause mortality Coronary revascularization
Fenofibrate PlaceboHR 089
95 CI 075 to 105p=016dagger
p=022
p=036
p=018
HR 07695 CI 062 to 094
p=001
HR 07995 CI 068 to 093
p=0003
Keech A et al Lancet 20053661849ndash1861
CHD mortality or nonfatal MIdaggerARR over course of study=07 NNT=143NNT number needed to treat
Keech p7 ndash 1E
Meta-analysis Fibrates may reduce CV events
but not all-cause mortality
151005
090 (082 to 100) p=0048I2=470 p for heterogeneity=0110
087 (081 to 093) plt00001I2=221 p for heterogeneity=0202
081 (075 to 089) plt00001I2=145 p for heterogeneity=0310
100 (093 to 108) p=0918I2=194 p for heterogeneity=0237
Relative risk (95 CI)
5Major CV events
16Coronary event
10Nonfatal coronary events
16All-cause mortality
Number of studies included
Favors placeboFavors fibrateRelative risk (95 CI)
Jun M et al Lancet 20103621563ndash1574Reprinted from The Lancet Volume 362 Jun M et al Effects of fibrates on cardiovascular outcomes
a systematic review and meta-analysis 1563ndash1574 Copyright 2010 with permission from ElsevierMI and stroke
Meta-analysis of 18 placebo-controlled fibrate trials (45 058 patients)
Docosahexenoic acid (DHA)
Eicosapentenoic acid (EPA)
PUFAs Found in fish oil and Mediterranean diet1
Have been used to lower TG1
Omega-3 fatty acids
EPA1
Marketed omega-3 fatty acids include Vascepa (ethyl-EPA)2
Lovaza (mixture of ethyl-esterified EPA DHA and other fish oils)3
1 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash17012 Vascepa Prescribing Information httpwwwdrugscomprovascepahtml
3 Lovaza Prescribing Information httpswwwgsksourcecomgskprmhtdocsdocumentsLOVAZA-PI-PILPDF
Placebo-controlled trials of omega-3 fatty acids
have reported beneficial effects on CV outcomes
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin vs placebo
DART1Men previous MI(n=2033)
Dietary fish intakeMean 2 years
No significant change in total-C over 2 years
All-cause mortality darr29 (plt005)
GISSI-P2 Recent MI (n=11 324)
Omega-3 PUFA1 gd vs control Mean 35 years
LDL-C uarr99 (p=0002) HDL-C uarr88 (p=NS)TGs darr34 (p=0001)
Death nonfatal MI or nonfatal stroke darr10 (p=0048)
GISSI-HF3 Chronic HF(n=6975)
Omega-3 PUFA1 gd vs placebo Median 39 years
TGs darr from 142 to 134 mmolL over 3 years with PUFA (plt00001 vs placebo)
All-cause death darr9 (p=0041)All-cause death or CV hospitalization darr8 (p=0009)
1 Burr ML et al Lancet 19892757ndash7612 GISSI-Prevenzione Investigators Lancet 1999354447ndash455
3 GISSI-HF Investigators Lancet 20083721223ndash1230
Statin use was 5 at study baseline rising to 46 after 42 monthsrsquo follow-upPatients were also randomized to rosuvastatin or placebo no interaction was recorded between PUFA and statin
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Cholesterol absorption inhibitor
Ezetimibe
ENHANCE Simvastatin + ezetimibe did not significantly reduce intima-medial
thickness vs simvastatin alone
00111
00058
0000
0005
0010
0015
Simvastatin + ezetimibe Simvastatin + placebo
Diff
eren
ce fr
om b
asel
ine
at M
onth
24
(mm
)
p=029
44
46
48
50
52
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Mea
n H
DL-
C (m
gdL
)
100
120
140
160
180
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Med
ian
TGs
(mg
dL)
0
100
200
300
400
Baseline Month 24
Simvastatin + placebo
Simvastatin + ezetimibe
Mea
n LD
L-C
(mg
dL)
plt001
p=078
plt001
Primary endpointChange in carotid intima-medial thickness at
Month 24
ENHANCE ezetimibe 10 mgd vs placebo (added to simvastatin 80 mgd) in 720 patients with familial hypercholesterolemia (follow-up 24 months)1
1 Kastelein JJP et al N Engl J Med 20083581431ndash14432 Zocor (simvastatin calcium) Prescribing Information Merck Sharp amp Dohme Ltd October 2012No longer a recommended dose of simvastatin2
Fibrates
ACCORD Fenofibrate had no significant effect on CV endpoints when added to a
statin in patients with diabetes
36
37
38
39
40
41
42
Baseline Study end
Placebo Fenofibrate
Mea
n H
DL-
C
chol
este
rol (
mg
dL)
100
120
140
160
180
Baseline Study end
Placebo Fenofibrate
Mea
n TG
s (m
gdL
)
224
258
132
038
147
241
270
144
036
161
00
05
10
15
20
25
30
Primary outcome Major coronary eventdagger Nonfatal MI Stroke All-cause mortality
Fenofibrate Placebo
Out
com
e ra
tey
r(
) p=NS for all endpoints(Primary outcome HR 092 95 CI 079 to 108 p=032 ARR 017 per year NNT 588 to avoid one event over 1 year)
p=001
plt0001
ACCORD fenofibrate (starting dose 160 mgd) vs placebo in 5518 patients with type 2 diabetes treated with open-label simvastatin (mean follow-up 47 years)
Ginsberg HN et al N Engl J Med 20103621563ndash1574Nonfatal MI nonfatal stroke or CV deathdaggerFatal coronary event nonfatal MI or unstable angina
Niacin
55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Treat patients aggressively with the right statin dose and intensity for the patients thatrsquos been proven to benefit most from statin treatment
LDL-C targets should NOT be the ONLY determination factor to initiate statin treatment Treat to reduce the CV risk and not just the LDL-C numbers alone
Jones P et al Comparison of the efficacy and safety of rosuvastatin versus atorvastatin simvastatin and pravastatin across doses (STELLAR Trial) Am J Cardiol 200392152-160
The STELLAR study
Rosuvastatin
Atorvastatin
Simvastatin
Pravastatin
X
X
X
ndash60
ndash50
ndash40
ndash30
ndash20
ndash10
0
Dose mg (log scale)10 20 40 80
X
n = 648
n = 473n = 634
n = 485
daggerDagger
Cha
nge
in L
DL-
C fr
om
base
line
() X
Plt002 vs atorvastatin 10 mg simvastatin 10 20 40 mg pravastatin 10 20 40 mgdaggerPlt002 vs atorvastatin 20 40 mg simvastatin 20 40 80 mg pravastatin 20 40 mgDaggerPlt002 vs atorvastatin 40 mg simvastatin 40 80 mg pravastatin 40 mg
dagger
Dagger
Scandinavian Simvastatin Survival Study Group Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease the Scandinavian Simvastatin Survival Study (4S) Lancet 19943441383-1389
085
080
000
00
100
095
090
Pro
porti
on a
live
Years since randomisation
Placebo
Simvastatin
64321 5
Log rank P = 0003
Non-statins have been investigated for potential benefit in atherosclerotic cardiovascular disease (ASCVD)
This presentation surveys the clinical evidence to date
bull Cholesterol absorption inhibitors (ezetimibe)
bull Fibrates
bull Omega-3 polyunsaturated fatty acids (PUFAs)
bull Niacin
bull Emerging products
bull PCSK9 inhibitors
bull Cholesterylester transfer protein (CETP) inhibitors
ACCAHA guidelines (2014) do not support routine use of non-statins alone or in combination with statins1
Benefits not acceptable relative to potential adverse effects NICE lipid guidelines (2014) recommend against
non-statins23
No evidence of benefit ESCEAS guidelines (2012) recommend non-statins in limited
situations4
Lipid target not reached with maximally tolerated statin
Statin not tolerated 1 Stone NJ et al J Am Coll Cardiol 2014632889ndash29342 Rabar S et al BMJ 2014349g4356 doi101136bmjg4356
3 National Institute for Health and Care ExcellenceLipid modification July 2014 httpwwwniceorgukGuidanceCG181
4 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash1701
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
FIELD Fenofibrate did not reduce primary outcome (CHD death or nonfatal
MI) in patients with diabetes
FIELD fenofibrate 200 mgd vs placebo in 9795 patients with type 2 diabetesMedian follow-up 5 years
307
11
193
31
11
20
26
112
187
243
113147
00
05
10
15
20
25
30
35
LDL-C HDL-C TGs
Placebo baseline Fenofibrate baseline
Placebo study end Fenofibrate study end
Mea
n lip
id le
vel (
mm
olL
)R
ate
1000
per
son-
year
s
104
44
64 64
142
119117
37
8471
129
150
02468
10121416
Primary outcome CHD mortality Nonfatal MI Stroke All-cause mortality Coronary revascularization
Fenofibrate PlaceboHR 089
95 CI 075 to 105p=016dagger
p=022
p=036
p=018
HR 07695 CI 062 to 094
p=001
HR 07995 CI 068 to 093
p=0003
Keech A et al Lancet 20053661849ndash1861
CHD mortality or nonfatal MIdaggerARR over course of study=07 NNT=143NNT number needed to treat
Keech p7 ndash 1E
Meta-analysis Fibrates may reduce CV events
but not all-cause mortality
151005
090 (082 to 100) p=0048I2=470 p for heterogeneity=0110
087 (081 to 093) plt00001I2=221 p for heterogeneity=0202
081 (075 to 089) plt00001I2=145 p for heterogeneity=0310
100 (093 to 108) p=0918I2=194 p for heterogeneity=0237
Relative risk (95 CI)
5Major CV events
16Coronary event
10Nonfatal coronary events
16All-cause mortality
Number of studies included
Favors placeboFavors fibrateRelative risk (95 CI)
Jun M et al Lancet 20103621563ndash1574Reprinted from The Lancet Volume 362 Jun M et al Effects of fibrates on cardiovascular outcomes
a systematic review and meta-analysis 1563ndash1574 Copyright 2010 with permission from ElsevierMI and stroke
Meta-analysis of 18 placebo-controlled fibrate trials (45 058 patients)
Docosahexenoic acid (DHA)
Eicosapentenoic acid (EPA)
PUFAs Found in fish oil and Mediterranean diet1
Have been used to lower TG1
Omega-3 fatty acids
EPA1
Marketed omega-3 fatty acids include Vascepa (ethyl-EPA)2
Lovaza (mixture of ethyl-esterified EPA DHA and other fish oils)3
1 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash17012 Vascepa Prescribing Information httpwwwdrugscomprovascepahtml
3 Lovaza Prescribing Information httpswwwgsksourcecomgskprmhtdocsdocumentsLOVAZA-PI-PILPDF
Placebo-controlled trials of omega-3 fatty acids
have reported beneficial effects on CV outcomes
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin vs placebo
DART1Men previous MI(n=2033)
Dietary fish intakeMean 2 years
No significant change in total-C over 2 years
All-cause mortality darr29 (plt005)
GISSI-P2 Recent MI (n=11 324)
Omega-3 PUFA1 gd vs control Mean 35 years
LDL-C uarr99 (p=0002) HDL-C uarr88 (p=NS)TGs darr34 (p=0001)
Death nonfatal MI or nonfatal stroke darr10 (p=0048)
GISSI-HF3 Chronic HF(n=6975)
Omega-3 PUFA1 gd vs placebo Median 39 years
TGs darr from 142 to 134 mmolL over 3 years with PUFA (plt00001 vs placebo)
All-cause death darr9 (p=0041)All-cause death or CV hospitalization darr8 (p=0009)
1 Burr ML et al Lancet 19892757ndash7612 GISSI-Prevenzione Investigators Lancet 1999354447ndash455
3 GISSI-HF Investigators Lancet 20083721223ndash1230
Statin use was 5 at study baseline rising to 46 after 42 monthsrsquo follow-upPatients were also randomized to rosuvastatin or placebo no interaction was recorded between PUFA and statin
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Cholesterol absorption inhibitor
Ezetimibe
ENHANCE Simvastatin + ezetimibe did not significantly reduce intima-medial
thickness vs simvastatin alone
00111
00058
0000
0005
0010
0015
Simvastatin + ezetimibe Simvastatin + placebo
Diff
eren
ce fr
om b
asel
ine
at M
onth
24
(mm
)
p=029
44
46
48
50
52
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Mea
n H
DL-
C (m
gdL
)
100
120
140
160
180
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Med
ian
TGs
(mg
dL)
0
100
200
300
400
Baseline Month 24
Simvastatin + placebo
Simvastatin + ezetimibe
Mea
n LD
L-C
(mg
dL)
plt001
p=078
plt001
Primary endpointChange in carotid intima-medial thickness at
Month 24
ENHANCE ezetimibe 10 mgd vs placebo (added to simvastatin 80 mgd) in 720 patients with familial hypercholesterolemia (follow-up 24 months)1
1 Kastelein JJP et al N Engl J Med 20083581431ndash14432 Zocor (simvastatin calcium) Prescribing Information Merck Sharp amp Dohme Ltd October 2012No longer a recommended dose of simvastatin2
Fibrates
ACCORD Fenofibrate had no significant effect on CV endpoints when added to a
statin in patients with diabetes
36
37
38
39
40
41
42
Baseline Study end
Placebo Fenofibrate
Mea
n H
DL-
C
chol
este
rol (
mg
dL)
100
120
140
160
180
Baseline Study end
Placebo Fenofibrate
Mea
n TG
s (m
gdL
)
224
258
132
038
147
241
270
144
036
161
00
05
10
15
20
25
30
Primary outcome Major coronary eventdagger Nonfatal MI Stroke All-cause mortality
Fenofibrate Placebo
Out
com
e ra
tey
r(
) p=NS for all endpoints(Primary outcome HR 092 95 CI 079 to 108 p=032 ARR 017 per year NNT 588 to avoid one event over 1 year)
p=001
plt0001
ACCORD fenofibrate (starting dose 160 mgd) vs placebo in 5518 patients with type 2 diabetes treated with open-label simvastatin (mean follow-up 47 years)
Ginsberg HN et al N Engl J Med 20103621563ndash1574Nonfatal MI nonfatal stroke or CV deathdaggerFatal coronary event nonfatal MI or unstable angina
Niacin
55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Jones P et al Comparison of the efficacy and safety of rosuvastatin versus atorvastatin simvastatin and pravastatin across doses (STELLAR Trial) Am J Cardiol 200392152-160
The STELLAR study
Rosuvastatin
Atorvastatin
Simvastatin
Pravastatin
X
X
X
ndash60
ndash50
ndash40
ndash30
ndash20
ndash10
0
Dose mg (log scale)10 20 40 80
X
n = 648
n = 473n = 634
n = 485
daggerDagger
Cha
nge
in L
DL-
C fr
om
base
line
() X
Plt002 vs atorvastatin 10 mg simvastatin 10 20 40 mg pravastatin 10 20 40 mgdaggerPlt002 vs atorvastatin 20 40 mg simvastatin 20 40 80 mg pravastatin 20 40 mgDaggerPlt002 vs atorvastatin 40 mg simvastatin 40 80 mg pravastatin 40 mg
dagger
Dagger
Scandinavian Simvastatin Survival Study Group Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease the Scandinavian Simvastatin Survival Study (4S) Lancet 19943441383-1389
085
080
000
00
100
095
090
Pro
porti
on a
live
Years since randomisation
Placebo
Simvastatin
64321 5
Log rank P = 0003
Non-statins have been investigated for potential benefit in atherosclerotic cardiovascular disease (ASCVD)
This presentation surveys the clinical evidence to date
bull Cholesterol absorption inhibitors (ezetimibe)
bull Fibrates
bull Omega-3 polyunsaturated fatty acids (PUFAs)
bull Niacin
bull Emerging products
bull PCSK9 inhibitors
bull Cholesterylester transfer protein (CETP) inhibitors
ACCAHA guidelines (2014) do not support routine use of non-statins alone or in combination with statins1
Benefits not acceptable relative to potential adverse effects NICE lipid guidelines (2014) recommend against
non-statins23
No evidence of benefit ESCEAS guidelines (2012) recommend non-statins in limited
situations4
Lipid target not reached with maximally tolerated statin
Statin not tolerated 1 Stone NJ et al J Am Coll Cardiol 2014632889ndash29342 Rabar S et al BMJ 2014349g4356 doi101136bmjg4356
3 National Institute for Health and Care ExcellenceLipid modification July 2014 httpwwwniceorgukGuidanceCG181
4 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash1701
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
FIELD Fenofibrate did not reduce primary outcome (CHD death or nonfatal
MI) in patients with diabetes
FIELD fenofibrate 200 mgd vs placebo in 9795 patients with type 2 diabetesMedian follow-up 5 years
307
11
193
31
11
20
26
112
187
243
113147
00
05
10
15
20
25
30
35
LDL-C HDL-C TGs
Placebo baseline Fenofibrate baseline
Placebo study end Fenofibrate study end
Mea
n lip
id le
vel (
mm
olL
)R
ate
1000
per
son-
year
s
104
44
64 64
142
119117
37
8471
129
150
02468
10121416
Primary outcome CHD mortality Nonfatal MI Stroke All-cause mortality Coronary revascularization
Fenofibrate PlaceboHR 089
95 CI 075 to 105p=016dagger
p=022
p=036
p=018
HR 07695 CI 062 to 094
p=001
HR 07995 CI 068 to 093
p=0003
Keech A et al Lancet 20053661849ndash1861
CHD mortality or nonfatal MIdaggerARR over course of study=07 NNT=143NNT number needed to treat
Keech p7 ndash 1E
Meta-analysis Fibrates may reduce CV events
but not all-cause mortality
151005
090 (082 to 100) p=0048I2=470 p for heterogeneity=0110
087 (081 to 093) plt00001I2=221 p for heterogeneity=0202
081 (075 to 089) plt00001I2=145 p for heterogeneity=0310
100 (093 to 108) p=0918I2=194 p for heterogeneity=0237
Relative risk (95 CI)
5Major CV events
16Coronary event
10Nonfatal coronary events
16All-cause mortality
Number of studies included
Favors placeboFavors fibrateRelative risk (95 CI)
Jun M et al Lancet 20103621563ndash1574Reprinted from The Lancet Volume 362 Jun M et al Effects of fibrates on cardiovascular outcomes
a systematic review and meta-analysis 1563ndash1574 Copyright 2010 with permission from ElsevierMI and stroke
Meta-analysis of 18 placebo-controlled fibrate trials (45 058 patients)
Docosahexenoic acid (DHA)
Eicosapentenoic acid (EPA)
PUFAs Found in fish oil and Mediterranean diet1
Have been used to lower TG1
Omega-3 fatty acids
EPA1
Marketed omega-3 fatty acids include Vascepa (ethyl-EPA)2
Lovaza (mixture of ethyl-esterified EPA DHA and other fish oils)3
1 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash17012 Vascepa Prescribing Information httpwwwdrugscomprovascepahtml
3 Lovaza Prescribing Information httpswwwgsksourcecomgskprmhtdocsdocumentsLOVAZA-PI-PILPDF
Placebo-controlled trials of omega-3 fatty acids
have reported beneficial effects on CV outcomes
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin vs placebo
DART1Men previous MI(n=2033)
Dietary fish intakeMean 2 years
No significant change in total-C over 2 years
All-cause mortality darr29 (plt005)
GISSI-P2 Recent MI (n=11 324)
Omega-3 PUFA1 gd vs control Mean 35 years
LDL-C uarr99 (p=0002) HDL-C uarr88 (p=NS)TGs darr34 (p=0001)
Death nonfatal MI or nonfatal stroke darr10 (p=0048)
GISSI-HF3 Chronic HF(n=6975)
Omega-3 PUFA1 gd vs placebo Median 39 years
TGs darr from 142 to 134 mmolL over 3 years with PUFA (plt00001 vs placebo)
All-cause death darr9 (p=0041)All-cause death or CV hospitalization darr8 (p=0009)
1 Burr ML et al Lancet 19892757ndash7612 GISSI-Prevenzione Investigators Lancet 1999354447ndash455
3 GISSI-HF Investigators Lancet 20083721223ndash1230
Statin use was 5 at study baseline rising to 46 after 42 monthsrsquo follow-upPatients were also randomized to rosuvastatin or placebo no interaction was recorded between PUFA and statin
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Cholesterol absorption inhibitor
Ezetimibe
ENHANCE Simvastatin + ezetimibe did not significantly reduce intima-medial
thickness vs simvastatin alone
00111
00058
0000
0005
0010
0015
Simvastatin + ezetimibe Simvastatin + placebo
Diff
eren
ce fr
om b
asel
ine
at M
onth
24
(mm
)
p=029
44
46
48
50
52
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Mea
n H
DL-
C (m
gdL
)
100
120
140
160
180
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Med
ian
TGs
(mg
dL)
0
100
200
300
400
Baseline Month 24
Simvastatin + placebo
Simvastatin + ezetimibe
Mea
n LD
L-C
(mg
dL)
plt001
p=078
plt001
Primary endpointChange in carotid intima-medial thickness at
Month 24
ENHANCE ezetimibe 10 mgd vs placebo (added to simvastatin 80 mgd) in 720 patients with familial hypercholesterolemia (follow-up 24 months)1
1 Kastelein JJP et al N Engl J Med 20083581431ndash14432 Zocor (simvastatin calcium) Prescribing Information Merck Sharp amp Dohme Ltd October 2012No longer a recommended dose of simvastatin2
Fibrates
ACCORD Fenofibrate had no significant effect on CV endpoints when added to a
statin in patients with diabetes
36
37
38
39
40
41
42
Baseline Study end
Placebo Fenofibrate
Mea
n H
DL-
C
chol
este
rol (
mg
dL)
100
120
140
160
180
Baseline Study end
Placebo Fenofibrate
Mea
n TG
s (m
gdL
)
224
258
132
038
147
241
270
144
036
161
00
05
10
15
20
25
30
Primary outcome Major coronary eventdagger Nonfatal MI Stroke All-cause mortality
Fenofibrate Placebo
Out
com
e ra
tey
r(
) p=NS for all endpoints(Primary outcome HR 092 95 CI 079 to 108 p=032 ARR 017 per year NNT 588 to avoid one event over 1 year)
p=001
plt0001
ACCORD fenofibrate (starting dose 160 mgd) vs placebo in 5518 patients with type 2 diabetes treated with open-label simvastatin (mean follow-up 47 years)
Ginsberg HN et al N Engl J Med 20103621563ndash1574Nonfatal MI nonfatal stroke or CV deathdaggerFatal coronary event nonfatal MI or unstable angina
Niacin
55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Scandinavian Simvastatin Survival Study Group Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease the Scandinavian Simvastatin Survival Study (4S) Lancet 19943441383-1389
085
080
000
00
100
095
090
Pro
porti
on a
live
Years since randomisation
Placebo
Simvastatin
64321 5
Log rank P = 0003
Non-statins have been investigated for potential benefit in atherosclerotic cardiovascular disease (ASCVD)
This presentation surveys the clinical evidence to date
bull Cholesterol absorption inhibitors (ezetimibe)
bull Fibrates
bull Omega-3 polyunsaturated fatty acids (PUFAs)
bull Niacin
bull Emerging products
bull PCSK9 inhibitors
bull Cholesterylester transfer protein (CETP) inhibitors
ACCAHA guidelines (2014) do not support routine use of non-statins alone or in combination with statins1
Benefits not acceptable relative to potential adverse effects NICE lipid guidelines (2014) recommend against
non-statins23
No evidence of benefit ESCEAS guidelines (2012) recommend non-statins in limited
situations4
Lipid target not reached with maximally tolerated statin
Statin not tolerated 1 Stone NJ et al J Am Coll Cardiol 2014632889ndash29342 Rabar S et al BMJ 2014349g4356 doi101136bmjg4356
3 National Institute for Health and Care ExcellenceLipid modification July 2014 httpwwwniceorgukGuidanceCG181
4 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash1701
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
FIELD Fenofibrate did not reduce primary outcome (CHD death or nonfatal
MI) in patients with diabetes
FIELD fenofibrate 200 mgd vs placebo in 9795 patients with type 2 diabetesMedian follow-up 5 years
307
11
193
31
11
20
26
112
187
243
113147
00
05
10
15
20
25
30
35
LDL-C HDL-C TGs
Placebo baseline Fenofibrate baseline
Placebo study end Fenofibrate study end
Mea
n lip
id le
vel (
mm
olL
)R
ate
1000
per
son-
year
s
104
44
64 64
142
119117
37
8471
129
150
02468
10121416
Primary outcome CHD mortality Nonfatal MI Stroke All-cause mortality Coronary revascularization
Fenofibrate PlaceboHR 089
95 CI 075 to 105p=016dagger
p=022
p=036
p=018
HR 07695 CI 062 to 094
p=001
HR 07995 CI 068 to 093
p=0003
Keech A et al Lancet 20053661849ndash1861
CHD mortality or nonfatal MIdaggerARR over course of study=07 NNT=143NNT number needed to treat
Keech p7 ndash 1E
Meta-analysis Fibrates may reduce CV events
but not all-cause mortality
151005
090 (082 to 100) p=0048I2=470 p for heterogeneity=0110
087 (081 to 093) plt00001I2=221 p for heterogeneity=0202
081 (075 to 089) plt00001I2=145 p for heterogeneity=0310
100 (093 to 108) p=0918I2=194 p for heterogeneity=0237
Relative risk (95 CI)
5Major CV events
16Coronary event
10Nonfatal coronary events
16All-cause mortality
Number of studies included
Favors placeboFavors fibrateRelative risk (95 CI)
Jun M et al Lancet 20103621563ndash1574Reprinted from The Lancet Volume 362 Jun M et al Effects of fibrates on cardiovascular outcomes
a systematic review and meta-analysis 1563ndash1574 Copyright 2010 with permission from ElsevierMI and stroke
Meta-analysis of 18 placebo-controlled fibrate trials (45 058 patients)
Docosahexenoic acid (DHA)
Eicosapentenoic acid (EPA)
PUFAs Found in fish oil and Mediterranean diet1
Have been used to lower TG1
Omega-3 fatty acids
EPA1
Marketed omega-3 fatty acids include Vascepa (ethyl-EPA)2
Lovaza (mixture of ethyl-esterified EPA DHA and other fish oils)3
1 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash17012 Vascepa Prescribing Information httpwwwdrugscomprovascepahtml
3 Lovaza Prescribing Information httpswwwgsksourcecomgskprmhtdocsdocumentsLOVAZA-PI-PILPDF
Placebo-controlled trials of omega-3 fatty acids
have reported beneficial effects on CV outcomes
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin vs placebo
DART1Men previous MI(n=2033)
Dietary fish intakeMean 2 years
No significant change in total-C over 2 years
All-cause mortality darr29 (plt005)
GISSI-P2 Recent MI (n=11 324)
Omega-3 PUFA1 gd vs control Mean 35 years
LDL-C uarr99 (p=0002) HDL-C uarr88 (p=NS)TGs darr34 (p=0001)
Death nonfatal MI or nonfatal stroke darr10 (p=0048)
GISSI-HF3 Chronic HF(n=6975)
Omega-3 PUFA1 gd vs placebo Median 39 years
TGs darr from 142 to 134 mmolL over 3 years with PUFA (plt00001 vs placebo)
All-cause death darr9 (p=0041)All-cause death or CV hospitalization darr8 (p=0009)
1 Burr ML et al Lancet 19892757ndash7612 GISSI-Prevenzione Investigators Lancet 1999354447ndash455
3 GISSI-HF Investigators Lancet 20083721223ndash1230
Statin use was 5 at study baseline rising to 46 after 42 monthsrsquo follow-upPatients were also randomized to rosuvastatin or placebo no interaction was recorded between PUFA and statin
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Cholesterol absorption inhibitor
Ezetimibe
ENHANCE Simvastatin + ezetimibe did not significantly reduce intima-medial
thickness vs simvastatin alone
00111
00058
0000
0005
0010
0015
Simvastatin + ezetimibe Simvastatin + placebo
Diff
eren
ce fr
om b
asel
ine
at M
onth
24
(mm
)
p=029
44
46
48
50
52
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Mea
n H
DL-
C (m
gdL
)
100
120
140
160
180
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Med
ian
TGs
(mg
dL)
0
100
200
300
400
Baseline Month 24
Simvastatin + placebo
Simvastatin + ezetimibe
Mea
n LD
L-C
(mg
dL)
plt001
p=078
plt001
Primary endpointChange in carotid intima-medial thickness at
Month 24
ENHANCE ezetimibe 10 mgd vs placebo (added to simvastatin 80 mgd) in 720 patients with familial hypercholesterolemia (follow-up 24 months)1
1 Kastelein JJP et al N Engl J Med 20083581431ndash14432 Zocor (simvastatin calcium) Prescribing Information Merck Sharp amp Dohme Ltd October 2012No longer a recommended dose of simvastatin2
Fibrates
ACCORD Fenofibrate had no significant effect on CV endpoints when added to a
statin in patients with diabetes
36
37
38
39
40
41
42
Baseline Study end
Placebo Fenofibrate
Mea
n H
DL-
C
chol
este
rol (
mg
dL)
100
120
140
160
180
Baseline Study end
Placebo Fenofibrate
Mea
n TG
s (m
gdL
)
224
258
132
038
147
241
270
144
036
161
00
05
10
15
20
25
30
Primary outcome Major coronary eventdagger Nonfatal MI Stroke All-cause mortality
Fenofibrate Placebo
Out
com
e ra
tey
r(
) p=NS for all endpoints(Primary outcome HR 092 95 CI 079 to 108 p=032 ARR 017 per year NNT 588 to avoid one event over 1 year)
p=001
plt0001
ACCORD fenofibrate (starting dose 160 mgd) vs placebo in 5518 patients with type 2 diabetes treated with open-label simvastatin (mean follow-up 47 years)
Ginsberg HN et al N Engl J Med 20103621563ndash1574Nonfatal MI nonfatal stroke or CV deathdaggerFatal coronary event nonfatal MI or unstable angina
Niacin
55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Non-statins have been investigated for potential benefit in atherosclerotic cardiovascular disease (ASCVD)
This presentation surveys the clinical evidence to date
bull Cholesterol absorption inhibitors (ezetimibe)
bull Fibrates
bull Omega-3 polyunsaturated fatty acids (PUFAs)
bull Niacin
bull Emerging products
bull PCSK9 inhibitors
bull Cholesterylester transfer protein (CETP) inhibitors
ACCAHA guidelines (2014) do not support routine use of non-statins alone or in combination with statins1
Benefits not acceptable relative to potential adverse effects NICE lipid guidelines (2014) recommend against
non-statins23
No evidence of benefit ESCEAS guidelines (2012) recommend non-statins in limited
situations4
Lipid target not reached with maximally tolerated statin
Statin not tolerated 1 Stone NJ et al J Am Coll Cardiol 2014632889ndash29342 Rabar S et al BMJ 2014349g4356 doi101136bmjg4356
3 National Institute for Health and Care ExcellenceLipid modification July 2014 httpwwwniceorgukGuidanceCG181
4 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash1701
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
FIELD Fenofibrate did not reduce primary outcome (CHD death or nonfatal
MI) in patients with diabetes
FIELD fenofibrate 200 mgd vs placebo in 9795 patients with type 2 diabetesMedian follow-up 5 years
307
11
193
31
11
20
26
112
187
243
113147
00
05
10
15
20
25
30
35
LDL-C HDL-C TGs
Placebo baseline Fenofibrate baseline
Placebo study end Fenofibrate study end
Mea
n lip
id le
vel (
mm
olL
)R
ate
1000
per
son-
year
s
104
44
64 64
142
119117
37
8471
129
150
02468
10121416
Primary outcome CHD mortality Nonfatal MI Stroke All-cause mortality Coronary revascularization
Fenofibrate PlaceboHR 089
95 CI 075 to 105p=016dagger
p=022
p=036
p=018
HR 07695 CI 062 to 094
p=001
HR 07995 CI 068 to 093
p=0003
Keech A et al Lancet 20053661849ndash1861
CHD mortality or nonfatal MIdaggerARR over course of study=07 NNT=143NNT number needed to treat
Keech p7 ndash 1E
Meta-analysis Fibrates may reduce CV events
but not all-cause mortality
151005
090 (082 to 100) p=0048I2=470 p for heterogeneity=0110
087 (081 to 093) plt00001I2=221 p for heterogeneity=0202
081 (075 to 089) plt00001I2=145 p for heterogeneity=0310
100 (093 to 108) p=0918I2=194 p for heterogeneity=0237
Relative risk (95 CI)
5Major CV events
16Coronary event
10Nonfatal coronary events
16All-cause mortality
Number of studies included
Favors placeboFavors fibrateRelative risk (95 CI)
Jun M et al Lancet 20103621563ndash1574Reprinted from The Lancet Volume 362 Jun M et al Effects of fibrates on cardiovascular outcomes
a systematic review and meta-analysis 1563ndash1574 Copyright 2010 with permission from ElsevierMI and stroke
Meta-analysis of 18 placebo-controlled fibrate trials (45 058 patients)
Docosahexenoic acid (DHA)
Eicosapentenoic acid (EPA)
PUFAs Found in fish oil and Mediterranean diet1
Have been used to lower TG1
Omega-3 fatty acids
EPA1
Marketed omega-3 fatty acids include Vascepa (ethyl-EPA)2
Lovaza (mixture of ethyl-esterified EPA DHA and other fish oils)3
1 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash17012 Vascepa Prescribing Information httpwwwdrugscomprovascepahtml
3 Lovaza Prescribing Information httpswwwgsksourcecomgskprmhtdocsdocumentsLOVAZA-PI-PILPDF
Placebo-controlled trials of omega-3 fatty acids
have reported beneficial effects on CV outcomes
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin vs placebo
DART1Men previous MI(n=2033)
Dietary fish intakeMean 2 years
No significant change in total-C over 2 years
All-cause mortality darr29 (plt005)
GISSI-P2 Recent MI (n=11 324)
Omega-3 PUFA1 gd vs control Mean 35 years
LDL-C uarr99 (p=0002) HDL-C uarr88 (p=NS)TGs darr34 (p=0001)
Death nonfatal MI or nonfatal stroke darr10 (p=0048)
GISSI-HF3 Chronic HF(n=6975)
Omega-3 PUFA1 gd vs placebo Median 39 years
TGs darr from 142 to 134 mmolL over 3 years with PUFA (plt00001 vs placebo)
All-cause death darr9 (p=0041)All-cause death or CV hospitalization darr8 (p=0009)
1 Burr ML et al Lancet 19892757ndash7612 GISSI-Prevenzione Investigators Lancet 1999354447ndash455
3 GISSI-HF Investigators Lancet 20083721223ndash1230
Statin use was 5 at study baseline rising to 46 after 42 monthsrsquo follow-upPatients were also randomized to rosuvastatin or placebo no interaction was recorded between PUFA and statin
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Cholesterol absorption inhibitor
Ezetimibe
ENHANCE Simvastatin + ezetimibe did not significantly reduce intima-medial
thickness vs simvastatin alone
00111
00058
0000
0005
0010
0015
Simvastatin + ezetimibe Simvastatin + placebo
Diff
eren
ce fr
om b
asel
ine
at M
onth
24
(mm
)
p=029
44
46
48
50
52
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Mea
n H
DL-
C (m
gdL
)
100
120
140
160
180
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Med
ian
TGs
(mg
dL)
0
100
200
300
400
Baseline Month 24
Simvastatin + placebo
Simvastatin + ezetimibe
Mea
n LD
L-C
(mg
dL)
plt001
p=078
plt001
Primary endpointChange in carotid intima-medial thickness at
Month 24
ENHANCE ezetimibe 10 mgd vs placebo (added to simvastatin 80 mgd) in 720 patients with familial hypercholesterolemia (follow-up 24 months)1
1 Kastelein JJP et al N Engl J Med 20083581431ndash14432 Zocor (simvastatin calcium) Prescribing Information Merck Sharp amp Dohme Ltd October 2012No longer a recommended dose of simvastatin2
Fibrates
ACCORD Fenofibrate had no significant effect on CV endpoints when added to a
statin in patients with diabetes
36
37
38
39
40
41
42
Baseline Study end
Placebo Fenofibrate
Mea
n H
DL-
C
chol
este
rol (
mg
dL)
100
120
140
160
180
Baseline Study end
Placebo Fenofibrate
Mea
n TG
s (m
gdL
)
224
258
132
038
147
241
270
144
036
161
00
05
10
15
20
25
30
Primary outcome Major coronary eventdagger Nonfatal MI Stroke All-cause mortality
Fenofibrate Placebo
Out
com
e ra
tey
r(
) p=NS for all endpoints(Primary outcome HR 092 95 CI 079 to 108 p=032 ARR 017 per year NNT 588 to avoid one event over 1 year)
p=001
plt0001
ACCORD fenofibrate (starting dose 160 mgd) vs placebo in 5518 patients with type 2 diabetes treated with open-label simvastatin (mean follow-up 47 years)
Ginsberg HN et al N Engl J Med 20103621563ndash1574Nonfatal MI nonfatal stroke or CV deathdaggerFatal coronary event nonfatal MI or unstable angina
Niacin
55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

ACCAHA guidelines (2014) do not support routine use of non-statins alone or in combination with statins1
Benefits not acceptable relative to potential adverse effects NICE lipid guidelines (2014) recommend against
non-statins23
No evidence of benefit ESCEAS guidelines (2012) recommend non-statins in limited
situations4
Lipid target not reached with maximally tolerated statin
Statin not tolerated 1 Stone NJ et al J Am Coll Cardiol 2014632889ndash29342 Rabar S et al BMJ 2014349g4356 doi101136bmjg4356
3 National Institute for Health and Care ExcellenceLipid modification July 2014 httpwwwniceorgukGuidanceCG181
4 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash1701
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
FIELD Fenofibrate did not reduce primary outcome (CHD death or nonfatal
MI) in patients with diabetes
FIELD fenofibrate 200 mgd vs placebo in 9795 patients with type 2 diabetesMedian follow-up 5 years
307
11
193
31
11
20
26
112
187
243
113147
00
05
10
15
20
25
30
35
LDL-C HDL-C TGs
Placebo baseline Fenofibrate baseline
Placebo study end Fenofibrate study end
Mea
n lip
id le
vel (
mm
olL
)R
ate
1000
per
son-
year
s
104
44
64 64
142
119117
37
8471
129
150
02468
10121416
Primary outcome CHD mortality Nonfatal MI Stroke All-cause mortality Coronary revascularization
Fenofibrate PlaceboHR 089
95 CI 075 to 105p=016dagger
p=022
p=036
p=018
HR 07695 CI 062 to 094
p=001
HR 07995 CI 068 to 093
p=0003
Keech A et al Lancet 20053661849ndash1861
CHD mortality or nonfatal MIdaggerARR over course of study=07 NNT=143NNT number needed to treat
Keech p7 ndash 1E
Meta-analysis Fibrates may reduce CV events
but not all-cause mortality
151005
090 (082 to 100) p=0048I2=470 p for heterogeneity=0110
087 (081 to 093) plt00001I2=221 p for heterogeneity=0202
081 (075 to 089) plt00001I2=145 p for heterogeneity=0310
100 (093 to 108) p=0918I2=194 p for heterogeneity=0237
Relative risk (95 CI)
5Major CV events
16Coronary event
10Nonfatal coronary events
16All-cause mortality
Number of studies included
Favors placeboFavors fibrateRelative risk (95 CI)
Jun M et al Lancet 20103621563ndash1574Reprinted from The Lancet Volume 362 Jun M et al Effects of fibrates on cardiovascular outcomes
a systematic review and meta-analysis 1563ndash1574 Copyright 2010 with permission from ElsevierMI and stroke
Meta-analysis of 18 placebo-controlled fibrate trials (45 058 patients)
Docosahexenoic acid (DHA)
Eicosapentenoic acid (EPA)
PUFAs Found in fish oil and Mediterranean diet1
Have been used to lower TG1
Omega-3 fatty acids
EPA1
Marketed omega-3 fatty acids include Vascepa (ethyl-EPA)2
Lovaza (mixture of ethyl-esterified EPA DHA and other fish oils)3
1 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash17012 Vascepa Prescribing Information httpwwwdrugscomprovascepahtml
3 Lovaza Prescribing Information httpswwwgsksourcecomgskprmhtdocsdocumentsLOVAZA-PI-PILPDF
Placebo-controlled trials of omega-3 fatty acids
have reported beneficial effects on CV outcomes
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin vs placebo
DART1Men previous MI(n=2033)
Dietary fish intakeMean 2 years
No significant change in total-C over 2 years
All-cause mortality darr29 (plt005)
GISSI-P2 Recent MI (n=11 324)
Omega-3 PUFA1 gd vs control Mean 35 years
LDL-C uarr99 (p=0002) HDL-C uarr88 (p=NS)TGs darr34 (p=0001)
Death nonfatal MI or nonfatal stroke darr10 (p=0048)
GISSI-HF3 Chronic HF(n=6975)
Omega-3 PUFA1 gd vs placebo Median 39 years
TGs darr from 142 to 134 mmolL over 3 years with PUFA (plt00001 vs placebo)
All-cause death darr9 (p=0041)All-cause death or CV hospitalization darr8 (p=0009)
1 Burr ML et al Lancet 19892757ndash7612 GISSI-Prevenzione Investigators Lancet 1999354447ndash455
3 GISSI-HF Investigators Lancet 20083721223ndash1230
Statin use was 5 at study baseline rising to 46 after 42 monthsrsquo follow-upPatients were also randomized to rosuvastatin or placebo no interaction was recorded between PUFA and statin
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Cholesterol absorption inhibitor
Ezetimibe
ENHANCE Simvastatin + ezetimibe did not significantly reduce intima-medial
thickness vs simvastatin alone
00111
00058
0000
0005
0010
0015
Simvastatin + ezetimibe Simvastatin + placebo
Diff
eren
ce fr
om b
asel
ine
at M
onth
24
(mm
)
p=029
44
46
48
50
52
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Mea
n H
DL-
C (m
gdL
)
100
120
140
160
180
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Med
ian
TGs
(mg
dL)
0
100
200
300
400
Baseline Month 24
Simvastatin + placebo
Simvastatin + ezetimibe
Mea
n LD
L-C
(mg
dL)
plt001
p=078
plt001
Primary endpointChange in carotid intima-medial thickness at
Month 24
ENHANCE ezetimibe 10 mgd vs placebo (added to simvastatin 80 mgd) in 720 patients with familial hypercholesterolemia (follow-up 24 months)1
1 Kastelein JJP et al N Engl J Med 20083581431ndash14432 Zocor (simvastatin calcium) Prescribing Information Merck Sharp amp Dohme Ltd October 2012No longer a recommended dose of simvastatin2
Fibrates
ACCORD Fenofibrate had no significant effect on CV endpoints when added to a
statin in patients with diabetes
36
37
38
39
40
41
42
Baseline Study end
Placebo Fenofibrate
Mea
n H
DL-
C
chol
este
rol (
mg
dL)
100
120
140
160
180
Baseline Study end
Placebo Fenofibrate
Mea
n TG
s (m
gdL
)
224
258
132
038
147
241
270
144
036
161
00
05
10
15
20
25
30
Primary outcome Major coronary eventdagger Nonfatal MI Stroke All-cause mortality
Fenofibrate Placebo
Out
com
e ra
tey
r(
) p=NS for all endpoints(Primary outcome HR 092 95 CI 079 to 108 p=032 ARR 017 per year NNT 588 to avoid one event over 1 year)
p=001
plt0001
ACCORD fenofibrate (starting dose 160 mgd) vs placebo in 5518 patients with type 2 diabetes treated with open-label simvastatin (mean follow-up 47 years)
Ginsberg HN et al N Engl J Med 20103621563ndash1574Nonfatal MI nonfatal stroke or CV deathdaggerFatal coronary event nonfatal MI or unstable angina
Niacin
55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
FIELD Fenofibrate did not reduce primary outcome (CHD death or nonfatal
MI) in patients with diabetes
FIELD fenofibrate 200 mgd vs placebo in 9795 patients with type 2 diabetesMedian follow-up 5 years
307
11
193
31
11
20
26
112
187
243
113147
00
05
10
15
20
25
30
35
LDL-C HDL-C TGs
Placebo baseline Fenofibrate baseline
Placebo study end Fenofibrate study end
Mea
n lip
id le
vel (
mm
olL
)R
ate
1000
per
son-
year
s
104
44
64 64
142
119117
37
8471
129
150
02468
10121416
Primary outcome CHD mortality Nonfatal MI Stroke All-cause mortality Coronary revascularization
Fenofibrate PlaceboHR 089
95 CI 075 to 105p=016dagger
p=022
p=036
p=018
HR 07695 CI 062 to 094
p=001
HR 07995 CI 068 to 093
p=0003
Keech A et al Lancet 20053661849ndash1861
CHD mortality or nonfatal MIdaggerARR over course of study=07 NNT=143NNT number needed to treat
Keech p7 ndash 1E
Meta-analysis Fibrates may reduce CV events
but not all-cause mortality
151005
090 (082 to 100) p=0048I2=470 p for heterogeneity=0110
087 (081 to 093) plt00001I2=221 p for heterogeneity=0202
081 (075 to 089) plt00001I2=145 p for heterogeneity=0310
100 (093 to 108) p=0918I2=194 p for heterogeneity=0237
Relative risk (95 CI)
5Major CV events
16Coronary event
10Nonfatal coronary events
16All-cause mortality
Number of studies included
Favors placeboFavors fibrateRelative risk (95 CI)
Jun M et al Lancet 20103621563ndash1574Reprinted from The Lancet Volume 362 Jun M et al Effects of fibrates on cardiovascular outcomes
a systematic review and meta-analysis 1563ndash1574 Copyright 2010 with permission from ElsevierMI and stroke
Meta-analysis of 18 placebo-controlled fibrate trials (45 058 patients)
Docosahexenoic acid (DHA)
Eicosapentenoic acid (EPA)
PUFAs Found in fish oil and Mediterranean diet1
Have been used to lower TG1
Omega-3 fatty acids
EPA1
Marketed omega-3 fatty acids include Vascepa (ethyl-EPA)2
Lovaza (mixture of ethyl-esterified EPA DHA and other fish oils)3
1 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash17012 Vascepa Prescribing Information httpwwwdrugscomprovascepahtml
3 Lovaza Prescribing Information httpswwwgsksourcecomgskprmhtdocsdocumentsLOVAZA-PI-PILPDF
Placebo-controlled trials of omega-3 fatty acids
have reported beneficial effects on CV outcomes
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin vs placebo
DART1Men previous MI(n=2033)
Dietary fish intakeMean 2 years
No significant change in total-C over 2 years
All-cause mortality darr29 (plt005)
GISSI-P2 Recent MI (n=11 324)
Omega-3 PUFA1 gd vs control Mean 35 years
LDL-C uarr99 (p=0002) HDL-C uarr88 (p=NS)TGs darr34 (p=0001)
Death nonfatal MI or nonfatal stroke darr10 (p=0048)
GISSI-HF3 Chronic HF(n=6975)
Omega-3 PUFA1 gd vs placebo Median 39 years
TGs darr from 142 to 134 mmolL over 3 years with PUFA (plt00001 vs placebo)
All-cause death darr9 (p=0041)All-cause death or CV hospitalization darr8 (p=0009)
1 Burr ML et al Lancet 19892757ndash7612 GISSI-Prevenzione Investigators Lancet 1999354447ndash455
3 GISSI-HF Investigators Lancet 20083721223ndash1230
Statin use was 5 at study baseline rising to 46 after 42 monthsrsquo follow-upPatients were also randomized to rosuvastatin or placebo no interaction was recorded between PUFA and statin
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Cholesterol absorption inhibitor
Ezetimibe
ENHANCE Simvastatin + ezetimibe did not significantly reduce intima-medial
thickness vs simvastatin alone
00111
00058
0000
0005
0010
0015
Simvastatin + ezetimibe Simvastatin + placebo
Diff
eren
ce fr
om b
asel
ine
at M
onth
24
(mm
)
p=029
44
46
48
50
52
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Mea
n H
DL-
C (m
gdL
)
100
120
140
160
180
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Med
ian
TGs
(mg
dL)
0
100
200
300
400
Baseline Month 24
Simvastatin + placebo
Simvastatin + ezetimibe
Mea
n LD
L-C
(mg
dL)
plt001
p=078
plt001
Primary endpointChange in carotid intima-medial thickness at
Month 24
ENHANCE ezetimibe 10 mgd vs placebo (added to simvastatin 80 mgd) in 720 patients with familial hypercholesterolemia (follow-up 24 months)1
1 Kastelein JJP et al N Engl J Med 20083581431ndash14432 Zocor (simvastatin calcium) Prescribing Information Merck Sharp amp Dohme Ltd October 2012No longer a recommended dose of simvastatin2
Fibrates
ACCORD Fenofibrate had no significant effect on CV endpoints when added to a
statin in patients with diabetes
36
37
38
39
40
41
42
Baseline Study end
Placebo Fenofibrate
Mea
n H
DL-
C
chol
este
rol (
mg
dL)
100
120
140
160
180
Baseline Study end
Placebo Fenofibrate
Mea
n TG
s (m
gdL
)
224
258
132
038
147
241
270
144
036
161
00
05
10
15
20
25
30
Primary outcome Major coronary eventdagger Nonfatal MI Stroke All-cause mortality
Fenofibrate Placebo
Out
com
e ra
tey
r(
) p=NS for all endpoints(Primary outcome HR 092 95 CI 079 to 108 p=032 ARR 017 per year NNT 588 to avoid one event over 1 year)
p=001
plt0001
ACCORD fenofibrate (starting dose 160 mgd) vs placebo in 5518 patients with type 2 diabetes treated with open-label simvastatin (mean follow-up 47 years)
Ginsberg HN et al N Engl J Med 20103621563ndash1574Nonfatal MI nonfatal stroke or CV deathdaggerFatal coronary event nonfatal MI or unstable angina
Niacin
55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

FIELD Fenofibrate did not reduce primary outcome (CHD death or nonfatal
MI) in patients with diabetes
FIELD fenofibrate 200 mgd vs placebo in 9795 patients with type 2 diabetesMedian follow-up 5 years
307
11
193
31
11
20
26
112
187
243
113147
00
05
10
15
20
25
30
35
LDL-C HDL-C TGs
Placebo baseline Fenofibrate baseline
Placebo study end Fenofibrate study end
Mea
n lip
id le
vel (
mm
olL
)R
ate
1000
per
son-
year
s
104
44
64 64
142
119117
37
8471
129
150
02468
10121416
Primary outcome CHD mortality Nonfatal MI Stroke All-cause mortality Coronary revascularization
Fenofibrate PlaceboHR 089
95 CI 075 to 105p=016dagger
p=022
p=036
p=018
HR 07695 CI 062 to 094
p=001
HR 07995 CI 068 to 093
p=0003
Keech A et al Lancet 20053661849ndash1861
CHD mortality or nonfatal MIdaggerARR over course of study=07 NNT=143NNT number needed to treat
Keech p7 ndash 1E
Meta-analysis Fibrates may reduce CV events
but not all-cause mortality
151005
090 (082 to 100) p=0048I2=470 p for heterogeneity=0110
087 (081 to 093) plt00001I2=221 p for heterogeneity=0202
081 (075 to 089) plt00001I2=145 p for heterogeneity=0310
100 (093 to 108) p=0918I2=194 p for heterogeneity=0237
Relative risk (95 CI)
5Major CV events
16Coronary event
10Nonfatal coronary events
16All-cause mortality
Number of studies included
Favors placeboFavors fibrateRelative risk (95 CI)
Jun M et al Lancet 20103621563ndash1574Reprinted from The Lancet Volume 362 Jun M et al Effects of fibrates on cardiovascular outcomes
a systematic review and meta-analysis 1563ndash1574 Copyright 2010 with permission from ElsevierMI and stroke
Meta-analysis of 18 placebo-controlled fibrate trials (45 058 patients)
Docosahexenoic acid (DHA)
Eicosapentenoic acid (EPA)
PUFAs Found in fish oil and Mediterranean diet1
Have been used to lower TG1
Omega-3 fatty acids
EPA1
Marketed omega-3 fatty acids include Vascepa (ethyl-EPA)2
Lovaza (mixture of ethyl-esterified EPA DHA and other fish oils)3
1 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash17012 Vascepa Prescribing Information httpwwwdrugscomprovascepahtml
3 Lovaza Prescribing Information httpswwwgsksourcecomgskprmhtdocsdocumentsLOVAZA-PI-PILPDF
Placebo-controlled trials of omega-3 fatty acids
have reported beneficial effects on CV outcomes
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin vs placebo
DART1Men previous MI(n=2033)
Dietary fish intakeMean 2 years
No significant change in total-C over 2 years
All-cause mortality darr29 (plt005)
GISSI-P2 Recent MI (n=11 324)
Omega-3 PUFA1 gd vs control Mean 35 years
LDL-C uarr99 (p=0002) HDL-C uarr88 (p=NS)TGs darr34 (p=0001)
Death nonfatal MI or nonfatal stroke darr10 (p=0048)
GISSI-HF3 Chronic HF(n=6975)
Omega-3 PUFA1 gd vs placebo Median 39 years
TGs darr from 142 to 134 mmolL over 3 years with PUFA (plt00001 vs placebo)
All-cause death darr9 (p=0041)All-cause death or CV hospitalization darr8 (p=0009)
1 Burr ML et al Lancet 19892757ndash7612 GISSI-Prevenzione Investigators Lancet 1999354447ndash455
3 GISSI-HF Investigators Lancet 20083721223ndash1230
Statin use was 5 at study baseline rising to 46 after 42 monthsrsquo follow-upPatients were also randomized to rosuvastatin or placebo no interaction was recorded between PUFA and statin
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Cholesterol absorption inhibitor
Ezetimibe
ENHANCE Simvastatin + ezetimibe did not significantly reduce intima-medial
thickness vs simvastatin alone
00111
00058
0000
0005
0010
0015
Simvastatin + ezetimibe Simvastatin + placebo
Diff
eren
ce fr
om b
asel
ine
at M
onth
24
(mm
)
p=029
44
46
48
50
52
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Mea
n H
DL-
C (m
gdL
)
100
120
140
160
180
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Med
ian
TGs
(mg
dL)
0
100
200
300
400
Baseline Month 24
Simvastatin + placebo
Simvastatin + ezetimibe
Mea
n LD
L-C
(mg
dL)
plt001
p=078
plt001
Primary endpointChange in carotid intima-medial thickness at
Month 24
ENHANCE ezetimibe 10 mgd vs placebo (added to simvastatin 80 mgd) in 720 patients with familial hypercholesterolemia (follow-up 24 months)1
1 Kastelein JJP et al N Engl J Med 20083581431ndash14432 Zocor (simvastatin calcium) Prescribing Information Merck Sharp amp Dohme Ltd October 2012No longer a recommended dose of simvastatin2
Fibrates
ACCORD Fenofibrate had no significant effect on CV endpoints when added to a
statin in patients with diabetes
36
37
38
39
40
41
42
Baseline Study end
Placebo Fenofibrate
Mea
n H
DL-
C
chol
este
rol (
mg
dL)
100
120
140
160
180
Baseline Study end
Placebo Fenofibrate
Mea
n TG
s (m
gdL
)
224
258
132
038
147
241
270
144
036
161
00
05
10
15
20
25
30
Primary outcome Major coronary eventdagger Nonfatal MI Stroke All-cause mortality
Fenofibrate Placebo
Out
com
e ra
tey
r(
) p=NS for all endpoints(Primary outcome HR 092 95 CI 079 to 108 p=032 ARR 017 per year NNT 588 to avoid one event over 1 year)
p=001
plt0001
ACCORD fenofibrate (starting dose 160 mgd) vs placebo in 5518 patients with type 2 diabetes treated with open-label simvastatin (mean follow-up 47 years)
Ginsberg HN et al N Engl J Med 20103621563ndash1574Nonfatal MI nonfatal stroke or CV deathdaggerFatal coronary event nonfatal MI or unstable angina
Niacin
55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Meta-analysis Fibrates may reduce CV events
but not all-cause mortality
151005
090 (082 to 100) p=0048I2=470 p for heterogeneity=0110
087 (081 to 093) plt00001I2=221 p for heterogeneity=0202
081 (075 to 089) plt00001I2=145 p for heterogeneity=0310
100 (093 to 108) p=0918I2=194 p for heterogeneity=0237
Relative risk (95 CI)
5Major CV events
16Coronary event
10Nonfatal coronary events
16All-cause mortality
Number of studies included
Favors placeboFavors fibrateRelative risk (95 CI)
Jun M et al Lancet 20103621563ndash1574Reprinted from The Lancet Volume 362 Jun M et al Effects of fibrates on cardiovascular outcomes
a systematic review and meta-analysis 1563ndash1574 Copyright 2010 with permission from ElsevierMI and stroke
Meta-analysis of 18 placebo-controlled fibrate trials (45 058 patients)
Docosahexenoic acid (DHA)
Eicosapentenoic acid (EPA)
PUFAs Found in fish oil and Mediterranean diet1
Have been used to lower TG1
Omega-3 fatty acids
EPA1
Marketed omega-3 fatty acids include Vascepa (ethyl-EPA)2
Lovaza (mixture of ethyl-esterified EPA DHA and other fish oils)3
1 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash17012 Vascepa Prescribing Information httpwwwdrugscomprovascepahtml
3 Lovaza Prescribing Information httpswwwgsksourcecomgskprmhtdocsdocumentsLOVAZA-PI-PILPDF
Placebo-controlled trials of omega-3 fatty acids
have reported beneficial effects on CV outcomes
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin vs placebo
DART1Men previous MI(n=2033)
Dietary fish intakeMean 2 years
No significant change in total-C over 2 years
All-cause mortality darr29 (plt005)
GISSI-P2 Recent MI (n=11 324)
Omega-3 PUFA1 gd vs control Mean 35 years
LDL-C uarr99 (p=0002) HDL-C uarr88 (p=NS)TGs darr34 (p=0001)
Death nonfatal MI or nonfatal stroke darr10 (p=0048)
GISSI-HF3 Chronic HF(n=6975)
Omega-3 PUFA1 gd vs placebo Median 39 years
TGs darr from 142 to 134 mmolL over 3 years with PUFA (plt00001 vs placebo)
All-cause death darr9 (p=0041)All-cause death or CV hospitalization darr8 (p=0009)
1 Burr ML et al Lancet 19892757ndash7612 GISSI-Prevenzione Investigators Lancet 1999354447ndash455
3 GISSI-HF Investigators Lancet 20083721223ndash1230
Statin use was 5 at study baseline rising to 46 after 42 monthsrsquo follow-upPatients were also randomized to rosuvastatin or placebo no interaction was recorded between PUFA and statin
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Cholesterol absorption inhibitor
Ezetimibe
ENHANCE Simvastatin + ezetimibe did not significantly reduce intima-medial
thickness vs simvastatin alone
00111
00058
0000
0005
0010
0015
Simvastatin + ezetimibe Simvastatin + placebo
Diff
eren
ce fr
om b
asel
ine
at M
onth
24
(mm
)
p=029
44
46
48
50
52
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Mea
n H
DL-
C (m
gdL
)
100
120
140
160
180
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Med
ian
TGs
(mg
dL)
0
100
200
300
400
Baseline Month 24
Simvastatin + placebo
Simvastatin + ezetimibe
Mea
n LD
L-C
(mg
dL)
plt001
p=078
plt001
Primary endpointChange in carotid intima-medial thickness at
Month 24
ENHANCE ezetimibe 10 mgd vs placebo (added to simvastatin 80 mgd) in 720 patients with familial hypercholesterolemia (follow-up 24 months)1
1 Kastelein JJP et al N Engl J Med 20083581431ndash14432 Zocor (simvastatin calcium) Prescribing Information Merck Sharp amp Dohme Ltd October 2012No longer a recommended dose of simvastatin2
Fibrates
ACCORD Fenofibrate had no significant effect on CV endpoints when added to a
statin in patients with diabetes
36
37
38
39
40
41
42
Baseline Study end
Placebo Fenofibrate
Mea
n H
DL-
C
chol
este
rol (
mg
dL)
100
120
140
160
180
Baseline Study end
Placebo Fenofibrate
Mea
n TG
s (m
gdL
)
224
258
132
038
147
241
270
144
036
161
00
05
10
15
20
25
30
Primary outcome Major coronary eventdagger Nonfatal MI Stroke All-cause mortality
Fenofibrate Placebo
Out
com
e ra
tey
r(
) p=NS for all endpoints(Primary outcome HR 092 95 CI 079 to 108 p=032 ARR 017 per year NNT 588 to avoid one event over 1 year)
p=001
plt0001
ACCORD fenofibrate (starting dose 160 mgd) vs placebo in 5518 patients with type 2 diabetes treated with open-label simvastatin (mean follow-up 47 years)
Ginsberg HN et al N Engl J Med 20103621563ndash1574Nonfatal MI nonfatal stroke or CV deathdaggerFatal coronary event nonfatal MI or unstable angina
Niacin
55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Docosahexenoic acid (DHA)
Eicosapentenoic acid (EPA)
PUFAs Found in fish oil and Mediterranean diet1
Have been used to lower TG1
Omega-3 fatty acids
EPA1
Marketed omega-3 fatty acids include Vascepa (ethyl-EPA)2
Lovaza (mixture of ethyl-esterified EPA DHA and other fish oils)3
1 Fifth Joint Task Force on CVD Prevention in Clinical Practice Eur Heart J 2012331635ndash17012 Vascepa Prescribing Information httpwwwdrugscomprovascepahtml
3 Lovaza Prescribing Information httpswwwgsksourcecomgskprmhtdocsdocumentsLOVAZA-PI-PILPDF
Placebo-controlled trials of omega-3 fatty acids
have reported beneficial effects on CV outcomes
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin vs placebo
DART1Men previous MI(n=2033)
Dietary fish intakeMean 2 years
No significant change in total-C over 2 years
All-cause mortality darr29 (plt005)
GISSI-P2 Recent MI (n=11 324)
Omega-3 PUFA1 gd vs control Mean 35 years
LDL-C uarr99 (p=0002) HDL-C uarr88 (p=NS)TGs darr34 (p=0001)
Death nonfatal MI or nonfatal stroke darr10 (p=0048)
GISSI-HF3 Chronic HF(n=6975)
Omega-3 PUFA1 gd vs placebo Median 39 years
TGs darr from 142 to 134 mmolL over 3 years with PUFA (plt00001 vs placebo)
All-cause death darr9 (p=0041)All-cause death or CV hospitalization darr8 (p=0009)
1 Burr ML et al Lancet 19892757ndash7612 GISSI-Prevenzione Investigators Lancet 1999354447ndash455
3 GISSI-HF Investigators Lancet 20083721223ndash1230
Statin use was 5 at study baseline rising to 46 after 42 monthsrsquo follow-upPatients were also randomized to rosuvastatin or placebo no interaction was recorded between PUFA and statin
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Cholesterol absorption inhibitor
Ezetimibe
ENHANCE Simvastatin + ezetimibe did not significantly reduce intima-medial
thickness vs simvastatin alone
00111
00058
0000
0005
0010
0015
Simvastatin + ezetimibe Simvastatin + placebo
Diff
eren
ce fr
om b
asel
ine
at M
onth
24
(mm
)
p=029
44
46
48
50
52
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Mea
n H
DL-
C (m
gdL
)
100
120
140
160
180
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Med
ian
TGs
(mg
dL)
0
100
200
300
400
Baseline Month 24
Simvastatin + placebo
Simvastatin + ezetimibe
Mea
n LD
L-C
(mg
dL)
plt001
p=078
plt001
Primary endpointChange in carotid intima-medial thickness at
Month 24
ENHANCE ezetimibe 10 mgd vs placebo (added to simvastatin 80 mgd) in 720 patients with familial hypercholesterolemia (follow-up 24 months)1
1 Kastelein JJP et al N Engl J Med 20083581431ndash14432 Zocor (simvastatin calcium) Prescribing Information Merck Sharp amp Dohme Ltd October 2012No longer a recommended dose of simvastatin2
Fibrates
ACCORD Fenofibrate had no significant effect on CV endpoints when added to a
statin in patients with diabetes
36
37
38
39
40
41
42
Baseline Study end
Placebo Fenofibrate
Mea
n H
DL-
C
chol
este
rol (
mg
dL)
100
120
140
160
180
Baseline Study end
Placebo Fenofibrate
Mea
n TG
s (m
gdL
)
224
258
132
038
147
241
270
144
036
161
00
05
10
15
20
25
30
Primary outcome Major coronary eventdagger Nonfatal MI Stroke All-cause mortality
Fenofibrate Placebo
Out
com
e ra
tey
r(
) p=NS for all endpoints(Primary outcome HR 092 95 CI 079 to 108 p=032 ARR 017 per year NNT 588 to avoid one event over 1 year)
p=001
plt0001
ACCORD fenofibrate (starting dose 160 mgd) vs placebo in 5518 patients with type 2 diabetes treated with open-label simvastatin (mean follow-up 47 years)
Ginsberg HN et al N Engl J Med 20103621563ndash1574Nonfatal MI nonfatal stroke or CV deathdaggerFatal coronary event nonfatal MI or unstable angina
Niacin
55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Placebo-controlled trials of omega-3 fatty acids
have reported beneficial effects on CV outcomes
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin vs placebo
DART1Men previous MI(n=2033)
Dietary fish intakeMean 2 years
No significant change in total-C over 2 years
All-cause mortality darr29 (plt005)
GISSI-P2 Recent MI (n=11 324)
Omega-3 PUFA1 gd vs control Mean 35 years
LDL-C uarr99 (p=0002) HDL-C uarr88 (p=NS)TGs darr34 (p=0001)
Death nonfatal MI or nonfatal stroke darr10 (p=0048)
GISSI-HF3 Chronic HF(n=6975)
Omega-3 PUFA1 gd vs placebo Median 39 years
TGs darr from 142 to 134 mmolL over 3 years with PUFA (plt00001 vs placebo)
All-cause death darr9 (p=0041)All-cause death or CV hospitalization darr8 (p=0009)
1 Burr ML et al Lancet 19892757ndash7612 GISSI-Prevenzione Investigators Lancet 1999354447ndash455
3 GISSI-HF Investigators Lancet 20083721223ndash1230
Statin use was 5 at study baseline rising to 46 after 42 monthsrsquo follow-upPatients were also randomized to rosuvastatin or placebo no interaction was recorded between PUFA and statin
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Cholesterol absorption inhibitor
Ezetimibe
ENHANCE Simvastatin + ezetimibe did not significantly reduce intima-medial
thickness vs simvastatin alone
00111
00058
0000
0005
0010
0015
Simvastatin + ezetimibe Simvastatin + placebo
Diff
eren
ce fr
om b
asel
ine
at M
onth
24
(mm
)
p=029
44
46
48
50
52
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Mea
n H
DL-
C (m
gdL
)
100
120
140
160
180
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Med
ian
TGs
(mg
dL)
0
100
200
300
400
Baseline Month 24
Simvastatin + placebo
Simvastatin + ezetimibe
Mea
n LD
L-C
(mg
dL)
plt001
p=078
plt001
Primary endpointChange in carotid intima-medial thickness at
Month 24
ENHANCE ezetimibe 10 mgd vs placebo (added to simvastatin 80 mgd) in 720 patients with familial hypercholesterolemia (follow-up 24 months)1
1 Kastelein JJP et al N Engl J Med 20083581431ndash14432 Zocor (simvastatin calcium) Prescribing Information Merck Sharp amp Dohme Ltd October 2012No longer a recommended dose of simvastatin2
Fibrates
ACCORD Fenofibrate had no significant effect on CV endpoints when added to a
statin in patients with diabetes
36
37
38
39
40
41
42
Baseline Study end
Placebo Fenofibrate
Mea
n H
DL-
C
chol
este
rol (
mg
dL)
100
120
140
160
180
Baseline Study end
Placebo Fenofibrate
Mea
n TG
s (m
gdL
)
224
258
132
038
147
241
270
144
036
161
00
05
10
15
20
25
30
Primary outcome Major coronary eventdagger Nonfatal MI Stroke All-cause mortality
Fenofibrate Placebo
Out
com
e ra
tey
r(
) p=NS for all endpoints(Primary outcome HR 092 95 CI 079 to 108 p=032 ARR 017 per year NNT 588 to avoid one event over 1 year)
p=001
plt0001
ACCORD fenofibrate (starting dose 160 mgd) vs placebo in 5518 patients with type 2 diabetes treated with open-label simvastatin (mean follow-up 47 years)
Ginsberg HN et al N Engl J Med 20103621563ndash1574Nonfatal MI nonfatal stroke or CV deathdaggerFatal coronary event nonfatal MI or unstable angina
Niacin
55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Cholesterol absorption inhibitor
Ezetimibe
ENHANCE Simvastatin + ezetimibe did not significantly reduce intima-medial
thickness vs simvastatin alone
00111
00058
0000
0005
0010
0015
Simvastatin + ezetimibe Simvastatin + placebo
Diff
eren
ce fr
om b
asel
ine
at M
onth
24
(mm
)
p=029
44
46
48
50
52
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Mea
n H
DL-
C (m
gdL
)
100
120
140
160
180
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Med
ian
TGs
(mg
dL)
0
100
200
300
400
Baseline Month 24
Simvastatin + placebo
Simvastatin + ezetimibe
Mea
n LD
L-C
(mg
dL)
plt001
p=078
plt001
Primary endpointChange in carotid intima-medial thickness at
Month 24
ENHANCE ezetimibe 10 mgd vs placebo (added to simvastatin 80 mgd) in 720 patients with familial hypercholesterolemia (follow-up 24 months)1
1 Kastelein JJP et al N Engl J Med 20083581431ndash14432 Zocor (simvastatin calcium) Prescribing Information Merck Sharp amp Dohme Ltd October 2012No longer a recommended dose of simvastatin2
Fibrates
ACCORD Fenofibrate had no significant effect on CV endpoints when added to a
statin in patients with diabetes
36
37
38
39
40
41
42
Baseline Study end
Placebo Fenofibrate
Mea
n H
DL-
C
chol
este
rol (
mg
dL)
100
120
140
160
180
Baseline Study end
Placebo Fenofibrate
Mea
n TG
s (m
gdL
)
224
258
132
038
147
241
270
144
036
161
00
05
10
15
20
25
30
Primary outcome Major coronary eventdagger Nonfatal MI Stroke All-cause mortality
Fenofibrate Placebo
Out
com
e ra
tey
r(
) p=NS for all endpoints(Primary outcome HR 092 95 CI 079 to 108 p=032 ARR 017 per year NNT 588 to avoid one event over 1 year)
p=001
plt0001
ACCORD fenofibrate (starting dose 160 mgd) vs placebo in 5518 patients with type 2 diabetes treated with open-label simvastatin (mean follow-up 47 years)
Ginsberg HN et al N Engl J Med 20103621563ndash1574Nonfatal MI nonfatal stroke or CV deathdaggerFatal coronary event nonfatal MI or unstable angina
Niacin
55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Cholesterol absorption inhibitor
Ezetimibe
ENHANCE Simvastatin + ezetimibe did not significantly reduce intima-medial
thickness vs simvastatin alone
00111
00058
0000
0005
0010
0015
Simvastatin + ezetimibe Simvastatin + placebo
Diff
eren
ce fr
om b
asel
ine
at M
onth
24
(mm
)
p=029
44
46
48
50
52
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Mea
n H
DL-
C (m
gdL
)
100
120
140
160
180
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Med
ian
TGs
(mg
dL)
0
100
200
300
400
Baseline Month 24
Simvastatin + placebo
Simvastatin + ezetimibe
Mea
n LD
L-C
(mg
dL)
plt001
p=078
plt001
Primary endpointChange in carotid intima-medial thickness at
Month 24
ENHANCE ezetimibe 10 mgd vs placebo (added to simvastatin 80 mgd) in 720 patients with familial hypercholesterolemia (follow-up 24 months)1
1 Kastelein JJP et al N Engl J Med 20083581431ndash14432 Zocor (simvastatin calcium) Prescribing Information Merck Sharp amp Dohme Ltd October 2012No longer a recommended dose of simvastatin2
Fibrates
ACCORD Fenofibrate had no significant effect on CV endpoints when added to a
statin in patients with diabetes
36
37
38
39
40
41
42
Baseline Study end
Placebo Fenofibrate
Mea
n H
DL-
C
chol
este
rol (
mg
dL)
100
120
140
160
180
Baseline Study end
Placebo Fenofibrate
Mea
n TG
s (m
gdL
)
224
258
132
038
147
241
270
144
036
161
00
05
10
15
20
25
30
Primary outcome Major coronary eventdagger Nonfatal MI Stroke All-cause mortality
Fenofibrate Placebo
Out
com
e ra
tey
r(
) p=NS for all endpoints(Primary outcome HR 092 95 CI 079 to 108 p=032 ARR 017 per year NNT 588 to avoid one event over 1 year)
p=001
plt0001
ACCORD fenofibrate (starting dose 160 mgd) vs placebo in 5518 patients with type 2 diabetes treated with open-label simvastatin (mean follow-up 47 years)
Ginsberg HN et al N Engl J Med 20103621563ndash1574Nonfatal MI nonfatal stroke or CV deathdaggerFatal coronary event nonfatal MI or unstable angina
Niacin
55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

ENHANCE Simvastatin + ezetimibe did not significantly reduce intima-medial
thickness vs simvastatin alone
00111
00058
0000
0005
0010
0015
Simvastatin + ezetimibe Simvastatin + placebo
Diff
eren
ce fr
om b
asel
ine
at M
onth
24
(mm
)
p=029
44
46
48
50
52
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Mea
n H
DL-
C (m
gdL
)
100
120
140
160
180
Baseline Month 24
Simvastatin + placeboSimvastatin + ezetimibe
Med
ian
TGs
(mg
dL)
0
100
200
300
400
Baseline Month 24
Simvastatin + placebo
Simvastatin + ezetimibe
Mea
n LD
L-C
(mg
dL)
plt001
p=078
plt001
Primary endpointChange in carotid intima-medial thickness at
Month 24
ENHANCE ezetimibe 10 mgd vs placebo (added to simvastatin 80 mgd) in 720 patients with familial hypercholesterolemia (follow-up 24 months)1
1 Kastelein JJP et al N Engl J Med 20083581431ndash14432 Zocor (simvastatin calcium) Prescribing Information Merck Sharp amp Dohme Ltd October 2012No longer a recommended dose of simvastatin2
Fibrates
ACCORD Fenofibrate had no significant effect on CV endpoints when added to a
statin in patients with diabetes
36
37
38
39
40
41
42
Baseline Study end
Placebo Fenofibrate
Mea
n H
DL-
C
chol
este
rol (
mg
dL)
100
120
140
160
180
Baseline Study end
Placebo Fenofibrate
Mea
n TG
s (m
gdL
)
224
258
132
038
147
241
270
144
036
161
00
05
10
15
20
25
30
Primary outcome Major coronary eventdagger Nonfatal MI Stroke All-cause mortality
Fenofibrate Placebo
Out
com
e ra
tey
r(
) p=NS for all endpoints(Primary outcome HR 092 95 CI 079 to 108 p=032 ARR 017 per year NNT 588 to avoid one event over 1 year)
p=001
plt0001
ACCORD fenofibrate (starting dose 160 mgd) vs placebo in 5518 patients with type 2 diabetes treated with open-label simvastatin (mean follow-up 47 years)
Ginsberg HN et al N Engl J Med 20103621563ndash1574Nonfatal MI nonfatal stroke or CV deathdaggerFatal coronary event nonfatal MI or unstable angina
Niacin
55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Fibrates
ACCORD Fenofibrate had no significant effect on CV endpoints when added to a
statin in patients with diabetes
36
37
38
39
40
41
42
Baseline Study end
Placebo Fenofibrate
Mea
n H
DL-
C
chol
este
rol (
mg
dL)
100
120
140
160
180
Baseline Study end
Placebo Fenofibrate
Mea
n TG
s (m
gdL
)
224
258
132
038
147
241
270
144
036
161
00
05
10
15
20
25
30
Primary outcome Major coronary eventdagger Nonfatal MI Stroke All-cause mortality
Fenofibrate Placebo
Out
com
e ra
tey
r(
) p=NS for all endpoints(Primary outcome HR 092 95 CI 079 to 108 p=032 ARR 017 per year NNT 588 to avoid one event over 1 year)
p=001
plt0001
ACCORD fenofibrate (starting dose 160 mgd) vs placebo in 5518 patients with type 2 diabetes treated with open-label simvastatin (mean follow-up 47 years)
Ginsberg HN et al N Engl J Med 20103621563ndash1574Nonfatal MI nonfatal stroke or CV deathdaggerFatal coronary event nonfatal MI or unstable angina
Niacin
55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

ACCORD Fenofibrate had no significant effect on CV endpoints when added to a
statin in patients with diabetes
36
37
38
39
40
41
42
Baseline Study end
Placebo Fenofibrate
Mea
n H
DL-
C
chol
este
rol (
mg
dL)
100
120
140
160
180
Baseline Study end
Placebo Fenofibrate
Mea
n TG
s (m
gdL
)
224
258
132
038
147
241
270
144
036
161
00
05
10
15
20
25
30
Primary outcome Major coronary eventdagger Nonfatal MI Stroke All-cause mortality
Fenofibrate Placebo
Out
com
e ra
tey
r(
) p=NS for all endpoints(Primary outcome HR 092 95 CI 079 to 108 p=032 ARR 017 per year NNT 588 to avoid one event over 1 year)
p=001
plt0001
ACCORD fenofibrate (starting dose 160 mgd) vs placebo in 5518 patients with type 2 diabetes treated with open-label simvastatin (mean follow-up 47 years)
Ginsberg HN et al N Engl J Med 20103621563ndash1574Nonfatal MI nonfatal stroke or CV deathdaggerFatal coronary event nonfatal MI or unstable angina
Niacin
55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Niacin
55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

55
60
65
70
75
Baseline Year 3
Statin + placebo Statin + niacin
162
15
47
09
4051
164
12
54
16
3747
02468
1012141618
Primary endpoint Death from CHD Nonfatal MI Ischemic stroke Hospitalization for ACS Revascularizationdagger
Statin + placebo Statin + niacin
AIM-HIGH trial of niacin
Discontinued early due to lack of efficacy
AIM-HIGH extended-release niacin 1500ndash2000 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 3414 patients with established CV disease Stopped after mean follow-up 3 yr
Patie
nts
(cum
ulat
ive
)
3032343638404244
Baseline Year 3
Statin + placebo Statin + niacin
Med
ian
HD
L-C
(mg
dL)
100
120
140
160
180
Baseline Year 3
Statin + placeboStatin + niacin
Med
ian
TGs
(mg
dL)
Med
ian
LDL-
C (m
gdL
)
plt0001
p=080
Boden WE et al N Engl J Med 20113652255ndash2267
Death from CHD nonfatal MI ischemic stroke hospitalization for ACS or symptom-driven coronary or cerebral revascularizationdaggerSymptom-driven coronary or cerebral revascularization
137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

137
54
39
70
132
5239
63
0
2
4
6
8
10
12
14
16
Primary outcome Any major coronary event Any stroke Any revascularization
Statin + placebo Statin + niacin-laropiprant
HPS-2-THRIVE Niacinndashlaropiprant had no effect on major vascular events
and increased serious AEs
HPS-2-THRIVE extended-release niacin 2000 mgd + laropiprant 40 mgd vs placebo (added to simvastatin plusmn ezetimibe) in 25 673 patients with vascular disease Median follow-up 39 year
-10
6
-33-40
-30
-20
-10
0
10
LDL-C HDL-C TGs
Cha
nge
in li
pids
nia
cin-
laro
pipr
antv
s pl
aceb
o (m
gdL
) Lipid levels
HR 09695 CI 090ndash103
p=029
p=051
p=056
Patie
nts
with
outc
ome
()
3830
04
66
19
4348
37
07
80
25
57
0
2
4
6
8
10
Gastrointestinal Musculoskeletal Skin Infection Bleeding New-onset diabetes
Statin + placebo Statin + niacin-laropiprant
plt0001
plt0001
p=0003
plt0001
plt0001
plt0001
Patie
nts
with
serio
us A
E (
)
HR 09095 CI 082ndash099
p=003
Haynes R et al N Engl J Med 2014371203ndash212Major vascular event (nonfatal MI death from coronary causes stroke or arterial revascularization
ARR 05NNT 200 over 39 years
Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Omega-3 fatty acids
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin vs statin alone
JELIS118 645 total-C gt65 mmolL
Statin + EPA 18 gd vs statin + placeboMean 46 years
LDL-C darr25 in both groupsTGs darr9 vs 4 (plt00001)
Major coronary events darr19 (p=0011)No difference for coronary or sudden cardiac death
OMEGA2 Prior MI(n=3851)
Omega-3 PUFA 1 gd vs placeboMean 1 year94 taking statin
TGs 137 vs 143 mmolL at study end (plt001)LDL-C 246 mmolL in both groups
Sudden cardiac death 15 in both groups (p=NS)
Alpha-Omega3
Prior MI(n=4837)
EPAndashDHA 400 mgd vs placeboMedian 34 years86 taking lipid-lowering drugs (mainly statins)
No significant differences in TGs or other risk markers
Fatal and nonfatal CV events and cardiac interventions 140 vs 138 (p=093)
ORIGIN4Dysglycemia + high CV risk(n=12 536)
Omega-3 ethyl esters 1 gd vs placeboMedian 62 yearsasymp54 taking statin
TGs darr235 mgdL with PUFA vs darr90 with placebo (plt00001)Other lipids NS
Death from CV causes 91 vs 93 (p=072)
Omega-3 fatty acids do not appear to augment the beneficial effects of
statins on CV outcomes
1 Yokoyama M et al Lancet 20073691090ndash10982 Rauch B et al Circulation 20101222152ndash2159
3 Kromhout D et al N Engl J Med 20103632015ndash20264 Bosch J et al N Engl J Med 2012367309ndash318
1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

1 Non-statin vs placebo
2 Non-statin vs placebo (on background of statin-based lipid lowering therapy)
3 Non-statin + statin vs placebo
Clinical trials of non-statin treatments
Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Ezetimibe
-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

-15
-10
-05
00
05 Placebo Simvastatin + ezetimibe
SHARP Simvastatin + ezetimibe reduced major atherosclerotic events
compared with placebo in CKD
SHARP simvastatin 20 mgd + ezetimibe 10 mgd or placebo in 9270 patients with CKDMedian follow-up 49 years
LDL-
C a
bsol
ute
chan
ge
(mm
olL
)
8ndash13 26ndash31 44ndash49
Time (months)
5
38
76
46
28
61
0
2
4
6
8
10
Any major coronary event Any non-hemorrhagic stroke Any revascularization
Placebo Simvastatin + ezetimibe
Patie
nts
() p=037
Risk ratio 07595 CI 060 to 094
p=001
25
00 1 2 3 4 5
5
10
15
20
Peop
le s
uffe
ring
even
ts
()
Rate reduction 17 (95 CI 6 to 26)Log-rank p=00021ARR 21 NNT 48 over 49 years
Time (years)
Primary endpoint1
PlaceboSimvastatin + ezetimibe
Risk ratio 07995 CI 068 to 093
p=00036
Nonfatal MI or coronary death non-hemorrhagic stroke or any arterial revascularization procedure
1Figure reprinted with permission from Elsevier (The Lancet 20113772181ndash2192)Baigent C et al Lancet 20113772181ndash2192
SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

SEAS Simvastatin + ezetimibe did not reduce major CV events in patients with
asymptomatic aortic stenosis
SEAS simvastatin 40 mgd + ezetimibe 10 mgd vs placebo in 1873 patients with mild-to-moderate asymptomatic aortic stenosis Median follow-up 522 months
Patie
nts
()
38
538
0
20
40
60
Placebo Simvastatin + ezetimibe
Red
uctio
nin
LD
L-C
() plt0001
062 061
0
02
04
06
08
Placebo Simvastatin + ezetimibe
Cha
nge
in p
eak
aort
ic
flow
vel
ocity
(ms
ec)
p=083
382
6
299
28
108
353
50
283
18
73
0
10
20
30
40
Primary outcome Death from CV causes Aortic valve replacement Nonfatal MI CABG
Placebo Simvastatin + ezetimibe
HR 09695 CI 083 to 112
p=059
p=034
p=097
p=015
HR 06895 CI 050 to 093
p=002
Rosseboslash A et al N Engl J Med 20083591343ndash1356Death from CV causes aortic valve replacement nonfatal MI hospitalization for acute angina HF coronary artery bypass grafting percutaneous coronary intervention and non-hemorrhagic stroke
ARR 29NNT 34 over 1 year
Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Non-statin trials Summary
Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Clinical trials of fenofibrate have reported limited effects on CV endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin vs placebo
FIELD1 Type 2 diabetes(n=9795)
Fenofibrate 200 mgPlaceboMedian 5 years
Final TGsFenofibrate 147 mmolLPlacebo 187 mmolL
CHD mortality or nonfatal MI darr11 (p=016)Nonfatal MI darr24 (p=001)Coronary revascularizaion darr21 (p=003)
Non-statin + statin vs statin alone
ACCORD2 Type 2 diabetes receiving simvastatin (n=5518)
Fenofibrate 160 mgPlaceboMean 47 years
Final TGsFenofibrate 122 mgdLPlacebo 144 mgdL
Major CV event darr8 (p=032)Major coronary eventdarr8 (p=026)All-cause mortalitydarr9 (p=033)
1 Keech A et al Lancet 20053661849ndash18612 Ginsberg HN et al N Engl J Med 20103621563ndash1574
Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Clinical trials of ezetimibe have reported inconsistent effects on CV events
Study Population Regimen follow-up Lipid effects CV endpointsNon-statin + statin vs statin alone
ENHANCE1FH (n=720)Receiving simva-statin 80 mg
Ezetimibe 10 mgPlacebo24 months
Final LDL-CEzetimibe 141 mgdLPlacebo 193 mgdL
Change in carotid IMT00111 vs 00058 mm(p=029)
IMPROVE-IT23Post-ACS (n=18 144)Receiving simva-statin 40ndash80 mg
Ezetimibe 10 mgPlaceboasymp6 years
Final LDL-CEzetimibe 532 mgdLPlacebo 699 mgdL
Primary endpointdarr64 (p=0016)
Non-statin + statin vs placebo
SHARP4 CKD(n=9270)
Ezetimibe 10 mg + simvastatin 20 mgPlaceboMedian 49 years
LDL-C darr(months 44ndash49)ES 084 mmolLPlacebo 008 mmolL
Major atherosclerotic events darr17 (p=00021)
SEAS5 Aortic stenosis (n=1873)
Ezetimibe 10 mg + simvastatin 40 mgPlaceboMedian 522 months
LDL-C darrES 538Placebo 38
Primary CV endpointdarr4 (p=059)
1Kastelein JJP et al N Engl J Med 20083581431ndash1443 2 Blazing MA et al Am Heart J 2014168205ndash2123 Cannon C AHA Chicago IL November 17 2014 4 Baigent C et al Lancet 20113772181ndash2192
5 Rosseboslash A et al N Engl J Med 20083591343ndash1356
Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Large endpoint trials of niacin reported no significant effect on primary CV
endpoints
Study PopulationRegimenfollow-up Lipid effects CV endpoints
Non-statin + statin plusmn ezetimibe vs statin plusmn ezetimibe alone
AIM-HIGH1 Established CVD (n=3414)
Niacin 1500ndash2000 mgPlaceboAdded to simvastatin plusmnezetimibeMean 3 years
Final HDL-CNiacin 42 mgdLPlacebo 37 mgdL
Primary CV endpointuarr2 (p=080)
HPS2-THRIVE2Established vascular disease(n=25673)
Niacin 2000 mg + laropiprant40 mgdPlaceboAdded to simvastatin plusmnezetimibeMedian 39 years
HDL-C uarr6 vs placebo Major vascular eventsdarr4 (p=029)
1 Boden WE et al N Engl J Med 20113652255ndash22672 Haynes R et al N Engl J Med 2014371203ndash212
Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Non-statins on the horizon
Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Non-statins on the horizon
PCSK9 inhibitors PCSK9 degrades LDL receptor and inhibits take-up and degradation of LDL1
Loss of PCSK9 reduces LDL-C and protects against CHD1
Monoclonal antibodies against PCSK9 are under development1
Preliminary results in heterozygous FH or high-risk patients receiving maximally tolerated statins2
ndash Marked reduction of LDL-Cndash Potential decrease in CV events
CETP inhibitors1
Torcetrapib withdrawn due to excess CV events Dalcetrapib no effect on recurrent CV events Next-generation CETP inhibitors are in development (anacetrapib evacetrapib)
Mipomersen1
Antisense oligonucleotide inhibitor of apo B synthesis (weekly injections) Approved in USA for homozygous familial hypercholesterolemia
1 Tomkin GH et al Expert Opin Investig Drugs 2014231411ndash14212 Robinson JG et al ESC Congress 2014
Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Supplements
Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Supplements are not primary treatment
Seeds and Grains Hypocholesterolemic effects and antioxidant activity in an ethyl acetate extract of fenugreek seed which may
be partly due to the presence of flavonoids especially naringenin1
Results from oat bran studies shows it had the ability to lower serum cholesterol levels in part by altering bile acid metabolism2
The few whole-grain studies show improvements in biomarkers blood lipid improvement3
Algae Antihypertensive and antihypercholesterolemic activities were found in some green brown and red algae
seaweeds4
Spirulina
Many pre-clinical studies and a few clinical studies suggest ability to reduce cholesterol 5
1 Belguith-Hadriche O1 Bouaziz M et al Lipid-lowering and antioxidant effects of an ethyl acetate extract of fenugreek seeds in high-cholesterol-fed rats J Agric Food Chem 2010 Feb 2458(4)2116-222 2Jusith AM Kathryn Bhet al Mechanisnm of serumcholesterol reduction by oat bran Hepatology (1994)20 (6) pages 1450ndash1457 3Joanne Slavin Why whole grains are protectrivebiological mechanisms Proceedings of the Nutrition Society (2003) 62 129ndash134 4 Dalin R Hiroyuki N et al Study on antihypertensive and antihyperlipidemiceffects of marine algae Fisheries science(1994) 60 (1) 83-88 5 Amha B Yoshimichi O et Al Current knowledge on potential health benefits of spirulina Journal of Applied Phycology (1993)5 (2) 235-241
Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67

Conclusions
The primary objective of lipid-modifying therapy is to reduce CV events
Guidelines recommend statins as first-line drugs for lipid-modifying therapy1ndash3
Guidelines do not recommend non-statins except in very limited circumstances1ndash3
In patients at high risk or with established CVD high-intensity statin is recommended rather than addition of a non-statin12
There are no data from RCTs supporting routine use of fibrates niacin or omega-3 fatty acids added to statin therapy to further reduce ASCVD12
Addition of ezetimibe to a moderate-intensity statin produces a modest further reduction in ASCVD events after ACS4
1 Stone NJ et al J Am Coll Cardiol 2014632889ndash2934 2 Rabar S et al BMJ 2014 349g4356 doi101136bmjg43563 Fifth Joint Task Force Eur Heart J 2012331635ndash1701 4 Cannon C AHA Chicago IL November 17 2014 LBCT02
5 Sever PS et al Lancet 20033611149ndash1158 6 Koren MD et al J Am Coll Cardiol 2004441772ndash1779 7 Colhoun HM et al Lancet 2004364685ndash6968 LaRosa JC et al N Engl J Med 20053521425ndash14359 Cannon CP et al N Engl J Med 20043501495ndash1504 10 Newman C et al Am J Cardiol 20069761ndash67