Embed Size (px)
Citation preview

ESMO SUMMIT LATIN AMERICA 2019
Head and Neck Cancer in Latin America
Dr. Nora Sobrevilla Moreno
Medical OncologistHead and Neck, Melanoma an GU cancers
Insituto Nacional de Cancerología, México City, Mexico

CONFLICT OF INTEREST DISCLOSURESub-title
Advisory board:BMS, MSD, Pfizer, Eisai, Ipsen, Bayer.
Speaker:BMS, MSD, Pfizer, Eisai, Ipsen, Bayer.
Research:BMS, MSD, Pfizer.

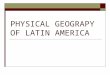
HEAD AND NECK CANCER IS A HETEROGENOUS DISEASE
90% of head and neck cancers have squamous-cell histology (HNSCC).
Other sites:• Paranasal sinuses• Salivary glands
Nasal antrum
Nasopharynx
OropharynxBase of tongueSoft palateTonsillar pillarand fossa
Hypopharynx
Esophagus
SupraglottisFalse cordsArytenoidsEpiglottisArytenoepiglottic foldGlottisSubglottis
LipBuccal mucosaAlveolar ridge and retromolar trigoneFloor of mouthHard palateOral tongue (anterior two thirds)
Oral cavity
Larynx
Pharynx

EPIDEMIOLOGY

Head and neck cancer respresent the seventh more common cause of cancer in the world. Approximately 705,781 new cases in the world.
https://gco.iarc.fr/today/home
Head and neck cancer respresent the eighth more common cause of cancer deaths in the world. Approximately 358,144 deaths in the world.
EPIDEMIOLOGY OF HNSCCWorld
Eighth cause of cancer in Latin America

Seventh cause of cancer deaths in Latin America
https://gco.iarc.fr/today/home
EPIDEMIOLOGY OF HNSCCWorld

EPIDEMIOLOGY OF HNSCCLatin America

Cancers ranked by age-standardized incidence rates among males in Central and South America
Sierra MS., et al. Cancer Epidemiol (2016);44S:S23-S42

Cancers ranked by age-standardized mortality rates among males in Central and South America
Sierra MS., et al. Cancer Epidemiol (2016);44S:S23-S42

Males have higher incidence thanwomen, with the lower male:femaleratios presenting in El Salvador, Peruand Guatemala (other: Mexico,Ecuador, Bolivia, Haiti).
Males have higher mortality ratesthan females, with the lowermale:female ratio in Peru andEcuador (other Guatemala, Boliviaand El Salvador).
MALE:FEMALE RATIO OF HNSCCLatin America

RISK FACTORS

RISK FACTORS FOR HEAD AND NECK CANCER
• Age: (patients older 60 years old).• Sex: Men
• Tobacco.• Alcohol.• Other oral substances: Betel nut.
• Virus HPV EBV
Chaturvedi AK, et al. J Clin Oncol. 2011;29:4294-4301.

ALCOHOL AN TOBACCO CONSUMPTION ARE RISK FACTORS FOR H&N CANCER
Hashibe M., et al. J Natl Cancer Inst 2007;99:777-89
At least 75% of H&N cancers areattributable to tobacco and alcoholdrinking.

PREVALENCE OF TOBACCO SMOKING IN LATIN AMERICA

CURRENT SMOKING PATTERNS IN LATIN AMERICA
Pineros M., et al. Cancer Epidemiol 2016;44S:S90-S99

PREVALENCE OF ALCOHOL CONSUMPTION STATUS IN THE WORLD
Global status report on alcohol and health 2018. Geneva: World Health Organization; 2018.

PORPORTION OF UNRECORDED TOTAL ALCOHOL PER CAPITA CONSUMPTION (APC) AMONG CURRENT DRINKERSWHO regions
Global status report on alcohol and health 2018. Geneva: World Health Organization; 2018.

TRENDS OF ALCOHOL CONSUMPTION IN THE WORLD
Global status report on alcohol and health 2018. Geneva: World Health Organization; 2018.

VIRAL INFECTION AND CANCER
https://gco.iarc.fr/causes/infections/home

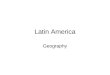
HPV IS ASSOCIATED WITH PROGNOSIS IN OP SCC
Low risk: HPV+ with ≤ 10 pk-yrs or > 10 pk-yrs and N0-N2a cancerIntermediate risk: HPV+ with > 10 pk-yrs or HPV‒ with ≤ 10 pk-yrsand T2-T3 cancerHigh risk: HPV‒ with ≤ 10 pk-yrs and T4 cancer or > 10 pk-yrs
93.0%
70.8%
46.2%
Ang KK, et al. N Engl J Med. 2010;363:24-35

AJCC 8TH EDITION: OROPHARYNX
Lydiatt WM., et al. CA Cancer J Clin 2017;67:122-137

HPV PREVALENCE IN HNSCC
Ndiaye C., et al. Lancet Oncol 2014;15:1319-31

HPV PREVALENCE IN HNSCC
p16/HPV16 positivity in OP varied according to region:
- Brazil: 4.1%- Europe: 31%- US: 59%
p < 0.001
D´Souza G., et al. Oral Oncol 2016;62:20-17

HPV PREVALENCE IN HNSCC
• 1090 cases of OP cancer over the world.
• 819 HPV-DNA negative.• 271 HPV-DNA positive.• 158 cases of OP cancer from Central
and South America
• Argentina, Bolivia, Chile, Colombia, Ecuador, Paraguay, Venezuela.
• Guatemala, Honduras, México.
Castellsagué X., et al. J Natl Cancer Inst 2016;108:djv403

DIAGNOSIS

https://gco.iarc.fr/tomorrow/home
TIME TRENDS FOR HNSCCWorld

LarynxLip, Oral cavity & Pharynx
INCIDENCE AND MORTALITY TIME TRENDSLatin America: 1985-2010
Perdomo S., et al. Cancer Epidemiology 2016;44S:S43-S52

Incidence Mortality
Lip, Oral Cavity
Larynx
Oropharynx
Hypopharynx
HEAD AND NECK INCIDENCE AND MORTALITY BURDEN: TIME TRENDS.
https://gco.iarc.fr/tomorrow/home

31%47%
18% 5%
Stage Distribution at Diagnosis*[1]
LocalizedRegionalDistantUnknown
83%61%
37% 49%
0.0%
100.0%
5-Year Relative Survival*[1]
56%
21%
19% 5%
Stage Distribution at Diagnosis*[1]
LocalizedRegionalDistantUnknown
75%
43% 35%56%
0.0%
100.0%
5-Year Relative Survival*[1]
1. National Cancer Institute. SEER Stat Fact Sheets: Oral Cavity and Pharynx Cancer. Available at: http://seer.cancer.gov/statfacts/ html/oralcav.html. Accessed September 15, 2014. 2. National Cancer Institute. SEER Stat Fact Sheets: Larynx Cancer. Available at: http://seer.cancer.gov/statfacts/html/laryn.html. Accessed September 15, 2014
Oral Cavity and Pharynx
Larynx
STAGE DISTRIBUTION AND SURVIVAL OF OC, PHARYNX AND LARYNX CANCER IN THE USA.

DISTRIBUTION OF CLINICAL STAGES IN HNSCCBrazil
D´Souza G., et al. Oral Oncol 2016;62:20-17

• Significant morbidity and mortality.• Survival advantage of early diagnosis.• Association of identifiable risk factors.• Ability to diagnose early stage tumors with a clinical
examination.
SCREENING FOR HNSCCWhy does it makes sense?

Three rounds of oral visual examination at three-year intervals.
PPV 74%. Sensitivity: 64%. Absolute reduction in oral cancer mortality non significant. Reduction of mortality in tobacco and alcohol users: 34% Conclusion: Oral visual screening has the potential to prevent 37000 deaths from oral cancer every year among
smokers and drinkers.
SCREENING EXPERIENCE IN HNSCCIndia
Gogarty DS. J Laryngol Otol 2016;130:8-14

National screening program for head and neck cancer malignancies. All citizens 15 years and above. Annual oral visual inspection by dentists.
Data collected between 1984-1990. Reference of 6091 patients (35% complied with referral).
Stage I diagnosis increased from 22.8% to 48.2% Stage II-IV cases decreased from 77.2 to 51.8%
SCREENING IN HNSCC Cuba experience
Gogarty DS. J Laryngol Otol 2016;130:8-14

TREATMENT

Developed countries: approximately 50%. Developing countries: >55%, may reach
70–80% of patients in some areas. Actual RTU developing countries: 25%-
40%. A radiotherapy machine is required for
every 400–600 new radiotherapy patientsper year.
High income countries 1:120 000 patients. Middle income countries 1: 1 million
patients. Low income countries 1: 5 million patients.
RADIOTHERAPY UTILIZATION RATES (RTU)
Rossenblatt E., et al. Radiotherapy in cancer care: facing the global challenge / International Atomic Energy Agency 2017.

RADIOTHERAPY NEEDS AND TYPE OF COVERAGE
Camacho-Rodríguez R., et al. Radiotherapy in cancer care: facing the global challenge / International Atomic Energy Agency 2017.

Chemoradiotherapy:
Organ preservation. Definitive. Adjuvant.
Induction chemotherapy.
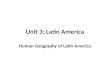
CHEMOTHERAPY IS A STANDARD OF CARE FOR LOCALLY ADVANCED HEAD AND NECK CANCERS

127153
83118
6582
4757
1930
173184
220222
815
13
HR : 0.80 (95% CI: 0.64-0.99; P = .04)
Chemotherapy only (n = 220) 20Chemo + cetuximab (n = 222) 36
Surv
ival
Pro
babi
lity
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 3 6 9 12 15 18 21 24
10.1 mos7.4 mos
Pts at Risk, nCTX only
CET + CTX
Survival Time (Mos)
ORR, %
Vermorken JB, et al. N Engl J Med. 2008;350:1116-1127. Ferris RL., et al. N Engl J Med 2016;375:1856
APPROVED TREATMENTS BEYOND CHEMOTHERAPY FOR HEAD AND NECK CANCERS

APPROVAL AND ACCESS OF CETUXIMAB AND NIVOLUMAB IN LATIN AMERICA
Country Cetuximab NivolumabLA HNSCC Recurrent/metastatic R/M Platinum resistant
Argentina Fully reimbursed Fully reimbursed Fully reimbursed
Brazil Not reimbursed Not reimbursed Not approved
Chile Partially reimbursed Partially reimbursed Partially reimbursed
Costa Rica Not reimbursed Fully reimbursed Not approved
Colombia NA NA Partially reimbursed
Dominican Republic Fully reimbursed Fully reimbursed Not approved
Ecuador Fully reimbursed Partially reimbursed Not approved
El Salvador Fully reimbursed Fully reimbursed Not approved
Guatemala Fully reimbursed Fully reimbursed Not approved
Honduras Fully reimbursed Fully reimbursed Not approved
Mexico Partially reimbursed Partially reimbursed Partially reimbursed
Nicaragua Fully reimbursed Fully reimbursed Not approved
Panama Fully reimbursed Fully reimbursed Not approved
Peru Fully reimbursed Not reimbursed Partially reimbursed
Venezuela Fully reimbursed Fully reimbursed Not approved
Data provided by Merck Mexico and BMS Mexico

ECONOMIC BURDEN OF NEWER THERAPIES IN HEAD AND NECK CANCER
Banford J., et al. Nat Rev Drug Disc 2017;16:235-36

REGISTERED CLINICAL TRIALS IN HEAD AND NECK CANCER IN LATIN AMERICA
Number of clinical studies
Completed/Terminated
Active, not recruiting
Recruiting Investigator Initiated
Pharma initiative
Argentina 14 9 3 2 1 13Brazil 33 19 7 7 19 14Chile 8 5 2 1 3 5Colombia 3 1 0 2 0 3Cuba 3 1 0 2 2 1Mexico 11 5 4 2 1 10Peru 4 4 0 1 3Uruguay 2 1 0 1 1 1
United States 1233 registered studies.Canada 171 registered studies.
https://clinicaltrials.gov/

PERSPECTIVES FOR HNSCC IN LATIN AMERICA
Decreasing incidence
Prevention programs:
• Tobacco• Alcohol
HPV:
• Vaccination??
Decreasing mortalityDiagnosis Treatment
Continued Education Programs:
• General practitioners• Dentists
Screening procedures???:
• Targeted poulations
Increase access:
• Inclusion to clinical trials.
• Increase government programs.
• Awareness to cancer associations.

GRACIAS