Embed Size (px)
Citation preview
ESRD Proposed Rule for 2016 and Beyond
Florida Renal Administrators Association
July 17, 2015
2
Objectives
• Identify the PPS base rate for 2016• Describe changes to the ESRD PPS for 2016• Identify the adjuster that will increase in 2016• Identify the adjusters that will be eliminated in 2016• Name two positive improvements to the PPS that the
industry has supported for years
Overview of Proposed Rule for 2016 ESRD PPS
• PPS Summary– Base rate reduced from $239.43 to $230.20
– Net market basket update of 0.15% (HOW? 2% MB less 1.25% PAMA and 0.6% productivity adjustments)
– Substantial revisions to patient and facility-level adjusters
– Proposed mechanism for introduction of new drugs into the bundle
• QIP Summary– Technical changes to scoring methodology for 2017
– For 2018, four Kt/V measures will be eliminated
– New measures for 2019 Dialysis Adequacy – % of all patients whose average dialysis dose meets specified threshold
Full-Season Influenza vaccine (reporting)
Ultrafiltration rate greater than 13mL/kg/hr (reporting)
PPS Overview
• CMS contends that the $9.23 reduction is attributable to:
– Market basket update = 0.15%
– Wage index budget neutrality adjustment = 0.003%
– Refinement budget neutrality adjustment* = - 4.297%
• Moran Company’s initial analysis indicates that it has
“grave concerns that the adjusters included in the ESRD PPS, including the revisions in the 2016 proposed rule, do not serve a meaningful policy objective. Further [they] are concerned that the assumptions underlying the calculation of adjuster values are not valid, and [they] believe there are serious flaws in the methodology.”
• Moran’s analysis is ongoing
* Accounts for additional dollars included in payment adjusters. 2011 refinement was -5.93%, brining the total adjustment to -9.9597%.
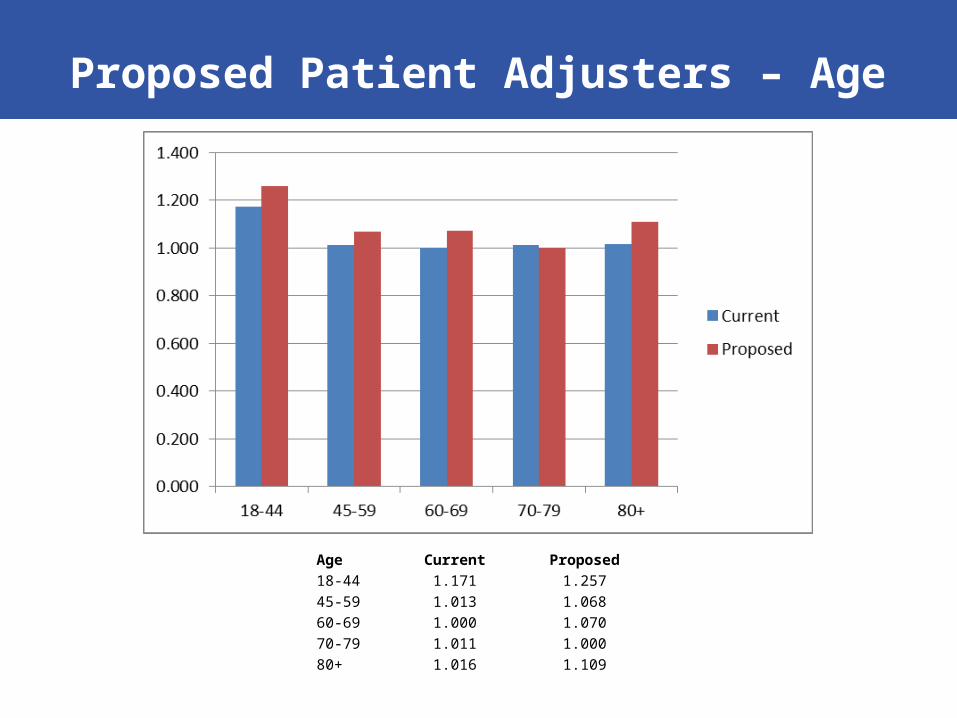
Proposed Patient Adjusters – Age
Age Current Proposed18-44 1.171 1.25745-59 1.013 1.06860-69 1.000 1.07070-79 1.011 1.00080+ 1.016 1.109
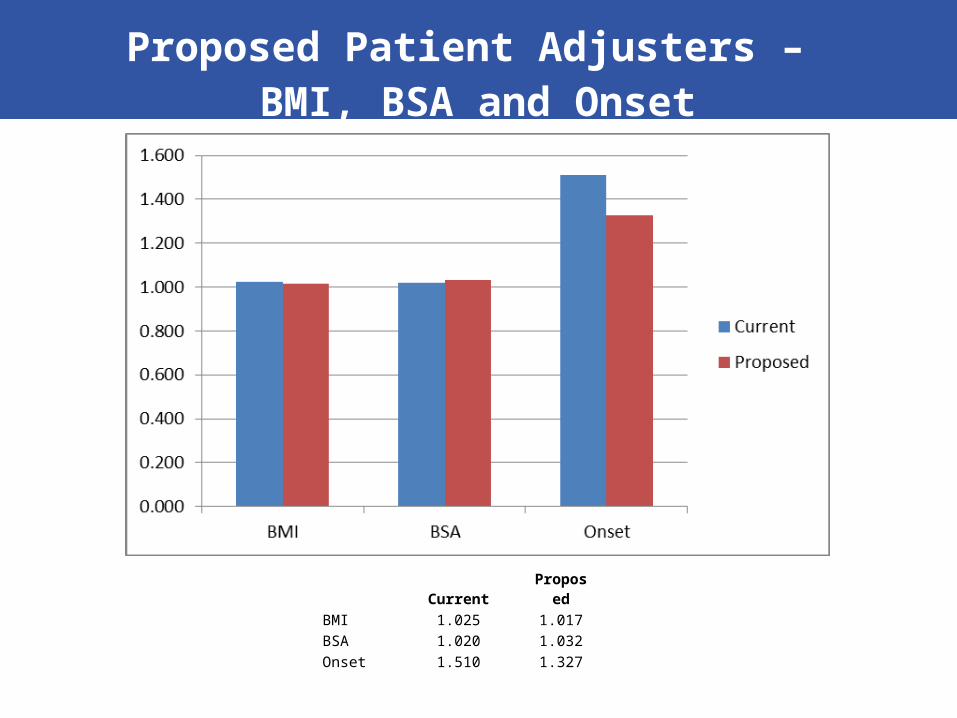
Proposed Patient Adjusters – BMI, BSA and Onset
Current ProposedBMI 1.025 1.017BSA 1.020 1.032Onset 1.510 1.327
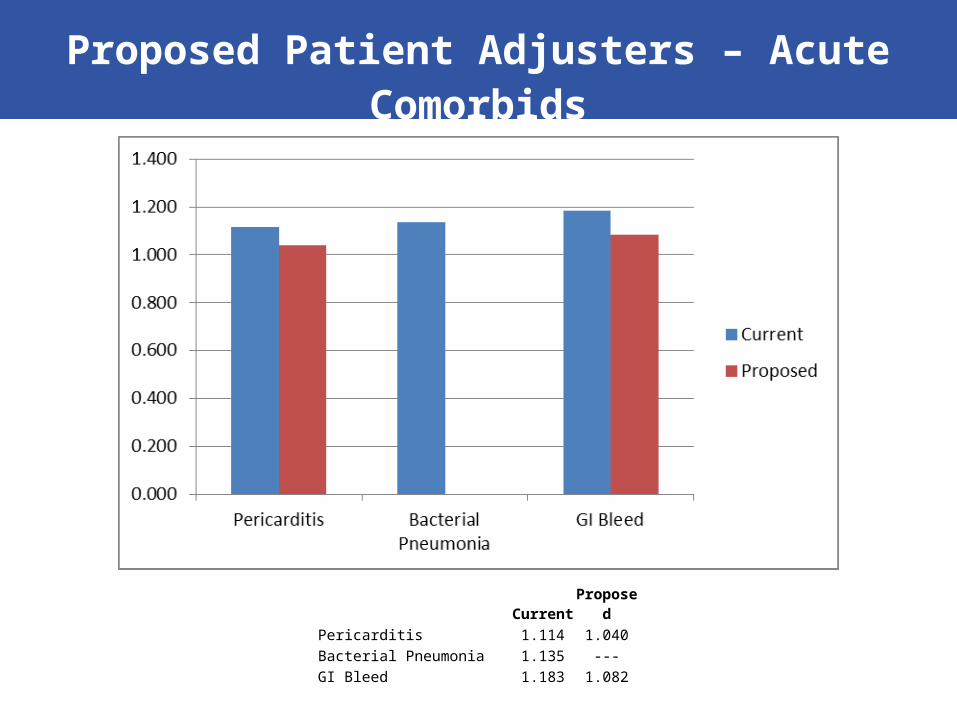
Proposed Patient Adjusters – Acute Comorbids
Current ProposedPericarditis 1.114 1.040Bacterial Pneumonia 1.135 ---GI Bleed 1.183 1.082
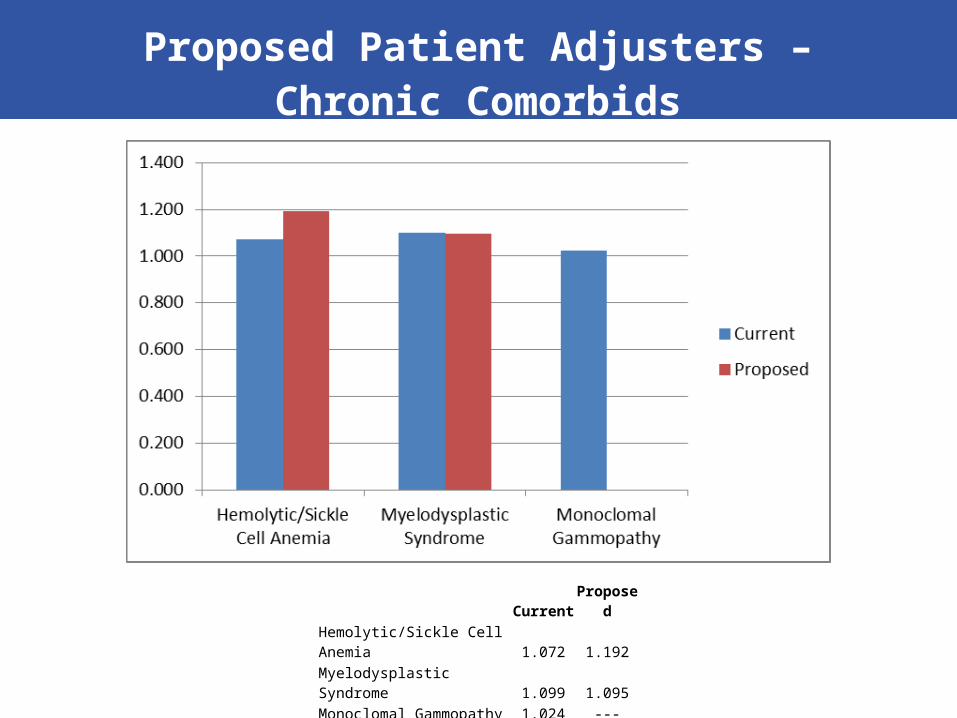
Proposed Patient Adjusters – Chronic Comorbids
Current ProposedHemolytic/Sickle Cell Anemia 1.072 1.192Myelodysplastic Syndrome 1.099 1.095Monoclomal Gammopathy 1.024 ---
Process for Inclusion of New Drugs in PPS
• Protecting Access to Medicare Act of 2014 (PAMA) required CMS to develop drug designation process for:
– Including new injectable and intravenous products into the PPS; and
– Determining when a product is no longer an oral-only drug
• To include new drugs, CMS will first determine whether they are reflected currently in PPS. CMS will asses based on whether product “can be used to treat or manage a condition for which there is an ESRD PPS functional category.”
– If so, new drug is in the bundle and no separate payment is available (though eligible for outlier payment at ASP +6%)
– If not, CMS will add a new functional category to account for drug and add drug to PPS after transition period (when facilities will be paid through transitional drug add-on payment)
New Drugs – Functional Categories
Functional categories used to treat conditions associated with ESRD
Access management AntipruriticAnemia management AnxiolyticBone and mineral metabolism Excess fluid managementCellular management Fluid and electrolyte managementAntiemetic Pain managementAnti-infectives
New Drugs – No Longer Oral Only
• CMS proposes that oral-only drug ceases to be oral only when FDA approves injectable or other form of administration of that drug
• So long as oral-only drugs are part of an ESRD functional category, once an injectable or other form of administration is approved by FDA, such drugs “would be considered reflected in the ESRD PPS bundled payment … so no additional payment would be available for inclusion of these drugs.”
• However, because CMS delayed inclusion of payment for calcimimetics and phosphate binders in the bundle, once injectable or other form of administration (e.g. IV Sensipar) is approved by FDA, CMS will:
– Include non-oral and oral forms of drug in the bundle; and
– Develop a computation for inclusion of the oral and non-oral forms of the drug so that it is appropriately reflected in the base rate.
• Obvious risk is dramatic underfunding of orals as in 2011
• Note – CMS is explicit that no drug in bone and mineral metabolism functional category other than calcimimetics and phosphate binders will add anything to the base rate.
Other PPS Provisions
• Labs– Lipid panels removed from base rate
– Industry had been advocating for this since 2011
– CMS reaffirms use of AY modifier for labs that are not for the treatment of ESRD but that are medically necessary for the patient
• Medical Director fees – CMS proposes to eliminate Reasonable Compensation Equivalent (RCE) limits
for reporting of medical director fees
– RCE had been set at $197,500 for 2015
– Industry had been advocating for elimination of RCE for years
Medicare Policy Changes for AKI
• Medicare coverage of AKI is currently limited to the hospital outpatient department– Has been found to be largely unmanageable for all concerned
• ESRD community has had many discussions with CMS on this subject
• Recent legislation (the trade bill) included a provision changing the coverage for AKI– NOTE: contributed savings to the bill as payment under current system
was twice that of ESRD PPS payment
Coverage & Payment for Renal Dialysis Services for Individuals With AKI
• WHO: Individual who has acute loss of renal function and does not receive renal dialysis services for which payment is made under the PPS
• WHAT: Payment equal to the base rate for ESRD dialysis services – adjusted by any applicable geographic adjustment factor, and – may be adjusted, on a budget neutral basis, by any other adjustment factor (that is
included in the PPS)
• WHEN: Beginning January 1, 2017
• WHERE: Furnished by a Medicare-approved renal dialysis facility (out-patient) or provider of services (hospital based)
• WHY: Treatment unrealistic in hospital outpatient department
Coverage & Payment for Renal Dialysis Services for Individuals With AKI
• Dialysis community will carefully review the proposed rule implementing this provision– once the MD submits a 2728 form, the patient should be eligible for all
adjusters related to the PPS, regardless of the fact that s/he has been dialyzing in an ESRD facility
• Time frame for the proposed rule is uncertain at this time