Embed Size (px)
Citation preview
Essential Thrombocythemia Followed by Acute Leukemia
Does therapy lead to leukemic transition or is it a failure of
accurate diagnosis?
Joel Saltzman MD
Hematology/Oncology Fellow
Metro Health Medical Center
63 yo male admitted with Appendicitis
• Diagnosed with Essential Thrombocythemia 1992. Treated with Chlorambucil to keep platelet count less than <600,000K
• 1999 diagnosed with AML; cytogenetics normal
• Offered induction therapy with 7+3. Pt refused. Continued on Chlorambucil.
• Stable AML x 2 years
WS labs.
• WBC: 14.0, 45% Segs, 7% Bands, 15%Blasts
• Plts: 693K
• PCR for BCR/ABL +
Objectives
• Establish the diagnostic criteria for Essential Thrombocythemia (ET)
• Discuss the natural history of ET
• Discuss the evidence supporting the treatment of ET
• Discuss acute Leukemia following ET
Diagnostic Criteria for ET
• Platelet count >600,000• Hematocrit,40 or normal RBC mass• Normal serum ferritin and MCV• No Philadelphia Chromosome or bcr/abl gene
rearrangement• Absence of collagen Fibrosis on bone marrow• No cytogenetic or morphologic evidence for a
myelodysplastic syndrome• No cause for reactive thrombocytosis
Presenting Features
• Vasomotor symptoms: Erythromelagia
• Headache, dizziness, visual disturbances
• Thrombosis or bleeding
• More common in women
• Splenomegaly
• Asymptomatic
Pathophysiology
• Clonal disorder of a multipotent stem cell which gives rise to erythrocytic, granulocytic, and megakaryocytic series
• Cytogenetic abnormalities demonstrated in <25% of patients– Trisomy 8 most common abnormality
Clinical Course
• No change in life expectancy
• Majority of patients have course complicated by thrombosis and hemorrhage.– Arterial thrombus > venous thrombus– Arterial thrombi more common with
smoking, hypertension, coronary artery disease, diabetes mellitus
What is the evidence supporting treatment for ET?
Cortelazzo et. al. New England Journal of Medicine, April 1995
• Randomized trial comparing treatment with Hydroxurea to no myelosuppression in 114 Pts with ET at high risk for thrombosis.
• Platelet count kept below 600,000 in the treatment group
What defined the High Risk Patient?
• Age > 60 years (55%)
• Previous history of thrombosis (15%)
• Both (30%)
• Platelet Count >1,500,000(excluded from randomization because of high risk of bleeding/thrombosis)
Methods
• 56 pts randomly assigned to hydroxyurea group. Seen every two weeks until plt count <600,000. Starting dose of hydroxyurea 15mg/kg/day.
• 58 patients were the control patients and were seen every two months
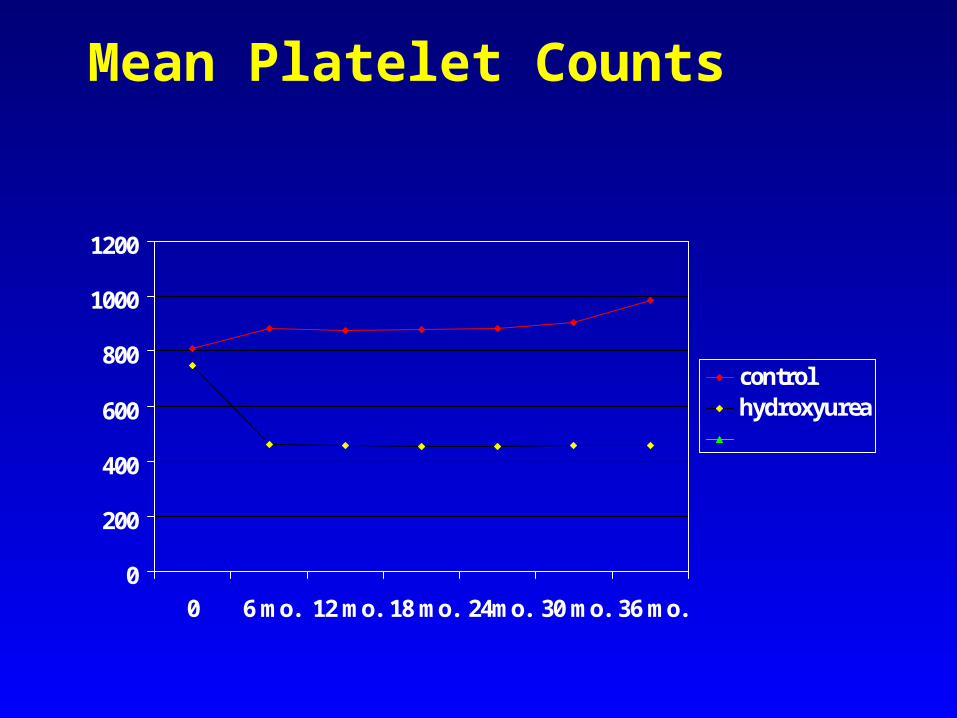
Mean Platelet Counts
0
200
400
600
800
1000
1200
0 6 mo. 12 mo. 18 mo. 24mo. 30 mo. 36 mo.
controlhydroxyurea
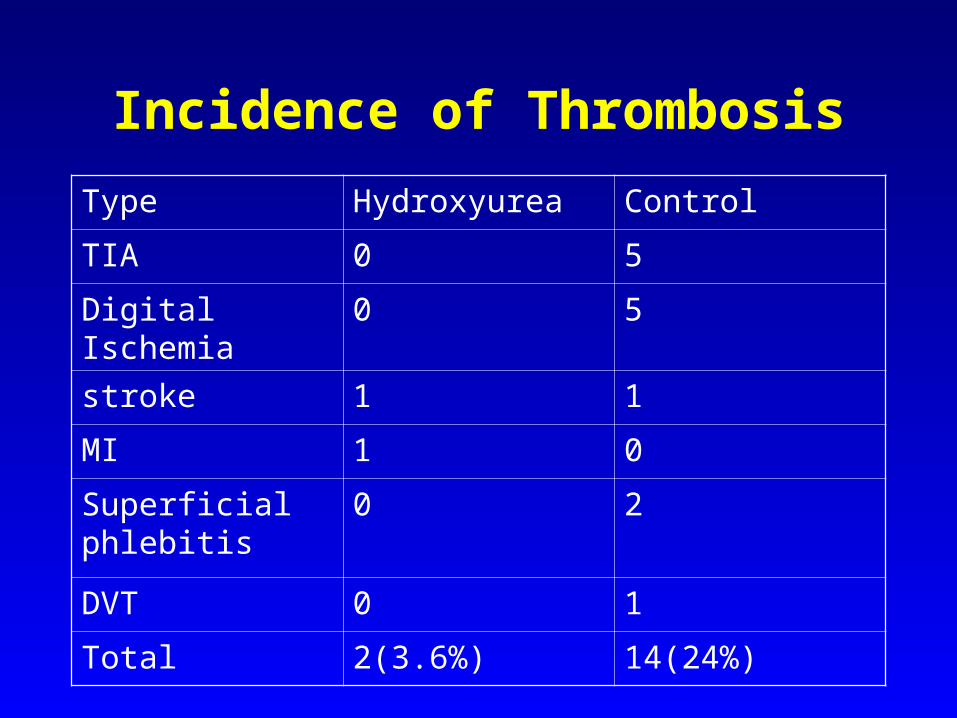
Incidence of Thrombosis
Type Hydroxyurea Control
TIA 0 5
Digital Ischemia 0 5
stroke 1 1
MI 1 0
Superficial phlebitis
0 2
DVT 0 1
Total 2(3.6%) 14(24%)
Hydroxyurea therapy
• Hydroxyurea reduces the incidence of major ischemic episodes from 24% to 3.6% in this high risk patient population
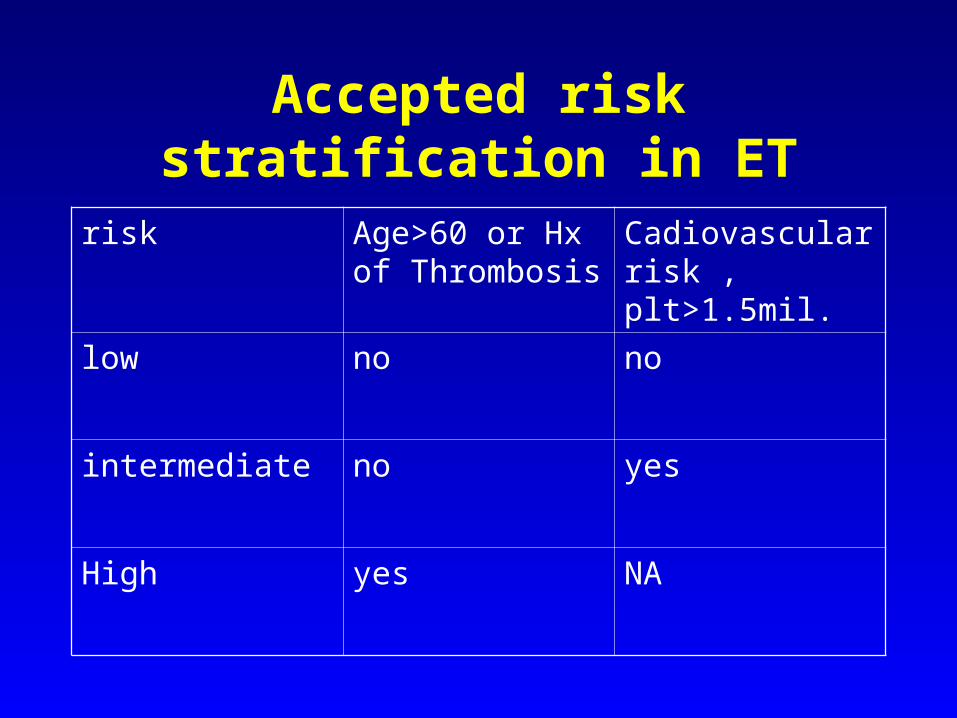
Accepted risk stratification in ET
risk Age>60 or Hx of Thrombosis
Cadiovascular risk , plt>1.5mil.
low no no
intermediate no yes
High yes NA
So Why Worry?
• Berk et. al. New England Journal of Medicine, 1981, “Increased Incidence of Acute Leukemia in Polycythemia Vera associated with Chlorambucil therapy”
• 431 patients randomized to phlebotomy alone, clorambucil, and radioactive phosphorus
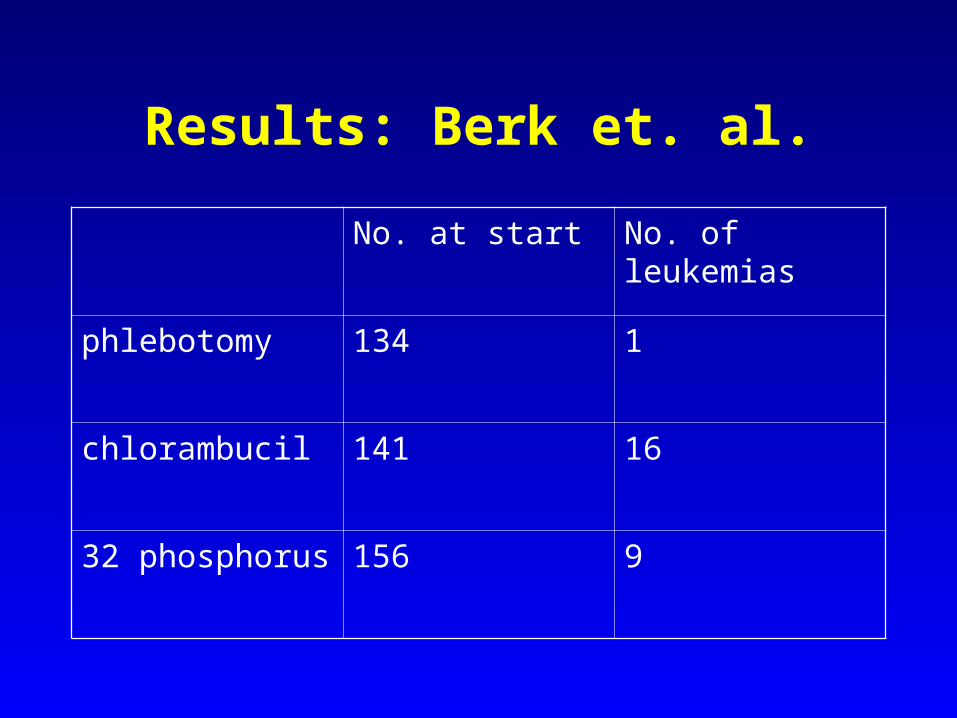
Results: Berk et. al.
No. at start No. of leukemias
phlebotomy 134 1
chlorambucil 141 16
32 phosphorus 156 9
Experience of the PVSG with ET
• Study the Clonal Myeloproliferative Diseases for the past 20 years– Polycythemia Vera– Essential Thrombocythemia– Chronic Myeloid Leukemia– Myelofibrosis
Modifications in the Diagnostic Criteria for ET
• Used to include stainable iron in marrow• Now a normal or increased ferritin is
accepted to r/o Iron Deficiency• Absence of bcr/abl gene rearrangement
or Philadelphia chromosome• No cytogenetic or morphologic evidence
of MDS. Absence of 5q- or ringed sideroblasts
Presenting Characteristics of 100 patients with original criteria
• PVSG chose only patients with plts> million. (9 were excluded)
• 50/91 met all the newly established criteria for ET
• 41 patients patients did not meet all established criteria.– Three major problems were found in these
41 patients
Major difficulties with 41pts
• Iron deficiency not rule out (28 pts)
• Polycythemia Vera was not formally excluded (9pts)
• Lack of karyotypic analysis to exclude Philadelphia chromosome
Lack of bone marrow karyotype adequate to rule-out PH1
• 18 patients lacked this analysis• 6 of these patients eventually had
karyotypic analysis consistent with CML. Most progressed to chronic phase CML and 5/6 progressed to acute blastic leukemia
• It is now recognized that some CML patients will have bcr/abl without chromosomal abnormality
Patients were placed in 4 prospective trials
• Protocol 54:randomization between radioactive phosphorus and Melphalan
• Protocol 10: same as above except increased dose of 32P
• Protocol 12: Hydroxyurea
• Seven patients were simply followed without treatment
PVSG experience with Hydroxyurea in ET
• 29/91 of these initial patients were enrolled in PSVG-12
• 6/29 developed acute leukemia
• No major differences were observed between the two groups were noted
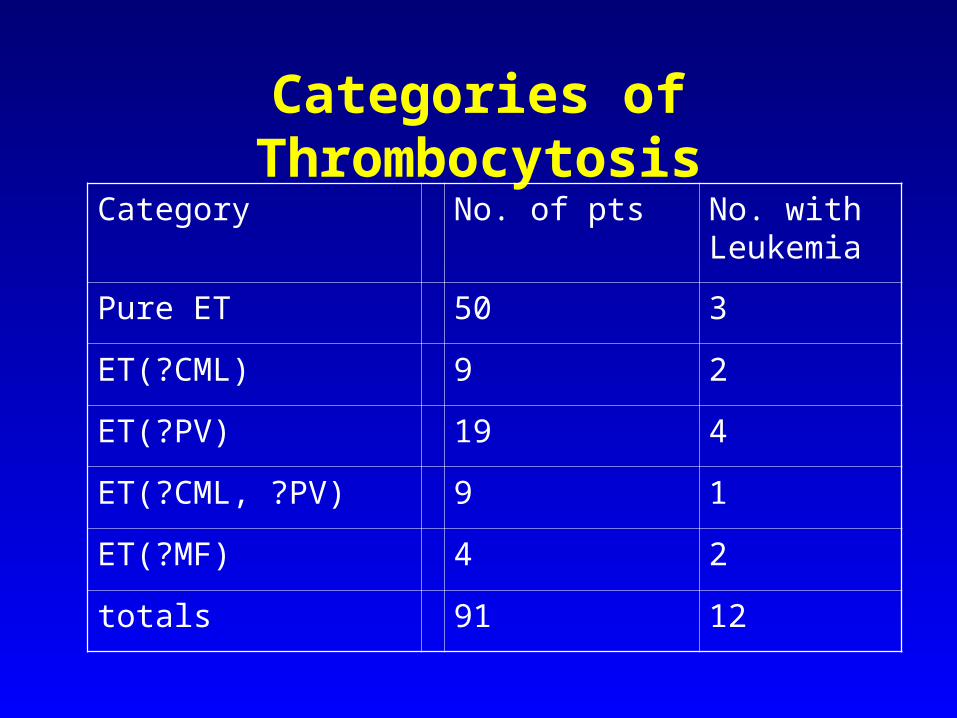
Categories of Thrombocytosis
Category No. of pts No. with Leukemia
Pure ET 50 3
ET(?CML) 9 2
ET(?PV) 19 4
ET(?CML, ?PV) 9 1
ET(?MF) 4 2
totals 91 12
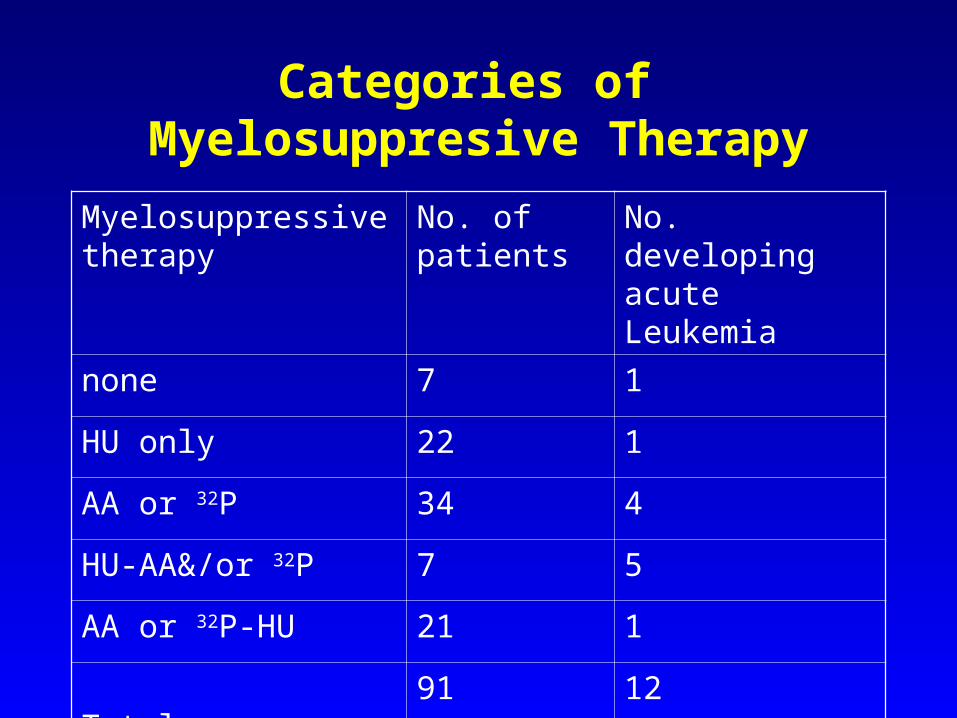
Categories of Myelosuppresive Therapy
Myelosuppressive therapy
No. of patients
No. developing acute Leukemia
none 7 1
HU only 22 1
AA or 32P 34 4
HU-AA&/or 32P 7 5
AA or 32P-HU 21 1
Totals 91 12
Conclusions
• Hydroxyurea remains the treatment of choice for patients at high risk for the thrombotic complications or at risk for them
• Low incidence of acute leukemias in patients treated with HU alone, suggests the lack of a leukemogenic effect
• Accurate diagnosis of ET is essential to long term management (I.E. send RT PCR for BCR/ABL)



















![[insert cool codename here] Ames Bielenberg David Saltzman](https://img.pdfslide.net/doc/110x75/56649d2d5503460f94a0457c/insert-cool-codename-here-ames-bielenberg-david-saltzman.jpg)









