Embed Size (px)
Citation preview

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Essentials of Human Diseases and Conditions
6th edition
Margaret Schell FrazierJeanette Wist Drzymkowski
1

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Chapter 4
Diseases and Conditions of the Endocrine System
2

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Learning ObjectivesLesson 4.1: Endocrine System Structures,
Functions, and Conditions1. Describe the importance of hormones and explain some of the critical body functions that they control.
2. List the major glands of the endocrine system.3. Explain the importance of normal pituitary function.
4. Compare gigantism to acromegaly.5. Describe the condition of dwarfism and its etiology.
6. Explain the cause of diabetes insipidus.
3

Copyright © 2016, Elsevier Inc. All Rights Reserved.
7. Explain the treatment of a simple goiter.8. Compare the signs and symptoms of thyroid hypofunction with those of thyroid hyperfunction.
9. List the signs and symptoms of Graves disease.10. Distinguish between cretinism and myxedema.
4
Learning ObjectivesLesson 4.1: Endocrine System Structures,
Functions, and Conditions (Cont.)

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Orderly Function of the Endocrine System
� The endocrine and nervous systems interact to:Ø Maintain homeostasisØ Respond to stress
� Nervous system creates an immediate but short-lived response
� Endocrine system has a slower onset and longer duration of action, uses hormones to control its response
5

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Major Glands of the Endocrine System
� Anterior and posterior pituitary� Thyroid and parathyroid� Adrenal cortex and adrenal medulla� Pancreas, ovaries, and testes� Thymus and pineal gland
6

Copyright © 2016, Elsevier Inc. All Rights Reserved.
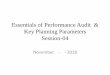
Major Glands of the Normal Endocrine System
7
From Patton KT, Thibodeau GA: The human body in health & disease, ed 6, St Louis, 2014, Elsevier.

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Hormones of the Endocrine System
� Regulate critical body functionsØ Urinary outputØ Cellular metabolic rateØ Growth and development
� Hormonal secretions typically are regulated by negative feedback
8

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Hypothalamus-Pituitary-Thyroid Gland Feedback Mechanism
9
From Gould B: Pathophysiology for the health professions, ed 3, Philadelphia, 2006, Saunders.

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Hormones and Endocrine Glands
� Tropic hormones stimulate secretion of other hormones
� Other secreting cells that perform endocrine functions may be scattered in the tissue
� Hormones regulate body function and promote health
� The pituitary gland plays a central role in regulating most of the endocrine glands
10

Copyright © 2016, Elsevier Inc. All Rights Reserved.
The Pituitary Gland
� Has a cascading effect on glands it stimulates� Divided into anterior and posterior lobes� The hypothalamus controls many activities of the pituitary gland through neural and chemical stimuli
� Pituitary dysfunction can affect some or all of the glands that are targets of hormones
11

Copyright © 2016, Elsevier Inc. All Rights Reserved.
The Effect of Pituitary Hormones on Target Tissues
12
From Applegate EJ: The anatomy and physiology learning system, ed 4, St Louis, 2011, Saunders.

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Gigantism
� When the hypersecretion of growth hormone (GH) occurs before puberty
� Symptoms include abnormal and accelerated growth, especially of the long bones
� Sexual/mental developments are retarded� An anterior pituitary adenoma is often the cause of over-secretion of GH
13

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Effects of Growth Hormone
14
From Thibodeau GA: Anatomy and physiology, ed 6, St Louis, 2006, Mosby. Courtesy of Dr. Edmund Beard, Cleveland.

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Treatment of Gigantism
� Reduce the amount of GH that is secretedØ Ideally done with surgeryØ Additional medicationØ RadiationØ Appropriate gonadal hormones (children)
15

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Transsphenoidal Approach
16
From Rudy E: Advanced neurological and neurosurgical nursing, St Louis, 1984, Mosby.

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Acromegaly
� Occurs with an excessive overgrowth of soft tissue
� The jaw grows, causing larger spaces between the teeth, joint pain occurs
� A pituitary tumor or adenoma often is the cause of acromegaly
17

Copyright © 2016, Elsevier Inc. All Rights Reserved.
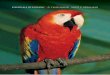
Clinical Features of Acromegaly
18
From Bennett JC, Plum F: Cecil textbook of medicine, ed 20, vol 2, Philadelphia, 1996, Saunders.

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Treatment of Acromegaly
� Reverse or prevent tumor mass effects and reduce the amount of GH secretedØ Ideally done with surgery with or without addition of medication or radiation to pituitary gland to reduce size
� No prevention is known
19

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Hypopituitarism
� Deficiency of pituitary hormones that can cause atrophy
� Reduced thyroid-stimulating hormone (TSH) secretion results in abnormal thyroid function
� Reduced corticotropin affects salt balance and nutrient metabolism
� Gonadotropin deficiency impairs sexual functions
20

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Hypopituitarism (Cont.)
� Cause may be a pituitary tumor or a tumor of the hypothalamusØ Some causes are congenital deficiencies and some are acquired
� The age of the patient, the severity and type of deficiency, and the underlying cause determine the treatment
21

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Dwarfism
� Hyposecretion of the pituitary gland hormones results in growth retardationØ The child is extremely short, with a body that is small in proportion
Ø The prepubescent child does not develop secondary sex characteristics
� Can be congenital, the result of a cranial tumor, or hemorrhage after birth
22

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Dwarfism (Cont.)
� Somatotropin (hGH) is administered until the child reaches a height of 5 feet
� These children also may need replacement of thyroid and adrenal hormones
� Sex hormones administered if needed� Known causes are not preventable
23

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Diabetes Insipidus
� Deficiency in the release of vasopressin, resulting in polyuriaØ The patient experiences excessive thirst, fatigue, and symptoms of dehydration
� The condition may be hereditary or may be the result of an insult to the hypothalamus or pituitary gland
24

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Treatment of Diabetes Insipidus
� Vasopressin injections, nasal spray, or oral desmopressin acetate Ø In nephrogenic diabetes insipidus, thiazide diuretics act by inducing mild volume depletion
Ø In kidneys, the hypovolemia induces an increase in proximal sodium and water resorption, reducing urine output
25

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Thyroid Gland Diseases
� May be resolved through medical and surgical intervention
� Under the control of TSH from the pituitary gland, the thyroid gland produces T3 and T4
� Thyroid hormones affect the metabolism of all body tissues
26

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Simple Goiter
� May be asymptomatic in the early stages� Patient may be unaware of the condition until the thyroid swells
� Hyperplasia causes difficulty swallowing and dyspnea
� Weight loss and heat intolerance may occur
27

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Goiter
28
Courtesy Mark W. Parker, MD, Charlotte, N.C.

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Simple (Nontoxic) Goiter
� Results from a shortage of iodine in the diet, which is necessary for the synthesis of both T3 and T4
� Early treatment: One drop per week of saturated solution of potassium iodide
� Sporadic goiter requires avoidance of goitrogenic drugs or food
29

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Hashimoto Thyroiditis
� Leading cause of goiter and hypothyroidism� Symptoms of hypothyroidism: sensitivity to cold, weight gain, fatigue, depression, and mental apathy
� Heredity plays a prominent roleØ Antibodies appear to destroy thyroid tissue instead of stimulating it
30

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Treatment of Hashimoto Thyroiditis
� Lifelong replacement of thyroid hormones in hypothyroid patients
� Mild hypothyroidism is common and usually responds well to thyroid replacement therapy
� No prevention is known
31

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Graves Disease
� Overproduction of thyroid hormone causes increased metabolism and multisystem changesØ Heartbeat and palpitations, nervousness, excitability, and insomnia
Ø Weight loss and profuse perspirationØ Hyperactive behavior, tremor, hair loss, and exophthalmos
32

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Graves Disease (Cont.)
33
From Stevens A, et al: Core pathology, ed 3, London, 2010, Mosby.

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Graves Disease (Cont.)
� Believed to be an autoimmune responseØ Antibodies to thyroid antigens stimulate the hyperactivity of the thyroid gland
� TreatmentØ Administration of antithyroid drugs and blockersØ Radioactive iodine or surgery
34

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Hypothyroidism
� Several possible causes must be considered, including familial tendency
� At first the symptoms may be subclinical or subtle
� A simple blood test measures the level of TSH secreted by the pituitary and levels of thyroid hormones T3 and T4
� Treated with hormone replacement
35

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Cretinism
� The thyroid gland is absent or thyroid hormone isn’t synthesized by thyroid glandØ Causes growth and mental retardationØ The child develops as a dwarf, stocky in stature with a protruding abdomen
Ø Sex organs don’t develop and there’s a lack of muscle tone
36

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Cretinism (Cont.)
� An error in fetal development may cause the thyroid gland to fail to develop or to functionØ The patient may have a congenital absence of one of the enzymes necessary for T3 and T4 synthesis
� Early treatment with thyroid hormone promotes normal physical growth, but may not prevent mental retardation
37

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Myxedema and Myxedema Coma
� Excessive fatigue, muscular weakness, loss of hair, weight gain, constipation, and intolerance to cold are common
� The skin is dry and scaly and there is puffiness of the hands and face in addition to an enlarged tongue
� Myxedema coma is a medical emergency
38

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Myxedema Facies
39
From Seidel HM, et al: Mosby's guide to physical examination, ed 7, St Louis, 2011, Mosby. Courtesy Paul W. Ladenson, MD, The
Johns Hopkins University and Hospital, Baltimore.

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Myxedema and Myxedema Coma (Cont.)
� The thyroid gland’s ability to synthesize T4 is impaired
� May be secondary to failure of the pituitary to produce thyrotropin
� The goal of medical management is normal thyroid function with the lowest possible doseØ Replacement therapy is required for life
40

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Learning ObjectivesLesson 4.2: Thyroid Issues and Diabetes Mellitus
11. Describe the signs and symptoms of thyroid malignancy. Discuss the most important prognostic factor.
12. Compare and contrast hyperparathyroidism and hypoparathyroidism.
13. Describe Cushing syndrome and Addison disease.
14. Explain the pathogenesis of diabetes mellitus.15. Identify the two major types of diabetes mellitus.
41

Copyright © 2016, Elsevier Inc. All Rights Reserved.
16. Distinguish between diabetic coma and insulin shock.
17. Explain the medical management of all three types of diabetes mellitus.
18. Discuss why early recognition of metabolic syndrome offers the patient an advantage to focus on intervention.
19. Explain why hypoglycemia can be a serious medical condition.
20. Define precocious puberty.
42
Learning ObjectivesLesson 4.2: Thyroid Issues and Diabetes Mellitus (Cont.)

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Thyroid Cancer
� Includes primary thyroid tumors, thyroid lymphoma, and metastases from breast, colon, kidney, or skin cancers
� Signs include a hard, painless lump on the thyroid gland, vocal cord paralysis, obstructive symptoms, and cervical lymphadenopathy
43

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Etiology of Thyroid Cancer
� Causes include multinodular goiter, Hashimoto thyroiditis, cysts, follicular adenomas
� The four main types of thyroid cancer are papillary, follicular, medullary, and anaplastic
� A genetic susceptibility to tumors is indicated
44

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Diagnosis and Treatment of Thyroid Cancer
� Thyroid nodules are usually discovered by the patient or found on physical examination Ø TSH is measured in all patients with thyroid nodules
Ø Fine-needle aspiration (FNA) and histologic exam of the nodule tissue are needed to confirm
� Primary therapy for papillary, follicular, and medullary thyroid cancers is surgery
45

Copyright © 2016, Elsevier Inc. All Rights Reserved.
More Treatments for Thyroid Cancer
� After surgery, patients are started on levothyroxine therapy to prevent TSH stimulation and to prevent hypothyroidism
� Anaplastic tumors require nonsurgical treatment
� Most recurrences of any type of thyroid neoplasm appear within 5 years
46

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Parathyroid Glands
47
From Patton KT, Thibodeau GA: Anthony's textbook of anatomy & physiology, ed 20, St Louis, 2013, Mosby.

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Hyperparathyroidism
� Hyperparathyroidism increases demineralization, resulting in hypercalcemiaØ Hypercalcemia reduces the irritability of nerve and muscle tissue, which causes muscle weakness, atrophy, gastrointestinal (GI) pain, and nausea
Ø Bone tenderness, arthritis type of pain, and easy fracturing of the bones
48

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Regulation of Blood Calcium Levels
49
From Patton KT, Thibodeau GA: Anthony's textbook of anatomy & physiology, ed 20, St Louis, 2013, Mosby.

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Hyperparathyroidism (Cont.)
� Primary hyperparathyroidism causeØ Increased activity of the parathyroid gland
� Secondary hyperparathyroidism causeØ Increased secretion of PTH induced by a low level of serum calcium or vitamin D level
� The treatment plan for hyperparathyroidism varies with the cause and is individualized
50

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Hypoparathyroidism
� When the level of PTH is insufficient, circulating levels of calcium are reduced, resulting in hypocalcemiaØ Initial symptoms include numbness and tingling of fingertips, toes, ears, or nose, followed by muscular spasms or twitching of the hands/feet
Ø Emotional changes, confusion, and irritability occur
51

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Hypoparathyroidism (Cont.)
� Most common cause of hypoparathyroidism is surgical destruction of the parathyroid glandsØ Acquired hypoparathyroidism can result from injury to the parathyroid glands, ischemia from an infarct, accidental radiation, neoplasia
� TreatmentØ Calcium replacement therapy with vitamin D
52

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Cushing Syndrome
� Symptoms: Fatigue, muscular weakness, weight gain, and changes in body appearanceØ Skin becomes thin, has a tendency to bruise easily, and develops red or purple striae
Ø Salt and water retention result in hypertension and edema, and in the characteristic moon face
53

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Appearance of Cushing Syndrome
54
From Wyngaarden J, Smith L, Bennett J: Cecil textbook of medicine, ed 19, Philadelphia, 1992, Saunders.)

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Cushing Syndrome (Cont.)
� Excessive levels of cortisol can be caused by: Ø Hyperplasia of the adrenal glandØ Excessive secretion of corticotropin from the pituitary gland
Ø A tumor of the adrenal cortexØ Production of corticotropin in another organ
� Treatment depends on the cause of oversecretion
55

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Addison Disease
� Symptoms of fatigue, weakness, anorexia, agitation, confusion, weight loss
� Depression, anxiety, and emotional distress are often experienced
� Can result from an autoimmune process, tuberculosis, hemorrhage, fungal infections, neoplasms, or surgical resection
56

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Treatment of Addison Disease
� Treatment includes replacement of the natural hormones with glucocorticoid and mineralocorticoid drugs, and correction of salt and potassium levels
� Early diagnosis and strict adherence to regimen can result in a good prognosis and the patient’s resistance to infection
57

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Before and After Therapy
58
From Zitelli BJ, Davis HW: Atlas of pediatric physical diagnosis, ed 6, Philadelphia, 2012, Mosby.

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Diabetes Mellitus
� Insulin normally reduces blood glucose levels by transporting glucose into the cells as energy and storage as glycogenØ Reduction in insulin results in hyperglycemia and deprives cells of fuel
Ø Ketonuria develops as excess ketone bodies are excreted in the urine, which leads to acidosis
59

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Types of Diabetes Mellitus
� Type 1Ø Has an early, abrupt onset, usually before 30 years of age, with little or no insulin being secreted by the patient
� Type 2Ø Some pancreatic function remains, permitting control of symptoms by dietary management
60

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Diabetic Ulcer
61
From Hill MJ: Skin disorders—Mosby's clinical nursing series, St Louis, 1994, Mosby.

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Diabetes Mellitus (Cont.)
� The disease is often familial but may be acquiredØ Type 1 diabetes
• Infection early in life may trigger an autoimmune process that produces antibodies that destroy the pancreatic �cells
Ø Type 2• Tends to occur in older, overweight adults
62

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Treatment of Diabetes Mellitus
� Type 1 diabetics require insulin replacement therapy that correlates closely with calculated carbohydrate intake
� Type 2 diabetics usually do not necessarily require insulin injections to control blood glucose levelsØ Regimen includes restricted caloric intake and exercise, or oral hypoglycemic medications
63

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Treatment of Diabetes Mellitus (Cont.)
� The sulfonylureas and meglitinide drugs (oral hypoglycemic drugs) stimulate insulin production
� Metformin primarily prevents the liver from producing hepatic glucose but also helps enhance the benefits of insulin
� Acarbose works in the Gl tract to delay the digestion of carbohydrates
64

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Prognosis and Prevention of Diabetes
� Today people with diabetes mellitus are living longer
� The precise causal mechanism of diabetes mellitus remains unknown
� Prediabetes has been identified as a risk factor for progression to type 2 diabetes
� Diabetes is monitored daily by a glucose meter
65

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Insulin Shock and Diabetic Coma
� The patient must be educated to recognize the symptoms of diabetic coma (high blood glucose with the release of ketone levels)
� Insulin shock (excessive insulin)� Take immediate action to correct these serious complications
66

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Insulin Pump Therapy
� Small computerized device that delivers small doses of insulin at regular intervals 24 hours a dayØ It is necessary to test the blood sugar throughout the day and then enter the data into the pump
� The pump is monitored by the patient or a trained caregiver
67

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Gestational Diabetes
� Detected between 24 and 28 weeks of gestation
� Pregnant patient may be asymptomatic or she may exhibit the usual signs of diabetes mellitus
� Increased destruction of insulin by the placenta plays a role in causing GDM
68

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Gestational Diabetes (Cont.)
� Management of GDM is surveillance of mother and fetus because of the increased risk of complications, control of the diet, and limits on simple sugars
� Oral hypoglycemic agents may be prescribed� The risk of cesarean delivery and neonatal complications is increased
69

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Metabolic Syndrome
� Early recognition of this syndrome can help determine suitable interventions
� Main componentsØ Central obesity Ø Blood pressure greater than 130/85Ø Abnormal triglycerides levels above 150 mg/dlØ Abnormal high-density lipoprotein cholesterol Ø Fasting glucose above 100 mg/dl
70

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Hypoglycemia
� Occurs when excessive insulin enters the bloodstream or when the glucose release rate falls below tissue demandsØ The symptoms include sweating, nervousness, weakness, hunger, dizziness, trembling, headache, and palpitations
� Major cause is insulin overdosage in a diabetic subject
71

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Hypoglycemia (Cont.)
� In acute hypoglycemia, the priority is to restore a normal blood glucose level through intravenous infusion of glucose
� Hypoglycemia associated with tumors may require surgery
� The diet is modified to correct hereditary fructose intolerance
72

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Precocious Puberty: Males
� Manifested by early development of secondary sex characteristics, gonadal development, and spermatogenesisØ Pubic hair and the beard begin to grow, the gonads and the penis increase in size, and sebaceous gland activity increases
� Idiopathic precocity may be transmitted genetically
73

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Precocious Puberty: Males (Cont.)
� Therapy depends on the cause of precocious pubertyØ When idiopathic, take hormones to suppress sexual maturation until the appropriate time
Ø When the cause is testicular tumor or brain tumor, the treatment is more invasive, and the prognosis is guarded
74

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Precocious Puberty: Females
� Marked by increased growth rate, breast enlargement, and the appearance of pubic hair and underarm hair before 8 years
� In most cases, precocious puberty in girls is idiopathic, without associated abnormalitiesØ Uncommon causes include intracranial tumors, encephalopathy, meningitis, and endocrine disorders
75

Copyright © 2016, Elsevier Inc. All Rights Reserved.
Precocious Puberty: Females (Cont.)
� Treatment of precocious female puberty depends on the causeØ Tumors, if treatable, may require surgery or radiation
Ø Hormone therapy may be used to suppress the secretion of gonadotropins and to prevent menstruation
76











![AP AMERICAN GOVERNMENT - Crawford's World · Title: Microsoft PowerPoint - Magleby_Ch03.ppt [Compatibility Mode] Author: rcrawford Created Date: 9/16/2012 2:46:37 PM](https://img.pdfslide.net/doc/110x75/5e9e49b4b941d33e274e7f77/ap-american-government-crawfords-title-microsoft-powerpoint-maglebych03ppt.jpg)