Embed Size (px)
Citation preview

250 Journal of Public Health Dentistry
Estimating Dental Treatment Needs among American Indians and Alaska Natives
Eric 6. Broderick, DDS, MPH; William J. Niendorff, DDS, MPH
Abstract
Objective: This paper describes the treatment needs of the American Indian and Alaska Native (Native American) population estimated from the 1991 Indian Health Service Oral Health Status and Treatment Needs Survey(l991 IHSpatient survey). Methods: The average per capita treatment need for the population is expressed both as fhe number of dental services and clinical time required to provide these services. Values for service minutes also are used to compare treatment needed with the treatment provided. Results: The need for dental care is greatest among adults aged2554 years. We anticbate that needs will increase with population growth and as teeth are retained longer. Large amounts of dental needs go unmet each year in the Native American population: because resources are not available to provide all needed care, dental services are prioritized and rationed. The basic premise upon which care is rationed is changing from basic care for all who have access, to more complex care for fewer individuals. This trend may be driven by the opportunity to generate third party revenue offered by more complex procedures. Conclusion: Evaluation is needed of the effects of new approaches on oral health and access to dental care. [J Public Health Dent 2000~60(S~ppl 1):250-5]
Key Words: American Indians, Alaska Natives, dental treatment needs.
The dental literature contains a wealth of information about the oral health status of many populations. It is sparse, however, with regard to studies of population-based needs for dental treatment (1-5). A fundamental function of the IHS patient monitoring system has been to estimate the dental treatment needs of the Native Ameri- can population (6). Historically, the IHS has used these data for the related purposes of program planning and de- velopment, estimating dental work force and clinic size needed to serve the Native American population, and distributing discretionary funds.
Over the past four decades the In- dian Health Service (IHS) has devel- oped a method of estimating the den- tal treatment needs of the American Indian and Alaska Native (Native American) population. The method used to collect the data required to develop these estimates has evolved over time (7-9).
Prior to the use of the American
Dental Association (ADA) standard nomenclature and procedure codes in 1979, the IHS estimated service minute (SM) values for 12 types of services based upon time and motion studies conducted in IHS clinics (10). In 1976-77 the Delphi group consensus technique was used to develop SM values for the extensive list of dental procedures reported by dentists as they actually provided treatment. More than 200 dentists working at IHS clinics were asked to estimate the av- erage amount of operatory time (in- cluding the expanded functions of dental auxiliaries) it took to complete common dental procedures. Dental specialists also were queried regard- ing certain specialty procedures. Each respondent provided an estimated time value in total minutes for each dental procedure. These times were then averaged for each procedure to include a range of one standard devia- tion and the results were again circu- lated to all dentists (not just the re-
spondents) to refine the time esti- mates. A h r d round of estimates was requested for procedures that needed tighter mathematical agreement. The SM values for procedures were as- signed from the final refined esti- mates. These SM values were used to quanbfy the treatment need require- ments identified in patient surveys conducted by the IHS. Actual treat- ment provided by IHS dentists each year also is expressed as an SM value. These values represent an average time, not an actual time, for dentists working in a wide variety of clinic en- vironments. For example, dentists may have expanded duty auxiliaries or may work alone, they may have much experience or be novices, and they may work in school-based pro- gram or in hospital dental programs. Pooled workload data in regional ag- gregates based upon these SM values have been used continually by the IHS to monitor clinical productivity and access to care, and to calculate annual resource distribution formulas.
Collection of Treatment Needs Data (1967-78)
From 1967-78 data on dental treat- ment needs were collected on every dental patient seen at all clinical facili- ties. Because it was a unique reporting system, well ahead of its time and be- fore the ADA created standard no- menclature for dental procedures, the IHS designed the system to be more reliable than sensitive in describing dental needs and treatment proce- dures. Only those procedures that the examining dentist felt would be planned and completed during the fis- cal year were entered into the system. Because it was national IHS policy to examine each patient annually, this methodology resulted in an estimate of the dental needs for the active treat- ment population. The examination
Send correspondence and reprint request to Dr. Broderick, Indian Health Service, Parklawn Building, Room 6A-30,5600 Fishers Lane, Rockville, h4D 20857. E-mail: [email protected]. Dr. Niendorff recently retired from the Indian Health Service and resides in Albuquerque, NM, where he works as a consultant.

Vol. 60, Supplement 4, Special Issue 2000 251
data were transferred to data entry forms and compiled monthly. They were processed with dental workload data to produce quarterly reports de- picting each clinic’s progress in ad- dressing dental needs, as well as an- nual reports estimating program re- source needs at local, regional, and national levels. Although incoming dentists were oriented to collecting needs data as stated in the IHS Manual (11), they were not trained to do so or tested on their ability.
The total units of each need were captured for the following treatment categories: preventive services (pro- phylaxis, topical fluoride), restora- tions (per tooth), periodontics (incipi- ent or overt), oral surgery (extractions, other), and orthodontics (interceptive, corrective). The system did not cap- ture endodontic treatment needs and no distinction was made between fixed and removable prosthetics. This system was well suited for reporting dental workload in the school-based incremental care programs empha- sized by the IHS up until the mid- 1970s (12); however, it lacked suffi- cient detail for capturing needs as the IHS began to treat more adults under a ”demand” care access strategy. Be- cause little care was being provided for adults during this time, their treat- ment needs were generally underre- ported. In other words, dentists were generally less likely to document needed treatment if they did not plan to provide it.
This paper describes the methods used to estimate treatment needs in the 1991 Oral Health Status and Treat- ment Needs Surveys (1991 IHS patient survey) and describes the current treatment needs of the Native Ameri- can population.
Methods In the 1983-84 IHS patient survey
(7), the collection of data on dental treatment needs was based on the methodology promoted by the WHO (13) to create more detailed estimates of resource needs for the entire popu- lation, and also to allow comparison of the needs of Native Americans with those of other populations. Although reporting of needs among adults was substantially better than examination data collected between 1967 and 1978, variability among examiners in re- porting treatment needs remained substantial. One of the objectives of the
1991 IHS patient survey was to make estimates of need more comparable among regions. Estimates of treatment needs were based upon a combination of decisions made by examiners in ad- dition to computed values automat- ically determined by algorithms dur- ing data analysis. Examiners could en- ter one or two treatment need codes for each tooth. Computed values were used to supplement, but not to replace, entries made by examining dentists, unless the entry was determined to be a logical error. Prior to the 1991 IHS patient survey, a working group of public health-trained IHS dentists for- mulated rules and assumptions for de- termining treatment needs based upon restoring oral health in the pri- mary and permanent dentitions. Ideal treatment methods were considered in relation to their cost effectiveness. The goal was to create consistency in de- veloping per capita needs statements across all regional programs using practical, rather than ideal, treatment planning criteria that would not be compromised by examiner omissions and preferences.
Tooth surfaces scored as carious by examiners were assumed to require treatment. Where caries was not pre- sent but examiners felt restoration was indicated, they were required to code the need for restorations using the fol- lowing criteria: (1) to replace a non- carious defective restoration, (2) to re- store a tooth scored as sound accord- ing to the survey criteria for caries, (3) to seal tooth surfaces scored as having incipient decay, (4) to restore surfaces scored as E (excluded) if the examiner judges restoration to be warranted, and (5) to spec+ the need for a cast restoration (crown or onlay) and cast bridge abutments and pontics. In pos- terior teeth, if only the mesial or distal surface was coded as decayed, the oc- clusal surface also was included in the restorative need. The need for occlusal sealants was assumed in sound per- manent molars in patients aged 5-14 years. Primary posterior teeth were as- sumed to need a stainless steel crown restoration when at least one proximal surface was carious on primary first molars of patients under age 7 years and if both proximal surfaces of pri- mary second molars were carious un- der age 9 years. Any primary tooth needing pdpal therapy was assumed to need coronal coverage.
Examiners coded missing teeth in
one of four ways: (1) needing replace- ment, (2) replaced by a fixed pontic, (3) replaced by a removable pontic, or (4) no replacement needed. Teeth coded as needing replacement were as- sumed to need a fixed bridge unless the removable prosthodontics need box was marked for the arch, in which case all missing teeth in the arch were included in the removable partial den- ture need. Fixed bridgework needed, in addition to a removable denture in the same arch, had to be coded sepa- rately for each abutment and pontic as already described. The same criteria were applied to permanent teeth coded as needing extraction. The need for space maintainers in the primary dentition was assumed for posterior teeth needing extraction, using differ- ent age limits for the first and second molars.
In the 1991 IHS patient survey, we attempted to estimate the need for en- dodontic therapy. Nonvital teeth, not coded for extraction, were coded in one of three ways: (1) the tooth needs endodontic therapy (Nl), (2) the tooth has received endodontic therapy (N2), or (3) the pulp status is uncertain or doubtful (N3). The need for endodon- tic therapy in second and third perma- nent molars was included only if the first molar and/or second molar were missing and either of the remaining molar(s) were to serve as abutments for existing or needed fixed or remov- able dentures. All N3 values were sys- tematically converted to N1 or N2 based upon specific tooth status char- acteristics and by random assignment. For pulp therapy in the primary den- tition, all N3 values in posterior teeth and cuspids not indicated for extrac- tion were assigned an N1 value for patients aged 9 years or younger. The need for restorative and endodontic therapy was not determined for pri- mary incisors for patients older than 3 years of age.
Permanent teeth having active car- ies and at least three decayed or filled surfaces were assumed to need cast crowns. The need for a crown also was assumed for teeth that had received endodontic treatment or teeth in need of endodontic treatment if a proximal surface was involved.
The Community Periodontal Index of Treatment Need (CPITN) scoring system was used to determine the periodontal needs for each patient based upon 10 index teeth (10). The
252 Journal of Public Health Dentistry
TABLE 1 Mean Number of Dental Services per Person Required in Permanent Dentition by Age and Type of Care, 1991
Age (Years)
5-1 9 29-34 3544 45-54 55-64 65+ Total
n
9,714 5,676 2,899 1,682 1,076
890 21,937
_ _ _ _ _
Prev. &
Diagn.
2.00 1.73 1.76 1.60 1.32 0.99 1.79
Restor- ative
Full Crowns
Fixed Tooth Pontics
Root Canal Ther.
Perio Pocket Ther.
1.41 2.56 1.90 1.32 1.01 0.65 1.72
0.15 1.18 1.60 1.39 0.94 0.57 0.76
0.04 0.38 0.50 0.37 0.25 0.12 0.23
0.08 0.34 0.32 0.25 0.18 0.09 0.20
0.10 1.13 1.60 1.45 1.23 0.81 0.76
Oral Surgery
0.14 0.89 0.82 1.4 1.48 1.47 0.63
Full Dent.
0.00 0.01 0.08 0.29 0.53 0.79 0.09
-
All Partial Tx Dent Needs
0.00 3.92 0.15 8.37 0.40 8.98 0.60 8.67 0.63 7.56 0.48 5.96 0.18 6.36
TABLE 2 Mean Number of Dental Services per Person Required in Primary Dentition, Patients Aged 0-9 Years, 1991
One Two Three Four Space Surfaces Needing Age Surface Surface Surface Surface Pulp Main- Rest- (Years) n Filling Filling Filling Filling Crown Therapy Extract. tainer oration./Extract.
0-4 2,761 1.5 0.46 0.06 0.001 0.72 0.27 0.17 0.02 4.8
0-9 6,259 1.1 0.46 0.06 0.001 0.63 0.23 0.15 0.04 4.1 5-9 3,498 0.6 0.47 0.06 0.001 0.52 0.19 0.13 0.06 3.3
need for a prophylaxis was assumed for patients having at least one sextant scored as 2 or higher. Patients having four or more sextants of 2 or higher were assumed to need a full mouth debridement (ADA procedure code 4335). The need for pocket therapy, in addition to a prophylaxis, was deter- mined on patients between the ages of 12 and 55 years, based upon the number of sextants having a CPlTN score of 3 or 4 and whether at least two teeth remained that were not marked for extraction. CPITN scores were ig- nored for patients marked as needing complete dentures. For purposes of needs analysis, those patients older than 55 years of age with a CPTT" score of 4, as well as patients receiving care at a clinic other than the one where they were examined and those marked as episodic care users were assigned the need for root planing
For determining orthodontic needs, examiners were not expected to take dentofacial measurements, but were expected to consider deviations in overbite, overjet, midline, and molar relations and also crowding and cross- bites. Need was classified as: none-minor or no deviations; lim-
only.
ited-minor defects that most likely could be treated effectively with space maintainers, removable appliances, or limited banding of teeth; or compre- hensive-included major deviations that would likely involve the extrac- tion of teeth and full arch banding. Skeletal deficiencies that may require jaw surgery also were noted as com- prehensive. Patients with orthodontic treatment in progress or completed therapy were also included in the analysis.
Results The mean number of treatment
services needed per person are pre- sented by age for primary and perma- nent teeth. Service minutes are applied to these treatment needs and pre- sented by type of dental care user-symptomic or regular. Mean minutes of treatment needed and met also are presented in service minutes. Table 1 lists the mean number of den- tal services needed per person in the permanent dentition by age and type of care. The 23 types of care collected in this survey were consolidated into nine broad categories, excluding or- thodontics. The greatest need for treat- ment services occurred between ages
20-54 years and peaked at ages 3544 years at nine services per person. Among patients aged 20-34 years, more than half the need for oral sur- gery services per patient (0.89/pa- tient) is due to impacted third molars. This figure does not include the need for tooth extractions associated with orthodontic care, which far exceeds the need to extract permanent teeth due to dental caries in this age group. Among patients aged 55 years and older, approximately 25 percent of the need for removable dentures is due to the need for reline or replacement of existing dentures.
Table 2 presents the mean number of dental services required per person in the primary dentition of children aged 9 years or less by type of need. Algorithms based upon the antici- pated age of exfoliation of anterior and posterior teeth, as well as the status of tooth eruption, limit the computation of the need for restorative care. For example, diseased anterior teeth are not listed as needing restoration in pa- tients older than 4 years of age, and primary first molars are not included for restoration in those older than 8 years of age. These decisions partially account for the finding that treatment
Vol. 60, Supplement 4, Special Issue 2000 253
FIGURE 1 Time Requirements for Dental Needs by Age and Pattern of Care Usage, 1991
Age Group
FIGURE 2 Mean Minutes of Treatment Needed Compared to Mean Minutes of treatment
Provided, 1991
cn Q
E C a
s
need among children aged 5 to 9 years is lower than that for the younger age group, which also has received less care than the older age group. Because of the algorithms used, the estimates of restorative need in both age groups may be slightly lower than the actual number of services that would be planned for individual patients. Pri- mary molars having proximal surface caries or needing pulp therapy are as- sumed to need crowns (steel or car- bonate), which, like tooth extractions, account for three surfaces of need computed in the final column of Table 2 (Total Tooth Surfaces Needing Res- toration or Extraction). Among the re- gional programs, the Navajo area re- ported the highest need in all catego- ries.
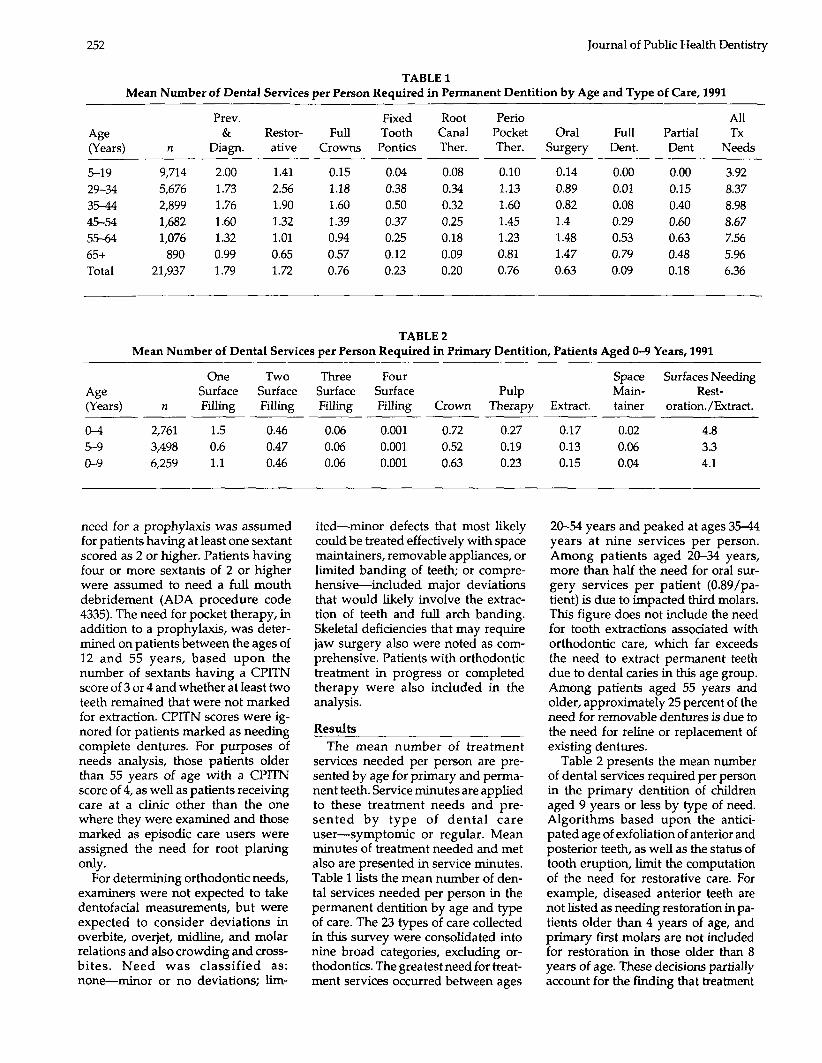
Figure 1 displays the per capita treatment need, expressed as the clini- cal time requirement in service min-
utes by age and care user type (symp- tomatic or routine). Patients were clas- sified as "symptomatic care users" by examiners if the individual sought care only for the relief of oral symp- toms in the three years before the ex- amination. The total per patient time requirement was greatest among adults aged 35-54 years, peaking at over 500 minutes (over 8.3 hours) per patient as the need for cast restorations and fixed prosthodontics became greatest. A decline in the treatment time requirement after age 45 years reflects a shift toward the need for re- movable dentures with increasing tooth loss (Table 1). Symptomatic care users averaged higher time require- ments to meet their needs than did routine care users among all age groups. Routine care users under age 35 years averaged approximately half the total time requirement of older
adults in the other four age groups. However, children aged 5-19 years re- quired over 1.5 hours of care per child, regardless of the care user type.
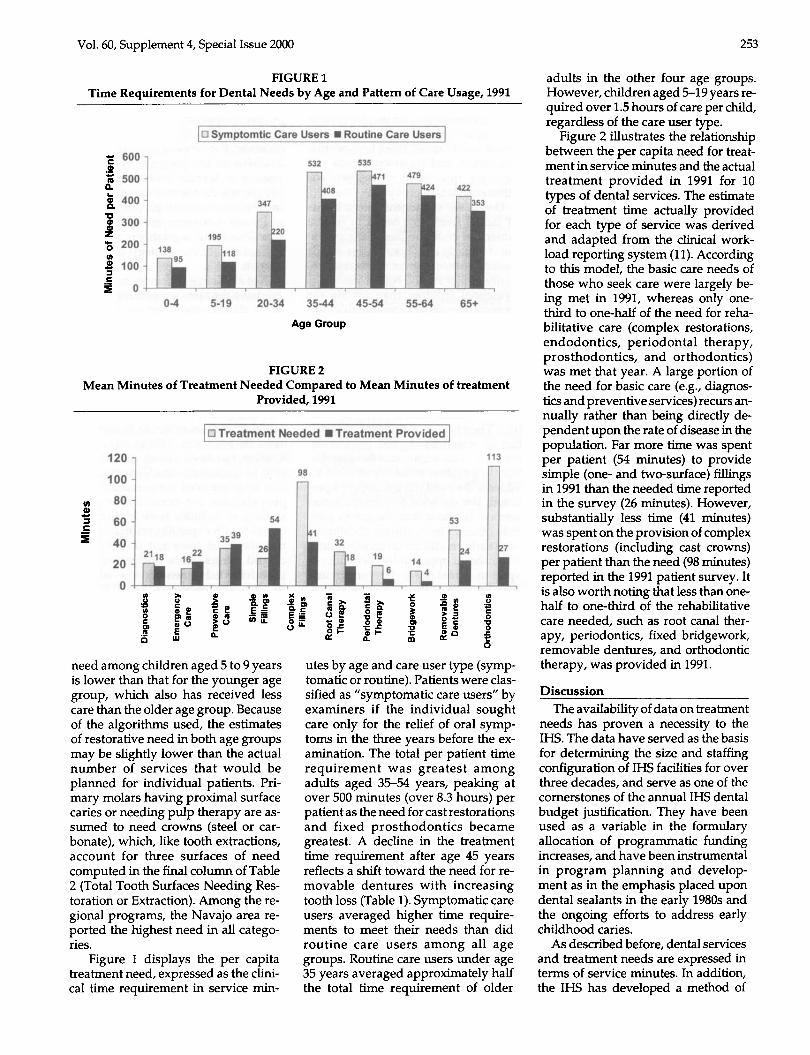
Figure 2 illustrates the relationship between the per capita need for treat- ment in service minutes and the actaal treatment provided in 1991 for 10 types of dental services. The estimate of treatment time actually provided for each type of service was derived and adapted from the clinical work- load reporting system (11). According to this model, the basic care needs of those who seek care were largely be- ing met in 1991, whereas only one- third to one-half of the need for reha- bilitative care (complex restorations, endodontics, periodontal therapy, prosthodontics, and orthodontics) was met that year. A large portion of the need for basic care (e.g., diagnos- tics and preventive services) recurs an- nually rather than being directly de- pendent upon the rate of disease in the population. Far more time was spent per patient (54 minutes) to provide simple (one- and two-surface) fillings in 1991 than the needed time reported in the survey (26 minutes). However, substantially less time (41 minutes) was spent on the provision of complex restorations (including cast crowns) per patient than the need (98 minutes) reported in the 1991 patient survey. It is also worth noting that less than one- half to one-third of the rehabilitative care needed, such as root canal ther- apy, periodontics, fixed bridgework, removable dentures, and orthodontic therapy, was provided in 1991.
Discussion The availability of data on treatment
needs has proven a necessity to the IHS. The data have served as the basis for determining the size and staffing configuration of IHS facilities for over three decades, and serve as one of the Cornerstones of the annual IHS dental budget justification. They have been used as a variable in the formulary allocation of programmatic funding increases, and have been instrumental in program planning and develop- ment as in the emphasis placed upon dental sealants in the early 1980s and the ongoing efforts to address early childhood caries.
As described before, dental services and treatment needs are expressed in terms of service minutes. In addition, the IHS has developed a method of

254 Journal of Public Health Dentistry
categorizing dental services according to priority. Called the “Schedule of Dental Services,” it categorizes all den- tal services into six levels of care, from the highest to lowest priority (14). Emergency care is the highest priority, followed by preventive care, basic re- storative care, limited rehabilitation, and rehabilitation. The schedule was developed to assist community dental programs in managing their resources effectively in a manner consistent with the public health premise of providing the most services to the most people at the lowest cost. Services that alleviate pain or prevent disease are given a higher priority than those intended to contain or correct damage caused by disease. Thus, emergency care has the highest priority, while providing ac- cess to complex rehabilitative care is given the lowest priority. Historically, most services provided to Native American people have been basic care services.
To estimate treatment needs from the 1991 IHS patient survey, the fol- lowing assumptions were made: (1) that the needs determined in this clinic-based survey represent the needs of the entire population, (2) that the need for basic diagnostic and most preventive services is recurring each year, and (3) that the need for more complex services represents the back- log of disease carried over from prior years. Because the backlog of disease is too large for practical elimination in a short period of time, the IHS has used the planning assumption that the re- sources to address the backlog of dis- ease would best be provided incre- mentally over a 10-year period. There- fore, the estimate of need for any given year includes all newly occurring dis- ease and 10 percent of the accrued backlog.
Based on the results of this survey, the age-adjusted per capita need for dental services in 1991 was 95 service minutes. In 1991 the IHS was able to address approximately 32 percent of this need. Since 1991, the IHS budget has not kept pace with population growth or inflation; therefore, the overall need of the population may have worsened. The IHS conducted a subsequent periodic survey of oral health status and treatment needs in 1999. This survey will permit a com- parison of how needs have changed over time and what portion of need is now being addressed.
A comparison of the dental treat- ment needs of the Native American population with those of other popu- lations is difficult. The unique system developed by the IHS to measure oral health needs is not used beyond this population and treatment needs sel- dom are quantified extensively for other population groups.
One of the sigruficant determinants of dental treatment needs in Native American communities is the preva- lence of early childhood caries. While the prevalence of this condition is gen- erally higher among Native American preschool children than among the general population, considerable vari- ation exists among Native American communities and the number of chil- dren who exhibit the worst manifesta- tion of the condition are relatively few. However, the cost of providing care to these children is high, currently esti- mated at more than $2,000 per case (15). Therefore, a sigrhcant propor- tion of resources is used to provide care to a small segment of the popula- tion. In a system without resources to address the needs of the entire popu- lation, the decision to provide some services is also a decision not to pro- vide others. The treatment of children with early childhood caries represents a sigruficant opportunity cost with re- spect to dental needs that remain un- met. Because of the pain often associ- ated with rampant caries and the age of those afflicted, the IHS providers and the communities they serve have opted to accept those opportunity costs and to invest in the treatment of early childhood caries. A considerable proportion of resources has been de- voted to the prevention of early child- hood caries and some progress has been made (15). The success of these efforts ultimately may allow the IHS to address a higher portion of overall treatment needs without increased re- sources.
The recent reorganization of the IHS has resulted in a significant delegation of decision making to the local level. In addition, tribes have assumed in- creased autonomy in management of their health programs. Both these trends have led to adoption of local treatment priorities heretofore not em- phasized by IHS. In some instances, programs have declared preferences for more rehabilitative care for fewer patients. This decision is often driven by the opportunity to increase revenue
collected from third party payers (Medicaid and private insurance) for care provided to Native American people eligible for these benefits. The long range goal of this approach is to increase the overall resource base available to the program by placing priority on services with the potential to generate the most revenue, and us- ing these revenues to support the pro- vision of nonrevenue-generating serv- ices. This trend is relatively new and the success of the strategy is not yet known.
Not all Native American communi- ties have the same opportunity to gen- erate third party revenues. Rates of Medicaid eligibility, state Medicaid dental benefits packages, local em- ployer dental benefit packages, serv- ices available in the local program (in- patient or outpatient), and the local program capacity to bill for and collect third party revenues all affect the po- tential for a local program to supple- ment its resources. Historically, IHS funding has been closely associated with its health facilities. Communities that have received congressional ap- propriations for construction and staffing of facilities have higher per capita health expenditures than com- munities that have not recently re- ceived funds. This budgeting ap- proach has led to inequitable availabil- ity of health resources. The IHS has distributed some discretionary re- sources based upon treatment needs; however, wholesale redistribution of resources to achieve equity or to better address health needs has been politi- cally untenable. It is unclear what ef- fect the availability of third party reve- nue will have upon per capita health expenditures. As the outlook for in- creased congressional budget appro- priations in the near future is not bright, the IHS and the tribes will come to depend more heavily on third party revenue. Because of this trend, we an- ticipated that issues of third party revenue will affect which dental serv- ices receive priority in the future.
The data on treatment needs de- scribed in this paper are based upon a survey of the IHS patient population, and may not represent the treatment needs of the entire population. This approach to the assessment of needs is directly related to the resources re- quired for community-based surveys in a program with a service mission. In addition, it is unlikely that the IHS will

Vol. 60, Supplement 4, Special Issue 2000 255
significantly expand services in the near future, but will continue to focus on people seeking care at IHS clinics. Nonetheless, it would be of interest to compare the treatment needs as esti- mated in this survey with those of the overall population. The opportunity to do this may best be realized in com- munity-based surveys of local popula- tions. We anticipate that needs may be underestimated because they are based on the needs of those who seek dental care; nevertheless, further study is required to validate that as- sumption. The estimated needs are based upon the assumption that serv- ices will be provided only for func- tional requirements; services to ad- dress primarily esthetic concerns were not considered.
The trend away from school-based programs, the use of expanded duty auxiliaries, and recent time-consum- ing infection control procedures have changed many of the original produc- tivity assumptions. Also, new proce- dures such as dental sealants and acid- etched bridges have been added to the
code list and assigned service minute values without a scientific basis. It would, therefore, be timely to reexam- ine the process of estimating the dental team time required to provide com- mon dental procedures.
References 1. Joshi A, Douglass CW, Feldman H,
Mitchell P, Jette A. Consequences of suc- cess: do more teeth translate into more disease and utilization? J Public Health Dent 199636190-7.
2. Grembowski D, Milgrom P, Fiset L. Fac- tors influencing dental decision making. J Public Health Dent 1988;48:159-76.
3. Finklestein MJ, Douglass CW, Chauncey HH. Cumulative incidence of need for restorative dental treatment. J Dent Educ 1985;49:757-62.
4. Hunt RJ, Strkilapanan P, Beck JD. Den- ture-related problems and prosthodontic treatment needs in the elderly. Gerodon- tics 1985;1:226-30.
5. Maryniuk GA, Kaplan SH. Longevity of restorations: survey results of dentists’ estimates and attitudes. J Am Dent Assoc 1986;112:3945.
6. Mecklenburg RE. A data system for den- tal program administration. J Am Dent
7. Niendorff WJ. Selected findings from the oral health survey of FY 1983-84. IHS Dent News 19853:47-51.
ASS 1970;80601-9.
8. Jones DB, Schlife CM, Phipps KR. An oral health survey of Head Start children in Alaska: oral health status, treatment needs, and cost of treatment. J Public Health Dent 1992,5286-93.
9. US Department of Health and Human Services, Indian Health Service. The oral health of Native Americans: a chart book of recent findings, trends, and regional differences. Albuquerque, NM IHS, 1994.
10. US Department of Health Education and Welfare, Indian Health Service. Dental resources criteria and program require- ments for the Indian Health Service. Rockville, MD: MS, 1974.
11. US Deparhnent of Health and Human Services, Indian Health Service. Oral health program guide for the Indian Health Service. Rockville, MD. MS, 1980.
12. Abramowik J. A children’s dental pro- gram for American Indians. J Am Dent Assoc 1970;28:395-405.
13. World Health Organization. Oral health surveys: basic methods. 3rd ed. Geneva: WHO, 1987.
14. US Department of Health and Human Services, Indian Health Service. Oral Health Program Guide for the Indian Health Service. Rockville, MD: IHS, 1997.
15. Bruerd 8, Kinney MB, Bothwell E. Pre- venting baby bottle tooth decay in American Indian and Alaska Native communities: a model for planning. Pub- lic Health Rep 1989;104:631-40.




















![American Indians and Alaska Natives in the U.S. …...Alaska Natives (AIANs) accounted for 1.1 percent of the U.S. civilian noninstitutional population age 16 and older in 2018.[1]](https://img.pdfslide.net/doc/110x75/5fc7e1c0dbd8b357571962f7/american-indians-and-alaska-natives-in-the-us-alaska-natives-aians-accounted.jpg)







