Embed Size (px)
Citation preview

Estimating tibial nail length using forearmreferencing
Stephen Blair*
78 Rotherham Road, Tickhill, South Yorkshire DN11 9NJ, UK
Accepted 25 September 2003
Introduction
Intramedullary nailing is widely used to managetibial fractures. It provides stability and facilitatesearly mobilisation. Several methods of estimatingtibial nail length have been described, such asradiographic templates3,5 and patient height.2
The simplest method is to measure the tibial tuber-osity to medial malleolus distance. This can bemeasured directly1 or indirectly.4 Most methodsrequire an intact contralateral tibia for measure-ment and are, therefore, not suitable for bilateralfractures. Furthermore, the contralateral tibia maybe difficult to measure because of wounds, obesity,other fractures, or a previous tibial fracture. Themain reason for pre-operative estimation of tibialnail length is to have the correct range of naillengths available in the operating theatre. Intra-operative estimation is the most accurate method,but it allows no pre-operative planning. Ideally, afull range of tibial nail lengths should be available,but this is not always the case, particularly whereemergent surgery is involved.
The aim of this study was to assess a simpleforearm referencing method, to estimate naillength preoperatively.
Method
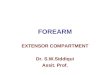
The forearm referencing technique involves mea-suring the distance from the olecranon tip to thehead of the little finger metacarpal (Fig. 1). This canbe described as the olecranon metacarpal distanceor OMD. The elbow and metacarpophalangeal jointsare flexed to 908 and the wrist is held in neutral.
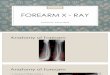
The OMD was measured in 60 members of staff(42 male and 18 female) at Doncaster Royal Infirm-ary, along with the tibial tuberosity to medialmalleolus distance of the ipsilateral tibia. The con-tralateral tibia was measured to exclude a signifi-cant leg length discrepancy. To measure the tibialtuberosity to medial malleolus distance (TMD), thedirect distance between the tibial tuberosityand medial malleolus was used, as described byColen.1 This is shown in Fig. 2. The most prominentpoint of the tibial tuberosity was used. This is notalways a clear landmark, and is a potential source oferror.
Injury, Int. J. Care Injured (2005) 36, 160—162
KEYWORDS
Pre-operative
estimation; Tibial
intramedullary nail
Summary Tibial nail length can be estimated pre-operatively by several methods, butthis usually requires an intact contralateral tibia. The purpose of this study is todescribe an alternative method using the forearm as a reference. A simple clinicalmethod using a forearm measurement is described. This method gives an accurateestimation of the likely range of nail length’s that may be required using a simpleformula.� 2004 Elsevier Ltd. All rights reserved.
*Tel.: þ44-1302-745831/7957658362(m).E-mail address: [email protected] (S. Blair).
0020–1383/$ — see front matter � 2004 Elsevier Ltd. All rights reserved.doi:10.1016/j.injury.2003.09.032

This differs slightly from the method describedby Lottes4 who described a method measuring thevertical distance from the medial malleolus to thelevel of the tibial tuberosity. Measuring directlybetween the landmarks is likely to give a morereproducible measure, but the direct distance willbe slightly longer than the vertical distance. Thedirect TMD measure has been shown to be an accu-rate preoperative nail estimation.1
None of the persons included in the study hadprevious tibial, forearm or metacarpal fractures.
All measurements were taken by the author. TheOMD was then compared with the TMD to look for acorrelation. Linear regression was used to analysethe data. (Using the SPSS for windows statisticalsoftware.)
Results
The mean TMD was 342 mm (range: 300—410 mm).The mean OMD was 352 mm (range: 312—415 mm).
In no case was the TMD longer than the OMD;the measures were equal in three cases. Thegreatest difference between OMD and TMD was35 mm.
The scatterplot of OMD and TMD was linear.Applying linear regression, the Pearson correlationcoefficient (r) is 0.93 (P < 0:005). The statisticalresults are summarised in Table 1.
The regression equation to predict the nail lengthis as follows:
TMD ¼ 9:1 þ ð0:93 � OMDÞ
For example, if the OMD is 350 mm, the TMD iscalculated as follows:
TMD ¼ 9:1 þ ð0:93 � 350Þ ¼ 335 mm
ð95%CI ¼ 303�344 mmÞ
In practice, the TMD does not exceed the OMDand, therefore, TMD represents the longest naillength required. The lower limit of the confidenceinterval represents the shortest nail lengthrequired.
Discussion
The results suggest that the forearm referencingmeasurement (OMD) represents the maximum tibialnail length required and that the shortest nail lengthis 35 mm less than OMD distance. Statistical analysisshows significant correlation between OMD and
Figure 1 Measuring the olecranon metacarpal distance(OMD).
Figure 2 Measuring the tibial tuberosity to medialmalleolus distance (TMD).
Table 1 Summary of linear regression analysis
r-value 0.93r2-value 0.86P-value <0.005Constant coefficient 9.1Regression coefficient 0.93 (95% CI ¼ 0.84— 1.05)
CI: confidence interval.
Estimating tibial nail length using forearm referencing 161

TMD (P < 0:005). The regression equation predictsthe most likely nail length.
The desired tibial nail length will also depend onthe fracture type. A distal fracture will demanda full length nail, just short of the subchondralbone. A slightly shorter nail can be used for amore proximal fracture where the distal nail isleft around 15 mm short of the subchondralbone. In such cases, shorter nails would need tobe available and the OMD distance minus 50 mm(35 mm þ 15 mm) would represent the shortestnail length required. The regression equation isuseful for predicting the nail length but a morepragmatic approach of applying forearm referen-cing is to estimate the range of tibial nailsrequired. In practice, the range is estimated fromthe formula:
Nail length range ðmmÞ ¼ ðOMD�50 mmÞ to OMD
For example, if the OMD was measured at 340 mmthen the nail range required is from 290 (340 �50 mm) to 340 mm. The author has measured theforearm reference in 10 cases of tibial nailing. In allcases, the length of nail used was within the rangeestimated from the forearm.
Conclusion
Forearm referencing provides a useful method ofestimating tibial nail length when the contralateraltibia cannot be used to do so. It provides a simplemethod of estimation that can easily be appliedin clinical practice. The surgeon can then ensurethat the correct range of nails is available in theoperating theatre before embarking on the surgicalprocedure.
References
1. Colen RP, Prieskorn DW. Tibial tubercle-medial malleolardistance in determining tibial nail length. J Orthop Trauma2000;14(5):345—8.
2. Fischmeister MF, Lang T, Reichl C, Wechselberger C. How topredict requisite nail length in tibial fractures. Arch OrthopTrauma Surg 1994;113:194—5.
3. Krettek C, Blauth M, Miclau T, Rudolf J, Konemann B,Schandelmaier P. Accuracy of intramedullary templates infemoral and tibial radiographs. J Bone Joint Surg Br1996;78(6):963—4.
4. Lottes JO. Blind nailing technique for insertion of thetriflange medullar nail. JAMA 1954;155:12.
5. Waldron VD. Predicting intramedullary nail length. Am JOrthop 1998;27(5):383.
162 S. Blair