Embed Size (px)
Citation preview
King Saud University Journal of Dental Sciences (2013) 4, 53–56
King Saud University
King Saud University Journal of Dental Sciences
www.ksu.edu.sawww.sciencedirect.com
ORIGINAL ARTICLE
Estimation of lipid peroxides and antioxidants
in smokers and non-smokers with periodontitis
* Corresponding author.
E-mail address: [email protected] (M.K. Reejamol).
Peer review under responsibility of King Saud University.
Production and hosting by Elsevier
2210-8157 ª 2013 Production and hosting by Elsevier B.V. on behalf of King Saud University.
http://dx.doi.org/10.1016/j.ksujds.2013.05.001
M.K. Reejamol a,*, Mythili Swaminathan b
a PMS College of Dental Science and Research, Vattapara, Indiab RajahMuthiah Dental College, Annamalai University, India
Received 25 September 2012; accepted 3 May 2013Available online 1 June 2013
KEYWORDS
Antioxidants;
Freeradical;
Lipidperoxide;
Smoking;
Periodontitis
Abstract Aim: The aim of the study is to evaluate the relationship between cigarette smoking and
periodontal damage in terms of free radicals and antioxidants.
Materials and methods: 15 Male patients (non-smokers) with chronic periodontitis (age 25–55) and
15 male patients (smokers) with chronic periodontitis were selected as the experimental group;
which is further subdivided as three groups based on the number of cigarettes smoked per day
(group I: <10 cigarettes/day, group II: 10–30 cigarettes/day, group III: >30 cigarettes/day). Dur-
ing surgery, samples of blood were collected from test and control subjects and were subjected to the
estimation of lipid peroxide, reduced Glutathione, Superoxide dismutase, Catalase and total Thiol.
Results: The levels of Lipid peroxide (TBARS), Catalase, and total Thiol in plasma showed a sig-
nificant increase in smokers than non-smokers in such a way that group III showed maximum level
when compared to group I and II. The levels of Superoxide dismutase, and reduced Glutathione
(GSH) in plasma showed a reduction in smokers when compared to non-smokers in which the least
level was obtained in group III.
Conclusion: Based on the results of the present investigation it is concluded that smoking increases
the level of free radicals in periodontal tissues, which in turn may be responsible for the destruction
seen in periodontal disease.ª 2013 Production and hosting by Elsevier B.V. on behalf of King Saud University.
1. Introduction
Periodontal diseases are inflammatory disorders that give riseto tissue damage and loss, as a result of complex interactions
between pathogenic bacteria and host immune response.1
The tissue destructive mechanism involves the release of prote-olytic enzymes and free oxygen radicals from activated neutro-phil.2 The most important reactive oxygen species implicated
in inflammatory injuries to tissues are the hydroxyl (OH) rad-ical, the superoxide anion (O�2 ), the nitrous oxide (NO�) rad-ical, hypochlorous acid, hydrogen peroxide and singlet
oxygen.3
Antioxidants are defined as those substances which whenpresent at low concentrations, compared to those of an oxi-disable substrate, will significantly delay or inhibit the

54 M.K. Reejamol, M. Swaminathan
oxidation of that substrate.4 In normal physiology there isa dynamic equilibrium between ROS (Reactive Oxygen Spe-cies) activity and antioxidant defense capacity. When that
equilibrium shifts in favour of ROS, either by a reductionin anti-oxidant defenses or an increase in ROS productionresults in oxidative stress leading to potential damage.4
Unbalanced radical and non-radical reactive oxygen speciescan damage cells by variant mechanisms including the per-oxidation of lipid membranes, protein inactivation and
introduction of DNA damage, and cytokine induced tissuedamage.5
Smoking exerts a major effect on protective elements ofimmune response, resulting in an increase in the extent
and severity of periodontal destruction.6 Smoking may havean adverse effect on fibroblast function, chemotaxis andphagocytosis of neutrophils, immunoglobulin, production
and induction of peripheral vasoconstriction.7 Exposure tonicotine increases the secretion of PGE2 by monocytes, ele-vated levels of TNF and GCF, elevated levels of neutrophil
elastase and matrix metallo proteinase-8.6 A major exoge-nous source of free radicals is cigarette smoke which con-tains two phases of free radicals one in the gas phase and
the other in tar.8 The obligatory use of body reserve of anti-oxidants to detoxify the excess of free radicals in smoker’sresults in alteration in the level of different antioxidants.The antioxidant disturbance in smokers may be further en-
hanced by their lower intake of both supplemental and die-tary antioxidants.8
Cigarette smoke contains free radicals and other oxidants
in abundance. In one puff of a cigarette, the gas phase ofsmoke exposes 15 times free radicals and oxidants than inthe tar phase. The direct exposure from cigarette smoke repre-
sents only a portion of total oxidative stress and contributes toadditional endogenous oxidant formation through effects oninflammatory immune response.9 In this backdrop, an attempt
has been made in the present study to evaluate the relationshipbetween smoking and levels of antioxidants and free radicals inchronic periodontitis patients.
2. Materials and methods
2.1. Patient selection criteria
The study was conducted at Rajah Muthiah Dental college,Annamalai University and patients devoid of any systemic
disease and had not received any periodontal treatment ormedication for last 6 months were selected. 30 male patientsof age group between 25 and 55 years with chronic peri-
odontitis (with probing pocket depth and attachment lossof 5 mm in at least four sites per quadrant) were selectedand were catagorised as smokers and Nonsmokers. The con-
trol group was nonsmokers comprising 15 patients withchronic periodontitis. Experimental group were smokers withchronic periodontitis and were subdivided into three subgroups based on the number of cigarette consumed per
day. They are,
Group-I: Five subjects smoking less than 10 cigarettes/day.
Group-II: Five subjects smoking 10–30 cigarettes/dayGroup-III: Five subjects smoking more than 30 cigarettes/day.
2.2. Experimental design
Following phase I therapy, prior to surgery, 3 ml of blood was
obtained from patients of control and experimental groups byvein puncture and were collected in pre-heparinised blood col-lection tubes.
2.3. Biochemical analysis
The blood thus obtained was subjected to biochemical tests
and the levels of lipid peroxidise, Superoxide dismutase(SOD), catalase, total Thiol group and reduced Glutathionewere determined.
2.4. Preparation of lysate
The blood was centrifuged at 200g for 20 min at 25 �C. Theplasma was removed aseptically. The red blood cell pellet
was washed three times with sterile saline (0.85 g/100 ml) to en-sure complete removal of plasma; leucocytes and platelets. Thewashed RBC’s were haemolyzed by the addition of sterile dis-
tilled water (1:5). Then, the lysate was centrifuged at 800g for15 min at 4 �C in order to make the lysate ghost free. Thesupernatant was used as a source of various antioxidants(enzymatic/non enzymatic).
2.5. Estimation of lipid peroxidation in plasma
Lipid peroxidation, was estimated by the method of Yagi et al.
as evidenced by the formation of and thio barbituric acid reac-tive substances.10 0.5 ml of plasma lysate was added to 4 ml of(0.083N) sulphuric acid and 0.5 ml 10% phosphotungstic acid,
mixed well, allowed to stand at room temperature for 5 minand centrifuged, and the supernatant was discarded. 2 ml ofsulphuric acid was added to it along with 0.3 ml of 10% phos-
photungestic acid, centrifuged for 10 min and the supernatantwas discarded. 4 ml of distilled water and 1 ml of thio barbitu-ric acid were added, boiled at 95� for 60 min and after cooling5 ml of n butanol was added, mixed vigorously and centrifuged
at 3000 rpm for 15 min and the colour extract in the butanollayer was read at 530 nm. Tubes containing standard malondi-aldehyde 1–5 mol were treated in a similar manner along with
a blank containing 4.0 ml of distilled water. Lipid peroxide lev-els were expressed as nmol/ml plasma.
2.6. Estimation of superoxide dismutase (SOD)
Superoxide dismutase (SOD) activity was assayed by the meth-od of Kakkar et al.11 0.5 ml of plasma /heamolysate was added
with 0.5 ml of water, 2.5 ml of ethanol and 1.5 mol of chloro-form. This mixture (5 ml) is shaken at 4 �C and the centrifugedsupernatant was taken for analysis .The SOD activity is ex-pressed as nmol/mg protein.
2.7. Estimation of catalase
Catalase activity was estimated calorimetrically by the method
of Sinha.12 0.1 ml of plasma/heamolysate was added with 1 mlof phosphate buffer and 0.4 ml of hydrogen peroxide, incu-
Estimation of lipid peroxides and antioxidants in smokers and non-smokers with periodontitis 55
bated for 90 s and to it added 2 ml of dichromate acetic acid.The mixture was incubated in a boiling water bath for10 min and then centrifuged at 10,062g for 15 min. The clear
supernatant obtained after centrifugation was used for mea-suring the absorbance at 620 nm using a spectrophotometer.
2.8. Estimation of total thiol group
The total thiol level was estimated in plasma by the method ofHu.13 0.2 ml sample of 10% plasma was mixed with water to
make the volume up to 0.5 ml. Two millilitres of 0.3 M Diso-dium hydrogen phosphate was added to each sample and0.25 ml of dithio-bis2nitrobenzoic acid (DTNB) reagent was
added just before measuring the absorbance at 412 nm. Totalthiol groups were calculated using an absorptivity of 13,600/cm/M.
2.9. Estimation of reduced glutathione
Reduced Glutathione was measured in plasma according tothe method of Beutler and Kelley.14 This method was based
on the development of yellow colour when dithio-bis-2-nitro-benzoic acid (DTNB) was added to compounds containingthe sulfhydryl groups.
2.10. Statistical analysis
Levels of lipid peroxide, reduced glutathione, superoxide dis-
mutase, catalase and total thiol in plasma between the controland experimental group were statistically treated with a non-parametric test.
3. Results
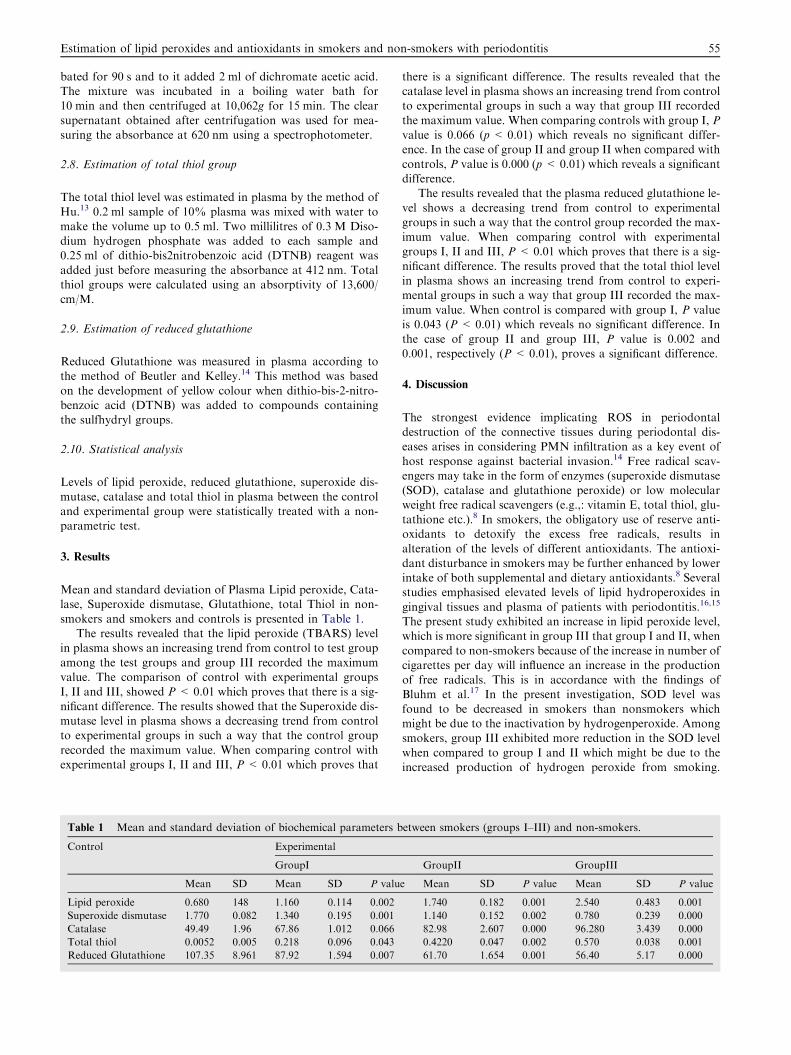
Mean and standard deviation of Plasma Lipid peroxide, Cata-lase, Superoxide dismutase, Glutathione, total Thiol in non-
smokers and smokers and controls is presented in Table 1.The results revealed that the lipid peroxide (TBARS) level
in plasma shows an increasing trend from control to test group
among the test groups and group III recorded the maximumvalue. The comparison of control with experimental groupsI, II and III, showed P < 0.01 which proves that there is a sig-
nificant difference. The results showed that the Superoxide dis-mutase level in plasma shows a decreasing trend from controlto experimental groups in such a way that the control group
recorded the maximum value. When comparing control withexperimental groups I, II and III, P < 0.01 which proves that
Table 1 Mean and standard deviation of biochemical parameters b
Control Experimental
GroupI
Mean SD Mean SD P valu
Lipid peroxide 0.680 148 1.160 0.114 0.002
Superoxide dismutase 1.770 0.082 1.340 0.195 0.001
Catalase 49.49 1.96 67.86 1.012 0.066
Total thiol 0.0052 0.005 0.218 0.096 0.043
Reduced Glutathione 107.35 8.961 87.92 1.594 0.007
there is a significant difference. The results revealed that thecatalase level in plasma shows an increasing trend from controlto experimental groups in such a way that group III recorded
the maximum value. When comparing controls with group I, Pvalue is 0.066 (p < 0.01) which reveals no significant differ-ence. In the case of group II and group II when compared with
controls, P value is 0.000 (p < 0.01) which reveals a significantdifference.
The results revealed that the plasma reduced glutathione le-
vel shows a decreasing trend from control to experimentalgroups in such a way that the control group recorded the max-imum value. When comparing control with experimentalgroups I, II and III, P < 0.01 which proves that there is a sig-
nificant difference. The results proved that the total thiol levelin plasma shows an increasing trend from control to experi-mental groups in such a way that group III recorded the max-
imum value. When control is compared with group I, P valueis 0.043 (P < 0.01) which reveals no significant difference. Inthe case of group II and group III, P value is 0.002 and
0.001, respectively (P < 0.01), proves a significant difference.
4. Discussion
The strongest evidence implicating ROS in periodontaldestruction of the connective tissues during periodontal dis-eases arises in considering PMN infiltration as a key event of
host response against bacterial invasion.14 Free radical scav-engers may take in the form of enzymes (superoxide dismutase(SOD), catalase and glutathione peroxide) or low molecularweight free radical scavengers (e.g.,: vitamin E, total thiol, glu-
tathione etc.).8 In smokers, the obligatory use of reserve anti-oxidants to detoxify the excess free radicals, results inalteration of the levels of different antioxidants. The antioxi-
dant disturbance in smokers may be further enhanced by lowerintake of both supplemental and dietary antioxidants.8 Severalstudies emphasised elevated levels of lipid hydroperoxides in
gingival tissues and plasma of patients with periodontitis.16,15
The present study exhibited an increase in lipid peroxide level,which is more significant in group III that group I and II, when
compared to non-smokers because of the increase in number ofcigarettes per day will influence an increase in the productionof free radicals. This is in accordance with the findings ofBluhm et al.17 In the present investigation, SOD level was
found to be decreased in smokers than nonsmokers whichmight be due to the inactivation by hydrogenperoxide. Amongsmokers, group III exhibited more reduction in the SOD level
when compared to group I and II which might be due to theincreased production of hydrogen peroxide from smoking.
etween smokers (groups I–III) and non-smokers.
GroupII GroupIII
e Mean SD P value Mean SD P value
1.740 0.182 0.001 2.540 0.483 0.001
1.140 0.152 0.002 0.780 0.239 0.000
82.98 2.607 0.000 96.280 3.439 0.000
0.4220 0.047 0.002 0.570 0.038 0.001
61.70 1.654 0.001 56.40 5.17 0.000

56 M.K. Reejamol, M. Swaminathan
Similar results obtained by Bray et al. suggested that free rad-icals, particularly hydrogen peroxide are generated by the di-rect interaction between smoke and periodontal tissues that
will lead to a significant change in the level of antioxidant en-zyme SOD.18 The present study observed an increase in cata-lytic activity in smokers than nonsmokers which might be
caused by higher levels of hydrogenperoxide formation, whichis evidenced in group III than the other two groups. Similartrend was observed in the findings of Hallivell and Gutterdge
et al. in which they observed that an initial rate of hydrogenperoxide removal is directly proportional to its concentration.They emphasised that the enzyme catalase comes into actiononly after an optimum concentration of hydrogen peroxide
has been obtained; below which catalase has no role to play.19
Work done on the status of antioxidants mainly glutathioneperoxidase (GPx) and reduced glutathione in saliva, GCF
and serum of chronic periodontitis patients proved that GSHis a scavenger of hydroxyl radicals and singlet oxygen. It func-tions as a substrate for the hydrogen peroxide removing en-
zyme, Glutathione peroxidase (GPx).20,21,15 The present
study revealed a reduction of GSH levels in smokers, amongwhich group III exhibited the least level. This might be due
to more flux of hydrogen peroxide and hydroxyl radicals influ-enced by smoking. This is in accordance with the study doneby Tribble and Jones. who reported that exposure of tissuesto a large flux of hydrogen peroxide and hydroxyl radicals
might result in an imbalance of GSH and GSSG (reduced/oxi-dised GSH) ratio. They stated that GSSG accumulates in tis-sues and paves the way to the inactivation of various
enzymes which lead to lower levels of GSH in smokers.22
The observation done by Wayner et al. postulated that amongsmokers, there might be some structural modifications in pro-
teins because of oxidative activity, that results in the exposureof protein linked thiol groups so as to react freely and thus de-picts a significantly higher total thiol level.23 The present study
is in favour of the above findings with elevated levels of totalthiol in smokers compared to non-smokers. An insignificantincrease in total thiol in tissues of group I smokers (smoking<10 cigarettes/day might be due to increased free radical pro-
duction but in amounts that are scavenged by antioxidants,such that the damage is limited to few protein molecules.
5. Conclusion
From the above study it is concluded that smoking itself mayproduce free radicals which will increase the Reactive Oxygen
Species (ROS) activity and influence in the increase of levels oflipid peroxide (TBARS), total thiol and catalase. Increase infree radicals may utilise more of antioxidants such as Superox-
ide dismutase, reduced glutathione (GSH) which may furtherinfluence the reduction in the level of these antioxidants insmokers.
References
1. Battino M, Ferrero MS, Gallardo, Newman HN, Bullon P. The
antioxidant capacity of saliva. J Clin Periodontal 2002;29:189–94.
2. Guslaffson A, Asman B. Increased release of free oxygen radicals
from peripheral neutrophils in adult periodontitis after FCR
receptor stimulation. J Clin Periodontol 1996;23:38–44.
3. Chappel ILC. Reactive oxygen species and antioxidants in
inflammatory diseases. J Clin Periodontal 1997;24, 287–229.
4. Iain LC, Chapple, John B Mathews. The role of relative oxygen
and antioxidant species in periodontal tissue destruction. Peri-
odontology 2000;2007(43):160–232.
5. Budueli N, Kardester, Wills CS, et al. Effects of smoking and
gingival inflammation on salivary antioxidant capacity. J Clin
Periodont 2006;33:159–64.
6. Carranza FA, Newman G, TAkei H, Khokkevold PR. Carranza’s
Clinical Periodontology. 10th ed, 2007. p. 251–6.
7. Kinane DFM, Radavar, et al. Smoking on mechanical and
antimicrobial periodontal therapy. J Periodontal 1997;68:467–72.
8. Garg N, Sing R, Dixit J, Jain A, Tewari V. Levels of lipid peroxide
and antioxidants in smokers and nonsmokers. J Periodont Res
2006;41:405–10.
9. Alberg AnthonyJ. The Influence of cigarette smoking on circula-
tory concentrations of antioxidant micronutrients. Toxicology
2002;180:121–37.
10. Yagi K. Lipid peroxides and human diseases. Chem Physiol Lip
1978;45:337–51.
11. Kakkar P, Das B, Viswanathan P. A modified spectrophotometric
assayof super oxide dismutase. Indian J Biochem Biophys
1984;21:130–2.
12. Sinha KA. Calorimetric assay of catalase. Anal Biochem
1972;13:114–7.
13. Hu M. Measurement of protein thiol groups and glutathione in
plasma. Meth Enzymol 1986;233:380–5.
14. Beutler E, Kelley BM. The effect of sodium nitrate on RBC
gltathione. Experientia 1963;19:96–7.
15. Battino M, Ferreiro MS, Bompadre S, et al. Elevated Hydroper-
oxide levels and antioxidants patterns in Papillon Leferve
syndrome. J Periodontol 2001;72, 1760-176.
16. Tuter G, Kurtis B, Serdar M. Interleukin –1B and thiobarbituric
acid reactive substance (TBARS) levels after phase I periodontal
therapy in patients with chronic periodontitis. J Periodontal
2001;72:883–8.
17. Bluhm AC, Western J, Sonsa JA. Free radical in tobacco smoke.
Nature 1971;229:500.
18. Bray RC, Cockle SA. Reduction and inactivation of super oxide
dismutase by hydrogen peroxide. Biochem J 1974;139:43–8.
19. Halliwell B, Gutterdge JMC. Free radical in biology and medical.
Oxford Classdon Press 1989;86–92.
20. Chappel ILC, Mason GI, Garner I, et al. Enhanced Chemilumi-
nescent assay for measuring the total antioxidant capacity of
serum, saliva and cervicular fluid. Ann Clin Biochem
1997;34(4):412–21.
21. Moore S, Calder KAC, Miller NJ, et al. Antioxidant activity of
saliva and periodontal disease. Free Radical Res
1994;21(6):417–25.
22. Tribble DL, Jones DP. Oxygen dependence of oxidative stress.
Rate of NaDPH supply for maintaining the GSH pool during
hypoxia. Biochem Pharmacol 1990;39:729–36.
23. Wayner DDM, Buston GW, Infol KU, et al. The relative
contributions of vitamin E, urate, ascorbate and proteins to the
total peroxyl radical trapping antioxidant capacity of human
blood plasma. Biochem Biophys Acta 1987;924:408–19.





























