Embed Size (px)
Citation preview

Contents lists available at ScienceDirect
Environment International
journal homepage: www.elsevier.com/locate/envint
Estimation of residential radon exposure and definition of Radon PriorityAreas based on expected lung cancer incidence
Elío J.a, Crowley Q.a,⁎, Scanlon R.b, Hodgson J.b, Zgaga L.c
aGeology, School of Natural Sciences, Trinity College, Dublin, IrelandbGeological Survey Irelandc Public Health and Primary Care, School of Medicine, Trinity College, Dublin, Ireland
A R T I C L E I N F O
Handling Editor: Kalantzi Olga Ioanna
Keywords:Indoor radonRadon exposureRadon priority areasLung cancerGeostatisticsKriging
A B S T R A C T
Radon is a naturally occurring gas, classified as a Class 1 human carcinogen, being the second most significantcause of lung cancer after tobacco smoking. A robust spatial definition of radon distribution in the built en-vironment is therefore essential for understanding the relationship between radon exposure and its adversehealth effects on the general population. Using Ireland as a case study, we present a methodology to estimate anaverage indoor radon concentration and calculate the expected radon-related lung cancer incidence. We use thisapproach to define Radon Priority Areas at the administrative level of Electoral Divisions (EDs).
Geostatistical methods were applied to a data set of almost 32,000 indoor radon measurements, sampled inIreland between 1992 and 2013. Average indoor radon concentrations by ED range from 21 to 338 Bqm−3,corresponding to an effective dose ranging from 0.8 to 13.3 mSv y−1 respectively. Radon-related lung cancerincidence by ED was calculated using a dose-effect model giving between 15 and 239 cases per million peopleper year, depending on the ED. Based on these calculations, together with the population density, we estimatethat of the approximately 2,300 lung cancer cases currently diagnosed in Ireland annually, about 280 may bedirectly linked to radon exposure. This figure does not account for the synergistic effect of radon exposure withother factors (e.g. tobacco smoking), so likely represents a minimum estimate. Our approach spatially definesareas with the expected highest incidence of radon-related lung cancer, even though indoor radon concentra-tions for these areas may be moderate or low. We therefore recommend that both indoor radon concentrationand population density by small area are considered when establishing national radon action plans.
1. Introduction
Radon is a natural radioactive gas present in all soils (Cothern andSmith, 1987), representing a significant source of ionizing radiation(WHO, 2009). When radon reaches the outdoor atmosphere it is dilutedto lower concentrations. In confined places (e.g. dwellings, workplaces,caves and underground mines) however, radon may accumulate tohigher concentrations where it may pose a substantial health risk (e.g.UNSCEAR, 2000a; US-EPA, 2003; WHO, 2009). Radon exposure isprincipally linked to lung cancer (e.g. Catelinois et al., 2006; ICRP,1987; Pérez-Ríos et al., 2010), but may also be a contributing factor forother diseases such as skin cancer, Non-Hodgkin's Lymphoma, stomachcancer and brain cancer (Ha et al., 2017; López-Abente et al., 2018;Vienneau et al., 2017).
Globally, lung cancer is one of the most common cancer types, re-sulting in approximately 1.6 million annual deaths worldwide(Sugawara and Nikaido, 2014). In Ireland, lung cancer is the fourth
most common cancer type, and with approximately 2,300 new casesevery year is currently the primary cause of cancer deaths (about 20%of total cancer deaths; NCRI, 2015). Survival rates are normallylow,< 20% after five years (e.g. Drolet and Martel, 2015; Jemal et al.,2010; NCRI, 2015), indicating that any reduction in the number of lungcancer cases will therefore have a significant positive impact on thehealth of the general population. Smoking has an overwhelming in-fluence on lung cancer (i.e. up to 90% may be attributed directly tosmoking; NCRI, 2011), and it may be difficult to identify any increase inthe risk due to other factors (e.g. radon, occupational exposure, airpollution). Darby et al. (2005), however, estimated that the risk of lungcancer increases by about 16% for each 100 Bqm−3 increase of radonexposure, and that between 3% to 14% of lung cancer fatalities globallymay be attributed to inhalation exposure of radon (WHO, 2009). Radonis therefore the second cause of lung cancer after tobacco smoking(WHO, 2009).
The number of annual lung cancer fatalities related to radon
https://doi.org/10.1016/j.envint.2018.02.025Received 6 December 2017; Received in revised form 29 January 2018; Accepted 11 February 2018
⁎ Corresponding author at: Museum Building, Geology, School of Natural Sciences, Trinity College, Dublin 2, Ireland.E-mail address: [email protected] (Q. Crowley).
Environment International 114 (2018) 69–76
0160-4120/ © 2018 Elsevier Ltd. All rights reserved.
T

exposure (e.g. around 18,000 in Europe, Gray et al., 2009; 21,000 in theUSA, Casey et al., 2015) indicates that radon is an important healthissue globally. Radon exposure can however be mitigated if appropriatemeasures are implemented. In this context, for example, the EU de-veloped Council Directive 2013/59/EURATOM, in which the strategiesto reduce exposure to ionizing radiation are defined. The EU Directiveespecially defines radon as one of the risks that Member States shouldaddress, and mentions that each Member State must identify areas (i.e.Radon Priority Areas) where a high radon exposure is probable (i.e.“areas where the radon concentration (as an annual average) in a sig-nificant number of buildings is expected to exceed the relevant national re-ference level”). The efficacy of national strategies has been demonstratedin Ireland where the national average indoor radon concentration hasbeen reduced from 89 Bqm−3 to 77 Bqm−3 since the introduction ofbuilding regulations in 1997 (Dowdall et al., 2017a, 2017b).
Although in this definition of priority areas the health effects are nottacitly mentioned, the EU Directive clearly remarks that the long-termgoal is to reduce the lung cancer risk attributed to radon exposure, andtherefore the main objective of a National Radon Action Plan is to re-duce the adverse health effects resulting from radon exposure. It istherefore beneficial to include the expected number of lung cancercases linked to radon exposure in the definition of Radon Priority Areas.Such a classification will have significant impact on the implementationof a cost-effective and spatially targeted Radon Action Plan (e.g.Bochicchio et al., 2017). Population density is consequently an im-portant consideration in a Linear No-Threshold scenario as described byDarby et al. (2005), since it is understood that there is no lower limit fora safe radon exposure and that exposure to low indoor radon con-centrations may also cause lung cancer. In this sense, for example, interms of lung cancer prevention it could be more effective to reduce theaverage indoor radon concentration in a highly populated area by5–10 Bqm−3 than attempting to do so by 15–20 Bqm−3 in areas with alower population density. Estimation of the number of lung cancer
cases due to radon exposure by administrative level, as proposed in thisstudy, will therefore allow a focussed effort in reduction of indoorradon concentrations in areas where more inhabitants are exposed toradon and, consequently, more lung cancer cases would be expected.
Data pertaining to adverse health effects are often aggregated atadministrative levels (e.g. Electoral Divisions, Municipalities; e.g.Bivand et al., 2008; Hansell et al., 2014), hence analysis of possibleadverse health effects of a contaminant requires estimation of its con-centration at the same domain. In this regard, for radon risk assessmentthe objective is to estimate an average indoor radon concentration in anadministrative area, based on indoor radon concentrations measuredfrom individual houses (Borgoni et al., 2010). Different methods havebeen proposed in the literature, including geostatistical methods (e.g.Borgoni et al., 2010; Ha et al., 2017; Hauri et al., 2012; Vienneau et al.,2017). The advantage of geostatistical methods is that they take intoaccount the spatial correlation between the data (modelled by thevariogram) to predict a value in a non-sample point.
In this paper, we apply a novel and robust method to define RadonPriority Areas, using Ireland as a case study. We estimate an averageindoor radon concentration by Electoral Division (3,409 EDs, with totalpopulation ranged from 66 to 38,900 and an average of 1,400 in-habitants, and areas ranged from 0.04 km2 to 162 km2; Census 2016Central Statistics Office Ireland), and then estimate the number of an-nual lung cancer cases attributed to this carcinogen. Data collected bythe National Cancer Registry are also at this level (NCR/NICR, 2011).The methodology described in this study represents an important ad-vance in the field of radiological protection, helping to define RadonPriority Areas based on a combination of indoor radon concentrationand human population distribution, thereby contributing to a cost-ef-fective national radon action plan.
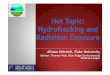
Fig. 1. Indoor radon measurements in Ireland between 1992 and 2013; a) location of indoor measurements (n=31,910), and b) number of dwellings sampled by Electoral Division (ED).
J. Elío et al. Environment International 114 (2018) 69–76
70

2. Material and methods
2.1. Indoor radon measurements
In total 31,910 dwellings (Fig. 1) were sampled between 1992 and2013 by the Environmental Protection Agency of Ireland (EPA), andthen geo-referenced by the Geological Survey Ireland and Ireland'sHealth Service Executive (Hodgson et al., 2014; HSE, 2013). The samedataset has been used as one of several input parameters for developinga new geogenic radon risk map of Ireland (Elío et al., 2017). Indoorradon (InRn) concentrations were measured by installing two alphatrack detectors (CR-39), one in the main living area and another in anoccupied bedroom (Fennell et al., 2002), for a minimum of threemonths and seasonally adjusted to give an annual value (Burke et al.,2010). The average concentration was assigned as the indoor radonconcentration, and the average outdoor radon concentration (i.e.5.6 Bqm−3; Gunning et al., 2014) was subtracted from the data(Hodgson et al., 2014), which improved log-normality (Fennell et al.,2002).
A low number of indoor radon measurements in some EDs hampersestimation of radon exposure in Ireland. In this regard, many EDs (i.e.266 EDs; approximately 8%) have no data or very few indoor radonmeasurements for representative summary statistics (i.e. 2,710 EDs,approximately 80%, have between 1 and 15 indoor radon data mea-surements; Fig. 1b). Geostatistical method overcome this difficulty byestimating an indoor radon concentration in non-sampled points, takinginto account the spatial correlation between observations.
2.2. Geostatistical analysis
The average indoor radon concentration was estimated over largerareas (Electoral Divisions - EDs) by ordinary kriging applying a trans-Gaussian kriging with Box-Cox transformation (Elío et al., 2016). Anindoor radon concentration was then estimated over a grid of100×100m, and the arithmetic mean and standard deviation of thepoints within each ED were calculated. The analysis was carried out onR software (R Core Team, 2016) using package “gstat” and function“krigeTg” (Pebesma, 2004). A variogram was derived from the entiredataset, with a maximum distance between pair of points (“cutoff”) of5,000m. The indoor radon concentration was predicted with a max-imum number of nearest points (“nmax”) of 50.
2.3. Lung cancer cases attributed to radon exposure
The number of lung cancer cases linked to radon exposure wereestimated based on a dose-effect model and the average indoor radonconcentration at ED level. The indoor radon concentration was used tocalculate an annual effective dose (mSv y−1) in each ED, and knowingthe adverse health effects of this radiation dose, the number of lungcancer cases can therefore be estimated. The following equation wasused (Quarto et al., 2015):
=−D [mSv y ] C ·F ·T·F ·F1
Rn E O D
where CRn is the average indoor radon concentration (Bqm−3), FE is theequilibrium factor (FE= 0.4), FO is the occupancy factor (FO=0.8), Tis time in hours in a year (T=8760 h y−1), and FD is the dose con-version factor (FD=14·10−6 mSv per Bqm−3 h).
The number of lung cancer cases per year per million people in eachED was calculated using a conversion factor of 18 mS v−1 y, as re-commended by the International Commission on RadiologicalProtection - ICRP (Quarto et al., 2015). Then knowing the population ineach ED, the total number of lung cancer cases linked to radon exposurewere estimated. The total lung cancer cases in Ireland is the sum of thelung cancer cases in each ED. These were calculated at the 95% con-fidence interval, estimated by Monte Carlo simulation (n=10,000; US-EPA, 2003), assuming a normal distribution of the average indoorradon concentration in each ED, with a mean of the average krigingpredictions, and the standard deviation of these predictions; a log-normal distribution of the equilibrium factor (FE ~ LN(0.40,1.15), US-EPA, 2003); a normal distribution of the occupancy factor (FO ~ N(0.8,0.03), i.e. ranged approximately from 0.7 to 0.9; e.g. Colgan et al.,2008; UNSCEAR, 2000b); a normal distribution of the dose conversionfactor (FD ~ N(14·10−6, 3·10−6), i.e. ranged approximately from3·10−6 to 24·10−6, e.g. EURATOM, 1996; Porstendörfer, 2001;UNSCEAR, 2000a); and a normal distribution of the conversion factorwith a mean of 18 and a standard deviation of 2 (i.e. ranged from ap-proximately 12 to 24).
3. Results
3.1. Indoor radon measurements
Indoor radon concentration data (n=31,910) ranged from 0.1(< limit of detection) to 9,708 Bqm−3, with median and mean valuesfrom the entire data set of 53.4 and 109.7 Bqm−3 respectively (Fig. 1).A log-normal distribution of indoor radon concentration was assumed,although the histogram and normal Q-Q plot (Fig. 2) show a slightdeviation from log-normality, with a left tail of low values (even withsome data lower than the detection limit of 10 Bqm−3, where an indoorradon concentration of 0.01 Bqm−3 were assigned) and some highvalues on the right tail, probably caused by a higher density of dwell-ings sampled in high radon risk areas, and as a consequence, withhigher indoor radon concentrations (Burke and Murphy, 2011). TheBox-Cox transformation (Box and Cox, 1964) confirms that data are notlog-normally distributed (the optimal lambda, and 95% confidence in-terval, was −0.011 [−0.017 to −0.005]), however, the optimallambda is very close to 0 and a log-normal distribution may be assumed(i.e. λ=0 in the trans-Gaussian kriging with the Box-Cox transforma-tion).
Geostatistical analysis indicates the existence of a spatial correlationin the data; the sample variogram being outside the envelope of allvariograms generated by random permutations of the data (Bivandet al., 2008). This spatial correlation was modelled by an exponentialmodel with a sill of 0.606, a range of 1,420m, and a nugget of 0.567(Fig. 2). The high nugget effect confirms that indoor radon concentra-tions have a high variability at a small spatial scale.
Fig. 2. Box-plot, histogram, and Q-Q plot of indoor radon measurements (n= 31,910), and experimental variogram and envelope from random permutation of radon samples.
J. Elío et al. Environment International 114 (2018) 69–76
71

3.2. Average indoor radon concentration and expected numbers of lungcancer cases
The average indoor radon concentrations by ED ranges from 20 to338 Bqm−3 (Table 1 and Fig. 3a), with a Relative Standard Deviation(RSD) mostly between 5% and 20% (Fig. 3b). These average con-centrations correspond to an effective dose ranging from 0.8 to13.3 mSv y−1. The expected number of lung cancer cases per year permillion people due to radon exposure vary therefore from a minimumvalue of 15 and maximum of 239, depending on the ED (Fig. 4a).
Knowing the population density in Ireland by ED (e.g. population in
2016, census data available from the Central Statistics Office - CSO;Fig. 4b), the expected number of lung cancer cases in each ED attrib-uted to indoor radon exposure may be calculated (e.g. number of lungcancer case in 2016; Fig. 4c). It should be noted that there are likelylarge uncertainties when calculating lung cancer incidence at low doserates (ICRP, 2007), however assuming a Linear-No-Threshold for radon-related lung cancer (Darby et al., 2005), this is still a valid approach.The number of lung cancer cases by ED linked to radon exposure in2016 ranged from 0.001 to 2.262, making a total in Ireland of 286(CI95%: 150–474). If the same analysis is carried out for 2011 (2011 and2016 are the last two census data sets available from the CSO in Ire-land), then the number of expected lung cancer cases would be 276(CI95%: 144–457).
4. Discussion
4.1. Average indoor radon concentration
The predicted average (PA) values obtained with geostatisticalmethods (i.e. ordinary kriging) were cross-validated with the arithmeticmean (AM) of the observations for EDs with>25 observations (Fig. 5).In general, the PA and the AM in these EDs are in agreement. The AMranges from 20 to 587 Bqm−3 while the average estimations (PA) rangefrom 24 to 289 Bqm−3 (Fig. 5a), and the differences between PA andAM (in %) are normally lower than±25% (Fig. 5b). These results areeven better for EDs where> 25 dwellings were sampled and the surfacearea is< 2 km2 (Fig. 5c and Fig. 5d). In these small EDs the number ofobservations are spatially well distributed and the AM may represent atrue value of the average radon concentration, hence the similaritiesbetween PA and AM indicate that PA also gives a realistic averageradon concentration in the EDs.
Indoor radon concentration may also have high spatial variability,even at a small scale (e.g. Friedmann et al., 2017; US-EPA, 2001). This
Table 1Number of Electoral Divisions (EDs), population, and estimated radon-related lung cancerincidences.
Average IndoorRadon (Bqm−3)
Number ofEDs
Population⁎ Estimated lungcancer cases
2011 2016 2011 2016
20–25 4 1791 1683 0 025–50 324 394,630 405,230 12 1250–75 1229 1,966,203 2,048,778 87 9175–100 850 1,121,589 1,167,142 68 71100–125 451 517,534 533,289 41 42125–150 267 251,055 258,696 24 25150–175 132 174,096 182,087 20 21175–200 68 89,221 91,546 12 12200–225 46 34,158 34,906 5 5225–250 17 16,055 16,298 3 3250–275 11 11,247 11,544 2 2275–338 10 10,673 10,666 2 2Total 3409 4,588,252 4,761,865 276 286
⁎ 2011 and 2016 are the last two years of census data available from the CentralStatistics Office in Ireland.
Fig. 3. Average indoor radon concentration and Relative Standard Deviation at Electoral Division level (n=3,409).
J. Elío et al. Environment International 114 (2018) 69–76
72

effect was corroborated by the high variability of the Standard Devia-tion (SD) in the EDs with> 25 observations (from 3.47 to 157), and thehigh nugget effect in the variogram (Fig. 2). In this regard the Con-fidence Interval (CI) of the AM may be large, even with high number ofobservations, and geostatistical methods improve the predictions.
Uncertainties on the estimation of radon exposure may also beproduced when indoor radon measurements are clustered around zoneswith high (or low) radon concentrations, and therefore the AM wouldbe not be spatially representative of the radon exposure in an ED,
although the number of data points are high. This effect may causediscrepancies between PA and GM estimates, however the geostatisticalmethods are preferable because these estimates are carried out bymodelling the spatial correlation between observations, and thereforethe effect of data clustering is minimised. The limitation of geostatis-tical methods in this case is when data clustering occurs because housesare built only in a small area of the EDs, where people principally live inrestricted zones. In these cases smoothing the radon concentration byEDs may underestimate, or overestimated, radon exposure. Avoiding
Fig. 4. a) Modelled lung cancer cases per year per million people by ED in Ireland; b) population density in 2016; and c) expected number of lung cancer cases due to radon exposure in2016 (if radon concentration and population by ED were constant, the scale would represent a number of lung cancer cases over a lifetime of 70 years of< 1, 1–5, 5–10, 10–20, 20–50,and> 50).
Fig. 5. Comparison between the predicted average (PA)and arithmetic mean (AM); a) PA vs. AM for EDs with 25 ormore indoor radon measurements (236 EDs, blue linex= y); b) histogram of the differences between PA and AMfor EDs with 25 or more indoor radon measurements; c) PAvs. AM for EDs with 25 or more indoor radon measurementsand an area lower than 2 km2 (33 EDs, blue line x= y) and,d) histogram of the differences between PA and AM for EDswith 25 or more indoor radon measurements and an arealower than 2 km2. (For interpretation of the references tocolour in this figure legend, the reader is referred to theweb version of this article.)
J. Elío et al. Environment International 114 (2018) 69–76
73

this effect would require further investigation of the dwelling dis-tribution at a local scale, potentially allowing for a better assessment ofradon exposure within some EDs. At a national scale level, however,such detail is currently not feasible.
4.2. Lung cancer cases attributed to radon exposure
It has been estimated that the average national indoor radon con-centration in Ireland has been reduced from 89 Bqm−3
(CI95%=88–91 Bqm−3) to 77 Bqm−3 (CI95%=71–83 Bqm−3) be-tween 2002 and 2015 (Dowdall et al., 2017a, 2017b). If the effectivedose and lung cancer incidence per million are estimated (Table 2), andthe total population is around 3.916 and 4.584 million for the periods2000–2004 and 2010–2014, respectively (CSO, 2017, 2006), then thetotal annual radon-related lung cancer incidence is estimated to be 246in 2000–2004 and 249 in 2010–2014 (Table 2). These estimates are inagreement with previous calculations in Ireland (i.e. 250; NRCS, 2014).The slight increase may correspond to an increase of the population byalmost 1 million (20%), even though the national average indoor radonconcentration was actually reduced.
The above estimates are also in agreement with the linear model ofthe dose-response relationship (Darby et al., 2005). In this case, anincrease in the risk of lung cancer is correlated to the radon con-centration by the expression IR= 1+ βCRn (where CRn is the radonconcentration and β is the increase in risk per unit increase in radon;0.16 (CI95%: 0.05–0.31) per 100 Bqm−3; Darby et al., 2005). By si-mulations (n=10,000; CRn2002~N(89,0.75); CRn2016~N(77,3); and β anormal square root distribution with an expected value of 0.16 ,Hassfjell et al., 2017), the increase in risk of lung cancer in Ireland inthe periods between 2000–2004 and 2010–2014 were found to be 1.14(1.05–1.27) and 1.12 (1.05–1.24), respectively. This corresponds to aproportion of the number of lung cancer cases (P= (IR− 1) / IR) at-tributed to radon of 12.5% (5.0%–21.3%) for 2000–2004 and 11%(4.4%–19.4%) for 2010–2014. With the annual average lung cancerincidence in Ireland (i.e. 1,726 in 2000–2004, and 2,332 in 2010–2014;National Cancer Registry Ireland, www.ncri.ie) the expected number ofannual lung cancer cases linked to radon may be calculated as 216(86–368) between 2000 and 2004 and 257 (100–452) in 2010–2014.Comparable to those estimated by the dose-effect model (Table 2).
A population-weighted average for indoor radon may be also usedfor estimating the number of lung cancer cases linked to radon ex-posure. In this case, we have calculated the average based on theaverage indoor radon concentration by ED and the inhabitants of eachED (AMPW= ∑ED(CRn(ED) · p(ER))/∑EDp(ED)), resulting in a population-weighted indoor radon average of 85 Bqm−3 (CI95%: 83–87). The an-nual radon lung cancer incidence may therefore be calculated as 279 or
275 using either the linear model or the dose-effect model, respectively(Table 2). If data obtained by the national radon surveys carried out bythe Environmental Protection Agency of Ireland are used (i.e. 91 and98 Bqm−3 for 2002 and 2016 respectively; Fennell et al., 2002; Walsh,2017; Murphy P., pers.comm., 29 Feb.), then the estimated annualnumber of lung cancer cases in the period 2000–2004 would be 220 and251, for the linear model and the dose-effect model respectively, and316 and 317 in the period 2010–2014 respectively (Table 2). The es-timates using both models are therefore in agreement, showing thatthey can be equally used to estimate radon-related lung cancer in-cidence.
Our calculations of the expected number of lung cancer cases linkedto radon exposure by ED (i.e. 276 [CI95%: 144–457] for 2011 and 286[CI95%: 150–474] for 2016) are similar to the estimates obtained basedon population-weighted averages (around 280–315 for 2010–2014;Table 2) but slightly higher than those obtained using the geographicmeans (around 250; Table 2). These results suggest that estimates basedon the geographic national average underestimate radon related lungcancers, and techniques which take into account the population densityare more accurate to evaluate the health effect of radon exposure. Theestimates by ED also have the advantage that they allow definition of aspatially targeted radon action plan.
A potential limitation of lung cancer estimates at administrativelevel (i.e. ED) with respect to calculations based on population-weighted arithmetic means is however that they are time and resourceconsuming, and therefore it may not be feasible apply this approachregularly to monitor the efficiency of a national radon action plan. Inthis sense, calculations of an average indoor radon concentration by EDrequires a high number of indoor measurements around the country(e.g. in this study we used around 32,000measurements), while anupdate on the arithmetic mean of the indoor radon concentration canbe made with a considerable lower number of houses tested (e.g. inIreland an update was carried out using around 700 randomly selectedhouses, and in less than one year; Dowdall et al., 2017a, 2017b).
On the contrary, although annual surveys represent the actual si-tuation in a country, these surveys may be influenced by the dwellingssampled and by temporal (seasonal) variations on indoor radon con-centration. The AM may therefore fluctuate and may not properly re-present radon exposure to the general population. In order to minimizethese effects the annual surveys may be aggregated in several years (e.g.5 years; minimum period to observe a change of lung cancer risk due toradon exposure, NRC, 1988; Tomášek et al., 2001) and thus the datawill be more representative of radon exposure over long periods. Fur-thermore, since lung cancer has a long latency period (Cheng et al.,2016; Field et al., 2002; NCRI, 2005), aggregating the data over several
Table 2Estimations of lung cancer incidence based on national average indoor radon concentrations.
Period AM SD Linear Model Dose-Effect
Proportion Average Annual Cases Annual Cases Cases per million Average Population (Million) Annual Cases
Geographic indoor radon average based on national surveys2000–2004 89 0.75 12.5
(5.0–21.3)1726 216
(86–368)63(33–104)
3.916 246(127–406)
2010–2014 77 3 11(4.4–19.4)
2332 257(100–452)
54(29–89)
4.584 249(133–408)
Population-weighted indoor radon average based on national surveys2000–2004 91 4⁎ 12.7
(5.0–22.2)1726 220
(86–383)64(36–103)
3.916 251(139–404)
2010–2014 98 4 13.6(5.3–23.4)
2332 316(124–546)
69(36–114)
4.584 317(166–523)
Population-weighted indoor radon average based on predictions by ED2010–2014 85 0.92 12
(4.6–21)2332 279
(107–490)60(36–115)
4.584 275(165–526)
⁎ The confidence interval was not provided in Fennell et al. (2002), so the same standard deviation (SD) as the 2010–2014 period was assumed.
J. Elío et al. Environment International 114 (2018) 69–76
74

years is likely a better approach to more accurately estimate the pos-sible adverse health effects of radon.
The annual lung cancer cases in Ireland linked to indoor radon ex-posure alone, are therefore estimated to be 270–280 (≈12% of theannual lung cancer cases). In the different estimates we have con-sidered, we see a temporal increase of radon-related lung cancer cases,despite a reduction of the national average indoor radon concentration(Table 1 and Table 2). This supports the hypothesis that the increase inabsolute numbers of lung cancer cases is due to an increase of the po-pulation, and further argues for including population data in suchstudies. It is also important to mention that although the geographicaverage has been reduced from an AM of 89 to 77 Bqm−3, the popu-lation-weighted average has increased from 91 to 98 Bqm−3, and to-gether with a population growth of almost 1 million, the expectednumber of lung cancer cases has apparently increased from around 250to 300 (Table 2). Although the ED-based predictions suggest this in-crease in radon-related lung cancer incidence may not be so severe(around 280), it indicates that radon prevention measurements could beimproved if demographic data are included. These results have to betaken with caution since other lung cancer causes (e.g. tobaccosmoking) were not taken into account in this study, however it showsthe importance of considering differential population growth as part ofthe evaluation for long-term effects of radon exposure to the generalpopulation, and in defining a rigorous national action plan.
5. Conclusion
In Ireland, the current annual numbers of lung cancer cases linkedto indoor radon exposure are estimated to be approximately 270–280(≈ 12% of the annual lung cancer incidence). Although the healthresults shown in this study are preliminary and more detailed epide-miological studies should be carried out to better understand the effectsof radon exposure in Ireland (especially to reduce the uncertaintiesassociated with the effective dose received by inhabitants, and toevaluate the synergistic effect of radon exposure and smoking), theyillustrate the importance of including the possible adverse health effectsof radon exposure in the definition of Radon Priority Areas.Additionally, we have demonstrated that carrying out such studies at anadministrative scale level (e.g. ED), rather than at a national level,improves national estimates of radon-related lung cancer incidence andallows defining and prioritising health protection in certain districts topromote radon awareness policies.
A strategy of estimating the probability of having an indoor radonconcentration higher than a reference level (e.g. Elío et al., 2017) is auseful approach in order to estimate the expected number of houses in acountry with an indoor radon concentration higher than this referencelevel. However, as there is no safe level of radon exposure, and lowradon concentration may also cause adverse health effects, only fo-cusing radon actions on reducing the indoor radon concentration whichare higher than a reference level (e.g. 200 Bqm−3 in Ireland) may notbe sufficient (e.g. Gray et al., 2009). Estimation of an average indoorradon concentration over large areas and the possible adverse healtheffects on the population as described in this study will thereforeovercome some of the limitations of the probability maps, and togetherwith them will help to define a spatially targeted national radon actionplan.
A national radon action plan based solely on radon concentration,or probability maps using geogenic information, will inherently have adifferent focus to one which takes population distribution into account.We do not view the different approaches as mutual exclusive, in that anational policy can be designed to use a combination of all methodol-ogies. Radiation protection has essentially two targets, protection ofindividuals and protection of the collective. The first implies reducingextremes, even if only one person is affected; this is where the prob-ability maps have an important contribution. The second implies a re-duction policy spatially focused where the majority of the collective
dose occurs. Such areas are where the highest radon-related lung cancerincidence is expected, even if indoor radon concentrations are relativelylow; this is where the methodologies as described in this study, areessential.
Acknowledgement
We wish to thank Dr. Kalantzi and the three anonymous reviewerswho greatly improved an early version of the manuscript. This work hasbeen financed by the Irish Research Council (IRC), through both theNew Foundations Scheme 2016 and the Enterprise Partnership SchemePostdoctoral Fellowship 2015 (EPSPD/2015/46), with the latter co-fi-nanced by the Geological Survey Ireland. The sole responsibility of thispublication lies with the authors. The IRC is not responsible for any usethat may be made of the information contained therein. The data usedin this project have been collated by the Environmental ProtectionAgency of Ireland, and the Geological Survey Ireland. We would like tothank Stephanie Long, and the Environmental Protection Agency ofIreland, for kindly providing the indoor radon data and their generalencouragement and help. We also thank Patrick Murphy (School ofMathematics and Statistics, University College Dublin, Ireland) forproviding the updated value of the national populated-weighted indoorradon concentration.
References
Bivand, R.S., Pebesma, E.J., Gómez-Rubio, V., 2008. Applied spatial data analysis with R.Springer New York, New York, NYhttps://doi.org/10.1007/978-0-387-78171-6.
Bochicchio, F., Venoso, G., Antignani, S., Carpentieri, C., 2017. Radon reference levelsand priority areas considering optimisation and avertable lung cancers. Radiat. Prot.Dosim. 177, 87–90. http://dx.doi.org/10.1093/rpd/ncx130.
Borgoni, R., Quatto, P., Somà, G., de Bartolo, D., 2010. A geostatistical approach to defineguidelines for radon prone area identification. JISS 19, 255–276. http://dx.doi.org/10.1007/s10260-009-0128-x.
Box, G.E.P., Cox, D.R., 1964. An analysis of transformations. J. R. Stat. Soc. Ser. BMethodol. 26, 211–252. http://dx.doi.org/10.2307/2287791.
Burke, O., Murphy, P., 2011. The use of volunteer radon measurements for radon map-ping purposes: an examination of sampling bias issues. J. Radiol. Prot. 31, 319–328.http://dx.doi.org/10.1088/0952-4746/31/3/001.
Burke, Ó., Long, S., Murphy, P., Organo, C., Fenton, D., Colgan, P.A., 2010. Estimation ofseasonal correction factors through Fourier decomposition analysis—a new model forindoor radon levels in Irish homes. J. Radiol. Prot. 30, 433–443. http://dx.doi.org/10.1088/0952-4746/30/3/002.
Casey, J.A., Ogburn, E.L., Rasmussen, S.G., Irving, J.K., Pollak, J., Locke, P.A., Schwartz,B.S., 2015. Predictors of indoor radon concentrations in Pennsylvania, 1989-2013.Environ. Health Perspect. 123, 1130–1137. http://dx.doi.org/10.1289/ehp.1409014.
Catelinois, O., Rogel, A., Laurier, D., Billon, S., Hemon, D., Verger, P., Tirmarche, M.,2006. Lung cancer attributable to indoor radon exposure in France: impact of the riskmodels and uncertainty analysis. Environ. Health Perspect. 114, 1361–1366. http://dx.doi.org/10.1289/ehp.9070.
Cheng, T.Y.D., Cramb, S.M., Baade, P.D., Youlden, D.R., Nwogu, C., Reid, M.E., 2016. Theinternational epidemiology of lung cancer: latest trends, disparities, and tumorcharacteristics. J. Thorac. Oncol. 11, 1653–1671. http://dx.doi.org/10.1016/j.jtho.2016.05.021.
Colgan, P., Organo, C., Hone, C., Fenton, D., 2008. Radiation Doses Received by the IrishPopulation.
Cothern, R., Smith, J., 1987. Environmental radon, Environmental science research. Vol.35 Plenum Press, New York.
CSO, 2006. Census 2006. Preliminary Report, Central Statistics Office.CSO, 2017. Census 2016 Summary Results – Part 1.Darby, S., Hill, D., Auvinen, A., Barros-Dios, J.M., Baysson, H., Bochicchio, F., Deo, H.,
Falk, R., Forastiere, F., Hakama, M., Heid, I., Kreienbrock, L., Kreuzer, M., Lagarde,F., Mäkeläinen, I., Muirhead, C., Oberaigner, W., Pershagen, G., Ruano-Ravina, A.,Ruosteenoja, E., Rosario, A.S., Tirmarche, M., Tomásek, L., Whitley, E., Wichmann,H.-E., Doll, R., 2005. Radon in homes and risk of lung cancer: collaborative analysisof individual data from 13 European case-control studies. BMJ 330, 223. http://dx.doi.org/10.1136/bmj.38308.477650.63.
Dowdall, A., Fenton, D., Flynn, S., Murphy, P., Murray, M., Pollard, D., Rafferty, B.,2017a. Updating Ireland's National Average Indoor Radon Concentration Using aNew Survey Protocol. Environmental Protectione Agency of Ireland.
Dowdall, A., Murphy, P., Pollard, D., Fenton, D., 2017b. Update of Ireland's nationalaverage indoor radon concentration – application of a new survey protocol. J.Environ. Radioact. 169, 1–8. http://dx.doi.org/10.1016/j.jenvrad.2016.11.034.
Drolet, J.-P., Martel, R., 2015. Distance to faults as a proxy for radon gas concentration indwellings. J. Environ. Radioact. 152, 8–15. http://dx.doi.org/10.1016/j.jenvrad.2015.10.023.
Elío, J., Ortega, M.F., Nisi, B., Mazadiego, L.F., Vaselli, O., Caballero, J., Chacon, E., 2016.A multi-statistical approach for estimating the total output of CO2 from diffuse soil
J. Elío et al. Environment International 114 (2018) 69–76
75

degassing by the accumulation chamber method. Int. J. Greenh. Gas Control. http://dx.doi.org/10.1016/j.ijggc.2016.02.012.
Elío, J., Crowley, Q., Scanlon, R., Hodgson, J., Long, S., 2017. Logistic regression modelfor detecting radon prone areas in Ireland. Sci. Total Environ. 599–600, 1317–1329.http://dx.doi.org/10.1016/j.scitotenv.2017.05.071.
EURATOM, 1996. 96/29/EURATOM. Council Directive of 13 May 1996 laying downbasic safety standards for the protection of the health of workers and the generalpublic against the dangers arising from ionizing radiation. Off. J. Eur. Union 159,1–114.
Fennell, S.G., Mackin, G.M., Madden, J.S., Mcgarry, A.T., Duffy, J.T., Colgan, P.A.,Pollard, D., 2002. Radon in Dwellings the Irish National Radon Survey.
Field, R.W., Smith, B.J., Steck, D.J., Lynch, C.F., 2002. Residential radon exposure andlung cancer: variation in risk estimates using alternative exposure scenarios. J. Expo.Anal. Environ. Epidemiol. 12, 197–203. http://dx.doi.org/10.1038/sj/jea/7500215.
Friedmann, H., Baumgartner, A., Gruber, V., Kaineder, H., Maringer, F.J., Ringer, W.,Seidel, C., 2017. The uncertainty in the radon hazard classification of areas as afunction of the number of measurements. J. Environ. Radioact. 173, 6–10. http://dx.doi.org/10.1016/j.jenvrad.2016.08.011.
Gray, A., Read, S., McGale, P., Darby, S., 2009. Lung cancer deaths from indoor radon andthe cost effectiveness and potential of policies to reduce them. BMJ 338, a3110.
Gunning, G.A., Pollard, D., Finch, E.C., 2014. An outdoor radon survey and minimizingthe uncertainties in low level measurements using CR-39 detectors. J. Radiol. Prot.34, 457–467. http://dx.doi.org/10.1088/0952-4746/34/2/457.
Ha, M., Hwang, S.-S., Kang, S., Park, N.-W., Chang, B.-U., Kim, Y., 2017. Geographicalcorrelations between indoor radon concentration and risks of lung cancer, non-Hodgkin's lymphoma, and leukemia during 1999–2008 in Korea. Int. J. Environ. Res.Public Health 14, 344. http://dx.doi.org/10.3390/ijerph14040344.
Hansell, A.L., Beale, L.A., Ghosh, R.E., Fortunato, L., Fecht, D., Jarup, L., Elliott, P., 2014.The Environment and Health Atlas for England and Wales. Oxford University Press,Oxford, UK.
Hassfjell, C.S., Grimsrud, T.K., Standring, W.J.F., Tretli, S., 2017. Lung cancer prevalenceassociated with radon exposure in Norwegian homes. Tidsskr. Den Nor. legeforening.http://dx.doi.org/10.4045/tidsskr.16.0127.
Hauri, D.D., Huss, A., Zimmermann, F., Kuehni, C.E., Röösli, M., 2012. A predictionmodel for assessing residential radon concentration in Switzerland. J. Environ.Radioact. 112, 83–89. http://dx.doi.org/10.1016/j.jenvrad.2012.03.014.
Hodgson, J., Carey, S., Scanlon, R., 2014. Developing a New National Radon Risk Map.Dublin, Ireland.
HSE, 2013. Pattern of Radon Levels - Ireland Data source: RPII. Ireland.ICRP, 1987. Lung Cancer Risk from Indoor Exposures to Radon Daughters. 50 ICRP
Publication.ICRP, 2007. The 2007 Recommendations of the International Commission on
Radiological Protection. ICRP Publication 103. Ann. ICRP 37. pp. 2–4.Jemal, A., Siegel, R., Xu, J., Ward, E., 2010. Cancer statistics, 2010. CA Cancer J. Clin. 60,
277–300. http://dx.doi.org/10.3322/caac.20073.López-Abente, G., Núñez, O., Fernández-Navarro, P., Barros-Dios, J.M., Martín-Méndez,
I., Bel-Lan, A., Locutura, J., Quindós, L., Sainz, C., Ruano-Ravina, A., 2018.Residential radon and cancer mortality in Galicia, Spain. Sci. Total Environ. 610–611,
1125–1132. http://dx.doi.org/10.1016/j.scitotenv.2017.08.144.NCR/NICR, 2011. All-Ireland Cancer Atlas 1995–2007. National Cancer Registry/
Northern Ireland Cancer Registry, Cork/Belfast.NCRI, 2005. Health Risks Due to Exposure to Radon in Homes in Ireland. The Implications
of Recently Published Data. Joint Statement by the Radiological Protection Instituteof Ireland and National Cancer Registry of Ireland.
NCRI, 2011. Lung Cancer Incidence, Mortality, Treatment and Survival in the Republic ofIreland: 1994–2008. Cork, Ireland.
NCRI, 2015. Cancer Trends - Lung Cancer. http://dx.doi.org/10.1038/299674b0.NRC, 1988. National Research Council. Health Risks of Radon and Other Internally
Deposited Alpha-Emitters: BEIR IV. National Academies Press, Washington, D.C.http://dx.doi.org/10.17226/1026.
NRCS, 2014. National Radon Control Strategy, Minister for the Environment (Ireland).Pebesma, E.J., 2004. Multivariable geostatistics in S: the gstat package. Comput. Geosci.
30, 683–691. http://dx.doi.org/10.1016/j.cageo.2004.03.012.Pérez-Ríos, M., Barros-Dios, J.M., Montes-Martínez, A., Ruano-Ravina, A., 2010.
Attributable mortality to radon exposure in Galicia, Spain. Is it necessary to act in theface of this health problem? BMC Public Health 10. http://dx.doi.org/10.1186/1471-2458-10-256.
Porstendörfer, J., 2001. Physical parameters and dose factors of the radon and thorondecay products. Radiat. Prot. Dosim. 94, 365–373. http://dx.doi.org/10.1093/oxfordjournals.rpd.a006512.
Quarto, M., Pugliese, M., La Verde, G., Loffredo, F., Roca, V., 2015. Radon exposureassessment and relative effective dose estimation to inhabitants of Puglia region,South Italy. Int. J. Environ. Res. Public Health 12, 14948–14957. http://dx.doi.org/10.3390/ijerph121114948.
R Core Team, 2016. R: A Language and Environment for Statistical Computing.Sugawara, E., Nikaido, H., 2014. World Cancer Report. International Agency for Research
on Cancer.Tomášek, L., Kunz, E., Müller, T., Hůlka, J., Heribanová, A., Matzner, J., Plaček, V.,
Burian, I., Holeček, J., 2001. Radon exposure and lung cancer risk — Czech cohortstudy on residential radon. Sci. Total Environ. 272, 43–51. http://dx.doi.org/10.1016/S0048-9697(01)00663-5.
UNSCEAR, 2000a. Exposures From Natural Radiation Sources. Rep. 2000 Annex B. pp.84–141.
UNSCEAR, 2000b. Annex E: Occupational radiation exposures, Sources and Effects ofIonizing Radiation.
US-EPA, 2001. Building Radon out. A Step-by-step Guide on How to Build Radon-resistantHomes.
US-EPA, 2003. EPA Assessment of Risks From Radon in Homes. Office of Radiation andIndoor Air, Washington, DC.
Vienneau, D., De Hoogh, K., Hauri, D., Vicedo-cabrera, A.M., Schindler, C., Huss, A.,2017. Effects of Radon and UV Exposure on Skin Cancer Mortality in Switzerland 1–8.http://dx.doi.org/10.1289/EHP825.
Walsh, P., 2017. A Revision of the Number of Radon Related Lung Cancers in Ireland.Irish National Radon Forum, Galway.
WHO, 2009. WHO Handbook on Indoor Radon: A Public Health Perspective. WorldHealth Organization, France.
J. Elío et al. Environment International 114 (2018) 69–76
76