Embed Size (px)
Citation preview
Ethical Di lemmas in Continuing a Zidovudine Trial After Early Termination of Similar Trials
Michael S. Simberkoff, MD, Pamela M. Hartigan, PhD, John D. Hamilton, MD, Daniel Deykin, MD, Mitchell Gall, MD, PhD, John G. Bartlett, MD, Paul Feorino, PhD, Robert Redfield, MD, Richard Roberts, MD, Dorothea Collins, MS, David DeMets, PhD, Willis Pritchett, RPh, Norton Spritz, MD, JD, Richard P. Wenzel, MD, MSc, and the VA Cooperative Study Group on AIDS Treatment, VA Medical Center, New York, New York
ABSTRACT: Ethical di lemmas caused by external events and an interim subset analysis raised concerns about continuing a long-term VA clinical trial comparing early with later z idovudine therapy for symptomatic human immunodeficiency virus (HIV) infection. The first external event was the early termination of other, apparent ly similar, trials conducted by the AIDS Clinical Trials Group (ACTG) and the announced clear benefits for the z idovudine- t reated patients. Interim analysis of the VA trial at this time did not show similar benefits. Subset analyses were performed to explore factors that might explain the different results. These suggested a difference in response to zi- dovudine in white and minority groups. The Data Monitoring Board and a special advisory panel reviewed these data and concluded that, since the VA results were neutral overall and the subset analyses based on small numbers , the trial should continue. By conference call, the s tudy cochairmen and biostatistician discussed this decision with s tudy personnel without revealing interim results, and s tudy personnel passed the information on to patients at the part icipating centers. The second event was in March 1990, when the Food and Drug Adminis t ra t ion (FDA) approved earlier use of zidovudine, which applied to patients still in the VA trial. Patients were asked to reaffirm their participation by signing a new informed consent that explained the findings repor ted by the ACTG, the FDA-approved revised recommendat ions , and the rationale for continuation of the VA trial. The consent form emphas ized that cont inued masked therapy was optional and that unmasked t reatment and follow-up would be provided to patients requesting it. Seventy-four percent of the part icipants
Address reprint requests to: Dr. Simberkoff, Infectious Diseases Section, NYVAMC, 423 East 23rd Street, New York, NY 10010.
Received December 11, 1991; revised August 12, 1992.
6 Controlled Clinical Trials 14:6-18 (1993) 0197-2456/93/$0.00 Published by Elsevier Science Publishing Co., Inc. 1993
655 Avenue of the Americas, New York, New York 10010

Ethical Dilemmas in a Zidovudine Trial 7
chose to continue masked therapy. We conclude that when new external data are announced, informed participation in a long-term clinical trial may require a revised consent form and that it is ethical and practical to present this without disclosure of interim study results.
KEY WORDS: Ethics, HIV infection, zidovudine, clinical trials, early stopping, informed consent
Dilemmas can arise in clinical trials when ethical principles or their appli- cation to participants are in conflict [1]. The data monitoring board (DMB) and other persons involved in monitoring a clinical trial often face these issues as information on treatment efficacy and toxicity accrues. Ethical dilemmas can also arise when external data become available during a trial or when unplanned analyses are performed. This article describes a Department of Veterans Affairs (VA) trial comparing early with later zidovudine treatment for patients with human immunodeficiency virus (HIV) infection, the ethical and scientific dilemmas, and their resolution.
THE VA CLINICAL TRIAL
The VA Cooperative Studies Program (CSP) initiated a multicenter, ran- domized, double-masked, clinical trial (CSP 298) to evaluate the efficacy and toxicity of zidovudine in AIDS-free, HIV-infected patients with initial CD4 + counts between 200 and 500 cells/mm 3. The trial was designed to compare early zidovudine therapy (initiated at the time of randomization) with later treatment (placebo followed by zidovudine when the peripheral blood CD4 + count fell to less than 200 cells/mm 3 or when AIDS developed, whichever came first). The study design used placebo-zidovudine rather than continuous placebo for the comparison group because zidovudine had been reported to be effective for symptomatic patients with CD4+ counts less than 200/mm 3 [2] and because the Food and Drug Administration (FDA) had approved its use in such patients. The VA trial enrolled 338 patients between January 1987 and January 1990, and masked follow-up of patients ended as planned in January 1991. The study design included plans for treatment modification in cases warranted by evidence of toxicity or by treatment differences observed during interim analyses. A detailed description of the patients, methods, and results of the study was published elsewhere [3].
The clinical outcomes of interest were development of AIDS or death and the immunological outcome of interest was a CD4+ count less than 200 cells/mm 3. Eligible patients who volunteered to participate in the study were randomly assigned to one of two treatment groups: zidovudine (1500 mg/day in divided doses) or placebo until an immunological or clinical outcome, as just defined, was reached. Patients who developed AIDS or whose CD4 + count fell below 200 cells/mm 3 were treated with unmasked zidovudine and continued in follow-up. The protocol specified that the trial would be ter- minated early if patient accrual was unsatisfactory or if a statistically significant difference was observed for the clinical events of AIDS or death, based on a modification of the O'Brien-Fleming boundary for interim monitoring [4].
Two external events occurred during the course of CSP 298 that threatened its continuation. These were the early termination of apparently similar trials
8 M.S. Simberkoff et al.
by the AIDS Clinical Trials Group (ACTG) and the FDA's approval of revised indications for the use of zidovudine. In addition, an interim subset analysis showed dissimilar trends in different racial and ethnic groups. These raised unanticipated ethical dilemmas and ultimately led to the development of a new informed consent for use in the study participants.
EVENTS AND ANALYSES AFFECTING V A TRIAL CONTINUATION
During the summer of 1989, the National Institute of Allergy and Infectious Diseases announced early termination of two ACTG trials that showed lower rates of disease progression with zidovudine treatment compared to placebo treatment in patient populations with CD4 + counts similar to those in CSP 298 [5, 6]. One was ACTG Protocol 016 in which 711 patients with symptomatic HIV infection and CD4 + counts between 200 and 800 cells/ram 3 were ran- domized to receive zidovudine (200 mg orally every 4 hours) or placebo [5]. Its outcome measures were death, an AIDS-defining diagnosis, or advanced AIDS-related complex (ARC) (CD4 + < 200 cells/ram 3 plus two symptoms of advanced HIV infection from among the following: thrush, oral hairy leu- koplakia, multidermatomal zoster, involuntary 10% weight loss, persistent diarrhea, fever). The trial reported that among the 351 and 360 patients ran- domized to placebo and zidovudine, there were 0 and 2 deaths, 21 and 5 patients who developed AIDS, and 15 and 8 patients who developed advanced ARC, respectively. Most of the clinical events occurred in patients with initial CD4 + concentrations < 500 cells/mm 3. The time to an ARC- or AIDs-defining event was significantly delayed in the zidovudine recipients.
The second trial to terminate prematurely was ACTG Protocol 019, which was a randomized trial of zidovudine vs. placebo in 1338 asymptomatic HIV- infected patients [6]. It had three treatment groups (placebo; low-dose zido- vudine 100 mg 5 times daily; high-dose zidovudine 300 mg 5 times daily) and three strata of patients defined by initial CD4 + count (< 200 cells/mm3; 200- 500 cells/mm3; 501-800 cells/mm3). Clinical outcomes of interest were identical to those listed for ACTG Protocol 016, but only the results for the two strata with lowest CD4 + cells were published. AIDS was diagnosed in 33, 11, and 14 patients randomized to placebo treatment, low-dose, and high-dose treat- ments, respectively. Most of the opportunistic infections, which accounted for the difference between the active treatment groups and placebo, occurred in patients whose CD4 + count had already fallen below 200 cells/mm 3. There were eight deaths in this trial: four in the placebo-treated group, one in the low-dose, and three in the high-dose zidovudine-treated groups. All deaths occurred in patients who had preceding AIDS events. The rate of progression was significantly reduced in both zidovudine-treated groups.
When the ACTG trials terminated, 297 patients had enrolled in the VA trial, and they had been followed on average for 12 months. Of these patients, 35 had experienced a clinical event. There were no differences between the treatment groups in the number of patients who had experienced clinical outcome events (Table 1) or in the time to these events (Fig. 1).
The patient accrual in CSP 298 had been satisfactory and interim analysis showed substantial numbers and rates of clinical outcomes, with no overall differences between the treatment groups and no unexpected or excess evi-

Ethical Dilemmas in a Zidovudine Trial 9
Tab le 1 Clinical O u t c o m e Events for CSP 298 as of N o v e m b e r 1989
Early Zidovudine Late Zidovudine Outcome (n = 149) (n = 148) P~
Death 9 b 9 0.85 AIDS 12 18 0.34 AIDS or death 17 18 0.97
ap = Log-rank test results. bNumber of patients.
dence of toxicity. Thus, there was no internal reason for p r e m a t u r e termi- nat ion of the trial. The p rob lems posed by the external events , however , r ema ined to be resolved.
The DMB, principal invest igators , and s tudy biostatistician of the VA trial me t wi th the principal invest igators and s tudy biostatist icians of the two ACTG trials to compare data and to identify differences and similarities a m o n g the trials. Both of the ACTG trials d e m o n s t r a t e d an increased risk for the combined event of AIDS or dea th a m o n g pat ients t reated wi th placebo com- pa red to pat ients t reated with z idovudine (Table 2), wi th relative risks of 2.45 and 4.75 in trials 019 and 016, respectively. The co r respond ing relative risk in the VA trial was only 1.06, showing no impor tan t differences be tween early and late use of z idovud ine on this combined outcome.
W h e n informat ion f rom these three trials was combined by weigh t ing the logar i thm of the relative risks inversely as their variances, a relative risk was ob ta ined that favored z idovud ine (95% confidence interval, 1.39-3.01). W h e n the VA data were combined with results f rom ACTG trial 016 only, the 95%
1.0
• .9 G) I m
14. I .8
rj)
.7
c 0 .6
, m
.5 a. o
~. .4
.3
" " . , , . , , . ; ~ Early
Later: ........ l i
P=0.34
1.0
c
• -> .8
¢/) .7
c .o .6 4.w I= .
0 a . . 5 0 I = -
r t .4
Early L~:. ,:
P=0.69
i I l I l ? l l I l
0 6 12 18 24 30 0 6 12 18 24 30
Time on Study {months) Time on Study {months)
Figure 1 Estimated Kaplan-Meier distribution of time to a diagnosis of AIDS (left) and time to death (right), according to trial group. Data are as of November 1989. Solid lines are patients randomized to early (immediate) zidovudine treatment and dashed lines are patients randomized to later (placebo-zi- dovudine) treatment.

10 M.S. Simberkoff et al.
Table 2 C o m p a r i s o n of the ACTG and VA Studies for the C o m b i n e d O u t c o m e of Death or AIDS as of Sep tember 10, 1989 for Patients with Entry CD4 + Counts of 500
Rates/100 No. of Patients Person-Years who Died or Relative Developed of Follow-up Risk
Study AIDS Placebo a ZDV (rr) b P~
ACTG Study 019 [6] 58 6.6 2.7 2.45 .0004 ACTG Study 016 [5] 23 8.2 1.7 4.75 .002 VA 298 [3] 33 12.4 12.0 1.06 .86
(019 + 016 + 298) 114 2.04 .0003 95% CI (1.39, 3.01)
(016 + 298) 56 1.63 .096 95% CI (.92, 2.90)
'~"Placebo" for the ACTG studies but "later ZDV" for the VA Study. bRelative risk is the rate ratio for 019 but the ratio of number of events (DI/D2) for 016 and 298. *Significance levels are computed by treating
[ln (rr)]2 ( ~ + ~22) ~ as a X 2 variate with 1 d.f. CI = Confidence interval; ZDV = zidovudine.
conf idence interval for relative risk was 0.92-2.90. This latter combinat ion was felt to have more justification because ACTG trial 016 and the VA trial enrol led symptoma t i c patients, whe reas ACTG trial 019 enrol led a sympto - matic pat ients . Calculat ions were also done to de te rmine w h e t h e r cont inuing CSP 298, and later combining data f rom the three trials, could lead to an al tered conclusion about the value of z idovudine . These calculations sug- ges ted that cont inuing CSP 298 would be unlikely to reverse the statistically significant result f rom the three trials combined , but could well lead to a statistically nonsignif icant result f rom the combina t ion of ACTG trial 016 and VA data if the latter r ema ined neutral (ie, a relative risk of 1.0).
Several considerat ions favored cont inuing the VA trial. First, the ACTG and VA trials m a d e different t r ea tment compar isons . The ACTG trials called for pat ients r andomized to z idovudine or placebo to remain on doub l e -masked therapy until they reached a clinical outcome (AIDS or advanced ARC), whereas the VA trial required pat ients to stay on doub le -masked t rea tment only until they reached a clinical or an immunologica l (CD4 + less than 200 cells/ram 3) event . Thus, the VA trial g roup was evaluat ing a compar i son of early vs. later z idovud ine t rea tment , which differed f rom the z idovudine vs. placebo com- par isons in the ACTG trials.
Second, the s tudy popula t ions were different. A quar ter of the pat ients in the VA trial had used in t ravenous drugs and one third were black or Hispanic. Only a tenth of the pat ients enrol led in ACTG trials 016 and 019 had used in t ravenous drugs and less than a fifth were black or Hispanic.
Third, the rates of bo th AIDS and dea th were higher in bo th the early and later t r ea tment a rms of the VA trial than they were in ei ther ACTG trial (Table 2). There had been 18 deaths a m o n g the 338 pat ients enrol led in the VA trial c o m p a r e d with 1 dea th in 515 pat ients in ACTG trial 016 and 8 dea ths in the
Ethical Dilemmas in a Zidovudine Trial ] 1
1338 patients in ACTG trail 019 in the < 500 CD4 + cells/ram 3 strata. Thus, continuation of the VA trial might provide valuable new information on sur- vival and other long-term effects of early vs. later use of zidovudine. The importance of these data was magnified by the observation that long-term zidovudine treatment was associated with in vitro resistance of HIV isolates, suggesting the possibility of a time-limited benefit [7]. Thus, the issue of the appropriate time to initiate zidovudine therapy became an important variable to assess, especially for long-term survival.
The feasibility of continuing the VA trial was also considered. At the time of the interim analysis, which was a year and a half prior to the study's scheduled end, the overall event rate was near that initially predicted. Pre- liminary inquiry, carried out by informal discussion between study personnel and patients at participating medical centers, suggested that fewer than a third of the patients might request termination of masked treatment following publication of the ACTG data and the anticipated broader guidelines for the use of zidovudine. On the basis of informal power calculations, we concluded that it would be worthwhile to continue follow-up and that the total number of combined clinical outcome events (AIDS or death) would not be substan- tially reduced by termination of masked treatment so late in the study.
At this time the DMB decided that the VA trial should continue. They also requested that special analyses be conducted to try to explain the discrepancy between the results of the VA trial and the two ACTG trials and to further investigate the deaths. Investigators were told by conference call of the DMB decision to continue the trial, and patients were notified by the local inves- tigators. The interim results were revealed to neither the investigators or the patients.
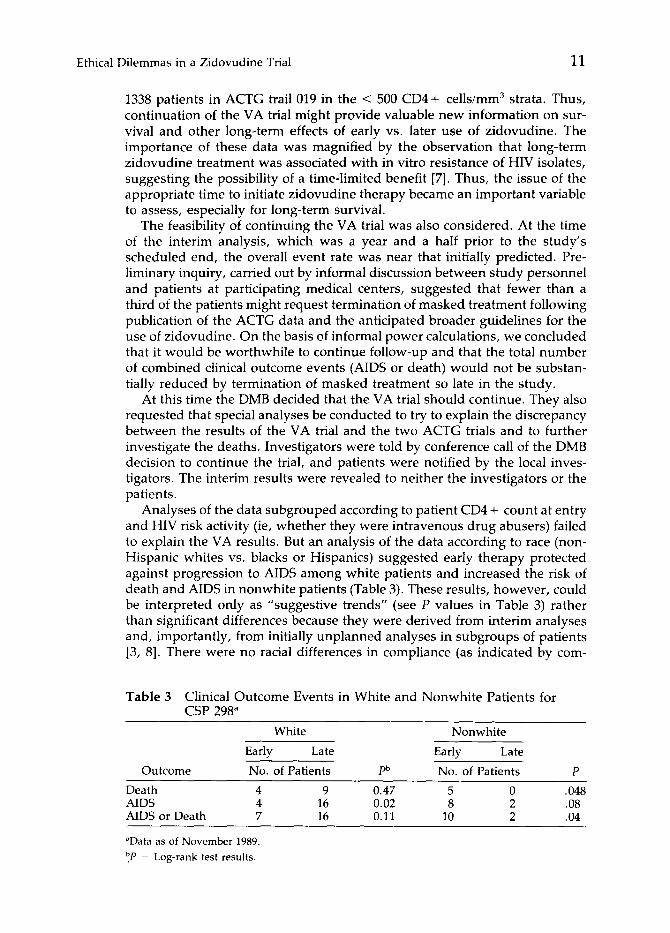
Analyses of the data subgrouped according to patient CD4 + count at entry and HIV risk activity (ie, whether they were intravenous drug abusers) failed to explain the VA results. But an analysis of the data according to race (non- Hispanic whites vs. blacks or Hispanics) suggested early therapy protected against progression to AIDS among white patients and increased the risk of death and AIDS in nonwhite patients (Table 3). These results, however, could be interpreted only as "suggestive trends" (see P values in Table 3) rather than significant differences because they were derived from interim analyses and, importantly, from initially unplanned analyses in subgroups of patients [3, 8]. There were no racial differences in compliance (as indicated by corn-
Table 3 Clinical Outcome Events in White and Nonwhite Patients for CSP 298 a
White Nonwhite
Early Late Early Late
Outcome No. of Patients pb No. of Patients P
Death 4 9 0.47 5 0 .048 AIDS 4 16 0.02 8 2 .08 AIDS or Death 7 16 0.11 10 2 .04
aData as of November 1989. b.p = Log-rank test results.

12 M.S. Simberkoff et al.
pliance with visits, pill count, or changes in mean corpuscular volume), re- actions to treatment, and pharmacokinetics, although the pharmacokinetic data were sparse and less than ideal.
Again, the DMB was faced with several scientific and ethical dilemmas. Should unplanned analyses be considered seriously? Should the trend in the white non-Hispanic early-zidovudine recipients, which agreed with the re- sults reported by an ACTG study [5], mandate termination of the trial in that subpopulation? What actions would be appropriate in response to the trends observed in the black and Hispanic subpopulation, and when should they be made?
To help resolve these dilemmas, an advisory panel of outside consultants was convened to review the interim analysis data from the VA and the ACTG reports and to advise the DMB. The advisory panel consisted of a physician- ethicist, a biostatistician, members of racial minorities, a VA Cooperative Studies Program Human Studies Committee member, and a distinguished scientist.
At that meeting, the DMB and advisory panel reviewed the VA and ACTG data, they agreed that the VA trial was providing valuable information on survival and on the long-term benefits of early vs. late zidovudine adminis- tration, and they discussed the possibility that delayed treatment might ac- tually offer a survival advantage. They concluded that the data on racial differences in treatment effects were not convincing for the following reasons:
1. These findings came from an unplanned analysis (data dredging), which was one of three subset categorizations considered, heightening the like- lihood of a chance result.
2. The findings were not confirmed in the ACTG studies; the ACTG data suggested that zidovudine, compared to placebo, delayed the onset of AIDS in blacks and Hispanics, as well as in non-Hispanic whites [9].
3. The number of events in the subsets was small. 4. There was no compelling biological reason to group Hispanics with blacks
instead of with non-Hispanic whites.
In view of the VA results on survival and on the combined outcome of AIDS or death, the DMB felt that it was ethical to continue to randomize and follow patients on masked therapy in the VA trial, as long as the patients were informed of their right to terminate masked treatment. With concurrence of the advisory panel, the DMB unanimously agreed to recommend continuation of the trial and to continue to treat all racial groups alike. This course of action was made easier by the realization that most patients assigned to "later" therapy would receive zidovudine before AIDS or death occurred.
In March 1990, the FDA approved broader indications for use of zidovu- dine. The new indications recommended a lower dose of 500 mg/day and use of the drug for all HIV-infected patients with CD4 + counts of 500 cells/mm 3 or less. These revised recommendations applied to all CSP 298 participants. By this time, the VA study had completed its accrual of patients and was to complete masked follow-up in less than a year. The DMB recommended that all patients be informed in writing of the revised FDA recommendations and that they be asked to sign a new informed consent document outlining their options to remain on blinded study medication at the originally planned

Ethical Dilemmas in a Zidovudine Trial 13
dosage (because the protocol specified mechanisms for dose reduct ion in cases of toxicity) or to receive open-label t rea tment at no expense. This was done (see Appendix) , and the subsequent status of pat ients is illustrated in Table 4. Seventy-four percent of those on bl inded t rea tment chose to cont inue while 26% switched to open-label therapy on review of the new informed consent .
DISCUSSION
Conduc t of clinical trials requires strict adherence to the principles of be- neficence, nonmaleficence, justice, and respect for pat ient au tonomy. These principles form the foundat ion of the phys ic ian-pa t ien t relat ionship and are the s tandard of conduct for research in h u m a n beings [10, 11]. They have been reaff irmed specifically for AIDS research [12, 13].
In relation to trials, the principle of a u t o n o m y requires that a pat ient or his or her guardian unde r s t and the nature of the trial, its potent ial risks and benefits, and the voluntary nature of participation. Beneficence requires that investigators strive to maintain a favorable balance be tween benefits and risks for the individual participants in the clinical trial and that medical science or pat ient care advance from the overall result. Nonmalef icence is the principle of doing no harm, a l though it mus t always be unde r s tood that unexpec ted results or side effects can arise dur ing a trial. Justice requires that pat ients be treated fairly, that bias be el iminated from the subject selection process, and that individuals be afforded equal access to the potential benefits and risks of a research protocol.
The VA trial illustrates several of the problems that may occur in the application of ethical principles to rapidly changing fields of clinical research. It is not u n c o m m o n for data external to the trial to become k n o w n dur ing the its p lanned course. When this occurs, the data mus t be cons idered to deter- mine whe the r the new information tests the same hypo theses in the same popula t ion as the trial in progress does and, if so, whe the r the repor ted data are sufficiently convincing to require terminat ion of the present trial u n d e r
Table 4 Status of Patients in CSP 298 on April 15, 1990
Assigned Treatment
Number of Patients: Early ZDV a Late ZDV Total
Randomized 170 168 338 Dead 12 12 24 Lost to follow-up 22 8 30 In follow-up 136 148 284
Not on blinded therapy or ZDV 19 21 40 On open-label ZDV on 3/30/90
By protocol 32 46 78 By choice 5 10 15
On blinded therapy on 3/30/90 80 71 151 Stayed on blinded therapy 66 46 112 Switched to open-label ZDV 14 25 39
after 3/30/90
aZDV, zidovudine.

14 M.S. Simberkoff et al.
the principles of beneficence or nonmaleficence. Independently developed protocols rarely test the same hypotheses with identical study designs and procedures, patient eligibility criteria, populations, and outcome measures. In this case, both the protocols and the populations were different. Even when protocols and populations are similar, valid reasons may exist for con- tinuing a clinical trial as long as patient autonomy is maintained. Clinicians are often reluctant to adopt new therapies without convincing evidence, and they are more likely to be influenced by cumulative data than by the results from a single trial. Often, physicians are skeptical about clinical trials and await confirmatory data before altering therapies.
Informed consent is the mechanism designed to help protect patient au- tonomy. The consent form normally describes the purpose and rationale for a trial, as well as the risks and benefits of participation in it. No informed consent document, however, can anticipate new data from external sources, and there is no generally accepted method for transmitting pertinent outside data to patients during the course of a clinical trial. Periodic letters, infor- mation sheets, and discussions between investigators and study participants can serve this purpose. Under some circumstances, a new consent may be desirable to confirm patient awareness and continued voluntary participation.
Another problem is how the differences in protocol, population, and ra- tionale for study continuation can be explained to masked participants and to investigators who are masked as well without divulging interim results. In fact, disclosure may jeopardize the progress of a clinical trial [14] because both investigators and patients may draw erroneous conclusions from pre- liminary results. The DMB of CSP 298 chose to require detailed briefings of investigators about the protocol differences and explanation of the decision to continue the trail without revealing its blinded results. Investigators, in turn, spoke to each of the study patients and distributed letters describing the status of the study. Ultimately, a new, signed statement of information and agreement to continue participation on blinded study drug treatment was required.
Other trials have informed participants about outside data and revised their informed consent while in progress. For example, investigators of the Macular Photocoagulation Study halted a randomized trial evaluating the effectiveness of laser therapy for senile macular degeneration (SMD) when it was shown to be of clear benefit in preserving vision, recommended treatment for all of the SMD patients originally randomized to no treatment, informed partici- pants in two other trials that were simultaneously in progress of the SMD findings, and revised and administered a new informed consent to the par- ticipants in these trials [15].
As a result of the analyses and deliberations by the DMB of CSP 298 described above, the principles of beneficence, nonmaleficence, and justice were considered seriously. As noted, minority patients constituted a large proportion of the participants in the VA study. There was concern that the risks and benefits of participation in the two treatment strategies (early vs. later zidovudine) were not equal in the different racial groups. Specifically, the trends of the interim analyses suggested that white non-Hispanic patients might benefit from early treatment with zidovudine, but that black or Hispanic

Ethical Dilemmas in a Zidovudine Trial 15
patients might not. Therefore, it was essential to consider how much evidence for a differential effect of treatment was provided by unplanned subset anal- yses [16].
Any data derived from unplanned subgroup analyses must be viewed with caution and skepticism, as illustrated in the paper by Lee et al. [17]. None- theless, such data may provide insights that are valuable in themselves and suggestive of future, more definitive studies. For the reasons discussed pre- viously, the DMB concluded that no convincing differences had been dem- onstrated in the effects of treatment between the racial groups. It chose to continue the study to obtain additional information on the major study end points of AIDS incidence and survival and to obtain additional information on possible racial differences on treatment efficacy. Further, the DMB con- sidered it important to obtain more definitive pharmacological data on zi- dovudine clearance in racial subgroups [18].
In retrospect, several undesirable consequences would have resulted from early termination of CSP 298. First, this study provided substantial evidence that survival is as good in those who receive zidovudine therapy late as it is in those who receive it early in the course of HIV infection [3]. Early termi- nation of the trial would have reduced its power to detect survival differences.
Second, continuation of the trial led to the demonstration of a twofold reduction in the rate of AIDS-defining events in patients assigned to early zidovudine treatment [3], in line with earlier published trials [5, 6]. This difference, although not defining the optimum time for initiation of therapy [19], supports the conclusion that the onset of AIDS will be delayed in patients treated with zidovudine before their CD4 + count falls below 200 cells/mm 3.
Third, publication or presentation of the data available in 1989 might have led some clinicians to withhold zidovudine in black or Hispanic patients. In retrospect, it seems that withholding zidovudine from such patients would be harmful, at least at later stages of disease, because the final data obtained in the VA trail were less suggestive of a differential treatment effect between racial and ethnic groups [3]. In addition, no racial differences in response to zidovudine were observed in the ACTG trials [5, 6, 9], and a recently reported nonrandomized, retrospective study from Maryland shows that minority pa- tients with AIDS who were given zidovudine had improved survival com- pared to patients who did not receive that drug [20].
The ethical dilemmas faced during this clinical trial are likely to occur elsewhere as the pace of clinical and laboratory investigation accelerates. Consideration needs to be given to how new information, whether derived from internal trial results or from external sources, will be evaluated and presented to study participants. Interpreting diverse sources of clinical trial information and adhering to valid clinical trial principles will continue to challenge our abilities. Ethics cannot be divorced from good science and, ultimately, our credibility depends on maintaining the highest standards in both pursuits.
This study was supported by the Cooperative Studies Program of the Medical Research Service, Department of Veterans Affairs, Central Office, Washington, D.C. and the US Army Medical Research and Development Command. Parts of this paper were presented at the Annual Meetings

16 M.S. Simberkoff et al.
of the AAP/ASCI/AFCR, Seattle, WA, May 3-6, 1991. The authors gratefully acknowledge the expert editorial assistance of Patricia Spivey, B.A., in the preparation of this manuscript.
REFERENCES
1. Childress JF: The normative principles of medical ethics. In: Medical Ethics. Veatch RM, ed. Boston, Jones and Barlett, 1989, 27-48
2. Fischl MA, Richman DD, Grieco MH, et al: The efficacy of azidothymidine (AZT) in the treatment of patients with AIDS and AIDS-related complex: A double-blind, placebo-controlled trial. N Engl J Med 317:185-191, 1987
3. Hamilton JD, Hartigan PM, Simberkoff MS, et al: A controlled trial of early versus later zidovudine in symptomatic human immunodeficiency virus infection: Results of a Veterans Affairs cooperative study. N Engl J Med 326:437-443, 1992
4. O'Brien PC, Fleming TR: A multiple testing procedure for clinical trials. Biometrics 35:549-556, 1979
5. Fischl MA, Richman DD, Hansen N, et al: The safety and efficacy of zidovudine (AZT) in the treatment of mildly symptomatic human immunodeficiency virus type 1 (HIV) infection: A double-blind, placebo-controlled trial. Ann Intern Med 112:727-737, 1990
6. Volberding PA, Lagakos SW, Koch MA, et al: Zidovudine in asymptomatic human immunodeficiency virus infection: A controlled trial in persons with fewer than 500 CD4-positive cells per cubic millimeter. N Engl J Med 322:941-949, 1990
7. Larder BA, Darby G, Richman DD: HIV with reduced sensitivity to zidovudine (AZT) isolated during prolonged therapy. Science 243:1731-1734, 1989
8. Geller NL, Pocock SJ: Interim analyses in randomized clinical trials: Ramifications and guidelines for practitioners. Biometrics 43:213-223, 1987
9. Lagakos S, Fischl MA, Stein DS, Lim L, Volberding P: Effects of zidovudine therapy in minority and other subpopulations with early HIV infection. JAMA 266:2709- 2712, 1991
10. The National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research: The Belmont Report: Ethical Principles and Guidelines for the Protection of Human Subjects of Research. DHEW Publication No. (OS) 78-0012. Ap- pendix I, DHEW Publication No. (os) 78-0013, Appendix II, DHEW Publication (OS) 78-0014. Washington, DC, 1978
11. Levine RJ: Ethics and the Regulation of Clinical Research, 2nd ed. Baltimore, Urban and Schwarzenberg, 1986 1-18
12. Walter L: Ethical issues in the prevention and treatment of HIV infection and AIDS. Science 239:597-603, 1988
13. Levine C: Has AIDS changed the ethics of human subjects research? Law Med Hlth Care 16:167-173, 1988
14. Pocock SJ: Clinical Trials: A Practical Approach. New York, John Wiley and Sons, 1983
15. Macular Photocoagulation Study Group: Changing the protocol: A case report from the macular photocoagulation study. Controlled Clin Trials 5:203-216, 1984
16. Meinert CL, Tonascia S: Clinical Trials: Design, Conduct and Analysis. New York, Oxford University Press, 1986, 208-216
17. Lee KL, McNeer JF, Starmer F, Harris PJ, Rosati PJ: Clinical judgement and sta- tistics: Lessons from a simulated randomized trial in coronary artery diseases. Circulation 61:508-515, 1980

Ethical Dilemmas in a Zidovudine Trial 17
18. Gitterman SR, Drusano GL, Egorin MJ, et al: Population pharmacokinetics of zidovudine. Clin Pharmacol Ther 48:161-167, 1990
19. Friedland GH: Early treatment for HIV infection: The time has come. N Engl J Med 322:1000-1002, 1990
20. Moore RD, Hidalgo J, Sugland BW, Chaisson RE: Zidovudine and the natural history of the acquired immunodeficiency syndrome. N Engl J Med 324:1412-1416, 1991
Appendix: Information and Consent Form for Participants, CSP 298
Since you are participating in a trial of the anti-AIDS-virus drug zidovudine (AZT), we wish to bring you up to date on some information that may have a bearing on whether you choose to continue in this program.
The VA study of which you are a part is officially known as CSP 298 "Treatment of AIDS and ARC: Part I. Treatment of Patients with AIDS-Related Complex (AZT Versus Placebo)." The study is currently in progress at six VA hospitals (New York, NY; Washington, DC; Miami, FL; Houston, TX; West Los Angeles, CA; San Francisco, CA) and at the Walter Reed Army Hospital.
The patients in the study, like you, are all people who are infected with the AIDS virus but do not have the disease AIDS. As you know, some of you are receiving AZT, and others are receiving capsules that look like AZT but do not contain an active medicine (placebo). All of the study patients were assigned to receive AZT or placebo by chance. However, all patients who received placebo initially are offered AZT as soon as their CD4 lympho- cyte levels drop below 200 or as soon as AIDS develops. Therefore, this trial really compares early AZT use against later AZT use. By seeing how well each group does, we hope to learn whether persons like you will benefit from receiving AZT initially at this early stage of infection with the AIDS virus.
As you may have learned from news reports, the National Institutes of Health (NIH) conducted two similar trials of AZT in persons who, like you, are infected with the AIDS virus but do not have the disease itself. The NIH decided to terminate these trials because their results showed that AZT de- layed the development of AIDS disease and delayed the symptoms closely related to AIDS. However, these studies were stopped before it could be determined whether early use of AZT increased survival.
The Antiviral Advisory Committee to the Food and Drug Administration (FDA) recently has reviewed the data from the NIH trials. They have rec- ommended that AZT should be made available for patients with AIDS virus infection and CD4 lymphocyte counts below 500. However, they acknowl- edged that there is a lack of information about the long-term benefits of early AZT treatment compared to later treatment with AZT, and they and other scientists are also concerned about the possibility that prolonged AZT treat- ment could increase the chance that the AIDS virus would become resistant to this drug. They specifically recommended continuation of the VA study.
We, of course, have looked at the possibility that, on the basis of these findings, it would be proper for the VA to discontinue the study in which you are participating. Our Data Monitoring Board, a group of experts who watch the results of our study in order to assure the safety of its participants, were asked to consider this question. They met together with other experts

18 M.S. Simberkoff et al.
in this area and reviewed the NIH trials as well as the data from the VA study.
It was the judgement of that group that we should go on with our study even though the NIH had decided to discontinue its trial. To date, in the VA study, there have been no significant differences in the rates of occurrence of AIDS events, and survival is virtually identical between those who took AZT initially and those who took placebo initially (but may have switched to AZT later).
The Data Monitoring Board and other experts who reviewed this study believed that it is important to learn whether early use of AZT provides long- term benefits and improves survival compared to giving AZT only after the CD4 lymphocyte level falls to less than 200 or after AIDS develops.
They felt that continuation of our trial continues to be important because it may answer questions that were unanswered by the NIH trial concerning the long-term benefits of early versus late treatment with AZT. As we ex- plained when you first entered this study, although this information may be important in determining the best way to use AZT in patients infected with the virus, continuation in the trial may not produce individual benefit to you.
If you choose to continue, it is important that you know that the results of the trial will continue to be monitored closely. If at any time our expert review panel feels that the important questions are answered or that contin- uation of the study has been shown to be dangerous for the participants, it will be discontinued. Furthermore, we are watching the blood counts of each participant and if the immune cells that are affected by the AIDS virus (CD4 lymphocytes) fall to a dangerous level (less than 200) you will be informed. You can then start to take AZT under the care of your study physician and nurses.
We are very grateful for your participation to date and hope that you will continue to work with us. However, you must understand that your contin- ued participation in this trial is entirely voluntary. Be assured that you will receive the best possible care and followup at this facility regardless of your decision.
We are providing two copies of this information and consent form to you. If you wish to continue, please sign one of these and return it to the inves- tigator or study nurse at your participating center. You should retain the other copy for your records.
I acknowledge that I have received a copy of this information and consent form and that I have read and understood its contents, and that my questions about it and any related matters have been fully answered.
(Patient's Signature) (Date)
(Witness' Signature) (Date)





























