Embed Size (px)
Citation preview

Ethnicity & Health: An Integrative Biopsychosocial Model of Risk & Resilience.
Hector F. Myers, Ph.D.Professor of Psychology
University of California, Los Angeles

Outline
Race/Ethnicity, SES & Health Disparities Social Status-Related Stresses & Health Lifespan Model of Psychosocial
Adversities, Psychosocial Reserve Capacity & Cumulative Vulnerability & Health Disparities
Some Potential Contributors to Resilience
Implications & Future Directions

Ethnic Health Disparities Significant disparities in chronic diseases and death. Leading causes of death:
CVD & cancer leading cause of death in all groups. HIV/AIDS: in top 3 causes of death for AA men and
women and for HA men. Diabetes is among top 5 causes of death for
women of color, especially AA, HA & NA. Whites & APIs suffer disproportionate risk for
COPD. NAs suffer more from chronic liver disease. NA, AA and HA men at disproportionate risk for
violent death.

CHD & stroke mortality dropped in the US in past 20 yrs.
Sig. ethnic disparities in prevalence of CHD, stroke and related risk factors. Whites have highest rate of CHD, but AA
have higher mortality. Whites & AA have comparable rates of
stroke, but AA have higher stroke-related mortality.
AA have highest rate of hypertension (35% of pop compared to 22% of W and 23% of HAs).

Group differences in CHD related to differences in risk factors.
Low SES: highest rate and greatest clustering of risk factors.
Smoking:Men Women
Whites: 25.2% 20.7% AA: 27.0% 18.5% HA: 23.2% 12.5% Asians: 21.3% 6.9% NA: 32.0% 36.9% (Health, US. 2003-2004, CDC/NCHS)

Hypertension (140mmhg/90mhg or on anti-hbp meds) Men Women
Whites: 30.6% 31.0% AA: 41.8% 45.4% MA: 27.8% 28.7% Asians (overall): 16.7% NA (overall): 21.2% Note: up to age 55 M>W, but postmenopause: W>M.

Overweight (BMI = 25.0kg/m2+) Obesity (BMI = 30.0kg/m2+):
Men Women Whites: 69.4% 57.2%
28.2% 30.7%AA: 62.9% 77.2% 27.9% 49.0%
MA: 73.1% 71.7% 27.3% 38.4%
Asians (overall): 34.5% overweight, 7% obese.

Metabolic syndrome Men Women
Whites: 24.3% 22.9% AA: 13.9% 20.9% MA: 20.8% 27.2%
High Cholesterol (240mg/dl = high risk) Whites: 17.8% 19.9% AA: 10.6% 17.7% MA: 17.8% 13.9%

Physical inactivity: Men Women
Whites: 34.4% 38.3% AA: 45.1% 55.1% HA: 52.6% 57.2% Asians: 33.4% 42.6% NA: 42.5% 55.5%

Cancer Significant group differences
overall, in risk for specific types, and in cancer mortality.
Overall rate = 447.1 Whites = 471.2 AA = 456.0 NA = 298.5 Asians = 314.7 HA = 323.5

AA men highest rates of prostate, lung & oral cancers.
White women highest rate of breast cancer, but AA women have highest mortality.
Vietnamese women 2.5x rate of cervical cancer, Hispanic women 2nd highest rate.
AA and Hispanic women have highest rate of cervical cancer mortality.
NA and AA women highest rate of lung & colorectal cancers.
NA men have highest rate of colorectal cancers Asians have lowest cancer rates overall, but Korean
and Vietnamese men have highest rates of stomach & liver cancers.

Diabetes Minorities, women & Native Americans
disproportionately affected. Overall rate: 10.3%
Men Women Whites: 8.4% 7.8% AA: 8.5% 12.1% HA: 17.8% 19% Asians: 20% 16% NA: 49.4% 51.1%

Minorities suffer disproportionately from the diabetic complications
AA = 6.6x > W from end-stage renal disease. MA = 7.x > W and NA from end-stage renal disease. Non-Whites 2x > W to suffer from blindness. AA > W and H to suffer blindness. Except for Asians, minorities higher mortality rates
from diabetes than Whites. Group differences suggest possible differences in
genetic vulnerability. Differences in functional outcomes suggest
differences in lifestyle, early screening, treatment seeking, disease tolerance and quality of care.

HIV/AIDS Percent New cases, 2004
Whites: 28.3% AA: 49.3% HA: 20.4% NA: 0.5% Asians: 1.1%

Adverse Birth OutcomesPercent of live births, 2005 Preterm (< 37 weeks of gestation)
All groups: 12.7% Whites: 11.7% AA: 18.4% Hispanics: 12.1% NA: 14.1% Asians: 10.8%

Low birthweight (< 2,500 grams) All groups: 8.2% Whites: 7.3% AA: 13.7% HA: 6.9% NA: 7.4% Asians: 8.0%Note: Similar pattern for very preterm (<32 Wks)
& very low birthweight (<1,500 grams).

Ethnic Disparities in Health Care Differences in access to & quality of health
care important contributors to health disparities. Patient-level variables Health-care system variables Care process variables Ethnic differences reduced among higher
SES, those with insurance, medical care in the military & VA systems.

How do we explain these differences?
We argue, contrary to current direct effects studies, that the accumulating evidence supports a more complex, multi-dimensional model of risk and resilience.

Social Status Stresses
The first factor in such a model is exposure to social status stresses & adversities
Social status stresses are stresses that are experienced because of attributes that define our status in the social hierarchy, such as race/ethnicity, social class, gender, sexual orientation, and age.

Social Status-Related Sources of Risk
Socio-Economic Status & History Current Status SES History & Trajectory
Race/Ethnicity Ethnic Identity and Ethnic Self-Esteem Cultural affiliation and Level of Acculturation
Race/Ethnicity and SES interact such that SES conditions race/ethnicity in predicting health & functional outcomes (Williams & Jackson, 2005).

Race/Ethnicity
SES
Health Outcomes

However, we argue that the race/ethnicity-SES interaction effects are likely mediated through exposure to psychosocial adversities. Chronic Daily Stresses Stressful Life Events Socio-Ecologic Stresses Racism & Discrimination

Race/Ethnicity
SES
Psychosocial Adversities
Health Outcomes

Racism, Discrimination & Health
Racism/discrimination is not “just another stressor”.
Despite important social changes, racial discrimination continues to be pervasive, expressed at multiple levels, and includes a range of attitudes and acts (Harrell, 2000).
While most studies have been conducted on African Americans, exposure to discrimination has been linked to functional outcomes in all ethnic groups.
However, the effect is greater and more pervasive in persons of color, especially in African Americans (Greene et al., 2006; Mays et al., 2007).

These experiences are linked to a variety of medical (e.g Hypertension, CVD), mental health (e.g. depression, anxiety, hostility) & behavioral disorders (e.g. violence, substance abuse) (Paradies et al., 2003; Brondolo et al., 2003; Landrine et al., 2006).
Exposure to discrimination are frequent for many groups, especially the poor and persons of color, and vary in the causal attributions made (e.g. race, color, nationality, immigration status, size, gender, etc.).
Exposure produces direct negative effects that are moderated by appraisal & coping.
These experiences are usually not forgotten and condition future appraisals, expectations and coping with future experiences (Brondolo et al., 2005).

Exposure to race-related and other stresses linked to disease in part by activating pre-existing or creating new biological vulnerabilities.
Biological heterogeneity of racial groups, yet there is clustering of genetically-mediated disorders within groups (e.g. hypertension, diabetes).
Evidence is also growing of environmental contributions to the acquisition of biological vulnerabilities (e.g. multi-generational exposure to pathogens & toxins).

Race Psychosocial Adversities
SES Biological Vulnerabilities
Health Outcomes

Strong evidence suggests, however, that these biological vulnerabilities are often manifested in patterns of physiological hyperreactivity or dysregulation of stress response mechanisms (e.g. BP, HRV, cortisol, immune changes, etc.).

Biological Stress Processes Allostatic Load
Stress Hormones Blood Pressure, Heart Rate & Heart Rate
Variability Metabolic Factors
Neurophysiologic Processes Immune Processes Disease-Specific Biomarkers

Race Psychosocial Adversities Health
Outcomes
Biological Biological SES Vulnerabilities Stress
Processes

Other evidence also identify processing of thoughts & emotions as implicated in health outcomes
Negative thoughts & emotions as risk enhancers Depression Fear & Anxiety Anger/Hostility Hopelessness
Positive thoughts & emotions as resilience enhancers Faith & Hope Optimism Tranquility

Race Processing thoughts & emotions
Psychosocial Adversities
SES Biological Biological
Vulnerabilities Stress Processes
Health Outcomes

Strong evidence notes that social adversities also exert their effects in part through the clustering of health risk behaviors.
These behaviors are disproportionately evident among the poor and persons of color.
Clustering of these behaviors have synergist rather than simply additive effects.
Health risk behaviors Physical Inactivity Poor dietary habits & excess weight Smoking Alcohol and recreational drugs Risky sexual behavior Poor health & illness management

Processing Race Thoughts & Emotions
Health Psychosocial Behaviors Health Adversities Outcomes
SES Biological Biological Vulnerabilities Stress
Processes

Recent evidence provide initial support for the role of histories of social resources (Singer & Riff, 1999) and psychosocial reserve capacity (Gallo & Mathews, 2003) in moderating or mediating the effects of race/ethnicity, SES and social adversities in predicting health outcomes.

Psychosocial Reserve Capacity Cultural Resources
Spirituality/Religiosity Cultural Wisdom
Interpersonal Resources Social Support Network of Social Relationships
Intrapersonal Resources Perceived Control Self-Esteem & Self-Efficacy Resilience(Gallo & Mathews, 2003; Gallo et al., 2005)

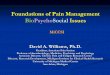
ProcessingRace Thoughts Health
& Emotions Behaviors
Health
Psychosocial Outcomes
Adversities Reserve
SES Biological Capacity Vulnerabilities
Biological Stress Processes

Finally, we argue that health disparities are the byproducts of the interactions of all of these risk factors moderated or mediated by reserve capacity to lead to Cumulative Vulnerabilities over time, and it is these relationships that in turn predict adverse health outcomes.


Implications & Future Directions
This is a reciprocal & recursive, lifespan meta-model that cannot be tested in a single study.
Serves as a framework to inform new hypothesis-driven studies of smaller models.
Model emphasizes the interplay of social context factors that exert their effects through cognitive-emotional, psychosocial risks & resources and biological pathways over the life course to predict current health status & functioning.

This framework asserts the value of both within and between group studies and recognizes the possibility that group-specific models may be worth investigating.
Specific models will also need to test to predict resilience in the face of race- and SES-related psychosocial adversities.
Finally, testing models such as this will likely require larger and more representative samples, new measures, longitudinal designs, multidisciplinary teams and advanced statistical procedures.