Embed Size (px)
DESCRIPTION
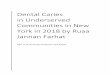
Etiology of Dental Caries. The four circles diagrammatically represent the factors involved in the carious process.all four factors must act concurrently (overlapping of the circles)for caries to occur. Micro- organisms. no caries. no caries. host & tooth. Sub- strate. caries. no - PowerPoint PPT Presentation
Citation preview

Etiology of Dental Etiology of Dental CariesCaries

The four circles diagrammatically
represent the factors involved
in the carious process.all four factors must act
concurrently (overlapping of the circles)for caries to occur
Micro-organisms
host & tooth
Sub-stratecaries
time
no caries
no caries
no caries
no caries

Host factor: saliva
What is saliva here mean?
a. major saliva glands
Saliva parotid, submandibular, sublingual
b. minor gland
c. gingival exudate

Why Saliva?
Animal experiments
Clinical observations

Animal experiment
Group No. hamsters Avg. no. Avg. caries carious teeth score
Intact salivary glands 20 2.3 4.0
Desalivated* 10 10.5 39.0
* Parotid, submandibular, and sublingual glands.
Effect of desalivation on caries in hamsters

Clinical observations
Xerostomia:
decreased or lack of salivary secretion
Cause: therapeutic radiation
salivary glands disorder (e.g. sjogren syndrome)
taking medicine

Clinical observation

Caries in a patient with impaired salivary function as result of radiation therapy (courtesy of Drs Jansma a
nd Vissink, RUG, the Netherlands.

The caries is different from common.
Decay offer seen in cervical area, a rapid
demineralization over broad surfaces with
no cavity. the huge change in quantity of
saliva is responsible.

In xerostomia
The amount of bacteria
The quality of plaque change
S.mutans, Lactobacillus, Yeast, Actinomyce
S. sanguis, Veillonella, Neisseria

A case report

Decayed, missing, and fill
ed teeth prior to the antich
olinergic therapy obtained
from the patient’s dental r
ecords and roentgenograp
hs

Full-mouth roentgenographs of patient showing rampant caries and pulpal involvement of mandibular anterior teeth

Decayed, missing, and filled teeth of a patient who received prolonged anticholinergic therapy for a duodenal ulcer. Note the steep caries increment (DMFT 27) that occurred during the time of xerostomia

Salivary composition and cariesRelationship between salivary characteristics and caries prevalence
Property Relationship Property Relationship
Flow rate ± pH -Buffer capacity + Ca -
PO4 -
NH3 -
AmylaseViscosity -Urea -
+ positive relation; ± some relation; - no relation.

Why flow rate?

Flushing and neutralizing effect refered a
s “Salivary Clearance” or “Oral Clearanc
e Capacity”

The Dawes (1983) model of oral clearance. Saliva is produced at a rate dependent on the concentration of sugar in the saliva. When a maximum volume of saliva (Vmax) is reached, a swallow occurs and the salivary volume decreases to a residual volu
me (Resid), thereby eliminating some of the sugar

Flow rate of saliva
Unstimulated 0.3ml/min
0.7~1.5L/day
Severe xerostomia 0.05ml/min

A computer simulation of the effect of changes in the unstimulated flow rate on the clearance of sucrose after a 10% sucrose mouthrinse. The simulation assumed average values for Resid (0.8ml), and Vmax (1.1 ml)

Sucrose concentrations in saliva at different sites and times after a 10% sucrose mouthrinse
WS=whole saliva; FUM=facial upper molarsFUI=facial palatal upper incisorsLLM=lingual lower molarsFLM=facial lower molars

high flow ratehigh buffer capacityflow rate bicarbonate concentration Na+
Electrolyte concentration as a function of salivary flow rate. See also chapter 3

Salivary composition and caries :
contradictory results, because of the
difficulties in study

Relationship between salivary characteristics and caries prevalence
Property Relationship Property Relationship
Flow rate ± pH -Buffer capacity + Ca -
PO4 -
NH3 -
AmylaseViscosity -Urea -
+ positive relation; ± some relation; - no relation.

Salivary buffers
In saliva, two chief buffer system,
bicarbonate-carbonic acid
(HCO3-/H2CO3, PK1=6.1) AND
phosphate (HPO4=/H2PO4
-, PK2=6.8)

Bicarbonate is most important
buffer system

Dialysis of saliva, remove all ion, keep
protein , no buffer capacity remained.

Diagram of a Stephan curve – the plaque pH response to a 10% glucose solution (Redrawn from Jenkins, The physiology and biochemistry of the mouth. Blackwell, London, 1978).

The effect of restricting the access of saliva to plaque upon the shape of the Stephan curve (Reproduced from) Jenkins, the physiology and biocbemistry of the
mouth. Black well, London, 1978)

Mean Stephan curved following rinsing with sucrose alone and following parafilm chewing or cheese chewing. Reproduced from Higham and Edgar; Caries Res 1989;23:42-48

Concept of “Critical pH”
In normal concentration of calcium
and phosphate, the critical pH is
5.5.

Antibacterial factor of
glandular origin

Lysozyme (溶菌酶)Hydrolytic enzyme, cleaves the 1-4 linkage between N-acetylglucosamine and (N- 乙酰葡糖胺) , N-acetylmuramic acid (N- 乙酰胞壁酸) a structure of cell wall of bacteria.

lysozyme, exist in many tissue fluid such as tear, egg, saliva etc.
Many bacteria is resistant to lysozyme by capsule and extracellular polymers.
Animal test show lysozyme alone could not prevent caries.
Lysozyme function by affecting the ecological balance between microorganism.

Salivary peroxidase
Thiocyanate ion (SCN-) from salivary glands硫氰酸盐
Hydrogen peroxide from bacteria
Salivary peroxidase system ( 唾液过氧化物酶系统)

H2O+SCN- OSCN-+H2O
OSCN- 硫氰酸盐中间产物,包括二氰代硫、氰亚磺酸、氰磺酸等
Peroxidase

OSCN- inactivate various enzyme
of the glycolytic pathway and
therefore inhibit growth, respiration
and metabolism of many bacteria.

Lactoferrin (乳铁蛋白)
Ferric iron (Fe3+) is an essential microbial nutrient
Lactoferrin binds ferric iron, make it unavailable for microbial use.
Unbound lactoferrin may also have bactericidal effect on some microorganisms such as S.mutans

Microorganism’s policy against LF
Some bacteria produce a protein (enterocheli
ns) binding Fe++ more effectively
Some bacteria degraded LF and use the releas
ed Fe++

Amylase (淀粉酶)
A calcium metalloenzyme hydrolyses t
he alpha 1-4 bond of starch

Amylase may help clean the teeth of carbohyd
rate debris. But why appear in tears, serum, br
ohchial ( 支气管) , male and female urogeni
tal secretions?
Recent discovery: amylase may specifically bi
nds to some oral micro-organism.

Histatins (富组蛋白)
A group of small histidin-rich protein.
Inhibitor of candida albicans ( 白色念珠菌)and S.mutans.
Unstimulate saliva: 2~30nmol/ml

Statherins (富酪蛋白)

a 43 residue protein, produced by acinar cell
Inhibit primary precipitation of calcium phosphate, entire molecule is needed.
Inhibit secondary precipitation (crystal
growth). Only first six residues are
needed.
StatherinsStatherins

In a given pH, only supersaturated saliva would prevent demineralization ( 脱矿 ) and promote remineralization ( 再矿化 ).
However, supersaturated with calcium phosphate will promote crystallization of calcium phosphate salts onto tooth surface.
Why inhibiting precipitation?Why inhibiting precipitation?

Proline-rich proteins (PRPs, 富脯蛋白 )
3 PRPs was identified, with around 150 amino acid residues.
Inhibition of crystal growth calculus formation, remineralization and calcium phosphate precipitation
the first by 30 residues at the amino-terminal part Important constituent of acquired pellicle Interaction with oral bacteria, modulation of ad
hesion of selected bacteria to tooth surface

The PRPs molecule is thought to bind to tooth surface via its amino-terminal segment.
tooth
Binding of this segment is sufficient to fulfill the primary role (inhibition of crystal growth), and leaves the carboxy-terminal region of the molecule, which has a different composition, directed to the oral cavity, and free to interact with oral bacteria.
N C

Caries Immunology
Immunological prevention of infection disease achieved vast success in this century.
smallpox, poliomyelitis etc.
How about dental caries?

inhibit colonization, surface protein (表面蛋白) , glucosyltransferase (葡糖基转移酶 GTF )
Opsonize (调理) bacteria, permitting phagocytosis
Theoretically, antibody may control cariogenic bacteria by

Humoral and cellular factors at the plaque/ tooth interface. Saliva provides secretory IgA, which can reach plaque both at the gingiva and at occlusal fissures.
Gingival exudate provides both humoral (IgG, IgM, and IgA) antibodies and cellular components (neutrophils, lymphocytes), but only to plaque in the gingival region.

Polypeptide chain structur
e of human IgA
Electron micrograph of a human dimeric IgA myeloma protein

Structure of human secretory IgA1 (sIgA1)

Animal studies
rodent or primates Diet containing sucrose (diet 2000) Infected test cariogenic bacteria Control group Caries development is determined by
Keyes method
Animial caries model


取唾液
取静脉血
本课题获国家自然科学基金重点项目资助

Whole cell Whole protein or peptide Part of peptide, one more dormain Cheramic peptide -- AgI/II~GTF DNA vaccin
Candidate antigen

SIgA, locally or via gut
serum antibody, via systematic
Passive immunization
Active immunization

Monoclonal antibody against S.mutans
Monoclonal antibody against the surface protein antigen of S.sobrinus (Pag)
Passive immunization

A 重组质粒 pCIA-P B 重组质粒 pCIA-PC 重组质粒 pCIA-P D 空载体制裁粒 pCIE 生理盐水
0
0. 5
1
1. 5
2
2. 5
3
3. 5
4
A B C D E
PAc - I gG血 清 抗PAc- I gA血 清 抗PAc- I gG唾 液 抗PAc- I gA唾 液 抗
各 实 验 组 大 鼠 血 清 及 唾 液 中 特 异 性 抗 体 水 平 分 析 ( O D 4 0 5)

0
10
20
30
40
50
60
70
80
A B C D E
E级龋损Ds级龋损Dm级龋损
各实验组大鼠磨牙龋齿计分分析


茸毛链球菌占总的可培养细菌的百分数
A 单抗处理组 B 腹水对照组 C PBS 处理组
A B C0
1
2
3
4
5 Series 1 Series 2
Series 3 Series 4
Series 5 Series 6
Series 7 Series 8
Series 9 Series 10
C. PBS处理组

Immunoelectron microscopy of PcAb against S.sobrinus 6715 whole cells reacted with the three bacteria
S.sobrinus S.mutans S.rattus

Immunoeletorn microscopy of McAb ZS2/286 reacted
with the three bacteria
S.sobrinus S.mutans S.rattus

Immunoeletorn microscopy of non-specific mice ascites reacted
with S.sobrinus 6715

Polyclonal antibody against a S.mutans
GTase-I overexpression strain
Polyclonal antibody against caries in milk
IgY against caries in hen egg-yolk

Western blot of overexpress GTase-I strain

Effect of specific bovine milk antibodies against dental caries construction of GTase-I overexpressing strain B29-33
intramuscular immunization
specific cow milk antibodies
mouse rinsing
colonization level of S.mutan on teeth surface


¡ý¡ý¡ý¡ý ¡ý¡ý ¡ý¡ý¡ý¡ý¡ý¡ý¡ý¡ý¡ý¡ý¡ý
immunization milk collection
Scheme of cow immunization

Two cows both immu
nized with the GTase o
ver-expression strain de
veloped good IgG in m
ilk.
Specific IgG level in bovine milk by ELISA
3 25 50 60 75 950
0.1
0.2
0.3
0.4
Series 1
OD(405nm)
days after parturition

4 30 62.5 1000
0.1
0.2
0.3
0.4
0.5OD405
temperature (℃)
The effects of temperature on IgG in milk

Effect of specific IgY on prevention of dental caries
killed S.mutans, S.sobrinus whole cells
egg yolk IgY
effect of specific IgY on S.mutans in vitro
effect of specific IgY on caries prevention in animal models
intramuscularimmunization


Host factors: tooth

Tooth morphology and arch form

Clinical Observation
Pit and fissure area o
f posterior teeth are h
ighly susceptible to c
aries. Food debris an
d microoganisms rea
dily impact in the fis
sures.

In same tooth, differences in surfaces regardin
g to susceptible to caries
In mandibular first molars occlusal > buccal > mesial > distal > lingual
In maxillary first molar occlusal > mesial > lingual (palatal) > distal > buccal

Reason:
Partly due to tooth morphology pit and fissure > smooth
few caries in cuspal area
In first molar, distal area is free to saliva for 4-5 year, whereas the mesia area readily for
m dental plaque in 4~5 day after eruption.


Defect in tooth
Plaque growth 24 hours after cleaning, on a central maxillary incisor of a patient who is an “abundant” plaque former. Note the spread along the gingival margin, the crack, and other surface defects.

Extensive dental caries on the left side of maxilla and mandible in a patient who has received > 40 Gy radiation dose to the area of the left parotid gland

Where dental plaque likely to form?
Stagnation area ( 滞留区)
Photograph of plaque accumulation in stagnation areas after omission of toothbrushing for 3 days. Note that accumulations preferentially occur along the gingival margin and interproximal spaces whereas no plaque accumulates in cuspal and incisal areas due to continuous mechanical wear on these areas

Irregularities in arch form, crowding
and over lapping of the teeth also favor
the development of carious lesions.
Because of more stagnation areas

Clinical features immediately after removal of orthodontic appliances and cleaning. The orthodontic treatrment had lasted for 2 years. Noe the marked gingival reaction and the characteristic chalky surface appearance of the active enamel lesion.
After 3 months with careful oral hygiene the gingival tissues have recovered and the active lesion has been completely arrested. The white appearance of the lesion has diminished markedly due to polishing away of the eroded outermost enamel surface

Tooth composition

Enamal surface is more caries-resistant than the subsurface
Microradiograph of white
spot lesionof enamel. Com
pare the extensive deminer
alization of the subsurface
enamel with the better min
eralized surface layer (orig
inal magnificaiton 100)

The surface enamel has more mineral and
organic matter but relatively less water. In
addition, certain elements, including
fluoride, chloride, zincaccumulate in
the enamel surface.

A-C Concentration
gradients of
different elements
in enamel from the
surface towards the
enamel-dentinal
junction

Changes of the enamel, such as a decrease
in density and permeability and a increase
in nitrogen and fluoride content occur with
age. This “maturation” maker the tooth
more resistant to caries.

Fluoride concentrations in surface enamel of deciduous canines as a function of dental caries prevalence in the deciduous dentition at the age of 6 years. No straightforward relationship to illustrate that a high fluoride concentration should be linked to a low caries prevalence is seen. However, when the caries experience is high, the fluoride concentration in enamel becomes high as well.

Substrate: Diet and Caries

Diet: food and drink taken by any person
from day to day.
Function: locally
systemic

Locally:
react with the enamel surface and by serving as a substrate for cariogenic microoganisms.
Systemically: Nutrition, on melabolic processes

Difficulties in identify diet role in
influencing caries
Reason:
difficulties in control diet for a long time
information only from diet history

Many researches indicate the sucrose
in the “arch criminal” in the etiology
of caries.

Cumulative dental decay pr
evalence, expressed as DM
F permanent teeth, in childr
en ages 11 to 12. Correspon
ding annual 1959 per capita
sucrose utilization data for
18 countries and the state of
Hawaii, from the food and
Agriculture Organization of
the United ations. (Courtesy
of Dr. T. Marthaler.)

Relationship between dental caries and mean sugar intake (g/day) for South African males (16 to 17 years old) of four different ethnic groups. There is a direct relationship between percent population caries-fr
ee and sugar intake. (Drawn from the data of Retief et al.)

Interventional human studies

Vipeholm study

Hopewood House study
Plot of the mean number of DMF teeth per child versus chronological age in state schools of Australia and in children of Hopewood House (with standard error of means). Note the extremely low caries increment of the institutionalized children while under strict dietary control and the steep increase in caries experience when dietary supervision was no longer in effect – at above 13 years of age. (Courtesy of T. Marthaler)

Special population groups
hereditary fructose intolerance (HFI)


Assessment of cariogenic potential of foodsuffs
In vitro model of caries adhesiveness of food enamel demineralization production of titratable acid
Monitoring of plaque pH changes acidogenicity is measured
Animal testing

Adhesiveness of foods
adhesiveness:
attacment between food and the tooth
surface, sticky food

Determining sucrose content

Plaque-pH curves following the application of A: lactose, glucose, maltose,
fructore and sucrose, and B: raw starch, cooked starch, maltose and sucros
e.

Telemetrically recorded pH of interdental plaque (5 days old) in a subject during and
17 min after rinsing with 15ml of 10 per cent test solutions of Lycasin, xylitol, sorbito
l, sorbose and sucrose. PC=3min paraffin chewing; U=2 min urea rinse.

Other dietary components
and caries

Phosphates
cariostatic activity
animal experiment support that adding phosphate in diet reduce caries in animal, by local effect.
Human study: not convincing
Reason: difference in animal and human and in experiment.

Trace elements
Relationship of mineral elements to caries

Frequency of eating and cariesVipeholm study
Results of the Vipeholm dental caries study. Sugar in various forms was given either between or with meals over several years, and the rate of caries increase was studied. The caries increment was much lower wen sugar was given with meals compared with sugar between meals. (courtesy of B.E. Gustafsson.)

The effect of between –
meal eating on caries a
ctivity in 5- to 6-year-o
ld children. The more s
nacks children eat, the
higher is the caries incr
ement. (def) Decayed, e
xtracted, filled (teeth).
(Courtesy of Weiss and
Trithart.)

Animal studies

Early theories of caries etiology

Worms:
虫牙学说
Humors体液学说 :
ancient greek; four fluid of body are not in balance

Vital theory (活体学说 )
18 century, disease originate tooth itself.
Chemieal theory (化学酸学说 )
parmly (1819) suggest acid may induce caries.
Parasitic or septic theory (寄生腐败学说 )
microorganism may play role, by microscope, many bacteria on tooth were found.

proteolysis-chelation theory
First organic matter dissolved, degraded, then, the end product may have chelating effect and thereby dissolve the minerals in the enamel.
This process may happen at neutral or alkaline pH

Miller chemico-parasitic theory
acid was present in caries
many food mixed with salive and incubate
at 37℃ could decalcify tooth
Several oral bacteria could produce acid to
cause caries
Different bacteria invade caries lesion

Current concepts of caries etiology
Micro-organisms
host & tooth
Sub-stratecaries
time
no caries
no caries
no caries
no caries

Clinical classification of caries

Rate of caries progression
1950’s study:
it took one year the enamel fissure caries develop into dentine.
1989’s study:
only 50% fissure developed into dentine within 2 years.
Fluoride application may retard caries progression

The progression rates of proximal caries lesions from initial enamel caries to dentinal caries in permanent dentition was estimate to 68 (2 years at age 7, 4 years at age 12).

Classification according to progression rate
Acute caries:
progress fast, often in children and teenagers, light colored cavity.

Rampant caries, many tooth involved at same time acute caries feature often accompanied by systematic disorder. Such as sjogren syndrome or saliva reduction after radiation.
Caries in a patient with impaired salivary function as result of radiation therapy (courtesy of Drs Jansma and Vissink, R
UG, the Netherlands).

Chronic caries progress slowly, black or brown colored cavity hard remaining dentine
Arrested caries caries stop progressing because of the local etiological change

Secondary caries (recurrent caries)
caries recurred after treatment. Often at the margin the filling materials restoration or beneath
The shadow located on the mesiolingual cusp adjacent to the larger occlusal amalgam restoration on the maxillary right first molar indicates the presence of carious denti
n

Classification according to the involving site
Occlusal caries
Root caries
Smooth surface caries

Classification according to the deepness Superfacial caries( 浅龋 ) white spot lesions, visibly frosted surface br
own spot Dentin caries ( 中龋 ) cavitated lesion involving the up part of de
ntin Deep caries ( 深龋 ) cavitated lesion involving the pupal third of
dentin

Diagnosis• Visual change
•Probing: rough surface or trapping point
pain upon probing
• Temperature test
• X-ray examination
• Transillumination

Visual change
Matte, white, active cervical lesions

Probing: rough surface or trapping point pain upon probing
The explorer tip can easily damage white spot lesions

Temperature test

X-ray examination

transillumination
Proximal caries lesion is detected in an anterior tooth with the use of transillumination

Superfacial caries( 浅龋 )
White spot or brown, dark lesion, rough upon probing
No complaint, no hyper sensitivity

Dentin caries ( 中龋 )
Cavity, hypersensitivity upon probing, hot or cold stimulus.

Deep caries ( 深龋 )
Deep cavity, very sensitive and some pain upon stimulus, however the pain disappear as soon as the stimulus is taken away.