Embed Size (px)
Citation preview

Point prevalence surveys of healthcare-associated infections and antimicrobial use in healthcare facilities
European Centre for Disease Prevention and Control
Carl Suetens, Tommi Karki, Diamantis Plachouras, Pete Kinross (HAI-Net), Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Programme, ECDC

ECDC point prevalence surveys (PPSs), 2016-2017
2Source: Plachouras D, et al.; Ricchizzi E, et al.; Suetens C, Latour K. et al. Eurosurveillance 15 November 2018.
• 2nd ECDC PPS of healthcare-associated infections and antimicrobial use in European acute care hospitals
• 3rd ECDC PPS of healthcare-associated infections and antimicrobial use in European long-term care facilities
Objectives
• To estimate the prevalence and burden of healthcare-associated infections (HAIs, all types) and antimicrobial use
• To describe key structures and processes for the prevention of HAIs and antimicrobial resistance at the hospital and ward level in hospitals in EU/EEA countries
• To describe patients/residents, infections (sites, micro-organisms including markers of antimicrobial resistance) and antimicrobials prescribed (compounds, indications)
• To disseminate results to those who need to know at local, regional, national and EU level
Raise awareness
Train and reinforce surveillance structures and skills
Identify common EU problems and set up priorities accordingly
Evaluate the effect of strategies and guide policies (repeated PPS)
• To provide a standardised tool to identify targets for quality improvement
3

Protocols and tools
http://ecdc.europa.eu/en/healthtopics/Healthcare-associated_infections/point-prevalence-survey/Pages/Point-prevalence-survey.aspx 4
• PPS II protocol v5.3, HALT-3 (v2.1)
• Extranet: Q&A (MS Excel), training materials, validation protocol
• Train-the-trainers: face-to-face + webinars
• HelicsWin.Net/HALT software
• Hospital/LTCF feedback reports

Methods
PPS in acute care hospitals(ECDC PPS-2)
PPS in long-term care facilities (HALT-3 PPS)
Where? All EU/EEA countries and (potential) candidate countries invited
When? 4 possible periods 2016 and 2017, April-June & September-November
Data collection duration One ward one day, hospital 2-3 weeks One day, larger facilities >1 day
Who? All patients on ward at 8:00 am All residents present at 8:00 am and living in the LTCF
Exclusion Accident and emergency wards,Day cases
e.g. hospitalised residents
HAI case definitions EU case definitions (PN, BSI, SSI, UTI, CDI, neonatal HAIs), other CDC 2008
case definitions
Modified CDC/SHEA/Mc Geer case definitions for HAIs in LTCFs
Active HAI Signs and symptoms present on day PPS or were present and patient/resident is still receiving treatment for that infection on day PPS
National validation `Mandatory’, + ECDC support, min. 250 pts in 5 hospitals
Voluntary, min 1 LTCF
5
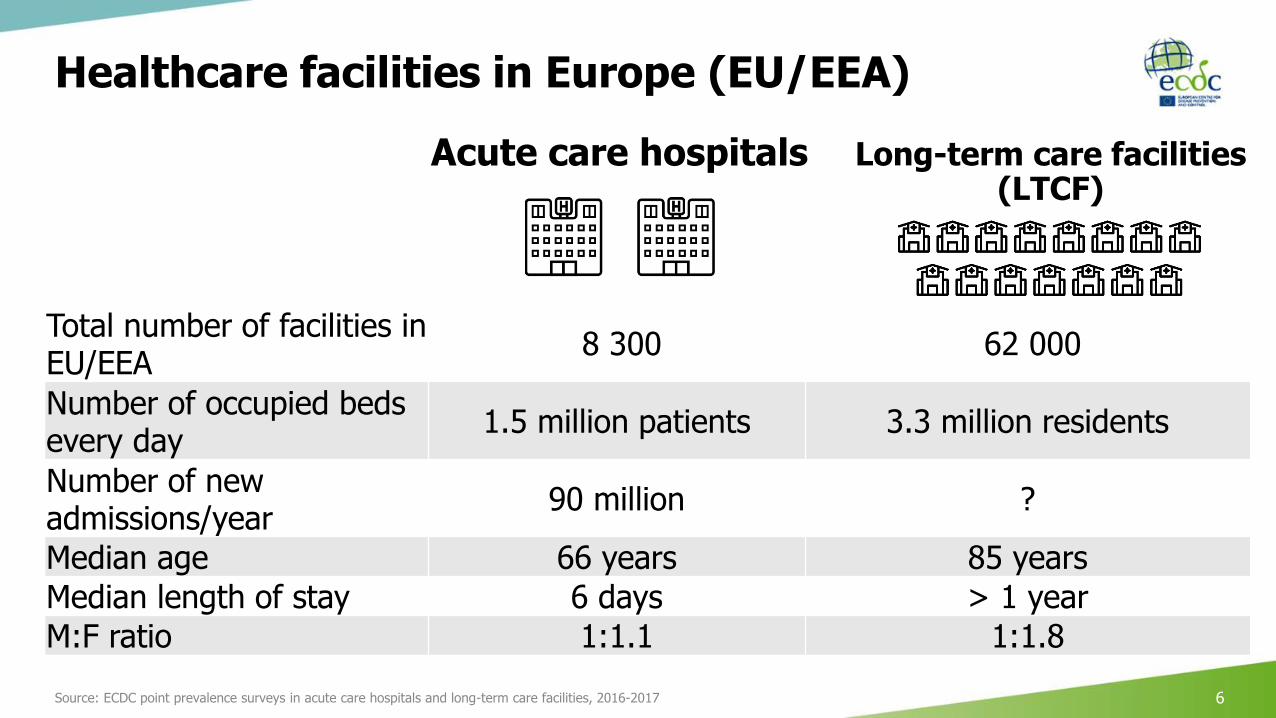
Healthcare facilities in Europe (EU/EEA)
Source: ECDC point prevalence surveys in acute care hospitals and long-term care facilities, 2016-2017 6
Acute care hospitals Long-term care facilities (LTCF)
Total number of facilities in EU/EEA
8 300 62 000
Number of occupied beds every day
1.5 million patients 3.3 million residents
Number of new admissions/year
90 million ?
Median age 66 years 85 years
Median length of stay 6 days > 1 year
M:F ratio 1:1.1 1:1.8
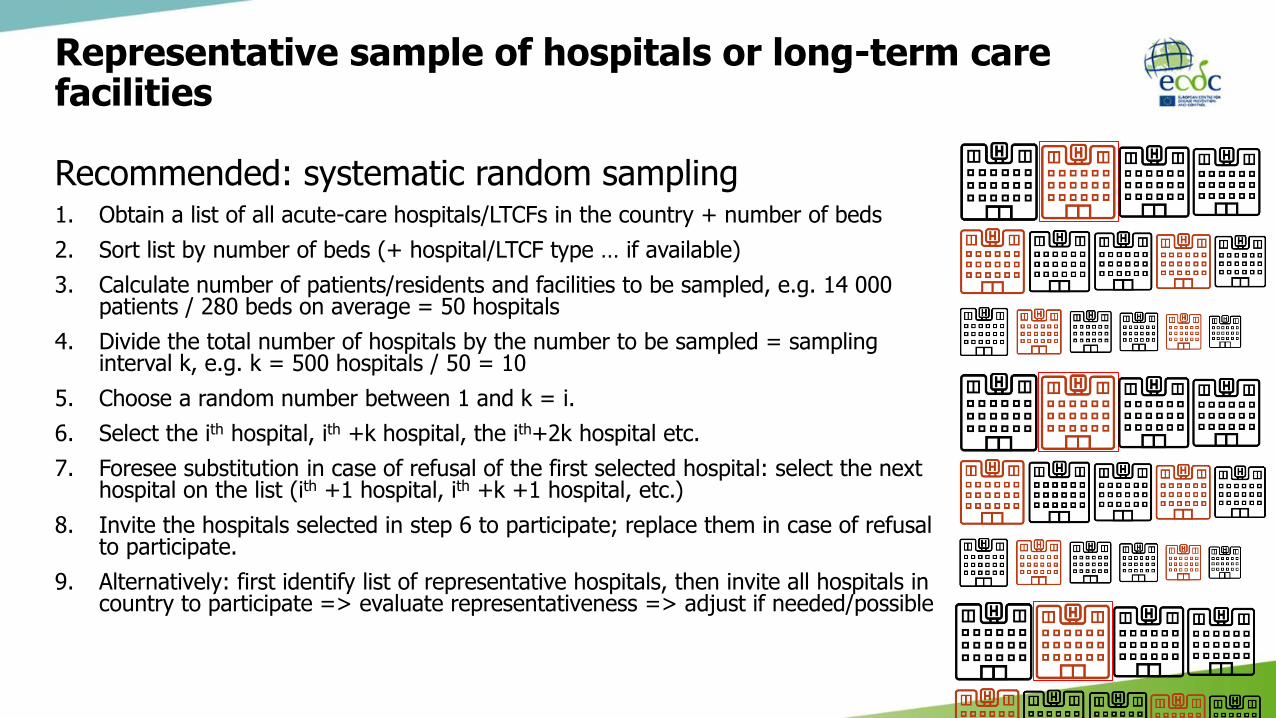
Representative sample of hospitals or long-term care facilities
Recommended: systematic random sampling1. Obtain a list of all acute-care hospitals/LTCFs in the country + number of beds
2. Sort list by number of beds (+ hospital/LTCF type … if available)
3. Calculate number of patients/residents and facilities to be sampled, e.g. 14 000 patients / 280 beds on average = 50 hospitals
4. Divide the total number of hospitals by the number to be sampled = sampling interval k, e.g. k = 500 hospitals / 50 = 10
5. Choose a random number between 1 and k = i.
6. Select the ith hospital, ith +k hospital, the ith+2k hospital etc.
7. Foresee substitution in case of refusal of the first selected hospital: select the next hospital on the list (ith +1 hospital, ith +k +1 hospital, etc.)
8. Invite the hospitals selected in step 6 to participate; replace them in case of refusal to participate.
9. Alternatively: first identify list of representative hospitals, then invite all hospitals in country to participate => evaluate representativeness => adjust if needed/possible
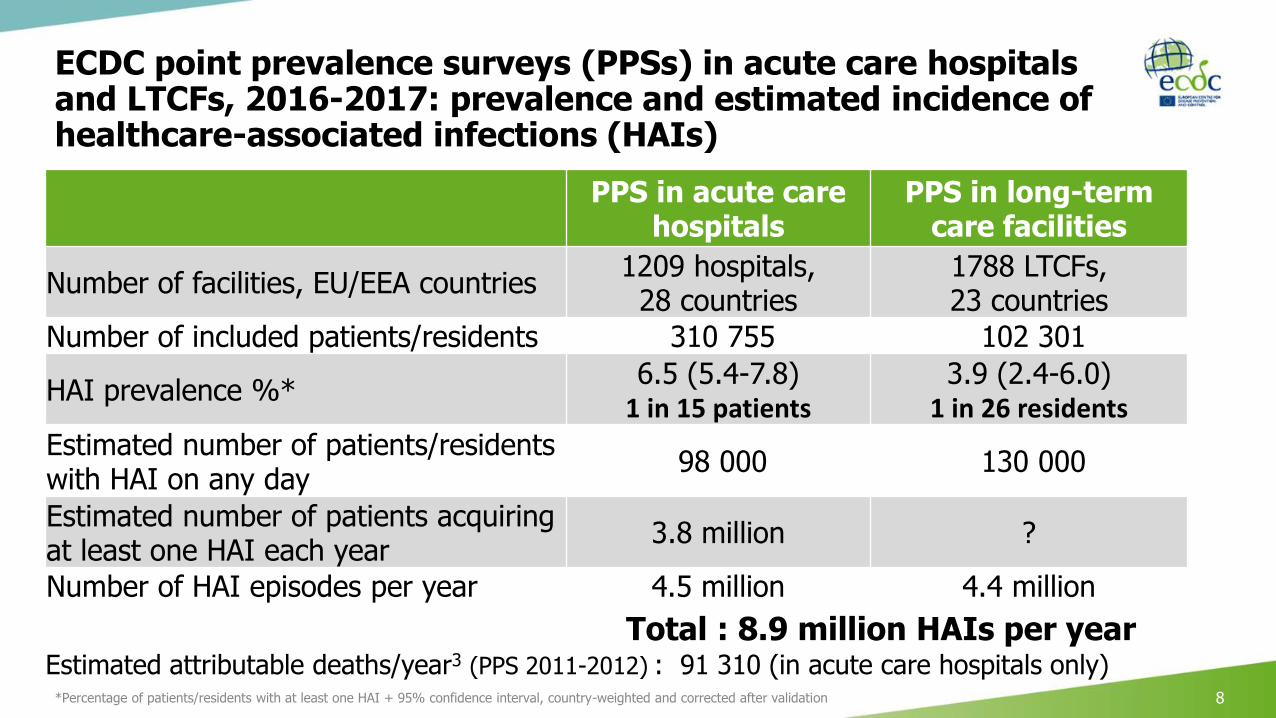
ECDC point prevalence surveys (PPSs) in acute care hospitals and LTCFs, 2016-2017: prevalence and estimated incidence of healthcare-associated infections (HAIs)
*Percentage of patients/residents with at least one HAI + 95% confidence interval, country-weighted and corrected after validation 8
PPS in acute care hospitals
PPS in long-term care facilities
Number of facilities, EU/EEA countries1209 hospitals, 28 countries
1788 LTCFs, 23 countries
Number of included patients/residents 310 755 102 301
HAI prevalence %*6.5 (5.4-7.8)
1 in 15 patients3.9 (2.4-6.0)
1 in 26 residents
Estimated number of patients/residents with HAI on any day
98 000 130 000
Estimated number of patients acquiring at least one HAI each year
3.8 million ?
Number of HAI episodes per year 4.5 million 4.4 million
Total : 8.9 million HAIs per year Estimated attributable deaths/year3 (PPS 2011-2012) : 91 310 (in acute care hospitals only)

PPS-1: Comparing the burden of HAIs with other infectious diseases
HAIsaccount for twice the burdenof 31 other infectious diseases
Burden of HAIs – 2011-2012 *Burden of 5 top ranking infectious diseases from BCoDE 2009-2013 **
Source: *Cassini A, et al. PLoS Med 2016;13(10):e1002150
** Cassini A, et al. Euro Surveill. 2018;23(16):pii=17-00454
AT
BE
BG
CY
CZ
DE
EE
ES
FI
FR
HR
HU
IEIS
IT
LT
LU
LV
MT
NO
PL
PT
RO
RS
SI
SK
UK-ENUK-NI
UK-SC
UK-WA
24
68
10
Patie
nts
with
at
least
one
HA
I (%
)
0 20 40 60 80 100
Blood cultures (No. per 1000 patient-days)
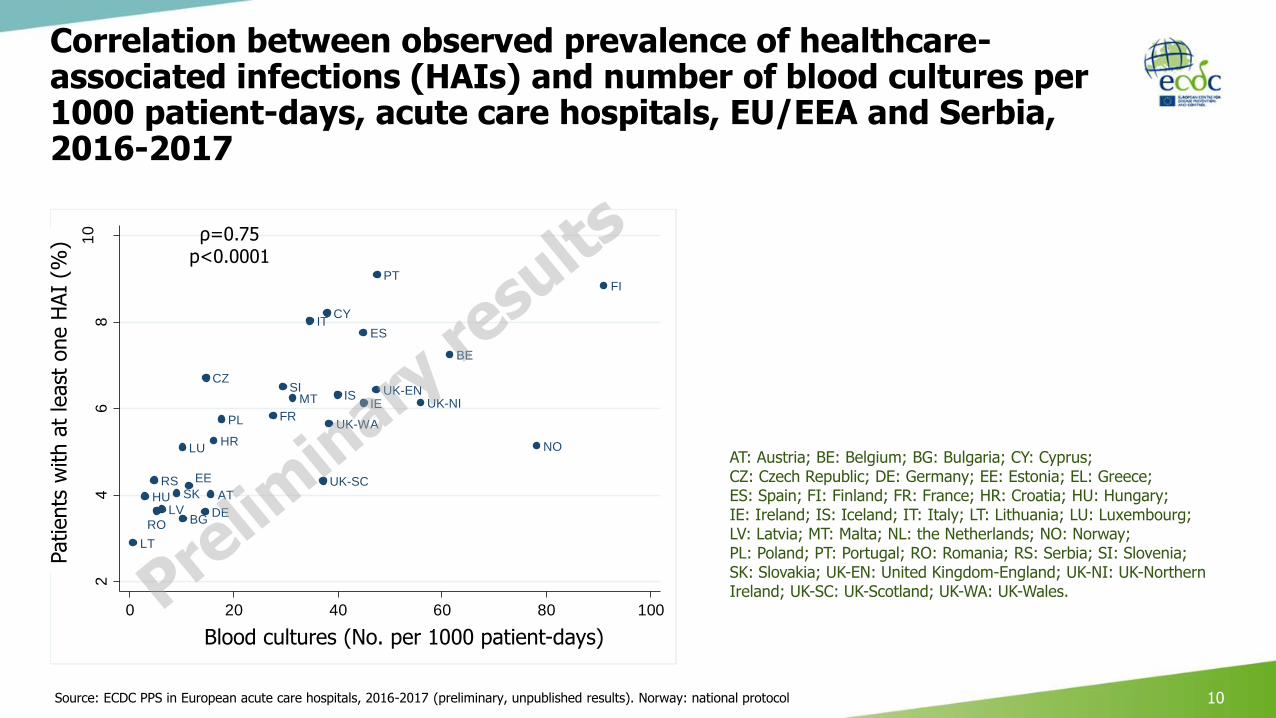
Correlation between observed prevalence of healthcare-associated infections (HAIs) and number of blood cultures per 1000 patient-days, acute care hospitals, EU/EEA and Serbia, 2016-2017
Source: ECDC PPS in European acute care hospitals, 2016-2017 (preliminary, unpublished results). Norway: national protocol 10
AT: Austria; BE: Belgium; BG: Bulgaria; CY: Cyprus; CZ: Czech Republic; DE: Germany; EE: Estonia; EL: Greece; ES: Spain; FI: Finland; FR: France; HR: Croatia; HU: Hungary; IE: Ireland; IS: Iceland; IT: Italy; LT: Lithuania; LU: Luxembourg; LV: Latvia; MT: Malta; NL: the Netherlands; NO: Norway; PL: Poland; PT: Portugal; RO: Romania; RS: Serbia; SI: Slovenia; SK: Slovakia; UK-EN: United Kingdom-England; UK-NI: UK-Northern Ireland; UK-SC: UK-Scotland; UK-WA: UK-Wales.
Patients
with a
t le
ast
one H
AI
(%)
Blood cultures (No. per 1000 patient-days)
ρ=0.75p<0.0001
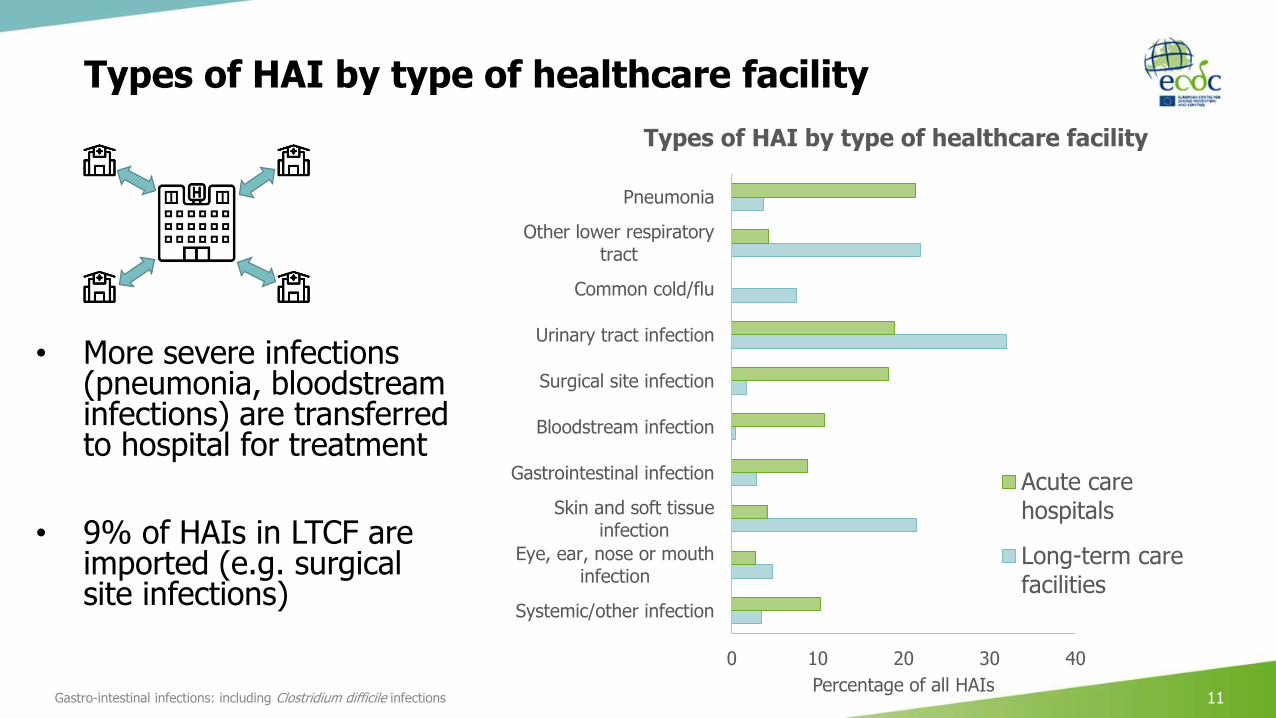
Types of HAI by type of healthcare facility
Gastro-intestinal infections: including Clostridium difficile infections 11
• More severe infections (pneumonia, bloodstream infections) are transferred to hospital for treatment
• 9% of HAIs in LTCF are imported (e.g. surgical site infections)
0 10 20 30 40
Systemic/other infection
Eye, ear, nose or mouthinfection
Skin and soft tissueinfection
Gastrointestinal infection
Bloodstream infection
Surgical site infection
Urinary tract infection
Common cold/flu
Other lower respiratorytract
Pneumonia
Percentage of all HAIs
Types of HAI by type of healthcare facility
Acute carehospitals
Long-term carefacilities

Site of infection in antimicrobial treatment by origin
12
34%
16%2%
13%
6%
15%
7%6%
27%
18%
8%11%
9%
19%
5%4%
40%
24%
4%
8%
7%
12%2%4%
32%
17%4%
12%
7%
16%
6%5%
Community infection (n=54347) Hospital infection (n=21328)
LTCF HAI (n=2159) Total
Respiratory tract Urinary tract
Bacteremia Gastrointestinal
Systemic Skin, soft tissue, bone/joint
Other sites Undefined/unknown
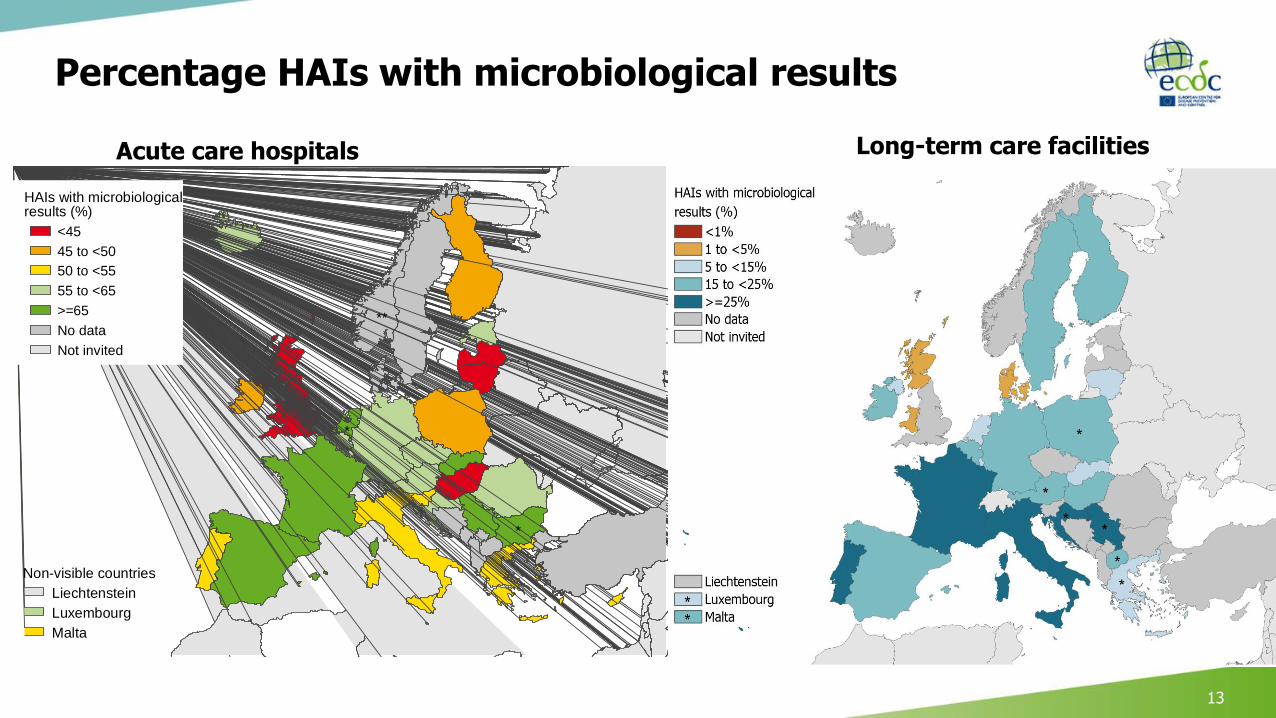
Percentage HAIs with microbiological results
13
Acute care hospitals
**
*
*
Liechtenstein
Luxembourg
Malta
Non-visible countries
<45
45 to <50
50 to <55
55 to <65
>=65
No data
Not invited
HAIs with microbiologicalresults (%)
Long-term care facilities
14
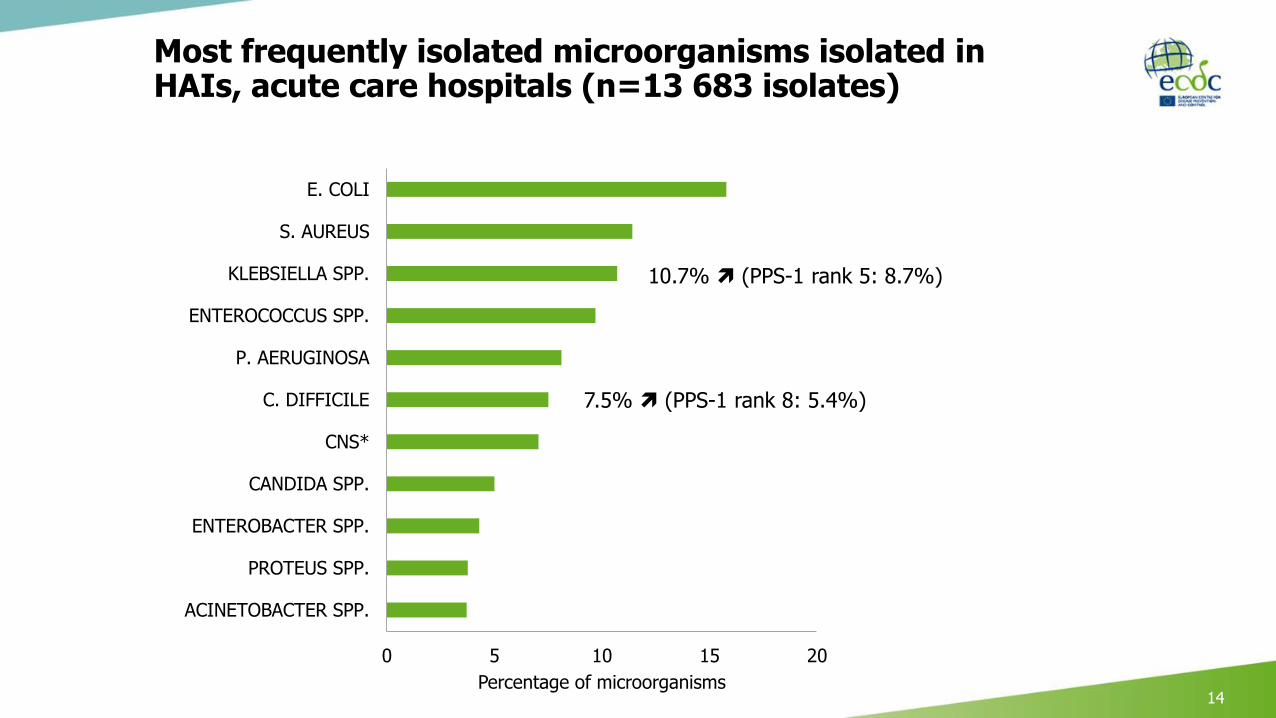
Most frequently isolated microorganisms isolated in HAIs, acute care hospitals (n=13 683 isolates)
14*CNS: coagulase-negative staphylococci
0 5 10 15 20
ACINETOBACTER SPP.
PROTEUS SPP.
ENTEROBACTER SPP.
CANDIDA SPP.
CNS*
C. DIFFICILE
P. AERUGINOSA
ENTEROCOCCUS SPP.
KLEBSIELLA SPP.
S. AUREUS
E. COLI
Percentage of microorganisms
10.7% (PPS-1 rank 5: 8.7%)
7.5% (PPS-1 rank 8: 5.4%)

Composite index* of antimicrobial resistance (AMR) in healthcare-associated infections from acute care hospitals, EU/EEA countries and Serbia, 2016-2017
15
**
*
*
Liechtenstein
Luxembourg
Malta
Non-visible countries
<5
5 to <20
20 to <35
35 to <50
>=50
No data
Not invited
Resistantisolates (%)
*Percentage of isolates resistant to first-level antimicrobial resistance markers in healthcare-associated infections, i.e.:- Staphylococcus aureus resistant to meticillin
(MRSA), - Enterococcus faecium and Enterococcus faecalis
resistant to vancomycin, - Enterobacteriaceae resistant to third-generation
cephalosporins, - Pseudomonas aeruginosa and Acinetobacter
baumannii resistant to carbapenems.
Adapted from: Suetens C, et al. Eurosurveillance 15 November 2018;
* Bulgaria and the Netherlands: poor national representativeness of acute care hospital sample; ** Norway: national protocol; Norway and UK-Scotland did not collect microbiological data..

Correlations between composite indices of antimicrobial resistance (AMR) from ECDC data
Adapted from: Suetens C, et al. Eurosurveillance 15 November 2018. 16
PPS long-term care facilities 2016-2017EARS-Net 2016
PP
S a
cu
te c
are
ho
sp
ita
ls 2
01
6-2
01
7
PP
S a
cu
te c
are
ho
sp
ita
ls 2
01
6-2
01
7

Estimated burden of infections with antibiotic-resistant bacteria, age-group standardised, EU/EEA, 2015
Source: Cassini A, et al. Lancet Infectious Diseases. 5 November 2018.
671 689 infections with antibiotic-resistant bacteria
33 110 attributable deaths
170 DALYs* per 100 000 population
• 63% of cases were HAIs,representing 75% of total burden (DALYs)
• 70% due to 4 top-ranking antibiotic-resistant bacteria
• 39% due to carbapenem- and/or colistin resistance
*DALYS, Disability-adjusted life years

Prevalence of antimicrobial use, 2016-2017
Eurosurveillance 15 November 2018 18
**
*
*
Liechtenstein
Luxembourg
Malta
Non-visible countries
<30
30 to <35
35 to <40
40 to <45
>=45
Did not participate
Not invited
Patients onantimicrobials (%)
**
*
*
Liechtenstein
Luxembourg
Malta
Non-visible countries
<30
30 to <35
35 to <40
40 to <45
>=45
Did not participate
Not invited
Patients onantimicrobials (%)
* Bulgaria, the Netherlands: poor national representativeness of acute care hospital sample; ** Norway: national protocol.
Acute care hospitals Long-term care facilities
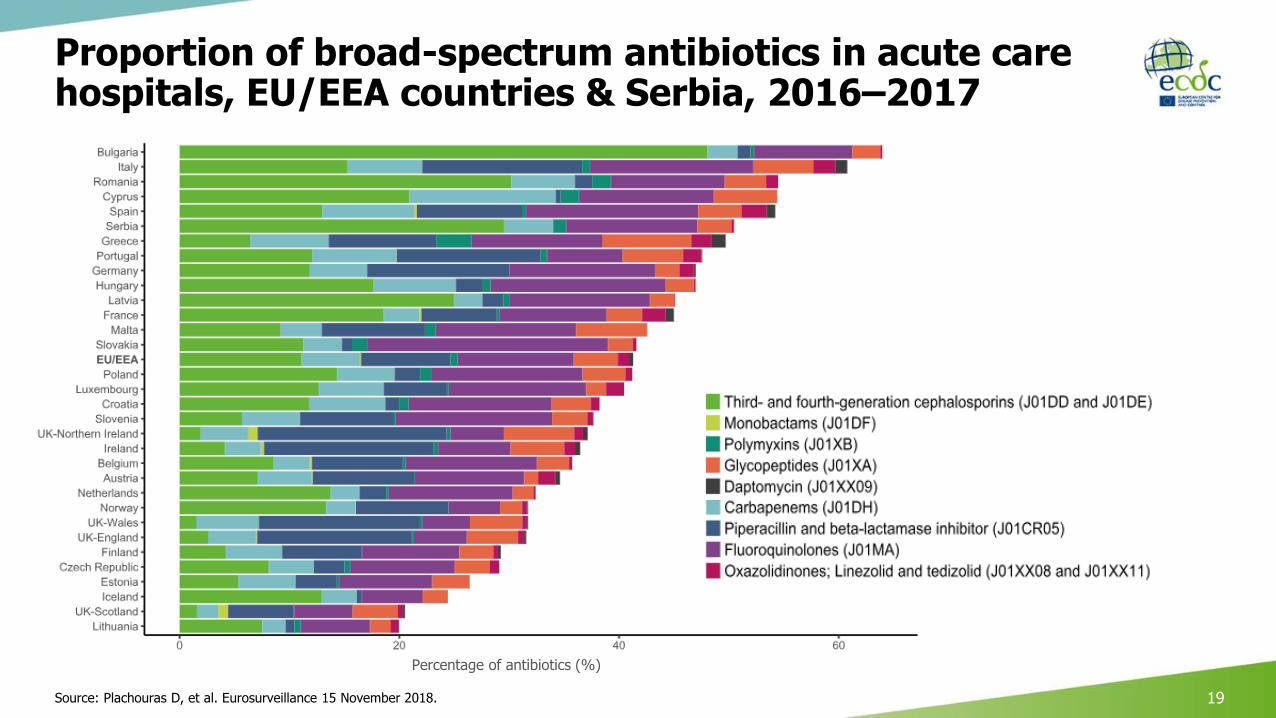
19Source: Plachouras D, et al. Eurosurveillance 15 November 2018.
Proportion of broad-spectrum antibiotics in acute care hospitals, EU/EEA countries & Serbia, 2016–2017
Percentage of antibiotics (%)
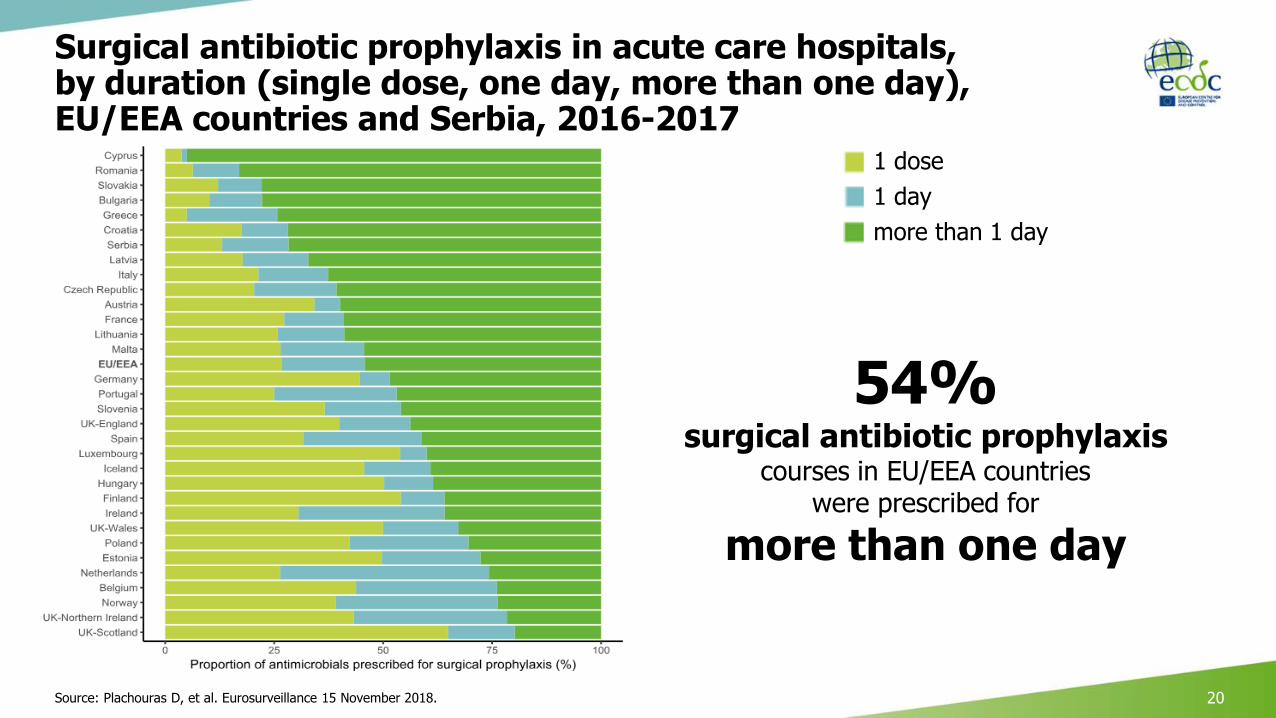
Surgical antibiotic prophylaxis in acute care hospitals, by duration (single dose, one day, more than one day), EU/EEA countries and Serbia, 2016-2017
20
54% surgical antibiotic prophylaxis
courses in EU/EEA countrieswere prescribed for
more than one day
1 dose
1 day
more than 1 day
Source: Plachouras D, et al. Eurosurveillance 15 November 2018.

Correlation of the composite index of AMR* with prevalence of antimicrobial use in acute care hospitals, EU/EEA countries and Serbia, 2016-2017
Adapted from Suetens C, et al. Eurosurveillance 15 November 2018; Plachouras D, et al. Eurosurveillance 15 November 2018 (unpublished results). 21
Patients
with a
least
one a
ntim
icro
bia
l (%
)Patients
with a
t le
ast
one a
ntim
icro
bia
l (%
)
Composite index of AMR (%)
*Percentage of isolates resistant to first-level antimicrobial resistance markers in healthcare-associated infections, i.e.:- Staphylococcus aureus resistant to meticillin (MRSA), - Enterococcus faecium and Enterococcus faecalis
resistant to vancomycin, - Enterobacteriaceae resistant to third-generation
cephalosporins, - Pseudomonas aeruginosa and Acinetobacter baumannii
resistant to carbapenems.
Multiple regression (preliminary results):% AMR significantly associated with:- Antimicrobial use (% of patients)- Presence of AHR dispensers at point of care
(% of beds)- Single(-room) beds (%)- FTE ICN (>0.4-0.5 IPCN/250 beds)- Case mix
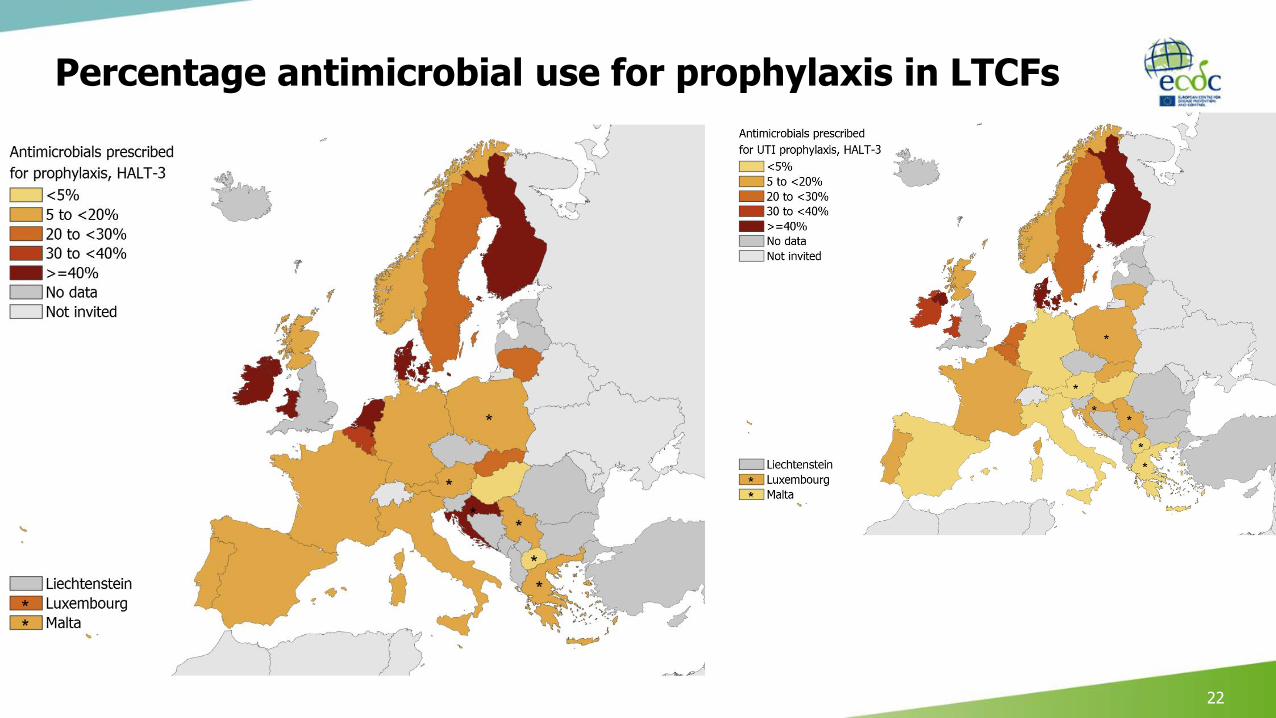
Percentage antimicrobial use for prophylaxis in LTCFs
22

ECDC PPS indicators of WHO core components of infection prevention and control (IPC) programmes
Source: ECDC, 2018 (see ECDC point prevalence survey of healthcare-associated infections and antimicrobial use in European acute care hospitals. Protocol version 5.3. 23
WHO Core Component Description ECDC PPS hospital indicators
1Infection prevention and control (IPC) programme
An effective IPC programme in an acute care hospital must include at least: one full-time specifically trained IPC-nurse ≤ 250 beds; a dedicated physician trained infection control; microbiological support; data management support
FTE IPC nurses and doctors IPC plan and report approved by hospital CEO Number of blood cultures, stool tests for CDI Microbiology services during weekends
2 IPC guidelinesEvidence-based guidelines + education, training of relevant health care workers and monitoring of adherence with guidelines
Presence of guidelines, audit and checklist for prevention of PN, BSI, UTI, SSI and for antimicrobial stewardship (as part of multimodal strategy, in ICU and hospital-wide)
3 IPC education and trainingIPC education and training involves frontline staff, and is team- and task-oriented
Presence of training in prevention of PN, BSI, UTI, SSI and antimicrobial stewardship (as part of multimodal strategy, ICU and hospital-wide)
4 SurveillanceParticipating in prospective surveillance and offering active feedback, preferably as part of a network
Participation in ICU, SSI, CDI, AMR and AMC surveillance networks
Surveillance as part of multimodal strategy
5 Multimodal strategiesImplementing infection control programmes follow a multimodal strategy including tools such as bundles and checklists developed by multidisciplinary teams and taking into account local conditions
Presence of guideline, bundle, training, checklist, audit, surveillance, feedback for prevention of PN, BSI, UTI, SSI and for antimicrobial stewardship
6Monitoring/audit of IPC practices and feedback
Organising audits as a standardized (scored) and systematic review of practice with timely feedback
Number of hand hygiene observations Alcohol hand rub consumption Audit and feedback as part of multimodal strategy
7Workload, staffing and bed occupancy
To make sure that the ward occupancy does not exceed the capacity for which it is designed and staffed; staffing and workload of frontline health-care workers must be adapted to acuity of care; and the number of pool/agency nurses and physicians minimized
Bed occupancy at midnight FTE registered nurses, hospital-wide and ICU FTE nursing assistants, hospital-wide and ICU
8Built environment, materials and equipment for IPC at the facility level
Sufficient availability of and easy access to material and equipment and optimized ergonomics; adequate number of single rooms (preferably with private toilet facilities) and/or rooms suitable for patient cohorting for the isolation of suspected /infected patients, including those with TB and multidrug-resistant organisms, to prevent transmission to other patients, staff and visitors
Alcohol hand rub dispensers at point of care+ carriage of AHR bottles by health-care workers
Number of single rooms Number of single rooms with toilet and shower Number of airborne infection isolation rooms
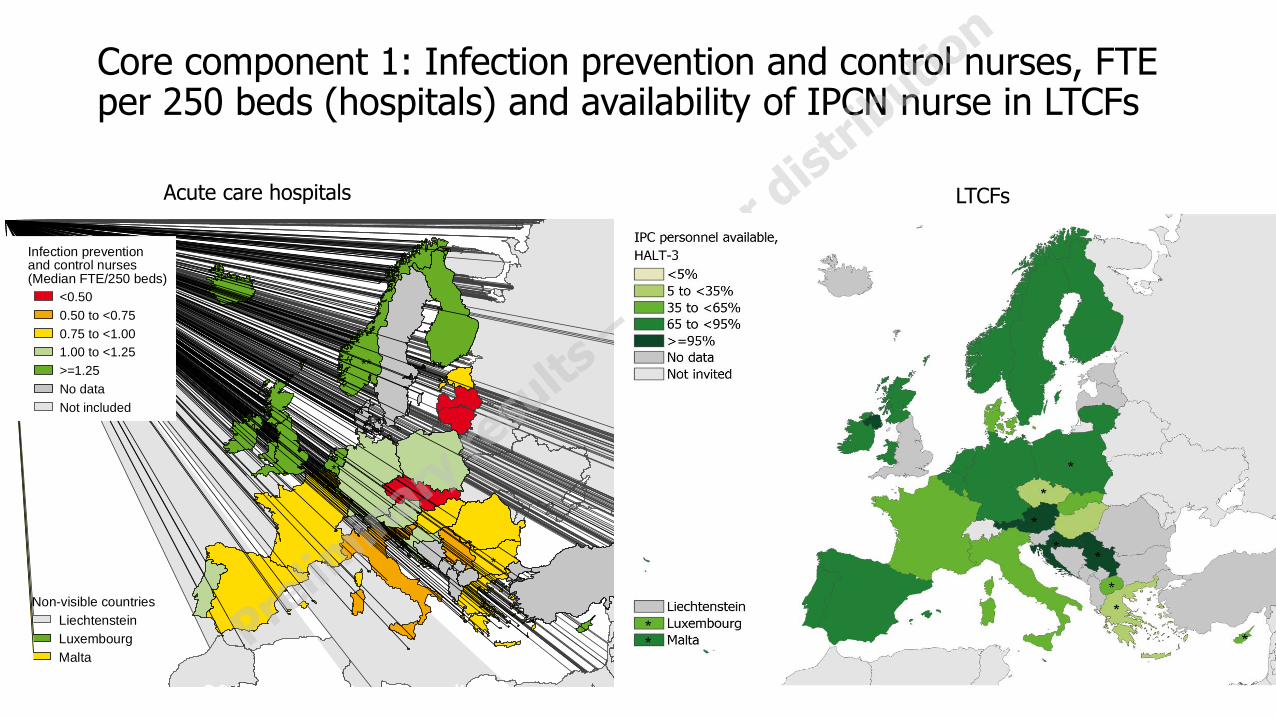
Core component 1: Infection prevention and control nurses, FTE per 250 beds (hospitals) and availability of IPCN nurse in LTCFs
Acute care hospitals
*poor representativeness, **Norway 2017: national PPS protocol
**
*
*
Liechtenstein
Luxembourg
Malta
Non-visible countries
<0.50
0.50 to <0.75
0.75 to <1.00
1.00 to <1.25
>=1.25
No data
Not included
Infection preventionand control nurses(Median FTE/250 beds)
2016-2017 data are preliminary.
LTCFs

Core component 6. monitoring of practices:Alcohol hand rub consumption (L/1000 patient-days)
Source: ECDC PPSs in European acute care hospitals, 2011-2012 & 2016-2017 (preliminary, unpublished results). 25
2011-2012
*poor country representativeness, **Norway 2017: national PPS protocol.
2016-2017
**
*
*
Liechtenstein
Luxembourg
Malta
Non-visible countries
<10
10-19.9
20-29.9
30-39.9
>=40
No data
Not included
Alcohol hand rubconsumption(L/1000 patient days)

Core component 8: environment – Beds with alcohol hand rub dispensers at point of care (%)
**
*
*
Liechtenstein
Luxembourg
Malta
Non-visible countries
<10
10 to <20
20 to <50
50 to <90
>=90
No data
Not invited
Beds with AHR dispenserat point of care (%)
05
10
15
20
25
Me
dia
n A
HR
con
sum
ption
(L
/100
0 p
atie
nt-
da
ys)
<50% beds with AHR >=50% beds with AHR
<25% HCW >=25% HCW <25% HCW >=25% HCW
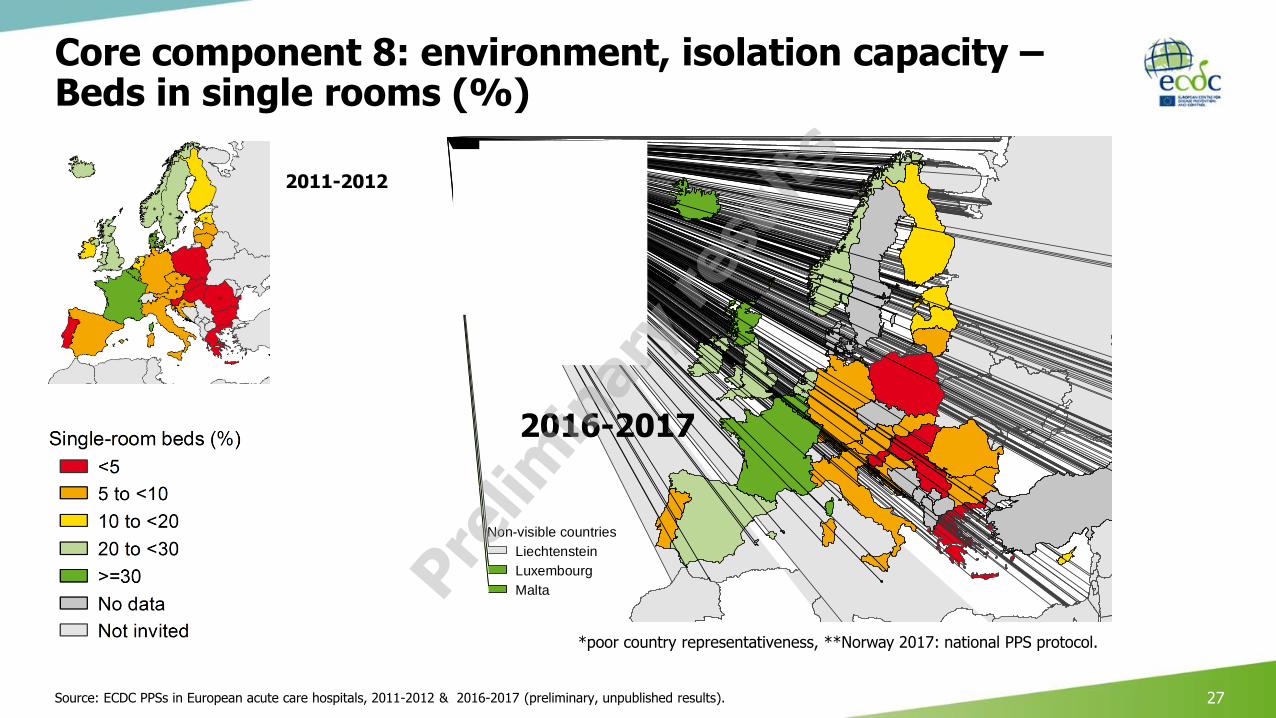
Core component 8: environment, isolation capacity –Beds in single rooms (%)
Source: ECDC PPSs in European acute care hospitals, 2011-2012 & 2016-2017 (preliminary, unpublished results). 27
2011-2012
**
*
*
Liechtenstein
Luxembourg
Malta
Non-visible countries
<5
5 to <10
10 to <20
20 to <30
>=30
No data
Not invited
Single-room beds (%)
2016-2017
*poor country representativeness, **Norway 2017: national PPS protocol.
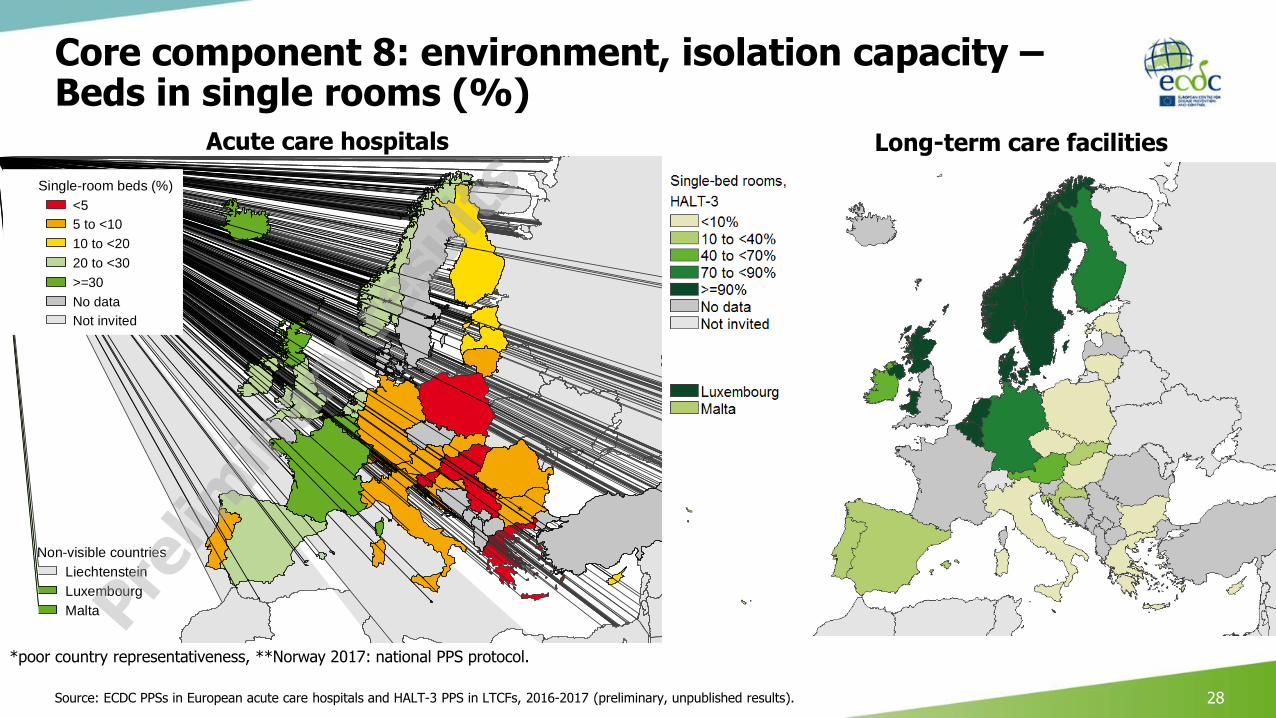
Core component 8: environment, isolation capacity –Beds in single rooms (%)
Source: ECDC PPSs in European acute care hospitals and HALT-3 PPS in LTCFs, 2016-2017 (preliminary, unpublished results). 28
**
*
*
Liechtenstein
Luxembourg
Malta
Non-visible countries
<5
5 to <10
10 to <20
20 to <30
>=30
No data
Not invited
Single-room beds (%)
*poor country representativeness, **Norway 2017: national PPS protocol.
Acute care hospitals Long-term care facilities
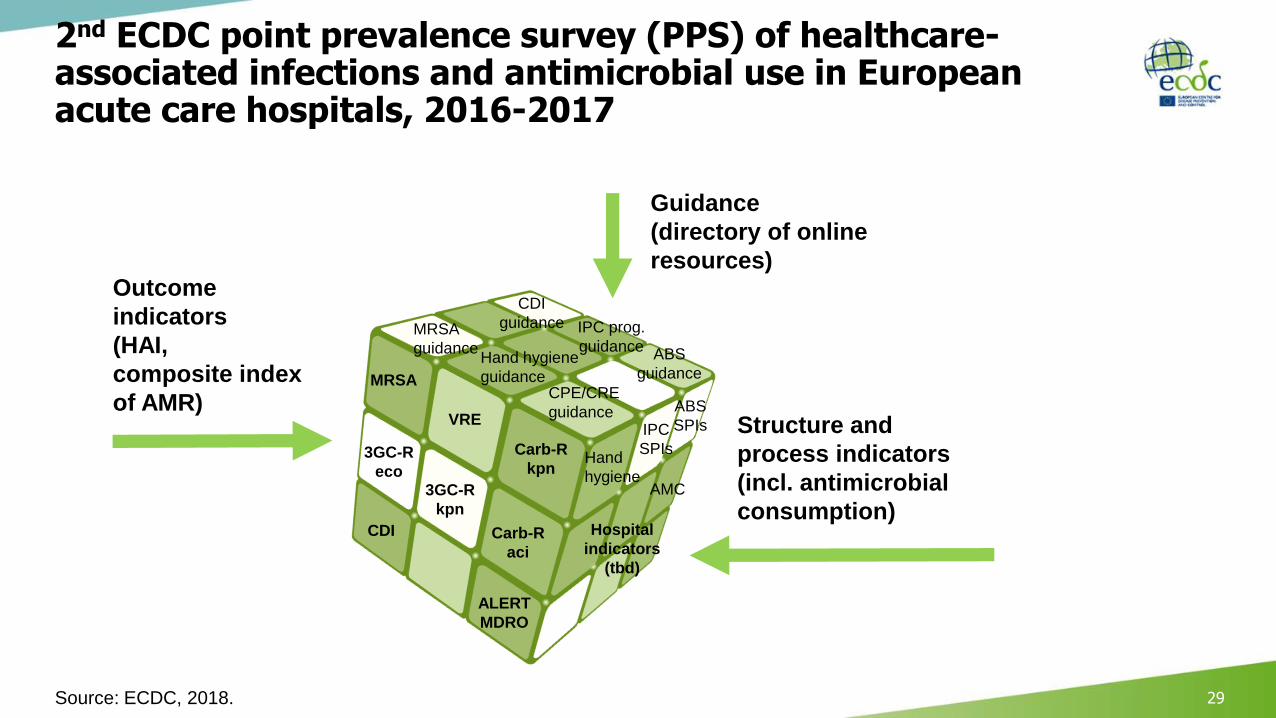
2nd ECDC point prevalence survey (PPS) of healthcare-associated infections and antimicrobial use in European acute care hospitals, 2016-2017
Source: ECDC, 2018. 29
MRSA
Carb-R
kpn
VRE
CDI
3GC-R
eco3GC-R
kpn
ALERT
MDRO
Carb-R
aci
MRSA
guidance
CDI
guidance
CPE/CRE
guidance
ABS
guidance
IPC prog.
guidanceHand hygiene
guidance
Outcome
indicators
(HAI,
composite index
of AMR)Structure and
process indicators
(incl. antimicrobial
consumption)
Guidance
(directory of online
resources)
Hospital
indicators
(tbd)
IPC
SPIsHand
hygiene
ABS
SPIs
AMC
Thank you
30

Active HAI
ONSET OF HAI CASE DEFINITION
Day 3 onwards AND Meets the case definition on the dayof surveyOR
Day 1 (day of admission) or day 2: SSI criteria met at any time after admission (including previous surgery 30 d/ 90 d)
ORORDay 1 or day 2 AND patient
discharged from acute care hospital in preceding 48 hours
ORDay 1 or day 2 AND patient discharged from acute care hospital in preceding 28
days if CDI present
Patient is receiving treatment* AND HAI has previously met the case definition between day 1 of treatment and survey day
OR
Day 1 or day 2 AND patient has relevant device inserted on this admission prior
to onset
OR
Day 1 or day 2 after birth for neonates
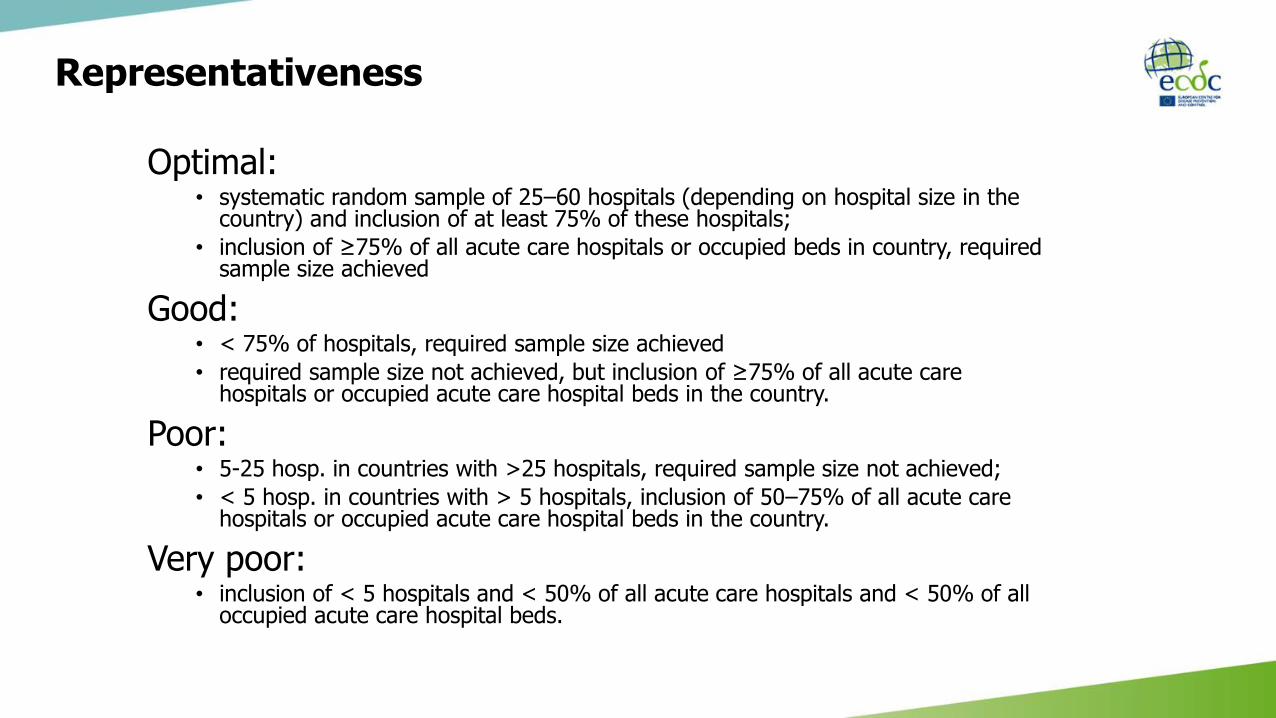
Representativeness
Optimal:• systematic random sample of 25–60 hospitals (depending on hospital size in the
country) and inclusion of at least 75% of these hospitals;
• inclusion of ≥75% of all acute care hospitals or occupied beds in country, required sample size achieved
Good:• < 75% of hospitals, required sample size achieved
• required sample size not achieved, but inclusion of ≥75% of all acute care hospitals or occupied acute care hospital beds in the country.
Poor: • 5-25 hosp. in countries with >25 hospitals, required sample size not achieved;
• < 5 hosp. in countries with > 5 hospitals, inclusion of 50–75% of all acute care hospitals or occupied acute care hospital beds in the country.
Very poor:• inclusion of < 5 hospitals and < 50% of all acute care hospitals and < 50% of all
occupied acute care hospital beds.
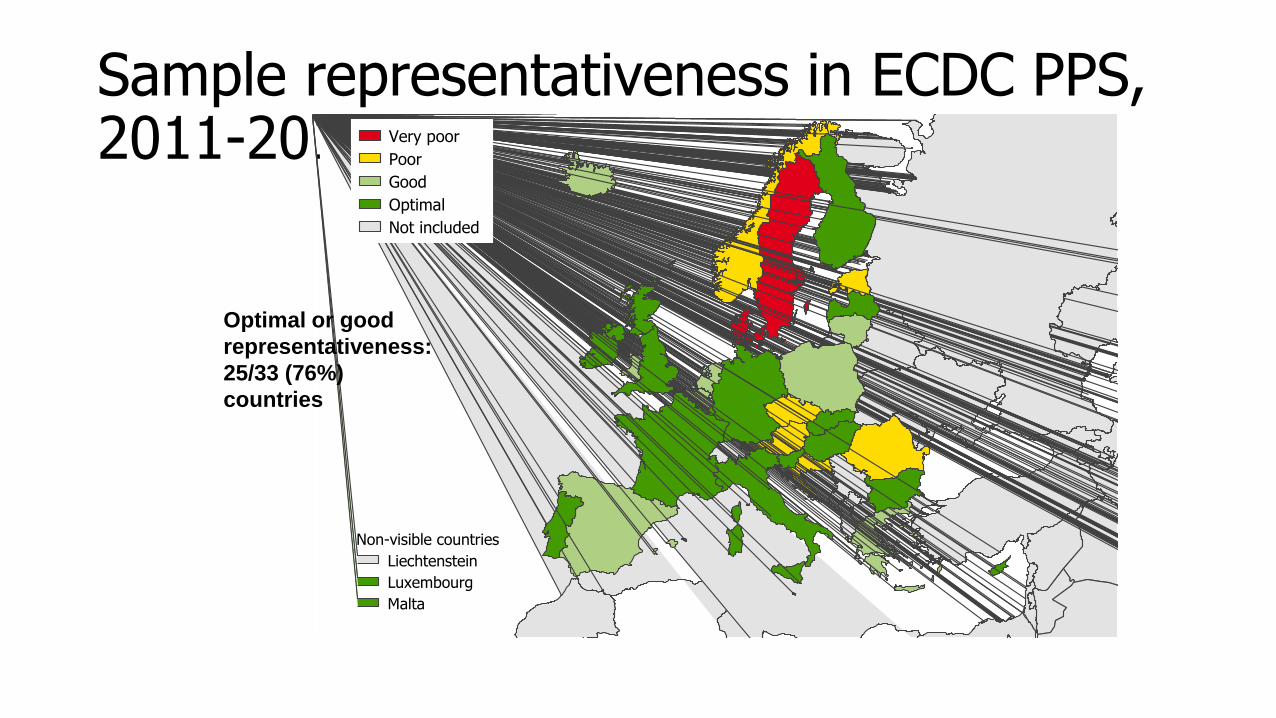
Sample representativeness in ECDC PPS, 2011-2012
Liechtenstein
Luxembourg
Malta
Non-visible countries
Very poor
Poor
Good
Optimal
Not included
Optimal or good
representativeness:
25/33 (76%)
countries
General Guidelines
All patients present on the ward at 8am and not discharged at the time of survey should be included
Complete each ward within one day
Complete the hospital within 2-3 weeks
Units where patients are admitted for elective procedures on a Monday should preferably be surveyed between Tuesday and Thursday

Included/Excluded?INCLUDED
• Hospitals
• All acute care hospitals/ facilities
• All sizes
• Wards
• All hospital wards, both acute and long-term care (including psychiatric wards & neonatal units)
• Include wards attached to A&E/ ER departments where patients are monitored >24 hours
• Patients
• All admitted to ward before 8 a.m. & not discharged at the time of the survey
EXCLUDED
• Hospitals
• Long term care facilities without acute care beds
• Wards
• accident & emergency department
• Patients
• Day cases including: same day treatment or surgery, outpatient, or emergency room (A&E) episode, renal dialysis day attenders

Inclusion and exclusion criteria by 8am rule
Legend:
W1: ward 1
W2: ward 2
Include those who are temporarily off the ward for investigations, procedures or on Patient Administration system but at home for a number of hours
Include all patients admitted to the ward before or at (≤) 8:00 AM and not discharged from the ward at the time of the survey

Distribution of PPS coordination activities (estimated % of total patient-days)
13%
5%
12%
9%
11%9%
8%
6%
11%
9%
7%1%
Prepare PPS tools/materials, excl. translation
Recruit/select. hospitals, nat. denom data
Prepare training, excl. translation
Translation
Delivering training course(s)
Helpdesk
Data collection in hosp. by national PPS team
Hospital data entry by national PPS team
Data management/prepare national database
Data quality check, feedback to hospitals
Prepare national data for TESSy and upload
Other
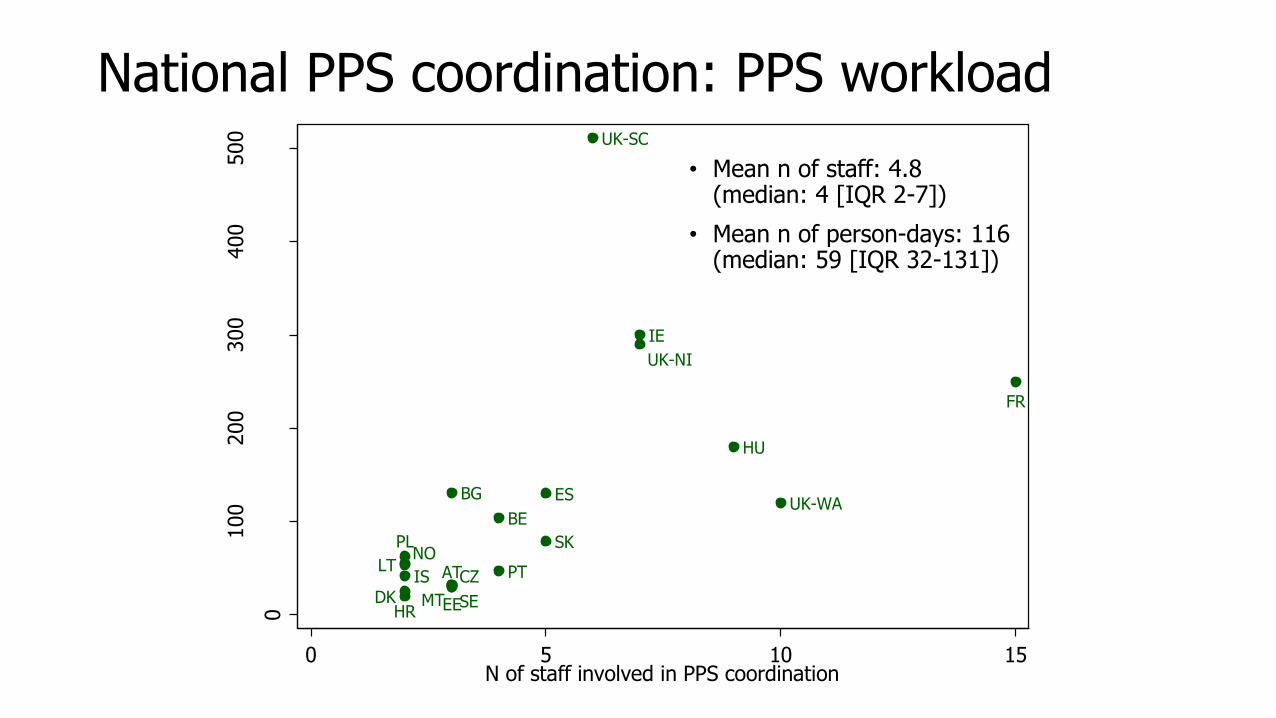
National PPS coordination: PPS workload
AT
BE
BG
CZDK EE
ES
FR
HR
HU
IE
ISLT
MT
NOPL
PT
SE
SK
UK-NI
UK-SC
UK-WA
0
100
200
300
400
500
Est
imate
d n
of
pers
on-d
ays
PPS c
oord
ination
0 5 10 15N of staff involved in PPS coordination
• Mean n of staff: 4.8 (median: 4 [IQR 2-7])
• Mean n of person-days: 116 (median: 59 [IQR 32-131])
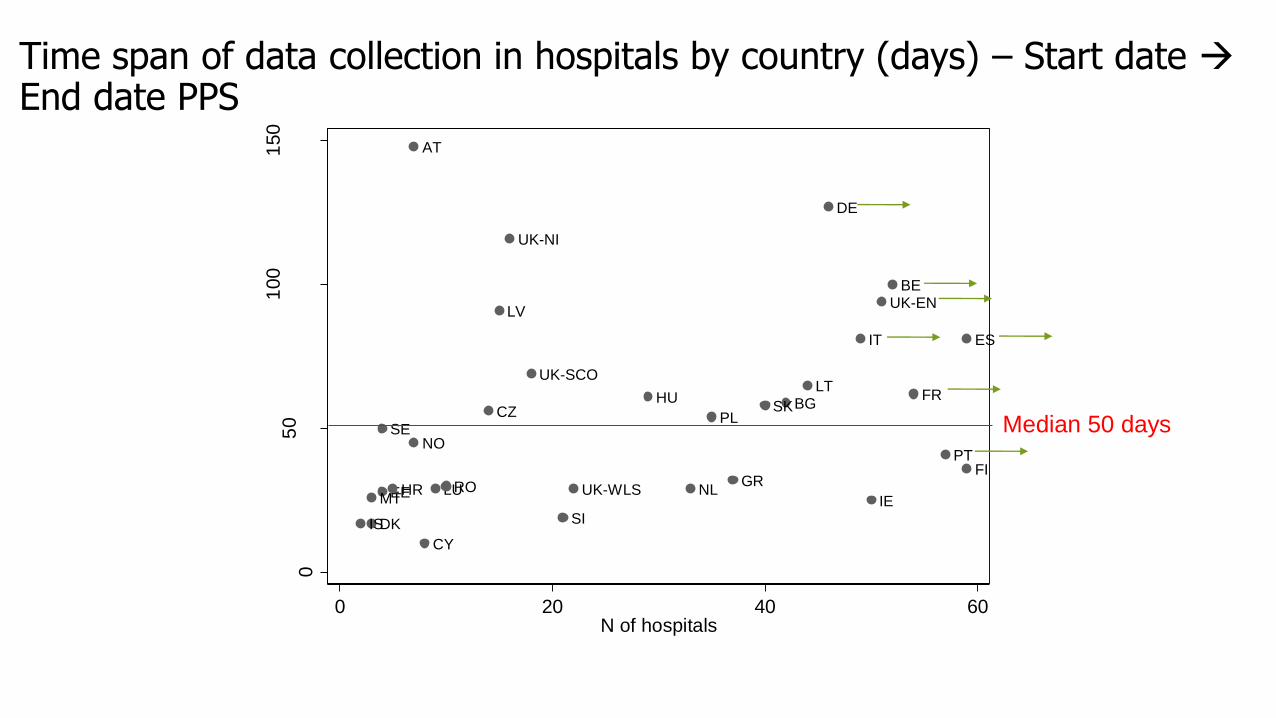
Time span of data collection in hospitals by country (days) – Start date End date PPS
AT
BE
BG
CY
CZ
DE
DK
EE
ES
FI
FR
GRHR
HU
IE
IS
IT
LT
LU
LV
MTNL
NO
PL
PT
RO
SE
SI
SK
UK-EN
UK-NI
UK-SCO
UK-WLS
05
01
00
150
Dura
tion
natio
na
l P
PS
(d
ays)
0 20 40 60N of hospitals
Median 50 days

Data collection days per 100 patients*
02
.75
10
15
20
N o
f da
ys/1
00
patie
nts
ATBE
BGCY
CZDE
DKEE
ENES
FIFR
GRHR
HUIE
ISIT
LTLU
LVMT
NINL
NOPL
PTRO
SCSE
SISK
WA
median
*excluding data entry and checking

European Prevalence Survey of Healthcare-Associated Infections and Antimicrobial Use
Form A. Standard protocol: Patient data, Antimicrobial (AM) use and HAI data
HAI 1 HAI 2
Case definition code
Relevant device (3) O Yes O No O Unknown O Yes O No O Unknown
Present on admission O Yes O No O Yes O No
Date of onset (4) / / / /
Origin of infectionO current hospital O other
hospital O other origin/ unk
O current hospital O other
hospital O other origin/ unk
HAI associated to
current wardO Yes O No O Unknown O Yes O No O Unknown
If BSI: source (5)
MO code
AMR PDR MO code
AMR PDRAM (6) SIR AM (6) SIR
Microorganism 1
Microorganism 2
Microorganism 3
Hospital code [__________] Ward name (abbr.)/Unit Id [__________]
Survey date: ___ / ___ / 20___ (dd/mm/yyyy)
Patient Counter: [_________________________________]
Age in years: [____] yrs; Age if < 2 year old: [_____] months
Sex: M / F Date of hospital admission: ___ / ___ / _____
Consultant/Patient Specialty: [__________]
Surgery since admission:
O No surgery O Minimal invasive/non-NHSN surgery
O NHSN surgery -> specify (optional): [__________] O Unknown
McCabe score:
O Non-fatal disease O Ultimately fatal disease
O Rapidly fatal disease O Unknown
If neonate, birth weight: [______] grams
Central vascular catheter: No Yes Unk
Peripheral vascular catheter: No Yes Unk
Urinary catheter: No Yes Unk
Intubation: No Yes Unk
Patient receives antimicrobial(s)(1): No Yes
Patient has active HAI(2): No Yes
(1) At the time of the survey, except for surgical prophylaxis 24h before 8:00 AM on the day
of the survey; if yes, fill antimicrobial use data; if patient receives >3 antimicrobials, add a
new form; (2) [infection with onset ≥ Day 3, OR SSI criteria met (surgery in previous
30d/90d), OR discharged from acute care hospital <48h ago, OR CDI and discharged from
acute care hospital < 28 days ago OR onset < Day 3 after invasive device/procedure on D1
or D2] AND [HAI case criteria met on survey day OR patient is receiving (any) treatment
for HAI AND case criteria are met between D1 of treatment and survey day]; if yes, fill HAI
data; if patient has > 2 HAIs, add new form.
Patient data (to collect for all patients)
IF YES
dd / mm / yyyy
X
(3) relevant device use before onset infection (intubation for PN, CVC/PVC for BSI, urinary catheter for UTI);
(4) Only for infections not present/active on admission (dd/mm/yyyy); (5) C-CVC, C-PVC, S-PUL, S-UTI, S-DIG,
S-SSI, S-SST, S-OTH, UO, UNK; (6) AB: tested antibiotic(s): STAAUR: OXA+ GLY; Enterococci: GLY;
Enterobacteriaceae: C3G + CAR; PSEAER and Acinetobacter: CAR; SIR: S=sensitive, I=intermediate,
R=resistant, U=unknown; PDR: Pan-drug resistant: N=no, P=possible, C=confirmed, U=Unknown
Antimicrobial
(generic or
brand name)
Ro
ute
Ind
icatio
n
Dia
gn
os
is
(site
)
Reaso
n in
no
tes
Date
sta
rt
AM
Ch
an
ged
?
(+ re
aso
n)
If ch
an
ged
:
Date
sta
rt
1stA
M
Dosage per day
Nu
mb
er
of d
oses
Strength
of 1 dose
mg
/g/IU
/ / / /
/ / / /
/ / / /
Route: P: parenteral, O: oral, R: rectal, I: inhalation; Indication: treatment intention for community (CI), long-
term care (LI) or acute hospital (HI) infection; surgical prophylaxis: SP1: single dose, SP2: one day, SP3: >1
day; MP: medical prophylaxis; O: other; UI: Unknown indication; Diagnosis: see site list, only for CI-LI-HI;
Reason in notes: Y/N; AM Changed? (+ reason): N=no change; E=escalation; D=De-escalation; S=switch IV
to oral; A=adverse effects; OU=changed, other/unknown reason; U=unknown; If changed, date start 1st AM
given for the indication; Dose/day e.g. 3 x 1 g; g=gram, mg=milligram, IU=international units, MU=million IU
Patient-based data (standard)
ALL PATIENTS
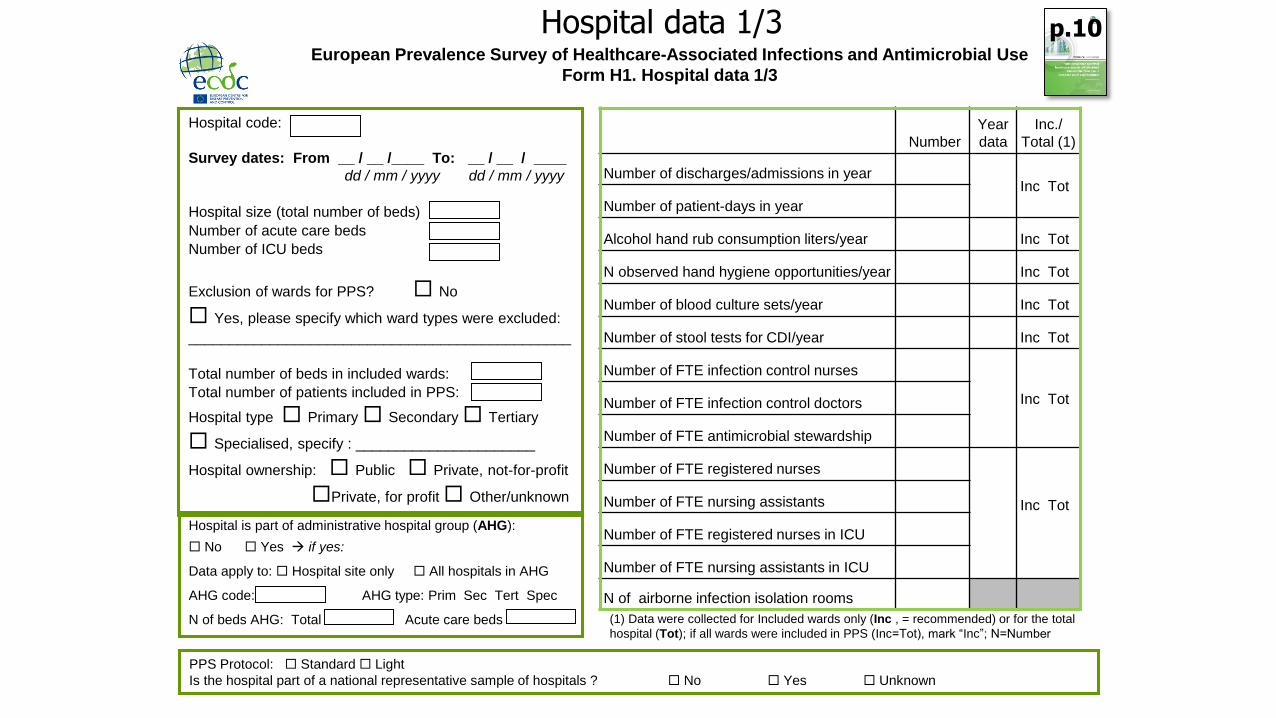
European Prevalence Survey of Healthcare-Associated Infections and Antimicrobial Use
Form H1. Hospital data 1/3
Hospital code:
Survey dates: From __ / __ /____ To: __ / __ / ____
dd / mm / yyyy dd / mm / yyyy
Hospital size (total number of beds)
Number of acute care beds
Number of ICU beds
Exclusion of wards for PPS? No
Yes, please specify which ward types were excluded:
_______________________________________________
Total number of beds in included wards:
Total number of patients included in PPS:
Hospital type Primary Secondary Tertiary
Specialised, specify : ______________________
Hospital ownership: Public Private, not-for-profit
Private, for profit Other/unknown
Number
Year
data
Inc./
Total (1)
Number of discharges/admissions in yearInc Tot
Number of patient-days in year
Alcohol hand rub consumption liters/year Inc Tot
N observed hand hygiene opportunities/year Inc Tot
Number of blood culture sets/year Inc Tot
Number of stool tests for CDI/year Inc Tot
Number of FTE infection control nurses
Inc TotNumber of FTE infection control doctors
Number of FTE antimicrobial stewardship
Number of FTE registered nurses
Inc TotNumber of FTE nursing assistants
Number of FTE registered nurses in ICU
Number of FTE nursing assistants in ICU
N of airborne infection isolation rooms
PPS Protocol: Standard Light
Is the hospital part of a national representative sample of hospitals ? No Yes Unknown
(1) Data were collected for Included wards only (Inc , = recommended) or for the total
hospital (Tot); if all wards were included in PPS (Inc=Tot), mark “Inc”; N=Number
Hospital is part of administrative hospital group (AHG):
No Yes if yes:
Data apply to: Hospital site only All hospitals in AHG
AHG code: AHG type: Prim Sec Tert Spec
N of beds AHG: Total Acute care beds
Hospital data 1/3 p.10





























