Embed Size (px)
DESCRIPTION
Citation preview

Pilot study of a resorbable poly-l-lactide Eustachian Tube stent;
feasibility and tolerability in two animal models
JA Litner M.D., CJ Linstrom M.D.,
P Presti, MD, CA Silverman Ph.D.,
S McCormick M.D.,
GP Yu M.D., J Arigo M.D.

Middle Ear Disease
Susceptibility is clearly multifactorial
Hypoventilation is regarded as the root cause
ET dysfunction is the principal culprit

Background:The Eustachian tube:
*Adam Images and Content under license from adam.com, Inc., © 2002 adam.com, Inc.

Theories of Causality
Eustachian tubes are mechanically obstructedTubal stenosis noted in nearly half of chronic ears1
No significant post-mortem alteration in tube caliber2
Eustachian tubes are functionally obstructedTubal hypercompliance, The Floppy Tube3
Alteration in tubal surface tension dynamics4-8
1Tos M. Journal of Laryngology and Otology 1980;94:25-302Sade et al. American Journal of Otology 1986;7(6)3Bluestone CD. Head and Neck Surgery- Otolaryngology. Ch. 111; 19934Miura M et al. Acta Otolaryngologica. 1996;116:840-445Fornadley JA et al. Otolaryngology- Head and Neck Surgery. 1994;110:110-46Nemechek AJ et al. Otolaryngology- Head and Neck Surgery. 1997;117:475-97Passali D et al. Respiration. 1987;51 supp.1:52-98Sujana S et al. Laryngoscope. 2004:114 ; 472-485

Significance
Most Common Reason For Sick visits to PMD’s for Children <3
5 Billion spent annually1
One Million children undergo myringotomy annually 1
Morbidity associated with MT
Frequent returns to the OR
Over prescription of Abx and rising resistance
No Modality that specifically addresses the underlying pathophysiology: Eustachian Tube Dysfunction
1Gates GA. Otolaryngology Head Neck Surg. 1996;114:525-530
Bluestone CD. Head and Neck Surgery- Otolaryngology. Ch. 111; 1993

Historical Interventions
ET insufflation prior to 19501
Elaborate surgical shunts, ET irradiation in 1960’s2-4
Armstrong tube invented in 19545
―Permanent‖ vent tubes
Silverstein tube6
Jahn Hydroxylvent tube7
1Shapiro SL. Eye Ear Nose and Throat Monthly. 1969;48:72-72Drettner B et al. Archives of Otolaryngology. 1969;90:122-8 3Goode RL et al. Laryngoscope. 1975;85:100-124House WF et al. Laryngoscope. 1969;79:1765-82 5Armstrong BW. Archives of Otolaryngology. 1954;59:653-46Silverstein H. Archives of Otolaryngology. 1970;91:313-87Jahn AF. Otolaryngology- Head and Neck Surgery. 1991;105(5):758-60

Problems with Current Approach
MedicalIncreased antibiotic resistance
SurgicalExtrusion
Scarring/Perforation
Infection
Cholesteatoma
Disruption of graft healing
Failure to alter natural course
About 25% of procedures are repeat

ET Stenting
Wright Jr., 1976 –Silastic Eustachian Tube Prosthesis (SETP)
Series of 138 patients with average 26 month follow-up
80% had an aerated ME behind intact TM after 6 months
Poor results after 6 months
No serious complications
Wright Jr. JW et al. Laryngoscope. 1977;87:207-14
Wright Jr. JW et al. ORL. 1978;86:834-7

Hypothesis
Functional restoration most physiologically sensible approach
ET Stenting should augment function and restore ventilation
Success achievable through advances in biomaterials science & capacity to elute drugs
Successful applications to other hollow viscera1-6
1Korpela A et al. Chest. 1999;115:490-952Tamai H et al. Circulation. 2000;102:399-4043Lumiaho J et al. Journal of Urology. 2000;164:1360-34Middleton JC et al. Medical Plastics and Biomaterials. 1998;March5van Berkel A et al. Gastrointestinal Endoscopy. 2000;51:19-226Sung JJY. Journal of Industrial Microbiology. 1995;15:152-5

Stent Design Issues
Stent Deployment
Stent Retrieval
Indwelling Effects
Perforation
Migration
Occlusion
Extrusion
Ascending infection
Reflux
Autophony/Patulous
symptoms
Longevity

Specific Aims
Aim 1– Explore technical ease
Aim 2– Establish safety profile
Aim 3– Determine tissue response
Aim 4– Assess extent of stent resorption

Stent Prototype
Manufactured by
PPD Méditech
Waterville, QC

Stent Location

Methodology- Study 1
Adult Chinchilla ear model
NYMC Dept. Comp. Med. facility—IACUC approved
Sample size of 5 animals
Baseline tympanograms & otomicroscopy
Stent implanted randomly via transbullar approach
Remaining ear matched control

Methodology
All animals treated with peri-operative systemic antibiotics
Serial testing at 4,6,8,10,14,18,22,26 weeks
Digital otomicro photos taken at each interval
One animal sacrificed at 10, 18, & 26 weeks
Temporal bones sectioned and evaluated blindly by head and neck pathologist
Statistical comparison of between-group differences in ME pressures over time

Results
2 animals died intra-operatively due to respiratory arrest
Follow-up available for 3 animals up to time of sacrifice
One animal developed transient post-operative otorrhea in implanted ear via existing myringotomy incision; resolved with ototopical antibiotics

Test
Ear
Control
Ear
Baseline 4 weeks 12 weeks 26 weeks
Otomicroscopy

Tympanometry
Peak C
om
plian
ce (
daP
a) Test
Ear
Control
Ear
Data Points
Zero Point
-25
22 26-125
-100
-75
-50
0
25
50
75
100
Animal #2, Test ear
Time (weeks)
-50
-100
-75
-50
-25
0
25
50
75 Animal #3, Test ear
Base 4 6 8 10 14 18 22 26-100
-75
-50
-25
0
25
50
75
100
Animal #1, Control ear
Time (weeks)
Peak C
om
plian
ce
(daP
a)
Base 4 6 8 10 14 18 22 26-100
-75
-50
-25
0
25
50
75
100
Animal #1, Test ear
Time (weeks)
Peak C
om
plian
ce
(daP
a)
Base 4 6 8 10 14 18 22 26-125
-100
-75
-50
-25
0
25
50
75
100
Animal #2, Control ear
Time (weeks)
Peak C
om
plian
ce
(daP
a)
Base 4 6 8 10 14 18
Base 4 6 8 10 14 18 22 26-100
-75
-25
0
25
50
75
100
Animal #3, Control ear
Time (weeks)
Peak C
om
plian
ce
(daP
a)
Base 4 6 8 10 14 18 22 26
100
Time (weeks)
Peak C
om
plian
ce
(daP
a)
Peak C
om
plian
ce
(daP
a)

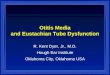
Pathology– Gross

Pathology– Micro
Control Ear
CLP
BO
TVP
N
Original Magnification x 60

Pathology– Micro
Test EarLP
C
B
O
TVP
N
Original Magnification x 60

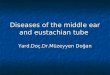
Pathology– Micro
Test Ear
Control Ear
G
G

Pathology– Micro
Test Ear
TZ
C

Stent Resorption

Data Analysis
Number Mean Standard
deviation
Z value† P value
Animal #1
Left 5 6.0 8.2 0.00 >0.05
Right 5 8.0 26.1
Animal #2
Left 9 -11.7 48.5 2.49 0.013
Right 9 -40.6 58.4
Animal #3
Left 7 8.6 22.7 1.89 0.058
Right 7 -17.9 46.4
† Wilcoxon signed ranks test.
Peak Compliance(daPa)

Methodology- Study 2
Adult NZ White Rabbit ear model
NYMC Dept. Comp. Med. facility—IACUC approved
Sample size of 10 animals
Similar study protocol-serial otomicroscopy at 2 week intervals
All animals sacrificed at 6 months

ResultsTest
Animal
Week
1-2
Week
3-4
Week
5-6
Week
7-8
Week
9-10
Week
11-12
Week
13-14
Week
15-16
Week
17 –18
Week
19-20
Week
21 –22
Week
23-24
#1 Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal
#2 OM OM and Facial
Cellulitis
Resolved
OM
Normal Normal Normal Normal Normal Normal Normal Normal Normal
#3 Normal Normal Normal Normal OM OM Normal Normal Normal Normal Normal Normal
#4 Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal
#5 Normal Normal OM Normal Normal Normal Normal Normal Normal Normal Normal Normal
#6 Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal
#7 Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal
#8 OM Resolved Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal
#9 Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal
#10 Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal
Findings on Otomicroscopy in Test Ears

Results
Specimen Implanted Ear Control Ear
1 No Inflammation No Inflammation
2 No Inflammation No Inflammation
3 No Inflammation No Inflammation /
Cholesteatoma
4 No Inflammation No Inflammation
5 No Inflammation No Inflammation
6 No Inflammation No Inflammation
7 No Inflammation No Inflammation
8 No Inflammation No Inflammation
9 No Inflammation No Inflammation
10 No Inflammation No Inflammation
Histologic Findings at 6 months

Results
Transient infections in 4 test ears
No chronic inflammatory response in all test ears after 6-month incubation
No remnants of stents noted at 6 months

Conclusions
Stents were easily implanted
Stents were well tolerated with development of transient otorrhea in few subjects
Stents engendered negligible inflammatory response
Differential resorption- Stents were minimally resorbed at 6 months in the Chinchilla model

Future Directions
Technology merits further testing for efficacy
Determine appropriate sterilization procedures
Clarify resorption spectrum
Explore use of surface agents or drug elution to improve biocompatilibity and reduce biofilm

Acknowledgments
Dr. Ellen Levee, DVM for supervision of animal care
New York Medical College DCM Staff
PPD Meditech, 50 Raymond, Waterville, QC
for manufacture and supply of stent prototypes