Embed Size (px)
Citation preview

ORIGINAL RESEARCH Open Access
Evaluating the effect of emergency departmentcrowding on triage destinationErin O’Connor1, Mathieu Gatien1, Cindy Weir1 and Lisa Calder1,2*
Abstract
Background: Emergency Department (ED) crowding has been studied for the last 20 years, yet many questionsremain about its impact on patient care. In this study, we aimed to determine if ED crowding influenced patienttriage destination and intensity of investigation, as well as rates of unscheduled returns to the ED. We focused onpatients presenting with chest pain or shortness of breath, triaged as high acuity, and who were subsequentlydischarged home.
Methods: This pilot study was a health records review of 500 patients presenting to two urban tertiary care EDswith chest pain or shortness of breath, triaged as high acuity and subsequently discharged home. Data extractedincluded triage time, date, treatment area, time to physician initial assessment, investigations ordered, disposition,and return ED visits within 14 days. We defined ED crowding as ED occupancy greater than 1.5. Data were analyzedusing descriptive statistics and the χ2 and Fisher exact tests.
Results: Over half of the patients, 260/500 (52.0%) presented during conditions of ED crowding. More patientswere triaged to the non-monitored area of the ED during ED crowding (65/260 (25.0%) vs. 39/240 (16.3%) whennot crowded, P = 0.02). During ED crowding, mean time to physician initial assessment was 132.0 minutes in thenon-monitored area vs. 99.1 minutes in the monitored area, P <0.0001. When the ED was not crowded, mean timeto physician initial assessment was 122.3 minutes in the non-monitored area vs. 67 minutes in the monitored area,P = 0.0003. Patients did not return to the ED more often when triaged during ED crowding: 24/260 (9.3%) vs. 29/240(12.1%) when ED was not crowded (P = 0.31). Overall, when triaged to the non-monitored area of the ED, 44/396(11.1%) patients returned, whereas in the monitored area 9/104 (8.7%) patients returned, P = 0.46.
Conclusions: ED crowding conditions appeared to influence triage destination in our ED leading to longer wait timesfor high acuity patients. This did not appear to lead to higher rates of return ED visits amongst discharged patients inthis cohort. Further research is needed to determine whether these delays lead to adverse patient outcomes.
Keywords: Emergency Department crowding; Emergency Department occupancy; High acuity; Overcrowding; Triage
BackgroundEmergency Department (ED) crowding was first identifiedas a problem over 20 years ago [1]. Research has since fo-cused on the effect of ED crowding on adverse patientoutcomes; however, the effect of ED crowding on triagedestination has not been studied. Triage and the assign-ment of the patient to an area of the ED is an importantpart of a patient’s visit to an ED. Triage destination can
greatly influence the course of the patient’s visit, includingtime to assessment, extent of workup, and length of stayin the ED [2]. Assignment of a triage score, and subse-quent placement in an non-monitored (less acute) vs.monitored (more acute) area of the ED affects physicianthinking and decision making about the patient’s pres-entation [3,4].ED crowding is a concern with regard to patient safety,
as it has been associated with adverse patient outcomesincluding increased patient mortality, delayed resuscita-tion efforts, increased adverse events, delayed antibioticadministration in patients with pneumonia, and in-creased in-hospital length of stay [5-10]. ED crowding
* Correspondence: [email protected] of Emergency Medicine, University of Ottawa, 1053 CarlingAvenue, Ottawa, ON K1Y 4E9, Canada2Clinical Epidemiology Program, Ottawa Hospital Research Institute, TheOttawa Hospital, Civic Campus, Rm F658, 1053 Carling Ave., Ottawa, ON K1Y4E9, Canada
© 2014 O’Connor et al.; licensee Springer. This is an Open Access article distributed under the terms of the Creative CommonsAttribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproductionin any medium, provided the original work is properly credited.
O’Connor et al. International Journal of Emergency Medicine 2014, 7:16http://www.intjem.com/content/7/1/16

has also been related to poor management of pain anddecrease in patient satisfaction [11-13].We present a pilot study of patients presenting with
chest pain or shortness of breath, triaged as high acuity,and who were discharged home on the index visit. Ourobjectives were to determine whether: 1) patients weretriaged to non-monitored areas of the ED more fre-quently during ED crowding; 2) patients were assessedby a physician more quickly in non-monitored ratherthan monitored areas during crowded conditions; 3) pa-tients triaged to the non-monitored area received thesame laboratory and imaging tests as those triaged tomonitored areas; 4) patients triaged during ED crowdingreceived the same laboratory and imaging tests as thosetriaged during non-crowded conditions; 5) the propor-tion of return ED visits was higher for patients triagedduring ED crowding; and 6) the proportion of return EDvisits was higher for patients triaged to the non-monitoredarea during crowded conditions.
MethodsStudy design and settingWe conducted a health records review of patients pre-senting to two ED campuses of a large urban tertiarycare Canadian academic teaching hospital, each with ap-proximately 75,000 patient visits per year. We usedInternational Classification of Diseases 10 codes to iden-tify patient visits corresponding with chief complaints ofchest pain or shortness of breath for the period betweenJanuary 1st and December 31st 2010. A total number of4,234 patient visits were identified. Using an Internet-basedrandom number generator (http://www.randomizer.org),we selected a sample of health records, with an overallgoal of 500 eligible visits. The Ottawa Hospital ResearchEthics Board approved this study.
Subjects and data collectionWe included patients older than 18, who presented witha chief complaint of either chest pain or shortness ofbreath, were assigned a Canadian Triage and Acuity Scale(CTAS) score of 2, and were discharged home on theindex visit [14]. CTAS is a five-category triage system de-signed to allow Canadian EDs to prioritize patients basedon their presenting complaint and the severity of theirsigns and symptoms. Triage nurses who have receivedtraining assign CTAS scores based on a published set ofguidelines [14]. CTAS scores are determined by present-ing complaint, with severity modifiers based on vital signs,past medical history, and brief history of the complaint[15]. Included in the CTAS score assignment system isnursing discretion, allowing for a higher CTAS score tobe assigned based on the judgment of the triage nurse.In our hospital there are guidelines for destination
based on CTAS score, but there is allowance for triagenurse discretion in assignment of patient destination. ACTAS score of 2 (Emergent) is assigned to conditionsthat are a potential threat to life limb or function and itis recommended that patients be seen by a physicianwithin 15 minutes 95% of the time [14,16]. We excludedpatients if they were admitted to the hospital on theindex visit. Patients were not excluded if they presentedmore than once. We divided the patients into cohortsby geographic destination in our department. Non-monitored patients were those who were assigned to theleast acute area of our department. Monitored patientswere those triaged to the most acute areas of our de-partment and were placed on continuous cardiac andrespiratory monitoring.A single reviewer (EO) who was not blinded to the study
hypothesis abstracted data onto a standardized MicrosoftExcel spreadsheet. Data were obtained from the electronichealth record, which contained scanned handwritten nurs-ing triage notes and physician notes as well as computer-ized laboratory and imaging results. We recorded thefollowing variables: triage time and date, triage score, tri-age destination, time of initial physician assessment, inves-tigations ordered, and referrals made. We also recordedwhether a patient’s destination changed during the EDvisit. Up-triage was defined as a patient moved from thenon-monitored area to the monitored area. Down-triagewas defined as moving from the monitored area to thenon-monitored area. Change in triage destination wasmade at the discretion of the bedside nurse or treatingphysician and could occur at any time during the patient’sstay in the ED. We do not have protocols in our ED forup-triage based on time to initial physician assessment.
Study outcome measuresStudy outcomes included: triage destination during EDcrowding conditions, time to physician assessment (thetime from patient arrival to assessment by a physician,in minutes), investigations ordered, and unscheduled returnto our institution within 14 days of the index visit.
ED crowding measureED crowding was measured using ED occupancy at thetime of patient triage, which was defined as the ratio oftotal number of patients in the ED (admitted and notadmitted) to the number of beds in the ED [17]. For ourdepartment, we included numbers of beds in all areas ofthe ED, monitored and non-monitored. ED occupancy isan accepted measure of ED crowding, but there is nouniversally accepted threshold that defines ED crowding[18,19]. We determined, based on local expert consensus,that an ED occupancy score of greater than 1.5 wouldindicate that our ED was crowded.
O’Connor et al. International Journal of Emergency Medicine 2014, 7:16 Page 2 of 7http://www.intjem.com/content/7/1/16

Sample size and statistical analysisA rate of return to our ED in this cohort of patients wasassumed to be 20% (based on previous studies in our de-partment) [20]. A difference in return rates of 10% wasdeemed significant, resulting in a sample size of 588. Inthis pilot study, the sample size of 500 charts was chosenfor convenience. Descriptive statistics were used to reportpatient and system characteristics. Univariate analysis wasperformed with the χ2 test for all dichotomous variables.The Fisher exact test was used to analyze nominal vari-ables and continuous variables were analyzed with theWilcoxon two-sample test.
ResultsStudy flowWe found 568 eligible health records during the studyperiod; 7 visits were excluded for a CTAS score otherthan 2 and 61 charts were excluded based on chief com-plaint. Finally, we included a total of 500 health recordsin our study (Figure 1).
Patient and system characteristicsOver half of the patients were male. Chest pain was themost common chief complaint. Approximately half of
the included patients were triaged during crowded condi-tions. Most of the patients were triaged to the monitoredarea (Table 1).
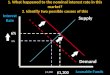
Triage decision making and time to initial physicianassessmentWe found that patients who presented with a chief com-plaint of chest pain or shortness of breath and wereassigned a CTAS score of 2 were triaged to the non-monitored area of the ED significantly more often whenthe ED was crowded (25.0% vs. 16.3%, P = 0.02) (Figure 2).The mean time to physician initial assessment was sig-
nificantly longer for those patients triaged when the EDwas crowded (107.3 minutes vs. 76.0 minutes, P <0.0001)(Figure 3a). The mean time to physician initial assessmentwas significantly longer in the non-monitored area of theED than in the monitored area (Figure 3b). This wasfound to be true both when the ED was crowded (132.0minutes vs. 99.1 minutes, P <0.0001) and when it wasnon-crowded (122.3 minutes vs. 67.0 minutes, P = 0.0003).Patients were not up-triaged more often from the
non-monitored area to a more acute area of the depart-ment when the ED was crowded than when the ED wasnon-crowded (3.1% (n = 8) vs. 1.3% (n = 3), P = 0.42).
ED crowding and geographical influence oninvestigations orderedED crowding did not appear to influence the proportionof patients who received ED investigations with the ex-ception of more chest computed tomography orderedwhen the ED was not crowded (9.2% vs. 5.4%, P = 0.01)(Figure 4).Data not depicted in the figures shows that investiga-
tions were influenced by the patient’s geographic location
Figure 1 Study flow diagram.
Table 1 Patient and system characteristics for 500 highacuity patients presenting with chest pain or shortness ofbreath
Patient characteristics n (%)
Male 269 (53.8)
Presenting complaint
Chest pain 392 (78.4)
Shortness of breath 108 (21.6)
System characteristics n (%)
ED crowding status1 at time of triage
Crowded 260 (52.0)
Non-crowded 240 (48.0)
Triaged ED location
Non-monitored 104 (20.8)
Monitored 396 (79.2)1ED Occupancy = Number of patients in the ED/Number of beds in the ED.Crowded is defined as an ED Occupancy >1.5.
O’Connor et al. International Journal of Emergency Medicine 2014, 7:16 Page 3 of 7http://www.intjem.com/content/7/1/16

in the ED, with more investigations ordered in the moni-tored area of the ED: complete blood count: 99.2% vs.67.31%, P <0.0001; electrolytes: 99.4% vs. 64.4%, P <0.0001;blood urea nitrogen: 99.2% vs. 66.4%, P <0.0001; venousor arterial blood gas: 6.6% vs. 1.0%, P = 0.03). Exceptionsto this were significantly fewer electrocardiograms (86.5%vs. 95.5%, P = 0.0009) and D-dimers (26.0% vs. 16.4%,P = 0.03) ordered in the monitored area. We found no sig-nificant difference in the number of chest radiographs(P = 0.61) and chest computed tomography scans (P = 0.52)ordered. More patients received a referral to another ser-vice, either as an inpatient or as an outpatient from themonitored area (51/396 (12.8%) vs. non-monitored 1/104(1%) P <0.0001).
Proportion of return visits to the EDOverall, rates of unscheduled returns to our ED werelower than anticipated: 51/500 (10.2%). We did not finda significant association between ED crowding and theproportion of patients who had an unscheduled returnto the ED within 14 days of the index visit (9.3% vs.12.1%, P = 0.31) (Figure 5a). In addition, the difference ingeographic ED location (non-monitored vs. monitored)was not significantly associated with an increase in theproportion of patients with an unscheduled return tothe ED (11.1% vs. 8.7%, P = 0.46) (Figure 5b).
DiscussionUnderstanding how ED crowding affects patient out-comes has been identified as a research priority in emer-gency medicine [21]. Assignment of a triage score anddestination in the emergency department has an import-ant impact on the course of a patient’s ED visit [4]. Wepostulated that the negative impact of ED crowding withregard to increased patient mortality, increased adverseevents, and delayed antibiotic administration in patientswith pneumonia reported in previous studies may be re-lated to differences in triage practices during times ofcrowding [5-10]. We hypothesized that patients wouldbe triaged more often to the non-monitored or lessacute area of our ED when the ED was crowded. Wetheorized that the patients in the non-monitored areawould have fewer investigations and the physicians’ per-ception of the severity of their illness would be nega-tively impacted [4]. We found that high acuity patientswere triaged to the non-monitored area of the ED moreoften when they presented during crowded conditions.This change in triage destination during crowded condi-tions may be based on an assumption by the triage nurs-ing staff that patients would be seen more quickly by aphysician if they are not required to wait for a moni-tored bed. This group of patients also received less bloodwork and fewer imaging tests than those sent to themonitored or more acute area of our ED. The differ-ences in investigations and imaging tests ordered forthese patients is potentially based on the physician’s per-ception of lower acuity of presentation because the pa-tient is in the non-monitored area of the ED. A few ofthe differences were unexpected, in particular the factthat fewer ECGs were ordered in the monitored area ofthe ED. It is possible that because the patients were oncontinuous cardiac monitors that 12 lead ECGs werenot obtained. Another possible explanation for this isthat ECGs performed on these patients were lost and notscanned in to the computer record from which we ob-tained our data. We speculate that more D-dimers wereordered in the non-monitored area of the ED because it isused more as a “rule-out” test. For patients perceived tobe more ill, a CT scan may have been ordered to
0
20
40
60
80
100
Crowded Non-Crowded
Pro
port
ion
of P
atie
nts
(%)
16.3%25.5%
p=0.02
Figure 2 Proportion of patients triaged to the non-monitoredarea during crowded and non-crowded conditions (n = 500).
(a)
(b)
0
20
40
60
80
100
120
Crowded Non-crowded
p<0.0001
Mea
n ti
me
to p
hysc
ian
asse
ssm
ent
(min
utes
)
t = 107.3
t = 76.0
0
20
40
60
80
100
120
140
Crowded Non-Crowded
Non-Monitored
Monitored
Mea
n ti
me
to p
hysi
cian
ass
essm
ent
(min
utes
)
t = 67.0
t = 122.3
t = 99.1
t = 132.0
p=0.0003
p<0.0001
Figure 3 Mean time from triage to physician initial assessmentduring crowded and non-crowded conditions (n = 500). (a) Overall.(b) Divided by non-monitored and monitored areas.
O’Connor et al. International Journal of Emergency Medicine 2014, 7:16 Page 4 of 7http://www.intjem.com/content/7/1/16

investigate pulmonary embolism with a D-dimer omittedfrom the work-up. Overall, ED crowding led to morehigh-acuity patients being triaged to the non-monitoredarea of our ED, with fewer investigations performed.We did not find that ED crowding conditions resulted
in an increase in return visits to the ED within 14 daysfor patients presenting with chest pain or shortness ofbreath and assigned a CTAS score of 2. Given that weexperienced overall rates of return that were lower thananticipated, our study may be underpowered to detect atrue difference. This finding is consistent, however, withprevious research by Hu et al., which found no correl-ation between unscheduled return visits to the ED andED crowding [22]. We did show an increase in time tophysician initial assessment for patients triaged duringcrowding conditions. A previous study by Guttman et al.showed a positive correlation between increased waitingtimes and admission to hospital or death within 7 daysfor discharged patients [23].We used ED occupancy rate as our measure of ED
crowding because it is a parsimonious, valid measurement
of ED crowding. ED occupancy rate has been shown toperform as well as the following markers of ED crowding:EDWIN score, patients left without being seen and ambu-lance diversion times [16]. ED occupancy has the advan-tage of being calculable for the time of patient triagerather than as an average over the course of a day andhence may offer increased precision. In this pilot study,we attempted to specifically examine the effect of EDcrowding on triage destination; therefore, a crowdingmeasure specific for the time of triage was felt to be themost useful. In future work in this area we would measurecrowding using the EDWIN score, ambulance diversionrates, and rates of left without being seen as well as usingED occupancy.There are several limitations to this study. Firstly, it
was restricted to a single institution that encompassestwo large tertiary care EDs and we were only able to de-tect return visits to our institution and not to other in-stitutions in our area. Previous studies conducted at ourcenter indicate that patients rarely return to other insti-tutions after an index visit to our ED [20]. Our sample
(a)
(b)
0102030405060708090
100
CBC Electrolytes BUN CK/TnI VBG/ABG D-Dimer
Crowded
Non-crowdedP
ropo
rtio
nof
Pat
ient
s (%
)
p=0.20 p=0.29 p=0.45p=0.53
p=0.23p=0.07
91.2% 94.2% 90.8% 93.3% 91.6% 93.3%86.1% 84.2%
4.3% 6.7%15.4%
21.7%
0
20
40
60
80
100
CXR CT Chest ECG
Crowded
Non-crowded
p=0.08p=0.81
Pro
port
ion
ofP
atie
nts
(%)
91.5 95.4
5.4%9.2%
93.9 93.3
p=0.01
Figure 4 Investigations ordered for high acuity ED patients triaged either to the non-monitored or monitored areas of the ED, presentingwith chest pain or with shortness of breath. (a) Blood-work ordered. (b) Imaging and ECGs ordered. [CBC, Complete Blood Count; BUN, BloodUrea Nitrogen; CK, Creatinine Kinase; TnI, Troponin I; VBG, Venous Blood Gas; ABG, Arterial Blood Gas; CXR, Chest Radiograph; CT Chest, ChestComputed Tomography; ECG, Electrocardiogram].
O’Connor et al. International Journal of Emergency Medicine 2014, 7:16 Page 5 of 7http://www.intjem.com/content/7/1/16

size was relatively small, with only 500 health records in-cluded. Previous studies at our institution estimated arate of return in this cohort of 20% [20]. However, in thegroup of patients we studied our rate of return was10.2%, meaning that our study was under-powered. Weset a cut-off for ED crowding at an occupancy level of1.5 – this may be too low to capture the times when ourdepartment was under the most stress. The cut-off wasbased on local expert consensus rather than literature-based, as there is no accepted threshold for ED crowdingusing ED occupancy in the literature. It is possible that ahigher ED occupancy level would show a larger differ-ence between the groups. Also, ED occupancy was cal-culated at the time of triage, reflecting only occupancyat that one time. Change in occupancy level throughoutthe patients’ stay in the ED may also have affected theinvestigations ordered and potentially the rate of returnto the ED. Due to the retrospective nature of the studydesign, we were unable to determine if CTAS scoreswere appropriately assigned for the patients in the study.Previous literature suggests that assignment of CTASscore has a good inter-rater reliability [24,25]. However,it is possible that ED crowding influenced assignment ofCTAS score. This study was based on the assumptionthat patients with the same chief complaint and the
same CTAS score have the same level of acuity and the-oretically then need the same amount of monitoring andinvestigation, which may not be true.This is the only study so far to examine the impact of
ED crowding on triage destination. A larger, multi-center study would be necessary to determine whetherchanges in triage destination have a negative impact onpatient outcomes. As triage is the first point of contactwith ED staff, this interaction influences the patient’s en-tire stay in the department and should be an importantarea for future ED crowding research.
ConclusionsIn this pilot study, we found that during crowded condi-tions, high acuity patients presenting with chest pain orshortness of breath had a higher rate of triage to thenon-monitored area of the ED, longer times to physicianinitial assessment, and an associated lower rate of inves-tigations. Despite these findings, with our small samplesize we could not detect a difference in rates of unsched-uled returns to our institution. Future research shouldbe directed at examining whether these changes in triagedestination during crowded conditions lead to worse pa-tient outcomes.
(a)
(b)
02468
101214161820
Crowded Non-crowded
Pro
port
ion
ofP
atie
nts
(%)
p=0.31
9.3%
12.1%
0
5
10
15
20
Monitored Non-monitored
Pro
port
ion
ofP
atie
nts
(%)
p=0.46
8.7%11.1%
Figure 5 Proportion of patients who return to the ED within 14 days of index visit. (a) Patients triaged during crowded or non-crowdedconditions. (b) Returns to the ED by initial triage destination.
O’Connor et al. International Journal of Emergency Medicine 2014, 7:16 Page 6 of 7http://www.intjem.com/content/7/1/16

AbbreviationsCTAS: Canadian Triage and Acuity Scale; ED: Emergency Department.
Competing interestsThe authors declare that they have no competing interests.
Authors’ contributionsEO conceived of the study, gathered data, and drafted the manuscript. MGrevised the manuscript. CW gathered data and revised the manuscript. LCsupervised development of the study design and coordination and revisedthe manuscript. All authors read and approved the final manuscript.
AcknowledgementsThe study was supported by a research grant from the Department ofEmergency Medicine, University of Ottawa. We thank Rina Marcantonio foridentification of health records, Angela Marcantonio for help withsubmission to the research ethics board and grant application, CherylGeymonat for help in obtaining data, Guy Hebert and Adam Cwinn for theirhelp in determining an ED occupancy cut-off, Tinghua Zhang for statisticalanalysis, and Ben Kenney for technical support with the database.
Received: 4 November 2013 Accepted: 4 April 2014Published: 28 April 2014
References1. Dickinson G: Emergency department overcrowding. CMAJ 1989,
140(3):270–271.2. Yoon P, Steiner I, Reinhardt G: Analysis of factors influencing length of
stay in the emergency department. CJEM 2003, 5(3):155–161.3. FitzGerald G, Jelinek GA, Scott D, Gerdtz MF: Emergency department triage
revisited. Emerg Med J 2010, 27(2):86–92.4. Croskerry P: The importance of cognitive errors in diagnosis and
strategies to minimize them. Acad Med 2003, 78(8):775–780.5. Richardson DB: Increase in patient mortality at 10 days associated with
emergency department overcrowding. Med J Aust 2006, 184(5):213–216.6. Hong KJ, Do SS, Song KJ, Cha WC, Cho JS: Association between ED
crowding and delay in resuscitation effort. Am J Emerg Med 2013,31(3):509–515.
7. Pines JM, Pollack CV, Diercks DB, Chang AM, Shofer FS, Hollander JE: Theassociation between emergency department crowding and adversecardiovascular outcomes in patients with chest pain. Acad Emerg Med2009, 16(7):617–625.
8. Pines JM, Hollander JE, Localio AR, Metlay JP: The association betweenemergency department crowding and hospital performance onantibiotic timing for pneumonia and percutaneous intervention formyocardial infarction. Acad Emerg Med 2006, 13(8):873–878.
9. Fee C, Weber EJ, Maak CA, Bacchetti P: Effect of emergency departmentcrowding on time to antibiotics in patients admitted withcommunity-acquired pneumonia. Ann Emerg Med 2007, 50(5):501–509.
10. Ackroyd-Stolarz S, Read Guernsey J, Mackinnon NJ, Kovacs G: Theassociation between a prolonged stay in the emergency departmentand adverse events in older patients admitted to hospital: aretrospective cohort study. BMJ Qual Saf 2011, 20(7):564–569.
11. Hwang U, Richardson LD, Sonuyi TO, Morrison RS: The effect of emergencydepartment crowding on the management of pain in older adults withhip fracture. J Am Geriatr Soc 2006, 54(2):270–275.
12. Pines JM, Hollander JE: Emergency department crowding is associatedwith poor care for patients with severe pain. Ann Emerg Med 2008,51(1):1–5.
13. Pines JM, Iyer S, Disbot M, Hollander JE, Shofer FS, Datner EM: The effect ofemergency department crowding on patient satisfaction for admittedpatients. Acad Emerg Med 2008, 15(9):825–831.
14. Bullard M, Unger B, Spence J, Grafstein E: Revisions to the CanadianEmergency Department Triage and Acuity Scale (CTAS) adult guidelines.CJEM 2008, 10(2):136–142.
15. Beveridge R, Ducharme J, Janes L, Beaulieu S, Walter S: Reliability of theCanadian emergency department triage and acuity scale: interrateragreement. Ann Emerg Med 1999, 34(2):155–159.
16. Beveridge R, Clarke B, Janes L, Savage N, Thompson J, Dodd G, Murray M,Nijssen-Jordan C, Warren D, Vadeboncoeur A: Canadian Emergency
Department Triage and Acuity Implementation Guidelines. CJEM 1999,1(3 suppl):S2–S28.
17. McCarthy ML, Aronsky D, Jones ID, Miner JR, Band RA, Baren JM, Desmond JS,Baumlin KM, Ding R, Shesser R: The emergency department occupancy rate:a simple measure of emergency department crowding? Ann Emerg Med2008, 51(1):15–24.
18. Moskop JC, Sklar DP, Geiderman JM, Schears RM, Bookman KJ: Emergencydepartment crowding, part 1–concept, causes, and moral consequences.Ann Emerg Med 2009, 53(5):605–611.
19. Ospina MB, Bond K, Schull M, Innes G, Blitz S, Rowe BH: Key indicators ofovercrowding in Canadian emergency departments: a Delphi study.CJEM 2007, 9(5):339–346.
20. Calder L, Tierney S, Jiang Y, Gagné A, Gee A, Hobden E, Vaillancourt C, Perry J,Stiell I, Forster A: Patient safety analysis of the ED care of patients with heartfailure and COPD exacerbations: a multicenter prospective cohort study.Am J Emerg Med 2014, 32(1):29–35.
21. Asplin BR, Magid DJ, Rhodes KV, Solberg LI, Lurie N, Camargo CA: Aconceptual model of emergency department crowding. Ann Emerg Med2003, 42(2):173–180.
22. Hu K-W, Lu Y-H, Lin H-J, Guo H-R, Foo N-P: Unscheduled return visits withand without admission post emergency department discharge. J EmergMed 2012, 43(6):1110–1118.
23. Guttmann A, Schull MJ, Vermeulen MJ, Stukel TA: Association betweenwaiting times and short term mortality and hospital admission afterdeparture from emergency department: population based cohort studyfrom Ontario. Canada. BMJ 2011, 342:d2983.
24. Fernandes CMB, Mcleod S, Krause J, Shah A, Jewell J, Smith B, Rollins L:Reliability of the Canadian Triage and Acuity Scale: interrater andintrarater agreement from a community and an academic emergencydepartment. CJEM 2013, 15(4):227–232.
25. Manos D, Petrie D, Beveridge R: Inter-observer agreement using theCanadian Emergency Department Triage and Acuity Scale. CJEM 2002,4(1):16–22.
doi:10.1186/1865-1380-7-16Cite this article as: O’Connor et al.: Evaluating the effect of emergencydepartment crowding on triage destination. International Journal ofEmergency Medicine 2014 7:16.
Submit your manuscript to a journal and benefi t from:
7 Convenient online submission
7 Rigorous peer review
7 Immediate publication on acceptance
7 Open access: articles freely available online
7 High visibility within the fi eld
7 Retaining the copyright to your article
Submit your next manuscript at 7 springeropen.com
O’Connor et al. International Journal of Emergency Medicine 2014, 7:16 Page 7 of 7http://www.intjem.com/content/7/1/16