Embed Size (px)
Citation preview

Evaluation and Management of Urethral Diverticula
Howard B. Goldman, MDSection of Female Pelvic Medicine and Reconstructive Surgery
Glickman Urologic and Kidney Institute
The Cleveland Clinic
Lerner College of Medicine
Case Western Reserve University

• 32 yo woman referred for cystocele
• No pain
• No voiding complaints
• Has noticed a vaginal bulge for 6 months
• G1P1 - vaginal


urethra

Urethral Diverticulum
• Defect in the periurethral fascia with an outpouching of mucosa– Infection within periurethral glands– Obstruction and abscess formation– Rupture into urethral lumen
outpouchings
• Typically located dorsally and laterally
• Most common in 3rd to 5th decades of life

Presentation
• “Dysuria, Dyspareunia and Dribbling”• Recurrent UTIs• Urethral pain, pelvic pain, vag wall tenderness• Purulent drainage per urethra• Overactive bladder complaints: urgency,
frequency, incontinence
• Romanzi et al. (J Urol, 2000): diverse presentations, mimics other disorders

Evaluation
• History and physical exam• Careful palpation of distal anterior vaginal wall
– Milk the urethra and observe meatus
• Cystoscopy• Radiographic evaluation
– Voiding cystourethrography (VCUG)– Ultrasonography (transvaginal, endourethral)– MRI
• ? Urodynamics - fluoro– Evaluate for stress urinary incontinence

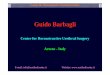
VCUG• Radiographic study of choice for years• Voiding and post-void views important
– Many patients cannot void on the table
• Blander et al. (Urology 2001): MRI and VCUG– VCUG missed 7% of diverticula and underestimated size and
complexity

VCUG
tic

Ultrasonography
• Transvaginal, endoluminal
• Relatively inexpensive, good visualization
• Operator dependant
• Siegel et al.: VCUG vs ultrasound. 13/15 diverticula detected with both modalities, but US showed extent and location better

Urethral diverticulum - UStransurethral
tic
neck

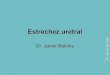
CT vs MRI

Urethral diverticulumaxial MRI

Urethral Diverticuli• Management:
– Conservative treatment measures: antibiotics, anticholinergics, anesthetics, etc..
• Acutely or for very small tics
– Operative• Spence procedure
– Very distal diverticulum
• Excision
• SUI considerations

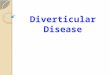
Prepare Vaginal Wall Flap

Inicise Periurethral Fascial
Tic

Prepare Periurethral Fascial Flaps
Periurethral fascia flaps

Dissect Out and Excise Tic

Identify Ostium

Close Ostium

Closure of Dead Space

Periurethral Fascial Defect Closure

Close with Vaginal Wall Flap
*Avoid overlapping suture lines

• 32 yo woman referred for cystocele
• No pain
• No voiding complaints
• Has noticed a vaginal bulge for 6 months
• G1P1 - vaginal




urethra



Urethral diverticulumaxial MRI -saggital

Urethral diverticulumaxial MRI - saggital




ostium

Martius flap

Management of Stress Incontinence
• Faerber et al: simultaneous diverticulectomy and sling, no complications, no erosions, no SUI
• Vasavada et al: 5 diverticulectomies, xenograft tissue for sling, no erosions, no SUI
• Some controversy over whether to place sling at time of diverticulectomy – if place – never use synthetic mesh

Postoperative management
• Urethral catheter for 14 days• VCUG??• complications:
– stress incontinence (de novo)– urethrovaginal fistula– recurrence
– Evaluate path specimen

4/5 (80%) with Invasive adenoca had history of urinary retention

Long Term f/u of Diverticulum Recurrence
• N=122 50 month avg f/u
• 10.7% had surgery for recurrence– Risk factors
• Proximal diverticulum
• Multiple diverticula
• Prior vaginal or urethral surgery
• 26% persistent pain/discomfort with voiding
• 39% UTI in prior yearIngber et al, J Urol, 2011

Conclusions
• Diagnosis of urethral diverticula may be difficult• High index of suspicion• MRI is the gold standard for evaluation of suspect
diverticula• Surgery is the mainstay of therapy• Careful exposure of all layers allows proper
reconstruction• Majority successfully treated