Embed Size (px)
Citation preview

SELECTED TOPICS IN EMERGENCY CARDIAC CARE 0733-8627/98 $8.00 + .OO
EVALUATION AND RISK STRATIFICATION OF PATIENTS
WITH CHEST PAIN IN THE EMERGENCY DEPARTMENT
Predictors of Life-Threatening Events
Robert J. Zalenski, MD, MA, Falah Shamsa, PhD, and Karla Jayne Pede, BS
While assessing a patient with chest pain consistent with acute myocardial infarction (AMI) or unstable angina, the emergency physi- cian must first estimate the patient’s probability of acute cardiac ischemia (ACI), a term that refers collectively to the spectrum of acute ischemic states. This first estimate of the short-term probability of ACI is inferred from the history, physical examination, and electrocardiogram (ECG). In some settings, an initial CK-MB test is also Patients who meet the physician and hospital’s threshold for ACI are further evaluated in the hospital to confirm or exclude this diagnosis, while other life-threat- ening diagnoses are excluded.64
To manage patients safely, the emergency physician must then make a second, different decision regarding the site of further testing and monitoring. The risk of life-threatening events determines the intensity of monitoring needed during diagnostic testing and thus the site of
From the Department of Emergency Medicine (RJZ, FS), the Division of Cardiology, Department of Medicine (RJZ), and the Center for Healthcare Effectiveness Research (FS), Wayne State University School of Medicine; the Section of Urgent Care, Depart- ment of Medicine (RJZ), John D. Dinghell Veterans Hospital, Detroit, Michigan; and the College of Medicine, University of Saskatchewan, Saskatoon (KJP), Saskatche- wan, Canada
EMERGENCY MEDICINE CLINICS OF NORTH AMERICA
VOLUME 16 * NUMBER 3 * AUGUST 1998 495

496 ZALENSKI et al
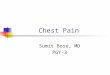
further medical care. Each of the potentially available choices, the coro- nary care unit (CCU), the intermediate care unit, the emergency depart- ment (ED) chest pain observation unit (CPOU), the hospital ward, or the outpatient setting, has its specific level of intensity, cost, and benefit. Appropriate patient selection requires a second, critical estimate: the probability of a short-term life-threatening event. This probability is the key variable for determining the necessary level of care.8, l8 This estimate must be used to match the availability of intensive, expensive resources appropriately (e.g., one-to-one nursing care) to the patients most likely to need them. Because admission to the CCU is widely viewed as conferring a 15% survival advantage on patients (with cardiac arrest), making the correct decision about disposition is important.56 Figure 1 depicts the pathway the emergency physician should take in making these decisions.
The CCU should be reserved for patients at higher risk for life- threatening events, the intermediate care unit for patients at lower risk for events but at higher probability for ACI;15717,65 the ED CPOU for patients at low risk (for events and ACI (but not low enough to be discharged,17, 46, 63, 65 and a timely community-based evaluation in the outpatient setting, for patients who are at low risk in the short term but at higher risk for cardiac events over the following 1 to 24 months.34, 58
The wide spectrum of settings for the evaluation of ACI has evolved only over the last 10 years. Intermediate care units and ED-based CPOUs are part of these developments and of the trend to increase the specificity of treatment and to decrease hospital use and the cost of care.17, 46, 63, 65
Utilization rates from the Multicenter Chest Pain Study (MCPS) show an astounding reversal of CCU and telemetry use.18 From 1984 to 1986, in a large sample of patients studied with acute chest pain (derivation set), 18% were admitted to intermediate care and 78% to the CCU. In the period from 1990 to 1994, in another set of patients studied (valida- tion set), 84% were admitted to intermediate care and 16% to the CCU.lS During these same two comparison periods, the "rule in" AM1 rate for the CCU increased from 31% to 50% and for intermediate care from 4% to 31% (p<O.OOl).'* The shift away from using intensive settings for monitoring patients is in further evidence in the recommendations made 1994 by the prestigious National Institutes of Health and endorsed by the American College of Emergency Physicians: that low-risk patients with symptoms of unstable angina should be evaluated in the outpa- tient setting6
To manage patients safely in this new paradigm, the emergency physician must understand that the risk of complications determines the intensity of monitoring needed during diagnostic testing6, l8 Appropri- ately matching a patient's risk to the intensity of service is the solution that reconciles the conflicting priorities with every practicing emergency physician is familiar: minimizing the inappropriate discharge of patients with ACI while maximizing the cost-effectiveness of hospital-based care. Missed AM1 is the leading cause of settlement costs because of malprac- tice in the ED settine; in addition, the high estimated mortality rate

PATIENTS WITH CHEST PAIN IN THE EMERGENCY DEPARTMENT 497
Yes b
Patient presents at triage with chest pain consistent with CAD
AdmittoCCU
Yes I
Yes b AdmittoCCU
yes
low-moderate risk EM 12 hour unit
or IM 23 hour unit
No 1 Yes Routine
follow-up cardiac events?
Expedited outpatient work-up with cardiologist
Figure 1. The pathway shows that the physician should first assess whether the acute symptoms are consistent with coronary artery disease. If so, then he should next determine if the patient is at high risk for life threatening events and, if so, admit the patient to the CCU. The next step directs the physician to admit to intermediate care or the emergency medicine observation unit if the patient is at risk of acute cardiac ischemia (ACI), but at lower risk of complications. Finally, if the patient is at low enough risk of ACI to be discharged but at higher risk of long-term cardiac events, an expedited work-up with a specialist is indicated. A typical example would be a patient with a history of CAD with heart failure who is judged stable enough for discharge from the emergency department.

498 ZALENSKI et a1
(25%) of the 2% to 4% of patients inappropriately discharged with AM1 is cause for concern.37, 42 Perhaps because of this concern there has been an excess of monitoring of chest pain patients in the CCU who are found to be nonischemic and who received no measurable benefit. This has driven the numerous attempts to achieve more cost-effective risk strati- fication.6, 17, 36, 46, 63 Achieving cost-effectiveness and high sensitivity for ACI, in fact, can occur only by using less expensive settings for the workup of ACI, such as the ED-based CPOU.17,50 This allows a reduction in the cost of care that partly or wholly offsets the cost of achieving the priority of carefully examining and testing patients who are at low risk
The focus of this article is the prediction of life-threatening events with ED measurements. These events include malignant arrythmias (e.g., ventricular fibrillation, tachycardia, and high-grade atrioventricular [AV] block), pump failure (e.g., cardiogenic shock and congestive heart fail- ure), cardiac arrest, and death. The ED measures include the history, physical examination, ECG, and their combinations. The authors also examine the prognostic value of newer cardiac markers and imaging tests. In a final section, we extend the risk stratification to patients who are at longer-term risk of cardiac death from 1 month to 2 years postdischarge. Such patients are commonly discharged from the ICU.
of ~ ~ 1 . 6 5
PREVALENCE OF LIFE-THREATENING CARDIAC EVENTS
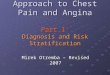
There are multiple large studies available to estimate the rate (or point prevalence) of short-term events. The best estimate comes from the Multicenter Chest Pain Study (MCPS), which examined 10,682 en- rolled ED patients for major events within 72 hours of enrollment.'* Major events were defined as malignant arrhythmias, cardiogenic shock or pump failure requiring intubation, cardiac arrest, or recurrent ische- mia requiring revascularization. The overall complication rate was 4.5%, the overall AM1 rate 15%, and the overall ACI rate was 31%. Thus, the cardiac event rates are much lower than the ACI rate. Figure 2 displays complication rates by site of care and final diagnosis. Most complications occurred in the CCU and in patients who had a final diagnosis of AMI. In a large single-ED study of 4,690 admitted patients, Karlson found that 18% died or suffered serious complication^.^^ The rates for the different types of complications were ventricular fibrillation (l?'~), third- degree AV block YO), treated ventricular tachycardia (VT, 2%), hypoten- sion requiring inotropics (3%), and severe congestive heart failure (12%). The in-hospital mortality rate was 5.2%.
Another report from the MCPS emphasizes that patients with an exacerbation of coronary artery disease (CAD) are a high-risk group.61 For in-hospital mortality, patients with an exacerbation of CAD and AM1 had a 9% rate compared with 5% for patients with first AM1 ( p < 0.01). Patients with unstable angina had a low in-hospital mortality rate

PATIENTS WITH CHEST PAIN IN THE EMERGENCY DEPARTMENT 499
c E Q
Q 2 n
25 fl I
20
15
10
5
0 Home/ward ccu UA Noncard
lntermed AM1 Othr card
Figure 2. The Multicenter Chest Pain Study (MCPS) provides data showing that cardiac event rates for patients discharged home were near zero, while the CCU had the highest proportion of events with a 10% event rate. Most events occur in patients with a final diagnosis of AM1 or unstable angina (the composite is termed ACI); however, because it is difficult to predict this diagnosis initially, and most cases of ACI have no events, and other diagnoses also have cardiac events, emergency department predictors of cardiac events rather than AM1 are needed. N = 10,682 emergency department patients.
(0.2%-0.3%), regardless of prior CAD history.61 Over a mean of 2.3 years follow-up, postdischarge cardiovascular survival was significantly better in patients with new-onset ischemic heart disease ( p < 0.05) and on multivariate analysis had a relative risk of 0.47% (95% confidence inter- val [CI] 0.23-0.97) of deaths. Patients without cardiovascular disease had a uniformly excellent short- and long-term prognosis.38
RELATIONSHIP OF THE DIAGNOSIS AND PROGNOSIS OF ACI
Estimating the likelihood of short-term, life-threatening events is more accurate when based not simply on a surrogate variable, the patient’s risk of ACI, but on other clinical and baseline variables.18, 32
Although the outcomes of the diagnosis of ACI and its prognosis are closely related, their independent predictors are different.8, 18, 32, 33, 67 In the AHCPR/NIH unstable angina guideline, separate estimates of the likelihood of CAD and of its complications were developed.6 Addition- ally, even within the subgroup of ED patients found to have AMI, significant ED predictors of prognosis have been delineated.4, 8, 53, 67 Al- though the risk of AM1 is part of assessing the risk of complications,6. l6
other factors include whether pain is present, the initial ECG, physical examination findings, and survival likelihood should an ischemic event occur.6 Multiple studies have shown that neither the degree of suspicion of AMI, its final diagnosis, nor initial ECG gives the best prediction, but

500 ZALENSKI et a1
rather a multivariate model that includes these and other ED presenting features.ls, 32
STATISTICAL METHODS
These authors conducted a review of the literature from 1967 to 1997 to examine reports that studied the ED predictors of the probability of life-threatening events during a short-term follow-up period (either hospital stay or 30 days from index evaluation). When such data were not available, we examined data from non-ED settings to answer this question. (Predictors of the likelihood of ACI is a different issue and has been extensively analyzed el~ewhere.~~) When available, actual use of the predictive rule in practice was examined and its clinical impact as~essed.~', 59, 6o A second issue addressed is the longer-term (2- to 24- month) prediction of cardiac events (e.g., death, revascularization, recur- rent AMI) in patients who are discharged to the community from the ED.
The primary statistics used in the studies included in this review, on univariate analysis, are odds ratios, relative risks, likelihood ratios, and their 95% CIS. Multivariate analyses used recursive partitioning or logistic regression models. When time to complication was the outcome predicted, Kaplan-Meier survival analysis and multivariate Cox propor- tional hazard techniques were used.'"
Several cautions are in order regarding the application of the pre- dictive variables or models to clinical practice. First, unlike diagnostic accuracy studies or double-blind trials of therapeutic agents, prognostic studies are hybrid types, employing diagnostic test findings to predict patient outcomes. These prognostic data often are poorly controlled for confounding effects. For example, data used to predict the need for intensive care often include outcomes from patients treated in the inten- sive care setting. These outcomes might not be the same had the patients been treated in a non-CCU setting, or if the prevalence of disease in the study sample is different from the proposed site of appli~ation.~~ Such studies must be validated in the ED prior to conclusions of value in patient care.51, 59,
Additionally, findings from other settings, such as the CCU or outpatient clinics cannot be directly generalized to the ED setting. A good example of this comes from data from the Framingham Study. Cardiac risk factors such as hyperten~ion~~ identified in a community were found to be predictive of AM1 over the long-term (14 years) but were falsely concluded to be important predictors for the short-term diagnosis of AM1 in the ED. A careful examination of this relationship showed this to be an error.3o Decisions made on such "pseudodiagnostic" information persist, however.20
Other relevant issues are the adequacy of model selection, its good- ness of fit, and the approaches taken to achieve the best model for a certain set of predictive factors for a particular data set. Studies do not commonly examine the full range of statistical inferences based on the

PATIENTS WITH CHEST PAIN IN THE EMERGENCY DEPARTMENT 501
type of model chosen. Variables were used in linear models but could also have been used in nonlinear or polynomial fashion to express a multiplicative or interaction effects. Had predictors been modeled on these appropriate strategies, the scientists may have reached additional inferences or conclusions. For example, multivariate logistic model3* and then applied a Cox hazard modeP3 under similar circumstances to pre- dict the same outcomes without elaborating on the statistical justifica- tions or testing the underlying assumptions corresponding to the models chosen. Furthermore, application of new statistical approaches should pay more attention to guarding against possible violations of statistical theory. Goldman et a1 did not elaborate on the problem of multiple comparisons caused by repeated statistical testings over various times on a cohort of patients.18
PREDICTIVE FACTORS
History and Physical Examination Factors
The MCPS identified pain that is worse than previous angina or the same as a prior MI as an independent predictor of early life-threatening complications.18 This single variable captures two separate predictor variables: patients with a history of ischemic heart disease, a known prognostic factor:' and patients with a very high likelihood of AM1 (worst angina or history like previous AMI).19 It also found two physical examination variables, systolic BP less than 110 mm Hg and bilateral rales above the bases, to be independent predictors of complications. A study by Karlson et a1 (discussed more fully below) found that degree of suspicion of AMI, age, history of CHF or diabetes mellitus, and active CHF or arrhythmias were predictive of severe complications or mortality. 32
Other historical variables were identified in a prospective "valida- tion" study of the Braunwald unstable angina classifi~ation.~ In 393 admitted patients with unstable angina (patients with AM1 were ex- cluded), six clinical factors predicted major cardiac events: death, AMI, congestive heart failure, cardiogenic shock, ventricular fibrillation (VF), or tachycardia, on multivariate analysis. These factors included 1) a history of AM1 within 14 days (odds ratio [OR] 5.72, p=0.002); 2) intravenous nitroglycerin administration (OR = 2.3, p = 0.005); 3 ) no treatment with a beta blocker or calcium channel blocker (OR = 3.8, p=O.OOl); 4) ST segment depression on baseline ECG (OR2.8, p=0.003); 5 ) diabetes mellitus (OR 2.2, p=0.006); and 6 ) age in increments by decade (OR = 1.5, p = 0.002). Intravenous nitrate use may be a surrogate marker for active and continuing pain. Active pain and recurrent ische- mic pain has been found to be a high-risk prognostic indicator in multiple ~tudies.'~, l8 In a study by Fesmire and Wears, ED patients with persistent or recurrent versus resolved pain had a 3.8 times higher rate of life-threatening complications ( p = 0.04).14 It should be noted that the study of the Braunwald classification was not a prospective test of its

502 ZALENSKI et a1
use, so that the classification cannot be recommended for routine use, because prospective validations of triage goals in conditions of actual use must precede widespread implementati~n.~~, 59, 6o
Electrocardiographic Features
The value of the initial ECG in the ED for the prediction of life- threatening in-hospital events has been extensively analyzed?, 12, 13, 53, %, 67
Most commonly, the ECG is dichotomized as positive or negative based on the presence or absence of any of the following: (1) ST segment depression or elevation of 0.1 mv, (2) T wave inversion (more negative than isoelectric), (3) new or presumed new Q waves, (4) left bundle branch block, and (5) paced rhythm. These observational studies have usually been of patients admitted to the hospital, primarily the CCU. The endpoint of these studies is a composite variable of life-threatening events, including malignant arrhythmias, cardiogenic shock, congestive heart failure, and death. In a large, prospective, single-hospital study of events, Karlson et a1 found that patients with a normal ECG had a death rate of 1%, and a life-threatening event rate 3%.32 The rate of events by ECG category is depicted in Figure 3.32 As can be seen, ST-segment elevation was associated with the highest mortality and complication rate, followed by Q waves, ST depression, and T-wave inversion. This
Figure 3. The study shows that findings of injury, necrosis, and ischemia have the highest mortality and complication rates during the hospital course. Note that T-wave inversion and a normal ECG have lower mortality rates. N=4690 hospitalized patients. Solid bar = mortality; open bar = complications. (Dafa from Karlson BW, Hallgren HP, Liliequist JA, et al: Emergency room prediction of mortality and severe complication in patients with sus- pected acute myocardial infarction. Eur Heart J 15:1558-1565, 1994.)

PATIENTS WITH CHEST PAIN IN THE EMERGENCY DEPARTMENT 503
comparison shows that the more severe patterns of injury, necrosis, and ischemia are associated with higher rates of cardiac events.
In a prospective study by Yusuf et al, 475 ED patients with suspected uncomplicated AM1 who were admitted to the CCU as a substudy of a trial of beta blockers.62 Patients with complications were excluded at baseline. ED ECGs were read blindly to classify patients as showing ST elevation (n = 306), ischemia or bundle branch block (n = 111) or normal (n=58) and were obtained at a mean of 5 hours from symptom onset. There were no differences at baseline in the three groups for history of AMI, CAD, heart rate, or blood pressure, but the normal ECG patients were 3 to 4 years younger and fewer of them had diabetes mellitus (5% vs. 0%). No patient with a normal ECG suffered cardiac arrest or died during the hospital stay compared with 11% in the group with ST- segment elevation (p<O.OOl). These differences persisted on 4-year fol- low-up study. The ED ECG was found to be an independent predictor of risk. This article was the first to provide empiric data to support a recommendation for non-CCU admission for low risk patients.62
In a prospective observation study of 469 ED patients with sus- pected AM1 who were admitted to the CCU, Brush et a1 examined the initial ECG for its predictive value for subsequent the life-threatening event and ECG classifications, as defined above.* On univariate analysis, patients with a positive ECG had a 14% (42/302) rate of at least one life- threatening event compared with 0.6% of 167 patients with a negative ECG. Life-threatening events were 23 times more likely if ECG were positive (p<O.OOl), whereas the risk of AM1 was only four times higher (p<O.OOl). Even when the diagnosis of AM1 is controlled for, complica- tions occurred in 25% of the group with positive ECGs but in only 4% of the group with negative ECGs. This suggests that the initial ECG is more strongly associated with life-threatening events than is the diagno- sis of AMI.8
Zalenski et a1 confirmed Brush's findings in a retrospective study of 211 ED patients admitted to the CCU for the same outcomes.67 In the 115 patients with a negative ECG, the rate of life-threatening complica- tions was 0% compared with 14.6% in the 96 patients with a positive ECG (p<O.OOl). The respective AM1 rates for positive versus negative ECGs was 11.3% versus 47.9%. Because several of the negative ECG patients received intravenous nitroglycerin, which is usually adminis- tered in the CCU, the authors suggested that patients with ongoing typical cardiac pain should be admitted to the CCU, even though their risk of complication is In a retrospective study of 775 ED patients admitted to the CCU, the initial ECGs were classified as normal (14%, n = 107), nonspecific ST-T changes YO, n = 73), and abnormal (73%, n = 595).53 ECG subgroups were examined for serious complications of infarction extension, cardiac arrest, sustained hypotension, VF or tachy- cardia, second- or third-degree heart block, Killip class 3, or death. Complication rates were 49'0, 11%, and 25% for the normal, nonspecific, and abnormal ECG groups, respectively (p = O.OOOl), and in-hospital death rates were O%, 1%, and 6%, respectively (p<0.02). The odds of

504 ZALENSKI et a1
death were 11.2 for positive-ECG group and the odds of AM1 were 6.7, suggesting that the ECG is more strongly associated with prognostic than diagnostic
In a case-control study of AM1 patients by Zalenski et al, 27 patients with a negative ECG and 35 patients with a positive ECG had a nonsta- tistically significant 12% difference in the complication rates, which was smaller than expected.66 The study’s results emphasized the importance of surveillance for ECG changes because ECG evolution most always preceded cardiac events when the initial ECG is nondiagnostic. The subgroup of patients with a negative ECG with no evolution had no events (95% CI, o%--33%).66 This is concordant with a study by Fesmire et a1 that found that patients with a changed ECG had a higher complica- tion rate than patients whose ECG was static.I2
The importance of left ventricular hypertrophy (LVH) was clarified in a secondary analysis of ECG data from a multicenter study of 5,355 ED patients. Larsen et a1 examined the short-term mortality rates for 413 (8%) patients with LVH on the ECG compared to primary ST-T findings, other abnormalities, and a normal ECG.35 The mortality rate for patients with LVH was 7.5%, significantly higher than that of patients with normal ECGs (1.1% mortality) and not significantly lower than the mortality rate of patients with primary ST-T abnormalities. Despite the much lower rate of ACI in cases with LVH versus primary ST-T changes (26.4% vs. 71.8%, respectively), patients with LVH had comparable mor- tality rates. The authors appropriately recommended selective admission to the CCU of patients with LVH despite their significantly lower rate of ACI. The study did not examine the role of ECG findings in a multivariate model, so that the question of the independent predictive value of LVH on the ECG was not addressed.
COMPUTER PROTOCOLS
A computer-based protocol consists of multivariate modeling per- formed on large data sets that examine several baseline variables or symptoms to predict an outcome of interest. Among the most commonly used models are recursive partitioning and logistic regression models. This section examines the application of these models.
The largest and most comprehensive study of patients with chest pain and cardiac events was reported by Goldman et a1 in 1996.lS This study consisted of derivation and validation sets of 10,682 and 4,676 patients. Major cardiac events were defined as arrhythmias (e.g., VF, cardiac arrest, new complete heart block, temporary pacing, emergent cardioversion), pump failure (e.g., cardiogenic shock, intra-aortic balloon pumping), or ischemia (recurrent pain requiring CABG or PTCA within 72 hours or prior to discharge). Using recursive partitioning analysis, patients were assigned to high-, moderate-, low-, or very low-risk catego- ries according two ECG variables, two physical examination variables, and one historical variable. The variables consisted of ST elevation or Q waves in two contiguous leads suggestive of AMI, ST-segment, or T-

PATIENTS WITH CHEST PAIN IN THE EMERGENCY DEPARTMENT 505
wave changes not known to be old, pain worse than prior angina or same as old MI, systolic blood pressure <110 mm Hg, and rales above the bases bilaterally. Using the algorithm reproduced in Figure 4, pa- tients can be classified a high (16.1%), moderate (7.8%), low (3.9%), or very low (0.6%) risk of major complications over the first 24 hours of care (figures from the derivation set).
After the first 12-hour period, the probability of a cardiac event in the subsequent 12- to 24-hour periods is markedly increased by the occurrence of any major or intermediate events in the preceding period.
Suspected MI on ECG
No
t Yes
Suspected ischemia
\ No
I High Risk I
t yT\ I
No risk One risk Two or more No or one Two or more factors factor risk factors risk factor risk factors
\
t t \ t risk
Figure 4. Derivation of the four initial risk groups (high, moderate, low, and very low) for cardiac events on the basis of data available at the time of presentation in the emergency department. MI is suspected if the ECG shows ST-segment elevation of at least 0.1 mV or pathological Q waves in two or more leads not known to be old. Ischemia is present if the ECG shows ST-segment depression of at least 0.1 mV or T-wave inversion in two or more leads not known to be old. Risk factors are any of the following: systolic blood pressure ~ 1 1 0 mm Hg., rales above the bases bilaterally, and known unstable ischemic heart disease, defined as worsening of previously stable angina, new onset of post-infarction angina or angina after a coronary-revascularization procedure, or pain that was the same as associated with a prior AMI. Reading the ECG and counting risk factors enables the emergency physician to assign risk classes which have a significantly different probability of complications in the first 12 hours (p<O.OOI). (From Goldman L, Cook EF, Johnson PA, et al: Prediction of the need for intensive care in patients who come to emergency departments with acute chest pain. N Engl J Med 334:1498-504, 1996; with permission.)

506 ZALENSKI et a1
Intermediate events included Mobitz type I or I1 block (provided not requiring treatment), atrial flutter, pulmonary edema without hypoten- sion, infarct extension, and pulmonary embolus. Major events with their absolute and adjusted risks are found in Table 1. It shows, for example, that the occurrence of documented MI in the first 12 hours raises the relative risk of a subsequent event by 6.8 in the derivation set and 11.1 in the validation set. This means that optimal risk stratification starts with presenting features in the ED, and then updates risk at 12, 24, 48, and 72 hours based on occurrences of any major or intermediate events. Patients at low risk for AM1 and complications during the first 12 hours of monitoring are able to be discharged safely provided they are not at high risk for ACI. These criteria make intuitive sense because they use the risk of AM1 initially or subsequently as a predictor plus the risk of pump failure as indicated by lower blood pressure or more than bibasilar rales.
Karlson et a1 used logistic regression techniques in a study of 4,690 ED patients hospitalized in the CCU or intermediate care wards for chest pain or other symptoms suggestive of AMI. These patients were followed for the outcomes of mortality, malignant arrhythmias, severe CHF, hypotension, AV block, or paced brady~ardia.~~ In patients seen in the ED and then hospitalized, the prevalence of AM1 was 20%, mortality 5%, and nonfatal complications was 16%. The independent predictors of hospital mortality were ST elevation on ED ECG, age, degree of suspi- cion of AMI, history of diabetes mellitus, arrhythmia on admission, history of CHF, acute ischemia on ECG, non-chest pain symptoms, and syncope. The authors provide a logistic regression equation that can be
Table 1. RELATIVE RISK OF A SUBSEQUENT MAJOR EVENT MORE THAN 12 HOURS AFTER PRESENTATION*
Prior Event
Major event Documented MI but no major
or intermediate event Intermediate event but no
major event or documented MI
intermediate event but no major event
Documented MI or
Subsequent Major Event-Relative Risk (95% C.l.)t
Unadjusted Analysis Adjusted Analysist
Derivation Set Validation Set Derivation Set Validation Set
68.9 (58.4-81.2) 55.0 (43.1-72.4) 18.9 (13.9-25.6) 26.5 (18-39.2) 12.2 (9.2-16.3) 13.4 (9.3-19.4) 4.0 (2.7-5.9) 5.6 (3.2-9.7)
14.6 (11.3-18.9) 29.2 (22.1-38.4) 7.7 (5.7-10.4) 18.0 (13.3-24.4)
16.5 (13.4-20.4) 21.2 (16.3-27.5) 6.8 (5.3-8.7) 11.1 (8.1-15.3)
'According to the prior event. tData shown are relative risks for each group as compared with patients without prior major or
intermediate events of documented myocardial infarction (MI). *Analysis was adjusted for stratification of the data according to the level of risk at the time of
presentation. CI = confidence interval. From Goldman L, Cook EF, Johnson PA, et al: Prediction of the need for intensive care in patients
who come to emergency departments with acute chest pain. N Engl J Med 334:1498-1504, 1996; with permission.

PATIENTS WITH CHEST PAIN IN THE EMERGENCY DEPARTMENT 507
used to calculate the exact probability of death for any patient. The model improves on a prediction of death using the suspicion of AM1 alone, as can be seen by the following comparison. The 64% of patients with a vague (symptoms atypical and ECG without ischemia) and no suspicion of AM1 disease had a 2.4% probability of death. Based on results from the fitted model, the 64% of patients with the lowest risk had a probability of death of only 1.2%. This finding suggests that the logistic model predicts better than the initial suspicion of AM1 based on symptoms and ECG.
CARDIAC ENZYMES AND BIOMARKERS
The previous sections have used variables that are universally avail- able in the ED and can even be used in the prehospital setting. New cardiac markers are another type of potential predictor that may improve on previous risk stratification efforts in the ED. Although most studies have tended to examine their univariate predictive value, the recent work of Hamm et a122 evaluates the information provided by the tropo- nins to the information contained in the ECG and creatine kinase-MB fraction (CK-MB).
The emergence of monoclonal antibody testing has enabled the rapid, accurate, and relatively inexpensive performance of a host of promising markers. The ones examined here are the mass assay of CK- MB, and the examination of the cardiospecific epitopes of the troponins. CK isoenzymes consist of three species of dimers composed of two possible subunits: MM, MB, and BB. CK-MM is primarily found in skeletal muscle, CK-BB in brain, and CK-MB in myocard i~m.~~ To in- crease the specificity of elevated CK-MB levels, an index is generated that is a ratio of CK-MB to total creatinine phosphokinase (or CPK). An elevation above 2.5 to 3.0 is the most commonly selected diagnostic level. Serial measures typically indicated a rise about 8 hours after symptom onset and fall after 24 hours as an essential feature of the diagnosis of AMI. The units of measurement are ng/mL. The troponin proteins are located on the thin filament of the contractile apparatus that is 22,000 D. There are three subunits, cardiac troponin T (cTnT), cardiac troponin I (cTnI), and troponin C. Antibodies to the specific isoforms of cardiac-specific cTnT and cTnI have been developed. Both quantitative and qualitative assays, which permit point-of-care testing, are available.52 This section examines the prognostic value of these markers in ED and CCU patients.
In one of the largest prospective multicenter-ED studies investigat- ing the prognostic value of CK-MB, Hoekstra et a1 enrolled 5,120 patients with chest pain without ST-segment elevation on the initial ED ECG and measured CK-MB on presentation and at 2 Ischemic events recorded were heart failure, cardiogenic shock, ventricular arrhythmias, new conduction defects, cardiac death, and recurrent AMI. The relative risk of an ischemic complication was 16.1 (95% CI, 11.0-23.6) for those with a positive versus negative ED CK-MB. The relative risk of death

508 ZALENSKI et a1
was 25.4 (95% CI, 10.8-60.2). The authors concluded that CK-MB testing is helpful in early risk stratification from the ED. This confirmed the results of preliminary work reported by Hedges et al.24 Subsequent reports have shown that the prognostic value of cTnT and cTnI is superior to CK-MB, however.
Ohman and colleagues studied 855 patients with acute ischemic heart disease (abnormal ECGs within 12 hours of symptoms) for the comparative utility of initial cardiac cTnT and CK-MB levels, and these were compared with the value of initial ECG findings.& The measured outcome, death, is not subject to observer bias, and the biochemical and electrocardiographic measurements were made at a blinded core laboratory. ECG classifications were similar to the Brush criteria; a posi- tive cTnT cutoff was 0.1 ng/mL and CK-MB was 7.0 ng/ml. An elevated cTnT was found to predict mortality at 30 days (11.9% vs. 3.9%, p<O.OOl). For our study of risk stratification, there are even two more interesting findings. Although ST segment displacement and paced rhythm each were associated separately with mortality, within these categories cTnT also selected high-risk patients. Even when the normal or elevated CK- MB level is stratified, cTnT selected higher-risk patients for mortality, meaning that the biochemical assessment by cTnT independently con- tributed to prognostic information provided by ECG and CK-MB.
In a study of the 1404 TIM1 IIIB patients with unstable angina or non-Q-wave infarction who presented within 24 hours of pain onset, findings concordant with the GUSTO study were present: cardiac cTnI, with a cutoff value of 0.4 ng/mL, was associated with an increased risk of mortality at 42 days even when one controls for the ECG finding of ST-segment depression, age, and other baseline characteristics.' More- over, cTnI discriminated those at higher risk even when CK-MB was negative. This finding suggests that this assay has an added value even beyond what is contributed by CKMB.
In a study by de Winter et al, ED patients at a short-stay facility with nomore than 12 hours from onset of pain who did not have AM1 were followed for 6 months for cardiac death, AMI, and revasculariz- ati0ns.I' On multivariate Cox proportional hazard analysis, documented history of CAD (by coronary angiography or a previous MI or positive exercise test), was the best predictor with a relative risk of 3.9 (95% CI, 1.2-11.3). CTnT had a relative risk of 2.8 (95 pc CI, 1.0-7.9; and myoglo- bin was 1.0, CK-MB was 0.9. There was a 19% event rate, and overall sensitivity of the markers was 33% (8/24) for cTnT, 21% (5/24) for myoglobin, and 17% (4/24) for CK-MB. The sensitivity for early (<8 days) events was 15% (2/14) for myoglobin, 23% (3/13) for CK-MB, and 46% (6/13) for cTnT. At 12 and 16 hours after symptom onset, 90% and 100% of cTnT tests were positive, respectively.
Brogan et a1 examined the prognostic value of cTnI for 171 unse- lected ED patients presenting with symptoms consistent with cardiac i~chemia.~ For those who presented within 6 hours of symptom onset and had elevated CK-MB or cTnI levels (1.4 ng/mL), there was an increased risk for cardiovascular events and/or interventions (CK-MB

PATIENTS WITH CHEST PAIN IN THE EMERGENCY DEPARTMENT 509
OR 5.8; 95% CI, 2.0-16.9) or cTnI OR 6.3 95% CI, 2.2-17.7);9 however, the article does not report sensitivity or the data needed to calculate it. At 9 hours from symptom onset, however, cTnI had only a 71% sensitivity for AMI.
In a multicenter study by Ravkilde involving 127 CCU patients with suspected but unconfirmed AMI, TnT measurements were determined in a blinded fashion, and this cohort was followed for 6 months to determine the rates of cardiac death and nonfatal AMI.45 In the subgroup with elevated TnT levels, 14% (6/44) had the composite outcome, com- pared with 4% (3/83) without TnT elevations (p=0.025). In an older study, Hamm et a1 demonstrated that in 84 hospitalized patients with acute rest angina (Braunwald class 111), the subgroup (33 or 39%) with elevated cTnT (<0.2 ng/mL) had a higher rate of in-hospital (nonpres- enting) infarctions (30 vs. 2%, p<O.OOl) and in-hospital deaths (15 vs 2%, ~ < 0 . 0 3 ) . ~ ~ In 84% of the patients with TnT elevations, the patients were positive in the first or second sample. In this patient group with known unstable angina, TnT may indicate a group needing intensive care.17
Hamm et a1 conducted a prospective study of the prognostic value for cTnT and cTnI in 773 patients with acute chest pain for less than 12 hours without ST-segment elevation on their presenting ECG.22 Testing was performed shortly after presentation and repeated 4 to 6 hours later so that all patients had a test performed 6 hours after symptom onset. Patients were followed for 30 days for the endpoints of cardiac death and nonfatal, recurrent (after 24 hours) AMI. The 773 patients had a final diagnosis of AM1 in 6%, unstable angina in 43%, stable angina in l6%, pulmonary embolism in 2%, heart failure in 2%, myocarditis in 1%; 33% had no evidence of CAD. Of 47 patients with AMI, 94% had a positive cTnT and 100% a positive cTnI during the ED testing; of 315 patients with unstable angina, 22% had a positive cTnT, 36% had a positive cTnI, and 5% a positive CK-MB. There were 34 cardiac events. CTnI had a sensitivity of 94% and cTnT of 79.4% for outcome events. The negative predictive value of cTnI was 99.7% and of cTnT was 98.9%. As shown in Table 2, a positive cTnI had an odds ratio of 55.1 for a cardiac event even after adjusting for ST-segment depression. The odds ratio of a positive CK-MB after adjustment for ST-segment depression was only 3.4. This study is the strongest to date suggesting that two measurements of cTnI after at least 6 hours of chest pain onset can discriminate cardiac events at 30-day follow-up. If replicated in other ED settings, it may prove to be the most important prognostic tool. One has reasons to be cautious, however, because a single center study in a non-US population will require further validation.
ED TESTING WITH SESTAMlBl
Technetium-99m-labeled sestamibi is a myocardial perfusion tracer and is taken up by the myocardium in proportion to regional blood flow. The myocardial distribution of the agent can be imaged with a standard gamma counter for up to 4 hours after injection of this radioiso-

510 ZALENSKI et a1
Table 2. RELATIVE VALUE OF SERUM MARKERS AND ECG ABNORMALITIES AS PREDICTORS OF CARDIAC EVENTS AT 30 DAYS
Predictor No. of Odds Ratio P
Patients (95% CI) Value
Troponin T' Troponin I* Creatinine kinase MB* ST-segment depression T-wave inversion Troponin T after ST-segment depressiont Troponin I after ST-segment depressiont Creatine kinase MB after ST-segment
Troponin T after creatine kinase MB Troponin I after creatine kinase MB
depression*
123 25.8 (9.6-48.6)
40 3.5 (1.4-8.9) 171 61.4 (14.9-511.7)
158 2.9 (1.47-5.9) 197 0.4 (0.1-1.1)
20.0 (8.6-46.4) 55.1 (14.2-467.3) 3.4 (1 3-8.5)
15.6 (6.5-37.5) 52.4 (12.8-285.6)
<0.001 <0.001
0.008 0.003 0.07
<0.001 <0.001
0.01
<0.001 <0.001
'Values over the analytic cutoff points are as follows: troponin T, 20.18 ng/m; troponin I, 20.10
tOdds ratios are as calculated when the EGG data were forced into the model first. CI = confidence interval. From Hamm CW, Goldman BU, Heeschen C, et al: Emergency room triage of patients with acute
chest pain by means of rapid testing for cardiac troponin T or troponin I. N Eng J Med 337:1648-1653, 1997; with permission.
ng/m; creatine kinase MB, >4.7 ng/mL.
tope, making its use feasible in the ED. Single-photon emission com- puted tomography (SPECT) can be performed to detect perfusion de- fects, and gating (synchronizing images) with the ECG permits the detection of segmental wall abnormalities, such as hyp~kinesia.~~
Varetto et a1 examined diagnostic and prognostic value in ED pa- tients with nondiagnostic ECGs. Sensitivity for AM1 was 100% (13/13), and there was a significant difference in 18 month follow-up complica- tion rates of 0 of 34 patients with normal perfusion scans versus six events in 30 patients with perfusion defects.57 Tatum examined the diagnostic and prognostic value of sestamibi's routine use in ED patients at low risk for AM1 and moderate risk for unstable angina without typical ECG findings (termed triage level 3 and level 4 patients).55 All patients had sestamibi injected at rest; and the sample included patients with and without active pain. In the 442 patients evaluated, there were no deaths and was a 3% and 0.7% AM1 rate and a 17% and 2.5% revascularization rate in level 3 and level 4 patients repectively. The scan was 100% sensitive for AM1 within the first 30 days. There was a 2.1% revascularization rate in patients with a normal scan versus a 30% revascularization rate in patients with a positive scan (p<O.OOl, relative risk 14.5, 95% confidence interval 6-34). From 1 to 12 months of follow- up there was a 0% versus 4% cardiac death rate (p=0.002) and a 0.9% vs 2% revascularization rate difference ( p = NS) in negative versus positive scans. A normal resting sestamibi scan appears to be a good prognostic marker; however, a multivariate analysis was not performed. Concordant prognostic outcomes have been found for chest pain patients tested in the outpatient setting3 One must be cautious about applying the test to patients who are pain free, because a study using sestamibi

PATIENTS WITH CHEST PAIN IN THE EMERGENCY DEPARTMENT 511
to diagnose unstable angina found high sensitivity when the patient experienced pain (96%), but there was a much reduced sensitivity (65%) when the patient was pain free.5 Also, because the clinician’s therapy may have been guided by the results of the scan, its validity as a predictor is thereby lessened.
In a prospective observational study of the prognostic value of rest sestamibi scanning, Hilton et a1 studied 102 ED patients with active symptoms of typical angina and a nondiagnostic ECG.27 Patients were followed for cardiac events, including AMI, revascularization, thrombol- ysis, and death. Normal compared with abnormal or equivocal scans had a sensitivity of 94%, a specificity of 83%, and an accuracy of 85% for cardiac events (risk ratio, 13.9, p = 0.0001). Multivariate analysis deter- mined that sestamibi scanning was the only predictor of cardiac events ( p = 0.009). Like the previous study, the validity is weakened because treating clinicians had access to the scan results, which may account for its strong association with outcome variables.
RISK STRATIFICATION WITH ECHOCARDIOGRAPHY
Bedside echocardiography provides real-time two-dimensional im- ages of the pericardium, myocardial walls, cardiac chambers, and heart valves. For the purposes of determining prognosis, the most important information is obtained by visualizing the ventricular walls and endocar- dial surface to identify regional wall motion abnormalities or abnormal myocardial thickening, which can then be a measure of global function if one uses these factors to estimate an ejection fraction.52 The limitations of echocardiography include the difficulty in detecting wall motion abnormalities and thickening, the 10% of patients who have no acoustic window and thus cannot be imaged, the technical expertise needed for performance and interpretation, and the time (10-15 min) required to perform the scan.52 It is the author’s intent to review the data on the use of echocardiography for prognosis; its diagnostic value has been re- viewed recently elsewhere.
One hundred seventy one ED patients with chest pain or shortness of breath within 4 hours of symptoms of at least 30 minutes’ duration were followed for early (<48 hr) and late (48 hr-2 y) cardiac events, which included nonfatal AMI, death, arrhythmias, and coronary revascu- larization. Measures of left ventricular systolic function were found to be a significant independent predictor of short- and long-term events, in addition to age and ECG abn~rmalities.~~ In 201 consecutive patients with AMI, Beming et a1 examined the predictive value of clinical and echocardiographically defined ejection fraction on for mortality at 2 month^.^ Age (pcO.01) and ejection fraction as dichotomized at 40% (p<O.OOOl) were the only significant predictors in the Cox regression model, which also examined nine other clinical variables. Other limited studies of echocardiography suggest that it has good sensitivity for AMIF2 however, there are no good studies that test whether it works in

512 ZALENSKI et a1
conditions of actual use or of its role in the ED as a predictor of early life-threatening events.
Risk Stratification of Patients Discharged from the Emergency Department
It is the intent of this section to extend risk stratification in an effort to examine predictors of cardiac death from 1 month to 2 years postdischarge in patients who are discharged from the ED. This prognos- tic information conceivably could be useful for making outpatient refer- rals for those patients needing more aggressive evaluations and follow- up care.
Many years ago, Shroeder observed that the patient hospitalized with acute ischemic chest pain without AM1 had a similar long-term outcome (6-24 mo) to the patient hospitalized with proven AMI.50 He therefore recommended that the groups with and without AM1 receive similar evaluations. Lee has observed that an analogous situation may exist between ED patients who are admitted with suspected AM and ruled out and those who are ruled out in the ED and dis~harged.~~ In a study of the long-term prognosis of 1,956 patients with chest pain, Lee found that there was a 6% (113/1956) cardiovascular death rate and a 10% overall death rate at a mean follow-up of 30.1 One half the cohort (964) were admitted and 992 were directly discharged from ED. There was no difference between 3-year survival rates of patients discharged from ED. There was no difference between 3-year survival rates of patients discharged from ED with known prior diagnosis of angina or MI (89%) from any the following disease groups discharged alive from the hospital: AM1 in hospital (85%), angina in hospital (87%), or other CV diagnoses (87%). If there was no prior diagnosis of CAD, the prognosis was excellent, with cardiovascular survival rates of over 95% over 3 years. Cox regression identified the following predictors of survival in patients discharged alive from either the ED or hospital: age in 10-year increments (1.4 mortality rate ratio, determined by exponenti- ation of the coefficients derived from a stepwise Cox proportional hazard model), history of CAD (2.2), ECG findings (2.1), CHF during ED evalua- tion or after admission (2.4), and cardiogenic shock after hospital admis- sion (3.7). The authors conclude that postdischarge noninvasive strate- gies like those for patients who “rule-in” should be applied to those who ”rule-out,” including patients with a history of CAD or symptoms of CAD who are stable enough to be discharged from the ED.36
Karlson et a1 examined whether mortality and ED revisits can be calculated using easily acquired data from 7,157 ED visits made by5,362 persons.33 Vital status at 1 year was known for 95% of the visits. The predictors of cardiac death were admitting ECG, degree of suspicion of AMI, age, history of diabetes mellitus, CHF, or hypertension, and other presenting findings. A regression equation permitted the computation of the risk of death at 1, 6, and 12 months. Patients discharged but at

PATIENTS WITH CHEST PAIN IN THE EMERGENCY DEPARTMENT 513
higher risk of death could be studied for the impact of aggressive outpatient care plans.33 For example, after discharge from the ED, LV dysfunction, or mitral regurgitation on transthoracic echocardiography predict mortality during a 29-month follow-up period on multivariate analysis.16 Villanueva also found that of 105 patients directly discharged from ED, 16 (15%) had cardiac events, most (11/32) of which occurred in patients with angina pectoris or CHF.58 Only one half of long-term events (>lo months) could be predicted from available ED measure- ments whereas 75% could be predicted within 48 hours (p=O.O4). In chest pain patients discharged from the ED, the 1-year mortality was not significantly higher in those with diabetes mellit~s.*~ Also, gender does not appear to affect the prognosis of patients discharged from the ED.26
CONCLUSION
Risk stratification is the key to choosing the appropriate setting of further evaluation from the CCU to the outpatient setting. Since the early studies of Yusef62 and Brush? the initial ECG is the simplest predictor of subsequent life-threatening events and is probably the most widely used. Clinical experience and research results also suggest that patients with active pain that is typical of myocardial ischemia are also at high risk.6, 9, 14, 18, 67 These are the simplest tools for risk stratification. The well-studied multivariate approach to risk stratification comes from the MCPS study in a model that uses readily available history, physical examination, and ECG variables.18 Such a model can be used to deter- mine the initial risk of complications and can then update the risk at 12 hours, and, if needed, 24 and 48 hours into the care of the patient. As yet, there has been no study to examine the clinical impact of this tool in conditions of actual use. A trial of providing the results of a similar algorithm for the risk of AM1 from the MCPS group was found to have no impact on care.39 The initial risk could be easily applied in the prehospital system and used for bypass to cardiac referral centers.
Data from cTnI testing appear to be especially promising for the risk stratification of chest pain patients without ST-segment elevation in the ED, the group for which prognosis is less clear. The impressive results reported in this reviewzz need to undergo prospective validation or careful implementation in the context of outpatient follow-up care, because decisions affecting the care of 5 million patients in the United States annually should be made on the basis of a study predicting only 34 cardiac events. In addition, the previous, more limited prognostic results from other ED trials do not appear to have achieved the same level of superior ~erformance.~, I1 Other technologies, including imaging tests, may be able to improve and perhaps shorten the testing needed during the ED stay for adequate risk stratificati~n.~~, 49, 55, 57 Comprehen- sive multicenter studies comparing the marginal prognostic value and cost assessment of such tests are needed.

514 ZALENSKI et a1
There is also a need for developing a more comprehensive statistical predictive models that combine the prognostic value of markers as they vary over time, along with other diagnostic tests (e.g., ECG), baseline variables, and physical history. For instance, rather than dichotomizing a certain threshold level of a marker, the changes of biologic over time could best be modeled using a mixed random effect approach, thus extracting maximal predictive value regarding outcomes.40, 41 Further- more, introducing newer statistical approaches that could account for the ordinal nature of the severity of the composite outcomes of cardiac events may provide a better risk assessment for this composite end- point.2 On the basis of such well-suited statistical models, the risk stratification of patients can be more adequately devised by partitioning the predicted risk scores and risk indexes.43 Finally, there may be addi- tional opportunities found in these models to intervene and prevent death and disability in selected subsets of patients who present to the ED with chest pain but whose long-term rather that short-term prognosis is unfavorable.
References
1. Antman EM, Tanasijevic MJ, Thompson B, et al: Cardiac-specific troponin I levels to predict the risk of mortality in patients with acute coronary syndromes. N Engl J Med 335:1342-1349, 1996
2. Agresti A: Categorical Data Analysis. New York, John Wiley & Sons, 1990 3. Berman DS, Hachamovitch R, Kiat H, et al: Incremental value of prognostic testing in
patients with known or suspected ischemic heart disease: A basis for optimal utiliza- tion of exercise technetium-99m sestamibi myocardial perfusion single-photon emis- sion computed tomography. J Am Coll Cardiol 26:639-647, 1995
4. Beming J, Launbjerg J, Appleyard M, et al: Echocardiographic algorithms for admission and predischarge prediction of mortality in acute myocardial infarction. Am J Cardiol
5 . Bilodeau L, Theroux P, Gregoire J, et al: Technetium-99m sestamibi tomography in patients with spontaneous chest pain: Correlations with clinical, electrocardiographic and angiographic findings. J Am Coll Cardiol 18:1684-1691, 1991
6 . Braunwald E, Mark DB, Jones RH, et al: Unstable Angina: Diagnosis and Management: Clinical Practice Guideline Number 10, AHCPR Publication No. 94-0602. Rockville, MD, Agency for Health Care Policy and Research and the National Heart, Lung, and Blood Institute, Public Health Service, US. Department of Health and Human Services, March 1994
7. Brogan GX, Hollander JE, McCuskey CF, et al: Evaluation of a new assay for cardiac troponin I vs creatine kinase-MB for the diagnosis of acute myocardial infarction. Acad Emerg Med 4612,1997
8. Brush JE, Brand DA, Acampora D, et al: Use of the initial electrocardiogram to predict in-hospital complications of acute myocardial infarction. N Engl J Med 3121137-1141, 1985
9. Calvin JE, Klein LW, VandenBerg BJ, et al: Risk stratification in unstable angina: Prospective validation of the braunwald classification. JAMA 273:136-141, 1995
10. Concato J, Feinstin A, Holford TR The risk of determining risk with multivariable models. Ann Intern Med 118,201-210, 1993
11. de Winter RJ, Koster RW, Schotveld JH, et al: Prognostic value of troponin T, myoglo- bin, and CK-MB mass in patients presenting with chest pain without acute myocardial infarction. Heart 75:235-239, 1996
69:1538-1544, 1992

PATIENTS WITH CHEST PAIN IN THE EMERGENCY DEPARTMENT 515
12. Fesmire FM, Percy RF, Wears RL, et al: Diagnostic and prognostic important of comparing the initial to the previous electrocardiogram in patients admitted for sus- pected acute myocardial infarction. South Med J 84:841-845, 1991
13. Fesmire FM, Percy RF, Wears RL, et al: Risk stratification according to the initial electrocardiogram in patients with suspected acute myocardial infarction. Arch Intern Med 149:1294-1296, 1989
14. Fesmire FM, Wears RL: The utility of the presence or absence of chest pain in patients with suspected acute myocardial infarction. Am J Emerg Med 7372-377, 1989
15. Fineberg HV, Scadden D, Goldman L: Care of patients with a low probability of acute myocardial infarction: Cost effectiveness of alternatives to coronary-care-unit admission. N Engl J Med 310:1301-1307, 1984
16. Fleischmann KE, Goldman L, Robiolio PA, et al: Echocardiographic correlates of survival in patients with chest pain. J Am Coll Cardiol23:1390-1396, 1994
17. Gaspoz JM, Lee TL, Weinstein MC, Cook EF, et al: Cost-effectiveness of a new short- stay unit to “rule out” acute myocardial infarction in low risk patients. J Am Coll Cardiol 24:1249-1259, 1994
18. Goldman L, Cook EF, Johnson PA, et al: Prediction of the need for intensive care in patients who come to emergency departments with acute chest pain. N Engl J Med
19. Goldman L, Cook EF, Brand DA, et al: A computer protocol to predict myocardiol infarction in emergency department patients with chest pain. N Engl J Med 318:797- 803, 1988
20. Green LA, Yates JF: Influence of pseudodiagnostic information on the evaluation of ischemic heart disease. Ann Emerg Med 25:451457, 1995
21. Hamm CW, Ravkilde J, Gerhardt W, et al: The prognostic value of serum troponin T in unstable angina. N Engl J Med 327146150, 1992
22. Hamm CW, Goldmann BU, Heeschen C, et al: Emergency room triage of patients with acute chest pain by means of rapid testing for cardiac troponin T or troponin I. N Engl J Med 3371648-1653, 1997
23. Hedges JR The role of CK-MD in chest pain decision-making. J Accident Emerg Med
24. Hedges JR, Young GP, Henkel GF, et al: Early CK-MB elevations predict ischemic events in stable chest pain patients. Acad Emerg Med 1:9-16, 1994
25. Herlitz J, Karlson BW, Edvardsson N, et al: Prognosis in diabetics with chest pain or other symptoms suggestive of acute myocardial infarction. Cardiology 80237-245,1992
26. Herlitz J, Karlson BW, Wiklund I, et al: Prognosis and gender differences in chest pain patients discharged from an ED. Am J Emerg Med 13:127-132, 1995
27. Hilton TC, Thompson RC, Williams HJ, et al: Technetium-99m sestamibi myocardial perfusion imaging in the emergency room evaluation of chest pain. J Am Coll Cardiol 23:1016-22, 1994
334~1498-1504, 1996
12:101-106, 1995
28. Hochberg Y Multiple Comparison Procedures. New York, John Wiley & Sons, 1987 29. Hoekstra JW, Hedges JR, Gibler WB, et al: Emergency department CK-MB: A predictor
of ischemic complications. National cooperative CK-MB project group. Acad Emerg Med 1:17-27, 1994
30. Jayes Jr RL, Beshanski JR, D’Agostino RB: Do patients’ coronary risk factor reports predict acute cardiac ischemia in the emergency department? A multicenter study. J Clin Epidemiol45:621-626, 1992
31. Kannel WB, Schwartz MJ, McNamara PM: Blood pressure and risk of coronary heart disease: The Framingham study. Dis Chest 56:43-52, 1969
32. Karlson BW, Hallgren HP, Liljeqvist JA, et al: Emergency room prediction of mortality and severe complications in patients with suspected acute myocardial infarction. Eur Heart J 15:1558-1565, 1994
33. Karlson BW, Herlitz J, Strombom U, et al: Improvement of ED prediction of cardiac mortality among patients with symptoms suggestive of acute myocardial infarction. Am J Emerg Med 15:l-7, 1997
34. Karlson BW, Wiklund I, Bengtson A, et al: Prognosis and symptoms one year after discharge from the emergency department in patients with acute chest pain. Chest 105:1442-1447, 1994

516 ZALENSKI et a1
35. Larsen GC, Griffith JL, Beshanski JR, et al: Electrocardiographic left ventricular hyper- trophy in patients with suspected acute cardiac ischemia-its influence on diagnosis, triage, and short-term prognosis: A multicenter study. J Gen Intern Med 9:666473,1994
36. Lee TH, Juarez G, Cook F, et al: Ruling out acute myocardial infarction: A prospective multicenter validation of a 12-hour strategy for patients at low risk. N Engl J Med
37. Lee TH, Rouan GW, Weisberg MC, et al: Clinical characteristics and natural history of patients with acute myocardial infarction sent home from the emergency room. Am J Cardiol 60:219-224, 1987
38. Lee TH, Ting HH, Shammash JB, et al: Long-term survival of emergency department patients with acute chest pain. Am J Cardiol 69:145-151, 1992
39. Lee TH, Pearson SD, Johnson PA, et a1 Failure of information as an intervention to modify clinical management: A time-series trial in patients with acute chest pain. Ann Intern Med 122:434-437, 1995
40. Lindstrom MJ, Bates DM: Newton-Raphson and EM algorithums for linear mixed- effects models for repeated-measure data. Journal of the American Statistical Associa- tion 83:1014-1022, 1988
324:1239-1246, 1991
41. Longford NT Random coefficient models. Oxford, Clarendon Press, 1993 42. McCarthy BD, Beshansky JR, DAgostino RB, et al: Missed diagnoses of acute myocar-
dial infarction in the emergency department: Results from a multicenter study. Ann Emerg Med 22579-582, 1993
43. Mike V, Stanley KE: Statistics in Medical Research Methods and Issues, with Applica- tions in Cancer Research. New York, John Wiley & Sons, 1982
44. Ohman EM, Armstrong PW, Christenson RH, et al: Cardiac troponin T levels for risk stratification in acute myocardial ischemia. N Engl J Med 335:1333-1341, 1996
45. Ravkilde J, Horder M, Gerhardt W, et a1 Diagnostic performance and prognostic value of serum troponin T in suspected acute myocardial infarction. Scand J Clin Lab Invest
46. Roberts RR, Zalenski RJ, Mensah EK, et al: Costs of emergency department-based accelerated diagnostic protocol vs hospitalization in patients with chest pain: A ran- domized controlled trial. JAMA 278:1670-1676, 1997
47. Rouan GW, Lee TH, Cook EF, et al: Clinical characteristics and outcome of acute myocardial infarction in patients with initially normal or nonspecific electrocardio- grams (a report from the multicenter chest pain study). Am J Cardiol 641087-1092, 1989
48. Rusnak RA, Stair TO, Hansen K, et a1 Litigation against the emergency physician: Common features in cases of missed myocardial infarction. Ann Emerg Med 18:1029-
53~677-685, 1993
- 1034, 1989
49. Sabia P. Abbott RD. Afrookteh A. et al: ImDortance of two-dimensional echocardio- graphic' assessment 'of left ventricular systdic function in patients presenting to the emergency room with cardiac-related symptoms. Circulation 84:1615-1624, 1991
50. Schroeder JS, Lamb IH, Hu M: Do patients in whom myocardial infarction has been ruled out have a better prognosis after hospitalization than those surviving infarction? N Engl J Med 303:l-5, 1980
51. Selker HP: Coronary care unit triage decision aids: How do we know when they work? Am J Med 87491493, 1989
52. Selker HP, Zalenski RJ, Antman EM, et al: An evaluation of technologies for identifying acute cardiac ischemia in the emergency department: A report from a national heart attack alert program working group. Ann Emerg Med 29:13-87, 1997
53. Slater DK, Hlatky MA, Mark DB, et al: Outcome in suspected acute myocardial infarction with normal or minimally abnormal admission electrocardiographic fmd- ings. Am J Cardiol 60:766-770, 1987
54. Sox HC, Hickam DH, Marton KI, et al: Using the patient's history to estimate the probability of coronary artery disease: A comparison of primary care and referral practices. Am J Med 89:7-14, 1990
55. Tatum JL, Jesse RL, Kontos MC, et al: Comprehensive strategy for the evaluation and triage of the chest pain patient. Ann Emerg Med 29:116-124, 1997
56. Tosteson AN, Goldman L, Udvarhelyi IS, et al: Cost-effectiveness of a coronary care

PATIENTS WITH CHEST PAIN IN THE EMERGENCY DEPARTMENT 517
unit versus an intermediate care unit for emergency department patients with chest pain. Circulation 94143-150,1996
57. Varetto T, Cantalupi D, Altieri A, et al: Emergency room Technetium-99m sestimibi imaging to rule out acute myocardial ischemic events in patients with nondiagnostic electrocardiograms. J Am Coll Cardiol22:1804-1808, 1993
58. Villaneuva FS, Sabia PJ, Afrookteh A, et al: Value and limitations of current methods of evaluating patients present to the emergency room with cardiac-related symptoms for determining long-term prognosis. Am J Cardiol 69:746-750, 1992
59. Weingarten SR, Ermann B, Riedinger MS, et al: Selecting the best triage rule for patients hospitalized with chest pain. Am J Med 87494-500, 1989
60. Weingarten S: Practice guidelines and prediction rules should be subject to careful clinical testing. JAMA 2771977-1978, 1997
61. White LD, Lee TH, Cook EF, et al: Comparison of the natural history of new onset and exacerbated chronic ischemic heart disease. J Am Coll Cardiol 16:304-310, 1990
62. Yusuf S, Pearson M, Sterry H, et al: The entry ECG in the early diagnosis and prognostic stratification of patients with suspected acute myocardial infarction. Eur Heart J 5:690-696, 1984
63. Zalenski RJ, McCarren M, Roberts R, et al: An evaluation of a chest pain diagnostic protocol to exclude acute cardiac ischemia in the emergency department. Arch Intern Med 1571085-1091, 1997
64. Zalenski RJ, Roberts RR: Chest pain. In Harwood-Nuss A, Linden C, Luten R, et al: The Clinical Practice of Emergency Medicine. Philadelphia, JB Lippincott, 1996
65. Zalenski RJ, Rydman RJ, McCarren M, et al: Feasibility of a rapid diagnostic protocol for an emergency department chest pain unit. Ann Emerg Med 29:99-108, 1997
66. Zalenski RJ, Rydman RJ, Sloan EP, et a1 The emergency department electrocardiogram and hospital complications in myocardial infarction patients. Acad Emerg Med 3:318- 325, 1996
67. Zalenski RJ, Sloan EP, Chen EH, et a1 The emergency department ECG and immedi- ately life-threatening complication sin initially uncomplicated suspected myocardial ischemia. Ann Emerg Med 17221-226, 1988
Address reprint requests to Robert J. Zalensky, MD, MA
University Health Center, 8D Wayne State University School of Medicine
4201 St. Antoine Detroit, MI 48201