Embed Size (px)
Citation preview

Evaluation of Efficacy and Safetyof the Glucagon ReceptorAntagonist LY2409021 in PatientsWith Type 2 Diabetes: 12- and24-Week Phase 2 StudiesDiabetes Care 2016;39:1241–1249 | DOI: 10.2337/dc15-1643
OBJECTIVE
Type 2 diabetes pathophysiology is characterized by dysregulated glucagon secre-tion. LY2409021, a potent, selective small-molecule glucagon receptor antagonistthat lowers glucose was evaluated for efficacy and safety in patients with type 2diabetes.
RESEARCH DESIGN AND METHODS
The efficacy (HbA1c and glucose) and safety (serum aminotransferase) of once-daily oral administration of LY2409021 was assessed in two double-blind studies.Phase 2a study patients were randomized to 10, 30, or 60 mg of LY2409021 orplacebo for 12 weeks. Phase 2b study patients were randomized to 2.5, 10, or20 mg LY2409021 or placebo for 24 weeks.
RESULTS
LY2409021 produced reductions in HbA1c that were significantly different fromplacebo over both 12 and 24 weeks. After 12 weeks, least squares (LS) meanchange from baseline in HbA1c was –0.83% (10 mg), –0.65% (30 mg), and –0.66%(60 mg) (all P < 0.05) vs. placebo, 0.11%. After 24 weeks, LS mean change frombaseline in HbA1c was –0.45% (2.5 mg), –0.78% (10 mg, P < 0.05), –0.92% (20 mg,P < 0.05), and –0.15% with placebo. Increases in serum aminotransferase, fastingglucagon, and total fasting glucagon-like peptide-1 (GLP-1) were observed; levelsreturned to baseline after drug washout. Fasting glucose was also lowered withLY2409021 at doses associated with only modest increases in aminotransferases(mean increase in alanine aminotransferase [ALT] £10 units/L). The incidenceof hypoglycemia in the LY2409021 groups was not statistically different fromplacebo.
CONCLUSIONS
In patients with type 2 diabetes, glucagon receptor antagonist treatment signif-icantly lowered HbA1c and glucose levels with good overall tolerability and a lowrisk for hypoglycemia. Modest, reversible increases in serum aminotransferaseswere observed.
1Eli Lilly and Company, Suresnes, France2Eli Lilly and Company, Indianapolis, IN3Lilly-NUS Centre for Clinical Pharmacology,Singapore4inVentiv Health Clinical, Clarksville, MD5National Research Institute, Los Angeles, CA
Corresponding author: Christof M. Kazda,[email protected].
Received 27 July 2015 and accepted 30 March2016.
Clinical trial reg. nos. NCT01241448 (phase 2a)and NCT00871572 (phase 2b), clinicaltrials.gov.
This article contains Supplementary Data onlineat http://care.diabetesjournals.org/lookup/suppl/doi:10.2337/dc15-1643/-/DC1.
Y.D. is currently affiliatedwith the Department ofBiostatistics, University of Pittsburgh, Pitts-burgh, PA, and C.N.L. is currently affiliated withthe Department of Experimental and ClinicalPharmacology, University of Minnesota TwinCities, Minneapolis, MN.
*Retired.
© 2016 by the American Diabetes Association.Readersmayuse this article as longas thework isproperly cited, the use is educational and not forprofit, and the work is not altered.
See accompanying article, p. 1075.
Christof M. Kazda,1 Ying Ding,2
Ronan P. Kelly,3 Parag Garhyan,2
Chunxue Shi,4 Chay Ngee Lim,2 Haoda Fu,2
David E. Watson,2 Andrew J. Lewin,5*
William H. Landschulz,2 Mark A. Deeg,2
David E. Moller,2 and Thomas A. Hardy2
Diabetes Care Volume 39, July 2016 1241
EMER
GINGTEC
HNOLO
GIES
ANDTH
ERAPEU
TICS

Type 2 diabetes is characterized bychronic hyperglycemia as a result ofimpaired insulin secretion and action.Dysregulated glucagon secretion (1–3)and resultant hepatic glucose overpro-duction are also characteristic patho-physiological features and contributeto hyperglycemia in type 2 diabetes(4–10). Previous studies with LY2409021have demonstrated that glucagon re-ceptor antagonism inhibits glucoseproduction in response to exogenoushyperglucagonemia in healthy volun-teers and improves hyperglycemia inpatients with type 2 diabetes throughreductions in both fasting and postpran-dial glucose (11,12). A 28-day phase 1study of LY2409021 in patients withtype 2 diabetes demonstrated improve-ment in glycemic parameters at dosesof 5–90 mg administered once daily(12). However, reversible, dose-relatedincreases in the levels of serum amino-transferases were observed in that study(12). Similar reversible increases in se-rum aminotransferases have been notedwith other glucagon receptor antago-nists, including a human glucagon recep-tor monoclonal antibody (13), othersmall molecules (14–17), and an anti-sense oligonucleotide targeting gluca-gon receptor expression (18).In the present phase 2a and 2b studies,
we further examined the glucose-loweringefficacy and safety of LY2409021 by com-paring the relationships between dosesof LY2409021 that lower HbA1c and glu-cose levels (efficacy) and those that in-crease serum aminotransferase levels(hepatic safety). The phase 2b study re-ported here represents the largest andlongest clinical trial of a glucagon recep-tor antagonist reported to date.
RESEARCH DESIGN AND METHODS
Study DesignBoth phase 2a (NCT00871572) andphase 2b (NCT01241448) studies wereconducted in accordance with regula-tory standards of good clinical practice,the Declaration of Helsinki, and all appli-cable local regulations. Study protocolswere approved by each site’s ethical re-view board. All patients provided writ-ten informed consent before initiationof study procedures. The phase 2a studywas a multicenter, randomized, double-blind, placebo-controlled, parallel-groupstudy with a 1-week single-blind placebolead-in period, a 12-week double-blind
active treatment period, and a 4-weekblinded posttreatment washout/follow-up period (Supplementary Fig. 1A). Pa-tients were randomly assigned to oneof the four treatment groups (Supple-mentary Fig. 1A) in a 1.5:2.1:1:1 ratio(60 mg:30 mg:10 mg:placebo). Unequalallocation was used to maximize the ex-posure to 30 mg LY2409021. Stratifica-tion was based on the absence orpresence of preexisting metformin ther-apy and on study site. The phase 2b studywas amulticenter, randomized, double-blind, placebo-controlled, parallel-groupstudy consisting of a 1-week single-blindplacebo lead-in period, a 24-week ac-tive treatment period, and a 4-week blin-ded posttreatment washout/follow-upper iod (Supplementary Fig . 1B ) .Patients were randomly assigned toone of the four treatment groups(Supplementary Fig. 1B) in a 1:1:1:1 ra-tio (20 mg:10 mg:2.5 mg:placebo).Stratification was based on preexistingmetformin therapy, baseline HbA1c
level (, or $8.2% [66 mmol/mol]),and baseline alanine aminotransferase(ALT) levels (# or . the upper limit ofnormal [ULN]). Patients were discontin-ued from study participation if they hadfasting glucose levels .270 mg/dLon three or more separate days overany 2-week period between randomiza-tion and week 6 of treatment, fasting glu-cose levels.240mg/dL on three ormoreseparate days over any 2-week period be-tween weeks 6 and 12, or fasting glucoselevels.200 mg/dL or HbA1c levels.8.0%(64 mmol/mol) from week 12 to week 24of treatment. The criteria for the two stud-ies were the same through 12 weeks oftreatment; the phase 2b study had morestringent criteria after 12 weeks.
The doses of LY2409021 used in thephase 2b study were selected on thebasis of the exposure response analysisof a phase 1, 28-day, multiple-dose studythat indicated that doses of LY2409021ranging from 30 to 90 mg/day producedsubstantial lowering of fasting glucoselevels in patients with type 2 diabetes(12) and the current phase 2a studythat demonstrated reductions in fastingglucose and HbA1c levels in patients withtype 2 diabetes at all dose levels (10, 30,and 60 mg). The doses of LY2409021 se-lected for the phase 2b study (2.5, 10,and 20 mg once daily) were used to iden-tify theminimal efficacious dose andmax-imize the ability to demonstrate clinically
meaningful efficacy with acceptable he-patic safety over the 24-week treatmentperiod.
Study ParticipantsPatients were adults (aged 18–70 years,inclusive) with diagnoses of type 2 dia-betes according to the World HealthOrganization diagnostic criteria (19) whohad been treated with diet and exercisealone or in combination with a stabledose of metformin ($1,000 mg/day)for at least 3 months before screening.Patients had HbA1c values of 6.5–10%(48–86 mmol/mol) and BMI between25 and 40 kg/m2, inclusive (phase 2astudy), and 7.0–10.5% (53–91 mmol/mol)and a BMI between 25 and 45 kg/m2, in-clusive (phase 2b study). Patients agreedto self-monitor blood glucose (SMBG) lev-els, complete study diaries, and maintainconsistent dietary, physical activity, andsleeping patterns throughout the study.Stable doses of antihypertensives orlipid-lowering medications were allowed.Clinical signs or symptomsof liver disease,previous diagnosis or serologic evidenceof hepatitis B or C infection, and use ofany antihyperglycemic medication otherthan metformin within the 3-month pe-riod before screening were exclusionaryfor both studies. Additional exclusion cri-teria at screening included aminotrans-ferase levels greater than two times theULNand fasting triglycerides.400mg/dLin the phase 2a study and aminotransfer-ase levels.2.5 times the ULN, nonfastingtriglyceride levels.600 mg/dL, and useof insulin or glucagon-like peptide-1(GLP-1) agonist for .5 days within the3-month period before screening in thephase 2b study.
Outcome MeasuresThe primary efficacy end point wasmean change in HbA1c level from base-line to end of the 12-week LY2409021treatment period (phase 2a study) andto the end of the 24-week treatmentperiod (phase 2b study). Secondaryend points (in both studies) includedchanges in fasting serum glucose, gluca-gon, and GLP-1 (total and active [7–36])levels and fasting serum insulin levels.Seven-point SMBG profiles consisted ofblood glucose values obtained beforeand 2 h after each meal and at bedtime(phase 2a study) or at 0300 h (phase 2bstudy) on two separate days during the5-day period before the respectivestudy visits. For the phase 2a study,
1242 Efficacy and Safety of LY2409021 Diabetes Care Volume 39, July 2016

fasting lipid profiles were collected atinitiation of treatment (week 0) and atend point (week 12); fasting bodyweight and sitting blood pressure mea-surements were collected before ran-domization and weekly throughout thetreatment period. For the phase 2bstudy, fasting lipid profiles were col-lected at baseline and weeks 8, 12, 16,and 24; fasting body weight and sittingblood pressure measurements werecollected before randomization and bi-weekly throughout the treatment period.Hepatic safety assessment includedweekly (phase2astudy)orbiweekly (phase2b study) monitoring of ALT; aspartateaminotransferase (AST); g-glutamyl trans-ferase (GGT); alkaline phosphatase (ALK);and total, direct, and indirect bilirubinlevels.
Analytical MethodsBlood samples for glucagon and GLP-1analysis were collected in prechilledtubes containing EDTA. After collection,aprotinin/Trasylol (Bayer) (glucagonsamples) and dipeptidyl peptidase-4 in-hibitor (GLP-1 samples) additives wereadded as a preservative. For the phase2a study, plasma glucagon concentra-tions were measured by radioimmuno-assay by ALPCODiagnostics (Salem, NH).For the phase 2b study, plasma glucagonconcentrations were measured using anelectrochemiluminescence sandwichimmunoassay (20). Both assays have,1% cross-reactivity to oxyntomodulinor gut glucagon-like immunoreactivity.LY2409021 does not cross-react with im-munoassays where glucagon and GLP-1are measured. LY2409021 binds only tothe receptor, not to ligands of the re-ceptor or related receptors. For bothphase 2a and 2b studies, total and active(7–36) plasma GLP-1 levels were mea-sured using an ELISA (Millipore Corp.,St. Charles, MO) and electrochemi-luminescence sandwich immunoassay(Meso Scale Discovery, Rockville, MD),respectively; fasting serum glucose lev-els were measured using a commerciallyvalidated method; serum insulin levelswere measured using direct chemilumi-nescent immunoassays (ADVIA Centaur;Siemens, New York, NY); patient 7-pointSMBG levels weremeasured using a cali-brated glucose meter; total cholesterol,HDL cholesterol, and triglyceride levelswere determined directly and LDL choles-terol was calculated and systolic and
diastolic blood pressure (SBP and DBP)were measured with an automated cuffwhile the patient was in a sitting position.
Data AnalysesFor both phase 2a and 2b studies, effi-cacy analyses were conducted on themodified intent-to-treat population, de-fined as all randomized patients with atleast one postbaselinemeasurement ac-cording to the treatment the patientswere assigned. Mixed-effects model re-peated measures (MMRM) analysis wasused for the primary analysis of HbA1clevels for both studies. The least squares(LS) mean differences, 90% CIs, and Pvalues reported were based on a modelthat included baseline HbA1c as a covari-ate and metformin use, visit, treatment,and visit-by-treatment interaction asfixed effects. Change in HbA1c level frombaseline to end point was also analyzedusing ANCOVA with baseline as a cova-riate and treatment andmetformin useas fixed effects. There were no adjust-ments of multiplicity for any analysesunless otherwise stated. Missing endpoints were imputed using last obser-vation carried forward. For the phase2b study, categorical analyses on HbA1cwere also performed to compare theproportions of patients who achievedHbA1c values #6.5% (48 mmol/mol)and ,7.0% (53 mmol/mol) at week24 by treatment group. A Cochran-Mantel-Haenszel test was used andstratified by baseline HbA1c values(,8.2%, $8.2% [66 mmol/mol]). Forboth phase 2a and 2b studies, analysesof secondary efficacy measures withcontinuous data were performed usingsimilar statistical models. Fisher exacttest also compared each treatmentgroup with the placebo group for cat-egorical outcomes. An ANCOVA wasperformed on the change from base-line aminotransferase values at eachvisit up to the end of the posttreat-ment washout period and analyzedusing an MMRM model. The modelconsisted of the baseline value as acovariate and visit, treatment, andvisit-by-treatment interaction as fixedeffects. Treatment comparisons werereported as the treatment LS mean,95% CI, and P value. Safety analyseswere performed on the safety popula-tion, which was defined as all random-ized patients who received at least onedose of the assigned study drug.
RESULTS
Patient Disposition, Demographics,and Baseline CharacteristicsIn the phase 2a study, 87 patients wererandomized, 68 (78.2%) completed thestudy, and 21.8% of patients prematurelydiscontinued (Supplementary Fig. 2A).The most commonly reported reason forstudy discontinuation was subject deci-sion (8.0%). Discontinuations due to ad-verse events (five patients, 5.9%) weredriven by abnormalities in laboratory val-ues (two events of liver aminotransferaselevel increases and three events of serumamylase and/or lipase level increases)without any clinical symptoms. All discon-tinuations due to adverse events oc-curred in patients receiving LY2409021.In the phase 2b study, 254 patientswere randomized and 151 (59%) com-pleted the study: 29 in the placebo group,36 in the 2.5-mg group, 43 in the 10-mggroup, and 43 in the 20-mg group(Supplementary Fig. 2B). Approximately40% of patients (103 of 254) discontinuedearly. Themost common reasons for earlydiscontinuation were loss of glycemiccontrol based on protocol discontinua-tion criteria (49 [19%]), protocol violation(24 [9%]), and subject decision (18 [7%]).Most of the per-protocol discontinua-tions due to inadequate glycemic controloccurred at week 14when hyperglycemiadiscontinuation criteria became morestringent. Specifically, eleven placebopatients (17%), eight 2.5-mg patients(13%), seven 10-mg patients (11%),and four 20-mg patients (6%) discon-tinued the study at week 14 becauseof protocol discontinuation criteria re-lated to inadequate glycemic control.The mean and median days of treat-ment were 130 and 167, respectively.
Baseline characteristics for phase 2astudy participants (Supplementary Table 1)showed that HbA1c values (mean, %[mmol/mol]) at week 0 for the LY2409021treatment groups were highest in the10-mg group (8.0% [64 mmol/mol]) andwere 7.5% (58mmol/mol) for the 30-mggroup, 7.6% (60mmol/mol) for the 60-mggroup, and 7.9% (62 mmol/mol) for theplacebo group. The most common con-comitant medication was metformin,used by 58.6% of patients.
Baseline characteristics for phase 2bstudy participants (Supplementary Table 2)showed overall similarity in treatmentgroup demographics. The mean HbA1c
care.diabetesjournals.org Kazda and Associates 1243

level was 8.0% (64 mmol/mol) at studyentry. Concomitant metformin use wassimilar among the treatment groups(ranging from 85.7 to 87.5%).
Glucose-Related EfficacyMeasurementsIn the phase 2a study, after 12 weeks oftreatment, LS mean (90% CI) changefrom baseline for HbA1c level in thethree LY2409021 dose groups was sig-nificantly greater than that in the pla-cebo group: –0.83% (–1.28, –0.38)(–9.1 mmol/mol) for the 10-mg group,–0.65% (–0.93, –0.37) (–7.1 mmol/mol)for the 30-mg group, and –0.66% (–1.00,–0.31) (–7.2 mmol/mol) for the 60-mggroup (P = 0.03, P = 0.04, and P = 0.05,respectively). The change from baselinefor the placebo group was 0.11% (–0.44,0.65) (1.2 mmol/mol). The LS meanchanges from baseline in HbA1c valuesfor all LY2409021 dose groups were sig-nificantly greater compared with thoseof the placebo group from week 6through week 12 (Fig. 1A). In the phase2b study, after 24 weeks of treatment,10 and 20 mg LY2409021 produced sta-tistically significantly lower (P , 0.001)HbA1c values than placebo (Fig. 1B). TheLS mean (90% CI) change from baselinefor HbA1c value was –0.92% (–1.12,–0.73) (–10.1 mmol/mol) at 20 mg,–0.78% (–0.97, –0.58) (–8.5 mmol/mol)at 10 mg, –0.45% (–0.65, –0.25)(–4.9 mmol/mol) at 2.5 mg, and–0.15% (–0.37, 0.06) (–1.6 mmol/mol) forthe placebo group. A small increase inHbA1c level was seen from week 12 tothe end of the active treatment period(week 24) in the 10- and 20-mg groups(Fig. 1B).MMRMwas used for the primaryanalysis of HbA1c levels for both studies.The ANCOVA (last observation carried for-ward) analysis demonstrated a greatermagnitude of reduction in HbA1c levelacross treatment groups (not shown)than the MMRM analysis. Nonetheless,the results for the MMRM and ANCOVAanalyses were generally similar.In the phase 2b study, one-third of the
20-mg treatment group achieved HbA1clevels #6.5% (48 mmol/mol; P , 0.001),and approximately half achieved HbA1clevels ,7% (53 mmol/mol; P = 0.004)comparedwith theplacebo (SupplementalFig. 3B).In the phase 2a study, LY2409021 pro-
duced statistically and clinically signifi-cant reductions in fasting glucose levels
compared with placebo (Fig. 1C). The 30-and 60-mg dose groups showed reduc-tions (P , 0.05) in fasting glucose levelsthat were sustained throughout the ac-tive treatment period. The LS meanchange from baseline in fasting glucoselevels for the phase 2b study is shownin Fig. 1D. LY2409021 produced dose-dependent, statistically significantlygreater changes from baseline in fastingglucose levels than placebo; maximaldecreases occurred within 2 weeks ofdosing. A small increase in fasting glu-cose level was observed from week 12to the end of the active treatment pe-riod (week 24) in the 10- and 20-mgdose groups (Fig. 1D).
In the phase 2a study, the means of7-point SMBG levels (Fig. 2A) decreasedfrom baseline in all three LY2409021treatment groups at all pre- and post-meal times and at all visits but generallyincreased from baseline in the placebogroup. In the phase 2b study, at baseline(week 0), all treatment groups had sim-ilar fasting, preprandial, postprandial,and 0300 h mean blood glucose values(Fig. 2B). By study end point (week 24),blood glucose levels were lower for the10- and 20-mg LY2409021 doses thanfor the placebo group across the timepoints (Fig. 2B); the 20-mg groupshowed significantly lower glucoselevels than the placebo group at mostpreprandial and postprandial timepoints.
Non–Glucose-RelatedPharmacodynamic MeasurementsIn both studies, dose-dependent in-creases in fasting glucagon levels wereobserved with LY2409021 treatmentand appeared to plateau after;4weeksof treatment (Fig. 3). Mean changesfrom baseline in fasting glucagon levels(Fig. 3A, phase 2a study) were largest inthe 60-mg treatment group (4.5-fold in-crease at week 4). An apparent increasein fasting glucagon levels in the placebogroup at weeks 6–10 was in part the re-sult of a postanalytical error in a singlepatient’s samples. In the phase 2b study(Fig. 3B), the LS mean changes frombaseline in fasting glucagon levels werelargest in the 20-mg group, with a 4.5-fold increase at week 4 similar to that inthe phase 2a study. Fasting glucagonlevels returned to baseline in all treat-ment groups by the end of the post-treatment washout period (Fig. 3).
LY2409021 treatment also led todose-related higher levels of fasting to-tal GLP-1 than placebo did; fasting totalGLP-1 levels followed a pattern similarto that of fasting glucagon levels in bothstudies (Fig. 3C and D). Total fastingGLP-1 levels returned to baseline (Fig.3C) during the posttreatment washoutperiod in the phase 2a study (GLP-1 lev-els were not measured during washoutin the phase 2b study). There were nostatistically significant differences infasting active GLP-1 levels betweenLY2409021 treatment at any dose andplacebo for either study. Fasting insulinvalues were not significantly differentbetween LY2409021 treatment and pla-cebo (data not shown).
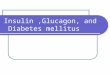
Safety and TolerabilityDose-related, reversible increases in se-rum ALT levels were observed duringactive treatment with LY2409021 (Fig. 4).In the phase 2a study, 4 of 85 patients hadALT levels three or more times the ULN: 1patient in the 30-mg group; 2 patients inthe 60-mg group; and 1 patient in the10-mg group, whose ALT level reachedfive or more times the ULN. There wasno dose-dependent change from baselinein GGT (data not shown). There were noclinically significant changes in bodyweight, lipid levels, blood pressure, heartrate, or electrocardiogram measurementsobserved in the phase 2a study.
In the phase 2b study, no placebo sub-jects and 8 of 191 patients receivingLY2409021 had ALT levels three or moretimes the ULN: 2 patients in the 2.5-mggroup, 4 patients in the 10-mg group, and2 patients in the 20-mg group. One pa-tient in the 20-mg group had an ALT levelfive or more times the ULN. No subjectwith elevated ALT exhibited concomitantelevation of bilirubin in either study, andno clinical signs or symptoms of liver in-jurywere reported. In all patients, the ALTlevels returned to baseline either withcontinued treatment or after cessationof treatment (Fig. 4). Changes in AST lev-els showed a similar dose-related trend aschanges in ALT levels but were less pro-nounced (data not shown). In the phase2b study, GGT values increased beginningat week 2 and continued to rise throughweek 24 in the 20-mg group. During the4-week posttreatment washout period,the GGT values of the 20-mg group beganto reverse but were still above baselinevalues and statistically significantly
1244 Efficacy and Safety of LY2409021 Diabetes Care Volume 39, July 2016

greater than those for the placebo group(data not shown). There were no dose-dependent changes from baseline in ALKor in total, direct, or indirect bilirubin ineither study (data not shown).In the phase 2b study, there were no
statistically significant differences inplasma lipid levels between any of theLY2409021 treatment groups and theplacebo group. In 8 of 12 biweekly visitsin the phase 2b study, there were nostatistically significant differences in LSmean change from baseline in SBP orDBP between any of the LY2409021treatment groups compared with theplacebo group. On four visits, the LSmean change from baseline for SBPand DBP was significantly greater forone or more LY2409021 dose groupscompared with the placebo group. After24 weeks of treatment, only the 2.5-mggroup showed a statistically significantdifference in LSmean change from base-line to end point in SBP relative to theplacebo group (LS mean difference,
4.9 mmHg; P = 0.038). The LS meanchange from baseline in DBP for all threeLY2409021 cohorts was ,1 mmHg atweek 24. Changes in body weight after24 weeks of treatment were as follows:placebo, –1.07 kg; 2.5 mg, –0.33 kg;10 mg, 0.55 kg; and 20 mg, 0.07 kg.Only the change for the 10-mg dosewas statistically significantly differentfrom the change for placebo (P = 0.033).
Adverse EventsThere were no severe treatment-emergentadverse events (TEAEs) or deaths report-ed in either study. The percentages ofpatients who experienced any TEAE inthe phase 2a study were similar acrosstreatment groups (Supplementary Table3). Nausea and hypoglycemia (4.7% ofpatients for each) were the most fre-quent TEAEs, but there was no dose de-pendency and no severe hypoglycemicevents observed in any group. Two seri-ous adverse events (SAEs) were report-ed: one subject in the 60-mg group had
cellulitis, which was considered not re-lated to study drug, and one patient inthe 10-mg group had elevated ALT, AST,and GGT levels. The investigator consid-ered the elevations related to studydrug; however, the subject had unde-tectable levels of LY2409021 at thetime of the event. Given the very longhalf-life of the study drug (;60 h), it ap-pears that the subject had not been re-cently compliant with treatment. BothSAEs were of moderate intensity andwere resolved.
In the phase 2b study, the percent-ages of patients who experienced anyTEAE (Supplementary Table 4) wereslightly higher in the LY2409021 groupsthan in the placebo group. The mostcommon TEAEs of all causes were ALTand AST level increases (6.7 and 5.1%,respectively) and headache (5.5%). A to-tal of seven patients reported SAEs: twopatients in the 10-mg group (AST levelincreased and atrial fibrillation), twopatients in the 20-mg group (ALT level
Figure 1—Time course for LSmean (90% CI) change from baseline in HbA1c level by week and treatment with LY2409021 or placebo over the 12-weekphase 2a study (A) and 24-week phase 2b study (B) treatment periods. Time course for LSmean (95% CI) change from baseline in fasting glucose levelby week and treatment with LY2409021 or placebo over the 12-week phase 2a study (C) and 24-week phase 2b study (D) treatment periods. *P,0.001 and †P , 0.05, compared with placebo. **P = 0.05, compared with placebo.
care.diabetesjournals.org Kazda and Associates 1245

increased and AST level increased), andthree placebo-treated patients (anklefracture [one patient], cholecystectomy[one patient], and gastritis and irondeficiency anemia [one patient]). Thethree SAEs related to increased ALTand/or AST levels were all asymptom-atic. The incidence of hypoglycemia(21) was low and not statistically differ-ent across drug treatment and placebogroups; 17 patients (7%) reported a totalof 20 events (placebo, 2 patients;2.5 mg, 4 patients; 10 mg, 6 patients;20 mg, 5 patients). None of the caseswas severe, and all cases were self-treated with an oral glucose source.
CONCLUSIONS
The role of insulin-glucagon imbalancecontinues to be of interest in under-standing the pathophysiology of type 2diabetes. Clinical data to support thepotential utility of glucagon receptor an-tagonism in the treatment of diabetes,however, have lagged (10,22). Over 10years has elapsed between publicationof the first clinical study of a glucagonreceptor antagonist (Bay 27-9955) (22)and the more recent studies of glucagonreceptor antagonists LY2409021 (11,12),LY2786890 (13), MK-0893 (14,15), PF-06691874 (16), LGD-6972 (17), and ISIS-GCGRRX (18).The current report details findings
from two studies that together composethe largest and longest experience eval-uating the safety and efficacy of a
glucagon receptor antagonist publishedto date. We have shown that once-dailytreatment with LY2409021 at doses of10–60 mg for up to 24 weeks producedstatistically significant and clinically rel-evant reductions in HbA1c levels andsecondary efficacy measures in patientswith type 2 diabetes without signifi-cantly increasing the risk of hypogly-cemia. The improvements in glycemicparameters in the present studies aregenerally consistent with the findingsof our previous studies with LY2409021(12), including reduction in glycemia atall time points during SMBG testing.This suggests that glucagon signalingcontributes to hyperglycemia in type 2diabetes in both the fasting and post-prandial states, as has been reportedby others (9,23). The reductions in fast-ing glucose and HbA1c in the currentstudies are less pronounced than thosethat have been reported with someother glucagon receptor antagonists(14,18). This may be due, in part, tothe fact that baseline HbA1c valueswere higher in those studies than inthe current report. Glucose-lowering ef-ficacy in the current studies is also likelyto have been reduced, in part, by ourefforts to find doses that are not associ-ated with aminotransferase elevations.Pharmacokinetic-pharmacodynamicmodeling using data from a study ofLY2409021-mediated antagonism ofexogenous hyperglucagonemia (11)suggests that the 20-mg dose used in
the current phase 2b study would pro-duce ;67% blockade of the gluca-gon receptor at steady state, andmaximal reductions in fasting glucoselevels were consistently produced onlyat doses of 60 mg and higher in a pre-vious study (12). Finally, the efficacy ob-served at the end of 24 weeks oftreatment in the phase 2b study was at-tenuated by the slight rise in HbA1c andfasting glucose levels after week 12 inthe 10- and 20-mg groups. Whetherthis reflects a waning of efficacy, an arti-fact of the higher discontinuation rateduring this phase of the study, or some-thing else is unclear.
LY2409021 produced dose-related in-creases in total GLP-1 levels that re-turned to baseline over the course ofthe 4-week posttreatment washoutperiod. Consistent with our previousfindings (12), levels of fasting activeGLP-1 did not change significantly withLY2409021 treatment. Both glucagonand GLP-1 are derived from the proglu-cagon precursor, and the parallel in-creases in total GLP-1 and glucagonsuggest the possibility that both gluca-gon and GLP-1 are secreted from pancre-atic a-cells as a result of an endocrinefeedback loop upon glucagon receptorblockade (24). Support for such a sys-temic feedback loop comes from resultsshowing that liver-selective “knockout”of the glucagon receptor inmice can pro-mote hyperglucagonemia (25). How-ever, the acute nature of the increase
Figure 2—LSmean (95% CI) change from baseline in SMBG level by time point and treatment with LY2409021 or placebo at end point week 12 (phase2a study) (A) and week 24 (phase 2b study) (B). The SMBG level at each visit consisted of blood glucose values collected before and 2 h after each ofthe three main meals and at bedtime (phase 2a study) or at 0300 h (phase 2b study) as described in RESEARCH DESIGN ANDMETHODS. *P, 0.05, comparedwith placebo at indicated time points (A).*P , 0.001 and †P , 0.05, compared with placebo at indicated time points (B).
1246 Efficacy and Safety of LY2409021 Diabetes Care Volume 39, July 2016

in circulating glucagon also suggeststhat partial blockade of the glucagonreceptor is most likely driven by a directsystemic feedback loop but might alsobe impacted by decreased overall glu-cagon clearance. Studies in mice haveprovided conflicting results regardingthe role of GLP-1 in the improved glu-cose metabolism observed in glucagonreceptor knockouts (26,27). Our resultssuggest that GLP-1 is unlikely to con-tribute to the efficacy of LY2409021because active hormone levels areunchanged.a-Cell hyperplasia has been raised
as a potential concern with pharmaco-logic antagonism of glucagon action(28). Mice with homozygous disruptionof the glucagon receptor gene developdramatic elevations in plasma gluca-gon levels (.1,000-fold), hyperplasiaof a-cells (29), and even neuroendo-crine tumors (30). However, mice with
heterozygous knockout of the glucagonreceptor gene have very modest in-creases in glucagon and do not developa-cell hyperplasia (29). In the presentphase 2a and 2b studies, fasting gluca-gon was increased in a dose-dependentmanner; maximummean increases were;4.5-fold. The changes in glucagonlevels seen with LY2409021 probablyreflect a direct pharmacologic effect ofglucagon receptor antagonism ratherthan an effect on a-cell number: the ef-fect occurred early, was nonprogressiveduring treatment, and reversed com-pletely during posttreatment washout.
Body weight, blood pressure, andlipid increases have been reported forother glucagon receptor antagonists(14,15). In the current studies, therewere no significant changes in plasmalipid levels with LY2409021 treatment.Changes in body weight and blood pres-sure were generally small and not dose
dependent, but some statistically signif-icant differences from baseline were ob-served in the larger phase 2b study.These parameters will continue to beof key interest in future studies. A studyto investigate the effect of LY2409021on 24-h blood pressure profiles as mea-sured by ambulatory blood pressuremeasurement is under way (31).
It is our view that hepatic safety re-mains the most important safety ques-tion facing the development of glucagonreceptor antagonists for the treatmentof type 2 diabetes. A key objective forboth studies reported here was to eval-uate the therapeutic margin betweendoses of LY2409021 that lower glucoselevels and those that increase serumaminotransferase levels. We were un-able to identify an efficacious dose ofLY2409021 that was not associatedwith an increase in mean serum amino-transferase levels. However, changes in
Figure 3—A: Time course for mean (6SE) change from baseline in fasting glucagon level (pmol/L) by week and treatment with LY2409021 or placeboover the 12-week phase 2a study treatment period. B: Time course for LS mean (95% CI) change from baseline in fasting glucagon level (pmol/L) byweek and treatment with LY2409021 or placebo over the 24-week phase 2b study treatment period. C: Time course for mean (6SE) change frombaseline in fasting total GLP-1 level (pmol/L) by week and treatment with LY2409021 or placebo over the 12-week phase 2a study treatment period.D: Time course for LS mean (95% CI) change from baseline in fasting total GLP-1 level (pmol/L) by week and treatment with LY2409021 or placeboover the 24-week phase 2b study treatment period. *P , 0.05, compared with placebo at indicated time points (A). *P , 0.001 and †P , 0.05,compared with placebo at indicated time points (B and D). No statistical analysis was conducted for fasting total GLP-1 level in C.
care.diabetesjournals.org Kazda and Associates 1247

ALT and AST levels were nonprogressiveover time, reversible with treatment dis-continuation, modest in magnitude, andnot associated with other signs or symp-toms of hepatic dysfunction. Changes inserum aminotransferases observed withLY2409021 are probably related directlyto antagonism of glucagon action; simi-lar, reversible increases in aminotrans-ferase levels have been seen in clinicalstudies with other small-molecule glu-cagon receptor antagonists (14–17),with the human glucagon receptormono-clonal antibody LY2786890 (13), and withan antisense oligonucleotide targetingglucagon receptor gene expression (18).The cellular mechanisms by which thesechanges occur remain unknown. Com-plete abrogation of glucagon signalinghas been reported to increase susceptibil-ity of mice to experimental liver injury(32,33). Hepatic steatosis has also beensuggested as a possible consequenceof blocking glucagon action (33). How-ever, results with pharmacologic orgenetic disruption of glucagon signal-ing in rodents have been contradictoryon this point (32,33,35–37). In light ofthese unresolved questions, we haveinitiated a 12-month placebo- and activecomparator–controlled hepatic safetystudy of LY2409021 that includes mag-netic resonance imaging to assess poten-tial changes in hepatic fat fraction (34).The results of this study could have sig-nificant implications for the future
development of LY2409021 and possiblyother glucagon receptor antagonists.
Publisher’s Note. An early version of thisarticle had been inadvertently accepted forpublication and published online before therevision process was completed. The AmericanDiabetes Association, the publisher of DiabetesCare, apologizes for any confusion this errormay have caused.
Acknowledgments. The authors thank theprincipal investigators and their clinical staff aswell as the many study participants who gener-ously agreed to participate in these clinical trials.The authors also thank the clinical operationsstaff for their excellent trial implementation andsupport. The authors thank Lakechie Turnipseed(Eli Lilly and Company) for contributions to studydesign, implementation, and management asthe clinical trial manager for the phase 2a study.The authors also thank Dr. Robert Panek (INCResearch, Raleigh, NC) who provided medicalwriting assistance.Duality of Interest. This study was sponsoredby Eli Lilly and Company and/or one of itssubsidiaries. C.M.K., R.P.K., P.G., H.F., D.E.W.,W.H.L., M.A.D., D.E.M., and T.A.H. are em-ployees and stockholders of Eli Lilly and Com-pany and/or one of its subsidiaries. Y.D. andC.N.L. were employees of Eli Lilly and Companyand/or one of its subsidiaries. A.J.L. was anemployee of the National Research Institute,Los Angeles, CA, at the time of this work and iscurrently retired. No other potential conflicts ofinterest relevant to this article were reported.AuthorContributions. For the phase 2a study,C.M.K., R.P.K., P.G., D.E.W., W.H.L., and M.A.D.contributed to the study concept and design,analysis and interpretation of data, and drafting
of the manuscript. C.S., C.N.L., and H.F. contrib-uted to drafting the manuscript and criticalrevisions. For the phase 2b study, C.M.K., R.P.K.,P.G., D.E.W., A.J.L., D.E.M., and T.A.H. contributedto the study concept and design, analysis andinterpretation of data, drafting the manuscript,and critical revisions. Y.D. contributed to the studyanalysis, interpretation of data, drafting the man-uscript, and critical revisions. The authors certifythatthismanuscriptrepresentsvalidworkandthatthis manuscript has not been published and is notbeing considered for publication elsewhere. Allauthors contributed to the writing and reviewprocess andapproved thefinalmanuscript. C.M.K.is the guarantor of this work and, as such, had fullaccess to all the data in the study and takesresponsibility for the integrity of the data andthe accuracy of the data analysis.Prior Presentation. The phase 2a study waspresented in part in poster form at the 72ndScientific Sessions of the American DiabetesAssociation, Philadelphia, PA, 8–12 June 2012,and at the 48th AnnualMeeting of the EuropeanAssociation for the Study of Diabetes, Berlin,Germany, 1–5 October 2012. The phase 2bstudy was presented in part in poster form atthe 73rd Scientific Sessions of the American Di-abetes Association, Chicago, IL, 21–25 June2013.
References1. Woerle HJ, Szoke E, Meyer C, et al. Mecha-nisms for abnormal postprandial glucose me-tabolism in type 2 diabetes. Am J PhysiolEndocrinol Metab 2006;290:E67–E772. Sloop KW, Michael MD, Moyers JS. Glucagonas a target for the treatment of type 2 diabetes.Expert Opin Ther Targets 2005;9:593–6003. Unger RH, Cherrington AD. Glucagonocentricrestructuring of diabetes: a pathophysiologicand therapeutic makeover. J Clin Invest 2012;122:4–12
Figure 4—A: Time course for mean (6SE) change from baseline in ALT level (units/L) by week and treatment with LY2409021 or placebo over the 12-week phase 2a study treatment period. TheULNs for ALT level were 43 units/L (dashed line, male) and 34 units/L (dotted line, female). B: Time coursefor LS mean change (95% CI) from baseline in ALT level (units/L) by week and treatment with LY2409021 or placebo over the 24-week phase 2b studytreatment period. Baseline ALT level = 32 units/L. *P , 0.05 and **P , 0.10, compared with placebo at indicated time points (A). *P , 0.05,compared with placebo at indicated time points (B).
1248 Efficacy and Safety of LY2409021 Diabetes Care Volume 39, July 2016

4. Muller WA, Faloona GR, Aguilar-Parada E,Unger RH. Abnormal alpha-cell function in di-abetes. Response to carbohydrate and proteiningestion. N Engl J Med 1970;283:109–1155. Hollander PM, Asplin CM, Palmer JP. Glucosemodulation of insulin and glucagon secretion innondiabetic and diabetic man. Diabetes 1982;31:489–4956. Ward WK, Best JD, Halter JB, Porte D Jr. Pro-longed infusion of somatostatin with glucagonreplacement increases plasma glucose and glu-cose turnover in man. J Clin Endocrinol Metab1984;58:449–4537. Dunning BE, Gerich JE. The role of alpha-celldysregulation in fasting and postprandial hyper-glycemia in type 2 diabetes and therapeutic im-plications. Endocr Rev 2007;28:253–2838. Gastaldelli A, Baldi S, Pettiti M, et al. Influenceof obesity and type 2diabeteson gluconeogenesisand glucose output in humans: a quantitativestudy. Diabetes 2000;49:1367–13739. Shah P, Vella A, Basu A, Basu R, SchwenkWF,Rizza RA. Lack of suppression of glucagon con-tributes to postprandial hyperglycemia in sub-jects with type 2 diabetes mellitus. J ClinEndocrinol Metab 2000;85:4053–405910. Bagger JI, Knop FK, Holst JJ, Vilsbøll T. Glu-cagon antagonism as a potential therapeutictarget in type 2 diabetes. Diabetes Obes Metab2011;13:965–97111. Tham LS, Abu-Raddad EJ, Lim CN. The glu-cagon receptor antagonist LY2409021 attenu-ates increases in hepatic glucose output (HGO)and blood glucose during hyperglucagonemia inhealthy male patients (Abstract 416-PP). Diabe-tes 2011;60(Suppl. 1):A11512. Kelly RP, Garhyan P, Raddad E, et al. Short-term administration of the glucagon receptorantagonist LY2409021 lowers blood glucose inhealthy people and in those with type 2 diabe-tes. Diabetes Obes Metab 2015;17:414–42213. Kelly RP, Garhyan P, Reynolds VL, et al.Glucagon receptor antibody LY2786890 re-duced glucose levels in type 2 diabetes mellituspatients (Abstract 106-LB). Diabetes 2015;64(Suppl.1A):LB2714. Engel SS, Xu L, Andryuk PJ, et al. Efficacy andtolerability of MK-0893, a glucagon receptor an-tagonist (GRA), in patients with type 2 diabetes(T2DM) (Abstract 309-OR). Diabetes 2011;60(Suppl. 1):A8515. Ruddy M, Pramanik B, Lunceford J, et al.Inhibition of glucagon-induced hyperglycemiapredicts glucose lowering efficacy of a glucagonreceptor antagonist, MK-0893, in type 2 diabe-tes (T2DM) (Abstract 311-OR). Diabetes 2011;60(Suppl. 1):A85–A86
16. Kazierad DJ, Bergman A, Tan B, Somayaji V,Lee DS, Rolph T. Pharmacokinetics (PK) andpharmacodynamics (PD) of PF-06291874 (PF),a glucagon receptor antagonist, in subjectswith T2DM (Abstract 1202-P). Diabetes 2015;64(Suppl. 1):A310–A31117. Vajda EG, Logan D, Lasseter K, et al. Phar-macokinetics and pharmacodynamics of theglucagon receptor antagonist LGD-6972 in amulti-dose clinical trial (Abstract 1193-P). Dia-betes 2015;64(Suppl. 1):A30818. MorganE, SmithA,Watts L, et al. ISIS-GCGRRX,an antisense glucagon receptor antagonist, causedrapid, robust, and sustained improvements in gly-cemic control without changes in BW, BP, lipids, orhypoglycemia in T2DM patients on stable metfor-min therapy (Abstract 109-LB). Diabetes 2014;63(Suppl. 1A):LB2819. Alberti KG, Zimmet PZ. Definition, diagnosisand classification of diabetes mellitus and itscomplications. Part 1: diagnosis and classificationof diabetes mellitus provisional report of a WHOconsultation. Diabet Med 1998;15:539–55320. Sloan JH, Siegel RW, Ivanova-Cox YT,Watson DE, Deeg MA, Konrad RJ. A novel high-sensitivity electrochemiluminescence (ECL)sandwich immunoassay for the specific quanti-tative measurement of plasma glucagon. ClinBiochem 2012;45:1640–164421. Expert Committee on the Diagnosis andClassification of Diabetes Mellitus. Report ofthe expert committee on the diagnosis and clas-sification of diabetes mellitus. Diabetes Care2003;26(Suppl. 1):S5–S2022. Petersen KF, Sullivan JT. Effects of a novelglucagon receptor antagonist (Bay 27-9955) onglucagon-stimulated glucose production in hu-mans. Diabetologia 2001;44:2018–202423. Baron AD, Schaeffer L, Shragg P, KoltermanOG. Role of hyperglucagonemia in mainte-nance of increased rates of hepatic glucose out-put in type II diabetics. Diabetes 1987;36:274–28324. Whalley NM, Pritchard LE, Smith DM,WhiteA. Processing of proglucagon to GLP-1 in pan-creatic a-cells: is this a paracrine mechanismenabling GLP-1 to act on b-cells? J Endocrinol2011;211:99–10625. Longuet C, Robledo AM, Dean ED, et al.Liver-specific disruption of the murine glucagonreceptor produces a-cell hyperplasia: evidencefor a circulating a-cell growth factor. Diabetes2013;62:1196–120526. Ali S, Lamont BJ, Charron MJ, Drucker DJ.Dual elimination of the glucagon and GLP-1 re-ceptors in mice reveals plasticity in the incretinaxis. J Clin Invest 2011;121:1917–1929
27. Gu W, Winters KA, Motani AS, et al. Gluca-gon receptor antagonist-mediated improve-ments in glycemic control are dependent onfunctional pancreatic GLP-1 receptor. Am JPhysiol Endocrinol Metab 2010;299:E624–E63228. Lefebvre PJ, Paquot N, Scheen AJ. Inhibitingor antagonizing glucagon: making progress indiabetes care. Diabetes Obes Metab 2015;17:720–72529. Gelling RW, Du XQ, Dichmann DS, et al.Lower blood glucose, hyperglucagonemia, andpancreatic alpha cell hyperplasia in glucagon re-ceptor knockout mice. Proc Natl Acad Sci U S A2003;100:1438–144330. Yu R, Dhall D, Nissen NN, Zhou C, Ren SG.Pancreatic neuroendocrine tumors in glucagonreceptor-deficient mice. PLoS One 2011;6:e2339731. Eli Lilly and Company. A study of LY2409021on blood pressure and pulse rate in participantswith type 2 diabetes mellitus. In: ClinicalTrials.gov[Internet]. Bethesda, MD, National Library of Med-icine, 2014. Available from http://clinicaltrials.gov/show/NCT02091362 NLM Identifier NCT02091362.Accessed 17 March 201632. Sinclair EM, Yusta B, Streutker C, et al. Glu-cagon receptor signaling is essential for controlof murine hepatocyte survival. Gastroenterol-ogy 2008;135:2096–210633. Conarello SL, Jiang G, Mu J, et al. Glucagonreceptor knockout mice are resistant to diet-induced obesity and streptozotocin-mediatedbeta cell loss and hyperglycaemia. Diabetologia2007;50:142–15034. Eli Lilly and Company. A phase 2, double-blind, placebo-controlled trial to evaluate thesafety and efficacy of LY2409021 compared tositagliptin in subjects with type 2 diabetes mel-litus. In: ClinicalTrials.gov [Internet]. Bethesda,MD, National Library of Medicine, 2014. Availablefrom http://clinicaltrials.gov/show/NCT02111096NLM Identifier NCT00004451. Accessed 12 January201635. Liang Y, Osborne MC, Monia BP, et al. Re-duction in glucagon receptor expression by anantisense oligonucleotide ameliorates diabeticsyndrome in db/db mice. Diabetes 2004;53:410–41736. Hancock AS, Du A, Liu J, Miller M, May CL. Glu-cagon deficiency reduces hepatic glucose produc-tion and improves glucose tolerance in adultmice. Mol Endocrinol 2010;24:1605–161437. Sloop KW, Cao JX, Siesky AM, et al. Hepaticand glucagon-like peptide-1-mediated reversalof diabetes by glucagon receptor antisense oligo-nucleotide inhibitors. J Clin Invest 2004;113:1571–1581
care.diabetesjournals.org Kazda and Associates 1249