Embed Size (px)
Citation preview

Evaluation of HCHDcommunity behavior health program 2005 - 2006
Evaluators:- Charles Begley- Scott Hickey- Britta Ostermeyer- Ann Teske
- Thien Vu
- Julia Wolf
- Mark Kunik

Outline
Background Objectives Evaluation framework and methods Results Discussion and recommendation

Background HCHD:- serves around 300,000
individuals/year, most are low income and/or underinsured
- Operates BTGH, Lyndon Johnson GH, Quentin Mease Community Hospital, 11 CHCs, 7 school-based clinics, a healthcare program for the homeless, a center for HIV/AIDS (Thomas st.) and a dental center
CBHP:- First launched by HCHD in
3 CHCs- Officially created in July
2005,- CBHP team includes
psychiatrists, psychotherapists, counselors, residents and med students in 11 HCHD CHCs, 5 partner centers, 2 school-based clinics

Background
Why CBHP?- Estimates: 20,000 children and
84,000 adults in Harris County needed mental health services in 2004
- There was only one District’s outpatient clinic at BTGH at the time
- Only 8,800 adults and 1,700 children were served
- Average appointment time: 6 months
CBHP objectives:1. to redirect BH patients to
community clinics (integrated care)
2. to provide specific BH services 3. to develop & provide
educational services for PCPs4. to consult and coordinate with
primary care providers

Evaluation framework

Evaluation objectives
Process evaluation• to describe major resources and features of the
program• to describe services provided and patients served
Preliminary impact evaluation• to evaluate initial impact on access, BH outcomes,
provider satisfaction and costs

MethodsVariables Measurement
methodData sources
Program resources and features:- Number and type of CBHP staff- Resources used
- simple calculation- aggregated
- Project documents- Monitoring report
Amount and type of services provided & characteristics of patient served: - # of patient seen by provider & patient types- demographic characteristics- types of counseling sessions by individual/group/family/total
- aggregated (using patient-coded medical records)
- CBHP integrated database
Initial impacts of the program:- Provider satisfaction
- Accessibility- Health outcomes
- Provider survey
- Pre-post analyses- BASIS-24 analysis
- 100 questionnaires PCPs, psychiatrists and BH therapists- HCHD database- patient’s BASIS-24 assessments

ResultsProgram resources and featuresProgram resources and features
Originally proposed:- hire 1 Prog. Director, 4
licensed Social workers & 1 psychiatrist
- Involve 4 HCHD’s CHC and 3 private community clinics
Actually implemented- As proposed- Additional: 1 project
coordinator, 6 social workers and 10 part time psychiatrists
- Involve all 11 HCHD’s CHC, 4 private community clinics
- Additional education sessions: teleconference lectures, psychotherapy referrals, DVD and audio tape lectures

2,895 patients seen - 2075 females and 820 males - 801 by psychiatrists, 1,824 by
BH therapists- 2,363 MH patients, 6 substance
abuse, 336 both- 34 referred by project Insight,
12 referred by Council on Alcohol & Drug Houston
- 75 < 6 years; 137 ages 7-12; 169 from 13-18; 2,376 from 19-64; 128 > 65
- 835 African American, 58 Asian, 754 Caucasian, 1225 Hispanic; 3 American Indian; 17 others
- 55 Katrina and 10 Rita victims
7,392 counseling sessions:- 1,696 psychiatry; 3,342
individual counseling, 562 group counseling, 830 families and 95 phone sessions
ResultsServices provided & patient characteristicsServices provided & patient characteristics
Timeframe: July 2005 – May 2006
ResultsInitial impact on patient’s health BASIS-24:- 24 questions- domains are psychiatric and
substance abuse functioning: depression, relationship, self-harm, emotional ability, psychosis and substance abuse
- administered at least twice in the study period with the follow-up assessment at least 30 days after the first
- responses scored using weighted average algorithm that give overall score for each assessment
Results:- Significant improvement
detected in overall score (p <.000) and 4 out of 6 domain scores: depression, self-harm; emotional lability and substance abuse (p<.000)
- Average improvement percent change: 26% in overall score, 30% in depression, 75% in self-harm, 37% in emotional lability and 72% in substance abuse scores
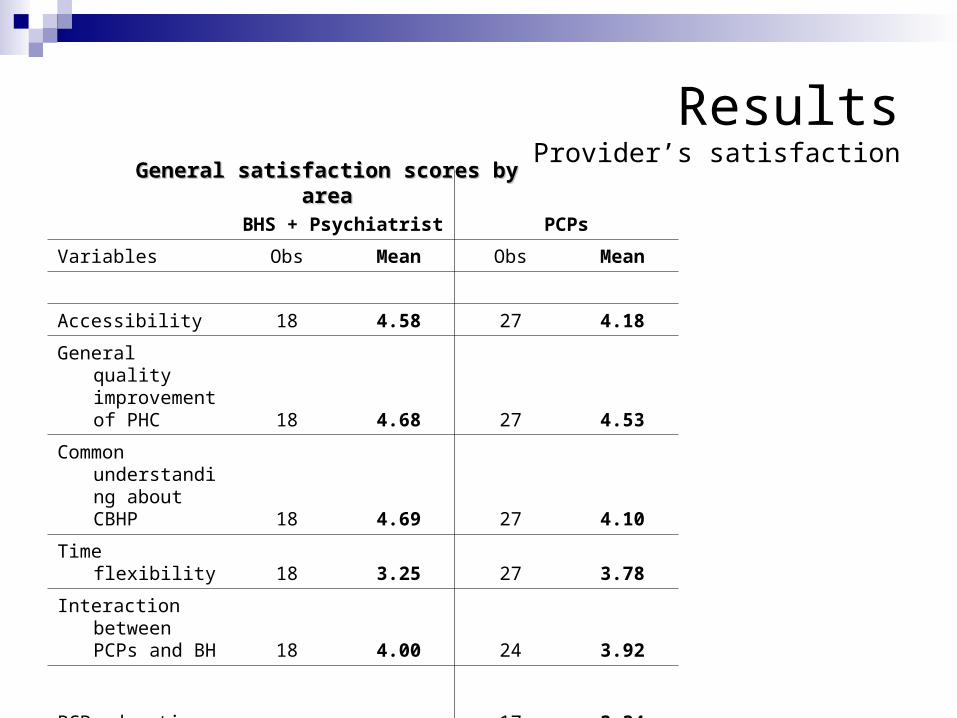
ResultsProvider’s satisfaction
BHS + Psychiatrist PCPs
Variables Obs Mean Obs Mean
Accessibility 18 4.58 27 4.18
General quality improvement of PHC 18 4.68 27 4.53
Common understanding about CBHP 18 4.69 27 4.10
Time flexibility 18 3.25 27 3.78
Interaction between PCPs and BH 18 4.00 24 3.92
PCP education 17 3.34
General satisfaction scores by areaGeneral satisfaction scores by area

ResultsProvider satisfaction – service accessibilityProvider satisfaction – service accessibility
VariableCombined
score BH + Psy PCPs
Poor accessibility prior to CBHP 4.42 4.56 4.33
Improved accessibility by CBHP 4.47 4.78 4.26
CBHP reduced ER visit 4.40 4.61 4.26
CBHP reduced length of time for accessing
BH services 4.16 4.44 3.96
CBHP helps improve access care in
appropriate time frame 4.24 4.50 4.07
Satisfaction scores on accessibility by provider type

ResultsProvider satisfaction - quality of careProvider satisfaction - quality of care
Variable BHS + Psy PCPs
BHC necessary for PHC 4.94 4.70
BHC improve adherence to treatment 4.89 4.67
BHC offered by CBHP improve general quality of PHC 4.72 4.44
CBHP enhances PCPs’ ability to provide BHC 4.44 4.52
BHC enhances quality of the clinics 4.39 4.30
Mean scores on quality of care variables by provider type

ResultsProvider satisfaction – time flexibility and staffingProvider satisfaction – time flexibility and staffing
Mean scores on time flexibility reported by providers
Variable Mean Min Max
Time flexibility of BH physicians 3.25 1 5
Time flexibility of PCPs 3.78 2 5
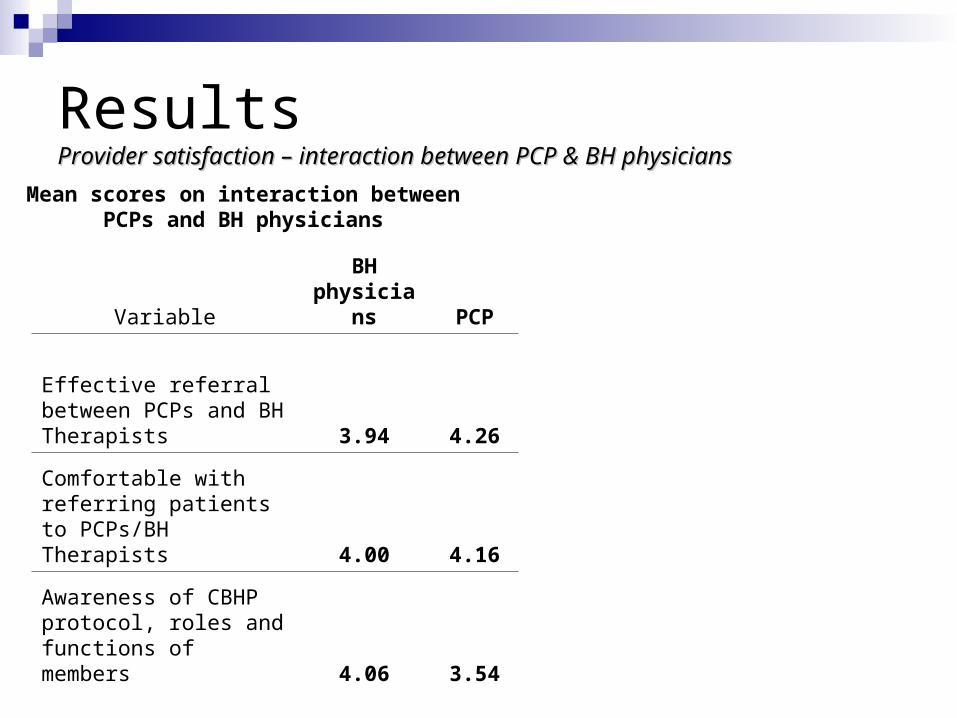
ResultsProvider satisfaction – interaction between PCP & BH physiciansProvider satisfaction – interaction between PCP & BH physicians
VariableBH
physicians PCP
Effective referral between PCPs and BH Therapists 3.94 4.26
Comfortable with referring patients to PCPs/BH Therapists 4.00 4.16
Awareness of CBHP protocol, roles and functions of members 4.06 3.54
Mean scores on interaction between PCPs and BH physicians
ResultsProvider satisfaction – Educational activities and materials for PCPsProvider satisfaction – Educational activities and materials for PCPs
Purpose: to improve PCP’s capacity to provide BH at CHC through on-going trainings and on-site consultation
Materials: teleconference lectures, DVD + audio tapes Result: negative • 52% of PCPs have not received any educational
materials• mean score on effectiveness of PCP education
session was 3.34, lower than cut point

ResultsProvider satisfaction – Common vision, understanding and overall satisfactionProvider satisfaction – Common vision, understanding and overall satisfaction
Variable Combined BH physicians PCP
Share sense of responsibility 4.40 4.78 4.15
Common treatment goals 4.40 4.67 4.22
Understanding of roles and responsibility 4.33 4.67 4.11
Formal and informal interaction 4.20 4.72 3.85
Share knowledge 4.38 4.78 4.11
Common vision/philosophy of CBHP 4.19
Total (combined score) 4.31 4.50 4.10
Mean scores on common vision, understanding by provider type

Results Service patternsService patterns

Results Service patternsService patterns
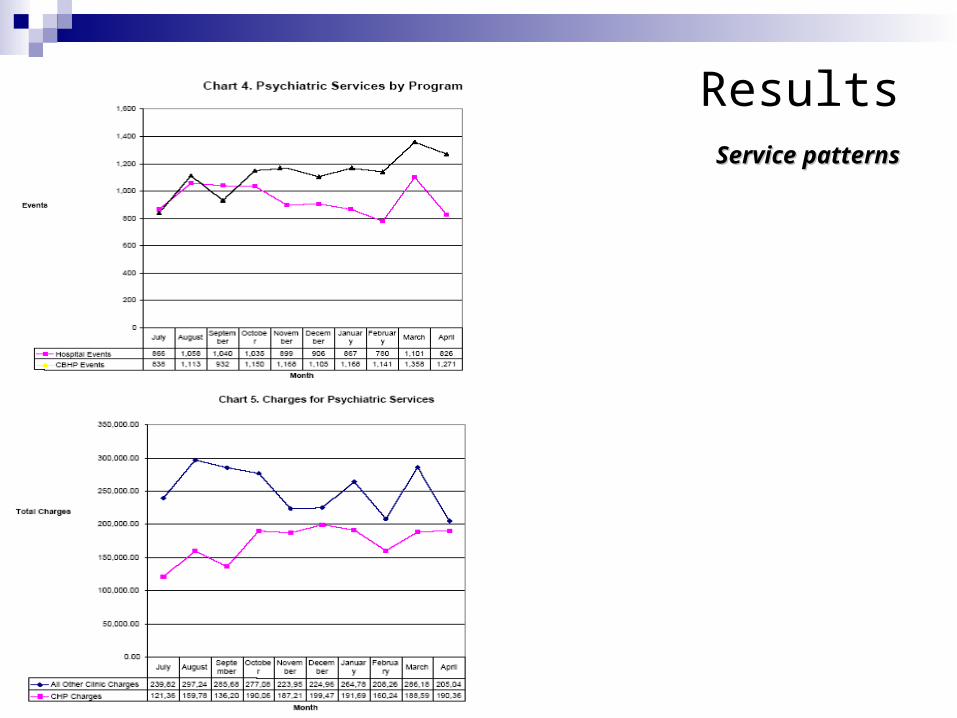
Results Service patternsService patterns

Conclusions & recommendations CBHP has achieved many
of its implementation objectives
Impacts of CBHP on patients’ health, accessibility to BH services were positive
Patient flow for BH was initially re-directed to lower cost and more convenient settings
BH providers’ working schedules should be more flexible
Interaction between PCPs and BH providers should be further facilitated for smoother operation of CBHP
More BH staff is needed More rigorous evaluation
plan should be developed Educational efforts should
be improved

















![[Roland J. Teske] Paradoxes of Time in Saint Augus(Bookos.org)](https://img.pdfslide.net/doc/110x75/55cf932b550346f57b9c5976/roland-j-teske-paradoxes-of-time-in-saint-augusbookosorg.jpg)











