Embed Size (px)
Citation preview
Evaluation of iris recognition systemfor wavefront-guided laser in situ keratomileusis
for myopic astigmatismSudipta Ghosh, DOMS, DNB, Terry A. Couper, DipAppSc, Ecosse Lamoureux, PhD, Vishal Jhanji, MD,
Hugh R. Taylor, FRANZCO, Rasik B. Vajpayee, MS, FRCSEd, FRANZCO
PURPOSE: To evaluate the visual and refractive outcomes of wavefront-guided laser in situ kerato-mileusis (LASIK) using an iris recognition system for the correction of myopic astigmatism.
SETTING: Centre for Eye Research Australia, Melbourne Excimer Laser Research Group, and RoyalVictorian Eye and Ear Hospital, East Melbourne, Victoria, Australia.
METHODS: A comparative analysis of wavefront-guided LASIK was performed with an iris recog-nition system (iris recognition group) and without iris recognition (control group). The main param-eters were uncorrected visual acuity (UCVA), best spectacle-corrected visual acuity, amount ofresidual cylinder, manifest spherical equivalent (SE), and the index of success using the Alpinsmethod of astigmatism analysis 1 and 3 months postoperatively. A P value less than 0.05 wasconsidered statistically significant.
RESULTS: Preoperatively, the mean SE was �4.32 diopters (D) G 1.59 (SD) in the iris recognitiongroup (100 eyes) and �4.55 G 1.87 D in the control group (98 eyes) (P Z .84). At 3 months, themean SE was �0.05 G 0.21 D and �0.20 G 0.40 D, respectively (P Z .001), and an SE withinG0.50 D of emmetropia was achieved in 92.0% and 85.7% of eyes, respectively (P Z .07). At3 months, the UCVA was 20/20 or better in 90.0% and 76.5% of eyes, respectively. A statisticallysignificant difference in the amount of astigmatic correction was seen between the 2 groups(P Z .00 and P Z .01 at 1 and 3 months, respectively). The index of success was 98.0% in theiris recognition group and 81.6% in the control group (P Z .03).
CONCLUSION: Iris recognition software may achieve better visual and refractive outcomes in wave-front-guided LASIK for myopic astigmatism.
J Cataract Refract Surg 2008; 34:215–221 Q 2008 ASCRS and ESCRS
ARTICLE
The safety and efficacy of laser in situ keratomileusis(LASIK) for the correction of various types of refrac-tive errors have been established in recent years, andLASIK has emerged as the procedure of choice forthe surgical correction of myopia andmyopic astigma-tism.1–3 Development of new surgical techniques andimprovements in laser systems3 and microkeratomes4
have paralleled a significant increase in the number ofpersons who have LASIK.5–7
Residual refractive error after LASIK often occurs asthe result of misalignment in the axes of treatmentcaused by rotation of the eye when the patient changesfrom a seated to a supine position.8–12 To eliminate orminimize the adverse effect of minor eye movementsdue to cyclorotation during LASIK, new softwareusing iris recognition technology was recently intro-duced. This software accounts for cyclorotational eye
Q 2008 ASCRS and ESCRS
Published by Elsevier Inc.
movements by directing the laser onto the precisearea of the cornea to allow pinpoint accuracy duringthe treatment.
In this study, we evaluated the visual outcomes ofwavefront-guided LASIK using the iris recognitionsystem for correction of myopic astigmatism andwhether this technology is beneficial in correctinghigh astigmatic errors and achieves a high index ofsurgical success.
PATIENTS AND METHODS
Study Design and Participants
This prospective study comprised 100 eyes of 50 consecu-tive patients who had wavefront-guided LASIKwith the useof the iris recognition technology from July 2006 to Septem-ber 2006 (iris recognition group). For comparison, 98 eyes of49 patients were randomly selected retrospectively from the
0886-3350/08/$dsee front matter 215doi:10.1016/j.jcrs.2007.09.022

216 IRIS RECOGNITION SYSTEM FOR WAVEFRONT-GUIDED LASIK
computerized data of 1310 patients who had LASIK withoutthe iris recognition system (control group) from September2005 to September 2006. In both groups, patients olderthan 18 years who had stable refractive correction for at least12 months were eligible to participate in the study. Otherinclusion criteria were a best spectacle-corrected visual acu-ity (BSCVA) of 20/60 or better in both eyes and stable kera-tometry after discontinuation of soft contact lenses and hardcontact lenses for at least 2 weeks and 1 month, respectively.Patients were excluded if they did not meet these criteria orhad a history of keratoconus, ocular surgery, or trauma.Informed consent was obtained from all patients. The studyprotocol and informed consent were approved by the Hu-man Research Ethics Committee of the Royal Victorian Eyeand Ear Hospital and the Melbourne Excimer Laser GroupEthics Committee. The study adhered to the tenets of theDeclaration of Helsinki.
Preoperatively, all patients were given a complete oph-thalmic examination including visual acuity, manifest andcycloplegic refractions, slitlamp biomicroscopy, applanationtonometry, and posterior segment evaluation with dilatedpupils. The preoperative assessment also included keratom-etry, corneal topography (Orbscan IIz, Bausch & Lomb),Zywave aberrometry (Bausch & Lomb) using wavefronttechnology, and ultrasonic pachymetry. The uncorrectedvisual acuity (UCVA) and BSCVA were recorded using log-MAR and Snellen charts.
Surgical Technique
All 99 patients had LASIK in both eyes at the same sitting.Patients were given 1 drop of ciprofloxacin 0.3% (Ciloxan)approximately 20 minutes before surgery. The skin areasurrounding the eye was prepared with povidone–iodine10%, and a sterile drape was used to cover the eyelashes.A nonguarded speculumwas then placed in the eye. Centralcorneal pachymetry was measured using ultrasound pachy-metry (Sonogage). Two 2.0 mm circular gentian violet markswere placed on the peripheral cornea to aid realignment af-ter the flap creation. The flap was then created using anAmadeus 1 microkeratome (AMO) with a 140 mm head,640 mm Hg controlled vacuum, 12000 oscillation, and3.5 mm advance rate. If the treatment was wavefront withiris recognition, the room and laser lights were dimmed toincrease the pupil diameter and the patient’s iris imagewas acquired. The active Zyoptix 100 tracker system wasaligned, with the center of the entrance pupil used as the
Accepted for publication September 2, 2007.
From the Centre for Eye Research Australia and University of Mel-bourne (Ghosh, Couper, Lamoureux, Taylor, Vajpayee), the Mel-bourne Excimer Laser Research Group (Couper, Taylor, Vajpayee),and the Royal Victorian Eye and Ear Hospital (Ghosh, Jhanji, Taylor,Vajpayee), East Melbourne, Victoria, Australia.
No author has a financial or proprietary interest in any material ormethod mentioned.
Corresponding author: Rasik B. Vajpayee, MS, FRCSEd, FRANZCO,Centre for Eye Research Australia, University of Melbourne, 32,Gisborne Street, East Melbourne, Victoria 3002, Australia. E-mail:[email protected].
J CATARACT REFRACT SUR
reference point for acquisition, and laser ablation wasperformed. After surgery, patients were started on a regimenof ciprofloxacin and fluorometholone acetate 1 drop 4 timesa day for 15 days; the drops and lubricants (carboxymethyl-cellulose sodium, 5 mg/mL) were then tapered over1 month.
Postoperative Follow-up
Patients were examined after 24 hours and at 1 and 3months. All parameters, including UCVA and BSCVA,were assessed at the 1-month and 3-month follow-ups. Aroutine slitlamp examination was performed, and theLASIK-treated eyes were evaluated for visibility of the flapedge, flap clarity, interface debris or epithelial cells, depositsand gaps, regularity of the epithelial surface, stromal edema,and haze at the interface.
The parameters evaluated and compared postoperativelyin both groups included gain or loss of 1 or 2 lines of visualacuity from the preoperative BSCVA, residual sphere, cylin-der, and mean spherical equivalent (SE) in both groups. Theintended correction was compared with the achieved correc-tion in both groups. The safety and efficacy indices weredefined as the mean postoperative BSCVA/mean preopera-tive BSCVA and the mean postoperative UCVA/mean pre-operative BSCVA, respectively. The surgical index ofsuccess in both groups was also determined using the Alpinsmethod of astigmatism analysis, which is based on the tar-geted induced astigmatism, surgically induced astigmatism(SIA), and difference vector.
Complications and adverse effects after the surgical proce-dure were recorded.
Statistical Analysis
Descriptive statistical analyses were performed to charac-terize the patients’ demographic and clinical data at baseline.A repeated-measures analysis of variance was used to com-pare the effect of wavefront-guided LASIK on specific clini-cal parameters between the iris recognition and controlgroups at baseline and 1 and 3 months after surgery. Datawere analyzed using SPSS statistical software (version 14.0,SPSS Science).
RESULTS
Demographic Profile
All 99 patients in this study completed the 1-monthand 3-month follow-ups. The mean patient age was40.72 years G 7.65 (SD) (range 29 to 62 years) in theiris recognition group and 38.43 G 9.16 years (range22 to 60 years) in the control group (P Z .18). Therewere 30 women and 20 men in the iris recognitiongroup and 34 women and 15 men in the control group(P Z .49).
Preoperative Refractive Data
Preoperatively, there was no statistically significantdifference in the meanmanifest sphere (P Z .75) or themean astigmatic error (P Z .44) between the 2 groups.Themean baseline SEwas�4.32 G 1.59 diopters (D) in
G - VOL 34, FEBRUARY 2008
217IRIS RECOGNITION SYSTEM FOR WAVEFRONT-GUIDED LASIK
the iris recognition group and �4.55 G 1.87 D in thecontrol group (P Z .84) (Table 1).
Postoperative Refractive Data
There was a significant improvement in themean SEbetween baseline and 1 and 3 months postoperativelyin both groups (P Z .00). There was no significant dif-ference between 1- and 3-month data in either group(P Z .36, iris recognition; P Z .10, control).
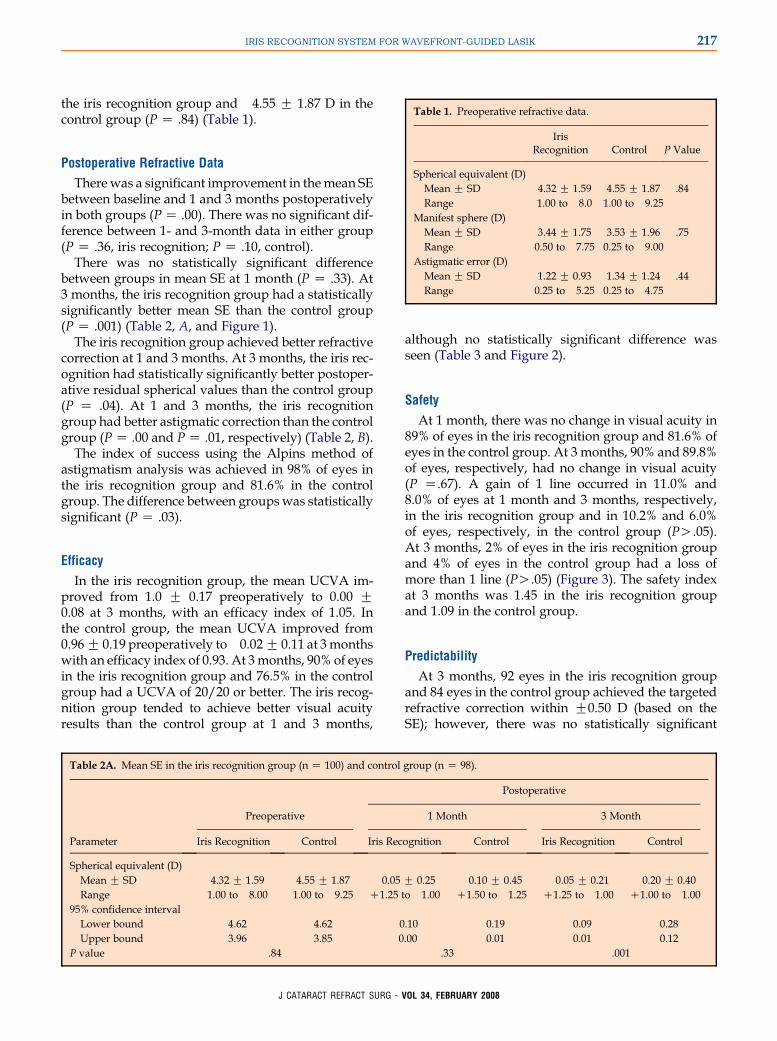
There was no statistically significant differencebetween groups in mean SE at 1 month (P Z .33). At3 months, the iris recognition group had a statisticallysignificantly better mean SE than the control group(P Z .001) (Table 2, A, and Figure 1).
The iris recognition group achieved better refractivecorrection at 1 and 3 months. At 3 months, the iris rec-ognition had statistically significantly better postoper-ative residual spherical values than the control group(P Z .04). At 1 and 3 months, the iris recognitiongroup had better astigmatic correction than the controlgroup (P Z .00 and P Z .01, respectively) (Table 2, B).
The index of success using the Alpins method ofastigmatism analysis was achieved in 98% of eyes inthe iris recognition group and 81.6% in the controlgroup. The difference between groupswas statisticallysignificant (P Z .03).
Efficacy
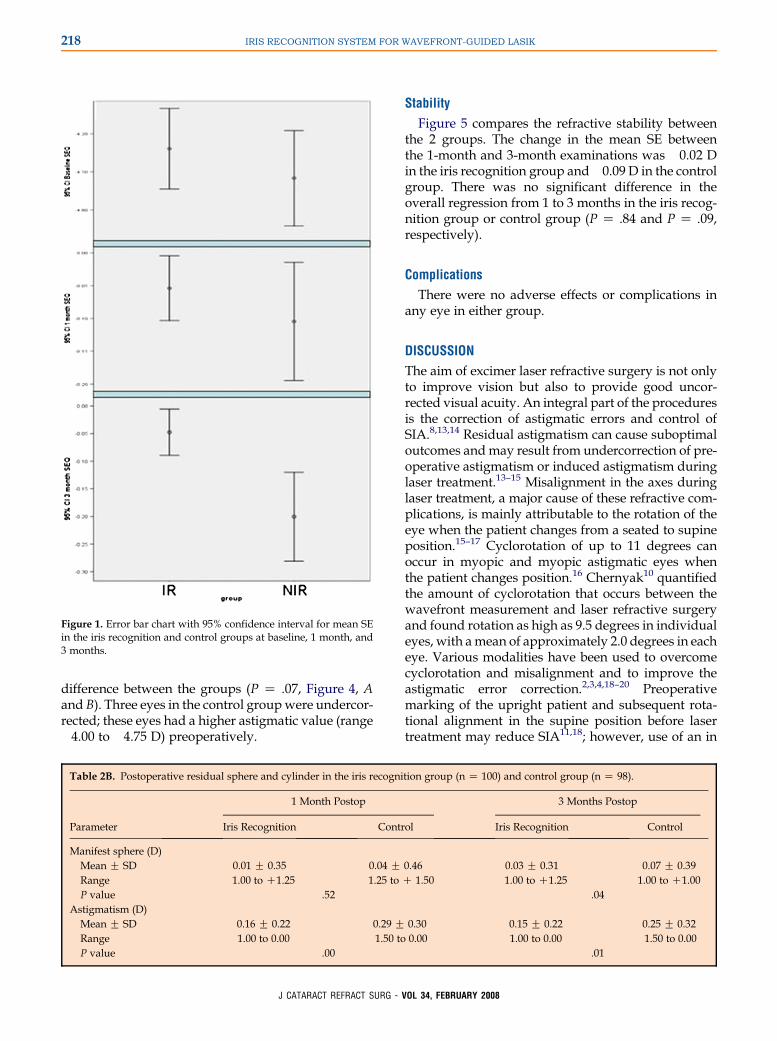
In the iris recognition group, the mean UCVA im-proved from 1.0 G 0.17 preoperatively to 0.00 G0.08 at 3 months, with an efficacy index of 1.05. Inthe control group, the mean UCVA improved from0.96 G 0.19 preoperatively to�0.02 G 0.11 at 3monthswith an efficacy index of 0.93. At 3months, 90% of eyesin the iris recognition group and 76.5% in the controlgroup had a UCVA of 20/20 or better. The iris recog-nition group tended to achieve better visual acuityresults than the control group at 1 and 3 months,
although no statistically significant difference wasseen (Table 3 and Figure 2).
Safety
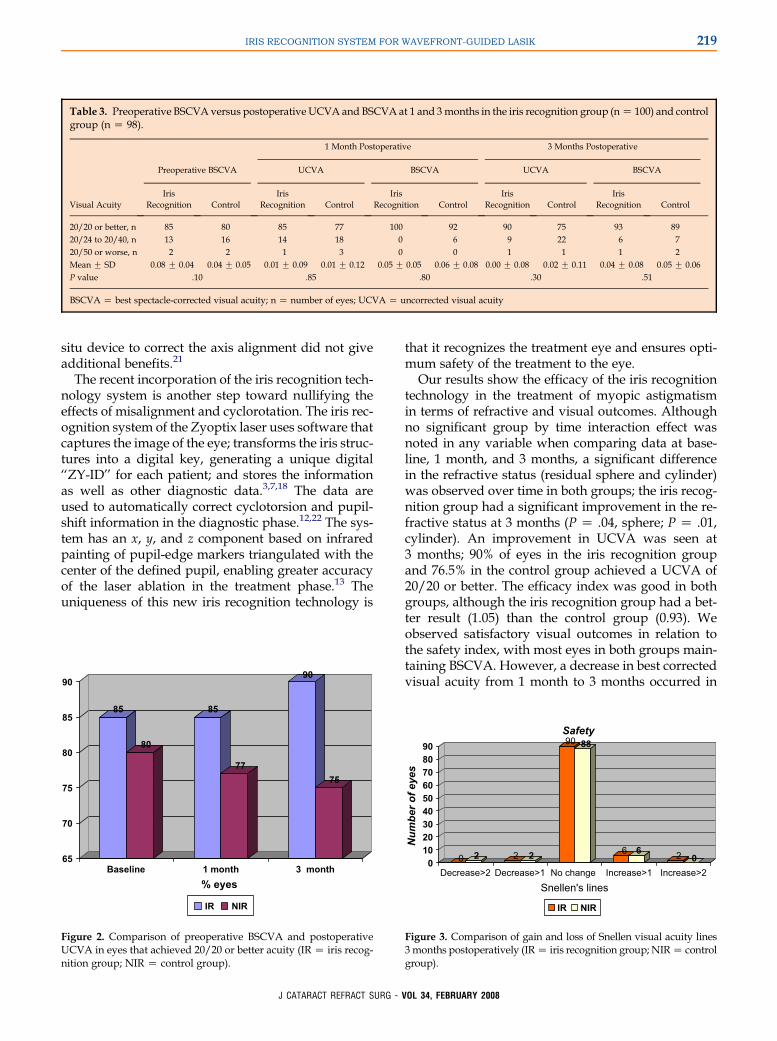
At 1 month, there was no change in visual acuity in89% of eyes in the iris recognition group and 81.6% ofeyes in the control group. At 3 months, 90% and 89.8%of eyes, respectively, had no change in visual acuity(P Z.67). A gain of 1 line occurred in 11.0% and8.0% of eyes at 1 month and 3 months, respectively,in the iris recognition group and in 10.2% and 6.0%of eyes, respectively, in the control group (PO.05).At 3 months, 2% of eyes in the iris recognition groupand 4% of eyes in the control group had a loss ofmore than 1 line (PO.05) (Figure 3). The safety indexat 3 months was 1.45 in the iris recognition groupand 1.09 in the control group.
Predictability
At 3 months, 92 eyes in the iris recognition groupand 84 eyes in the control group achieved the targetedrefractive correction within G0.50 D (based on theSE); however, there was no statistically significant
Table 1. Preoperative refractive data.
IrisRecognition Control P Value
Spherical equivalent (D)Mean G SD �4.32 G 1.59 �4.55 G 1.87 .84Range �1.00 to �8.0 �1.00 to �9.25
Manifest sphere (D)Mean G SD �3.44 G 1.75 �3.53 G 1.96 .75Range �0.50 to �7.75�0.25 to �9.00
Astigmatic error (D)Mean G SD �1.22 G 0.93 �1.34 G 1.24 .44Range �0.25 to �5.25�0.25 to �4.75
Table 2A. Mean SE in the iris recognition group (n Z 100) and control group (n Z 98).
Postoperative
Preoperative 1 Month 3 Month
Parameter Iris Recognition Control Iris Recognition Control Iris Recognition Control
Spherical equivalent (D)Mean G SD �4.32 G 1.59 �4.55 G 1.87 �0.05 G 0.25 �0.10 G 0.45 �0.05 G 0.21 �0.20 G 0.40Range �1.00 to �8.00 �1.00 to �9.25 C1.25 to �1.00 C1.50 to �1.25 C1.25 to �1.00 C1.00 to �1.00
95% confidence intervalLower bound �4.62 �4.62 �0.10 �0.19 �0.09 �0.28Upper bound �3.96 �3.85 0.00 �0.01 �0.01 �0.12
P value .84 .33 .001
J CATARACT REFRACT SURG - VOL 34, FEBRUARY 2008
218 IRIS RECOGNITION SYSTEM FOR WAVEFRONT-GUIDED LASIK
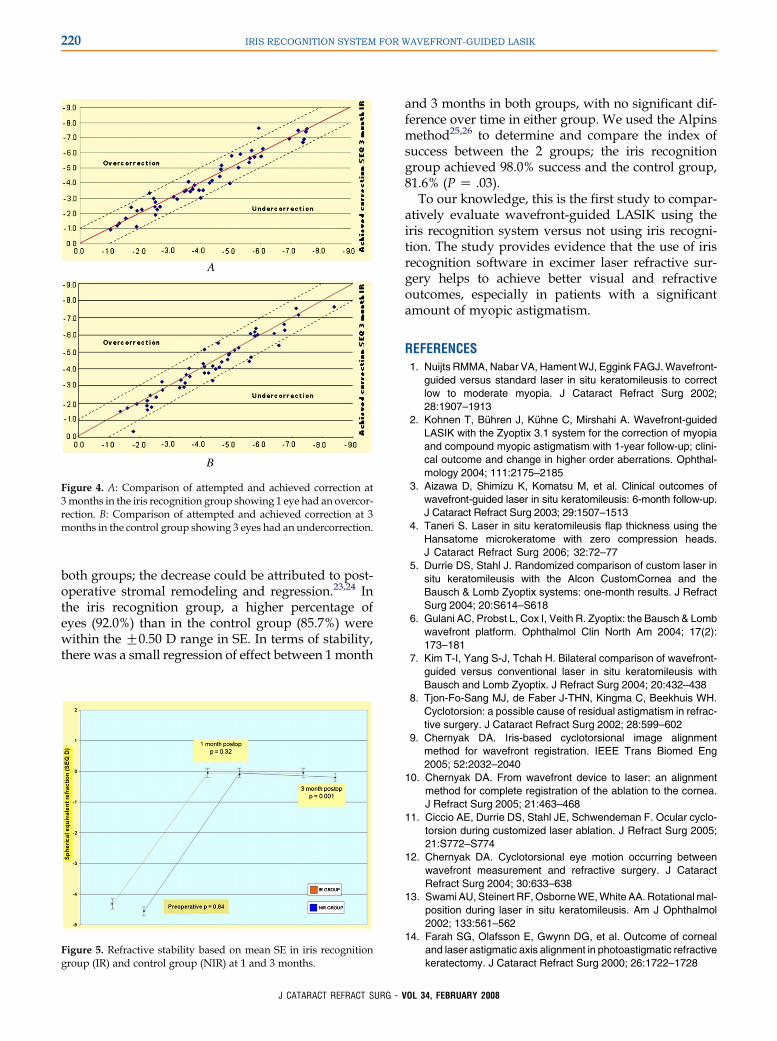
difference between the groups (P Z .07, Figure 4, Aand B). Three eyes in the control groupwere undercor-rected; these eyes had a higher astigmatic value (range�4.00 to �4.75 D) preoperatively.
Figure 1. Error bar chart with 95% confidence interval for mean SEin the iris recognition and control groups at baseline, 1 month, and3 months.
Stability
Figure 5 compares the refractive stability betweenthe 2 groups. The change in the mean SE betweenthe 1-month and 3-month examinations was �0.02 Din the iris recognition group and�0.09 D in the controlgroup. There was no significant difference in theoverall regression from 1 to 3 months in the iris recog-nition group or control group (P Z .84 and P Z .09,respectively).
Complications
There were no adverse effects or complications inany eye in either group.
DISCUSSION
The aim of excimer laser refractive surgery is not onlyto improve vision but also to provide good uncor-rected visual acuity. An integral part of the proceduresis the correction of astigmatic errors and control ofSIA.8,13,14 Residual astigmatism can cause suboptimaloutcomes andmay result from undercorrection of pre-operative astigmatism or induced astigmatism duringlaser treatment.13–15 Misalignment in the axes duringlaser treatment, a major cause of these refractive com-plications, is mainly attributable to the rotation of theeye when the patient changes from a seated to supineposition.15–17 Cyclorotation of up to 11 degrees canoccur in myopic and myopic astigmatic eyes whenthe patient changes position.16 Chernyak10 quantifiedthe amount of cyclorotation that occurs between thewavefront measurement and laser refractive surgeryand found rotation as high as 9.5 degrees in individualeyes, with amean of approximately 2.0 degrees in eacheye. Various modalities have been used to overcomecyclorotation and misalignment and to improve theastigmatic error correction.2,3,4,18–20 Preoperativemarking of the upright patient and subsequent rota-tional alignment in the supine position before lasertreatment may reduce SIA11,18; however, use of an in
Table 2B. Postoperative residual sphere and cylinder in the iris recognition group (n Z 100) and control group (n Z 98).
1 Month Postop 3 Months Postop
Parameter Iris Recognition Control Iris Recognition Control
Manifest sphere (D)Mean G SD 0.01 G 0.35 0.04 G 0.46 0.03 G 0.31 �0.07 G 0.39Range �1.00 to C1.25 � 1.25 to C 1.50 �1.00 to C1.25 �1.00 to C1.00P value .52 .04
Astigmatism (D)Mean G SD �0.16 G 0.22 �0.29 G 0.30 �0.15 G 0.22 �0.25 G 0.32Range �1.00 to 0.00 � 1.50 to 0.00 �1.00 to 0.00 � 1.50 to 0.00P value .00 .01
J CATARACT REFRACT SURG - VOL 34, FEBRUARY 2008
219IRIS RECOGNITION SYSTEM FOR WAVEFRONT-GUIDED LASIK
Table 3. Preoperative BSCVA versus postoperative UCVA and BSCVA at 1 and 3months in the iris recognition group (n Z 100) and controlgroup (n Z 98).
1 Month Postoperative 3 Months Postoperative
Preoperative BSCVA UCVA BSCVA UCVA BSCVA
Visual AcuityIris
Recognition ControlIris
Recognition ControlIris
Recognition ControlIris
Recognition ControlIris
Recognition Control
20/20 or better, n 85 80 85 77 100 92 90 75 93 8920/24 to 20/40, n 13 16 14 18 0 6 9 22 6 720/50 or worse, n 2 2 1 3 0 0 1 1 1 2Mean G SD �0.08 G 0.04 �0.04 G 0.05 �0.01 G 0.09 �0.01 G 0.12 �0.05 G 0.05 �0.06 G 0.08 0.00 G 0.08 �0.02 G 0.11 �0.04 G 0.08 �0.05 G 0.06P value .10 .85 .80 .30 .51
BSCVA Z best spectacle-corrected visual acuity; n Z number of eyes; UCVA Z uncorrected visual acuity
situ device to correct the axis alignment did not giveadditional benefits.21
The recent incorporation of the iris recognition tech-nology system is another step toward nullifying theeffects of misalignment and cyclorotation. The iris rec-ognition system of the Zyoptix laser uses software thatcaptures the image of the eye; transforms the iris struc-tures into a digital key, generating a unique digital‘‘ZY-ID’’ for each patient; and stores the informationas well as other diagnostic data.3,7,18 The data areused to automatically correct cyclotorsion and pupil-shift information in the diagnostic phase.12,22 The sys-tem has an x, y, and z component based on infraredpainting of pupil-edge markers triangulated with thecenter of the defined pupil, enabling greater accuracyof the laser ablation in the treatment phase.13 Theuniqueness of this new iris recognition technology is
85
80
85
77
90
75
65
70
75
80
85
90
Baseline 1 month 3 month
% eyes
IR NIR
Figure 2. Comparison of preoperative BSCVA and postoperativeUCVA in eyes that achieved 20/20 or better acuity (IR Z iris recog-nition group; NIR Z control group).
J CATARACT REFRACT SURG
that it recognizes the treatment eye and ensures opti-mum safety of the treatment to the eye.
Our results show the efficacy of the iris recognitiontechnology in the treatment of myopic astigmatismin terms of refractive and visual outcomes. Althoughno significant group by time interaction effect wasnoted in any variable when comparing data at base-line, 1 month, and 3 months, a significant differencein the refractive status (residual sphere and cylinder)was observed over time in both groups; the iris recog-nition group had a significant improvement in the re-fractive status at 3 months (P Z .04, sphere; P Z .01,cylinder). An improvement in UCVA was seen at3 months; 90% of eyes in the iris recognition groupand 76.5% in the control group achieved a UCVA of20/20 or better. The efficacy index was good in bothgroups, although the iris recognition group had a bet-ter result (1.05) than the control group (0.93). Weobserved satisfactory visual outcomes in relation tothe safety index, with most eyes in both groups main-taining BSCVA. However, a decrease in best correctedvisual acuity from 1 month to 3 months occurred in
0 2 2 2
9088
6 6 20
0
10
20
30
40
50
60
70
80
90
Nu
mb
er o
f eyes
Decrease>2 Decrease>1 No change Increase>1 Increase>2Snellen's lines
Safety
IR NIR
Figure 3. Comparison of gain and loss of Snellen visual acuity lines3months postoperatively (IR Z iris recognition group; NIR Z controlgroup).
- VOL 34, FEBRUARY 2008
220 IRIS RECOGNITION SYSTEM FOR WAVEFRONT-GUIDED LASIK
both groups; the decrease could be attributed to post-operative stromal remodeling and regression.23,24 Inthe iris recognition group, a higher percentage ofeyes (92.0%) than in the control group (85.7%) werewithin the G0.50 D range in SE. In terms of stability,there was a small regression of effect between 1 month
Figure 4. A: Comparison of attempted and achieved correction at3months in the iris recognition group showing 1 eye had an overcor-rection. B: Comparison of attempted and achieved correction at 3months in the control group showing 3 eyes had an undercorrection.
Figure 5. Refractive stability based on mean SE in iris recognitiongroup (IR) and control group (NIR) at 1 and 3 months.
J CATARACT REFRACT SURG
and 3 months in both groups, with no significant dif-ference over time in either group. We used the Alpinsmethod25,26 to determine and compare the index ofsuccess between the 2 groups; the iris recognitiongroup achieved 98.0% success and the control group,81.6% (P Z .03).
To our knowledge, this is the first study to compar-atively evaluate wavefront-guided LASIK using theiris recognition system versus not using iris recogni-tion. The study provides evidence that the use of irisrecognition software in excimer laser refractive sur-gery helps to achieve better visual and refractiveoutcomes, especially in patients with a significantamount of myopic astigmatism.
REFERENCES1. Nuijts RMMA, Nabar VA, Hament WJ, Eggink FAGJ. Wavefront-
guided versus standard laser in situ keratomileusis to correct
low to moderate myopia. J Cataract Refract Surg 2002;
28:1907–1913
2. Kohnen T, Buhren J, Kuhne C, Mirshahi A. Wavefront-guided
LASIK with the Zyoptix 3.1 system for the correction of myopia
and compound myopic astigmatism with 1-year follow-up; clini-
cal outcome and change in higher order aberrations. Ophthal-
mology 2004; 111:2175–2185
3. Aizawa D, Shimizu K, Komatsu M, et al. Clinical outcomes of
wavefront-guided laser in situ keratomileusis: 6-month follow-up.
J Cataract Refract Surg 2003; 29:1507–1513
4. Taneri S. Laser in situ keratomileusis flap thickness using the
Hansatome microkeratome with zero compression heads.
J Cataract Refract Surg 2006; 32:72–77
5. Durrie DS, Stahl J. Randomized comparison of custom laser in
situ keratomileusis with the Alcon CustomCornea and the
Bausch & Lomb Zyoptix systems: one-month results. J Refract
Surg 2004; 20:S614–S618
6. Gulani AC, Probst L, Cox I, Veith R. Zyoptix: the Bausch & Lomb
wavefront platform. Ophthalmol Clin North Am 2004; 17(2):
173–181
7. Kim T-I, Yang S-J, Tchah H. Bilateral comparison of wavefront-
guided versus conventional laser in situ keratomileusis with
Bausch and Lomb Zyoptix. J Refract Surg 2004; 20:432–438
8. Tjon-Fo-Sang MJ, de Faber J-THN, Kingma C, Beekhuis WH.
Cyclotorsion: a possible cause of residual astigmatism in refrac-
tive surgery. J Cataract Refract Surg 2002; 28:599–602
9. Chernyak DA. Iris-based cyclotorsional image alignment
method for wavefront registration. IEEE Trans Biomed Eng
2005; 52:2032–2040
10. Chernyak DA. From wavefront device to laser: an alignment
method for complete registration of the ablation to the cornea.
J Refract Surg 2005; 21:463–468
11. Ciccio AE, Durrie DS, Stahl JE, Schwendeman F. Ocular cyclo-
torsion during customized laser ablation. J Refract Surg 2005;
21:S772–S774
12. Chernyak DA. Cyclotorsional eye motion occurring between
wavefront measurement and refractive surgery. J Cataract
Refract Surg 2004; 30:633–638
13. Swami AU, Steinert RF, Osborne WE, White AA. Rotational mal-
position during laser in situ keratomileusis. Am J Ophthalmol
2002; 133:561–562
14. Farah SG, Olafsson E, Gwynn DG, et al. Outcome of corneal
and laser astigmatic axis alignment in photoastigmatic refractive
keratectomy. J Cataract Refract Surg 2000; 26:1722–1728
- VOL 34, FEBRUARY 2008

221IRIS RECOGNITION SYSTEM FOR WAVEFRONT-GUIDED LASIK
15. Smith EM Jr, Talamo JH. Cyclotorsion in the seated and supine
patient. J Cataract Refract Surg 1995; 21:402–403
16. Stevens JD. Astigmatic excimer laser treatment: theoretical
effects of axis misalignment. Eur J Implant Refract Surg 1994;
6:310–318
17. Smith EM Jr, Talamo JH, Assil KK, Petashnick DE. Comparison
of astigmatic axis in the seated and supine positions. J Refract
Corneal Surg 1994; 10:615–620
18. Kanjani N, Jacob S, Agarwal A, et al. Wavefront- and topogra-
phy-guided ablation in myopic eyes using Zyoptix. J Cataract
Refract Surg 2004; 30:398–402
19. Guell JL, Muller A. Laser in situ keratomileusis (LASIK) for myo-
pia from �7 to �18 diopters. J Refract Surg 1996; 12:222–228
20. Marinho A, Pinto MC, Pinto R, et al. LASIK for high myopia: one
year experience. Ophthalmic Surg Lasers 1996; 27:S517–S520
21. Vajpayee RB, McCarty CA, Taylor HR. Evaluation of axis
alignment system for correction of myopic astigmatism with
the excimer laser. J Cataract Refract Surg 1998; 24:911–916
22. Yang Y, Thompson K, Burns SA. Pupil location under mesopic,
photopic, and pharmacologically dilated conditions. Invest
Ophthalmol Vis Sci 2002; 43:2508–2512
J CATARACT REFRACT SURG
23. Kymionis GD, Tsiklis NS, Astyrakakis N, et al. Eleven-year
follow-up of laser in situ keratomileusis. J Cataract Refract
Surg 2007; 33:191–196
24. Magallanes R, Shah S, Zadok D, et al. Stability after laser in situ
keratomileusis in moderately and extremely myopic eyes. J Cat-
aract Refract Surg 2001; 27:1007–1012
25. Alpins NA. Vector analysis of astigmatism changes by flattening,
steepening, and torque. J Cataract Refract Surg 1997; 23:1503–
1514
26. Alpins N. Astigmatism analysis by the Alpins method. J Cataract
Refract Surg 2001; 27:31–49
First author:Sudipta Ghosh, DOMS, DNB
Centre for Eye Research Australia,University of Melbourne, East Melbourne,Victoria, Australia
- VOL 34, FEBRUARY 2008








![Assessment of refractive astigmatism and simulated ... · sia after laser in situ keratomileusis (LASIK) [3], decen-tered refractive surgery [4] and may also occur after any type](https://img.pdfslide.net/doc/110x75/5f7926886f72081034179347/assessment-of-refractive-astigmatism-and-simulated-sia-after-laser-in-situ-keratomileusis.jpg)