Embed Size (px)
Citation preview

3Scientific Papers
Evaluation of Transanal Hemorrhoidal Dearterialization as a Minimally Invasive Therapeutic Approach to HemorrhoidsAuthors: Carlo Ratto, M.D. • Lorenza Donisi, M.D. • Angelo Parello, M.D. • Francesco Litta, M.D. • Giovanni Battista Doglietto, M.D.Department of Surgical Sciences, Catholic University, Rome, Italy
Read at the meeting of The American Society of Colon and Rectal Surgeons, Hollywood, Florida, May 2 to 6, 2009.
PurposeTransanal hemorrhoidal dearterialization (THD) is an innovative technique to treat hemorrhoids using a specially designed proctoscope for Doppler-guided transanal ligation of hemorrhoidal arteries. We analyzed results of experience at a single-institution with this THD device.
MethodsOverall, 170 patients were submitted to THD during the period July 2005 through October 2008. The operation consisted of hemorrhoidal dearterialization (of 6 arteries) in all patients, with major mucosal/submucosal pexy in 56 patients (32.9%). The first consecutive 11 patients (6.4%) were treated under general/spinal anesthesia, the remaining 159 (93.6%) by sedation with propofol, supported by analgesia with remifentanil. Following THD surgery, patients were regularly evaluated at 2 weeks, 1 and 3 months, and once a year after operation.
ResultsThe mean age of the 170 patients was 47.3 ± 13.0 years; 102 (60%) were men. Hemorrhoidal disease was grade II in 13 (7.6%); grade III in 141 (82.7%), and grade IV in 16 (9.6%). Postoperative bleeding requiring surgical hemostasis occurred in 2 cases (1.2%). Mean follow-up was 11.5 ± 12 (range, 1-41) months. Hemorrhoidal thrombosis occurred in 4 patients (2.3%), chronic pain and fecal incontinence in none. Hemorrhoidal prolapse was reported at follow-up by 50 patients (29.5%), but prolapse was confirmed only in 18 (10.5%) and was mild; some patients reporting prolapse were found to have skin tags. Overall, long-term control of bleeding was obtained in 159 patients (93.5%) and control of prolapse in 152 (89.5%). Recurrence of hemorrhoidal disease requiring surgery was found in 7 patients (4.1%).
ConclusionsTHD appears to be a very effective minimally invasive option to treat hemorrhoids and can be performed in a day-surgery setting. Future controlled trials comparing THD with other procedures will show the real potential of THD and define adequate indications for this approach.
KeywordsHemorrhoids; Transanal hemorrhoidal dearterialization; THD; Hemorrhoidal artery ligation; Doppler-guided; Bleeding; Prolapse.
Source: Dis. Colon Rectum 2010;53 (5): 803-811

4 Scientific Papers
Since the 1980s, considerations of the pain and risks of postoperative morbidity involved in traditional hemorrhoidal excision have given rise to enthusiastic research to find less aggressive but effective approaches to the treatment of hemorrhoids. Despite progress, controversy remains concerning appropriate indications and methods of surgical treatment. Doppler-guided transanal ligation of hemorrhoidal arteries within the lower rectum was introduced by Morinaga et al.1 in 1995. The primary aim of this procedure is to drastically reduce arterial inflow to the hemorrhoidal plexus,2 and then optimize the status of hemorrhoidal cushions, without excision, to achieve clinical resolution of symptoms while preserving hemorrhoidal tissue. Various proctoscopes coupled with Doppler transducers have been used for the procedure.3 The terms hemorrhoidal artery ligation (HAL) and transanal hemorrhoidal dearterialization (THD) have been used interchangeably,3 although the term THD was introduced in connection with a specific type of proctoscope.4-6 In this report, we present results of experience at a single institution using this THD device.
Patients and methodsWe analyzed medical records of 170 patients with hemorrhoidal disease who underwent THD surgery at our institution from July 2005 through October 2008. Institutional Review Board approval was obtained to perform this procedure in our department. All patients gave written informed consent. All patients underwent clinical evaluation, i.e., patient history (in particular, reports of anal bleeding and hemorrhoidal or muco-hemorrhoidal prolapse) and physical examination (including digital examination and anoproctoscopy) for diagnosis of hemorrhoid engorgement and easy-bleeding, prolapsing hemorrhoids, skin tags, and other associated anorectal diseases. Common guidelines for screening of colorectal diseases were followed, and patients with neoplastic or other non-neoplastic diseases were excluded. Severity of hemorrhoidal disease was graded according to Goligher’s classification.7 In this regard, whether a patient was referred because of spontaneous or provoked reduction of prolapse was considered very important and related to features of the physical examination. A finding of external hemorrhoids was meticulously distinguished from that of skin tags. In fact, the purpose of THD was to treat internal and external hemorrhoids, but not skin tags, which were individually excised when indicated. Patients with grade I hemorrhoids were excluded from any surgical approach. Those with grade II hemorrhoids were enrolled for THD only if resistant to medical treatment, rubber-band ligation, or sclerotherapy, mainly presenting significant hemorrhoidal bleeding and/or prolapse.
EquipmentThe THD system (THD S.p.A., Correggio, Italy) consists of a specifically designed proctoscope equipped with a Doppler probe (placed on the lateral profile of the device), and a light source (Fig. 1). Continuous Doppler technology is provided, with a double crystal allowing specific focusing of the ultrasound waves and capture of large-diameter arteries located in the superficial layers of the rectal wall. The acoustic signal is optimized because sufficient space is provided around the membranes for adequate vibration. The Doppler probe is oriented toward the operative window, so that the artery identified by the Doppler signal lies within the operative window and can be selectively ligated. Precision and standardization of ligation are obtained by using the circular pivot located in the center of the proctoscope lumen.The THD proctoscope models changed during the study period. The first model (original THD proctoscope, Fig. 2A) had an elliptical section and was equipped with an operative window very close to the Doppler probe, devised in order to place sutures through the rectal wall under the guidance of Doppler acoustic identification of the arterial vessels. The second model (THD Surgy, THD S.p.A.) was an adjunctive proctoscope to be used for mucopexy, which became available in July 2007 (adjunctive proctoscope, Fig. 2B). This model was designed to offer a completely open superior window to expose the entire operative field, from the dearterialization site to the external anal opening. A new model (THD Slide, THD S.p.A.) became available in September of 2008 (sliding proctoscope, Fig. 2C). This model has a sliding part of the superior profile corresponding to the Doppler probe, so that the operator can move this part of the proctoscope up or down. The sliding proctoscope maintains the original elliptical section, with an external maximum diameter of 33 to 34 mm, but with a minimum diameter of 20 to 34 mm.

5Scientific Papers
Surgical techniqueOver time, the surgical setting of the THD approach changed in several aspects. Regional anesthesia was used only in the first 11 patients (6.4%; spinal in 1, posterior perianal block in 10). Sedation with propofol supported by analgesia with remifentanil was used in the other 159 patients (93.6%); patients were maintained either in spontaneous breathing or a laryngeal mask was used. All patients were treated in an outpatient surgery setting. Antibiotics were not administered before, during or after surgery. All operations were performed by the same surgeon (C.R.). Following gel lubrication, the proctoscope was inserted through the anal canal reaching the lower rectum, about 6 to 7 cm from the anal verge. Tilting the proctoscope, the best Doppler signals were sought corresponding to all 6 main trunks of the hemorrhoidal arteries. The patients were in a lithotomy position; thus, the 6 arterial trunks, identified at 1, 3, 5, 7, 9, and 11 o’clock, were almost invariably of low rectal circumference. The rectal mucosa and submucosa wall were then transfixed with a “Z” suture (stitch of 2-0 absorbable polyglycolic acid with a 5/8-inch needle) to ligate the artery. The depth of the transfixed stitches was easily and safely calibrated by using the pivot hole provided in the center of the proctoscope lumen. The tip of the needle holder was introduced into the pivot hole and rotated so that the needle penetrated the rectal wall at a maximum depth of 6 mm, avoiding perforation of the entire rectal wall and involving primarily only the mucosa and submucosa. Pulling the suture back abolished or significantly reduced the Doppler signal, thus confirming the hold of the artery. Each suture was tied and dearterialization completed. In patients with hemorrhoidal or mucohemorrhoidal prolapse (external prolapse of hemorrhoids alone or of hemorrhoids and rectal mucosa) requiring mucopexy, the procedure was performed with the original proctoscope making multiple passages of continuous suture through the mucosa and submucosa, below the dearterialization site, moving the proctoscope back step by step (with steps 0.5 cm from each other). Thereafter, the proctoscope was re-introduced and the suture gently tied. When the adjunctive proctoscope was used, the original proctoscope was removed after the dearterialization phase, leaving the tied suture in place. The suture was then continued distally with the adjunctive proctoscope until the anorectal ring was reached. When the sliding proctoscope was used, it remained in place after dearterialization, and only the sliding part was moved back, exposing the rectal mucosa to be transfixed in order to perform mucopexy under direct visualization, up to the anorectal ring. The suture was then gently tied. The sliding proctoscope allowed an easier mucopexy, because any visual limitations due to hemorrhoidal piles proliferating into the operative field were avoided. During the mucopexy procedure, the anal canal mucosa was always spared from the suture. Need for minor or major mucopexy was determined based on the amount of prolapsing tissue. Mucopexy was considered to be minor when 1) a small prolapse was reduced with the “Z” stitches of dearterialization; 2) it was performed by using a maximum of 2 passages within the mucosa-submucosa below the dearterialization site; 3) it was limited to a single rectal circumferential quadrant. Mucopexy was considered major when it concerned a larger prolapse that needed to be reduced by using a number of mucosal-submucosal passages (more than 2) below the dearterialization site.
Follow-upDuring the postoperative period, patients were advised to maintain a diet rich in liquids and fibers in order to avoid constipation and straining. If necessary, stool softeners were also advised. Analgesics were prescribed only if requested by the patient. Routine follow-up was scheduled at 2 weeks, 1 and 3 months, and once a year after the operation. Moreover, during the period from October through November 2008, all patients were recalled for an additional follow-up session, regardless of the length of time since the operation. All were examined clinically (postoperative history, digital examination, and anoscopy). At the last follow-up, patients were asked to rate the resolution of symptoms on a visual analogue scale (VAS) ranging from 1 (minimum resolution) to 10 (maximum resolution). The patients and the surgeon were also asked to rate satisfaction with the outcome using on a VAS ranging from 1 (minimum satisfaction) to 10 (maximum satisfaction). The patient satisfaction scale aimed to evaluate both symptoms and quality of life, the surgeon’s satisfaction scale referred to both resolution of symptoms and physical evidence. All patients were asked about their fecal continence, both preoperatively and postoperatively, and information about any incontinence was scrupulously collected.

6 Scientific Papers
Statistical analysisStatistical analysis was performed using SPSS software for Windows, version 17 (SPSS, Chicago, IL, USA). Results were expressed as mean ± standard deviation (SD). Differences between groups were analyzed using the 2-tailed χ2 test or 2-tailed Wilcoxon matched-pairs test for categorical variables and paired or unpaired 2-tailed t test for continuous variables. A 2-tailed P value of <.05 was considered statistically significant. Agreement between patient and surgeon satisfaction was evaluated using the Cohen test (high level of agreement, κ ≥ 0.75; medium level of agreement, κ < 0.75 but > 0.40; low level of agreement: κ ≤ 0.40.
ResultsDuring the first year of the surgeon’s experience, 29 patients (17.1%) were operated upon, 46 (27.1%) during the second year, 59 (34.7%) during the third year, and 36 (21.2%) during the 4 months thereafter. The patients’ preoperative characteristics are shown in Table 1.The surgical procedure took 20 ± 5 minutes when only dearterialization was performed and 30 ± 10 minutes when mucopexy was added. Intraoperatively, no complications or adverse events occurred. In all cases, dearterialization was performed with 6 sutures ligating the main trunks of the hemorrhoidal arteries. During mucosal submucosal transfixion, a transient submucosal hematoma occurred in 10 patients (5.9%). The hematoma was always brought under control with an adjunctive suture placed proximally to the previous one, and hematoma had already disappeared at the first postoperative follow-up at 2 weeks. Mucopexy was performed in all patients with grade III or IV hemorrhoids; the mucopexy was minor in 101 patients (59.4%), and major mucopexy was necessary in 56 patients (32.9%). In 11 patients (0.6%), a single prolapsing hemorrhoidal pile was removed according to the Ferguson technique. One or more skin tags were excised in 10 patients (0.6%). In 23 patients suffering from anal fissure, an internal lateral sphincterotomy was performed, always before starting the THD procedure.The hospitalization program (from 2-24 hours after THD surgery) was respected in all patients except 2; the hospital stay was 3 days because of postoperative pain in one, and 7 days because of immediate postoperative stroke in the other.Representative results of the procedure are shown in Figure 3. During the 30-day postoperative period, anal or rectal pain was reported by a total of 27 patients (15.9%). Pain occurred during defecation in 12 patients (7.1%), after defecation in 15 patients (8.8%), and without relation to defecation in 4 patients (2.4%). However, only 8 patients (4.7%) needed to take analgesics, and mean duration of analgesics consumption was 6.6 ± 4.1 days. No significant differences in postoperative pain or analgesics consumption were seen in patients who underwent additional procedures compared with those who did not (Table 2), or in those who underwent major mucopexy compared with those who did not (Table 3).Rectal discomfort/tenesmus was reported by 41 patients (24.1%), pruritus by 27 patients (15.9%), anal burning by 34 patients (20%), and mucus discharge by 20 patients (11.8%); all of these postoperative symptoms were transient and disappeared within the first 10 postoperative days. None of the patients reported any form of fecal incontinence.However, 49 patients (28.8%) continued to suffer from constipation. Postoperative bleeding requiring surgical hemostasis was reported by 2 patients (1.2%), occurring after 7 days in one and after 10 days in the other.Median follow-up was 11.5 ± 12 (range, 1-41) months. At follow-up, 11 patients (6.5%) reported episodes of bleeding during defecation. Symptoms reported by patients did not correlate with signs found by the surgeon at follow-up. Prolapsing hemorrhoids were reported by 50 patients (29.5%); this was reported to have occurred only at defecation in 22 patients (13.2%), after defecation in 14 (8.5%), and was reported to be occasional in 25 (14.7%) and persistent in 9 (5.4%). However, during physical examination, a mild prolapse was detected in 18 patients (10.5%); the prolapse was hemorrhoidal only in 13 (7.6%) and muco-hemorrhoidal in 5 (2.9%). In the other 32 patients reporting prolapse, only anal skin tags were detected at physical examination.Hemorrhoidal thrombosis was found in 4 patients (2.3%); only 1 required surgical excision of the 2 external piles showing evidence of thrombosis. No patients reported either minor or major fecal incontinence episodes following the THD procedure.

7Scientific Papers
TABLE 1 . PREOPERATIVE CHARACTERISTICS OF PATIENTS UNDERGOING THD
Features n (%)
Patients 170
Men 102 (60.0)
Women 68 (40.0)
Age, mean ± SD (range) 47.3 ± 13.0 (22-81)
Hemorrhoid gradea
II 13 (7.7)
III 141 (82.9)
IV 16 (9.4)
Previous treatments
Topical medical 59 (34.7)
Per os medical 128 (75.3)
Other surgery 15 (8.8)
Symptoms
Bleeding 160 (94.1)
≥1 episode/week 87 (54.4)
>1 episode/month <1 episode/week 50 (31.2)
≤1 episode/month 23 (14.4)
Anal pain 78 (45.9)
Tenesmus 15 (8.8)
Dyschezia 13 (7.6)
Associated anal fissure 23 (13.5)
THD = transanal hemorrhoidal dearterialization.aGoligher classification7
TABLE 2 . POSTOPERATIVE PAIN AND ANALGESICS CONSUMPTION IN PATIENTS WITH OR WITHOUT ADDITIONAL SURGICAL PROCEDURES DURING THD PROCEDURE
Additional proceduresa
Total Yes No P
n=31 n=139
Postoperative pain .16
Yes 27 4 (12.9) 23 (16.5)
No 143 27 (87.1) 116 (83.5)
Analgesics consumption .62
Yes 8 2 (6.5) 6 (4.3)
No 162 29 (93.5) 133 (95.7)
THD = transanal hemorrhoidal dearterialization.aPartial hemorrhoidectomy, skin tag removal, or lateral internal sphincterotomy.Data are numbers of patients with percentages in parentheses.
TABLE 3. POSTOPERATIVE PAIN AND ANALGESICS CONSUMPTION IN RELATION TO PERFORMANCE OF MAJOR MUCOPEXY DURING THD PROCEDURE
Mucopexy
n Yes No P
Postoperative pain .14
Yes 27 8 (14.3) 19 (16.7)
No 143 48 (85.7) 95 (83.3)
Analgesics consumption .40
Yes 8 4 (7.1) 4 (3.5)
No 162 52 (92.9) 110 (96.5)
THD = transanal hemorrhoidal dearterialization.Data are numbers of patients with percentages in parentheses.
TA B L E 4 . D I S T R I B U T I O N PAT I E N T R AT I N G S O F S Y M P TO M R E S O L U T I O N I N R E L AT I O N TO P R E O P E R AT I V E G R A D E O F H E M O R R H O I D A L D I S E A S E
Symptom Resolution Score (VAS)
Grade n 1–3 4–5 6–7 8–10
II 13 0 (0) 0 (0) 3 (23.0) 10 (77.0)
III 141 10 (7.1) 17 (12.1) 19 (13.5) 95 (67.4)
IV 16 0 (0) 2 (12.5) 1 (6.3) 13 (81.2)
All 170 10 (5.9) 19 (11.2) 23 (13.5) 118 (69.4)
VAS = visual analogue scale (1 = minimum resolution; 10 = maximum resolution).Data are numbers of patients with percentages in parentheses.
TA B L E 5 . D I S T R I B U T I O N O F PAT I E N T R AT I N G O F S Y M P TO M R E S O L U T I O N I N R E L AT I O N TO L E N G T H O F S U R G E O N ’ S E X P E R I E N C E
Symptom Resolution Score (VAS)
Years of experience n 1–3 4–5 6–7 8–10
1 29 3 (10.3) 4 (13.8) 3 (10.3) 19 (65.6)
2 46 6 (13.0) 6 (13.0) 5 (10.9) 29 (63.1)
3 59 0 (0) 9 (15.3) 10 (16.9) 40 (67.8)
4 36 1 (2.8) 0 (0) 5 (13.9) 30 (83.3)
Total 170 10 (5.9) 19 (11.2) 23 (13.5) 118 (69.4)
VAS = visual analogue scale (1 = minimum resolution; 10 = maximum resolution); Year 1 = July 2005–June 2006; Year 2 = July 2006–June 2007; Year 3 = July 2007–June 2008; Year 4 = July 2008–October 2008. Data are numbers of patients with percentages in parentheses.
TABLE 6 . COMPARISON OF PATIENT VS. SURGEON SATISFACTION WITH OUTCOME
AT LAST FOLLOW-UP AFTER THD
VAS score Patients Surgeons
8–10 140 (82.3) 146 (85.9)
6–7 23 (13.3) 22 (12.9)
4–5 7 (4.1) 2 (1.1)
1–3 0 (0) 0 (0)
Total 170 170
THD = transanal hemorrhoidal dearterialization; VAS = visual analogue scale (1 = minimum resolution; 10 = maximum resolution). Data are numbers of patients with percentages in parentheses.

8 Scientific Papers
During the follow-up period, 7 patients (4.1%) required re-operation for relapse of symptoms of hemorrhoidal disease (bleeding in 5 patients, occurring 5, 12, 12, 15, and 17 months after the operation; hemorrhoidal prolapse in 2 patients, occurring 5 and 19 months after the operation). Four patients underwent the THD procedure again (consisting, in all cases, of ligation of a single hemorrhoidal artery detected by Doppler probe), and 3 patients underwent hemorrhoidectomy according to the Milligan-Morgan procedure.Table 4 shows the distribution of patient ratings of symptom resolution at the last follow-up visit in relation to preoperative grade of hemorrhoidal disease. Overall, 69.4% of patients rated symptoms as being maximally or near maximally resolved (VAS score 8–10), and no relation between judgment of resolution and grade of hemorrhoidal disease was seen. Ratings of symptom resolution according to length of the surgeon’s experience in performing THD are shown in Table 5. Most patients indicated a high degree of satisfaction, regardless of the surgeon’s number of years of experience. However, satisfaction appeared greatest in the fourth year of the surgeon’s experience.A high level of agreement (κ = 0.81) was found between patient and surgeon ratings of overall satisfaction with outcome at last follow-up for each VAS category (Table 6). Patient-surgeon agreement regarding satisfaction was not influenced by degree of hemorrhoidal disease, as assessed preoperatively.
DiscussionThe THD system uses a transanal approach to reach the distal third of the rectum. Owing to the elliptic shape of the THD device, fibers of the internal anal sphincter are submitted to a negligible dilating stretch. Thus, fecal incontinence was avoided in the patients of this study. The targets of this treatment are the main vessels of the hemorrhoidal arteries, located in the inferior part of the rectum. In our experience, these arteries were identified almost constantly at the 1, 3, 5, 7, 9, and 11 o’clock positions of the low rectum. However, definitive proof of this anatomic feature is a matter for future studies. The Doppler probe allows the 6 main arterial branches to be selectively found with a careful intraoperative search that is not time-consuming. The technological characteristics of the THD system (continuous Doppler, double crystal, adequate space for membrane vibration, Doppler probe shape and circular pivot) allow accuracy and precision of identification and ligation of arteries. These characteristics may explain differences in the number of ligatures performed with THD (always 6) 4,5,8-10 and HAL (varying between 4 and 11).11-17 The selective ligation of arteries leaves a free space between each stitch to avoid a complete blockage of venous outflow from the hemorrhoids that might cause thrombosis.Originally, Doppler-guided transanal hemorrhoidal artery ligation was used only for low- or moderate-grade hemorrhoidal disease. Subsequently, technical modifications of the proctoscopes and Doppler equipment have made it possible to treat advanced degrees of hemorrhoidal disease, with the addition of rectal mucopexy or anopexy to control mucosal-hemorrhoidal prolapse.18-21 In the presence of a hemorrhoidal or muco-hemorrhoidal prolapse, it is possible to perform a mucopexy with the same stitch as the dearterialization, which proceeds distally, transfixing the rectal mucosal and submucosal tissue. In our study, the anal canal was always spared to reduce postoperative pain as far as possible. The latest technical modification to the THD proctoscope makes the rectal mucopexy procedure easier, more effective, and safer than before. As when the Milligan-Morgan technique and the procedure for prolapse and hemorrhoids (PPH) are indicated in the treatment of prolapsing hemorrhoids, mucopexy must be considered crucial in addition to the THD technique in the treatment of grade III or IV hemorrhoids. Although with Milligan-Morgan operation, the surgeon can usually check the operative field in any step and then decide the extension of tissue excision, with PPH, the amount of tissue resected and further location of the definitive suture line are almost always unpredictable, because the main step of the operation is performed “blindly”. In contrast, the THD procedure ensures that both the amount of tissue to be plicated and the sites where mucopexy is started and stopped are very well visualized.THD surgery time is short, with or without mucopexy. The THD operation is possible with either general or spinal anesthesia, or with sedation plus analgesia, resulting in a significant reduction in hospitalization time. In our study, all patients were treated in the day-surgery setting. No clinically significant intraoperative complications occurred in our patients. There were only a few cases of transient submucosal hematoma, and these were without

9Scientific Papers
consequences. Rectal mucopexy was performed as needed, depending on the degree of mucosal prolapse. At follow-up, some degree of hemorrhoidal prolapse was reported by 29.5% of our patients, but a complete evaluation (including physical examination) showed that only 10.5% of all patients actually had a mucosal prolapse, which was mild in all cases. This discrepancy could be explained because many patients confused hemorrhoidal prolapse with skin tags. In our follow-up evaluation, the “surgeon’s findings” considered both patient complaints (either “true” or “false” reports of prolapse or skin tags) and features at physical examination. Data in the literature concerning results of HAL or THD procedures4,5,8-17 report an incidence of mucosal prolapse of 3% to 25%. Skin tags should not be considered as hemorrhoidal prolapse and should be surgically excised, if necessary; in fact “skin tag-pexy” is not one of the aims of THD surgery. This should be clearly explained to patients, because they could mistake skin tags for hemorrhoidal prolapse.Usually, postoperative bleeding occurs only in a few patients; in our study, surgical hemostasis was necessary in only 2 (1.2%). Data in the literature report hemorrhoidal bleeding at follow-up in 1% to 15% of patients submitted to Doppler-guided dearterialization1,4,8,9,11-17 (in 6.5% of our patients, necessitating further surgery in 2.9%). Hemorrhoidal thrombosis rarely occurred in our study. Postoperative pain occurred in 15.9% of our patients, but only a small number (4.7%) required analgesics. Sometimes, major mucopexy can be responsible for postoperative pain or rectal discomfort, probably due to ischemia or inflammation of the mucosa-submucosa trapped by the suture. However, this is a transient event. Whereas data in the literature report pain after Doppler-guided hemorrhoidal dearterialization in up to 12% of patients,4,5,8-17 none of our patients reported pain or discomfort at follow-up. Overall, more than 95% of our patients were pleased with the results of THD surgery, this being due to the complete or good resolution of symptoms. The surgeon’s satisfaction was comparable.In conclusion, THD surgery appears to be a valid therapeutic option for nonexcisional surgery of hemorrhoids, being safe and effective, with an acceptable incidence of mild -never chronic- complications compared with other methods.22 The surgeon can control each surgical step and thus adjust the extent of mucopexy, if necessary. Tying of the hemorrhoidal arterial branches is efficiently performed with Doppler-guidance; this is, therefore, not “blind” surgery. Finally, patient satisfaction with the results is very high. Future studies comparing THD with other procedures in controlled trials will define the real potential of THD and adequate indications for this approach.
Figure 1. Illustration of the THD proctoscope, equipped with a Doppler probe, as inserted into the low rectum.
10 Scientific Papers
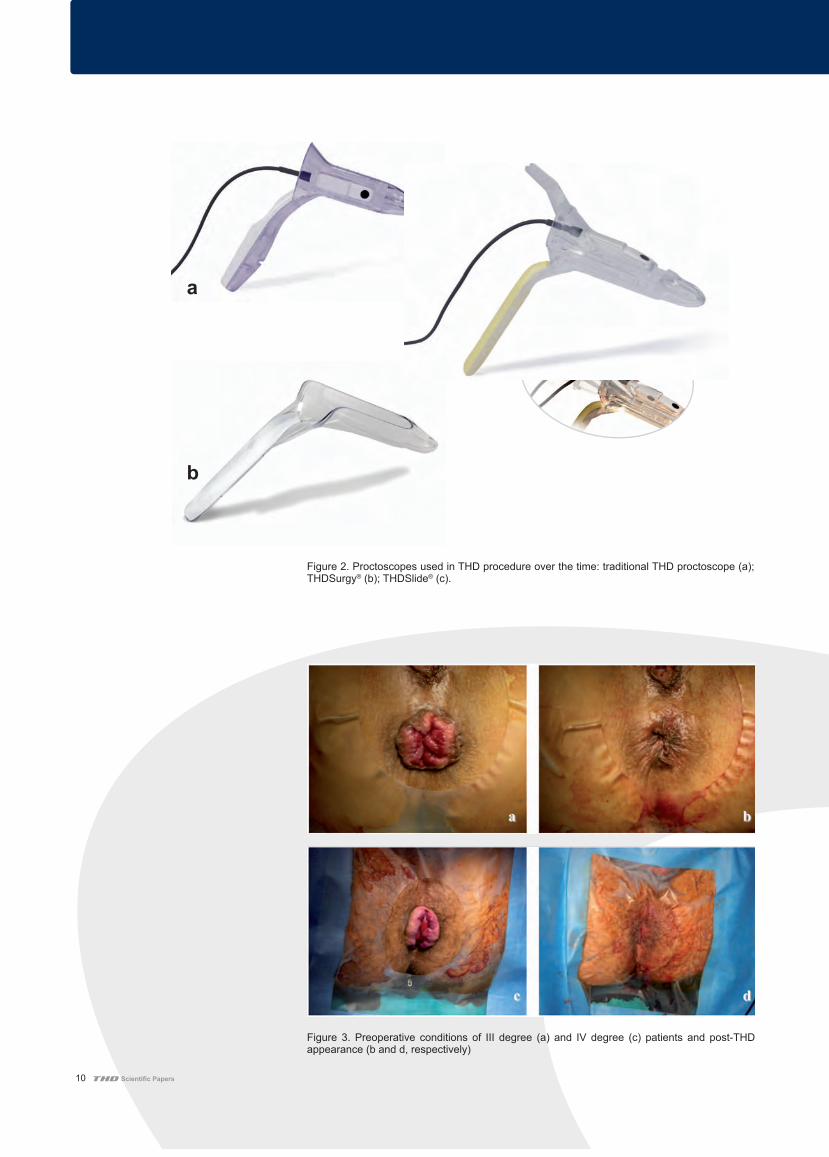
Figure 2. Proctoscopes used in THD procedure over the time: traditional THD proctoscope (a); THDSurgy® (b); THDSlide® (c).
Figure 3. Preoperative conditions of III degree (a) and IV degree (c) patients and post-THD appearance (b and d, respectively)
a
b
c

11Scientific Papers
References1. Morinaga K, Hasuda K, Ikeda T. A novel therapy for internal hemorrhoids: ligation of the
hemorrhoidal artery with a newly devised instrument (Moricorn) in conjunction with a Doppler flowmeter. Am J Gastroenterol. 1995;90:610-613.
2. Aigner F, Bodner G, Conrad F, et al. The superior rectal artery and its branching pattern with regard to its clinical influence on ligation techniques for internal hemorrhoids. Am J Surg 2004;187:102-108.
3. Giordano P, Overton J, Madeddu F, Zaman S, Gravante G. Transanal hemorrhoidal dearterialization: a systematic review. Dis Colon Rectum 2009;52:1665-1671.
4. Sohn N, Aronoff JS, Cohen FS, Weinstein MA. Transanal hemorrhoidal dearterialization is an alternative to operative hemorrhoidectomy. Am J Surg 2001;182:515-519.
5. Dal Monte PP, Tagariello C, Sarago M, et al. Transanal haemorrhoidal dearterialisation: nonexcisional surgery for the treatment of haemorrhoidal disease. Tech Coloproctol 2007;11:333-338
6. Lienert M, Horstmann O. Transanale-Hämorrhoiden-Dearterialisation (THD) und Hämorrhoidal-Arterien-Ligatur (HAL): Evaluation der minimal-invasiven Therapie des Hämorrhoidalleidens. 34. Deutscher Koloproktologen-Kongress: Abstracts. Coloproctology 2008;30:77–96.
7. Goligher JC, Leacock AG, Brossy JJ. The surgical anatomy of the anal canal. Br J Surg 1955;43:51-61.
8. Bursics A, Morvay K, Kupcsulik P, Flautner L. Comparison of early and 1-year follow-up results of conventional hemorrhoidectomy and hemorrhoid artery ligation: a randomized study. Int J Colorectal Dis 2004;19:176-180.
9. Lienert M, Ulrich B. [Doppler-guided ligation of the hemorrhoidal arteries. Report of experiences with 248 patients]. Dtsch Med Wochenschr 2004;129:947-950.
10. Cantero R, Balibrea JM, Ferrigni C, et al. [Doppler-guided transanal haemorrhoidal dearterialisation. An alternative treatment for haemorrhoids] In Spanish. Cir Esp 2008;83:252-255.
11. Felice G, Privitera A, Ellul E, Klaumann M. Doppler-guided hemorrhoidal artery ligation: an alternative to hemorrhoidectomy. Dis Colon Rectum 2005;48:2090-2093.
12. Abdeldaim Y, Mabadeje O, Muhammad KM, Mc Avinchey D. Doppler-guided haemorrhoidal arteries ligation: preliminary clinical experience. Ir Med J 2007;100:535-537.
13. Arnold S, Antonietti E, Rollinger G, Scheyer M. [Doppler ultrasound assisted hemorrhoid artery ligation. A new therapy in symptomatic hemorrhoids] In German. Chirurg 2002;73:269-273.
14. Narro JL. [Hemorrhoid Therapy with Doppler Guided Hemorrhoidal Artery Ligation via Proctoscope KM-25. A New Alternative to Hemorrhoidectomy and Rubber Band Ligation?] In German. Zentralbl Chir 2004;129:208-210.
15. Greenberg R, Karin E, Avital S, Skornick Y, Werbin N. First 100 cases with Doppler-guided hemorrhoidal artery ligation. Dis Colon Rectum 2006; 49:485-489.
16. Wallis de Vries BM, van der Beek ES, de Wijkerslooth LR, et al. Treatment of grade 2 and 3 hemorrhoids with Doppler-guided hemorrhoidal artery ligation. Dig Surg 2007;24:436-440.
17. Vavra P, Dostalik J, Gunkova P, Matinek L, Gunka I. [Initial experience with Doppler guided hemorrhoidal artery ligation (DGHAL)] In Czech. Rozhl Chir 2004;83:79-81.
18. Infantino A, Bellomo R, Dal Monte PP, et al. Transanal Haemorrhoidal Artery Echodoppler Ligation and anopexy (THD) is effective for II and III degree haemorrhoids: a prospective multicentric study. Colorectal Dis. 2009.
19. Theodoropoulos GE, Sevrisarianos N, Papaconstantinou J, et al. Doppler- Guided haemorrhoidal artery ligation (DGHAL), rectoanal repair (RAR), sutured haemorrhoidopexy (SHP) and minimal mucocutaneous excision (MMCE) for Grade III-IV haemorrhoids: A multicenter prospective study of safety and efficacy. Colorectal Dis 2008.
20. Satzinger U, Feil W, Glaser K. Recto Anal Repair (RAR): a viable new treatment option for high-grade hemorrhoids. One year results of a prospective study. Pelviperineology 2009;28:37-42.
21. Zagriadskii EA. [Trans-anal disarterization of internal hemorrhoids under Doppler control with mucopexy and lifting in treatment of stage III-IV hemorrhoids]. Khirurgiia (Mosk) 2009:52-58.
22. Festen S, van Hoogstraten MJ, van Geloven AA, Gerhards MF. Treatment of grade III and IV haemorrhoidal disease with PPH or THD. A randomized trial on postoperative complications and short-term results. Int J Colorectal Dis 2009;24:1401-1405.

Original article
Novel bulking agent for faecal incontinence
C. Ratto1, A. Parello1, L. Donisi1, F. Litta1, V. De Simone1, L. Spazzafumo2 and P. Giordano3
1Department of Surgical Sciences, Catholic University, Rome, and 2Centre of Statistics, Istituto Nazionale di Ricovero e Cura per Anziani, Ancona, Italy,and 3Department of Surgery, Whipps Cross University Hospital, London, UKCorrespondence to: Dr C. Ratto, Department of Surgical Sciences, Catholic University, Largo A. Gemelli, 8, 00168, Rome, Italy (e-mail: [email protected])
Background: Various injectable bulking agents have been used for the treatment of faecal incontinence(FI). However, encouraging early results are not maintained over time. This study aimed to assess short-and medium-term results of a new bulking agent for the treatment of FI.Methods: The GatekeeperTM prosthesis comprises a thin solid polyacrylonitrile cylinder that becomesthicker, shorter and softer within 24 h after implantation. Fourteen patients with FI underwent treatmentwith GatekeeperTM under local anaesthesia. Four prostheses were implanted in the intersphincteric spacein each patient, under endoanal ultrasound guidance. Number of episodes of major FI, Cleveland ClinicFI score (CCFIS), Vaizey score, anorectal manometry, endoanal ultrasonography (EUS), health statusand quality of life (Short Form 36 and Faecal Incontinence Quality of Life questionnaires) were assessedbefore and after treatment.Results: Mean(s.d.) follow-up was 33·5(12·4) months. There were no complications. There was asignificant decrease in major FI episodes from 7·1(7·4) per week at baseline to 1·4(4·0), 1·0(3·2) and0·4(0·6) per week respectively at 1-month, 3-month and last follow-up (P = 0·002). CCFIS improvedsignificantly from 12·7(3·3) to 4·1(3·0), 3·9(2·6) and 5·1(3·0) respectively (P < 0·001), and Vaizey scorefrom 15·4(3·3) to 7·1(3·9), 4·7(3·0) and 6·9(5·0) respectively (P = 0·010). Soiling and ability to postponedefaecation improved significantly, and patients reported significant improvement in health status andquality of life. At follow-up, manometric parameters had not changed and EUS did not demonstrate anyprosthesis dislocation.Conclusion: The GatekeeperTM anal implant seemed safe, reliable and effective. Initial clinicalimprovement was maintained over time, and follow-up data were encouraging.
Paper accepted 4 August 2011Published online in Wiley Online Library (www.bjs.co.uk). DOI: 10.1002/bjs.7699
Introduction
Faecal incontinence (FI) is a common problem that canpresent with a wide variety of symptoms ranging frominvoluntary but recognized passage of gas, liquid or solidstool to unrecognized anal leakage of mucus, fluid orstool. Depending on the degree of symptoms, FI can bea highly distressing and socially incapacitating problem.The wide variety of aetiologies and difficulty in accuratelydefining the cause of the problem make treatment difficult.Appropriate treatment relies on accurate diagnosis andcareful patient selection. Various injectable anal bulkingagents have been used to treat FI1–7, but procedureshave not been standardized, and the most effective site
Re-use of this article is permitted is accordance with the Termsand Conditions set out at http://wileyonlinelibrary.com/onlineopen#OnlineOpen_Terms
of placement as well as the amount of agent to be deliveredhas yet to be established. Moreover, depending on thematerial used, dislocation, migration and absorption canoccur. Owing to significant differences between bulkingagents and clinical conditions in which they are used,results are controversial and difficult to interpret. It seemsthat early positive results of anal bulking agents are oftennot confirmed in the long term.
This aim of this study was assess the short- and medium-term results of a new bulking agent used for the treatmentof FI.
Methods
This study, carried out at the Department of SurgicalSciences, Catholic University, Rome, was approved by theinstitutional ethics committee.
2011 British Journal of Surgery Society Ltd British Journal of SurgeryPublished by John Wiley & Sons Ltd

C. Ratto, A. Parello, L. Donisi, F. Litta, V. De Simone, L. Spazzafumo and P. Giordano
Anal bulking agent
GatekeeperTM
prostheses (originally from Medtronic, Min-neapolis, Minnesota, USA; now from THD, Correg-gio, Italy) were used as anal bulking agent. These arethin solid cylinders (length 21 mm, diameter 1·2 mm) ofHYEXPAN
TM(polyacrylonitrile), a hydrophilic material
that, within 24 h of implantation in contact with human tis-sue, changes shape and volume, becoming thicker (diameter7 mm), shorter (length 17 mm) and of softer consistency(Fig. 1). Their final shape yields a 720 per cent volumeincrease compared with the volume inserted. The materialis identifiable on palpation and ultrasonography.
Selection criteria and preoperative data collection
Patients with at least a 6-month history of episodesof FI (soiling or incontinence to liquid and/or solidstools) occurring at least once a week that had failedto improve with conservative measures were invited toparticipate. Patients with isolated incontinence to gas,risk of significant postoperative complications, includinguncontrolled diabetes, anal sepsis, inflammatory boweldiseases with anorectal involvement or any colorec-tal cancer undergoing active treatment, were excluded.Patients with an isolated external anal sphincter (EAS)defect demonstrated on endoanal ultrasonography (EUS)were also excluded. Patient selection was based on datacollected from the history, physical examination, conti-nence diary recorded for 14 days (assessing incontinenceepisodes to gas, liquid and solid stool; postevacuation
soiling episodes; and inability to postpone defaecation),Cleveland Clinic FI score (CCFIS)8 and Vaizey score9.Further information on health status and quality of lifewas obtained from questionnaires: Short Form 36 healthsurvey (SF-36; QualityMetric, Lincoln, Rhode Island,USA)10 and Faecal Incontinence Quality of Life (FIQL)11.All patients were assessed with anorectal manometry andEUS.
Implantation technique
The procedure was performed as a day case, underlocal anaesthesia using a posterior perineal block withthe patient placed in the lithotomy position. Four 2-mm skin incisions were made at 3, 6, 9 and 12 o’clockpositions in the perianal area 2 cm from the anal verge.With an Eisenhammer retractor inserted in the analcanal, a dedicated introducer formed by an introducerguide and an external sheath (Fig. 2) was tunnelled fromthe skin incision to the intersphincteric margin, andadvanced into the intersphincteric space until the tipof the introducer reached the level of the puborectalismuscle. The introducer guide was removed, leaving thesheath in the intersphincteric space. The prosthesis wasinserted into the lumen of the introducer sheath andadvanced. When the prosthesis reached the middle–upperanal canal the introducer sheath was removed, leaving theprosthesis in place. The same procedure was repeatedfor all four positions. All prosthesis placement stepswere carried out under direct vision and under EUSguidance (Model 1850 equipped with a system for
a Before implantation b 24 h after implantation
Fig. 1 GatekeeperTM prosthesis a before implantation and b 24 h after implantation
2011 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of SurgeryPublished by John Wiley & Sons Ltd

Novel bulking agent for faecal incontinence
a Guide–sheath assembly
b Prosthesis in sheath
c Prosthesis released from sheath
d EUS check for position of prostheses
Fig. 2 Implantation of GatekeeperTM prosthesis: a metal guide and external sheath assembled together; b following removal of the metalguide, the prosthesis is introduced through the sheath; c the prosthesis is released from the sheath; d the position of the prosthesis ischecked by endoanal ultrasonography (EUS) at the end of the procedure
three-dimensional reconstruction; B-K Medical, Herlev,Copenhagen, Denmark). At the end of procedure, thecorrect positioning of the prostheses was confirmed byEUS (Fig. 2). After the procedure patients were dischargedhome, with advice to avoid heavy physical activity for atleast 48 h. All patients received oral antibiotic prophylaxisfor 3 days.
Follow-up
Patients were reviewed in outpatients at 7, 30 and 90 days,and 6 months thereafter. All patients were recalled forfurther evaluation at the time of study closure. Anorectalmanometry was performed at 30 and 90 days, and atfinal follow-up. Each patient kept a continence diaryfor 14 days before the follow-up appointments 30 and90 days after operation and the last follow-up. Dataobtained from the continence diary were used to calculatethe CCFIS and Vaizey score. At the last follow-upappointment patients were also asked to complete theSF-36 and FIQL questionnaires. All adverse eventsoccurring during the first 3 months after the procedurewere recorded.
Study endpoints
The primary endpoint was safety of the surgicaltechnique assessed as intraoperative and postoperativecomplications, prosthesis displacement and any othermorbidity. Secondary endpoints were therapeutic efficacy
of GatekeeperTM
injection in terms of improvement inFI symptoms, changes in manometric parameters, andchanges in health status and quality of life.
Statistical analysis
Continuous data were presented as mean(s.d.), andcompared using the Wilcoxon test. Fisher’s exact testwas used for analysis of categorical data. P < 0·050 wasconsidered statistically significant. Analyses were carriedout with SPSS version 12.0 software for Windows
(SPSS, Chicago, Illinois, USA).
Results
Fourteen consecutive patients (6 men, 8 women) with amean age of 63·5(17·0) (range 28–83) years were enrolledfrom May 2005 to January 2008. Table 1 shows the history,and baseline clinical and quality-of-life data. All eightwomen enrolled in the study had given birth, two bycaesarean and six by vaginal delivery; four of the vaginaldeliveries included an episiotomy.
Postevacuation soiling was reported to occur always innine patients, sometimes in two, rarely in two and neverin one patient. The mean number of major incontinenceepisodes was 7·1(7·4) per week overall, 6·2(6·0) per weekto liquids and 0·9(1·4) per week to solids. The meanCCFIS was 12·7(3·3) (range 7–18); only three patients hada CCFIS below 10. The mean Vaizey score was 15·4(3·3)(range 11–21). Patients could postpone defaecation for a
2011 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of SurgeryPublished by John Wiley & Sons Ltd
C. Ratto, A. Parello, L. Donisi, F. Litta, V. De Simone, L. Spazzafumo and P. Giordano
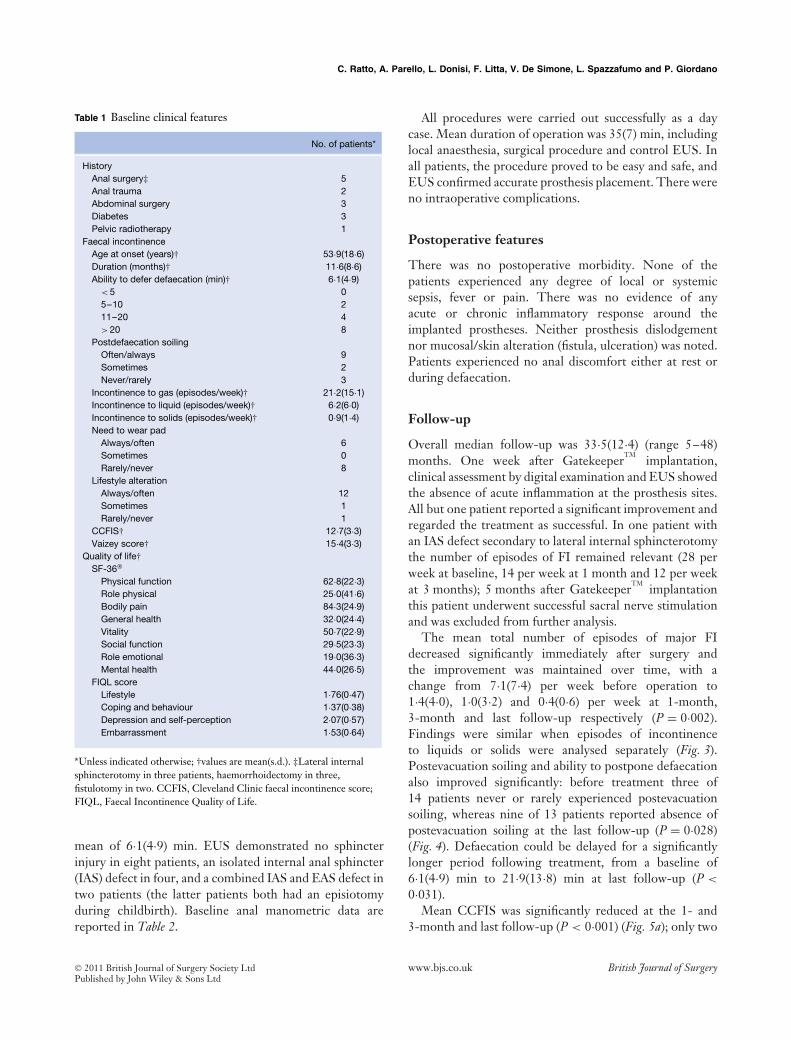
Table 1 Baseline clinical features
No. of patients*
HistoryAnal surgery‡ 5Anal trauma 2Abdominal surgery 3Diabetes 3Pelvic radiotherapy 1
Faecal incontinenceAge at onset (years)† 53·9(18·6)Duration (months)† 11·6(8·6)Ability to defer defaecation (min)† 6·1(4·9)
< 5 05–10 211–20 4> 20 8
Postdefaecation soilingOften/always 9Sometimes 2Never/rarely 3
Incontinence to gas (episodes/week)† 21·2(15·1)Incontinence to liquid (episodes/week)† 6·2(6·0)Incontinence to solids (episodes/week)† 0·9(1·4)Need to wear pad
Always/often 6Sometimes 0Rarely/never 8
Lifestyle alterationAlways/often 12Sometimes 1Rarely/never 1
CCFIS† 12·7(3·3)Vaizey score† 15·4(3·3)
Quality of life†SF-36
Physical function 62·8(22·3)Role physical 25·0(41·6)Bodily pain 84·3(24·9)General health 32·0(24·4)Vitality 50·7(22·9)Social function 29·5(23·3)Role emotional 19·0(36·3)Mental health 44·0(26·5)
FIQL scoreLifestyle 1·76(0·47)Coping and behaviour 1·37(0·38)Depression and self-perception 2·07(0·57)Embarrassment 1·53(0·64)
*Unless indicated otherwise; †values are mean(s.d.). ‡Lateral internalsphincterotomy in three patients, haemorrhoidectomy in three,fistulotomy in two. CCFIS, Cleveland Clinic faecal incontinence score;FIQL, Faecal Incontinence Quality of Life.
mean of 6·1(4·9) min. EUS demonstrated no sphincterinjury in eight patients, an isolated internal anal sphincter(IAS) defect in four, and a combined IAS and EAS defect intwo patients (the latter patients both had an episiotomyduring childbirth). Baseline anal manometric data arereported in Table 2.
All procedures were carried out successfully as a daycase. Mean duration of operation was 35(7) min, includinglocal anaesthesia, surgical procedure and control EUS. Inall patients, the procedure proved to be easy and safe, andEUS confirmed accurate prosthesis placement. There wereno intraoperative complications.
Postoperative features
There was no postoperative morbidity. None of thepatients experienced any degree of local or systemicsepsis, fever or pain. There was no evidence of anyacute or chronic inflammatory response around theimplanted prostheses. Neither prosthesis dislodgementnor mucosal/skin alteration (fistula, ulceration) was noted.Patients experienced no anal discomfort either at rest orduring defaecation.
Follow-up
Overall median follow-up was 33·5(12·4) (range 5–48)months. One week after Gatekeeper
TMimplantation,
clinical assessment by digital examination and EUS showedthe absence of acute inflammation at the prosthesis sites.All but one patient reported a significant improvement andregarded the treatment as successful. In one patient withan IAS defect secondary to lateral internal sphincterotomythe number of episodes of FI remained relevant (28 perweek at baseline, 14 per week at 1 month and 12 per weekat 3 months); 5 months after Gatekeeper
TMimplantation
this patient underwent successful sacral nerve stimulationand was excluded from further analysis.
The mean total number of episodes of major FIdecreased significantly immediately after surgery andthe improvement was maintained over time, with achange from 7·1(7·4) per week before operation to1·4(4·0), 1·0(3·2) and 0·4(0·6) per week at 1-month,3-month and last follow-up respectively (P = 0·002).Findings were similar when episodes of incontinenceto liquids or solids were analysed separately (Fig. 3).Postevacuation soiling and ability to postpone defaecationalso improved significantly: before treatment three of14 patients never or rarely experienced postevacuationsoiling, whereas nine of 13 patients reported absence ofpostevacuation soiling at the last follow-up (P = 0·028)(Fig. 4). Defaecation could be delayed for a significantlylonger period following treatment, from a baseline of6·1(4·9) min to 21·9(13·8) min at last follow-up (P <
0·031).Mean CCFIS was significantly reduced at the 1- and
3-month and last follow-up (P < 0·001) (Fig. 5a); only two
2011 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of SurgeryPublished by John Wiley & Sons Ltd

Novel bulking agent for faecal incontinence
Table 2 Anorectal manometry data
Follow-up
Baseline 1 month 3 months Last P*
Functional anal canal length (cm) 3·0(1·2) 3·6(1·0) 3·5(1·1) 3·5(0·8) 0·065Maximum resting pressure (mmHg) 79·0(30·8) 81·7(31·2) 81·0(29·2) 73·8(33·8) 0·872Mean resting pressure (mmHg) 36·1(14·0) 37·7(15·0) 38·6(17·6) 34·5(16·5) 0·910Squeeze pressure (mmHg) 90·5(66·4) 103·5(63·6) 93·0(58·9) 76·8(59·8) 0·102Threshold rectal sensation (ml) 59·3(31·7) 73·4(44·1) 73·9(42·0) 75·0(38·0) 0·115Urge rectal sensation (ml) 105·6(42·8) 121·1(55·3) 124·6(45·4) 131·1(49·9) 0·097Rectal maximum tolerated volume (ml) 153·9(52·5) 181·4(74·5) 179·3(68·7) 190·0(60·5) 0·084
Values are mean(s.d.). *Baseline versus 1 month versus 3 months versus last follow-up (Wilcoxon test). There were no significant differences betweenfollow-up and baseline values.
16
Total
12
8
4
0
No.
of e
piso
des
of F
I per
wee
k
Baseline Last follow-up
Liquid
Solid
Fig. 3 Mean(s.d.) number of episodes of major faecalincontinence (FI) overall, to liquid and to solid faeces at baselineand last follow-up after GatekeeperTM implantation. *P < 0·050versus baseline (Wilcoxon test)
12
10
8
6
4
2
0
No.
of p
atie
nts
Baseline Last follow-up
Never/rarely
Sometimes
Often/always
Fig. 4 Number of patients affected by soiling and symptomfrequency at baseline and last follow-up after GatekeeperTM
implantation. P = 0·028 (Fisher’s exact test)
20
15
10
5
0
CC
FIS
Baseline 1 month 3 months Last follow-up
a CCFIS
24
18
12
6
0
Vai
zey
scor
e
Baseline 1 month 3 months Last follow-up
b Vaizey score
Fig. 5 Mean(s.d.) a Cleveland Clinic faecal incontinence score (CCFIS) and b Vaizey score at baseline and during follow-up afterGatekeeperTM implantation. a P < 0·001, b P = 0·010 (Wilcoxon test)
2011 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of SurgeryPublished by John Wiley & Sons Ltd
C. Ratto, A. Parello, L. Donisi, F. Litta, V. De Simone, L. Spazzafumo and P. Giordano
of 13 patients had a CCFIS higher than 7 at the finalevaluation. Mean Vaizey score changed from a baseline of15·4(3·3) to 7·1(3·9), 4·7(3·0) and 6·9(5·0) at 1-month, 3-month and last follow-up respectively (P = 0·010) (Fig. 5b).
There was no correlation between anal sphincter defecton EUS and clinical outcome, with no differences betweenthe subset of patients without sphincter lesions and thosewith sphincter disruption.
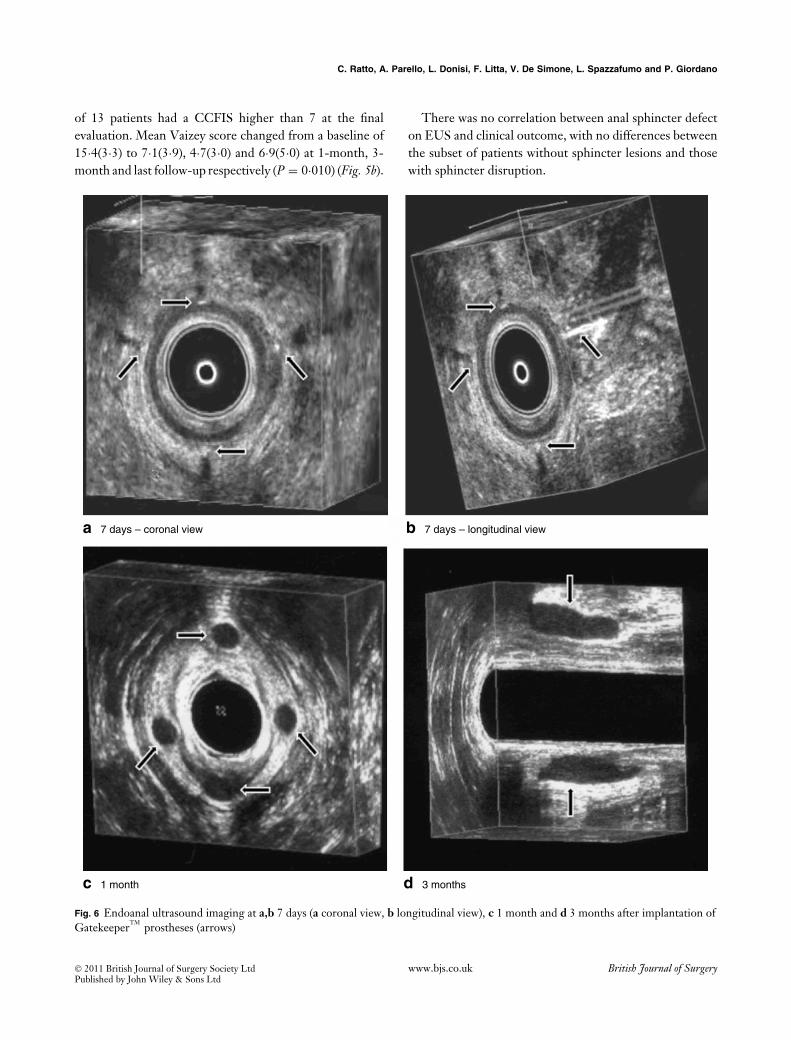
a 7 days – coronal view b 7 days – longitudinal view
c 1 month d 3 months
Fig. 6 Endoanal ultrasound imaging at a,b 7 days (a coronal view, b longitudinal view), c 1 month and d 3 months after implantation ofGatekeeperTM prostheses (arrows)
2011 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of SurgeryPublished by John Wiley & Sons Ltd
Novel bulking agent for faecal incontinence
100
80
60
40
20
0Physicalfunction
Rolephysical
Bodilypain
Generalhealth
Vitality Socialfunction
Roleemotional
Mentalhealth
SF
-36
sco
re
5
4
3
2
1
0
FIQ
L sc
ore
Lifestyle Coping andbehaviour
Depression andself-perception
Embarrassment
a SF-36
b FIQL
Baseline
Follow-up
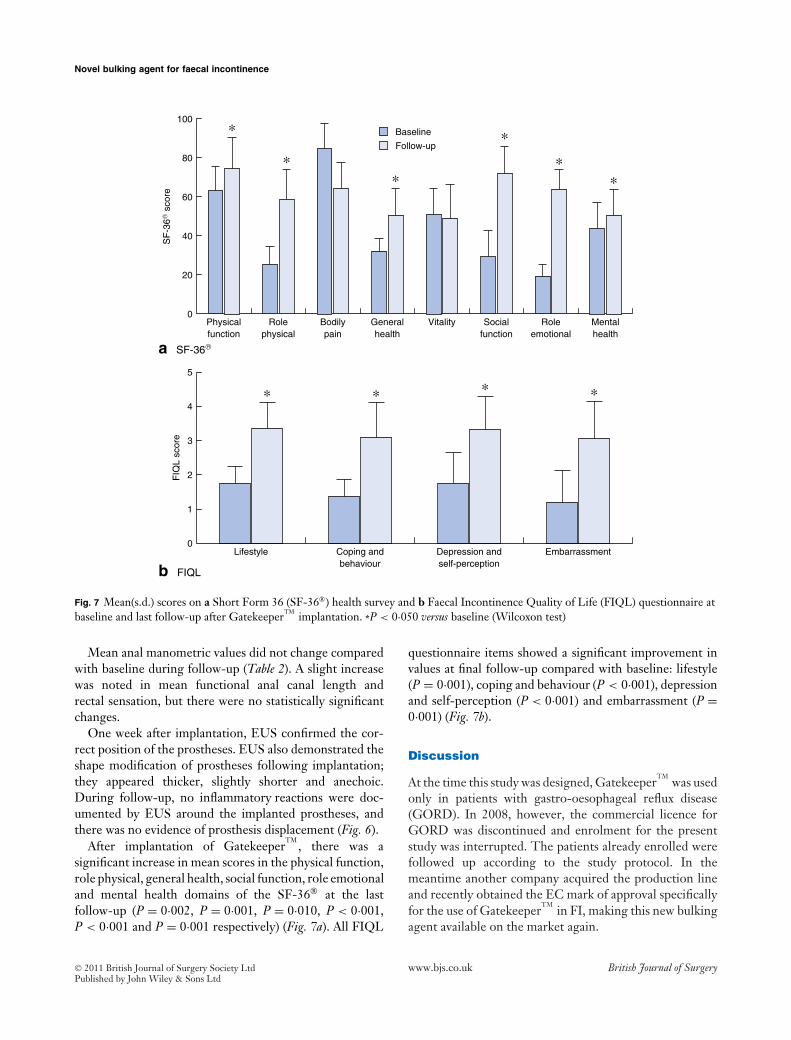
Fig. 7 Mean(s.d.) scores on a Short Form 36 (SF-36) health survey and b Faecal Incontinence Quality of Life (FIQL) questionnaire atbaseline and last follow-up after GatekeeperTM implantation. *P < 0·050 versus baseline (Wilcoxon test)
Mean anal manometric values did not change comparedwith baseline during follow-up (Table 2). A slight increasewas noted in mean functional anal canal length andrectal sensation, but there were no statistically significantchanges.
One week after implantation, EUS confirmed the cor-rect position of the prostheses. EUS also demonstrated theshape modification of prostheses following implantation;they appeared thicker, slightly shorter and anechoic.During follow-up, no inflammatory reactions were doc-umented by EUS around the implanted prostheses, andthere was no evidence of prosthesis displacement (Fig. 6).
After implantation of GatekeeperTM
, there was asignificant increase in mean scores in the physical function,role physical, general health, social function, role emotionaland mental health domains of the SF-36 at the lastfollow-up (P = 0·002, P = 0·001, P = 0·010, P < 0·001,P < 0·001 and P = 0·001 respectively) (Fig. 7a). All FIQL
questionnaire items showed a significant improvement invalues at final follow-up compared with baseline: lifestyle(P = 0·001), coping and behaviour (P < 0·001), depressionand self-perception (P < 0·001) and embarrassment (P =0·001) (Fig. 7b).
Discussion
At the time this study was designed, GatekeeperTM
was usedonly in patients with gastro-oesophageal reflux disease(GORD). In 2008, however, the commercial licence forGORD was discontinued and enrolment for the presentstudy was interrupted. The patients already enrolled werefollowed up according to the study protocol. In themeantime another company acquired the production lineand recently obtained the EC mark of approval specificallyfor the use of Gatekeeper
TMin FI, making this new bulking
agent available on the market again.
2011 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of SurgeryPublished by John Wiley & Sons Ltd

C. Ratto, A. Parello, L. Donisi, F. Litta, V. De Simone, L. Spazzafumo and P. Giordano
GatekeeperTM
prostheses are made of a unique material(HYEXPAN
TM) that is solid at the time of delivery, but
slowly absorbs water and expands once implanted. Within48 h the prosthesis has reached its final size and shape. Atthis stage the consistency of the material has changed fromhard to soft, giving the implant a pliable texture that makesit compliant to external pressures without losing its originalshape. For these reasons it was decided to place the implantsin the intersphincteric space, in the belief that this wouldachieve a more effective distribution of the bulking effectthan would be achieved with submucosal positioning, andthus exploiting the physical characteristic of the implantmost effectively. The intersphincteric location shouldalso minimize the potential risk of erosion, ulceration,fistulation of the anal canal and possible displacement of theprosthesis. This is particularly important in view of the solidstate of the prostheses at the time of implantation. In thisseries there were no complications related to implantationof the prostheses, and ultrasonographic surveillance fora mean of almost 3 years confirmed that none of theimplants had become displaced. The ultrasound results alsoshowed that the size of all prostheses remained virtuallyunchanged over time, thus confirming the durability ofthe Gatekeeper
TM. The present cohort included not only
patients with an intact IAS but also those with an IAStear, or both IAS and EAS defects; patients with isolatedEAS defects, however, were excluded. The prostheses wereplaced in the same position in all patients, irrespective ofthe location of the sphincter lesion.
Skin incisions were made about 2 cm away from the analverge to minimize the risk of wound contamination duringbowel movements. The non-linear tunnelling through thesoft subcutaneous tissues to reach the intersphincteric planefrom the skin incision should also avoid possible prosthesisextrusion along the track. Prosthesis placement was per-formed under EUS guidance, to control the procedure stepby step and ensure correct positioning of the prostheses.The operator could easily reach the intersphincteric spaceand decide on the exact position for each prosthesis. More-over, the introducer could be followed by direct visionand digital palpation, and visualized by EUS. Therefore,lesions in the rectoanal mucosal/submucosal layer could beavoided. The contribution of EUS during Gatekeeper
TM
placement was fundamental to guiding placement of theprosthesis. However, the authors do not believe that it isnecessarily mandatory; the procedure could be performedsafely under digital guidance by an experienced clinician.Four prostheses were always implanted; this choice wasarbitrary but seemed effective. The prostheses were placedat 3, 6, 9 and 12 o’clock positions for convenience but it islikely that, provided the implants are inserted correctly and
distributed equally around the anal canal, the actual posi-tion may not influence the outcome. Whether the numberof prostheses implanted influences the outcome is not clearat this stage.
In recent literature reviews, Vaizey and Kamm12 andVaizey and Maeda13 analysed available data on thevarious bulking agents used in FI. A paucity of reportsconcerning different types of agent makes it difficult toestablish which is truly effective. In a Cochrane review,Maeda and colleagues14 found only four eligible random-ized trials7,15–17, including a total of 176 patients treatedwith injectable bulking agents: hydrogel cross-linkedwith polyacrylamide (Bulkamid
TM; Contura, Soeborg,
Denmark)7, porcine dermal collagen (PermacolTM
; Covi-dien, Dublin, Ireland)7, polydimethylsiloxane elastomerimplants15,16, silicone biomaterial (PTQ
TM; Uroplasty,
Geleen, The Netherlands)17 and carbon-coated beads(Durasphere; Carbon Medical Technologies, St Paul,Minnesota, USA)17. Unfortunately, the review authorsfound significant concerns of bias in all trials but one.They were unable to demonstrate significant effectivenessof perianal injection of bulking agents owing to the limitednumber of identified trials together with methodologicalweaknesses. Moreover, with limited follow-up (maximum12 months) only a short-term benefit from injections wasreported, regardless of the material used. A silicone bio-material (PTQ
TM) provided some advantages and was safer
in treating FI than carbon-coated beads (Durasphere)in the short term. However, PTQ
TMdid not show obvi-
ous clinical benefit compared with normal saline injection.Delivery of the bulking agent under ultrasound guidance,compared with digital guidance, was more effective.
The major problem with other anal bulking agentsused so far is their reduced efficacy with time, probablydue to a variable combination of degradation and/ordiffusion through the tissue adjacent to the injection site or,sometimes, far from that site (Contigen, Bard, Covington,Georgia, USA; Zuidex
TM, Q-Med, Uppsala, Sweden). The
present data suggest that the GatekeeperTM
overcomes all ofthese potential problems. In this preliminary experience,implantation of the Gatekeeper
TMin the anal canal was
safe, without any morbidity, either during or after surgery.The entire procedure was painless and well tolerated.Wounds healed in all patients and no discomfort was notedeither at rest or on defaecation. Adverse events, sometimessevere, have been described for some other bulking agentsused in urinary incontinence or FI, including pulmonaryembolism, fatal stroke, periurethral mass and suspecteddisease transmission18–21. No adverse events were reportedin the present series.
2011 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of SurgeryPublished by John Wiley & Sons Ltd

Novel bulking agent for faecal incontinence
Of utmost importance was the significant improvementin episodes of major FI and both CCFIS and Vaizeyscore. Ability to postpone defaecation for longer andpostevacuation soiling were both significantly improved inthe majority of patients. Of note was the improvement inboth SF-36 and FIQL scores in this series, suggestingregained health and quality of life in patients treatedwith Gatekeeper
TM. Furthermore, findings observed in the
short and medium term appeared substantially unchangedat the final evaluation. This is important as some ofthe other bulking agents demonstrated very poor long-term results and have had no further clinical use despitepreliminary reports suggesting good clinical effectiveness(polytetrafluoroethylene, autologous fat1,2).
This preliminary study demonstrated that theGatekeeper
TManal implant was a safe, reliable and effective
treatment for FI, with results maintained over time. Theseresults call for larger series and longer follow-up better toestablish the role of the Gatekeeper
TMin the management
of FI.
Acknowledgements
The authors declare no conflict of interest.
References
1 Shafik A. Polytetrafluoroethylene injection for the treatmentof partial fecal incontinence. Int Surg 1993; 78: 159–161.
2 Shafik A. Perianal injection of autologous fat for treatment ofsphincteric incontinence. Dis Colon Rectum 1995; 38:583–587.
3 Kumar D, Benson MJ, Bland JE. Glutaraldehydecross-linked collagen in the treatment of faecal incontinence.Br J Surg 1998; 85: 978–979.
4 Malouf AJ, Vaizey CJ, Norton CS, Kamm MA. Internal analsphincter augmentation for fecal incontinence usinginjectable silicone biomaterial. Dis Colon Rectum 2001; 44:595–600.
5 Davis K, Kumar D, Poloniecki J. Preliminary evaluation ofan injectable anal sphincter bulking agent (Durasphere) inthe management of faecal incontinence. Aliment PharmacolTher 2003; 18: 237–243.
6 Ganio E, Trompetto M, Realis Luc A, Clerico G. Initialclinical results using Coaptite for the treatment of fecalincontinence. Dis Colon Rectum 2004; 47: 569.
7 Maeda Y, Vaizey CJ, Kamm MA. Pilot study of two newinjectable bulking agents for the treatment of faecalincontinence. Colorectal Dis 2008; 10: 268–272.
8 Jorge JM, Wexner SD. Etiology and management of faecalincontinence. Dis Colon Rectum 1993; 36: 77–97.
9 Vaizey CJ, Carapeti E, Cahill JA, Kamm MA. Prospectivecomparison of faecal incontinence grading systems. Gut1999; 44: 77–80.
10 Ware JE Jr, Sherbourne CD. The MOS 36-item short-formhealth survey (SF-36). I. Conceptual framework and itemselection. Med Care 1992; 30: 473–483.
11 Rockwood TH, Church JM, Fleshman JW, Kane RL,Mavrantonis C, Thorson AG et al. Fecal IncontinenceQuality of Life Scale: quality of life instrument for patientswith fecal incontinence. Dis Colon Rectum 2000; 43: 9–16.
12 Vaizey CJ, Kamm MA. Injectable bulking agents for treatingfaecal incontinence. Br J Surg 2005; 92: 521–527.
13 Vaizey CJ, Maeda Y. Injectable bulking agents. In FecalIncontinence. Diagnosis and Treatment, Ratto C, Doglietto GB,Lowry AC, Pahlman L, Romano G (eds). Springer: Milan,2007; 221–226.
14 Maeda Y, Lauberg S, Norton C. Perianal injectable bulkingagents as treatment for faecal incontinence in adults. CochraneDatabase Syst Rev 2010; (5)CD007959.
15 Tjandra JJ, Lim JF, Hiscock R, Rajendra P. Injectablesilicone biomaterial for fecal incontinence caused by internalanal sphincter dysfunction is effective. Dis Colon Rectum 2004;47: 2138–2146.
16 Siproudhis L, Morcet J, Laine F. Elastomer implantsin faecal incontinence: a blind, randomized placebo-controlled study. Aliment Pharmacol Ther 2007; 25:1125–1132.
17 Tjandra JJ, Chan MK, Yeh HC. Injectable siliconebiomaterial (PTQ) is more effective than carbon-coatedbeads (Durasphere) in treating passive faecal incontinence – arandomized trial. Colorectal Dis 2009; 11: 382–389.
18 Currie I, Drutz HP, Deck J, Oxorn D. Adipose tissue andlipid droplet embolism following periurethral injection ofautologous fat: case report and review of the literature. IntUrogynecol J Pelvic Floor Dysfunct 1997; 8: 377–380.
19 Sweat SD, Lightener DJ. Complications of sterile abscessformation and pulmonary embolism following periurethralbulking agents. J Urol 1999; 161: 93–96.
20 Yoon SS, Chang DI, Chung KC. Acute fatal strokeimmediately following autologous fat injection into the face.Neurology 2003; 61: 1151–1152.
21 Stojkovic SG, Lim M, Burke D, Finan PJ, Sagar PM.Intra-anal collagen injection for the treatment of faecalincontinence. Br J Surg 2006; 93: 1514–1518.
2011 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of SurgeryPublished by John Wiley & Sons Ltd

Original article
Assessment of haemorrhoidal artery network using colourduplex imaging and clinical implications
C. Ratto, A. Parello, L. Donisi, F. Litta, G. Zaccone and G. B. DogliettoDepartment of Surgical Sciences, Catholic University, Largo A. Gemelli, 8, 00168, Rome, ItalyCorrespondence to: Dr C. Ratto (e-mail: [email protected])
Background: Dearterialization should reduce arterial overflow to haemorrhoids. The purpose of thisstudy was to assess the topography of haemorrhoidal arteries.Methods: Fifty patients with haemorrhoidal disease were studied. Using endorectal ultrasonography, sixsectors were identified within the lower rectal circumference. Starting from the highest level (6 cm abovethe anorectal junction), the same procedure was repeated every 1 cm until the lowest level was reached(1 cm above the anorectal junction). Colour duplex imaging examinations identified haemorrhoidalarteries related to the rectal wall layers, and the arterial depth was calculated.Results: Haemorrhoidal arteries were detected in 64·3, 66·0, 66·0, 98·3, 99·3 and 99·7 per cent ofthe sectors 6, 5, 4, 3, 2 and 1 cm above the anorectal junction respectively (P < 0·001). Most ofthe haemorrhoidal arteries were external to the rectal wall at 6 and 5 cm (97·9 and 90·9 per cent),intramuscular at 4 cm (55·0 per cent), and within the submucosa at 3, 2 and 1 cm above the anorectaljunction (67·1, 96·6 and 100 per cent) (P < 0·001). The mean arterial depth decreased significantly from8·3 mm at 6 cm to 1·9 mm at 1 cm above the anorectal junction (P < 0·001).Conclusion: This study demonstrated that the vast majority of haemorrhoidal arteries lie within therectal submucosa at the lowest 2 cm above the anorectal junction. This should therefore be the best sitefor performing haemorrhoidal dearterialization.
Presented in part to the Annual Meeting of the American Society of Colon and Rectal Surgeons, Minneapolis, Minnesota,USA, May 2010, and published in abstract form as Dis Colon Rectum 2010; 53: 578
Paper accepted 4 August 2011Published online in Wiley Online Library (www.bjs.co.uk). DOI: 10.1002/bjs.7700
Introduction
The anatomical and physiological characteristics of haem-orrhoids have not been elucidated fully. Microscopically,haemorrhoidal piles are sinusoids (vascular structureswithout a muscular wall)1. Direct arteriovenous com-munications have been demonstrated histologically andradiologically, and some authors have noted a resemblanceto erectile tissue2. Traditionally, haemorrhoidal piles fre-quently appear to be localized to the left lateral, rightposterolateral and right anterolateral sites in the anal canalcircumference with the patient in the lithotomy position;however, this configuration is demonstrated in less than20 per cent of patients3. In reality, a wider network ofarterial and venous vessels has been described4, althoughthe distribution and relationship to rectal and anal layers isunclear.
Recently, haemorrhoidal disease (HD) has often beentreated using non-excisional procedures. Some surgical
techniques address the reduction of arterial inflow tohaemorrhoids.
Transanal haemorrhoidal dearterialization (THD) andDoppler-guided haemorrhoidal artery ligation (DG-HAL)are the main surgical procedures with this aim, anduse specifically designed devices for arterial ligation inthe lower rectum guided by a Doppler signal5. Stapledhaemorrhoidopexy (SH) divides the haemorrhoidal arteriesin the suture line6.
Assessment of the optimal site for these surgicalapproaches should improve the clinical efficacy. Thepurpose of this study was to localize precisely the arteriesrunning into the rectum and directed to haemorrhoids.
Methods
The local institutional review board approved this study.Patients with HD were enrolled prospectively. Each patientsigned an informed consent form regarding the procedures
2011 British Journal of Surgery Society Ltd British Journal of SurgeryPublished by John Wiley & Sons Ltd
C. Ratto, A. Parello, L. Donisi, F. Litta, G. Zaccone and G. B. Doglietto
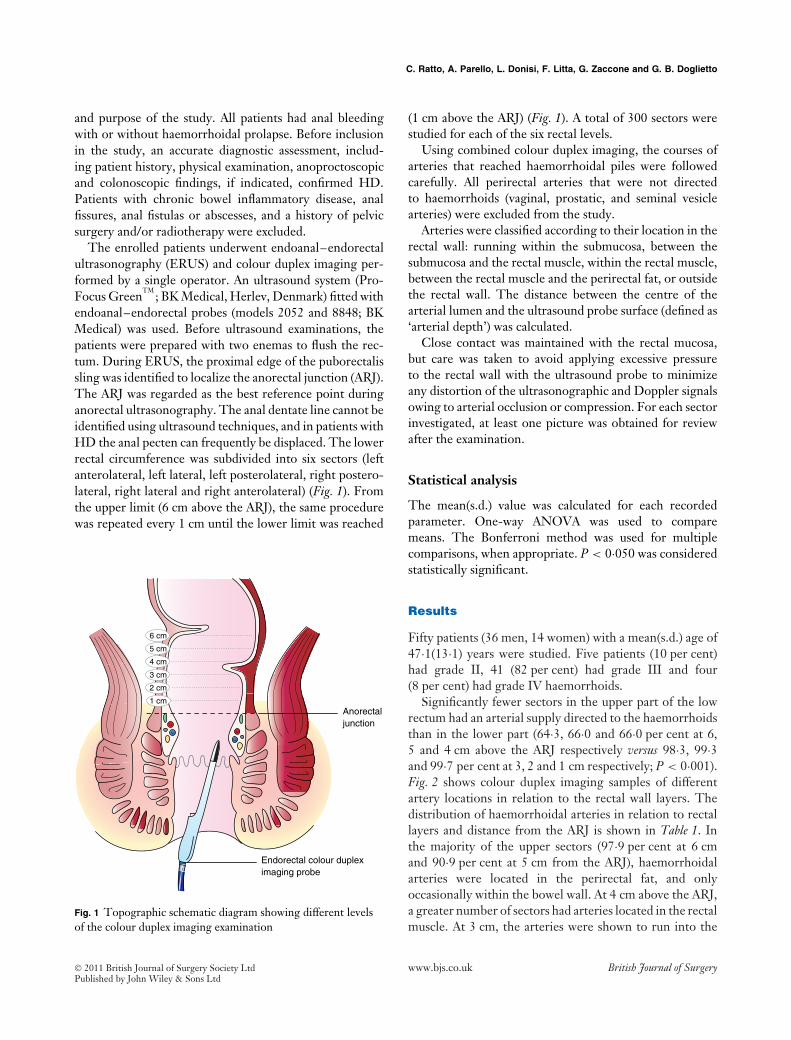
and purpose of the study. All patients had anal bleedingwith or without haemorrhoidal prolapse. Before inclusionin the study, an accurate diagnostic assessment, includ-ing patient history, physical examination, anoproctoscopicand colonoscopic findings, if indicated, confirmed HD.Patients with chronic bowel inflammatory disease, analfissures, anal fistulas or abscesses, and a history of pelvicsurgery and/or radiotherapy were excluded.
The enrolled patients underwent endoanal–endorectalultrasonography (ERUS) and colour duplex imaging per-formed by a single operator. An ultrasound system (Pro-Focus Green
TM; BK Medical, Herlev, Denmark) fitted with
endoanal–endorectal probes (models 2052 and 8848; BKMedical) was used. Before ultrasound examinations, thepatients were prepared with two enemas to flush the rec-tum. During ERUS, the proximal edge of the puborectalissling was identified to localize the anorectal junction (ARJ).The ARJ was regarded as the best reference point duringanorectal ultrasonography. The anal dentate line cannot beidentified using ultrasound techniques, and in patients withHD the anal pecten can frequently be displaced. The lowerrectal circumference was subdivided into six sectors (leftanterolateral, left lateral, left posterolateral, right postero-lateral, right lateral and right anterolateral) (Fig. 1). Fromthe upper limit (6 cm above the ARJ), the same procedurewas repeated every 1 cm until the lower limit was reached
Anorectaljunction
3 cm
2 cm
1 cm
4 cm
5 cm
6 cm
Endorectal colour dupleximaging probe
Fig. 1 Topographic schematic diagram showing different levelsof the colour duplex imaging examination
(1 cm above the ARJ) (Fig. 1). A total of 300 sectors werestudied for each of the six rectal levels.
Using combined colour duplex imaging, the courses ofarteries that reached haemorrhoidal piles were followedcarefully. All perirectal arteries that were not directedto haemorrhoids (vaginal, prostatic, and seminal vesiclearteries) were excluded from the study.
Arteries were classified according to their location in therectal wall: running within the submucosa, between thesubmucosa and the rectal muscle, within the rectal muscle,between the rectal muscle and the perirectal fat, or outsidethe rectal wall. The distance between the centre of thearterial lumen and the ultrasound probe surface (defined as‘arterial depth’) was calculated.
Close contact was maintained with the rectal mucosa,but care was taken to avoid applying excessive pressureto the rectal wall with the ultrasound probe to minimizeany distortion of the ultrasonographic and Doppler signalsowing to arterial occlusion or compression. For each sectorinvestigated, at least one picture was obtained for reviewafter the examination.
Statistical analysis
The mean(s.d.) value was calculated for each recordedparameter. One-way ANOVA was used to comparemeans. The Bonferroni method was used for multiplecomparisons, when appropriate. P < 0·050 was consideredstatistically significant.
Results
Fifty patients (36 men, 14 women) with a mean(s.d.) age of47·1(13·1) years were studied. Five patients (10 per cent)had grade II, 41 (82 per cent) had grade III and four(8 per cent) had grade IV haemorrhoids.
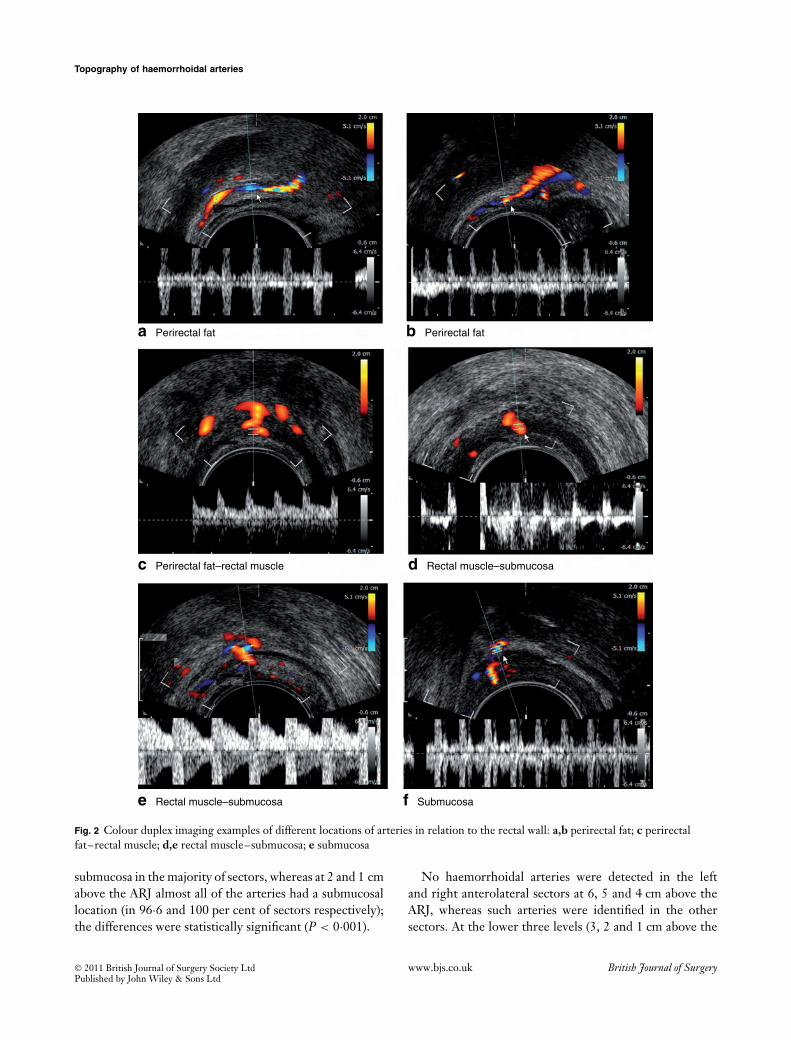
Significantly fewer sectors in the upper part of the lowrectum had an arterial supply directed to the haemorrhoidsthan in the lower part (64·3, 66·0 and 66·0 per cent at 6,5 and 4 cm above the ARJ respectively versus 98·3, 99·3and 99·7 per cent at 3, 2 and 1 cm respectively; P < 0·001).Fig. 2 shows colour duplex imaging samples of differentartery locations in relation to the rectal wall layers. Thedistribution of haemorrhoidal arteries in relation to rectallayers and distance from the ARJ is shown in Table 1. Inthe majority of the upper sectors (97·9 per cent at 6 cmand 90·9 per cent at 5 cm from the ARJ), haemorrhoidalarteries were located in the perirectal fat, and onlyoccasionally within the bowel wall. At 4 cm above the ARJ,a greater number of sectors had arteries located in the rectalmuscle. At 3 cm, the arteries were shown to run into the
2011 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of SurgeryPublished by John Wiley & Sons Ltd
Topography of haemorrhoidal arteries
a Perirectal fat b Perirectal fat
c Perirectal fat–rectal muscle d Rectal muscle–submucosa
e Rectal muscle–submucosa f Submucosa
Fig. 2 Colour duplex imaging examples of different locations of arteries in relation to the rectal wall: a,b perirectal fat; c perirectalfat–rectal muscle; d,e rectal muscle–submucosa; e submucosa
submucosa in the majority of sectors, whereas at 2 and 1 cmabove the ARJ almost all of the arteries had a submucosallocation (in 96·6 and 100 per cent of sectors respectively);the differences were statistically significant (P < 0·001).
No haemorrhoidal arteries were detected in the leftand right anterolateral sectors at 6, 5 and 4 cm above theARJ, whereas such arteries were identified in the othersectors. At the lower three levels (3, 2 and 1 cm above the
2011 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of SurgeryPublished by John Wiley & Sons Ltd
C. Ratto, A. Parello, L. Donisi, F. Litta, G. Zaccone and G. B. Doglietto
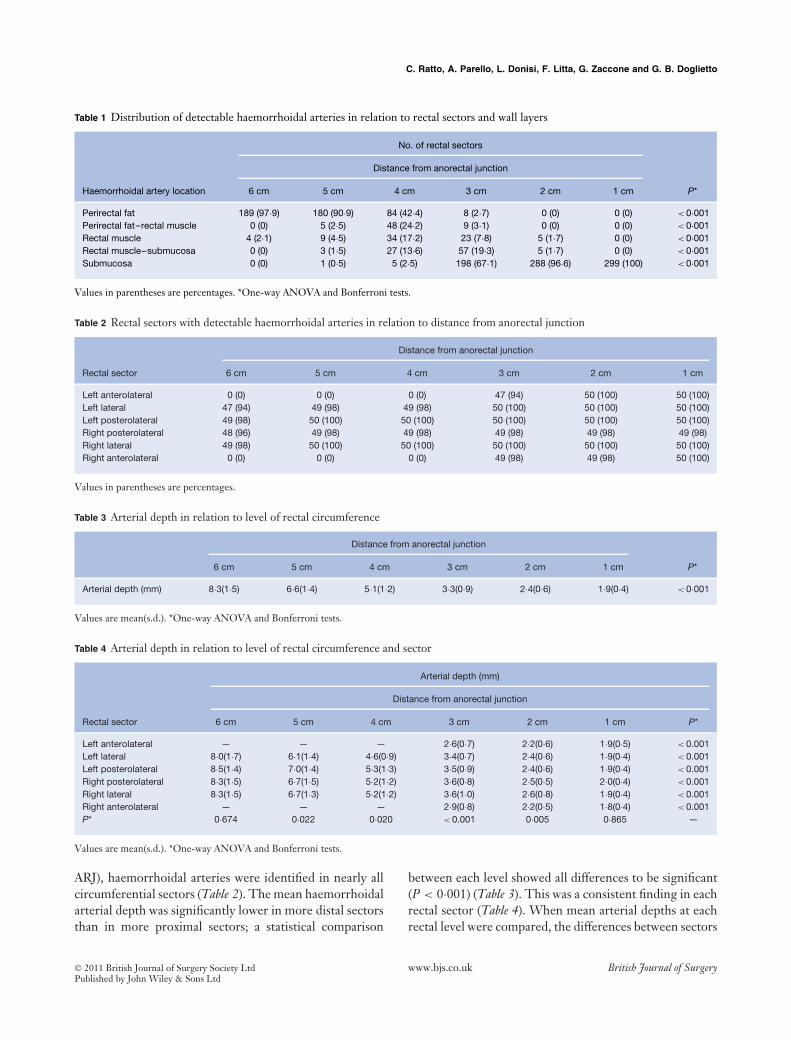
Table 1 Distribution of detectable haemorrhoidal arteries in relation to rectal sectors and wall layers
No. of rectal sectors
Distance from anorectal junction
Haemorrhoidal artery location 6 cm 5 cm 4 cm 3 cm 2 cm 1 cm P*
Perirectal fat 189 (97·9) 180 (90·9) 84 (42·4) 8 (2·7) 0 (0) 0 (0) < 0·001Perirectal fat–rectal muscle 0 (0) 5 (2·5) 48 (24·2) 9 (3·1) 0 (0) 0 (0) < 0·001Rectal muscle 4 (2·1) 9 (4·5) 34 (17·2) 23 (7·8) 5 (1·7) 0 (0) < 0·001Rectal muscle–submucosa 0 (0) 3 (1·5) 27 (13·6) 57 (19·3) 5 (1·7) 0 (0) < 0·001Submucosa 0 (0) 1 (0·5) 5 (2·5) 198 (67·1) 288 (96·6) 299 (100) < 0·001
Values in parentheses are percentages. *One-way ANOVA and Bonferroni tests.
Table 2 Rectal sectors with detectable haemorrhoidal arteries in relation to distance from anorectal junction
Distance from anorectal junction
Rectal sector 6 cm 5 cm 4 cm 3 cm 2 cm 1 cm
Left anterolateral 0 (0) 0 (0) 0 (0) 47 (94) 50 (100) 50 (100)Left lateral 47 (94) 49 (98) 49 (98) 50 (100) 50 (100) 50 (100)Left posterolateral 49 (98) 50 (100) 50 (100) 50 (100) 50 (100) 50 (100)Right posterolateral 48 (96) 49 (98) 49 (98) 49 (98) 49 (98) 49 (98)Right lateral 49 (98) 50 (100) 50 (100) 50 (100) 50 (100) 50 (100)Right anterolateral 0 (0) 0 (0) 0 (0) 49 (98) 49 (98) 50 (100)
Values in parentheses are percentages.
Table 3 Arterial depth in relation to level of rectal circumference
Distance from anorectal junction
6 cm 5 cm 4 cm 3 cm 2 cm 1 cm P*
Arterial depth (mm) 8·3(1·5) 6·6(1·4) 5·1(1·2) 3·3(0·9) 2·4(0·6) 1·9(0·4) < 0·001
Values are mean(s.d.). *One-way ANOVA and Bonferroni tests.
Table 4 Arterial depth in relation to level of rectal circumference and sector
Arterial depth (mm)
Distance from anorectal junction
Rectal sector 6 cm 5 cm 4 cm 3 cm 2 cm 1 cm P*
Left anterolateral — — — 2·6(0·7) 2·2(0·6) 1·9(0·5) < 0.001Left lateral 8·0(1·7) 6·1(1·4) 4·6(0·9) 3·4(0·7) 2·4(0·6) 1·9(0·4) < 0.001Left posterolateral 8·5(1·4) 7·0(1·4) 5·3(1·3) 3·5(0·9) 2·4(0·6) 1·9(0·4) < 0.001Right posterolateral 8·3(1·5) 6·7(1·5) 5·2(1·2) 3·6(0·8) 2·5(0·5) 2·0(0·4) < 0.001Right lateral 8·3(1·5) 6·7(1·3) 5·2(1·2) 3·6(1·0) 2·6(0·8) 1·9(0·4) < 0.001Right anterolateral — — — 2·9(0·8) 2·2(0·5) 1·8(0·4) < 0.001P* 0·674 0·022 0·020 < 0.001 0·005 0·865 —
Values are mean(s.d.). *One-way ANOVA and Bonferroni tests.
ARJ), haemorrhoidal arteries were identified in nearly allcircumferential sectors (Table 2). The mean haemorrhoidalarterial depth was significantly lower in more distal sectorsthan in more proximal sectors; a statistical comparison
between each level showed all differences to be significant(P < 0·001) (Table 3). This was a consistent finding in eachrectal sector (Table 4). When mean arterial depths at eachrectal level were compared, the differences between sectors
2011 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of SurgeryPublished by John Wiley & Sons Ltd

Topography of haemorrhoidal arteries
were not statistically different at 6 cm above (P = 0·674)or 1 cm below (P = 0·865) the ARJ, whereas differencesbetween sectors were statistically significant at 5, 4, 3 and2 cm above the ARJ (P = 0·022, P = 0·020, P < 0·001 andP = 0·005 respectively).
Discussion
The pathogenesis of HD is unclear, but is probably multi-factorial. A number of elements have been claimed to becausative or predisposing factors. Disruption of supportivetissue surrounding haemorrhoids is considered to be animportant factor in haemorrhoidal prolapse7 and a numberof inflammatory mediators have also been cited8,9. A hyper-tonic internal anal sphincter has frequently been associatedwith HD and is regarded as a possible cause of haem-orrhoidal symptoms10. Haemorrhoidal vascularizationappears to play a central role in the pathophysiology of HD.
Hyperplasia of the arteriovenous network within theanorectal submucosa (corpus cavernosum recti, CCR)results in increased vascular pressure. Blood overflow tothe CCR should also cause increased intravascular pres-sure, and is thus a significant predisposing factor forHD11. Aigner and colleagues12 confirmed the relationshipbetween arterial overflow and HD. Using a transperinealDoppler probe to investigate haemorrhoidal arteries, theyfound a significantly higher arterial calibre and flow veloc-ity in patients with HD compared with controls. They thenhypothesized that the coordinated filling and drainage ofthe anorectal vascular plexus is regulated by the intrinsicvascular sphincter mechanism, and that the morpholog-ical and functional failure of this vascular system maycontribute to the development of HD13.
A comprehensive understanding of anorectal vascular-ization should contribute to outlining the pathophysiologyof HD. A recent study by Schuurman and co-workers14
highlighted how vascularization of the CCR is providedalmost exclusively by branches of the superior rectal artery(SRA), a terminal branch of the inferior mesenteric artery.A previous study by Shafik and Mostafa15 indicated thatthe lower half of the rectum is vascularized by the terminalbranches of the SRA (two or three main branches), withplexiform patterns at the ends. The middle rectal artery hasbeen reported in only 50 per cent of cadaver specimens15,and the functional role of this artery seems negligiblein light of these anatomical inconsistencies. DiDio andcolleagues16 also studied the middle rectal artery in 30cadavers; it was present in 56·7 per cent of specimens,bilaterally (36·7 per cent) or unilaterally (20·0 per cent).The middle rectal artery arose from the internal puden-dal artery in 40 per cent of specimens, the inferior gluteal
artery in 26·7 per cent, and the internal iliac artery in16·8 per cent. The consistent findings of the above stud-ies appear to demonstrate that the SRA branches play apredominant role in CCR vascularization. Therefore, it isparticularly important to define the topography of thesevessels within the rectal–perirectal area. Aigner et al.17
analysed five macroscopic preparations of human pelvis;they described the division of the SRA into left and rightbranches, then into three to five terminal branches pen-etrating the rectal wall in the middle and lower rectum.On examining microscopic preparations from 27 fetuses,they identified two to four terminal vessels penetrating therectal wall and reaching the submucosa, especially in theposterolateral position (71 per cent of specimens)17.
In the present study, the majority of arterial branches atthe three highest levels (6, 5 and 4 cm from the ARJ) werelocated outside the rectal wall in the right lateral, right pos-terolateral, left posterolateral and left lateral sectors, wherethese vessels arise. In contrast, no haemorrhoidal arterieswere detected in several sectors in the higher three levels;in particular, none was found in the right and left antero-lateral sectors. These findings suggest that the arterialpulses detected by Doppler ultrasonography in the ante-rior highest three levels of the low rectum during surgicalprocedures using this technology can be regarded as beinggenerated by vessels that are not directed to haemorrhoids.In contrast, in the lower 2 cm, haemorrhoidal arteries weredetected in 98 per cent of sectors; specifically, at 2 and 1 cmfrom the ARJ, arteries were identified in the submucosain 96·6 per cent and 100 per cent of sectors respectively.These features can be confirmed easily during Doppler-guided surgical procedures. Investigation of the position ofthe arteries in relation to rectal layers and levels showed thatthe mean arterial depth decreased significantly from thehighest to the lowest level, reaching the shallowest depthat the most distal 2 cm of the rectum where nearly all of thearteries were in the submucosa; this feature was invariablyfound regardless of the circumferential sector investigated.
Both anatomical and physiological evidence obtainedfrom the literature and the present study has implicationsfor the various therapeutic approaches that are currentlyavailable. In this regard, the most innovative surgicaltechniques are SH (also known as Longo’s technique)and Doppler-guided ligation of haemorrhoidal arteries,including THD and DG-HAL techniques. The goal of thefirst method is to treat haemorrhoidal prolapse by resectingthe rectal mucosa approximately 3–4 cm above the den-tate line18; however, the level of anastomosis is frequentlyunpredictable as it is affected by the traction applied to thepreviously performed rectal purse-string. In fact, it has beenestablished that, even though SH is performed according
2011 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of SurgeryPublished by John Wiley & Sons Ltd

C. Ratto, A. Parello, L. Donisi, F. Litta, G. Zaccone and G. B. Doglietto
to well established technical guidelines, the intended loca-tion of the staple line is too difficult to standardize, asdemonstrated by the wide range of anatomicopathologi-cal results reported by Ohana and co-workers19. Based onthese data and the present findings, only a suture locatedwithin the distal 2 cm of the low rectum plays a role inthe control of arterial overflow in patients treated withSH. However, even if SH and Doppler-guided ligation ofhaemorrhoidal arteries were applied, some doubts aboutLongo’s procedure remain with respect to the circum-ferential suture performed with the specifically designedstapling device. This type of suture cannot ensure selectiveligation of haemorrhoidal arteries as it can also involveboth major and minor arterial vessels. Moreover, the cir-cumferential suture could generate an unpredictable riskof venous outflow blockage, thus damaging the drainagesystem, as described previously13.
The correlation between SH and rectal vasculariza-tion was highlighted in another study in which a perinealDoppler probe was used in patients who underwent SH forHD and a group of healthy subjects20. Baseline measure-ments differed significantly between patient and controlgroups. Postoperative follow-up showed no significantalterations in physiological parameters. Patients with ahigher rate of recurrence of HD had higher baseline arte-rial flow velocity values. The study showed that SH did notreduce arterial inflow in the vessels feeding the anorectalvascular plexus. The present data may explain the reasonsfor the failure to reduce vascular overflow. In that study20,the anastomosis was performed 3·5–4 cm above the den-tate line, a level at which most terminal arterial branchesare not in the submucosa. Indeed, a meta-analysis of large-scale studies of patients undergoing SH demonstrated thatthese patients are more likely to develop recurrent HDwith prolapse and bleeding at any time than those havingconventional haemorrhoidectomy21,22.
The goal of THD and DG-HAL is significantly toreduce arterial overflow to haemorrhoidal piles by dearte-rialization, that is Doppler-guided ligation of the haemor-rhoidal arteries in the upper part of the low rectum. Theresults of these operations seem promising23–31. In par-ticular, most studies have shown that recurrent bleedingis limited to a minority of patients (5–20 per cent afterTHD; 1–21 per cent after DG-HAL)23–31.
However, traditional dearterialization might fail toinclude the haemorrhoidal arteries in some sites owingto their deep location (within the muscularis propria orin perirectal fat), particularly on the anterior side of therectum. The reported frequency of recurrent bleeding inpatients undergoing dearterialization alone using the ‘higharterial ligation’ technique (31 per cent)26 supports this
view. When mucopexy is included in THD or DG-HALprocedures, the possibility of excluding arteries may belower as the running suture (even one that begins in theupper part of the low rectum to perform high ligation ofhaemorrhoidal arteries) is usually continued by transfix-ing the mucosa and submucosa to the ARJ, thus involvingarterial branches directed to the haemorrhoidal piles.
By selectively ligating the haemorrhoidal arteries usinga very precise Doppler system26, the THD technique canaccurately identify the location of arterial vessels in thesubmucosa of the low rectum, thus achieving a significantreduction in arterial overflow to haemorrhoids. Based onthe present findings, dearterialization should be more effec-tive if performed 1 and 2 cm from the ARJ, where almostall of the arteries are localized in the submucosa, with amean depth of 1·9–2·4 mm. In contrast, arterial ligation3 cm from the ARJ may not be effective in certain sectors.At this level, 67·1 per cent of the vessels identified werelocated in the submucosa. Above this level, a smaller per-centage of submucosal arteries was found, possibly makingdearterialization less accurate at higher levels.
This study provides new insight into the functionalanatomy of haemorrhoids, with a direct impact on patho-physiology and treatment. The location of almost all thebranches of the SRA in the submucosa provides a clear tar-get for surgical treatments that recognize vascular overflowas a fundamental factor in the aetiology of HD. Opti-mizing dearterialization is essential for improving clinicaloutcome. In this regard, Doppler imaging plays a pivotalrole during the surgical procedure by providing preciseidentification, then guided ligation of arteries. Clinical tri-als are required to confirm the therapeutic implications ofthese findings.
Acknowledgements
The authors declare no conflict of interest.
References
1 Lucha PA. Pathophysiology of hemorroidal disease. InSurgical Treatment of Hemorrhoids, Khubchandani I,Paonessa N, Azimuddin K (eds). Springer: London, 2009;15–17.
2 Loder PB, Kamm MA, Nicholls RJ, Philips RK.Haemorrhoids: pathology, pathophysiology and aetiology. BrJ Surg 1994; 81: 946–954.
3 Thomson WH. The anatomy and nature of piles. In TheHaemorrhoid Syndrome, Kaufman HD (ed.). Abacus Press:Tunbridge Wells, 1981; 15–33.
4 Shafik A. Surgical anatomy of hemorrhoids. In SurgicalTreatment of Hemorrhoids, Khubchandani I, Paonessa N,Azimuddin K (eds). Springer: London, 2009; 7–13.
2011 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of SurgeryPublished by John Wiley & Sons Ltd

Topography of haemorrhoidal arteries
5 Giordano P, Overton J, Madeddu F, Zaman S, Gravante G.Transanal hemorrhoidal dearterialization: a systematicreview. Dis Colon Rectum 2009; 52: 1665–1671.
6 Sultan S, Rabahi N, Etienney I, Atienza P. Stapledhaemorrhoidopexy: 6 years’ experience of a referral centre.Colorectal Dis 2010; 12: 921–926.
7 Shafik A. The pathogenesis of hemorrhoids and theirtreatment by anorectal bandotomy. J Clin Gastroenterol 1984;6: 129–137.
8 Klink C, Binnebosel M, Kammer D, Willis S, Prescher A,Klinge U et al. Haemorrhoids are related to changes of cellfunction in mucosa and submucosa. Int J Colorectal Dis 2009;24: 1389–1394.
9 Taweevisit M, Wisadeopas N, Phumsuk U, Thorner PS.Increased mast cell density in haemorrhoid venous bloodvessels suggests a role in pathogenesis. Singapore Med J 2008;49: 977–979.
10 Vyslouzil K, Zboril P, Skalicky P, Vomackova K. Effect ofhemorrhoidectomy on anorectal physiology. Int J ColorectalDis 2010; 25: 259–265.
11 Stelzner F, Staubesand J, Machleidt H. [The corpus caver-nosum recti – basis of internal hemorrhoids.] LangenbecksArch Klin Chir Ver Dtsch Z Chir 1962; 299: 302–312.
12 Aigner F, Bodner G, Gruber H, Conrad F, Fritsch H,Margreiter R et al. The vascular nature of hemorrhoids.J Gastrointest Surg 2006; 10: 1044–1050.
13 Aigner F, Gruber H, Conrad F, Eder J, Wedel T, Zelger Bet al. Revised morphology and hemodynamics of theanorectal vascular plexus: impact on the course ofhemorrhoidal disease. Int J Colorectal Dis 2009; 24: 105–113.
14 Schuurman JP, Go PM, Bleys RL. Anatomical branches ofthe superior rectal artery in the distal rectum. Colorectal Dis2009; 11: 967–971.
15 Shafik A, Mostafa H. Study of the arterial pattern of therectum and its clinical application. Acta Anat (Basel) 1996;157: 80–86.
16 DiDio LJ, Diaz-Franco C, Schemainda R, Bezerra AJ.Morphology of the middle rectal arteries. A study of30 cadaveric dissections. Surg Radiol Anat 1986; 8:229–236.
17 Aigner F, Bodner G, Conrad F, Mbaka G, Kreczy A, FritschH. The superior rectal artery and its branching pattern withregard to its clinical influence on ligation techniques forinternal hemorrhoids. Am J Surg 2004; 187: 102–108.
18 Corman ML, Gravie JF, Hager T, Loudon MA, Mascagni D,Nystrom PO et al. Stapled haemorrhoidopexy: a consensusposition paper by an international workingparty – indications, contra-indications and technique.Colorectal Dis 2003; 5: 304–310.
19 Ohana G, Myslovaty B, Ariche A, Dreznik Z, Koren R,Rath-Wolfson L. Mid-term results of stapled
hemorrhoidopexy for third- and fourth-degreehemorrhoids – correlation with the histological features ofthe resected tissue. World J Surg 2007; 31: 1336–1342.
20 Aigner F, Bonatti H, Peer S, Conrad F, Fritsch H,Margreiter R et al. Vascular considerations for stapledhaemorrhoidopexy. Colorectal Dis 2010; 12: 452–458.
21 Jayaraman S, Colquhoun PH, Malthaner RA. Stapled versusconventional surgery for hemorrhoids. Cochrane Database SystRev 2006; (4)CD005393.
22 Shao WJ. Systematic review and meta-analysis of randomizedcontrolled trials comparing stapled haemorrhoidopexy withconventional haemorrhoidectomy. Br J Surg 2008; 95:147–160.
23 Cantero R, Balibrea JM, Ferrigni C, Sanz M, GarcıaPerez JC, Perez R et al. [Doppler-guided transanalhaemorrhoidal dearterialisation. An alternative treatment forhaemorrhoids.] Cir Esp 2008; 83: 252–255.
24 Infantino A, Bellomo R, Dal Monte PP, Salafia C,Tagariello C, Tonizzo CA et al. Transanal haemorrhoidalartery echodoppler ligation and anopexy (THD) is effectivefor II and III degree haemorrhoids: a prospectivemulticentric study. Colorectal Dis 2010; 12: 804–809.
25 Festen S, van Hoogstraten MJ, van Geloven AA,Gerhards MF. Treatment of grade III and IV haemorrhoidaldisease with PPH or THD. A randomized trial onpostoperative complications and short-term results. Int JColorectal Dis. 2009; 24: 1401–1405.
26 Ratto C, Donisi L, Parello A, Litta F, Doglietto GB.Evaluation of transanal hemorrhoidal dearterialization as aminimally invasive therapeutic approach to hemorrhoids. DisColon Rectum 2010; 53: 803–811.
27 Arnold S, Antonietti E, Rollinger G, Scheyer M. [Dopplerultrasound assisted hemorrhoid artery ligation. A new therapyin symptomatic hemorrhoids.] Chirurg 2002; 73: 269–273.
28 Scheyer M, Antonietti E, Rollinger G, Mall H, Arnold S.Doppler-guided hemorrhoidal artery ligation. Am J Surg2006; 191: 89–93.
29 Greenberg R, Karin E, Avital S, Skornick Y, Werbin N. First100 cases with Doppler-guided hemorrhoidal artery ligation.Dis Colon Rectum 2006; 49: 485–489.
30 Wallis de Vries BM, van der Beek ES, de Wijkerslooth LR,van der Zwet WC, van der Hoeven JA, EeftinckSchattenkerk M et al. Treatment of grade 2 and 3hemorrhoids with Doppler-guided hemorrhoidal arteryligation. Dig Surg 2007; 24: 436–440.
31 Wałega P, Scheyer M, Kenig J, Herman RM, Arnold S,Nowak M et al. Two-center experience in the treatment ofhemorrhoidal disease using Doppler-guided hemorrhoidalartery ligation: functional results after 1-year follow-up. SurgEndosc 2008; 22: 2379–2383.
2011 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of SurgeryPublished by John Wiley & Sons Ltd





























![Review Article ApproachtoRectalCancerSurgeryproposed for local excision either via transanal excision or transanal endoscopic microsurgery (TEMS) [4–6]. While some report good outcomes](https://img.pdfslide.net/doc/110x75/60f7e35d60455642d5494efa/review-article-approachtorectalcancersurgery-proposed-for-local-excision-either.jpg)