Embed Size (px)
Citation preview
Service Evaluation of Bluebell Nurses’ Mums’ Comfort Zone & Bluebell Buddy Services
“ knowing I wasn’t the only person who sometimes couldn’t cope “
Providing Support for Young Mums and Families in South Bristol Affected by Depression in Relation to Pregnancy and Birth.
Written By Anna Mathieson, Ruth Jackson, Sally Cottrell and Rachel JenkinsBluebell Nurses registered charity No. 1136818 Ltd Company no. 7101628. registered address VealeWasbrough Vizards,
Orchard Court, Orchard Lane, Bristol, BS15WS. Address for correspondence Tall Pines, 26a Henbury Road, Bristol, BS9 3HJ.
www.bluebellnurses.org
Contents Page
TITLE PAGE Page 1
EXECUTIVE SUMMARY Page 3
INTRODUCTION Page 5
Aims and Objectives of the evaluation Page 6
BACKGROUND INFORMATION Page 7
Rationale for the evaluation Page 8
Costing Page 9
The evaluation Page 9
Programme Page 11
EVALUATION Page 12
Evaluation Methods Page 13
Evaluation Findings Page 14
1. Satisfaction with group Page 14
2. Improvements in health and wellbeing Page 15
3. Most useful part of the group Page 16
Knowledge café table cloths Page 17
Overall evaluation of the group programme Page 18
Activity implementation at home Page 20
Longer term follow up Page 21
DISCUSSION Page 22
Satisfaction with group Page 23
Improvements in health and wellbeing Page 23
Most useful part of the group Page 23
Knowledge café table cloths Page 24
Overall evaluation of the group programme Page 24
Activity implementation at home Page 24
Longer term follow up Page 24
Limitations Page 25
Final conclusions Page 25
Recommendations for practice Page 26
ACKNOWLEDGEMENTS Page 28
REFERENCES Page 29
APPENDICES Page 30
Appendix A- Information about the charity Page 30
Appendix B- Statements of income and expenditure Page 33
Appendix C- Referral form Page 34
Appendix D- Questionnaires: EPDS and GAD7 Page 36
Appendix E- Session evaluation form Page 39
Appendix F- Support group evaluation form Page 40
2
Executive Summary
“ I found ways to copeand ways to help me calm down “
4
The aim of this evaluation report was to ascertain whether the overall aim of
Bluebell Nurses (henceforth referred to as Bluebell) of reducing levels of anxiety
and depression in young mothers was achieved in the charity’s pilot year, through
the use of the Mums’ Comfort Zone group programme. The main objective was
to investigate whether the structure and content of the group programme was
effective and beneficial to the group attendees.
In order to achieve the aims and objectives, mothers were asked to complete
various questionnaires to feed back upon the group, as well as completing anxiety
and depression questionnaires at the start and at the completion of the group.
An alternative method of feedback
was also provided during a ‘knowledge
café’ session, where the mothers
were asked to draw or write on table
cloths to express how they had been
feeling at the start of the programme,
and compare that to how they were
now feeling upon completing the
programme.
The results found that the service
succeeded in achieving its main aim
of reducing the levels of anxiety and
depression in the young mothers
after attending the group programme
either alone or in combination with the Buddy support service also
provided by Bluebell. Mothers reported that attending the group was a positive
experience for them, mainly due to meeting others in a similar situation and
sharing their experiences. A comparison of their emotional expression at the
beginning and at the end of the group indicates that the programme provided the
mothers with techniques for managing their perinatal mental health, their day to
day routine and ways to reduce their social isolation.
In the future, Bluebell services will be extended to support partners of those
who have experienced perinatal mental health issues. The charity also plans to
replicate the Mums' Comfort Zone group programme and Buddy service in other
locations within Bristol to reach mothers from more diverse ethnic and socio-
economic groups and to make the services available for all ages of parents, not
just young mums.
An alternative method of feedback
was also provided during a ‘knowledge
café’ session, where the mothers
were asked to draw or write on table
cloths to express how they had been
feeling at the start of the programme,
and compare that to how they were
after attending the group programme
Introduction
“ You’re not alone “
6
The evaluation aimed to establish whether the group programme
offered by Bluebell was effective in reducing the levels of anxiety
and depression in young mothers.
The objectives were:
a) Does attendance at the group programme reduce
anxiety in young mothers?
b) Does attendance at the group programme reduce
depression in young mothers?
c) Are there any changes that need to be made to the
structure of the group?
Bluebell is a registered charity providing support to young mothers who have
experienced or are experiencing perinatal depression and anxiety in Bristol. Under
evaluation in this report are the group programmes provided by Bluebell from
September 2011 to September 2012. These included the buddy service (Bluebell
Buddy) that provides one to one sessions, a text service and telephone support.
The main programme involved group education and support, and sessions ran
over 12 weeks entitled ‘Mums’ Comfort Zone’. These groups took up to ten mothers
in a 12-week programme providing a free crèche and ran according to a structured
schedule throughout the year, with a lighter drop-in programme over the summer
period of July and August 2012.
The initial year of this project has been funded by Pfizer UK Foundation (an initiative
of Pfizer Limited) from September 2011 to September 2012 and the charity has
been successful in securing further funding of £65,000 from Comic Relief’s young
persons’ mental health fund to continue this work for a further three years.
Aims and objectives of the evaluation
Background Information
“ I don’t think there is anything to change because from my point of view you have helped me so much and I am so thankful “
Rationale for the evaluation
In 2010, there were 32,552 conceptions in those aged under 18 years old in England
(Annual Conception Statistics, 2010). It has been found that teenage mothers have
three times the rate of post-natal depression of older mothers and a higher risk
of poor mental health for three years after the birth (‘Teenage Pregnancy Strategy:
Beyond 2010’, Department of Health). Evidently these service users have an
increased need for support, not only in the short term but also in the years after
giving birth.
According to the National Institute for Clinical Excellence (NICE) guidelines for
Antenatal and Postnatal Mental Health (2007), at the point of first contact in
either the antenatal or postnatal period, mothers should be asked questions by
health professionals in order to detect whether they may be at risk of depression,
anxiety or other mental health issues related to their pregnancy. These include
questions about their past mental health, and whether there is any family history
of perinatal mental health issues.
The NICE guidelines also state that before any treatment commences, the risks
and benefits of psychological treatment should be explained to the mother.
However, the guidelines also have a medical focus, with the main treatment
offered being anti-depressant medication. This is not always desirable for
mothers, particularly those who are currently pregnant or breast feeding. Self-help
strategies, counselling and psychotherapy are suggested for mothers with mild
to moderate depression during pregnancy or the postnatal period. Alternative
treatments and support should be offered to those mothers who do not fit such
criteria, or do not wish to receive such treatments. Therefore services such as
Bluebell are vital in providing support and filling a gap in current services.
The NICE guidelines also state that "providing information about the nature,
course and treatment of a mental disorder during pregnancy and the postnatal
period facilitates access to services, and improves understanding and
collaboration between the woman, her partner, family members, carers and
healthcare professionals" (page 10, section 1.1.1). This is an area where Bluebell
can fill a gap in service provision, by educating mothers (and therefore indirectly
their partners) about depression and other mental health issues, and by bringing
together those who have had similar experiences, who can share and learn from
each other’s experiences.
Further information about the charity is provided in Appendix A.
8
CostingThe group has been estimated to cost £10 per week to support one young mother
and to care for her baby in the crèche with the Buddy service costing £100 per week
to support 10 young mums, so also £10 per mother. This means that for £20 per
week a young mum can access the buddy service, the therapeutic group and place
her child in a crèche for 3 hours. The Government published a figure of £300 per
month cost to care for a mother affected by post-natal depression making Bluebell
services significantly more cost-effective. Statements of income and expenditure
are included in Appendix B. The economic cost of treating post-natal depression
has been estimated to be between £35 million and £45 million (Petrou et al, 2002).
This figure includes the cost of the increased contact time with health and social
care professionals. However it does not include the economic costs to society of a
mother’s reduced ability to return to work or to work at full capacity.
The cost of training health visitors in post natal depression detection and
intervention has been estimated at £1400 per health visitor (Petrou et al, 2006).
The evaluationUnder evaluation was the 12 week group programme, ‘Mum’s Comfort Zone’ and the
Bluebell Buddy service. The Buddy service was run by a member of Bluebell staff
who was herself a young mother who experienced perinatal mental health problems,
and has since overcome these problems. One to one sessions, telephone and text
support were all offered by the buddy. This part of the service was open to all group
attendees, but it was left up to them to decide whether they accessed the service
or not. The buddy attended each week of the programme, but was also available
to support those who did not attend the programme. The Buddy service was also
offered to those for whom a group was not appropriate or who felt unable to leave
the house due to their depression. The Buddy service and the group work together as
a whole intervention, with most of the mothers’ preferring to use a combination of
both. Therefore the evaluation results captured relate to both services.
The first 12 week group programme was launched in September 2011 and consisted
of a structured schedule which involved information giving, strategies for
managing anxiety and depression and a varied programme of group activities, all
aimed at reducing anxiety and depression. There were also home activities for the
attendees to complete outside of the group.
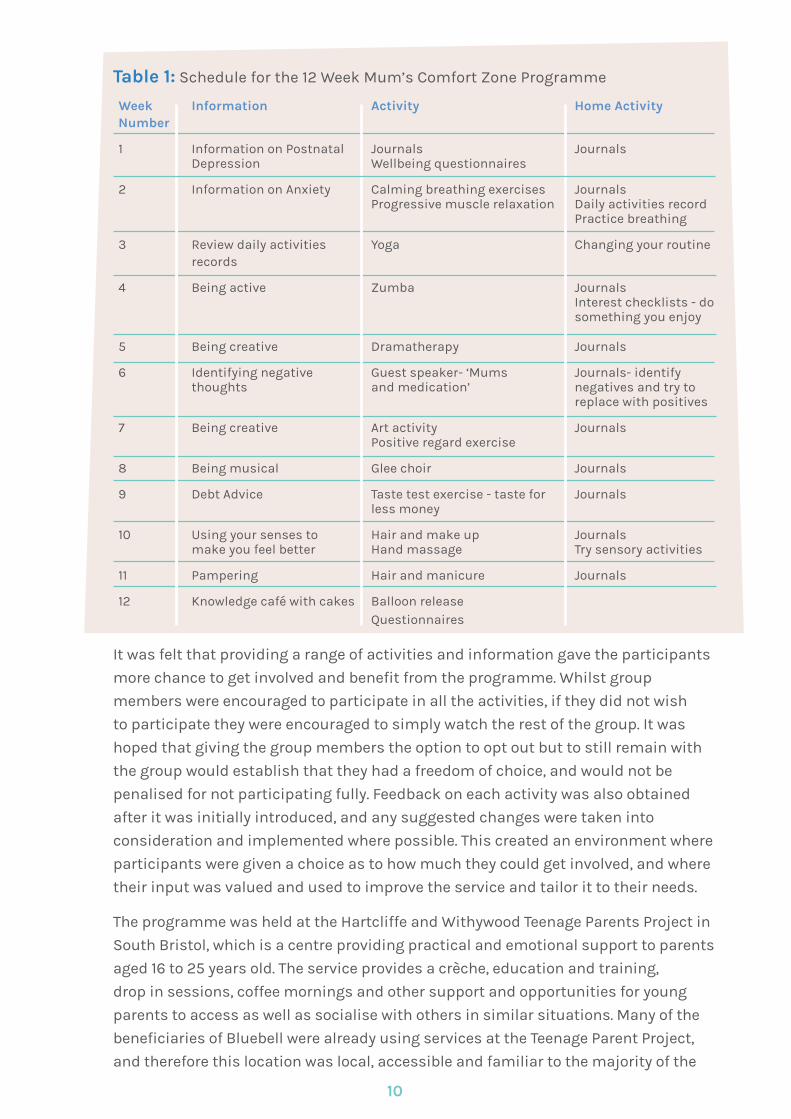
Table 1 below shows the programme schedule. The schedule was flexible and up for
discussion each week with the group members. The course could accommodate
up to ten mothers, all of whom had a diagnosis of post-natal or antenatal
depression from a registered health professional. The group was led by an
Occupational Therapist with the Buddy worker acting as the co-facilitator and all
Bluebell workers received professional clinical supervision.
9
It was felt that providing a range of activities and information gave the participants
more chance to get involved and benefit from the programme. Whilst group
members were encouraged to participate in all the activities, if they did not wish
to participate they were encouraged to simply watch the rest of the group. It was
hoped that giving the group members the option to opt out but to still remain with
the group would establish that they had a freedom of choice, and would not be
penalised for not participating fully. Feedback on each activity was also obtained
after it was initially introduced, and any suggested changes were taken into
consideration and implemented where possible. This created an environment where
participants were given a choice as to how much they could get involved, and where
their input was valued and used to improve the service and tailor it to their needs.
The programme was held at the Hartcliffe and Withywood Teenage Parents Project in
South Bristol, which is a centre providing practical and emotional support to parents
aged 16 to 25 years old. The service provides a crèche, education and training,
drop in sessions, coffee mornings and other support and opportunities for young
parents to access as well as socialise with others in similar situations. Many of the
beneficiaries of Bluebell were already using services at the Teenage Parent Project,
and therefore this location was local, accessible and familiar to the majority of the
Table 1: Schedule for the 12 Week Mum’s Comfort Zone Programme
Week Information Activity Home Activity Number
1 Information on Postnatal Journals Journals Depression Wellbeing questionnaires
2 Information on Anxiety Calming breathing exercises Journals Progressive muscle relaxation Daily activities record Practice breathing
3 Review daily activities Yoga Changing your routine records
4 Being active Zumba Journals Interest checklists - do something you enjoy
5 Being creative Dramatherapy Journals
6 Identifying negative Guest speaker- ‘Mums Journals- identify thoughts and medication’ negatives and try to replace with positives
7 Being creative Art activity Journals Positive regard exercise
8 Being musical Glee choir Journals
9 Debt Advice Taste test exercise - taste for Journals less money
10 Using your senses to Hair and make up Journals make you feel better Hand massage Try sensory activities
11 Pampering Hair and manicure Journals
12 Knowledge café with cakes Balloon release Questionnaires
10
service users. This location was conducive to creating an atmosphere of familiarity,
trust and relaxation. The Buddy service is also provided in this same area of Bristol,
however it is not restricted to a centre and can provide support to any young mother
affected by perinatal depression in the South Bristol area.
The programme draws on elements on a Cognitive Behaviour Therapy approach
(CBT) which Rachel Jenkins, the Occupational Therapist and group leader, has
developed to focus more on behaviour rather than cognitive aspects. This is due to
the fact that the young mothers have difficulty comprehending these aspects due
to low literacy levels. This approach facilitates service user involvement, which is
the foundation of Bluebell. For example, the mothers were involved in a session on
designing the marketing tools for the charity. They were also involved in creating the
name of the course, and the colours and language used on the marketing materials.
Programme background (section written by Rachel Jenkins)
"As an occupational therapist I am interested in the use of meaningful activity
(occupation) in order to promote the health and wellbeing of individuals. The Model
of Human Occupation (Kielhofner, 2008) is a dynamic framework which explains
how the process of doing helps us organise our mind and body, which in turn helps
us organise our occupations. Components such as our values and interests as well
as our motivation, habits, roles and environment can all influence our ability to
carry out meaningful activities.
When an individual has post-natal depression (PND) there is often an imbalance of
occupations within their lives e.g. too little sleep, not enough leisure time. There is
often a loss of meaningful roles (e.g. a working mum not being able to go to work)
and old habits and routines are abandoned during the chaos of new motherhood.
As an occupational therapist I assess the areas of concern and support the
individual to re-motivate themselves and rebalance their occupations (personal
care, work, leisure) thus improving their health and wellbeing.
The 12 week programme for Mums’ Comfort Zone utilizes cognitive behavioural
therapy and occupational therapy principles in order help with the recovery
process. Whereas the cognitive elements work on changing the negative thought
processes often found in individuals with PND the behavioural changes are
promoted by exploring the use of meaningful activities (occupation). There has
been little research into the effect of occupation on PND but there is a wealth
of evidence to support the use of creative activity (music, art, dance, drama)
and aerobic exercise for depression. This research also demonstrates that
meaningful activity is made all the more meaningful when it is done within a
supportive social environment. Mums’ Comfort Zone combines the bio-psycho-
social elements essential for restoring life balance by focusing on group
discussion, information giving and meaningful activity".
11
Evaluation
“ The support given wasamazing “
Evaluation Methods
An internal evaluation was conducted in accordance with the requirements of
the funding organisations. The aim of the evaluation was to ascertain whether
the charity was achieving its aims of reducing anxiety and depression in young
mothers through providing them with new tools and strategies for managing
their mental health, reducing isolation and increasing their ability to ask for help.
Therefore the main question that needed to be answered was whether the anxiety
and depression levels of the young mothers reduced as a result of attending the
group programme.
In order to do this, participants were asked to complete session questionnaires
to rate their feelings before and after the group session each week. Participants
also answered support group evaluation questionnaires at the end of the 12 week
group programme, to discuss and evaluate the programme overall. Participants
completed the Generalised Anxiety Disorder 7 (GAD 7) questionnaire and the
Edinburgh Post Natal Depression Scale (EPDS) before and after the 12 week course.
At the end of the programme, participants attended a session called a ‘knowledge
café’ where they had the opportunity to visually demonstrate their thoughts and
feelings in relation to the programme by drawing and writing on paper table
cloths. This was run in accordance with the guidelines from ‘The World Café
presents Café to go’ (2008).
Data analysis was conducted by an
independent research assistant, in
conjunction with colleagues at the University
of West England who have expertise in service
evaluation design.
As this project was an internal service
evaluation, it was decided that a formal
research ethics application was not needed.
Informed consent was sought from all
participants, and participants were aware
that their feedback data and reflections would be used for the purposes
of evaluating the service. All data protection guidelines were adhered to.
13
Evaluation Findings
Forty four mothers attended the group sessions over the year, with approximately ten
mothers dropping out completely from the group programmes throughout the year.
Thirty six mothers in total were also seen by the buddy service. The charity set a target
of providing the services to 50 mothers over the course of the first year, and therefore
this target was exceeded.
1. Satisfaction with the group
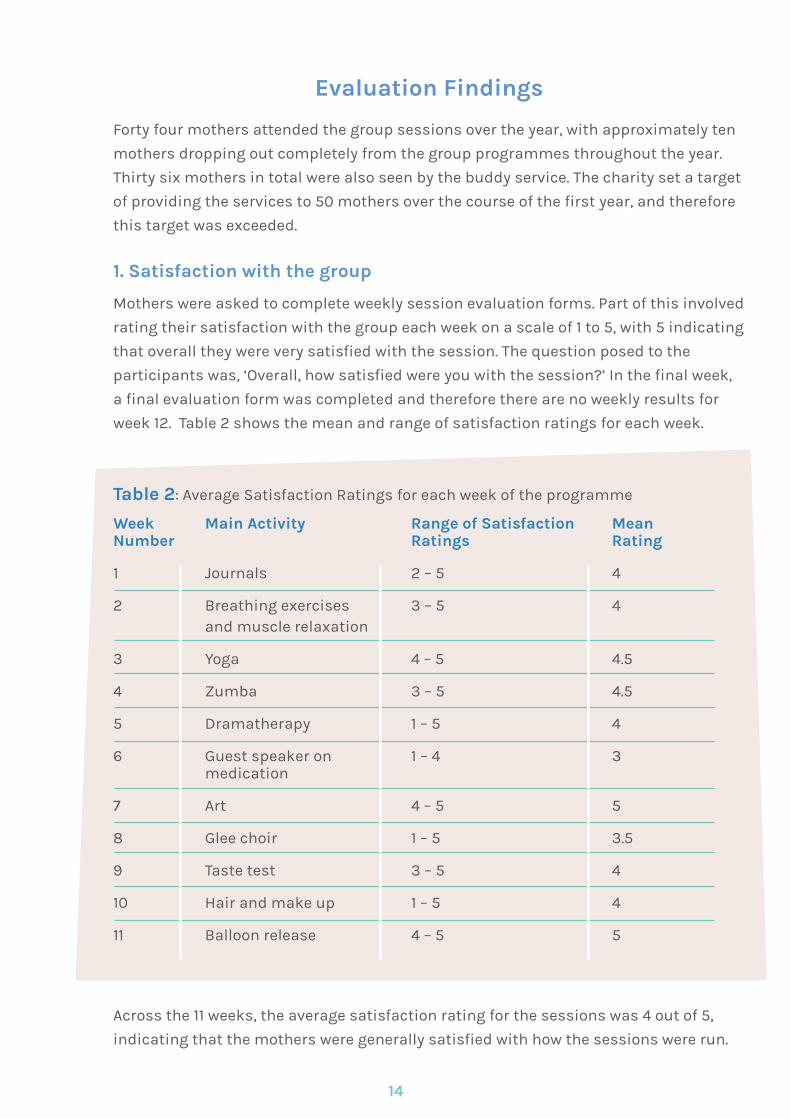
Mothers were asked to complete weekly session evaluation forms. Part of this involved
rating their satisfaction with the group each week on a scale of 1 to 5, with 5 indicating
that overall they were very satisfied with the session. The question posed to the
participants was, ‘Overall, how satisfied were you with the session?’ In the final week,
a final evaluation form was completed and therefore there are no weekly results for
week 12. Table 2 shows the mean and range of satisfaction ratings for each week.
Table 2: Average Satisfaction Ratings for each week of the programme
Week Main Activity Range of Satisfaction MeanNumber Ratings Rating
1 Journals 2 – 5 4
2 Breathing exercises 3 – 5 4 and muscle relaxation
3 Yoga 4 – 5 4.5
4 Zumba 3 – 5 4.5
5 Dramatherapy 1 – 5 4
6 Guest speaker on 1 – 4 3 medication
7 Art 4 – 5 5
8 Glee choir 1 – 5 3.5
9 Taste test 3 – 5 4
10 Hair and make up 1 – 5 4
11 Balloon release 4 – 5 5
Across the 11 weeks, the average satisfaction rating for the sessions was 4 out of 5,
indicating that the mothers were generally satisfied with how the sessions were run.
14
Overall, the mothers felt that Bluebell’s services were valuable and were positive
about their involvement with the services. For example, in their qualitative
answers, mothers stated, "I found ways to cope and ways to help me calm down"; It was
great because I would be stuck at home doing nothing; "The support given was amazing".
Group attendees were also positive about the way that the group was run, and
how topics were communicated: "They were very welcoming" and "are great to talk to";
"Everyone had a chance to say something".
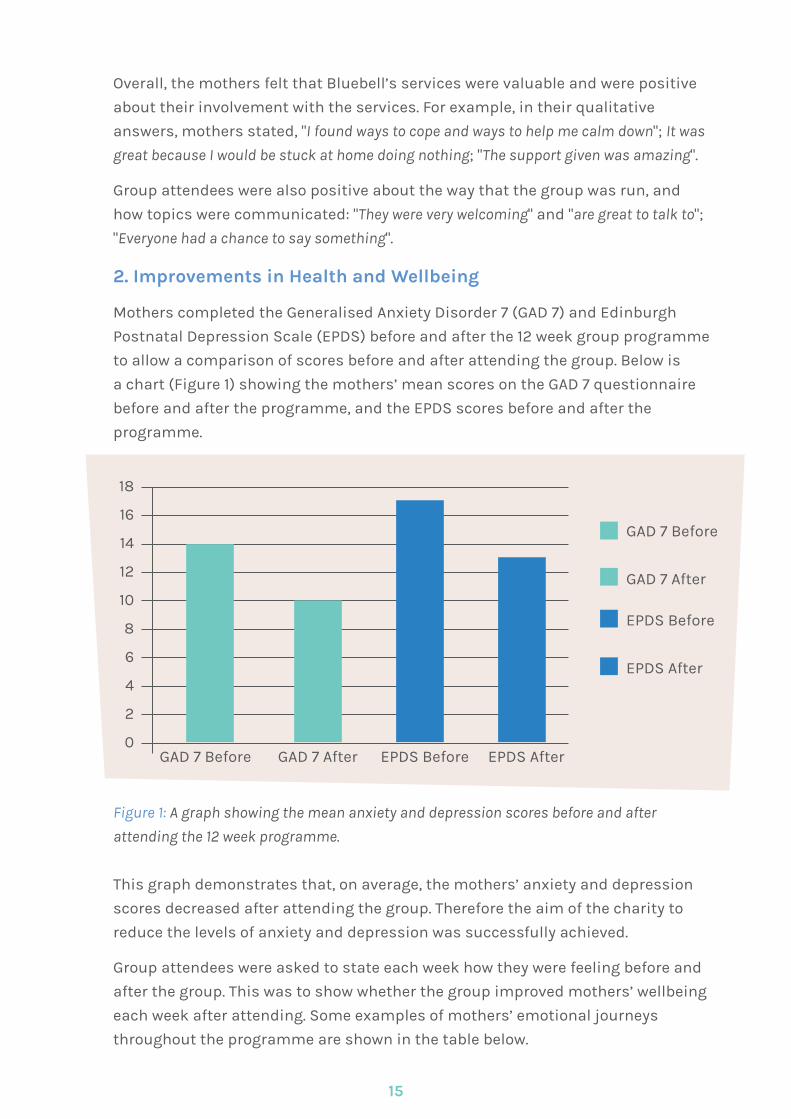
2. Improvements in Health and Wellbeing
Mothers completed the Generalised Anxiety Disorder 7 (GAD 7) and Edinburgh
Postnatal Depression Scale (EPDS) before and after the 12 week group programme
to allow a comparison of scores before and after attending the group. Below is
a chart (Figure 1) showing the mothers’ mean scores on the GAD 7 questionnaire
before and after the programme, and the EPDS scores before and after the
programme.
Figure 1: A graph showing the mean anxiety and depression scores before and after
attending the 12 week programme.
This graph demonstrates that, on average, the mothers’ anxiety and depression
scores decreased after attending the group. Therefore the aim of the charity to
reduce the levels of anxiety and depression was successfully achieved.
Group attendees were asked to state each week how they were feeling before and
after the group. This was to show whether the group improved mothers’ wellbeing
each week after attending. Some examples of mothers’ emotional journeys
throughout the programme are shown in the table below.
18
16
14
12
10
8
6
4
2
0GAD 7 Before GAD 7 After EPDS Before EPDS After
GAD 7 Before
GAD 7 After
EPDS Before
EPDS After
15

3. Most useful part of the group.Mothers were asked to state each week what they had found most useful about
the group. The majority of responses indicated that the most useful part was
meeting others who were in a similar situation. Some quotes to illustrate this
are, "You’re not alone"; "Learning people close to you were going through the same things",
"Everyone sharing their problems and people listening to each other", and, "I thought it
was really good to do a group where you all have something in common". However, one
attendee felt that the usefulness of the group was short lived: "For the first couple of
weeks it has helped me but now I just feel even more stressed". This could be a reflection
of the nature of depression often resulting in the need for longer term support. In
this particular case, the young mother is still receiving support through the Buddy
service. The Buddy service is offered to all mothers after they complete their group
programme to provide continuing support and reduce feelings of abandonment.
Others felt that the advice giving side of the programme was most useful: "The
debt advice and pampering sessions"; "More relaxed. Know how to deal with my problems";
"Ways to calm myself down and putting my children in a routine helped millions and
16
Examples of Mothers’ Journeys through the Group Programme
Week Start FinishNumber
1 Unconfident Surprised Exhausted Happy
2 Sad Relaxed Anxious Happy
3 Angry Happy Upset Relaxed
4 Excited Happy Happy Laughing
5 Tired Laughing Upset Happy
6 Tired Happy Headache Headache
7 Exhausted Tired Tired
8 Happy Relaxed Excited
9 Tired Happy Bored Fun
10 Excited Happy Scared Anxious
11 Bored Impressed Tired Relaxed
knowing I wasn’t the only person who sometimes couldn’t cope"; "Learnt different
techniques when dealing with things".
Mothers were asked to give any suggestions for how the group could be run
differently. Some suggestions were as follows: "More group activities"; "I didn’t enjoy
the drama therapy", and "Last longer". However, most felt that there wasn’t any need
for changes, with one mother stating, "I don’t think there is anything to change because
from my point of view you have helped me so much and I am so thankful".
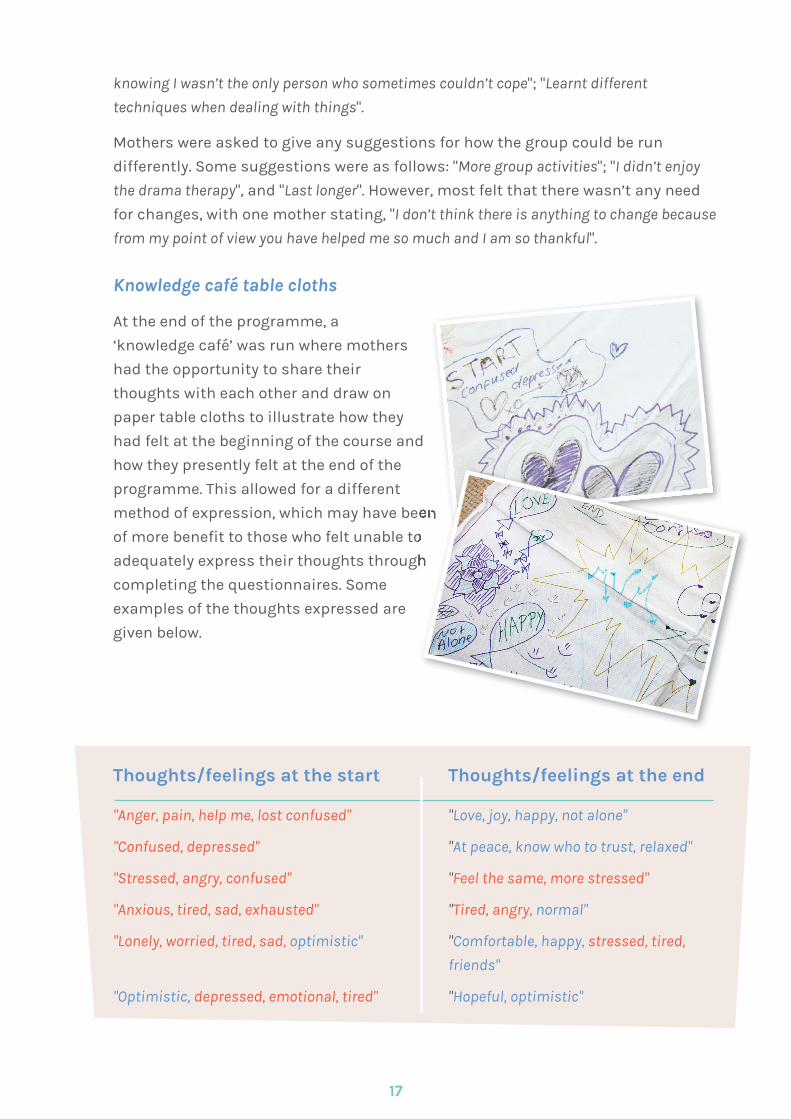
Knowledge café table cloths
At the end of the programme, a
‘knowledge café’ was run where mothers
had the opportunity to share their
thoughts with each other and draw on
paper table cloths to illustrate how they
had felt at the beginning of the course and
how they presently felt at the end of the
programme. This allowed for a different
method of expression, which may have been
of more benefit to those who felt unable to
adequately express their thoughts through
completing the questionnaires. Some
examples of the thoughts expressed are
given below.
Thoughts/feelings at the start Thoughts/feelings at the end
"Anger, pain, help me, lost confused" "Love, joy, happy, not alone"
"Confused, depressed" "At peace, know who to trust, relaxed"
"Stressed, angry, confused" "Feel the same, more stressed"
"Anxious, tired, sad, exhausted" "Tired, angry, normal"
"Lonely, worried, tired, sad, optimistic" "Comfortable, happy, stressed, tired,
friends"
"Optimistic, depressed, emotional, tired" "Hopeful, optimistic"
17
method of expression, which may have been
of more benefit to those who felt unable to
adequately express their thoughts through
method of expression, which may have been
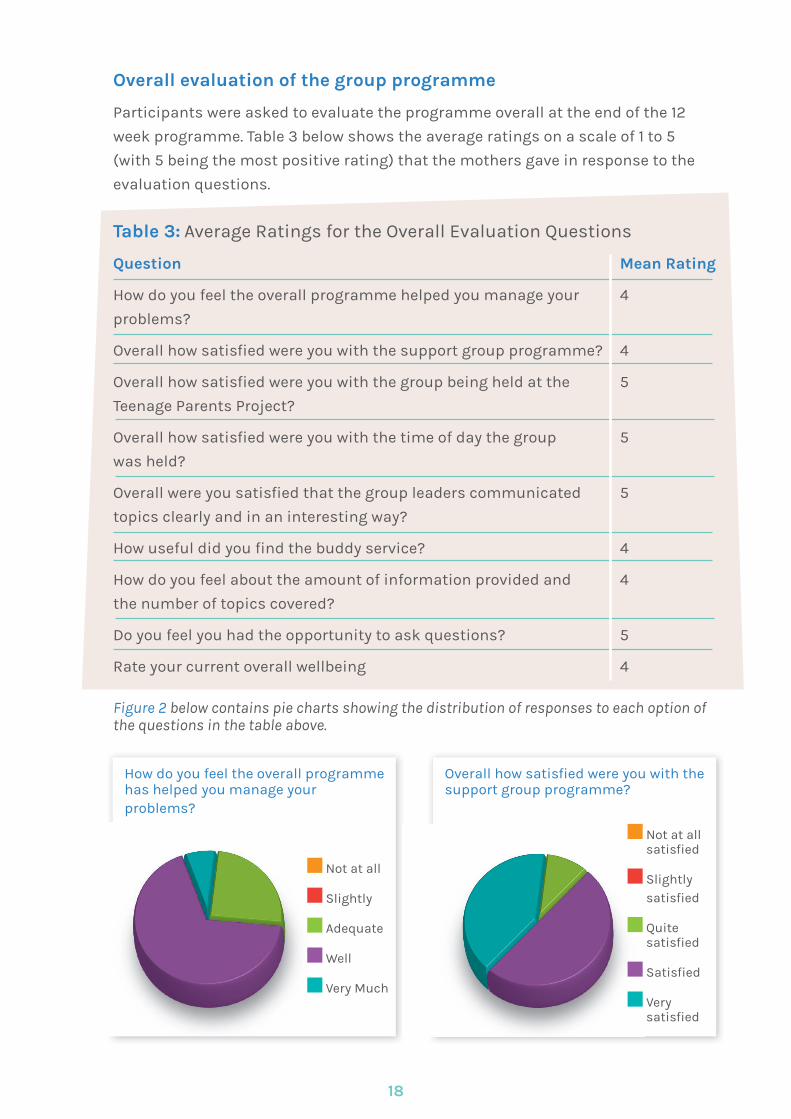
Overall evaluation of the group programme
Participants were asked to evaluate the programme overall at the end of the 12
week programme. Table 3 below shows the average ratings on a scale of 1 to 5
(with 5 being the most positive rating) that the mothers gave in response to the
evaluation questions.
Table 3: Average Ratings for the Overall Evaluation Questions
Question Mean Rating
How do you feel the overall programme helped you manage your 4
problems?
Overall how satisfied were you with the support group programme? 4
Overall how satisfied were you with the group being held at the 5
Teenage Parents Project?
Overall how satisfied were you with the time of day the group 5
was held?
Overall were you satisfied that the group leaders communicated 5
topics clearly and in an interesting way?
How useful did you find the buddy service? 4
How do you feel about the amount of information provided and 4
the number of topics covered?
Do you feel you had the opportunity to ask questions? 5
Rate your current overall wellbeing 4
Figure 2 below contains pie charts showing the distribution of responses to each option ofthe questions in the table above.
18
How do you feel the overall programme has helped you manage your problems?
Not at all
Slightly
Adequate
Well
Very Much
Overall how satisfied were you with thesupport group programme?
Not at all satisfied
Slightly satisfied
Quite satisfied
Satisfied
Very satisfied
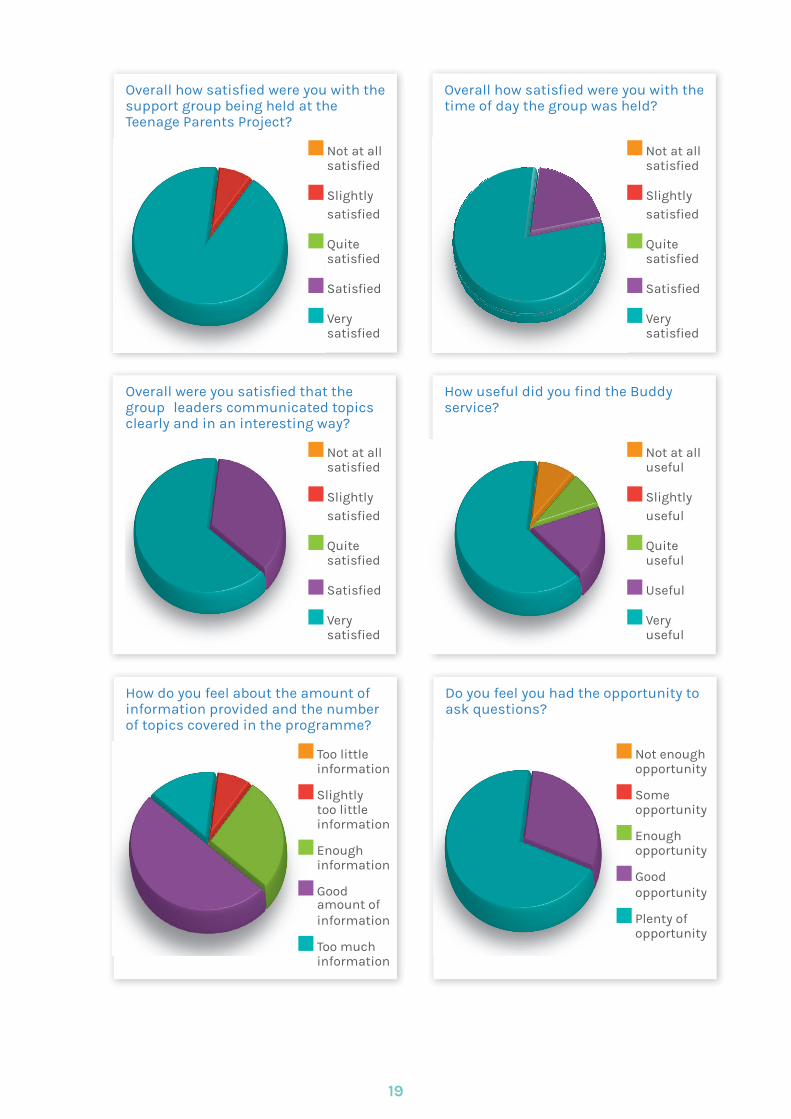
Overall how satisfied were you with thesupport group being held at the Teenage Parents Project?
Not at all satisfied
Slightly satisfied
Quite satisfied
Satisfied
Very satisfied
Overall how satisfied were you with thetime of day the group was held?
Not at all satisfied
Slightly satisfied
Quite satisfied
Satisfied
Very satisfied
Overall were you satisfied that the group leaders communicated topics clearly and in an interesting way?
Not at all satisfied
Slightly satisfied
Quite satisfied
Satisfied
Very satisfied
How useful did you find the Buddy service?
Not at all useful
Slightly useful
Quite useful
Useful
Very useful
How do you feel about the amount of information provided and the number of topics covered in the programme?
Too little information
Slightly too little information
Enough information
Good amount of information
Too much information
Do you feel you had the opportunity to ask questions?
Not enough opportunity
Some opportunity
Enough opportunity
Good opportunity
Plenty of opportunity
19
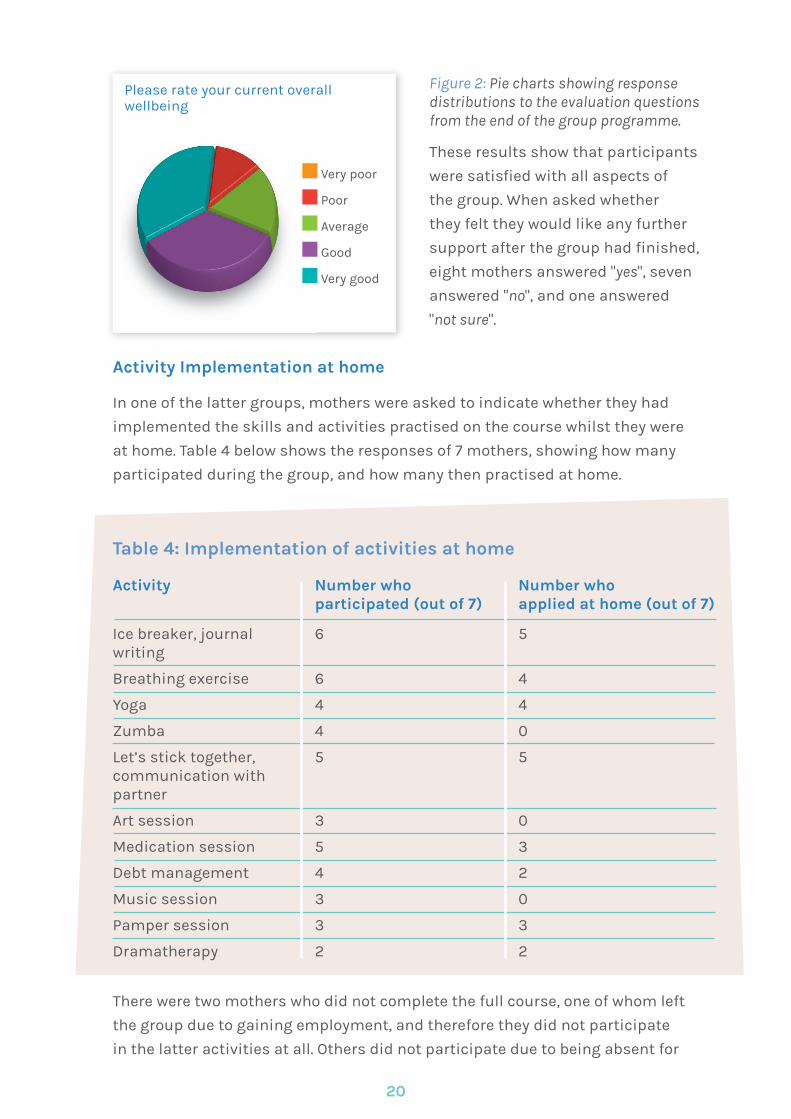
Figure 2: Pie charts showing response distributions to the evaluation questions from the end of the group programme.
These results show that participants
were satisfied with all aspects of
the group. When asked whether
they felt they would like any further
support after the group had finished,
eight mothers answered "yes", seven
answered "no", and one answered
"not sure".
Activity Implementation at home
In one of the latter groups, mothers were asked to indicate whether they had
implemented the skills and activities practised on the course whilst they were
at home. Table 4 below shows the responses of 7 mothers, showing how many
participated during the group, and how many then practised at home.
There were two mothers who did not complete the full course, one of whom left
the group due to gaining employment, and therefore they did not participate
in the latter activities at all. Others did not participate due to being absent for
Please rate your current overall wellbeing
Very poor
Poor
Average
Good
Very good
Table 4: Implementation of activities at home
Activity Number who Number who participated (out of 7) applied at home (out of 7)
Ice breaker, journal 6 5 writing
Breathing exercise 6 4
Yoga 4 4
Zumba 4 0
Let’s stick together, 5 5 communication with partner
Art session 3 0
Medication session 5 3
Debt management 4 2
Music session 3 0
Pamper session 3 3
Dramatherapy 2 2
20
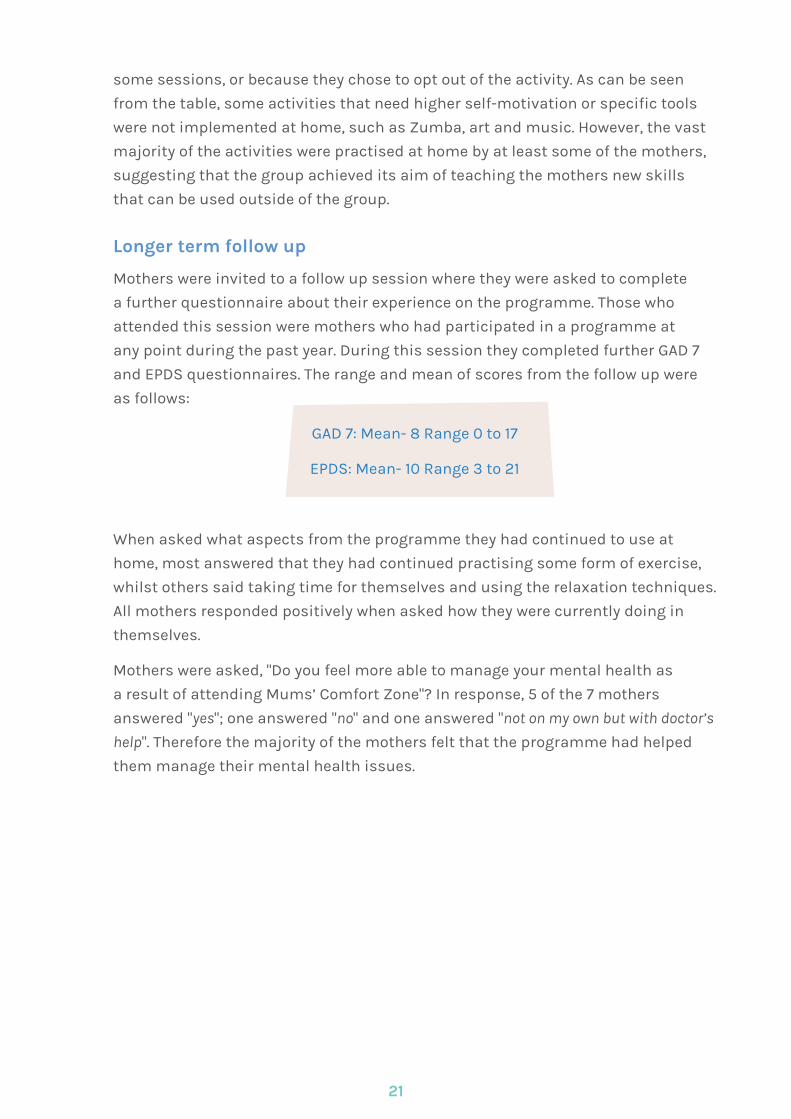
some sessions, or because they chose to opt out of the activity. As can be seen
from the table, some activities that need higher self-motivation or specific tools
were not implemented at home, such as Zumba, art and music. However, the vast
majority of the activities were practised at home by at least some of the mothers,
suggesting that the group achieved its aim of teaching the mothers new skills
that can be used outside of the group.
Longer term follow up
Mothers were invited to a follow up session where they were asked to complete
a further questionnaire about their experience on the programme. Those who
attended this session were mothers who had participated in a programme at
any point during the past year. During this session they completed further GAD 7
and EPDS questionnaires. The range and mean of scores from the follow up were
as follows:
GAD 7: Mean- 8 Range 0 to 17
EPDS: Mean- 10 Range 3 to 21
When asked what aspects from the programme they had continued to use at
home, most answered that they had continued practising some form of exercise,
whilst others said taking time for themselves and using the relaxation techniques.
All mothers responded positively when asked how they were currently doing in
themselves.
Mothers were asked, "Do you feel more able to manage your mental health as
a result of attending Mums’ Comfort Zone"? In response, 5 of the 7 mothers
answered "yes"; one answered "no" and one answered "not on my own but with doctor’s
help". Therefore the majority of the mothers felt that the programme had helped
them manage their mental health issues.
21
Discussion
“ They were very welcoming
and are great to talk to “
This evaluation set out to establish whether the services offered by Bluebell
were making a positive impact to the wellbeing of young mothers with perinatal
mental health issues. The results show that the service is making a valuable
contribution to the wellbeing of the young mothers, primarily because the average
depression and anxiety scores reduced as a result of attending the group. The
qualitative data results also illustrate that the mothers felt that attending the
group was a positive experience for them, and that meeting others in a similar
situation was particularly beneficial. Due to these results, the aims of the charity
as a whole were also achieved, as the mothers’ anxiety and depression levels were
reduced overall, and new strategies were learnt that the young mothers could then
implement at home when the group had ended.
Satisfaction with the group
In their weekly session evaluation forms, the mothers gave satisfaction ratings
for each week. Although the ratings varied, the vast majority of the mothers stated
that they were satisfied or very satisfied with the sessions. Across the whole
programme, the average rating that the mothers gave was 4 out of 5, indicating
that they were satisfied with the content of the sessions. Mothers also stated that
they felt that the group provided valuable support and that the topics covered
were communicated clearly. Therefore the service is working according to the NICE
guidelines through providing information and advice on mental health aspects of
perinatal health in a way that is accessible and valuable to the mothers involved.
Improvements in health and wellbeing
On average, the mothers’ anxiety and depression scores decreased by a similar
margin as a result of attending the group programme in comparison with their
scores at the start of the programme. Depression scores reduced by a larger margin
over the course of the group compared to anxiety scores. Therefore the main aim
of the charity has been achieved, as anxiety and depression levels were reduced
as a result of attending the group sessions. From the illustration of examples of
mothers’ journeys throughout the group, it can be seen that although the mothers
experienced high and lows throughout the group, in general attending the sessions
resulted in a positive wellbeing experience overall. This is a very encouraging
result for the charity after its first pilot year, as the standardised measurement
of the mothers’ mental health proved that the group did result in a significant
improvement in wellbeing.
Most useful part of the group
The overwhelming response to the question of which part of the group was most
useful was that it was meeting others in a similar situation and sharing their
experiences. The mothers also valued receiving information and advice from
reliable and trusted sources. This relates to the NICE guidelines in that providing
23
information and advice can improve mothers’ wellbeing and better equip them
with strategies for managing their mental health.
Group attendees were asked to make suggestions for ways to improve the
programme. Many stated that they did not have any suggestions of how to
improve the group. The suggestions that were given were that there should be
more group activities and that the sessions should last longer.
Knowledge café table cloths
The table cloths session at the knowledge café provided the mothers with an
alternative method of expressing themselves and feeding back about their
experiences. As can be seen from the results, the mothers indicated on the table
cloths that there was a significant improvement in their positive emotions and
wellbeing after attending the programme. The majority of the words used to
express their emotions at the start of the group had negative connotations, and
there is an obvious difference between these and the words that were used to
express their emotions at the end of the programme, which were mostly positive.
This is further evidence that the group programme had significant positive effects
on the wellbeing of the young mothers.
Overall evaluation of the group programme
In the final evaluation questionnaire, mothers were asked to reflect upon their
experiences of the programme across the whole 12 weeks. On average, the
mothers stated that they were either satisfied or very satisfied with every aspect
of the programme.
The results overall demonstrate that the structure and content of the programme
are satisfactory to the group attendees. Mothers benefitted from meeting others
in a similar situation to themselves and receiving information and advice from a
trusted and credible source.
Activity implementation at home
Mothers were able to implement the activities from the course at home, apart from
those that required specific tools i.e. art and music. This is very encouraging as it
indicates that the skills being taught and practised are being used by the mothers
outside of the course, and therefore the programme is succeeding in teaching new
long term skills. However, not everyone practised the new skills. This could be due to
lower motivation which may be a consequence of low mood. In the future it may be
beneficial to discuss with the mothers ways in which the programme leaders can
help them to implement the activities outside of the group.
Longer term follow up
At the follow up session, the mean scores on the GAD 7 and EPDS questionnaires
were lower than the mean scores on the questionnaires completed by the mothers
24
when they initially finished their programme. Whilst direct conclusions cannot be
drawn from this, it is possible that there is a beneficial long term effect of attending
the programme in relation to anxiety and depression scores lowering over time.
The vast majority of the mothers stated that attending the group had helped them
to manage their mental health. This is a very encouraging result as it shows that
the overall aim of the programme is being achieved, as the group is providing
the mothers with skills and opportunities to improve their ability to cope with
perinatal mental health issues.
Limitations
One limitation of these results is that the number of participants involved in the
evaluation was not sufficient to generalise the findings to the wider population.
However the results do provide a valuable insight into the experiences of young
mothers in the South Bristol area.
The literacy levels of the mothers provided a particular challenge in evaluating
the service, as completing questionnaires each week requires a certain level of
reading and writing ability, as well as motivation and concentration. This method
may also impact upon the ability of the mothers to express their thoughts about
the service, as a questionnaire has limited space for respondents to answer and
some may find that written emotional expression is not an adequate method.
It is possible that due to the low literacy levels amongst the young mothers,
the evaluation methods were not able to comprehensively collect the mothers’
feedback and experiences. In the future it may be necessary to include further
creative methods of evaluating the service. However, asking the mothers to
decorate the table cloths during the ‘knowledge café’ session in whatever way they
wished (e.g. drawing, writing key words) provided an alternative, more imaginative
way of evaluating the programme that may have helped to overcome any literacy
problems. Mothers were also given the chance to have one on one interviews with
the Buddy, or record their experiences in a film through interviews and using
cards to hold up key words to describe their feelings in a non-verbal manner
(please see the link on you tube http://www.youtube.com/watch?v=TiJHen_XCF
M&list=PL4AD32AFD77534329&index=15&feature=plpp_video). Therefore, there
were a number of ways for the young mothers to provide feedback about the
service.
Final Conclusions
This evaluation found that the services that Bluebell has been providing over the
past year have had a positive impact upon the mothers that have been involved.
Average anxiety and depression scores decreased after attending the group, and
the attendees were satisfied with how the group was run as well as the content
and structure. Therefore, these services will continue to run in order to support
25
young mothers who are experiencing perinatal mental health problems. The
learning from this evaluation will be utilised to expand the service and inform
further projects supporting partners of those experiencing perinatal anxiety
and depression, as well as mothers from other locations within Bristol. Current
funding has been restricted to supporting young mothers, however with further
funding the services can be offered to parents of all ages and socio economic
statuses. More one to one support could also be offered, as additional workers
could be recruited and trained to provide a bigger Buddy service.
26
Recommendations for practice
Written by Rachel Jenkins, Occupational Therapist, Anna Thompson, Project Manager & Ruth Jackson, Charity Director.
From our experience of establishing and running the Mums’ Comfort Zone
therapeutic group programme and the Bluebell Buddy service for one year, we
recommend the following for practitioners and organisations considering setting
up a similar service:
l Practitioners should try and cultivate an empathy with teenage mums who
contact them for help with suspected postnatal depression. One of the
key points made by the mums was that they felt listened to for the first
time when attending the group. They also felt respected, which gave their
confidence a huge boost.
l Practitioners should take time to explain medical jargon. Some mothers
on medication did not feel they understood their medication clearly,
including side effects, dosages and withdrawal symptoms.
l Introducing a parenting element into the programme would probably help
the mums develop coping strategies for their PND.
l It is effective to involve project beneficiaries in developing and designing a
programme from the outset, including marketing materials and language,
so they feel their ideas and needs are being listened to and have a sense of
ownership.
l That offering a peer-to-peer support, such as the Buddy role, would be
recommended as a key way to engage with hard to reach young mums who
demonstrate high levels of suspicion around professionals including GP’s
& Social Workers.
l We would emphasise the importance of having realistic expectations
about service users’ abilities to always engage with the offered provision.

l It is beneficial to try to think ‘outside of the box’ when thinking of ways to
overcome obstacles to accessing the provision of new services.
l When accepting new clients on to courses it is vital to ascertain some
personal history and very useful to have details of engagement with
previous services.
l During initial assessment it can be really useful to ascertain the levels of
users’ literacy in order to target any course materials effectively and put
support in place where it is needed.
l Offering a 1:1 visit with potential clients prior to uptake of any offered
provision has proved invaluable.
27
28
Acknowledgements
Avon Primary Care Research Collaborative
Avon Hello Tomorrow Fund
Comic Relief
Glamour magazine
Health Together - money raised through the Health Lottery
OMB Direct limited
Dr James Costello, PHD, the University of the West of England
The Co-operative Membership Community Fund
The Hartcliffe & Withywood Teenage Parents’ Project
The Pfizer UK Foundation (an initiative of Pfizer Limited)
References
Annual Conception Statistics, 2010. Office for National
Statistics, 2012. From education.gov.uk, accessed on
26-07-2012 at 16.21.
Kielhofner, G. (2008) Model of Human Occupation Theory and
Application. 4th edition. Baltimore:Lippincott, Williams &
Wilkins.
NICE Guidelines for Antenatal and Postnatal Mental
Health: Clinical management and service guidance (2007)
Petrou, S.; Cooper, P.; Murray, L. & Davidson, L. L. (2002).
Economic costs of Post-natal Depression in a high-risk
British Cohort. British Journal of Psychiatry, 181, 505-512.
Petrou, S.; Cooper, P.; Murray, L. & Davidson, L. L. (2006).
Cost-effectiveness of a preventative counselling and
support package for post natal depression. International
Journal of Technology Assessment in Health Care, 22, 443-453.
Rogers, C. R. (1979). The Foundations of the Person-Centred
Approach. Centre for Studies of the Person. La Jolla,
California.
‘Teenage Pregnancy Strategy: Beyond 2010’, Department
of Health; Department for Children, Schools and Families,
Crown Copyright.
World Café Presents Café to go (2008).
http://www.theworldcafe.com
29
Appendices
Appendix A- Information about the Charity
Bluebell was founded by Ruth Jackson and registered as a charity in 2010. Due to
her own personal experiences and her background in the voluntary and charitable
sectors, Ruth founded the charity with the aim of providing more support to all
those affected by perinatal mental health problems. Specifically the aims are to
reduce anxiety and depression in the perinatal period, increase education and
awareness about perinatal mental health problems, and to provide support where
there are currently gaps in service provision. Bluebell is proud to be user led, and
to have its foundations built upon the identified needs and gaps in services for
service users.
In order to establish whether there was a need for increased support, some
community events were run in cafes as informal public consultations as to
what the community felt was needed reaching over 100 local parents and health
professionals.
This led to the registration as a charity, and a bid for funding which was
successfully received from the Avon Hello Tomorrow Fund, which Bluebell won in a
national competition run by Glamour Magazine receiving more public votes than
any other project.
The next step was to ascertain which service user groups would most benefit
from increased support. To achieve this, focus groups were conducted in Bristol
from March to June 2011 with various service user groups. Focus groups attendees
represented Black and Ethnic Minority mothers, single mothers, partners of those
who had severe post-natal depression, young mothers and mothers from a middle
class background. From these sessions, it emerged that young mothers may
benefit most from the support services that Bluebell planned to offer. This more
specific focus led to funding from The Pfizer UK Foundation (an initiative of Pfizer
Limited) for the first year of the programme, and from Comic Relief for a further
three years of the programme with young mothers.
From the focus groups, the main themes that emerged were a desire for peer to
peer support, more information on signs and symptoms of post-natal depression
and anxiety, and a need for normalisation of post-natal depression, and
reassurance that things will get better. All of these themes are fundamental to
Bluebell’s work, and the focus group themes laid the groundwork for the services
that are now provided.
30
A board of trustees was also established in this time, including a Consultant
Psychiatrist from a local Mother and Baby unit and a Social Worker. The
board works in conjunction with a wider management committee which has
representation from health visitors and midwives, as well as mothers and fathers.
Therefore the charity is represented by those with relevant qualifications and
experience, as well as service users themselves.
Service users can be referred in to the charity through a health professional,
or they are also able to self-refer. Advertising materials for Bluebell include a
telephone referral number, which when contacted leads to a one to one visit
being arranged.
The referral criteria for the charity dictates that those with very complex needs
should be signposted to others agencies, for example to their General Practitioner
(GP), health visitor or other health professional. However Bluebell is flexible in their
referral criteria and do accept those with multiple and complex needs, working
in partnership with other agencies to ensure best practise and that high levels of
care are provided.
Alongside the group programme, a ‘buddy service’ was provided. The buddy
service was run by a member of Bluebell staff who was herself a young mother
who experienced perinatal mental health problems, and has since overcome these
problems. One to one sessions, telephone and text support were all offered by the
buddy. This part of the service was open to all group attendees, but it was left up
to them to decide whether they accessed the service or not. The buddy attended
each week of the programme, but was also available to support those who did not
attend the programme. The young mothers were also given journals to reflect upon
their experiences each week.
Future Directions
Bluebell has recently received funding to provide support to fathers and partners
of those who have perinatal mental health issues. The NICE guidelines for
Antenatal and Post-natal Mental Health state that "Healthcare professionals should
assess and, where appropriate address, the needs of the partner, family members and
carers of a woman with a mental disorder during pregnancy and the post-natal period"
(page 11, section 1.1.2.1). Therefore it is acknowledged that partners also require
support, and Bluebell plan to again address a gap in services and provide
additional support to fathers and partners outside of the medical model.
Funding is currently being sought to roll out new groups. These groups will be
open to mothers of all ages, and will be run in areas that are more ethnically
diverse than the area in which the current group was conducted. Therefore
there may be new challenges whose first language/or for whom English is not
31
the first language is not English and cultural differences that haven’t yet been
encountered. The model under evaluation in this report will be replicated for the
new groups, including the processes of designing the marketing materials. This
will ensure that the new group is tailored to the specific needs of the new service
users from the very beginning. Any changes will be service user led and more
events may need to be offered to gather views from other mothers as to how they
would want the groups to be run.
The aims of the new services are to meet the needs highlighted by the community
in relation to perinatal mental health issues, for example by supporting those
around the mothers as well as the mothers themselves. The current services
aimed to support 50 mothers each year, and the new branches of the service will
aim for a similar number to support directly, as well as those that the service can
indirectly support such as partners and children. Therefore through the group for
young mothers as well as the two new groups to be set up, it is hoped that Bluebell
will be supporting approximately 150 individuals directly in the near future, in
addition to the support that will be provided to partners. The service will also aim
to reach mothers of all backgrounds and cultures. The service users included in
this evaluation were mostly of Caucasian origin, and therefore it is hoped that
providing services in other areas of Bristol will make the group more accessible to
other minority ethnic groups.
In the long term, Bluebell hopes to measure the impact that the services it is
providing is having on the wider system around a mother with perinatal mental
health issues. For example, it may be possible to measure the impact that the
increased support has had on the children’s development and wellbeing. This
could be done through interviews or questionnaires with teachers, other family
members, and health professionals to gather opinions on whether the children
of mothers who have experienced perinatal mental health problems have been
affected adversely. A comparison could be made between children of those who
had received support from Bluebell and those who have not.
32
Appendix B- Statements of Income and Expenditure
Income:
l £10,000 - start up funding from the Avon UK Foundation to enable Bluebell
to run focus groups across Bristol with parents with lived experience of
depression related to pregnancy and birth to gather their views on gaps in
services.
l £30,000 - One year funding from The Pfizer UK Foundation (an initiative of
Pfizer Limited) to run pilot project with young mums in South Bristol - Mums’
Comfort Zone and the Bluebell Buddy services launched in September 2011.
l £65,000 - Three year funding from Comic Relief from June 2012 to continue the
project with young parents in South Bristol until 2015.
l £2,000 - recent donation from the Co-op community fund to start work with
young Dads who are supporting their partners though perinatal depression.
l £10,000 - a recent grant received towards our Dads’ Zone project with
young fathers from money raised by HealthTogether. 51 Community Interest
Companies raising money to address health inequalities across England,
Scotland and Wales through The Health Lottery.
Expenditure:
l £10 per week will fund one young mum to attend the 2 hour Mums’ Comfort
Zone group programme and enable her child to access the creche for 2 hours.
l £10 will fund one young mum to receive support from the Bluebell Buddy for up
to two hours per week either at home or in the community
l £200 per week will enable 10 young mums affected by depression to access
group and buddy support compared to £300 quoted by the Government as the
average cost for just one mum to receive support.
l £500 every quarter will pay for sessional workers to come and deliver sessions
on art, drama, music, Zumba, Yoga and pampering to allow the mums some
time out and to complement the therapeutic programme.
l £1,000 per annum will enable Bluebell to produce all the marketing, flyers and
postcards needed to promote our services in the local community.
33
34
Appendix C - Referral form
1
BLUEBELL BUDDY/MUMS’COMFORT ZONE REFERRAL FORM
(to be returned to: Danielle Sealy c/o The Teenage Parents’ Project, Tenants’ Centre, Gatehouse Way, Withywood, Bristol, BS13 9AN or tel. 07517 374699 in case of query)
Bluebell Client number:
Please note that all referrals must be made with the consent of the individual. The individual should
have been affected with depression relating to pregnancy and/or birth
Have you discussed this referral with the individual prior to completing this form? YES/NO
We aim to respond to all referrers within 2 weeks after receiving the referral to report progress. If you have any issues or concerns about the referral process or the support for the individual please contact Danielle Sealy on [email protected] or [email protected]
Name of client........................................................................ Date..............................................
Address.........................................................................................................................................
................................................................................................... Postcode...................................
Tel No...................................................................... Mobile No...................................................
Date of Birth...................................................... Marital Status...................................................
Number of children.............................. Ages of children.............................................................
Please provide details of any other agencies currently involved with the family:
....................................................................................................................................................
.....................................................................................................................................................
....................................................................................................................................................
...................................................................................................................................................
Please provide details of any previous history of mental health issues:
....................................................................................................................................................
....................................................................................................................................................
....................................................................................................................................................
2
Can you describe briefly why you are referring, providing any other information that you think will be useful to be aware of when assessing the client’s needs?
.....................................................................................................................................................
.....................................................................................................................................................
......................................................................................................................................................
.......................................................................................................................................................
.......................................................................................................................................................
.......................................................................................................................................................
......................................................................................................................................................
......................................................................................................................................................
......................................................................................................................................................
......................................................................................................................................................
Referred by:
Name Family Doctor
Agency Tel
Address Health Visitor
Tel Tel
Appendix C - continued
35
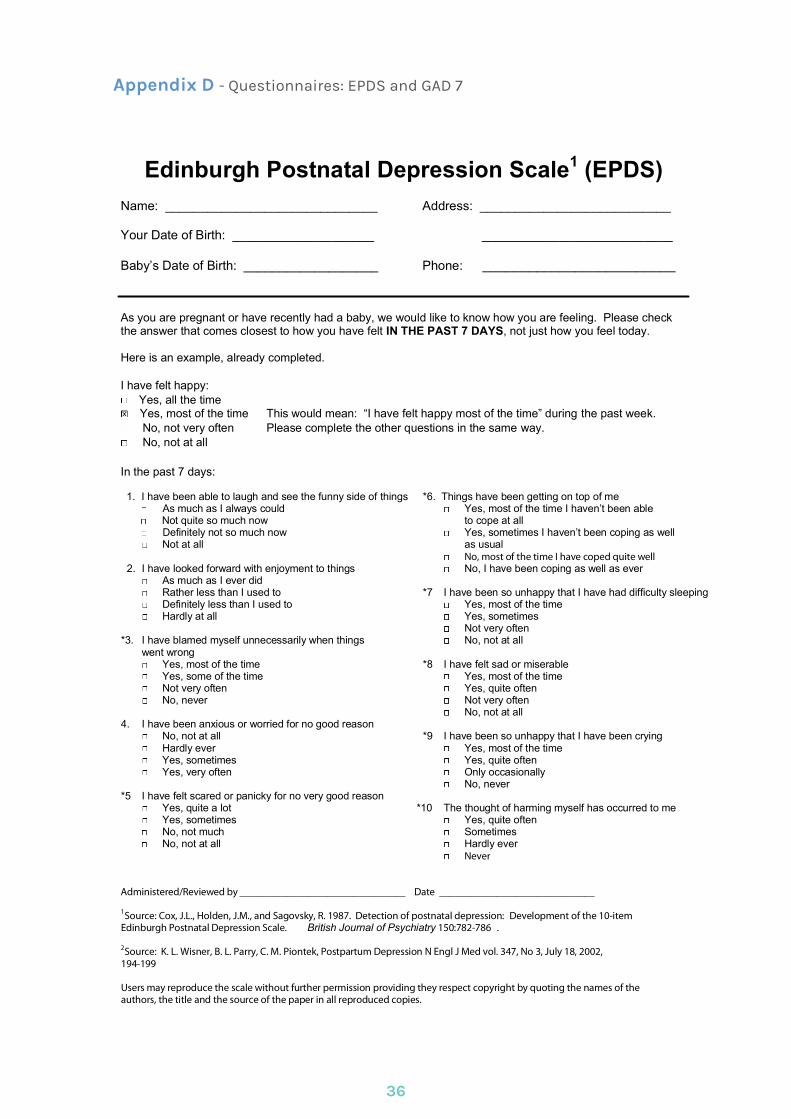
Appendix D - Questionnaires: EPDS and GAD 7
36
Edinburgh Postnatal Depression Scale 1 (EPDS) Name: ______________________________ Address: ___________________________
Your Date of Birth: ____________________ ___________________________
Baby’s Date of Birth: ___________________ Phone: _________________________
As you are pregnant or have recently had a baby, we would like to know how you are feeling. Please check the answer that comes closest to how you have felt IN THE PAST 7 DAYS, not just how you feel today.
Here is an example, already completed.
I have felt happy: Yes, all the time Yes, most of the time This would mean: “I have felt happy most of the time” during the past week. No, not very often Please complete the other questions in the same way. No, not at all
In the past 7 days:
1. I have been able to laugh and see the funny side of things *6. Things have been getting on top of me As much as I always could Yes, most of the time I haven’t been able Not quite so much now to cope at all Definitely not so much now Yes, sometimes I haven’t been coping as well Not at all as usual
2. I have looked forward with enjoyment to things No, I have been coping as well as ever As much as I ever did Rather less than I used to *7 I have been so unhappy that I have had difficulty sleeping Definitely less than I used to Yes, most of the time Hardly at all Yes, sometimes
Not very often *3. I have blamed myself unnecessarily when things No, not at all
went wrong Yes, most of the time *8 I have felt sad or miserable Yes, some of the time Yes, most of the time Not very often Yes, quite often No, never Not very often
No, not at all 4. I have been anxious or worried for no good reason
No, not at all *9 I have been so unhappy that I have been crying Hardly ever Yes, most of the time Yes, sometimes Yes, quite often Yes, very often Only occasionally
No, never *5 I have felt scared or panicky for no very good reason
Yes, quite a lot *10 The thought of harming myself has occurred to me Yes, sometimes Yes, quite often No, not much Sometimes No, not at all Hardly ever
Never
Administered/Reviewed by ________________________________ Date ______________________________
1 Source: Cox, J.L., Holden, J.M., and Sagovsky, R. 1987. Detection of postnatal depression: Development of the 10-item Edinburgh Postnatal Depression Scale. British Journal of Psychiatry 150:782-786 .
2 Source: K. L. Wisner, B. L. Parry, C. M. Piontek, Postpartum Depression N Engl J Med vol. 347, No 3, July 18, 2002, 194-199
Users may reproduce the scale without further permission providing they respect copyright by quoting the names of the authors, the title and the source of the paper in all reproduced copies.
No, most of the time I have coped quite well
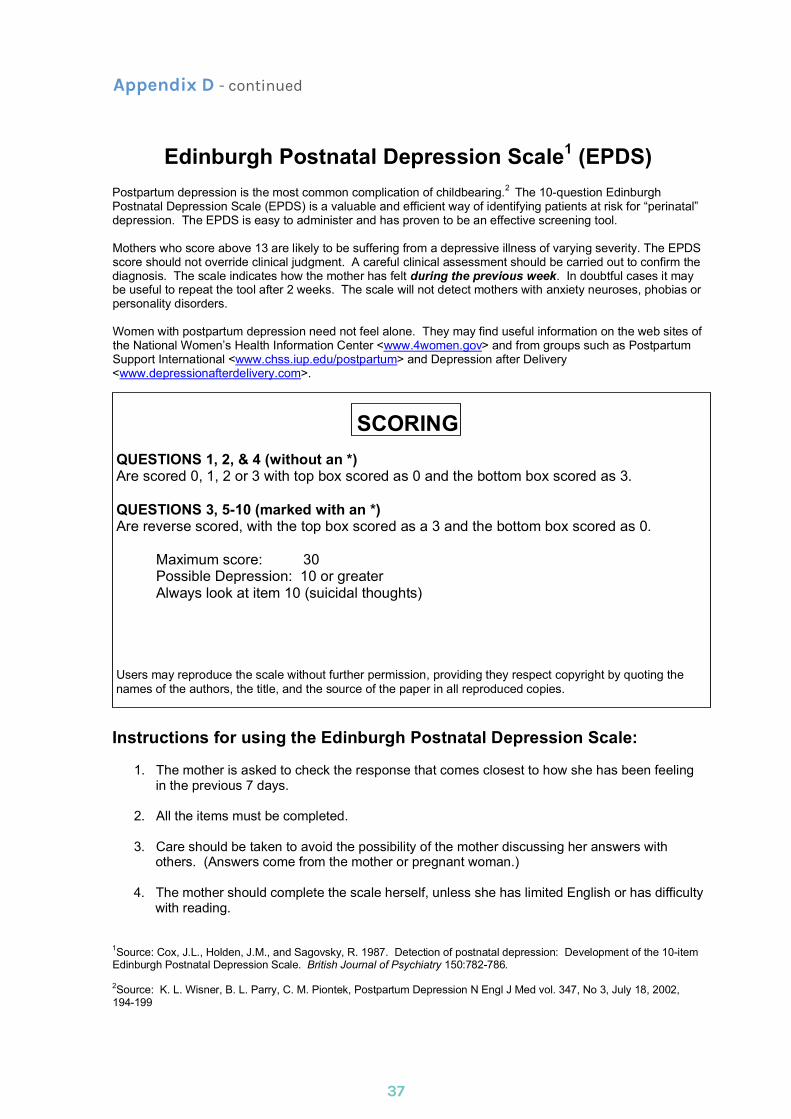
Edinburgh Postnatal Depression Scale 1 (EPDS) Postpartum depression is the most common complication of childbearing. 2 The 10-question Edinburgh Postnatal Depression Scale (EPDS) is a valuable and efficient way of identifying patients at risk for “perinatal” depression. The EPDS is easy to administer and has proven to be an effective screening tool.
Mothers who score above 13 are likely to be suffering from a depressive illness of varying severity. The EPDS score should not override clinical judgment. A careful clinical assessment should be carried out to confirm the diagnosis. The scale indicates how the mother has felt during the previous week. In doubtful cases it may be useful to repeat the tool after 2 weeks. The scale will not detect mothers with anxiety neuroses, phobias or personality disorders.
Women with postpartum depression need not feel alone. They may find useful information on the web sites of the National Women’s Health Information Center <www.4women.gov> and from groups such as Postpartum Support International <www.chss.iup.edu/postpartum> and Depression after Delivery <www.depressionafterdelivery.com>.
SCORING QUESTIONS 1, 2, & 4 (without an *) Are scored 0, 1, 2 or 3 with top box scored as 0 and the bottom box scored as 3.
QUESTIONS 3, 510 (marked with an *) Are reverse scored, with the top box scored as a 3 and the bottom box scored as 0.
Maximum score: 30 Possible Depression: 10 or greater Always look at item 10 (suicidal thoughts)
Users may reproduce the scale without further permission, providing they respect copyright by quoting the names of the authors, the title, and the source of the paper in all reproduced copies.
Instructions for using the Edinburgh Postnatal Depression Scale:
1. The mother is asked to check the response that comes closest to how she has been feeling in the previous 7 days.
2. All the items must be completed.
3. Care should be taken to avoid the possibility of the mother discussing her answers with others. (Answers come from the mother or pregnant woman.)
4. The mother should complete the scale herself, unless she has limited English or has difficulty with reading.
1 Source: Cox, J.L., Holden, J.M., and Sagovsky, R. 1987. Detection of postnatal depression: Development of the 10-item Edinburgh Postnatal Depression Scale. British Journal of Psychiatry 150:782-786.
2 Source: K. L. Wisner, B. L. Parry, C. M. Piontek, Postpartum Depression N Engl J Med vol. 347, No 3, July 18, 2002, 194-199
Appendix D - continued
37
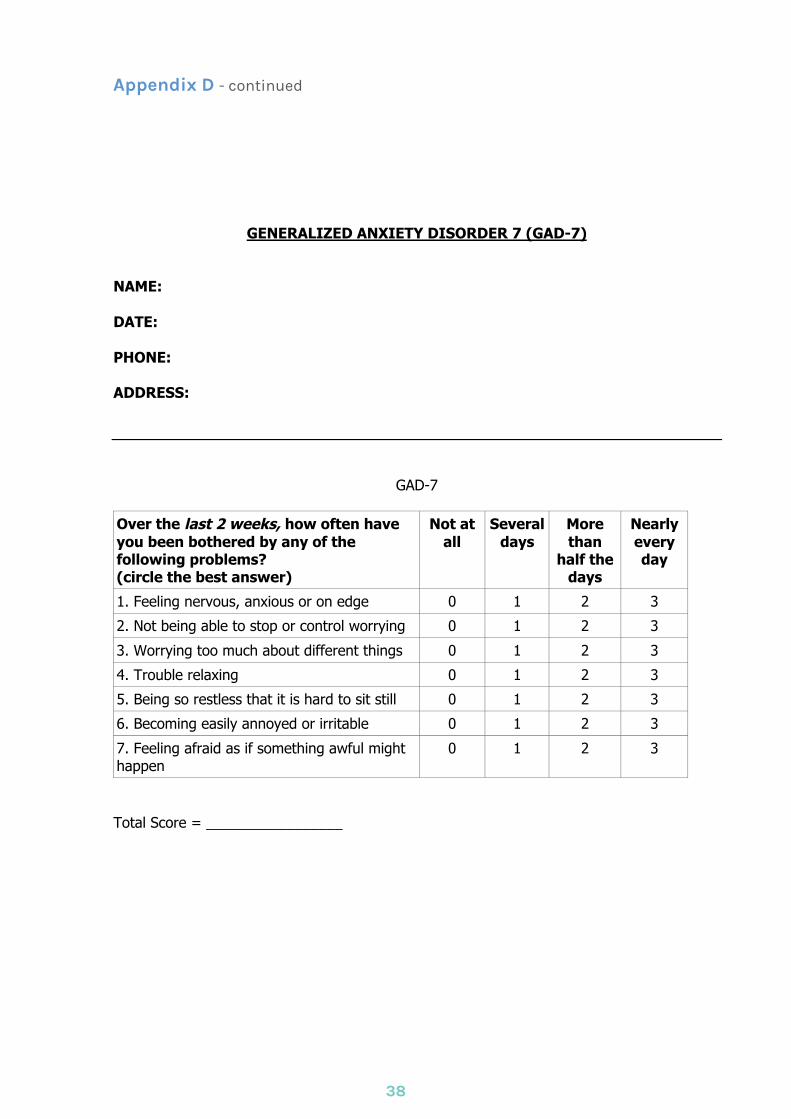
GENERALIZED ANXIETY DISORDER 7 (GAD-7)
NAME: DATE: PHONE: ADDRESS:
GAD-7
Over the last 2 weeks, how often have you been bothered by any of the following problems? (circle the best answer)
Not at all
Several days
More than
half the days
Nearly every day
1. Feeling nervous, anxious or on edge 0 1 2 3
2. Not being able to stop or control worrying 0 1 2 3
3. Worrying too much about different things 0 1 2 3
4. Trouble relaxing 0 1 2 3
5. Being so restless that it is hard to sit still 0 1 2 3
6. Becoming easily annoyed or irritable 0 1 2 3
7. Feeling afraid as if something awful might happen
0 1 2 3
Total Score = _________________
Appendix D - continued
38
Appendix E- Session evaluation form
39
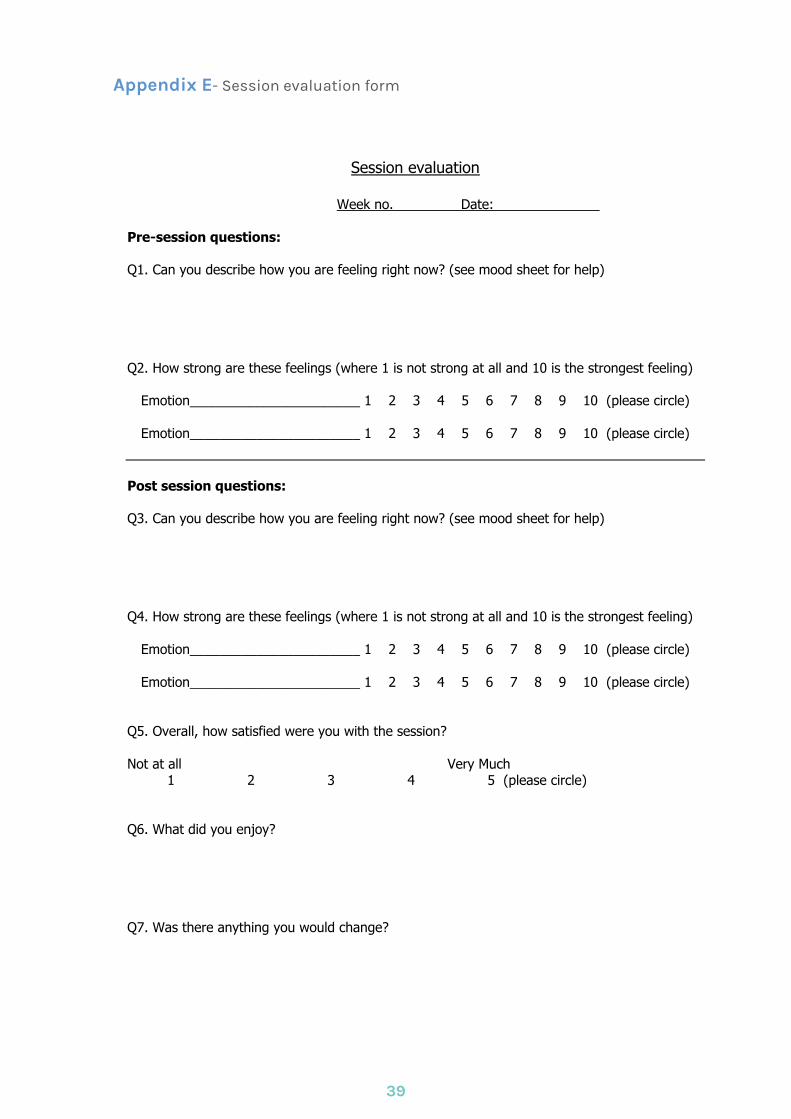
Session evaluation
Week no. Date:
Pre-session questions: Q1. Can you describe how you are feeling right now? (see mood sheet for help) Q2. How strong are these feelings (where 1 is not strong at all and 10 is the strongest feeling)
Emotion_______________________ 1 2 3 4 5 6 7 8 9 10 (please circle)
Emotion_______________________ 1 2 3 4 5 6 7 8 9 10 (please circle)
Post session questions: Q3. Can you describe how you are feeling right now? (see mood sheet for help) Q4. How strong are these feelings (where 1 is not strong at all and 10 is the strongest feeling)
Emotion_______________________ 1 2 3 4 5 6 7 8 9 10 (please circle)
Emotion_______________________ 1 2 3 4 5 6 7 8 9 10 (please circle) Q5. Overall, how satisfied were you with the session? Not at all Very Much 1 2 3 4 5 (please circle) Q6. What did you enjoy? Q7. Was there anything you would change?
Appendix F- Support group evaluation form
40
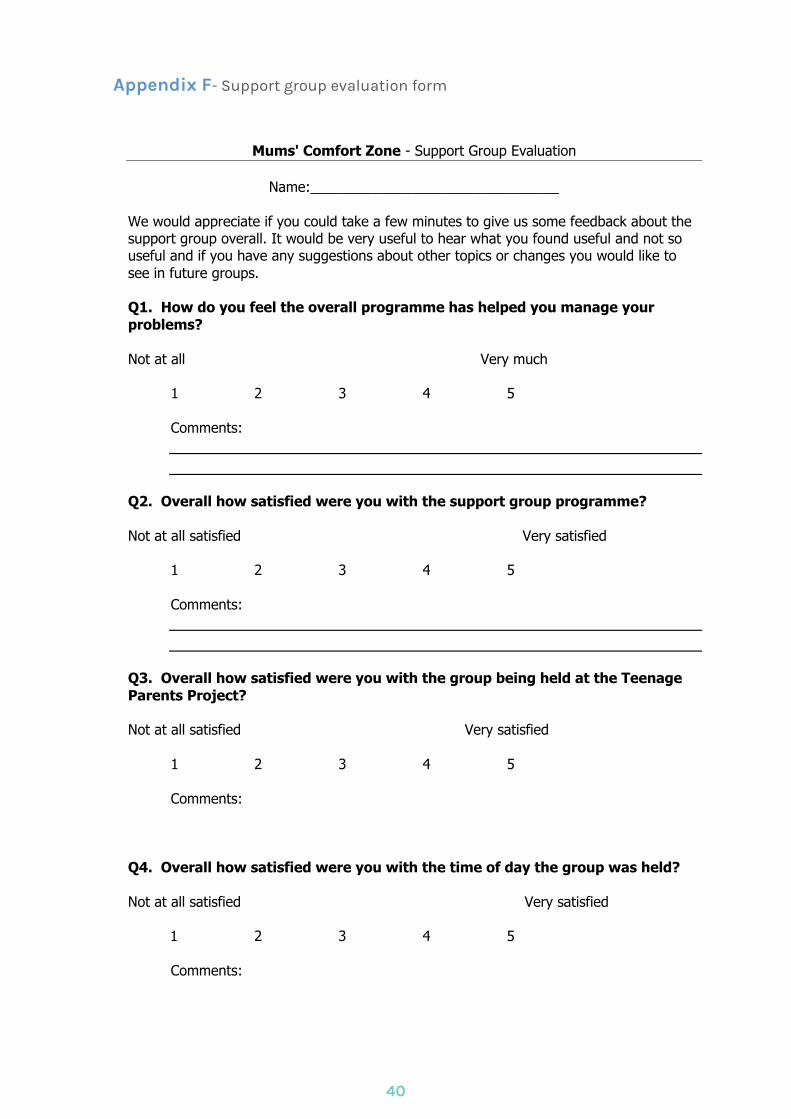
Mums' Comfort Zone - Support Group Evaluation
Name:________________________________
We would appreciate if you could take a few minutes to give us some feedback about the support group overall. It would be very useful to hear what you found useful and not so useful and if you have any suggestions about other topics or changes you would like to see in future groups. Q1. How do you feel the overall programme has helped you manage your problems? Not at all Very much
1 2 3 4 5 Comments:
Q2. Overall how satisfied were you with the support group programme? Not at all satisfied Very satisfied
1 2 3 4 5
Comments:
Q3. Overall how satisfied were you with the group being held at the Teenage Parents Project? Not at all satisfied Very satisfied
1 2 3 4 5
Comments: Q4. Overall how satisfied were you with the time of day the group was held? Not at all satisfied Very satisfied 1 2 3 4 5
Comments:
Q5. Overall were you satisfied that the group leaders communicated topics clearly and in an interesting way? Not at all satisfied Very satisfied 1 2 3 4 5
Comments:
Q6. How useful did you find the buddy service provided by Danielle? Not at all useful Very useful 1 2 3 4 5 Is there anything else you would have liked from the buddy service? e.g more contact, more information on other services? ________________________________________________________________________ _______________________________________________________________________ Q7. How do you feel about the amount of information provided and the number of topics covered in the programme? Too little information Too much information
1 2 3 4 5
Comments:
Q8. Do you feel you had the opportunity to ask questions? Not enough opportunity Plenty of opportunity
1 2 3 4 5
Comments:
Q9. What were the things that you found most useful? Or how do you feel you have benefited from attending the group programme?
Appendix F- continued
41
Q10. Do you have any suggestions for things we could change about the course? Or any further comments about the course. Q11. Please rate your current overall wellbeing Very poor Very good 1 2 3 4 5 Q12. Do you feel you need some more support now that the group support programme has ended? Yes/No (please circle) If yes, would you like Bluebell Nurses to contact you to discuss one-to-one support and other options? Yes/No (please circle) As part of the programme we may want to contact you in future for further feedback. If you do NOT wish to be contacted please tick this box □ As part of promoting future groups we may use information that you have supplied on the evaluation form to inform others of the benefits of attending (anonymously), if you do NOT want your information to be used in this way please tick this box □ Thank you very much for your time and commitment to this group. Your comments are valued and much appreciated.
Appendix F- continued
42