Embed Size (px)
Citation preview

Every Woman, Every Time:
Disparities in Breast Cancer
Tony L. Weaver, D.O. ALOMA 2015

Disclosures
I have no financial, personal or professional disclosures to report. All of the opinions expressed in this presentation are my own and are not indicative of the views of my past or current employers.
Objectives
● Define Health Equity & Disparities
● Describe the existing Health Disparities in Breast Cancer
● Discuss the factors contributing to Health Disparities in Breast Cancer
● Introduce & Inspire change in Breast Cancer Care

Defining the SystemEquity: the absence of unfair, avoidable or remediable differences in health among population groups defined socially, economically, demographically or geographically.
Disparities: differences in the incidence, prevalence, mortality, burden of cancer & related adverse health conditions, beyond what would be expected under equitable circumstances that exist among specific population groups in the United States.
Health Disparities
Small Differences that eventually lead to Major Inequalities in patient outcome.

Populations Facing Disparities
● Racial/Ethnic Groups● Gender● Age ● Socioeconomic Status ● Geographical Location● Poorly Educated

Defining the Problem Breast Cancer Facts:
● Breast cancer is the most common cancer and the leading cause of cancer deaths in women worldwide.
● 2nd MCC of death in women in USA.
● Studies suggest that disparities in outcomes by race & ethnicity have not improved over time.
● Breast Cancer 14.0% of all new cancer diagnoses
● An estimated 235,000 new cases of breast cancer each year and an estimated 40,000 women will die.
● 1 in 8 women will be Diagnosed.

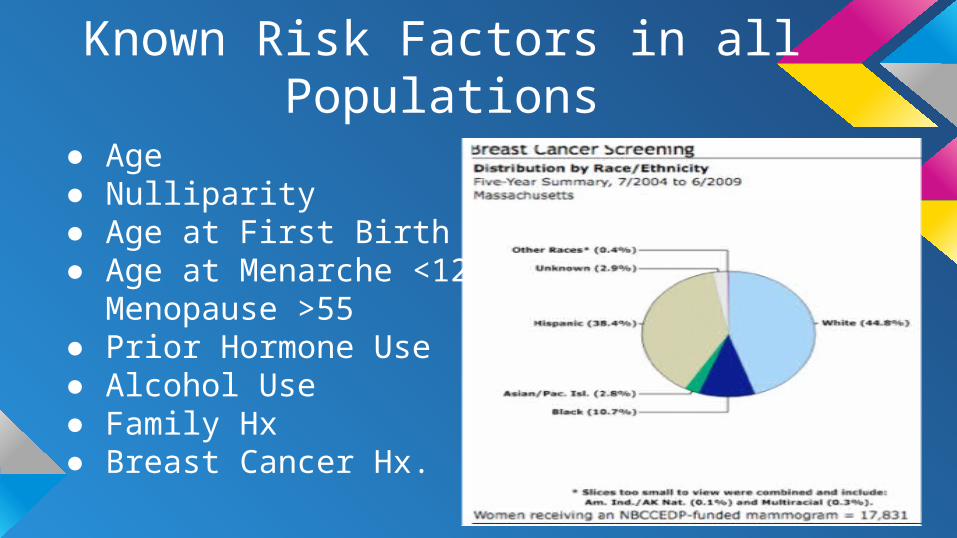
Known Risk Factors in all Populations
● Age● Nulliparity● Age at First Birth ● Age at Menarche <12 &
Menopause >55● Prior Hormone Use ● Alcohol Use● Family Hx● Breast Cancer Hx.

Disparities Unmasked Incidence
● Breast Cancer Incidence continues to rise for all patients.
● 122:100,00 for White Women ● 117:100,000 for Black Women
Mortality: ● Black Women: 27 Deaths per 100
breast Cancers ● White Women: 18 Deaths per 100
breast Cancers ● 45% (Black) vs 35% (White)
Diagnosed at Late Stage● Significantly Higher Mortality for
Similar Stage
Is this an Isolated Problem?
Confirmed Disparities in:
● Routine Screening● Pain Management● Access to Surgery ● Timely consultation ● Outcomes in cardiac, cancer and
kidney care● Mental Health Treatment ● Hospital Admissions● Less Likely to have PCP

Breast Cancer Deaths

Possible Causes Cost: ● Uninsured or Underinsured Patients● Cancer Pts 2X more likely to file
bankruptcy
Access: ● Transportation & Location
Quality/Behavior: ● Fewer High Risk women get BCT● Inadequate pain control● Social determinates of Health ● Provider Bias

Social Determinates of Health

JAMA Study nearly 375,000 Women ● Black women were less likely to be diagnosed with stage I breast
cancer 37.0% vs 50.8%; Non-Hispanic white women● 2x More likely to die w/ small-sized tumors (7-year actuarial risk for
death from stage I Disease 6.2% vs 3.0%.)● Asian had the earliest Diagnosis and Were the least Likely to Die.
(0.8% vs 1.5%, respectively; hazard ratio, 0.60 [95% CI, 0.49-0.73]; P < .001).
● The difference between black women and non-Hispanic white women remained after adjusting for income and estrogen receptor (ER) status and after excluding patients with triple-negative breast cancer.
● Biology is a Huge factor. BUT not the ONLY.

Problem Identified
Inequalities on Every Level:
● Risk Assessment ● Treatment ● Follow up
Undetermined Differences in Biology

Screening
● The American Cancer Society (ACS) recommends annual mammography for women age 40 and older.
● USPSTF biannually starting at age 50.
● Diagnostic vs Screening
Routine use of Breast Cancer Risk Model for all Patients >35.
Risk Assessment Tools BCRAT
Intended for women who have never had a diagnosis of breast cancer, DCIS or LCIS, and who do not have a strong family history suggesting inherited breast cancer.
Gail Model uses data primarily from studies of white and black.
Accuracy of Gail model ● Current age (the tool for >35 and older)● Age of menarche● Age at first live birth of a child● Number of first degree relatives with breast
cancer● Number of previous breast biopsies● Whether any breast biopsy has shown
atypical hyperplasia● Race (and subrace/ethnicity if the woman is
Asian American)


There are women who have come to think of their
breasts as the enemy. —Dr. Kenneth Offit
National Cancer Data Base Analysis revealed:
● 12% of women who received surgery for Stages 0-to-3 breast cancer underwent a double mastectomy, up from 2% in 1998.
● In 2014 Nearly 30% of women under age 45.
● Mortality Outcomes have been statistically the same.
● 13% Risk of Developing a different Cancer.
● Offers some cosmetic and convenience benefit.

Follow Up & Outcomes
Behavior:● Higher Non-Compliance w/
Endocrine therapy. ● Feeling of hopelessness
● 34% had survival knowledge vs 57% in white women.
● Communication Barriers ● Distrust of Healthcare System

What’s the Real Solution?
Disparities Start & END
with Differences.