Embed Size (px)
DESCRIPTION
Evidence Based Approach To Falls. Dr Larry Dian Division Of Geriatric Medicine U.B.C. Evidence Based Approach. This page is intentionally left blank. Epidemiology. Falls are common; 50% for those 80 years and older fall yearly - PowerPoint PPT Presentation
Citation preview

Evidence Based Approach To Falls
Dr Larry Dian
Division Of Geriatric Medicine
U.B.C.

Evidence Based Approach
This page is intentionally left blank

Epidemiology
Falls are common; 50% for those 80 years and older fall yearly
60 % of those with a history of a fall in the previous year will have a subsequent fall
Most falls result in an injury of some type 10% major injury, 5 % lead to
hospitalization, >70% fear of falling

Scenario 1
You receive a call from the emergency physician regarding your 86 year old patient who is being sent home after receiving sutures for a scalp laceration that occurred after a fall. CT head “normal”.

Acute Fall
Why did the person Fall?

5 Step Assessment
Question 1: Did the fall result as a loss of consciousness?
If yes: Sz. or Stokes- Adams attack
EEG, 24 hour holter, echocardiogram Micro burst of LOC likely not significantConfusion or drowsiness after fall
somewhat supportiveCollateral history very helpful

If No Loss of Consciousness
Was Fall preceded by dizziness?Was Fall preceded by dizziness?Type 1: Vertigo- Central/peripheral
BPV commonestType 2 Lightheadedness/
transient cerebral hypo-perfusion/orthostatic hypotension
Type 3: “Dizziness of legs”/unsteadiness Type 4: De-afferentation /psychological

If No Dizziness
Was the fall associated with an acute medical illness?
Atypical presentation Delirium
“Round up all the usual suspects”

If No Acute Illness
What was the mechanism of the fall?Be as precise as possible recreating actions before and after the fall
Avoid leading questions; patients may not remember
Collateral history very useful

If No Mechanism For Fall
Falls are either multi-factorial or lower limb weakness
“Just Fall” fall –eccentric weakness of quadriceps muscle

5 Step Algorhythm
Provides a rational strategy for mechanistic determination of the fall
Provides a strategy for fall risk reduction

Scenario 2
The family of your 89 year old patient wants your opinion about moving their reluctant mother in a nursing home because of the concern that she might fall and “hurt herself”

Risk Factors
Past history of a fall Lower extremity weakness Age Female gender Cognitive impairment Balance problems
Psychotropic drug use
Arthritis History of stroke Orthostatic
hypotension Dizziness Anemia

Chronic Diseases
Parkinson's disease Osteoarthritis of the knee, feet ankle Cognitive impairment (mmse 18-23) 2x
increased risk of falls Risk increases with increasing number of
chronic diseases Number and type of medications Alcohol use

Targeted Physical Exam
Cardiovascular system Central nervous system Musculoskeletal system; lower limbs

Targeted Physical Exam
Postural blood pressure Heart failure, Atrial fib, Aortic stenosis Mental status, Parkinson’s disease, stroke
peripheral neuropathy, visual acuity Arthritis of knees feet, podiatric problems Strength of hip flexors, ankle dorsi-flexors Environmental factors, footwear, mobility aids

Supplemental Tests
Get Up and Go Test Functional reach test Sternal nudge test; unipedal and tandem stance

Get Up and Go Test
Have the patient sit in a straight-backed high-seat chair
Instructions for patient: Get up (without use of armrests, if possible)
Stand still momentarily Walk forward 10 ft (3 m) Turn around and walk back to chair Turn and be seated

Get Up and Go Test
Factors to note: Sitting balance Transfers from sitting to standing Pace and stability of walking Ability to turn without staggering

Diagram of functional reach test to assess balance in elderly persons

e-mail this to a colleague
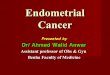
Algorithm summarizing the assessment and management of falls

Therapy
Address medical issues Review home environment Provide appropriate walking aid Gait and balance exercise training

Falls are not random events Falls are common and are associated
with significant morbidity and mortality Standardized assessment tools exist A coherent mechanism can be
developed in most cases Consider referral to falls clinic in complex
cases