Embed Size (px)
Citation preview

1
Evidence based treatment
recommendations for lateral
epicondylalgia
Josh McCormack, PT, PhD, OCS
Provider Disclaimer
• Allied Health Education and the presenter of this webinar
do not have any financial or other associations with the
manufacturers of any products or suppliers of
commercial services that may be discussed or displayed
in this presentation.
• There was no commercial support for this presentation.
• The views expressed in this presentation are the views
and opinions of the presenter.
• Participants must use discretion when using the
information contained in this presentation.
Objectives
• 1) Select the most appropriate clinical tests to rule in a diagnosis of lateral epicondylagia and to rule out other conditions such as cervical radiculopathy.
• 2) Understand the difference between tendinitis, tendinosis, and tendinopathy and how this affects treatment strategies.
• 3) Describe the current research on which interventions are most effective for lateral epicondylagia
• 4) Perform manual therapy techniques that have been demonstrated to be useful for patients with lateral epicondylagia.
• 5) Develop an evidence based treatment plan for patients with lateral epicondylagia.
• 6) Describe the most relevant and commonly used functional outcome measures for patients with lateral epicondylagia.

2
Review• Very common
– Most common cause of elbow/forearm pain in adults
– Prevalence of 1-3% of adults and 7% in workers
– Only 5-10% of cases involve tennis players
• Peak incidence between 40-50 years– If over 50 consider C-spine or OA of elbow
• Repetitive overuse injury/Insidious onset– Handling tools heavier than 1kg (2.2lbs)
– Lifting load heavier than 20kg (44lbs) more than 10 times per day
– Repetitive movements more than 10 times per day
• Dominant arm more common– Bilateral is rare
• Smoking, obesity, diabetes increase risk
• Self limiting condition– 12-18 month resolution
• Pain over common extensor tendon
– ECRB
– EDCImage from: painguy.com
Important Terminology
• Often confusing as terms are commonly misused and used interchangeably
• Tendonitis (Epicondylitis)– Commonly used incorrectly as a blanket term
for all tendon injuries
– Indicates presence of inflammation • Not typical except with acute conditions
• Tendinosis (Epicondylosis)– Absence of inflammation
– State of tendon degeneration
– More common clinically
• Tendinopathy – General descriptor for any tendon injuries
withy resultant pain and dysfunction
– This is the term we will primarily use today
– Has been suggested that –osis and –itis be reserved for cases where underlying pathology has been proven
– Epicondyalgia (pain)
Stages of development
1) Slight pain a few hours after activity
2) Pain immediately after activity
3) Pain during activity that increases after
stopping
4) Constant pain that limits activity

3
Etiology/Pathogenesis
• Still some uncertainty
• Classically believed to be an inflammatory process hence the term epicondylitis– Histology studies show minimal to no inflammation
present
• Findings– Microscopic tearing
– Degenerative changes
– Incomplete healing
– Tissue necrosis
– Neovascularization and neural ingrowth
– Presence of disorganized and immature collagen formation with increased immature fibroblastic and vascular elements
Examination/Diagnosis
Common Findings:
– Tenderness over the lateral epicondyle and common extensor tendon
– Pain with resisted wrist extension
– Discomfort at end range of wrist flexion
– Pain with decreased grip strength
– Positive middle digit extension test
– Positive Cozen’s test
– Postive Mill’s test
Special Tests (Sn/Sp not reported)
• Middle digit extension (Maudsley’s)– Elbow extended and wrist in neutral
– Palpate over lateral epicondyle
– Manual resistance applied over distal middle digit
– Positive if pain over lateral epicondyle
• Cozen’s– Stabilize patients arm in 90 degrees of flexion while palpating over
lateral epicondyle
– Patient’s makes fist while placing forearm/wrist into radial deviation and pronation
– Manual resistance to wrist extension applied
– Positive if painful over lateral epicondyle
• Mill’s– Palpate lateral epicondyle while pronating forearm, flexing wrist, and
performing radial deviation with elbow extended
– Positive if pain over lateral epicondyle
4
Special Test Videos
• Maudsley’s – https://www.youtube.com/watch?v=JPHUQfxweiQ
• Cozen’s– https://www.youtube.com/watch?v=3Sx6d3D-YEA
• Mill’s– https://www.youtube.com/watch?v=Bp9Ld-1sU44
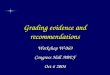
Differential Diagnosis
• Radiculopathy– Screen C-spine ROM
– Clinical Prediction Rule
• <60 degrees rotation, positive cervical distraction, positive Spurling’s (with SB), positive ULTTA*
• OA– Men over 50
– Pain at endrange of ROM
– Reduced ROM and subjective stiffness
– Crepitus
• Radial Nerve/Radial Tunnel Syndrome– Pain is distal and/or lateral to
epicondyle
– Pain with resisted supination
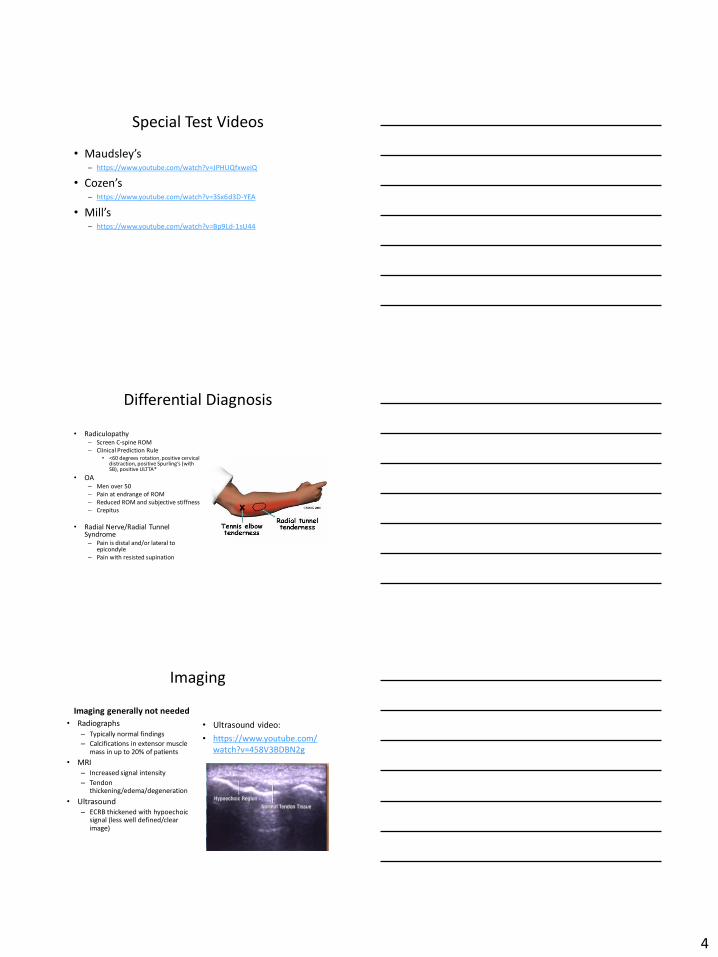
Imaging
Imaging generally not needed
• Radiographs
– Typically normal findings
– Calcifications in extensor muscle mass in up to 20% of patients
• MRI
– Increased signal intensity
– Tendon thickening/edema/degeneration
• Ultrasound
– ECRB thickened with hypoechoic signal (less well defined/clear image)
• Ultrasound video:
• https://www.youtube.com/
watch?v=458V3BDBN2g

5
Treatment Options
– Lots of research, mixed results
– PT is generally considered to be an effective treatment
option
– Multi-modal approach most likely to result in positive
outcomes
• Systematic review suggests exercise, soft tissue mobilization, and
mobilization/manipulation recommended treatment
Exercise
• Strengthening- Strong recommendation
– Wrist extensors
• Type of exercise
– Evidence supports eccentrics over concentrics/isometrics
» Head to Head RCT- faster pain reduction and 10% higher
success rate ecc vs con
» Not as clear-cut as it is with Achilles
» Some benefit of each has been found
– May use combination of both
– Ideal parameters unclear
» 2-3 sets of 10-15 repetitions 1-2 times per day
Eccentrics
Images from: thera-bandacademy.com, probraces.com, completephysiotherpay.co.uk

6
Flexbar eccentric Video
• https://m.youtube.com/watch?v=gsKGbqA9a
No
Why Eccentrics
• No definitive answers – Most research on Achilles tendon injuries
• Improved tendon structure/remodeling to allow proper healing hypothesized
• Studies have demonstrated:– Increased type I collagen synthesis rate
– Decreased tendon thickness
– Normalized collagen structure
– Destruction of neovascularity
• Likely a combination of these and possibly other factors involved
Why eccentricsRees JD, Wilson AM, Wolman RL. Current concepts in the management of tendon disorders. Rheumatology (Oxford). 2006;45:508-521.

7
Exercise
• Stretching
• Evidence supports combined stretching and
strengthening program
– Wrist extensors and flexors
• Add finger flexion for EDC
Images from webmd.com and teachpe.com
Manual Therapy
• Less evidence/support than exercise
• Favorable outcomes when combined with
exercise
– Soft tissue treatments
– Mobilization with movement
– Mill’s manipulation– Scaphoid Manipulation
– Cervical/thoracic manual therapy
Soft tissue treatment • Hands only (transverse friction) or instrument assisted techniques
– Long term benefits when combined with exercise but unclear if one approach is best
– Recent area popularity and research focus, may see more clarity with future studies
• Goal: tissue regeneration/remodeling
Images from: Sevier and Stegink-Janesn, physio-pedia.com, Blachhette and Normand

8
Astym• 78% response rate for Astym (plus exercise) vs 41% for exercise
• Greater improvements in DASH scores and grip strength for Astym (plus exercise)
Graston
• 27 subjects
• Group 1– STM treatment with Graston 2x/week 5 weeks
• Group 2– Education that LE is self limiting
– Ergonomics education
– Wrist flexor/extensor stretches for HEP
• Patient Rated-Tennis Elbow Evaluation, VAS, and pain free grip
• Both groups improved significantly at 6 week and 3 month follow ups– Improvements favored the Graston group but sample size
was too small – no significant difference between groups
Soft tissue mobilization
• Suggested to stimulate affected soft tissue to regenerate and heal and a cellular level
• Increased fibroblast recruitment and activation has been demonstrated in multiple studies of rat tendons
• Possible role in destruction of neovascularity?
• Similar explanations as provided for eccentric exercise
– Lends support for combined treatment program

9
Mobilization with Movement
• Mulligan technique
– Lateral glide at elbow while
patient performs a previously
identified painful task (gripping
or wrist extension)
– Several studies demonstrate
short term benefit
– Long term benefit when
combined with other
treatments
Images from: clinicalgate.com and researchgate.net
MWM
• Video 1:
https://m.youtube.com
/watch?v=aEzBL5t2h3s
• Image from: cl inicalgate.com
• Self Treatment:
Elbow/Wrist Manipulations• Immediate short term symptom relief
• Long term benefit unclear
• Mill’s Manipulation– Forearm pronation
– Wrist flexion
– Ipsilateral SB
– Elbow extension thrust
• Scaphoid Manipulation
– Palm down and supported on table
– Grip scaphoid between thumb and index finger
– Wrist into extension with thrust of scaphoid ventrally
– Images from: physio-pedia.com

10
Videos
• Mill’s Manipulation
• Video 1: https://m.youtube.com/watch?v=nNIH0sYcZnw
• Video 2: https://m.youtube.com/watch?v=t8VaMFWLlJM
• Scaphoid Manipulation
• https://m.youtube.com
/watch?v=edJpqY0Yr7g
CT Spine Manual Therapy
• Short term benefits demonstrated
– Immediate improvements in grip, tenderness, and pain lasting up to 24 hours
• Long term benefits unclear
• Cervical > thoracic
• Large retrospective study found no notable improvement in outcomes when adding c-spine treatment but patients receiving c-spine treatment had fewer visits
Why manual therapy?

11
Ultrasound
• Mixed and inconclusive results
• Ultrasound less effective than exercise
• 2/3 US studies showed no benefit vs placebo
in short term, more favorable results in mid
term (13 weeks) but inconclusive
• Some studies look at US 5 days/week
Ionto
• 1 study found similar results between ionto
and injection in short and long term
• 3 studies found short term benefits vs placebo
but no evidence of mid or long term benefit
Wrist Splint or Counterforce Brace• Mixed results regarding effectiveness
• 2/3 head to head studies found splint to be more effective on pain relief
– Other showed no difference between the two
• Splint
– decreases activity of wrist extensors
• Brace:
– reduces force transmission across extensor tendon…second origin point
Images from: Garg et al

12
Laser
• Inconsistent results in several studies
– Short term evidence inconclusive, mid and long
term shows no benefit
– Discrepancies with parameters
– May be more clear with additional research
– 4/6 studies vs placebo found no difference
Images from: gizmodo.com
E-stim
• Low level evidence showing benefit in short
term versus placebo only
Multi-modal approach
• Tier 1 – All patients – Exercise – eccentrics and stretching
• Tier 2 – Consider for most patients – Soft tissue treatment
– Elbow mobilization with movement
– Mill’s manipulation– Scaphoid manipulation
• Tier 3 – Consider in specific situations• More inconsistent results and/or demonstrated short term
benefits only
• Considered based on exam findings, pain limiting ability to perform exercises, not progressing as expected
– Manual therapy directed a CT spine
– Ionto /US
– Counterforce strap or wrist extension brace
– Laser
•
13
Non PT interventions
• Steroid injections
• PRP
• Autologous whole blood
• Polidocanol
• Botox
• Shockwave therapy
• Tenex
Corticosteroid Injections
• Short term benefit
• High recurrence rate (34-74%)
• PT has been shown to be more effective in moderate and long term in multiple studies
• May be of most benefit for patients having too much pain to tolerate PT interventions – Should start PT shortly
afterwards
– Also consider for patients not responding to PT within ~6-8 sessions
• Image from newhealthadvisor.com
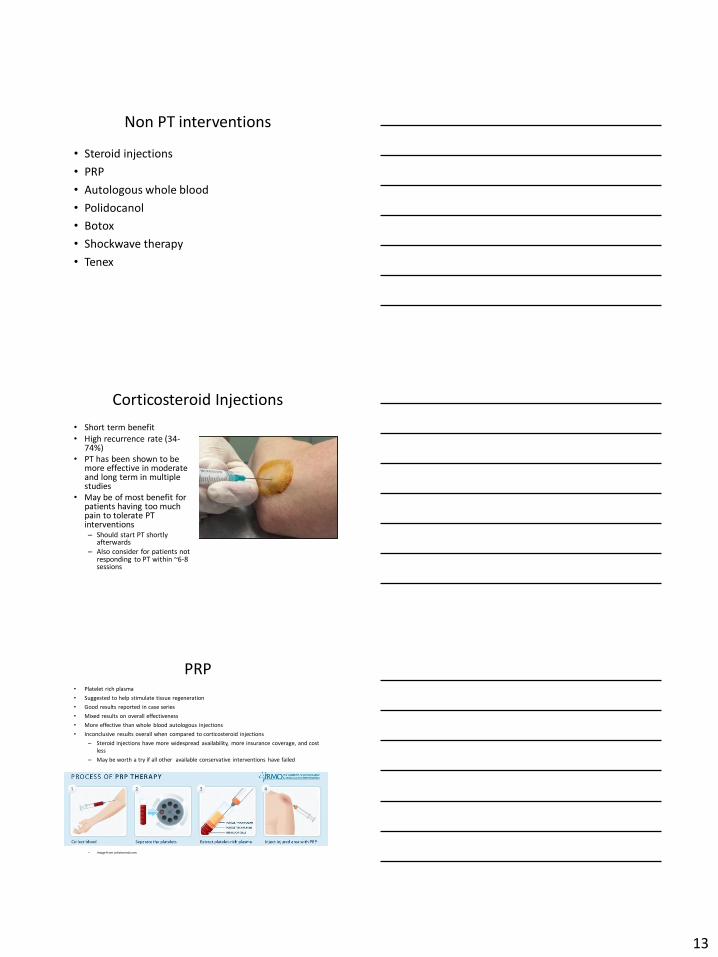
PRP• Platelet rich plasma
• Suggested to help stimulate tissue regeneration
• Good results reported in case series
• Mixed results on overall effectiveness
• More effective than whole blood autologous injections
• Inconclusive results overall when compared to corticosteroid injections
– Steroid injections have more widespread availability, more insurance coverage, and cost
less
– May be worth a try if all other available conservative interventions have failed
– Image from johstonmd.com

14
Polidocanol injections
• Used to treat varicose veins
• Sclerosing agent has been shown to be
potentially useful in Achilles and patellar
tendinopathy
– Destroy neovascularization/neural ingrowth
• Introduces an inflammatory response
• Early evidence is promising but insufficient to
recommend routinely
Botox injection
• 3 of 4 studies found improvements in pain when compared to placebo
• 1 study found Botox injection was less effective at reducing pain compared to a corticosteroid injection
• Accompanying transient extensor muscle weakness not acceptable to many patients especially when considering the studies showing less effective than steroids
Shockwave Therapy
• Based on treatments used for kidney stones
• Uses intense short energy waves travelling faster than speed of sound
• Promising results with LE
• Suggested to help stimulate healing process to occur in degenerative tendons
• Costly
– Limited insurance coverage
• Limited availability in many areas

15
Tenex• Ultrasonic Percutaneous
Tenotomy– Also called FAST (fasciotomy
and surgical tenotomy)
• Minimal invasive in-office procedure with local anesthesia – Incision ~1/8 to 1/4 inch
– Insert microtip which uses ultrasonic energy for target microresection of damaged tendon tissue
– Procedure takes ~15 minutes
• 2 large case series only
• Good short and long term (1-3 years) results reported
Image from: tenexhealth.com
Surgical procedures
• Multiple surgical procedures have been
described with 75-90% success rates reported
in various studies
Outcomes
• Outcomes collection highly recommended and
may be required in the future (sort of is already
with Medicare G-codes)
• Upper extremity functional index
• Disabilities of the arm, shoulder, hand shortened
• Patient Rated tennis elbow evaluation
• Patient specific functional scale

16
UEFI
QDASH
Patient Rated tennis elbow evaluation

17
PSFS
• Have patient list 2-3 activities that they have
difficulty with because of their pain
• Have them rate each activity based on level of
difficulty on scale below
• Total score= sum of scores/number of
activities
Summary
• Physical therapy effective for most patients
– Multimodal treatment approach
• Eccentrics and stretching
• Soft tissue mobilization
• Manual therapy (extremity/spine)
• Modalities
• Bracing
• Injections may be a reasonable option in certain cases
– Steroid injections first option
– PRP/ Polidocanol worth considering if available
• Tenex or Shockwave may be considered before surgery
Questions

18
References• Bisset L, Paungmali A, Vicenzino B, Beller E. A systematic review and meta-analysis of clinical trials on physical
interventions for lateral epicondylalgia. British journal of sports medicine. 2005;39(7):411-22; discussion -22.
• Blanchette MA, Normand MC. Augmented soft tissue mobilization vs natural history in the treatment of lateral epicondylitis: a pilot study. Journal of manipulative and physiological therapeutics. 2011;34(2):123-30.
• Cleland JA, Whitman JM, Fritz JM. Effectiveness of manual physical therapy to the cervical spine in the management of lateral epicondylalgia: a retrospective analysis. The Journal of orthopaedic and sports physical therapy. 2004;34(11):713-22; discussion 22-4.
• Cullinane FL, Boocock MG, Trevelyan FC. Is eccentric exercise an effective treatment for lateral epicondylitis? A systematic review. Clinical rehabilitation. 2014;28(1):3-19.
• Dingemanse R, Randsdorp M, Koes BW, Huisstede BM. Evidence for the effectiveness of electrophysical modalities for treatment of medial and lateral epicondylitis: a systematic review. British journal of sports medicine. 2014;48(12):957-65.
• Dion S, Wong JJ, Cote P, Yu H, Sutton D, Randhawa K, et al. Are Passive Physical Modalities Effective for the Management of Common Soft Tissue Injuries of the Elbow? A Systematic Review by the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. The Clinical journal of pain. 2016.
• Fathy AA. Iontophoresis Versus Cyriax-Type exercises in Chronic Tennis Elbow among industrial workers. Electronic physician. 2015;7(5):1277-83.
• Fernandez-Carnero J, Cleland JA, Arbizu RL. Examination of motor and hypoalgesic effects of cervical vs thoracic spine manipulation in patients with lateral epicondylalgia: a clinical trial. Journal of manipulative and physiological therapeutics. 2011;34(7):432-40.
• Garg R, Adamson GJ, Dawson PA, Shankwiler JA, Pink MM. A prospective randomized study comparing a forearm strap brace versus a wrist splint for the treatment of lateral epicondylitis. Journal of shoulder and elbow surgery. 2010;19(4):508-12.
• Hoogvliet P, Randsdorp MS, Dingemanse R, Koes BW, Huisstede BM. Does effectiveness of exercise therapy and mobilisation techniques offer guidance for the treatment of lateral and medial epicondylitis? A systematic review. British journal of sports medicine. 2013;47(17):1112-9.
• Loew LM, Brosseau L, Tugwell P, Wells GA, Welch V, Shea B, et al. Deep transverse friction massage for treating lateral elbow or lateral knee tendinitis. The Cochrane database of systematic reviews. 2014(11):CD003528.
References• Peterson M, Butler S, Eriksson M, Svardsudd K. A randomized controlled trial of eccentric vs. concentric graded exercise in
chronic tennis elbow (lateral elbow tendinopathy). Clinical rehabilitation. 2014;28(9):862-72.
• Raman J, MacDermid JC, Grewal R. Effectiveness of different methods of resistance exercises in lateral epicondylosis--a systematic review. Journal of hand therapy : official journal of the American Society of Hand Therapists. 2012;25(1):5-25; quiz 6.
• Sevier TL, Stegink-Jansen CW. Astym treatment vs. eccentric exercise for lateral elbow tendinopathy: a randomized controlled clinical trial. PeerJ. 2015;3:e967.
• Sims SE, Miller K, Elfar JC, Hammert WC. Non-surgical treatment of lateral epicondylitis: a systematic review of randomized controlled trials. Hand. 2014;9(4):419-46.
• Smidt N, van der Windt DA, Assendelft WJ, Deville WL, Korthals-de Bos IB, Bouter LM. Corticosteroid injections, physiotherapy, or a wait-and-see policy for lateral epicondylitis: a randomised controlled trial. Lancet. 2002;359(9307):657-62.
• Sutton D, Gross DP, Cote P, Randhawa K, Yu H, Wong JJ, et al. Multimodal care for the management of musculoskeletal disorders of the elbow, forearm, wrist and hand: a systematic review by the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. Chiropractic & manual therapies. 2016;24:8.
• Vicenzino B, Smith D, Cleland J, Bisset L. Development of a clinical prediction rule to identify initial responders to mobilisation with movement and exercise for lateral epicondylalgia. Manual therapy. 2009;14(5):550-4.
• Weber C, Thai V, Neuheuser K, Groover K, Christ O. Efficacy of physical therapy for the treatment of lateral epicondylitis: a meta-analysis. BMC musculoskeletal disorders. 2015;16:223.
• Abrams RA, Tsai AM, Watson B, Jamali A, Lieber RL. Skeletal muscle recovery after tenotomy and 7-day delayed muscle length restoration. Muscle Nerve. 2000;23(5):707-14.
• Koh JS, Mohan PC, Howe TS, Lee BP, Chia SL, Yang Z, et al. Fasciotomy and surgical tenotomy for recalcitrant lateral elbow tendinopathy: early clinical experience with a novel device for minimally invasive percutaneous microresection. The American journal of sports medicine. 2013;41(3):636-44.
• Seng C, Mohan PC, Koh SB, Howe TS, Lim YG, Lee BP, et al. Ultrasonic Percutaneous Tenotomy for Recalcitrant Lateral Elbow Tendinopathy: Sustainability and Sonographic Progression at 3 Years. The American journal of sports medicine. 2016;44(2):504-10.
• Arirachakaran A, Sukthuayat A, Sisayanarane T, Laoratanavoraphong S, Kanchanatawan W, Kongtharvonskul J. Platelet-rich plasma versus autologous blood versus steroid injection in lateral epicondylitis: systematic review and network meta-analysis. Journal of orthopaedics and traumatology : official journal of the Italian Society of Orthopaedics and Traumatology. 2016;17(2):101-12.
• Balasubramaniam U, Dissanayake R, Annabell L. Efficacy of platelet-rich plasma injections in pain associated with chronic tendinopathy: A systematic review. The Physician and sportsmedicine. 2015;43(3):253-61.
References• Brkljac M, Kumar S, Kalloo D, Hirehal K. The effect of platelet-rich plasma injection on lateral epicondylitis following
failed conservative management. Journal of orthopaedics. 2015;12(Suppl 2):S166-70.
• Calandruccio JH, Steiner MM. Autologous Blood and Platelet-Rich Plasma Injections for Treatment of Lateral Epicondylitis. The Orthopedic clinics of North America. 2017;48(3):351-7.
• de Vos RJ, Weir A, Tol JL, Verhaar JA, Weinans H, van Schie HT. No effects of PRP on ultrasonographic tendon structure and neovascularisation in chronic midportion Achilles tendinopathy. Br J Sports Med. 2011;45(5):387-92.
• de Vos RJ, Windt J, Weir A. Strong evidence against platelet-rich plasma injections for chronic lateral epicondylar tendinopathy: a systematic review. British journal of sports medicine. 2014;48(12):952-6.
• Kaeding C, Best TM. Tendinosis: pathophysiology and nonoperative treatment. Sports health. 2009;1(4):284-92.
• Maffulli N, Longo UG, Denaro V. Novel approaches for the management of tendinopathy. The Journal of bone and joint surgery. American volume. 2010;92(15):2604-13.
• Mi B, Liu G, Zhou W, Lv H, Liu Y, Wu Q, et al. Platelet rich plasma versus steroid on lateral epicondylitis: meta-analysis of randomized clinical trials. The Physician and sportsmedicine. 2017;45(2):97-104.
Molloy T, Wang Y, Murrell G. The roles of growth factors in tendon and ligament healing. Sports Med. 2003;33(5):381-94.
• Murray DJ, Javed S, Jain N, Kemp S, Watts AC. Platelet-Rich-Plasma Injections in Treating Lateral Epicondylosis: a Review of the Recent Evidence. Journal of hand and microsurgery. 2015;7(2):320-5.
• Palacio EP, Schiavetti RR, Kanematsu M, Ikeda TM, Mizobuchi RR, Galbiatti JA. Effects of platelet-rich plasma on lateral epicondylitis of the elbow: prospective randomized controlled trial. Revista brasileira de ortopedia. 2016;51(1):90-5.
• Barnes DE, Beckley JM, Smith J. Percutaneous ultrasonic tenotomy for chronic elbow tendinosis: a prospective study. Journal of shoulder and elbow surgery. 2015;24(1):67-73.
• Barr S, Cerisola FL, Blanchard V. Effectiveness of corticosteroid injections compared with physiotherapeutic interventions for lateral epicondylitis: a systematic review. Physiotherapy. 2009;95(4):251-65.
• Bisset L, Beller E, Jull G, Brooks P, Darnell R, Vicenzino B. Mobilisation with movement and exercise, corticosteroid injection, or wait and see for tennis elbow: randomised trial. Bmj. 2006;333(7575):939-0.
• Murtezani A, Ibraimi Z, Vllasolli TO, Sllamniku S, Krasniqi S, Vokrri L. Exercise and Therapeutic Ultrasound Compared with Corticosteroid Injection for Chronic Lateral Epicondylitis: A Randomized Controlled Trial. Ortopedia, traumatologia, rehabilitacja. 2015;17(4):351-7.
• Olaussen M, Holmedal O, Mdala I, Brage S, Lindbaek M. Corticosteroid or placebo injection combined with deep transverse friction massage, Mills manipulation, stretching and eccentric exercise for acute lateral epicondylitis: a randomised, controlled trial. BMC musculoskeletal disorders. 2015;16:122
• Bialosky JE, Bishop MD, Price DD, Robinson ME, George SZ. The mechanisms of manual therapy in the treatment of musculoskeletal pain: a comprehensive model. Man Ther. 2009;14(5):531-8.