Embed Size (px)
Citation preview
Journal of Nursing & Interprofessional Leadership in Quality & Journal of Nursing & Interprofessional Leadership in Quality &
Safety Safety
Volume 2 Issue 1 Article 2
February 2018
Evidence-Based Skin Champion Program Reduces Evidence-Based Skin Champion Program Reduces
Pressure Injuries in a Pediatric Hospital Pressure Injuries in a Pediatric Hospital
Alexandra Luton MN, RN, NCNS-BC [email protected]
Mary D. Gordon PhD, RN, CNS-BC Texas Children's Hospital, [email protected]
Megnon Stewart MSN, RN Texas Children's Hospital, [email protected]
Ellena Steward-Scott MSN, RN Texas Children's Hospital, [email protected]
Joellan Mullen MSN, RN, CCRN-K Texas Children's Hospital, [email protected]
See next page for additional authors
Follow this and additional works at: https://digitalcommons.library.tmc.edu/uthoustonjqualsafe
Part of the Pediatric Nursing Commons
Recommended Citation Recommended Citation Luton, A., Gordon, M. D., Stewart, M., Steward-Scott, E., Mullen, J., Jones, A., & Hagan, J. (2018). Evidence-Based Skin Champion Program Reduces Pressure Injuries in a Pediatric Hospital. Journal of Nursing & Interprofessional Leadership in Quality & Safety, 2 (1). Retrieved from https://digitalcommons.library.tmc.edu/uthoustonjqualsafe/vol2/iss1/2
This article is free and open access to the full extent allowed by the CC BY NC-ND license governing this journal's content. For more details on permitted use, please see About This Journal.

Evidence-Based Skin Champion Program Reduces Pressure Injuries in a Pediatric Evidence-Based Skin Champion Program Reduces Pressure Injuries in a Pediatric Hospital Hospital
Abstract Abstract Prevention of pressure injuries (PIs) in pediatric patients is an important nurse-sensitive quality goal. The PI rate at a large urban pediatric hospital triggered a call to action by the Chief Nursing Officer to establish a Hospital Acquired PI (HAPI) Task Force which identified the Skin Champion program as a key improvement strategy. The goals of the Skin Champion program are to lower the rate of HAPIs, empower front line care providers to implement evidence-based care bundles, achieve consistency of practice, and provide resource availability at the point of care. The implementation of the Skin Champion quality improvement program achieved an 85% reduction in severe harm and “reportable" HAPI incidence, which is lower than the HAPI national average in pediatric patients (Solutions for Patient Safety, 2018), and an increase in nurse compliance with the HAPI prevention bundle. The HAPI incidence rate has remained near 0.05 per 1000 patient days.
Keywords Keywords Pressure injuries, Prevention, Pediatric, Skin Champion Program
Cover Page Footnote Cover Page Footnote Skin Champion Acknowledgement Special thanks to the Skin Champions, who accepted ownership of their practice and spread evidence based practices at the bedside. Their actions prevent numerous pressure injuries from occurring in our pediatric population and continue as strong practices today.
Authors Authors Alexandra Luton MN, RN, NCNS-BC; Mary D. Gordon PhD, RN, CNS-BC; Megnon Stewart MSN, RN; Ellena Steward-Scott MSN, RN; Joellan Mullen MSN, RN, CCRN-K; Angela Jones MN, RN, NE-BC; and Joseph Hagan ScD
This qi report/quality improvement study is available in Journal of Nursing & Interprofessional Leadership in Quality & Safety: https://digitalcommons.library.tmc.edu/uthoustonjqualsafe/vol2/iss1/2

Introduction
Problem Description
Prevention of pressure injuries (PIs) in pediatric patients is an important nurse-sensitive quality
goal because achievement of the goal depends in part on the quantity and quality of nursing care provided
to the patient ("SPS Pressure injury prevention bundle elements," 2018). Preventable PIs still occur in
pediatric patients and frequently cause pain and disfigurement. The national pediatric PI prevalence
rates are reported to be 0% to 7.3% (Baharestani, 2007; Baldwin, 2002; Razmus, 2017; Waterlow, 1997;
Willock, 2000). PI prevention is an important nursing function and incidence/prevalence rates are used
to benchmark quality of nursing care across healthcare organizations. In September 2013, the PI rate at
a large urban pediatric hospital increased to 0.45/1000 patient days. A call to action by the Chief Nursing
Officer established a Hospital Acquired PI (HAPI) Task Force which identified the Skin Champion program
as a key intervention.
Available Knowledge
Pressure injuries are a common occurrence in hospitals across the nation. Although some pressure
injuries may be unavoidable, it is possible to reduce the overall level of patient harm caused by such
injuries through early detection and intervention. Baharestani (2007) described pressure injury incidence
rates in neonatal and pediatric intensive care units to be as high as 23% -27%. Hospitals have a financial
incentive to improve care and patient outcomes now that CMS no longer reimburses hospitals for
treatment of hospital-acquired pressure injuries (HAPI) (Centers for Medicare & Medicaid Services, 2008).
The change in reimbursement shifts the responsibility of pressure injury prevention to health care
organizations, thereby incentivizing pressure injury prevention activities. Hospitals started to prioritize
and support pressure injury prevention practices and teams to improve processes and outcomes.
Review of Literature
A review of successful Skin Champion programs identified critical program components that
contributed to success and sustainability. The teams responsible for design and implementation of Skin
Champion programs are multidisciplinary and include many combinations of nurses and nurses’ aides,
wound experts, executive leadership, educators, and Advanced Practice Nurses, to name a few
(Niederhauser et al., 2012). It is important to identify and include stakeholders early in the planning
process so they have an opportunity to participate in program discussions (Ahroni, 2014; Visscher, 2013).
A pressure injury prevention program dedicated to improving patient safety outcomes must involve
middle and top leaders in the organization and align with organizational priorities. It is key that quality
improvement processes be included to evaluate the continuous performance of team (Kelleher, Moorer,
& Makic, 2012; Visscher, 2013; Wang, 2006).
An important first step in Skin Champion program design is to find a unique and recognizable
name for the group to communicate a consistent identity. The name should communicate the primary
function, role or purpose of the group and solidify the identity of the team. Additional suggestions
include using shirts, vests or jackets to aide in program recognition while pressure injury prevention staff
are on clinical units (Ahroni, 2014).
The success of a Skin Champion program requires a strong infrastructure to support the Champion
role. The program needs a house-wide policy and procedure that clarifies the evidence and best practices
for pressure prevention and routines of care. Also, there is need for a continuing education program to
teach skin anatomy, PI risk assessment, pressure relief interventions, interdisciplinary involvement, and
products to support clinical care goals (Ahroni, 2014; Bergquist-Beringer, Derganc, & Dunton, 2009). Best
1
Luton et al.: Skin Champion Program Reduces Pressure Injuries
Published by the Baylor College of Medicine, Division of Academic General Pediatrics, 2018
practices are bundled and used as a prevention intervention package for all staff. Ongoing clinical
monitoring of bundle compliance is recommended to ensure compliance with existing prevention
interventions, and to encourage behavior changes. Bundle compliance can be checked by rounding on
high-risk patients and completing chart audits. Frequent sharing of compliance data with leadership and
clinical staff will facilitate progress toward achieving the goal (Bergquist-Beringer et al., 2009; Kelleher
et al., 2012; Niederhauser et al., 2012; Sullivan & Schoelles, 2013; Visscher, 2013).
Skin Champion roles and responsibilities should be made clear during the recruitment process
(Pasek et al., 2008). Common descriptions of the role include involvement with prevalence studies,
rounding, and monthly chart audits. The Champions are considered to be content experts who promote
prevention interventions with their peers. They are familiar with hospital skin care resources, as well as
PI prevention products and devices. Skin Champions also work as a mentor and educator to others in the
unit (Bergquist-Beringer et al., 2009; Niederhauser et al., 2012; Pasek et al., 2008; Rodgers, 2014) and
employ strategies to generate enthusiasm and increase awareness about the new program to ensure staff
engagement, ownership and dedication. Providing real-time data in staff meetings or newsletters and
giving staff/team recognition for the improvements made are a few suggestions. Celebrating each success
also stimulates healthy competition among units and provides a sense of pride in their accomplishments
(Bergquist-Beringer et al., 2009; Niederhauser et al., 2012).
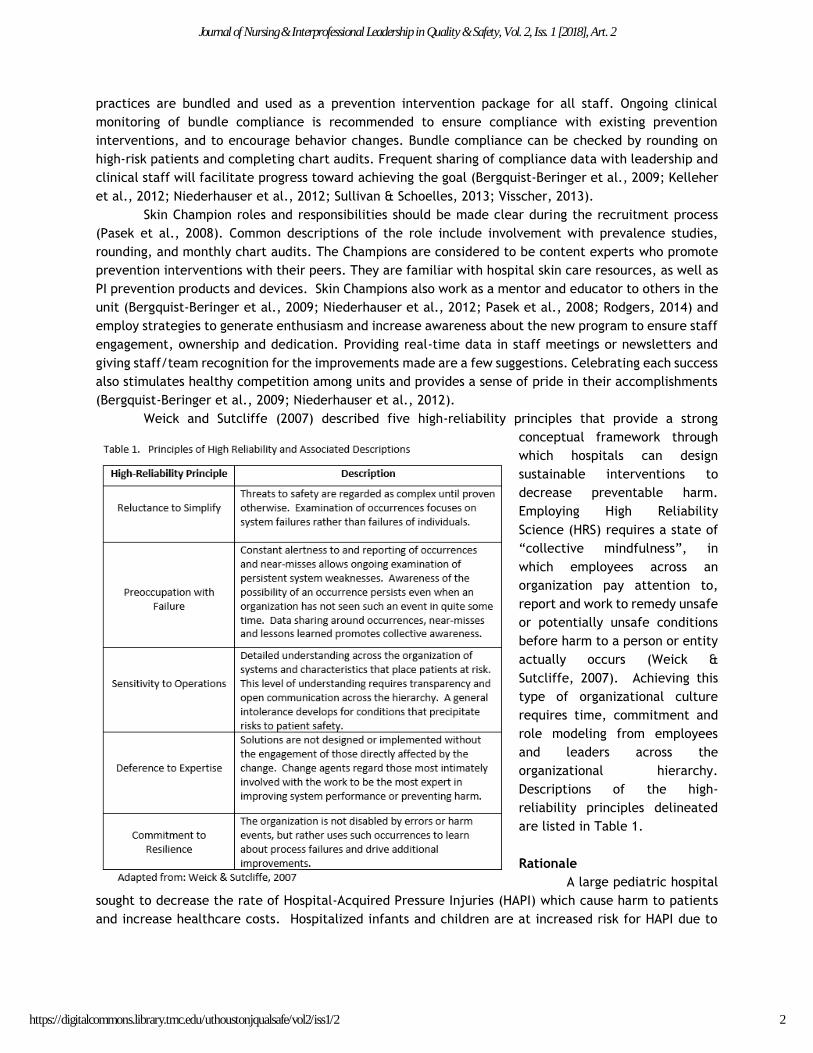
Weick and Sutcliffe (2007) described five high-reliability principles that provide a strong
conceptual framework through
which hospitals can design
sustainable interventions to
decrease preventable harm.
Employing High Reliability
Science (HRS) requires a state of
“collective mindfulness”, in
which employees across an
organization pay attention to,
report and work to remedy unsafe
or potentially unsafe conditions
before harm to a person or entity
actually occurs (Weick &
Sutcliffe, 2007). Achieving this
type of organizational culture
requires time, commitment and
role modeling from employees
and leaders across the
organizational hierarchy.
Descriptions of the high-
reliability principles delineated
are listed in Table 1.
Rationale
A large pediatric hospital
sought to decrease the rate of Hospital-Acquired Pressure Injuries (HAPI) which cause harm to patients
and increase healthcare costs. Hospitalized infants and children are at increased risk for HAPI due to
2
Journal of Nursing & Interprofessional Leadership in Quality & Safety, Vol. 2, Iss. 1 [2018], Art. 2
https://digitalcommons.library.tmc.edu/uthoustonjqualsafe/vol2/iss1/2

both inherent and iatrogenic factors. Table 2 outlines inherent and acquired risk factors for skin
breakdown in hospitalized infants and children.
In an effort to achieve sustainable improvements in HAPI rate, we formed an interprofessional
task force with executive support
to reduce HAPI. The task force
sought to employ tenets of HRS in
designing and implementing
solutions (Chassin, 2013).
Specific Aims
The primary aim of the
HAPI Reduction Task Force
initiative was to decrease the
number of severe-harm HAPI by
20% in targeted areas by the
conclusion of each fiscal year.
Methods
Context
The project took place in a large pediatric hospital with an annual volume of 3.3 million patient
encounters and over 32,000 admissions. The patient population encompasses a diverse mix of chronic
and acutely ill patients. It is a Magnet® organization, recognized since 2003 for nursing excellence by
the American Nurses Credentialing Center (ANCC). The contextual elements of the program include a
Skin Champion team composed of caregivers who are passionate about PI prevention and strive to know
more about how they can influence a decrease in the pressure injury rates. Executive leadership supports
progress of the Skin Champion team and a strong multidisciplinary faculty who are content experts that
partner with nursing to grow the Skin Champion team.
The program supports the continuing education of the Champions. An educational calendar is
planned every six months so that content for monthly meetings included could be tailored to meet
specific learning needs. A four-hour pressure injury prevention course is provided annually as a refresher
for existing Champions and a requirement for new Champions. The faculty prepares slides for each
Champion meeting to discuss pressure injuries that occurred during the past month and recommend
interventions to prevent another similar occurrence. PI prevention bundle compliance for each unit is
discussed in detail as well as identified barriers toward goal achievement and improvement strategies.
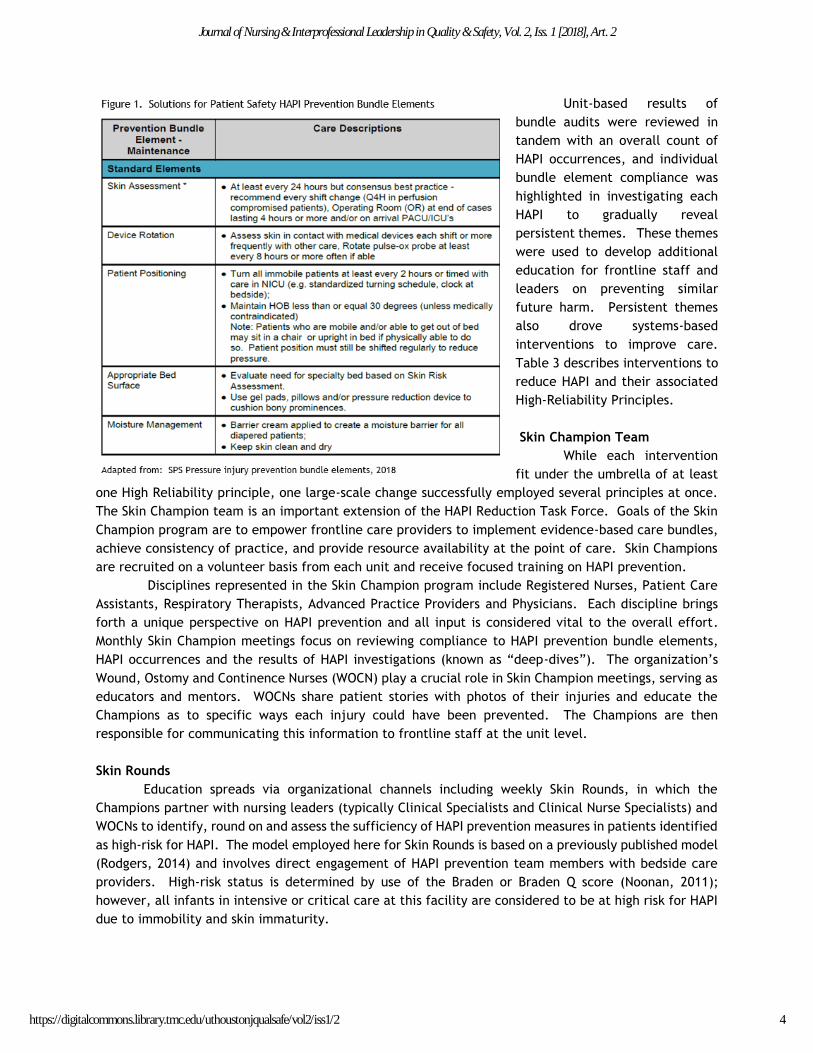
Interventions
The HAPI Reduction Task Force implemented system-based changes that would sustain regardless
of personnel availability, ongoing training, or patient acuity. Interventions tied directly to High
Reliability Principles and focused on first gaining understanding of patients’ inherent and acquired risk
factors. The organization then employed prevention measures in accordance with those required by the
Solutions for Patient Safety Collaborative, subsequently auditing and reporting adherence to the “HAPI
Prevention Bundle” of care practices (Figure 1), with the goal of achieving compliance to the bundle of
at least 90%.
3
Luton et al.: Skin Champion Program Reduces Pressure Injuries
Published by the Baylor College of Medicine, Division of Academic General Pediatrics, 2018
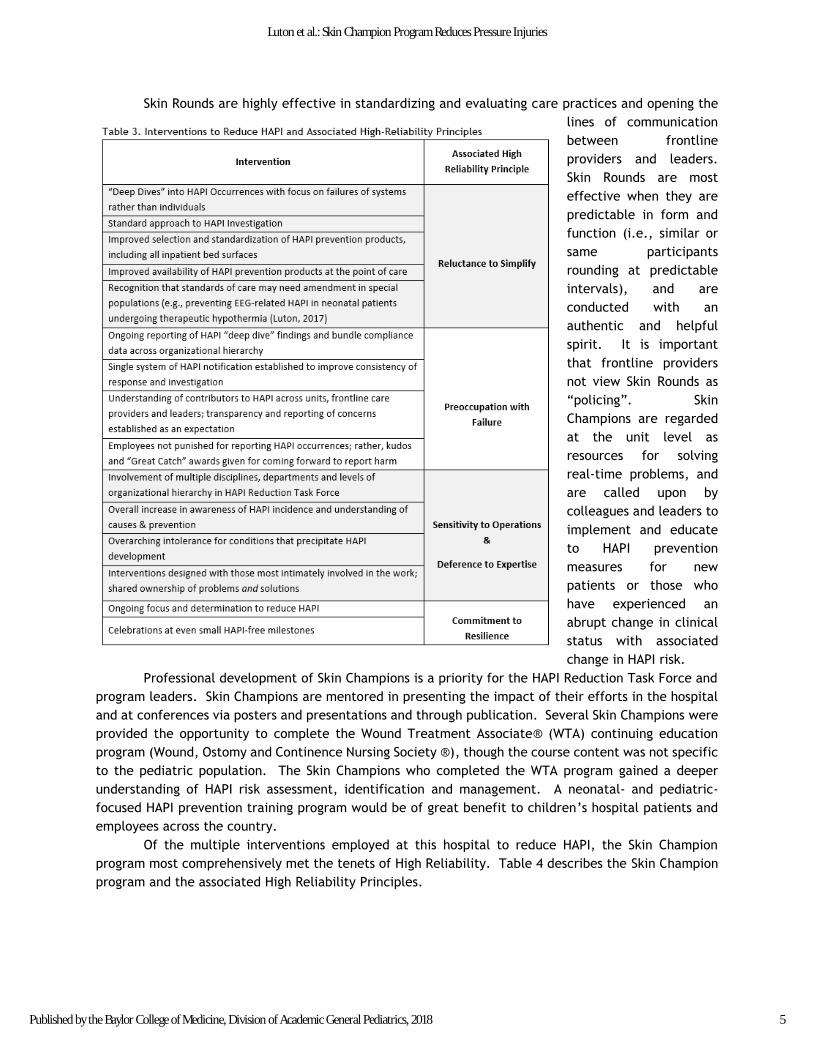
Unit-based results of
bundle audits were reviewed in
tandem with an overall count of
HAPI occurrences, and individual
bundle element compliance was
highlighted in investigating each
HAPI to gradually reveal
persistent themes. These themes
were used to develop additional
education for frontline staff and
leaders on preventing similar
future harm. Persistent themes
also drove systems-based
interventions to improve care.
Table 3 describes interventions to
reduce HAPI and their associated
High-Reliability Principles.
Skin Champion Team
While each intervention
fit under the umbrella of at least
one High Reliability principle, one large-scale change successfully employed several principles at once.
The Skin Champion team is an important extension of the HAPI Reduction Task Force. Goals of the Skin
Champion program are to empower frontline care providers to implement evidence-based care bundles,
achieve consistency of practice, and provide resource availability at the point of care. Skin Champions
are recruited on a volunteer basis from each unit and receive focused training on HAPI prevention.
Disciplines represented in the Skin Champion program include Registered Nurses, Patient Care
Assistants, Respiratory Therapists, Advanced Practice Providers and Physicians. Each discipline brings
forth a unique perspective on HAPI prevention and all input is considered vital to the overall effort.
Monthly Skin Champion meetings focus on reviewing compliance to HAPI prevention bundle elements,
HAPI occurrences and the results of HAPI investigations (known as “deep-dives”). The organization’s
Wound, Ostomy and Continence Nurses (WOCN) play a crucial role in Skin Champion meetings, serving as
educators and mentors. WOCNs share patient stories with photos of their injuries and educate the
Champions as to specific ways each injury could have been prevented. The Champions are then
responsible for communicating this information to frontline staff at the unit level.
Skin Rounds
Education spreads via organizational channels including weekly Skin Rounds, in which the
Champions partner with nursing leaders (typically Clinical Specialists and Clinical Nurse Specialists) and
WOCNs to identify, round on and assess the sufficiency of HAPI prevention measures in patients identified
as high-risk for HAPI. The model employed here for Skin Rounds is based on a previously published model
(Rodgers, 2014) and involves direct engagement of HAPI prevention team members with bedside care
providers. High-risk status is determined by use of the Braden or Braden Q score (Noonan, 2011);
however, all infants in intensive or critical care at this facility are considered to be at high risk for HAPI
due to immobility and skin immaturity.
4
Journal of Nursing & Interprofessional Leadership in Quality & Safety, Vol. 2, Iss. 1 [2018], Art. 2
https://digitalcommons.library.tmc.edu/uthoustonjqualsafe/vol2/iss1/2
Skin Rounds are highly effective in standardizing and evaluating care practices and opening the
lines of communication
between frontline
providers and leaders.
Skin Rounds are most
effective when they are
predictable in form and
function (i.e., similar or
same participants
rounding at predictable
intervals), and are
conducted with an
authentic and helpful
spirit. It is important
that frontline providers
not view Skin Rounds as
“policing”. Skin
Champions are regarded
at the unit level as
resources for solving
real-time problems, and
are called upon by
colleagues and leaders to
implement and educate
to HAPI prevention
measures for new
patients or those who
have experienced an
abrupt change in clinical
status with associated
change in HAPI risk.
Professional development of Skin Champions is a priority for the HAPI Reduction Task Force and
program leaders. Skin Champions are mentored in presenting the impact of their efforts in the hospital
and at conferences via posters and presentations and through publication. Several Skin Champions were
provided the opportunity to complete the Wound Treatment Associate® (WTA) continuing education
program (Wound, Ostomy and Continence Nursing Society ®), though the course content was not specific
to the pediatric population. The Skin Champions who completed the WTA program gained a deeper
understanding of HAPI risk assessment, identification and management. A neonatal- and pediatric-
focused HAPI prevention training program would be of great benefit to children’s hospital patients and
employees across the country.
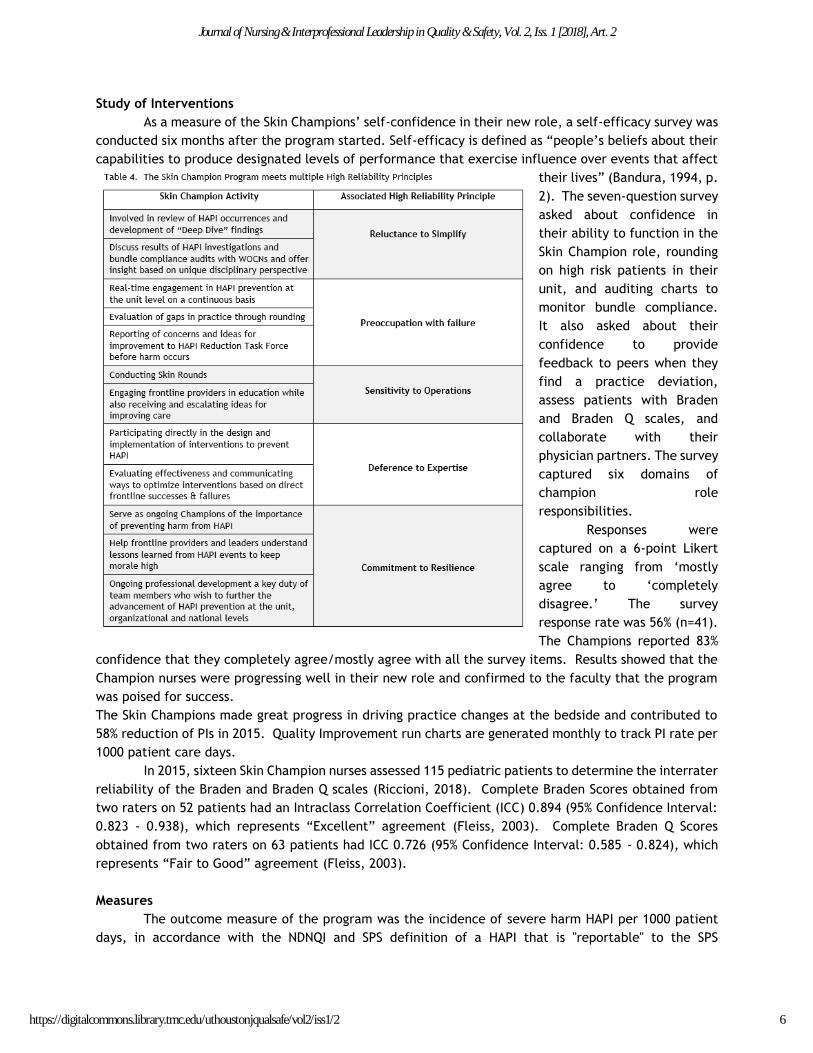
Of the multiple interventions employed at this hospital to reduce HAPI, the Skin Champion
program most comprehensively met the tenets of High Reliability. Table 4 describes the Skin Champion
program and the associated High Reliability Principles.
5
Luton et al.: Skin Champion Program Reduces Pressure Injuries
Published by the Baylor College of Medicine, Division of Academic General Pediatrics, 2018
Study of Interventions
As a measure of the Skin Champions’ self-confidence in their new role, a self-efficacy survey was
conducted six months after the program started. Self-efficacy is defined as “people’s beliefs about their
capabilities to produce designated levels of performance that exercise influence over events that affect
their lives” (Bandura, 1994, p.
2). The seven-question survey
asked about confidence in
their ability to function in the
Skin Champion role, rounding
on high risk patients in their
unit, and auditing charts to
monitor bundle compliance.
It also asked about their
confidence to provide
feedback to peers when they
find a practice deviation,
assess patients with Braden
and Braden Q scales, and
collaborate with their
physician partners. The survey
captured six domains of
champion role
responsibilities.
Responses were
captured on a 6-point Likert
scale ranging from ‘mostly
agree to ‘completely
disagree.’ The survey
response rate was 56% (n=41).
The Champions reported 83%
confidence that they completely agree/mostly agree with all the survey items. Results showed that the
Champion nurses were progressing well in their new role and confirmed to the faculty that the program
was poised for success.
The Skin Champions made great progress in driving practice changes at the bedside and contributed to
58% reduction of PIs in 2015. Quality Improvement run charts are generated monthly to track PI rate per
1000 patient care days.
In 2015, sixteen Skin Champion nurses assessed 115 pediatric patients to determine the interrater
reliability of the Braden and Braden Q scales (Riccioni, 2018). Complete Braden Scores obtained from
two raters on 52 patients had an Intraclass Correlation Coefficient (ICC) 0.894 (95% Confidence Interval:
0.823 - 0.938), which represents “Excellent” agreement (Fleiss, 2003). Complete Braden Q Scores
obtained from two raters on 63 patients had ICC 0.726 (95% Confidence Interval: 0.585 - 0.824), which
represents “Fair to Good” agreement (Fleiss, 2003).
Measures
The outcome measure of the program was the incidence of severe harm HAPI per 1000 patient
days, in accordance with the NDNQI and SPS definition of a HAPI that is "reportable" to the SPS
6
Journal of Nursing & Interprofessional Leadership in Quality & Safety, Vol. 2, Iss. 1 [2018], Art. 2
https://digitalcommons.library.tmc.edu/uthoustonjqualsafe/vol2/iss1/2
Collaborative (those classified by a WOCN as a Stage 3, Stage 4 or Unstageable HAPI). It is important to
note that Deep Tissue Injuries (DTI) were considered "reportable" to SPS until January 15, 2015, at which
point these injuries were deemed "reportable" only if they progressed to a Stage 3, Stage 4 or Unstageable
HAPI (Safety, 2015). Our data were amended to retroactively reflect the change in definition.
Analysis
A U-chart was used to display the reportable HAPI incidence over time. The u-chart is a statistical
process control chart that displays a rate over time where the rate is quantified by the number of events
of interest divided by the “area of opportunity” for the events to occur. For this project the monthly
reportable HAPI rate per 1000 patient days was displayed in the U-chart.
Results
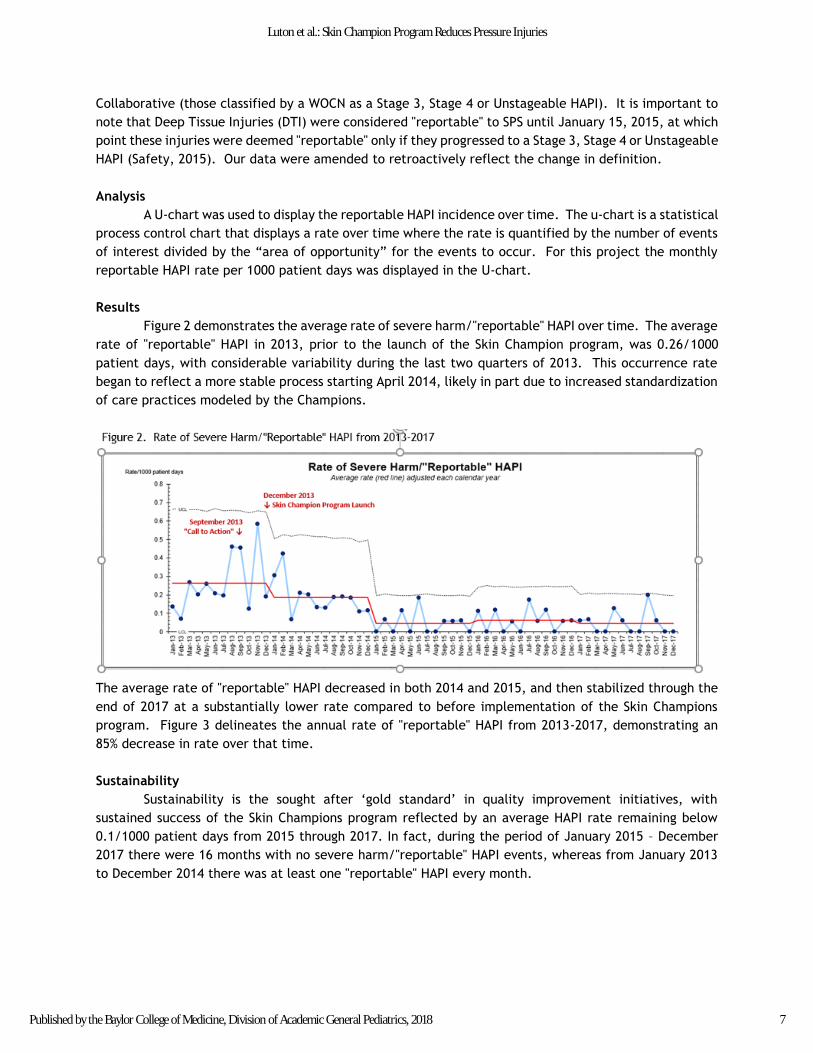
Figure 2 demonstrates the average rate of severe harm/"reportable" HAPI over time. The average
rate of "reportable" HAPI in 2013, prior to the launch of the Skin Champion program, was 0.26/1000
patient days, with considerable variability during the last two quarters of 2013. This occurrence rate
began to reflect a more stable process starting April 2014, likely in part due to increased standardization
of care practices modeled by the Champions.
The average rate of "reportable" HAPI decreased in both 2014 and 2015, and then stabilized through the
end of 2017 at a substantially lower rate compared to before implementation of the Skin Champions
program. Figure 3 delineates the annual rate of "reportable" HAPI from 2013-2017, demonstrating an
85% decrease in rate over that time.
Sustainability
Sustainability is the sought after ‘gold standard’ in quality improvement initiatives, with
sustained success of the Skin Champions program reflected by an average HAPI rate remaining below
0.1/1000 patient days from 2015 through 2017. In fact, during the period of January 2015 – December
2017 there were 16 months with no severe harm/"reportable" HAPI events, whereas from January 2013
to December 2014 there was at least one "reportable" HAPI every month.
7
Luton et al.: Skin Champion Program Reduces Pressure Injuries
Published by the Baylor College of Medicine, Division of Academic General Pediatrics, 2018
Discussion
Summary and Future Direction
The implementation of the Skin Champions noted a significant reduction in severe
harm/"reportable" HAPI and an increase in prevention bundle compliance. The results are attributable
to systems-based changes and the commitment made by the HAPI Reduction Task Force, executive
leaders, Skin Champion Faculty, and Skin Champions to have a successful program. The Skin Champion
program at this facility has been instrumental in bringing prevention measures to the bedside. Champions
adapt care management processes that achieve effective and safe care and mobilize their colleagues’
involvement (Bergquist-Beringer et al., 2009). The program centers around ongoing education of Skin
Champions on assessment, prevention, products, and treatment to manage PI.
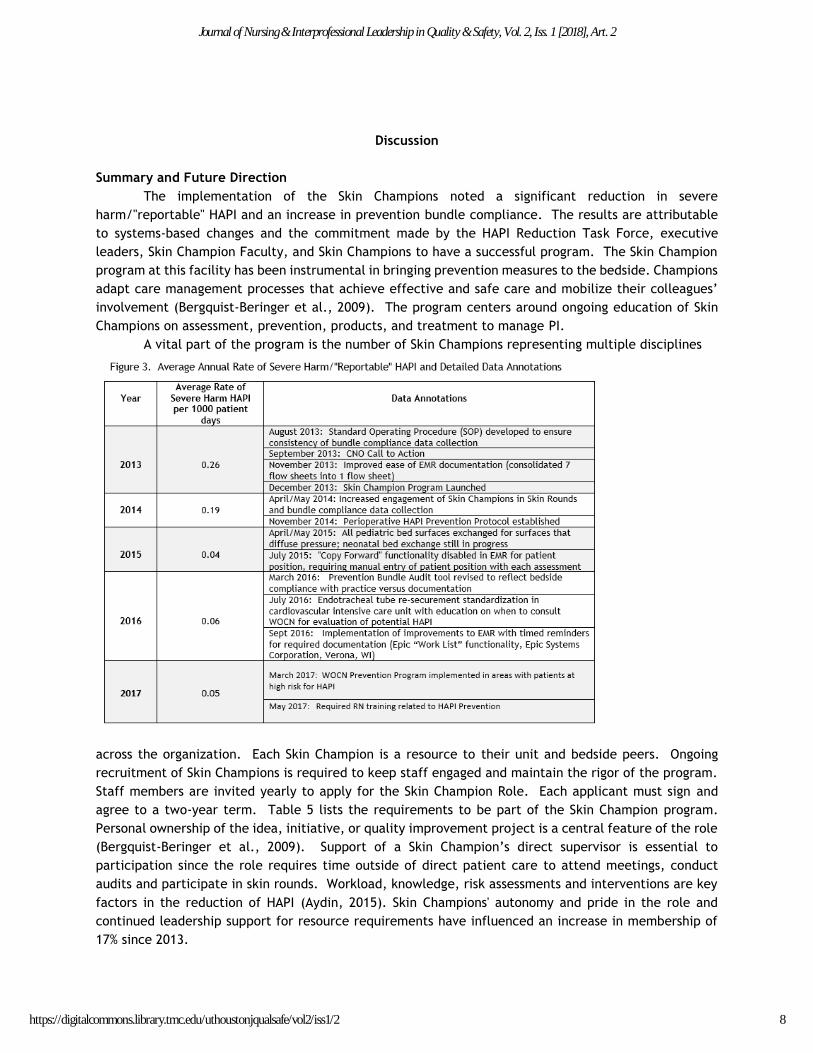
A vital part of the program is the number of Skin Champions representing multiple disciplines
across the organization. Each Skin Champion is a resource to their unit and bedside peers. Ongoing
recruitment of Skin Champions is required to keep staff engaged and maintain the rigor of the program.
Staff members are invited yearly to apply for the Skin Champion Role. Each applicant must sign and
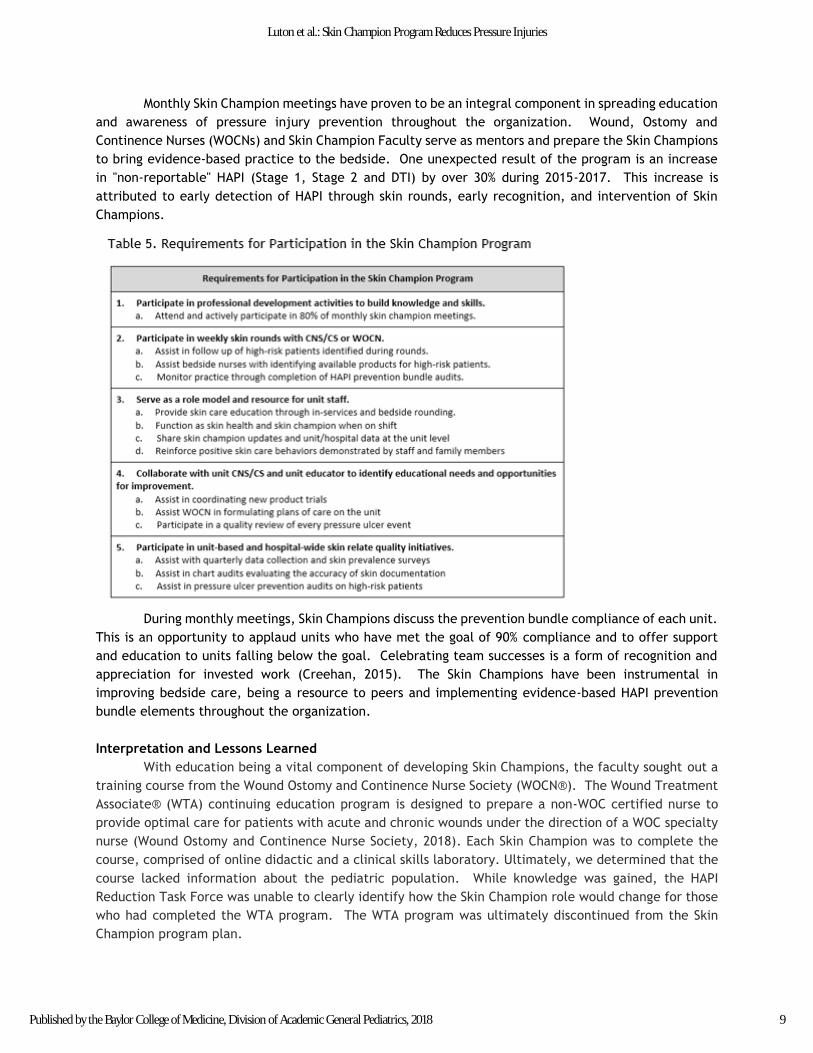
agree to a two-year term. Table 5 lists the requirements to be part of the Skin Champion program.
Personal ownership of the idea, initiative, or quality improvement project is a central feature of the role
(Bergquist-Beringer et al., 2009). Support of a Skin Champion’s direct supervisor is essential to
participation since the role requires time outside of direct patient care to attend meetings, conduct
audits and participate in skin rounds. Workload, knowledge, risk assessments and interventions are key
factors in the reduction of HAPI (Aydin, 2015). Skin Champions' autonomy and pride in the role and
continued leadership support for resource requirements have influenced an increase in membership of
17% since 2013.
8
Journal of Nursing & Interprofessional Leadership in Quality & Safety, Vol. 2, Iss. 1 [2018], Art. 2
https://digitalcommons.library.tmc.edu/uthoustonjqualsafe/vol2/iss1/2
Monthly Skin Champion meetings have proven to be an integral component in spreading education
and awareness of pressure injury prevention throughout the organization. Wound, Ostomy and
Continence Nurses (WOCNs) and Skin Champion Faculty serve as mentors and prepare the Skin Champions
to bring evidence-based practice to the bedside. One unexpected result of the program is an increase
in "non-reportable" HAPI (Stage 1, Stage 2 and DTI) by over 30% during 2015-2017. This increase is
attributed to early detection of HAPI through skin rounds, early recognition, and intervention of Skin
Champions.
During monthly meetings, Skin Champions discuss the prevention bundle compliance of each unit.
This is an opportunity to applaud units who have met the goal of 90% compliance and to offer support
and education to units falling below the goal. Celebrating team successes is a form of recognition and
appreciation for invested work (Creehan, 2015). The Skin Champions have been instrumental in
improving bedside care, being a resource to peers and implementing evidence-based HAPI prevention
bundle elements throughout the organization.
Interpretation and Lessons Learned
With education being a vital component of developing Skin Champions, the faculty sought out a
training course from the Wound Ostomy and Continence Nurse Society (WOCN®). The Wound Treatment
Associate® (WTA) continuing education program is designed to prepare a non-WOC certified nurse to
provide optimal care for patients with acute and chronic wounds under the direction of a WOC specialty
nurse (Wound Ostomy and Continence Nurse Society, 2018). Each Skin Champion was to complete the
course, comprised of online didactic and a clinical skills laboratory. Ultimately, we determined that the
course lacked information about the pediatric population. While knowledge was gained, the HAPI
Reduction Task Force was unable to clearly identify how the Skin Champion role would change for those
who had completed the WTA program. The WTA program was ultimately discontinued from the Skin
Champion program plan.
9
Luton et al.: Skin Champion Program Reduces Pressure Injuries
Published by the Baylor College of Medicine, Division of Academic General Pediatrics, 2018

Additional lessons have been learned about maintaining competency and engagement of the
senior Skin Champions. With success of the program, a majority of the Skin Champions continue
involvement beyond the initial two-year commitment. To keep them engaged, two additional
components were added to the monthly meetings; a "product of the month" item and unit-based "deep-
dive" into a HAPI occurrence. Each month a vendor or a WOCN presents a product related to skin and
wound care. A unit-based Clinical Specialist or Clinical Nurse Specialist presents the findings of a deep-
dive investigation into any severe-harm/"reportable" HAPI that occurred on the unit, with a focus on
missed opportunities for prevention. Both additions empower the Skin Champions to proactively engage
in product review and research and take preventive measures back to the bedside.
Limitations
We noted a lack of supplemental educational resources focused on pediatric patients. Thus, the
content experts at the hospital developed a HAPI Prevention Course for Pediatric Patients. It requires
financial support, time and personnel to successfully execute on an annual basis.
Conclusion
Since the implementation of the Skin Champion program in 2013, the HAPI rate has decreased by
85%. The rate has remained near 0.05/1000 patient days, which is lower than the HAPI national average
in pediatric patients (Solutions for Patient Safety, 2018). The program is sustainable because the Skin
Champion team remains strong with active participation from several disciplines, and much of the team’s
success can be attributed to leadership support at the organizational level as well as at the unit level.
Support is provided as protected time for meetings and education, financial support for educational
endeavors, as well as physical presence and interaction with the Champion team members while on the
unit and in meetings. The Champion model is useful for other hospital acquired condition reduction
initiatives. The facility’s central line associated bloodstream infections (CLABSI) and peripheral
intravenous infiltration and extravasations (PIVIE) Champion groups have demonstrated similar successful
outcomes.
References
Ahroni, J. (2014). Developing a wound and skin care program. Journal of Wound Ostomy & Continence
Nursing 41(6), 549-555.
Aydin, C., Donaldson, N., Stotts, N. A., Fridman, M., & Brown, D. S. . (2015). Modeling hospital-acquired
pressure ulcer prevalence on medical-surgical units: Nurse workload, expertise, and clinical
processes of care. Health Services Research 50, 19-24.
Baharestani, M., & Ratliff, C. R. (2007). Pressure ulers in neonates and children: An NPUAP white paper.
Advances in Skin & Wound Care 20(4), 208-220.
Baldwin, K. (2002). Incidence and prevalence of pressure ulcers in children. Advances in Skin & Wound
Care 15(3), 121-124.
Bandura, A. (1994).Self-efficacy. In V. S. Ramachaudran (Ed.), Encyclopedia of human behavior (Vol. 4,
pp. 71-81). New York: Academic Press. (Reprinted in H. Friedman [Ed.], Encyclopedia of mental
health. San Diego: Academic Press, 1998).
Bergquist-Beringer, S., Derganc, K., & Dunton, N. (2009). Embracing the use of skin care champions.
Nursing Management, December, 19-23.
Chassin, M.,& Loeb, J. M. (2013). High reliability health care: Getting there from here. The Milbank
Quarterly, 91(3), 459-490.
10
Journal of Nursing & Interprofessional Leadership in Quality & Safety, Vol. 2, Iss. 1 [2018], Art. 2
https://digitalcommons.library.tmc.edu/uthoustonjqualsafe/vol2/iss1/2
Creehan, S. (2015). Building nursing unit staff champion programs to improve clinical outcomes. Nurse
Leader 13(4), 31-35.
Fleiss, J. L., Levin, B., & Paik, M.C. (2003). Statistical Methods for Rates and Proportions (3rd ed.).
Hoboken, NJ: John Wiley & Sons.
Kelleher, A., Moorer, A., & Makic, M. (2012). Hospital-acquired pressure ulcer prevalence in a surgical
intensive care unit. Journal of Wound Ostomy & Continence Nursing 39(2), 152-157.
Luton, A., Hernandez, J., Patterson, C, Neilsen-Farrell, J, Thompson, A,& Kaiser, J. (2017). Preventing
pressure injuries for neonates undergoing therapeutic hypothermia for hypoxic ischemic
encephalopathy: An interprofessional quality improvement project. Advances in Neonatal Care
17(4), 237-244.
Niederhauser, A., Lukas, C., Parker, V., Ayello, E., Zulkowski, K., & Berlowitz, D. (2012). Comprehensive
programs for preventing pressure ulcers: A review of the literature. Advances in Skin and Wound
Care 25(4), 167-188.
Noonan, C., Quigley, S, & Curley, M. A. Q. (2011). Using the braden q scale to predict pressure ulcer risk
in pediatric patients. Journal of Pediatric Nursing 26(6), 566-575.
Pasek, T. A., Geyser, A., Sidoni, M., Harris, P., Warner, J., Spence, A., . . . Weicheck, S. (2008). Skin
care team in the pediatric intensive care unit: A model for excellence. Critical Care Nurse 28(2),
125-135.
Razmus, I., & Bergquist-Beringer, S. (2017). Pressure injury prevalence and the rate of hospital-acquired
pressure injury among pediatric patients in acute care. Journal of Wound Ostomy & Continence
Nursing 44(2), 110-117.
Riccioni, N., Berlanga, R, Hagan, J, Schier, R, & Gordon, M. (2019). Interrater reliability of the Braden
and Braden Q by skin champion nurses. Journal of Pediatric Nursing 44, 9-15.
Rodgers, E., Nist, M.; Gardikes-Gingery, R., Shepherd, E., Ruth, B., & Keller, L. (2014). Skin rounds: A
standardized approach to pressure injury detection and reporting in the neonatal intensive care
unit. Journal of Obstetric, Gynecologic & Neonatal Nursing 43 (Supp 1), S29-30.
Safety, O. C. S. H. S. F. P. (2015). Operational Definition Measurement Pressure Ulcers. Retrieved from
http://www.solutionsforpatientsafety.org/wp-content/uploads/sps-operating-definitions.pdf
SPS Pressure injury prevention bundle elements. (2018). Solutions for Patient Safety. Retrieved from
http://www.solutionsforpatientsafety.org/wp-content/uploads/SPS-Prevention-Bundles.pdf
Sullivan, N., & Schoelles, K. (2013). Preventing in-facility pressure ulcers as a patient safety strategy.
Annals of Internal Medicine 158(5), Supplement.
Visscher, M., King, A., Nie, A., Schaffer, P., Taylor, T., Pruitt, D., … Keswani, S. (2013). A quality
improvement collaborative project to reduce pressure ulcers in PICUs. Pediatrics 131(6), e1950-
e1960.
Wang, M., Hyun, J.K., Harrison, M., Shortell, S.M., & Fraser, I. (2006). Redesigning health systems for
quality: Lessons from emerging practices. Joint Commision Journal on Quality and Patient Safety
32(11), 599-611.
Waterlow, J. (1997). Pressure sore risk assessment in children. Paediatric Nursing 9(6), 21-24.
Weick, K., & Sutcliffe, K. (2007). Preventing Pressure Injuries for Neonates Undergoing Therapeutic
Hypothermia for Hypoxic Ischemic Encephalopathy: An Interprofessional Quality Improvement
Project (Vol. 2nd edition). San Francisco: John Wiley &Sons, Inc.
Willock, J., Hughes, J, Tickel, S, Rossiter, G, Johnson, C, & Pye, H. (2000). Pressure sores in children:
The acute hospital perspective. Journal of Tissue Viability 10(2), 59-62.
11
Luton et al.: Skin Champion Program Reduces Pressure Injuries
Published by the Baylor College of Medicine, Division of Academic General Pediatrics, 2018





























