Embed Size (px)
Citation preview
04/04/2016
1
Matthew Caster PT, DPT, OCS
Allegheny Chesapeake Physical Therapy
Evidence Based Treatment of the
Lumbar Spine
Objectives
Discuss incidence, prevalence and economic impact of low
back pain
Discuss current guidelines and classification systems
Present current updated Treatment Based Classification
System (TBC)
Case examples
LBP defined
Pain, stiffness or muscle tension below the costal margin and
above the inferior gluteal folds
Can be with or without leg pain
Chronicity
Acute < 6 weeks
Sub-acute 6 to 12 weeks
Chronic > 12 weeks
04/04/2016
2
LBP
Common disorder that is a burden to individuals and society
Lifetime prevalence approximately 84%
60 to 80% of Americans will suffer an episode of LBP
resulting in loss of work
Economic Impact
USA: annual cost over $50 billion
Low Back Pain
Non-Mechanical
Prevalence 3%
Mechanical
Prevalence 97%
Pathologies
Red Flag / Non-mechanical (prevalence 1%)
Neoplasia
Infection
Inflammatory arthritis
Paget and Scheumerman disease
Jarvik and Deyo. Diagnostic Evaluation of Low Back Pain with Emphasis on Imaging. Annals of Internal Medicine
2002; 137: 586-597.
04/04/2016
3
Pathologies
Red Flag / Visceral (prevalence 2%)
Aortic aneurysm
Pelvic
Renal
GI
Jarvik and Deyo. Diagnostic Evaluation of Low Back Pain with Emphasis on Imaging. Annals of Internal Medicine
2002; 137: 586-597.
Pathologies
Mechanical LBP (prevalence 97%)
Strain
DDD / facet
Herniated disc
Stenosis
FX
Spondy
Congenital
Instability
Jarvik and Deyo. Diagnostic Evaluation of Low Back Pain with Emphasis on Imaging. Annals of Internal Medicine
2002; 137: 586-597.
Approximately 85% of patients are unable to be given a
specific structurally based (patho-anatomic) diagnosis
“Non-specific low back pain”
How can we effectively treat this large group?
Deyo RA, Phillips WR. Low back pain: a primary care challenge. Spine (Phila Pa 1976) 1996;21:2826-32.
04/04/2016
4
Guidelines vs Classification Systems
Guidelines
Summary of available evidence
Developed from a clinical perspective
Classification Systems
Match treatments to patient sub-groups using a clinically driven
decision making process
American College of Physicians &
American Pain Society Acute LBP
Spinal Manipulation
Chronic / sub-acute LBP Interdisciplinary rehabilitation Exercise therapy Acupuncture Massage therapy Spinal manipulation Yoga Cognitive behavioral therapy
o Chou et al. Diagnosis and Treatment of Low Back Pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann Intern Med 2007; 147(7):478-491.
European Spine Journal 2011
Intervention Effectiveness
Exercise Therapy
“Back School”
TENS
Heat / Cold
Low-level Laser Therapy
Patient Education
Traction
Massage
Behavioral Treatments
Lumbar Support
Multidisciplinary Treatment
Middlekoop et al. A systematic review on the effectiveness of physical and rehabilitation
interventions for chronic-non specific low back pain. Eur Spine J 2011 20: 19-39
04/04/2016
5
European Spine Journal 2011
Intervention Effectiveness
Exercise Therapy
“Back School”
TENS
Heat / Cold
Low-level Laser Therapy
Patient Education
Traction
Massage
Behavioral Treatments
Lumbar Support
Multidisciplinary Treatment
Middlekoop et al. A systematic review on the effectiveness of physical and rehabilitation
interventions for chronic-non specific low back pain. Eur Spine J 2011 20: 19-39
European Spine Journal 2010
Summary of recommendations for the treatment of low back
pain
Acute or Sub acute
Re-assure patients
Advise to stay active
Prescribe meds if necessary (time contingent)
Discourage bed rest
Do not advise a supervised exercise program
Koes et al. Eur Spine J. 2010 Dec; 19 (12): 2074-94.
European Spine Journal
Summary of recommendations for the treatment of low back
pain
Chronic low back pain
Discourage use of modalities
Short term use of meds / manipulation
Supervised exercise
Cognitive behavioral therapy
Multidisciplinary treatment
Koes et al. Eur Spine J. 2010 Dec; 19 (12): 2074-94.
04/04/2016
6
Treatment results?
Despite much research there is little consensus on the most
effective treatments for individuals with non-specific low
back pain.
Guidelines summarize research
Heterogeneous sample sizes + wide inclusion criteria
= diluted treatment effect
Classification Systems
Mechanical Diagnosis and Treatment (MDT)
Treatment Based Classification (TBC)
Pathoanatomic Based Classification (PBC)
Movement System Impairment Syndromes (MSI)
O’sullivan Classification System
Treatment Based Classification (TBC)
Developed in 1995
3 “levels”
1. Referral?
2. Staged based on acuity if symptoms
3. Classified into “syndromes”
History and examination drive the decision making process
04/04/2016
7
Treatment Based Classification (TBC)
Updated in 2007
Clinical trials showed improved patient outcomes
Clinical prediction rules were further developed
FABQ (fear avoidance)
4 classification groups emerged
Treatment Based Classification (TBC)
Group into one of four categories based on patient response
to examination:
Specific Exercise
Mobilization
Immobilization (stabilization)
Traction
Specific Exercise
Prescribe exercises that “centralize”, reduce symptoms or
address the primary condition
Centralization: pain arising from the spine and felt laterally or
distally into an extremity is reduced and moves to a more
central position during certain movements
Creates a “directional preference”
Similar to McKenzie approach
04/04/2016
8
Specific Exercise
Inclusion criteria:
Centralization with two or more movements in the same
direction
Or
Centralize with movement in one direction and perpheralize
with an opposite movement
Study: 84% of patients who performed appropriate directional preference
ex had significant decrease in pain and disability in 2 weeks
Long et al. Specific directional exercises for patients with low back pain: a case series. Physiother Can. 2008:60(4):307-
317.
Centralization
Mobilization
Inclusion criteria:
Duration of symptoms less than 16 days
No symptoms distal to the knee
Low FABQ (less than 19)
Hip internal rotation > 35°
Hypomobility with spring testing
Must meet 3
≥ 4 = 50% reduction in ODI score over 2 treatments Childs et al. A clinical prediction rule to indentify patients with low back pain most likely to benefit from spinal
manipulation: a validation study. Ann Intern Med. 2004 141(12):920-928

04/04/2016
9
Manipulation / mobilization
Stabilization
Inclusion criteria:
Average SLR > 90°
Positive prone instability test
Positive abberant movements
Age < 40
≥ 3 = 80% probability of improvement Fritz et al Subgrouping patients with low back pain: evolution of a classification approach to physical therapy. J Orthop
Sports Phys Ther. 2007;37:290-302.
Stabilization
04/04/2016
10
Traction
Inclusion criteria:
Signs and symptoms of nerve root compression
+SLR, reflex / sensory / muscular weakness
Pain or numbness distal to the buttock in previous 24 hours
Peripheralization / symptoms with extension
+XSLR
Must meet all criteria (short term benefit compared to no
traction group) Fritz et al. Is there a subgroup of patients with low back pain likely to benefit from mechanical traction: results of a
randomized clinical trial and subgrouping analysis. Spine (Phila Pa 1976). 2007; 32:E793-E800.
Traction
Limitations of 2007 TBC model
25% of test subjects met criteria for more than one subgroup
Most common overlap: Mobilization & specific exercise
Another 25% did not meet any subgroup
Stanton et al. Evaluation of a treatment based classification algorithm for low back pain: a cross sectional study. Phys Ther.
2011;91:496-509.
04/04/2016
11
TBC 2015 Update
Initial “first contact” triage (various health care providers)
3 Managements tracks
Rehab professional triage process
3 Approaches
Assess risk at both levels (1st provider & rehab professional)
Co-morbidities
Fear avoidance
Alrwaily et al. Treatment based classification system for low back pain: revision and update. Phys Ther 2016. DOI
http://dx.doi.org/10.2522/ptj.20150345
Triage by “first contact” health care
provider
Medical management
Red-flag
Screen co-morbidities
Self-care management
Unlikely to develop disabling LBP during current episode
Provide advice / guidance
Rehabilitation management
Majority of patients with LBP
Triage by rehabilitation provider Placed into one of 3 rehabilitation “approaches”
Symptom modulation
Movement control
Functional optimization
Relies on assessment of pain, disability and perception of clinical status (risk)
STarT Back Tool
Orebro Musculoskeletal Pain Questionnaire
FABQ
04/04/2016
12
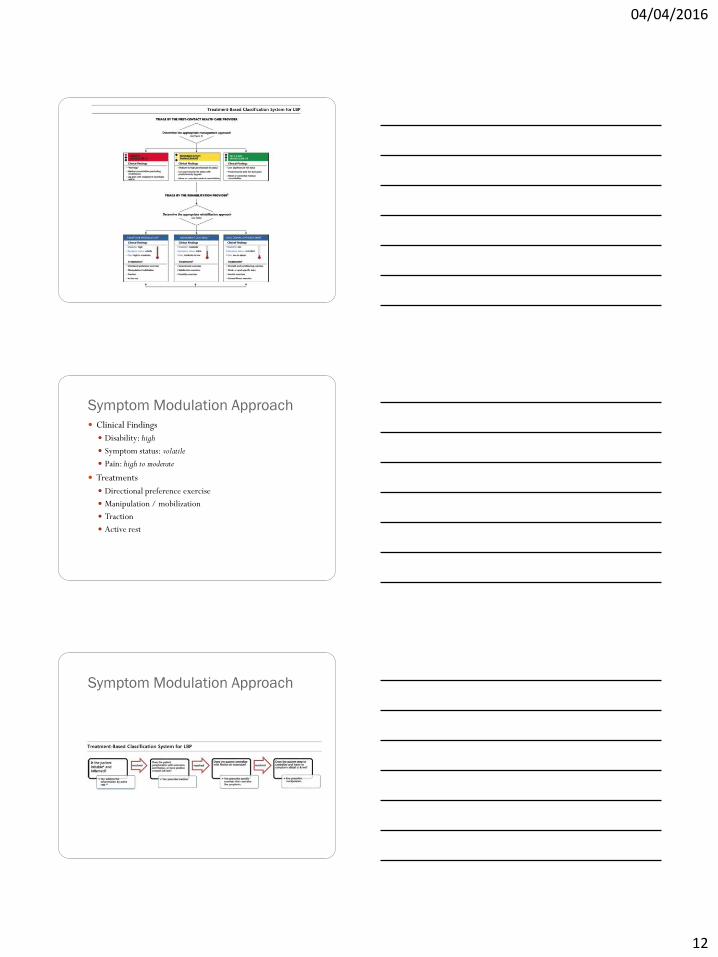
Symptom Modulation Approach
Clinical Findings
Disability: high
Symptom status: volatile
Pain: high to moderate
Treatments
Directional preference exercise
Manipulation / mobilization
Traction
Active rest
Symptom Modulation Approach
04/04/2016
13
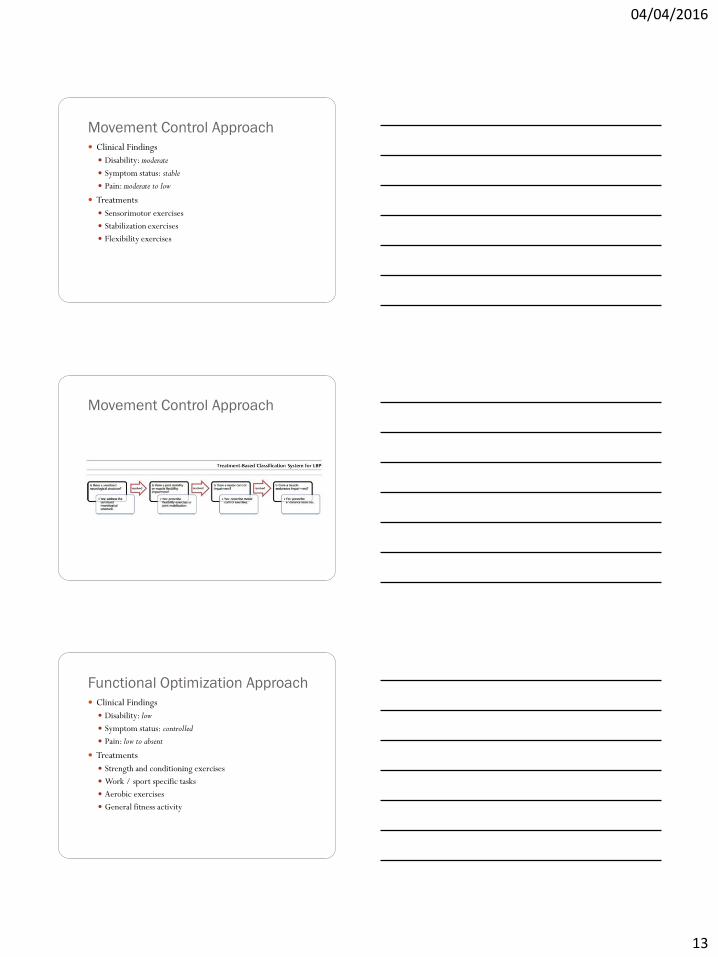
Movement Control Approach
Clinical Findings
Disability: moderate
Symptom status: stable
Pain: moderate to low
Treatments
Sensorimotor exercises
Stabilization exercises
Flexibility exercises
Movement Control Approach
Functional Optimization Approach
Clinical Findings
Disability: low
Symptom status: controlled
Pain: low to absent
Treatments
Strength and conditioning exercises
Work / sport specific tasks
Aerobic exercises
General fitness activity
04/04/2016
14
Functional Optimization Approach
Case 1
55 y/o housekeeping employee at SNF
Injured left low back moving hospital bed
Symptom duration: 2 weeks
Pain: 4/10 intermittent bending / lifting
Work status: light duty
Medication: Naprosyn, Flexeril
Wishes to resume resistance exercise
PMH: HBP, TTDM
Case 1
55 y/o housekeeping employee at SNF
Exam:
FABQ 10
FOTO score 55
Lumbar AROM WNL: pain with extension overpressure (L lumbar)
Limited P-A mobility left L4 – L5 segments
04/04/2016
15
Case 1
55 y/o housekeeping employee at SNF
Decision making using updated TBC
Symptoms: stable
Pain: moderate to low
Disability: moderate
Movement control approach
Sensitized neurologic structure? No
Joint mobility impairment? Yes
Treatment: manipulation
3 visits: 1/10 pain, FOTO score 72
Case 2
27 y/o graduate student / barrista
Belted driver in MVA 3 weeks ago
Pain 8/10 central low back and right leg
Symptoms: sleep, walk, stand
Meds: hydrocodone
Unable to return to school / work due to symptoms
Case 2
27 y/o graduate student / barrista
Exam
FABQ 60
ODI 74
Pain and limited AROM: flexion and extension
+ right SLR
Symptoms centralize with extension
04/04/2016
16
Case 2
27 y/o graduate student / barrista
Decision making using updated TBC
Symptoms: volatile
Pain: high
Disability: high
Symptom modulation approach
Symptom centralization? Yes, extension
Treatment: prescribe extension exercises
6 visits: ODI 34, return to work / school
Stay tuned!
More research to be published on TBC
Thank you!