Embed Size (px)
Citation preview

1
Evolution of Drug Resistance in Environmental Bacteria
Richard M. Mariita
Adviser: Pamela Yeh
PhD Prospectus
Project Summary
A comprehensive understanding of the diversity and abundance of drug-resistant bacteria, and the selection pressures operating in the environments is critically needed. In this study, diversity, abundance and potential for evolution of antibiotic resistance of Staphylococci isolates from different public transportation vehicles in Portland, Oregon will be evaluated. Samples will be collected from the seats and handholds and analyzed for the diversity, abundance and potential for evolution of drug resistance. I will identify isolates by sequencing for 16S rRNA genes. Antibiotic susceptibility testing against ten commonly used antibiotics will be performed by minimum inhibitory concentration (MIC) and mutant prevention concentration (MPC) methods. Results from the study could influence clinical and public health decisions, as well as increase public understanding of bacteria found on the environment.

2
CHAPTER 1: INTRODUCTION
1.1 Background
The emergence of antimicrobial resistance among pathogenic and commensal bacteria, including environmental bacteria, is a growing concern for humans and other organisms [1-4]. The evolution of drug resistant bacteria is a significant problem, as it can affect how diseases progress and whether specific therapies will be effective [5, 6]. Significantly, increased antibiotic use for treatment of humans, as well as for use in industrial agriculture, often naturally selects for drug-resistant bacteria, increasing the likelihood for the evolution of new drug resistant strains [6-9]. Furthermore, recent studies indicate that hospital and agricultural antibiotic use is contaminating natural environments [6, 10, 11]; therefore creating environmental bacteria with high levels of drug resistance [12, 13]. Therefore, the use of antibiotics may have consequences for not only pathogenic and commensal bacteria, but environmental bacteria as well as it is a heterogeneous community of bacteria, hence exchanging genetic materials [14].
1.2 Statement of the problem and justification Methicillin resistant Staphylococcus aureus (MRSA) can be acquired in hospitals, medical vehicles and patient homes [11, 15], as well as in public spaces [6, 16]. Both nosocomial and community-acquired infections are now considered important public health threats, with some countries even starting to carry out annual surveys on their prevalence for infection control and antibiotic treatment policies, because of their increasing toll on healthcare cost, morbidity and mortality [10,17-21]. The evolution of drug resistance and techniques of surveillance for such resistance has been well studied in clinical microorganisms, but few surveillance strategies have been developed for emerging environmental drug resistant bacteria. Also, the effect of spatial and temporal heterogeneities in the environment on the evolutionary processes during the emergence of drug resistance has typically been overlooked [3]. Because the biological consequences of drug resistant environmental bacteria could potentially be serious and widespread; studies on their potential to evolve drug resistance are critical to understanding the extent of the environmental resistome, defined as a collection of all the antibiotic resistance genes and their precursors in pathogenic and non-pathogenic bacteria. [22]. The study will focus on Staphylococcus species because these bacteria are ubiquitous, are a leading cause of bacterial infections and a major concern due to evolution of antibiotic-resistance [22]. While antimicrobial resistance may either be acquired horizontally through incorporation of resistance genes or vertically through accumulation of base substitutions via spontaneous mutations in bacteria [4, 10, 23], I will focus on the latter. The study will examine the diversity and distribution of Staphylococcus species within urban environments and determine their potential to evolve drug resistance. I will use a combination of field and laboratory methods to determine microbial densities, levels of antibiotic resistance and genetic diversity of Staphylococcus species by 16S rRNA gene sequencing.

3
Here we extend the definition of resistance to encapsulate not only the MIC but also the MPC. The minimum inhibitory concentrations (MICs) are defined as the lowest concentration of an antibiotic that inhibits visible growth of microorganisms after 18-20 hours of incubation [24] (Fig. 1). As a new parameter used to predict antibiotic efficacy for preventing emergence of resistant bacteria, the mutant prevention concentration (MPC), can be defined as the minimum inhibitory concentration (MIC) of the least drug-susceptible single-step mutant population of more than 1010 cells [25-27]. The concentration range within the upper and lower boundary based on the MPC and MIC in which mutants are selectively enriched is defined as the Mutant-Selection Window (MSW) [10, 26, 27]. Dong et al., came up with the idea of coming up with the MPC concept, and suggested that antibiotic concentrations between the MIC and MPC should be used to inhibit selection of mutant populations [28]
Fig 1: MIC, MPC and MSW. Yeh et al., 2009. 1.3 Specific aims The study will address the following aims:
1) Determine the abundance and diversity of Staphylococcus species in a range of public transportation train lines in Portland, Oregon, across temporal and spatial variation in sampling.
2) Determine the potential for evolution of antibiotic resistance against various antibiotics in environmental Staphylococcus species, as measured by the Mutant Prevention Concentration (MPC).
3) Determine the range of drug interaction types in Staphylococci across a network of drug interactions, and determine if phylogenetic relatedness affects drug interaction type.

4
1.4 Significance and Impact of the Study
To our knowledge, this will be the first study to examine the potential for resistance in environmental microbes, to systematically measure and examine drug interaction types in environmental bacteria, and to determine whether phylogenetic relatedness affects either of these traits. This is a study with public health implications, as the results will be applicable for public health policy officials as well as clinicians. Furthermore, this study will provide important baseline data for bacteria in public transit, and can serve as the basis for a long-term study to track changes in the abundance, diversity, and levels of drug resistance.

5
CHAPTER 2: LITERATURE REVIEW
2.1 Antibiotic Resistance Resistance is a response of microbe population to antibiotic treatment [10]. Since the introduction of antibiotics, many facets of the resulting antimicrobial resistance problems have been studied, including: the emergence of microorganisms that are resistant to different antimicrobial agents, resistance mechanisms, the frequencies of antibiotic resistances, and clinical surveillance studies collecting MIC values of different drugs [23]. Antibiotic resistant pathogens have historically been limited to the hospital settings but since the 1990s, they have been found to be affecting outpatients in health care-associated settings such as nursing homes, dialysis centers, infusion centers and among recently hospitalized patients [29]. The emergence of Community-acquire (CA) infections with more severe virulence factors, like Panton–Valentine leukocidin (PVL) in CA- MRSA has increased the need for regular surveillance antibiotic resistance in environmental microbes[30]. Antibiotic selection essentially enriches the number of resistance genes in a particular setting, but these genes already exist before selection operates [23, 31]. The global increase in drug resistance has been found to be in partly because of the therapeutic concentrations currently used, that selectively enrich the resistant mutant portion of the population [31]. Hence, several recent studies have emphasized the importance MPC-based dosing strategies (Fig. 2) to improve therapeutic outcomes and to restrict the selection of resistant mutants [10, 23, 31].
Fig. 2: MSW and MPC. Figure illustrating three different situations where an antibiotic is administered (Canton and Morosini, 2011).

6
Sites that are often touched by humans can become contaminated with staphylococci and other species and act as fomites for the transmission of bacteria between humans [33]. Such sites could provide a reservoir for community-associated MRSA (CA-MRSA). In agriculture, the evolution of antibiotic resistance usually results from selective enrichment of resistant bacteria from the use of antibiotics as growth-promoters in animal production, for therapy and prophylaxis [34, 35]. The incorporation of antibiotic resistance genes from these bacteria into the pathogenic or commensals bacteria ends up heightening infections [9, 12, 13, 35].
2.2 Mechanisms of Antibiotic Resistance in Bacteria Bacteria possess different structural characteristics and these differences determine the mechanisms for primary resistance (Table 1). Table 1: General mechanisms of resistance to antimicrobial agents Resistance Mechanism Antibiotic class Decreased outer membrane permeability
Β-Lactams
Decreased cytoplasmic membrane transport
Quinolones Aminoglycosides (decreased energy)
Drug inactivation (reversible or irreversible)
Β-Lactams
Alteration of 16S rRNA, r-protein S12; modification of drug structure.
Aminoglycosides Aminoglycosides (modifying enzymes) Chloramphenicol (inactivating enzymes)
Target modification Quinolones (gyrase modifications) Rifampin (DNA polymerase binding) Β-Lactams (PBP changes) Macrolides (rRNA methylation) Linezolid (23s rRNA modifications)
Alteration of dihydrofolate reductase (Target bypass) Trimethoprim (Dihydrofolate reductase
inhibitor Chen et al., 2009 Antibiotic resistance in bacteria has been globally identified in isolates from environmental, animal and human sources [34]. There are several mechanisms that lead to antibiotic resistance. This can be through mutations that occur in the natural environment
7
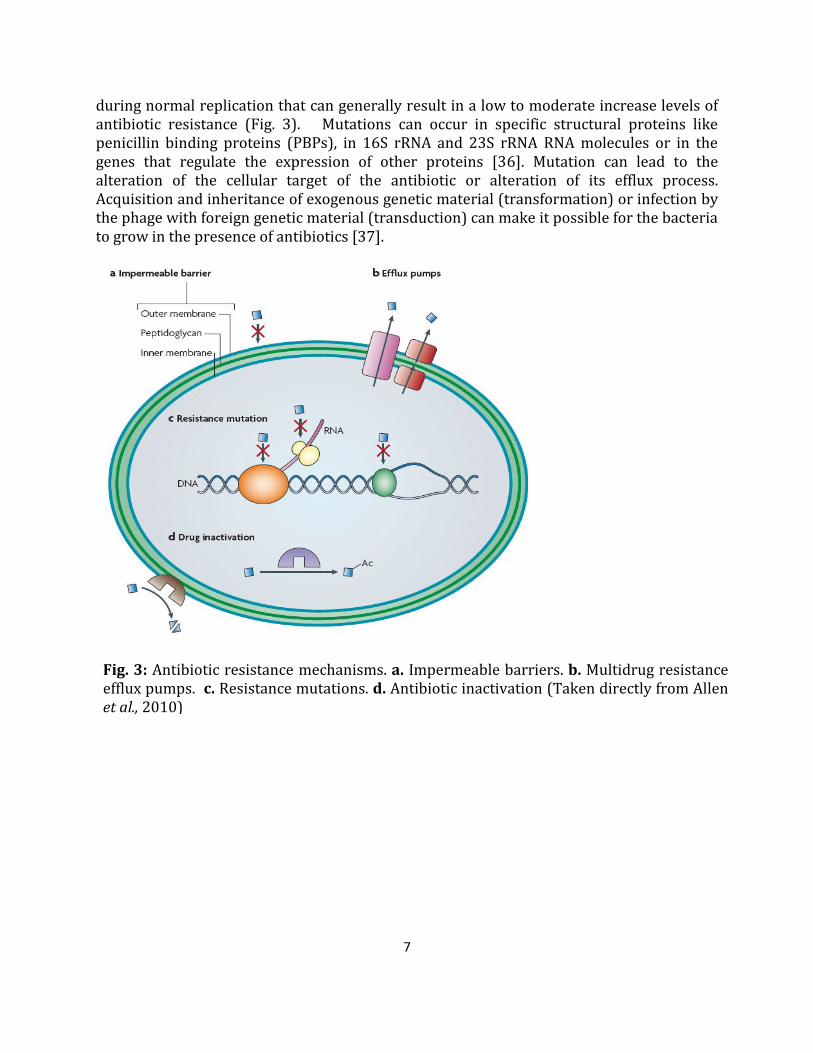
during normal replication that can generally result in a low to moderate increase levels of antibiotic resistance (Fig. 3). Mutations can occur in specific structural proteins like penicillin binding proteins (PBPs), in 16S rRNA and 23S rRNA RNA molecules or in the genes that regulate the expression of other proteins [36]. Mutation can lead to the alteration of the cellular target of the antibiotic or alteration of its efflux process. Acquisition and inheritance of exogenous genetic material (transformation) or infection by the phage with foreign genetic material (transduction) can make it possible for the bacteria to grow in the presence of antibiotics [37].
I
Fig. 3: Antibiotic resistance mechanisms. a. Impermeable barriers. b. Multidrug resistance efflux pumps. c. Resistance mutations. d. Antibiotic inactivation (Taken directly from Allen et al., 2010)

8
CHAPTER 3: MATERIALS AND METHODS
3.1 Bacterial strains Samples for isolation of bacterial strains from four different public transportation train lines (Blue, Red, Yellow and Green) in Portland, Oregon, will be collected. Two different locations will be sampled: seats and handholds. Baird-Parker (BP) agar, to be prepared by suspending 58 g of media in 0.95 liter of sterile distilled water and autoclaved at 121°C for 15 minutes, will be used in selective isolation of Staphylococci. This media contains lithium chloride and tellurite to inhibit the growth of other bacteria, pyruvate and glycine to selectively stimulate the growth of Staphylococci. After cooling the BP media to 45-50°C, 50 mL of egg-yolk tellurite emulsion (for colony differentiation) and 0.05g sulfamethazine to help suppress the growth and swarming of Proteus species will be added. Using sterile swabs, a sample area of 8 cm2 for location will be swibed and streaking for isolation done on already prepared agar plates [20]. Agar plates will then be labeled with date, time collected and trimet number and incubated at 37°C for 48 hours. In total, 40 swabs (2 sampling sites X 5 replicates X 4 max lines) will be collected from the four max lines and examined.
3.2 Bacterial counts and phenotypic identification After incubating for 48 hours, all colonies will be counted. A subset of single colonies will then be inoculated into Luria-Bertani (LB) broth and incubated in a shaker (250 rpm) overnight at 37°C until they reach an absorbance of between 0.3 - 0.6 at an optical density of 600nm(OD600) before being processed for storage.
3.3 Storage of Bacterial Isolates
Pure isolates obtained from sub-culturing on LB agar will be processed and stored in master set tubes in 17% glycerol broth and stored at -80°C. From the master set tubes, aliquots will be made and stored at -80°C for further analysis [8].
3.4 Preparation of bacterial DNA and PCR amplification
Pure subcultured bacterial isolates from 17% glycerol stocks will be used for genomic DNA (gDNA) extraction, to be done as outlined by Ajiboye et al., [38] and Boone and Popa [39]. The bacteria will suspended in 500 µL of 1 X phosphate- buffered saline (pH 7.4) solution, boiled for 10 minutes, frozen overnight in a -80°C freezer, thawed, resuspended, reboiled for 10 minutes, and centrifuged. After visualizing the PCR product on a 1.5% agarose gel stained with ethidium bromide and visualized under UV transillumination to confirm purity of gDNA, 2 µL of the supernatant, to be used as DNA template will be pipetted into 25 µL of PCR mixture and used for 16S rRNA gene sequencing.

9
3.5 Sanger Sequencing Sequence-based identification techniques of organisms are becoming more reliable than phenotypic methods. In Sanger dideoxy terminator sequencing, the bacterial gDNA extracts will be used as template for a DNA polymerase reaction to help identify isolates. Sequencing will be performed at the state of the art DNA research facilities, GENEWIZTM Seattle, WA. 16S rRNA gene universal primers (16S rRNA Forward: AGA GTT TGA TCC TGG CTC AG, 16S rRNA Reverse: ACG GCT ACC TTG TTA CGA CTT) will be used to sequence and compare to various Staphylococcus species’ 16S rRNA gene [40]. Chromatograms will be viewed, aligned, assembled and analyzed using FinchTV program [39]. Basic Local Alignment Search Tool (BLAST) from the National Center for Biotechnology Information (NCBI) will be used to compare nucleotide sequences to find possible matches [40,41, 39]. Analysis of phylogenetic relatedness of the various bacterial sequences will also be performed to develop a maximum likehood tree. Relative abundance will also be assessed using 16S rRNA gene sequences.
3.6 Antibiotic stock solutions
Antibiotics will be obtained in standard powder form from Sigma-Aldrich (U.S.A). Stock solutions will be prepared (Table 2) and stored according to the manufacturer’s instructions. Suitable ranges of antibiotic concentrations will be used to test against Staphylococci species. Table 2: Antibiotic stock solutions, their mechanisms and solubility Drug Mechanism Solubility Max. concentration
1 Amikacin sulfate salt Aminoglycoside -30S Water 50mg/ml
2 Streptomycin sulfate salt 30S Water 50mg/ml
3 Clindamycin hydrochloride
50S Water ~
4 Ciprofloxacin Fluoroquinolone – DNA gyrase
Water ~
5 Nalidixic acid sodium salt
DNA gyrase Water 100mg/ml
6 Chloramphenicol* Chain elongation Water 50mg/ml
7 Oxacillin sodium salt Β-lactamase – Cell wall Water 50mg/ml
8 Vancomycin hydrochloride hydrate
Cell wall Water 50mg/ml
9 Rifampicin* RNA synthesis ~ 1-2.5mg/ml
10
10 Trimethoprim lactate salt*
Folic acid ~ 20mg/ml
11 Sulfamonomethoxine* Folic acid ~ 4mg/ml
*Rifampicin requires DMSO, Trimethoprim lactate salt requires water (1 mL) + 10 μl glacial acetic acid, and Sulfamonomethoxine requires water and 0.1 M NaOH dropwise as solvents to dissolve (Andrews, 2006).
3.7 Determination of Minimum Inhibitory Concentration (MIC)
MIC is defined as the lowest concentration of antimicrobial that will inhibit visible growth of a microorganism, when compared to the untreated controls, after incubating for 24 hours [8]. The range of antibiotic concentrations to be used in MIC determination will be in doubling dilution steps as described below [4, 8]. Using a 96-well plate, a serial dilution will be prepared where a maximum, very-high concentration of antibiotic in a growth medium will be diluted by half in each subsequent column of the plate, with the 12th column of the plate lacking drug, as a negative control. A library replicator will be used to inoculate all wells of the plate with the bacterial strain to be tested, and the plate incubated overnight at 37°C while shaking at 600rpm. This wide range of drug concentrations will be used to find a column/concentration that will be an initial known inhibition concentration, and an initial known maximum tested concentration at which inhibition does not occur. Inhibition will be measured on the basis of absorbance at 600nm using PerkinElmer 2030 plate-reader, with inhibition visible as a steep drop from light-absorbent wells that are dense with bacteria to wells with minimal absorbance, where few or no bacteria have grown. Subsequent tests will employ a 96-well plate prepared with an equidistant gradient of concentrations inoculated with bacteria in a similar fashion, set up to test higher and lower than the initial known inhibition concentration and initial known maximum non-inhibitory concentration. The lowest concentration at which inhibition occurs and the highest non-inhibitory concentration will again be used to set up another equidistant gradient in this fashion until a sufficiently precise minimum inhibitory concentration (MIC) is known
3.8 Determination of Mutant prevention Concentration (MPC) and Mutant Selection Window (MSW)
High antibiotic concentrations block the growth of single step mutants most of the time [10]. Above such a concentration, a second resistance mutation must be present for growth to occur. MPC which is the drug concentration at which all first-step resistant mutants will be eradicated along with the susceptible cells, for each drug combination. This therefore means that for fully susceptible (wild-type) cells to grow above the MPC, they must acquire two resistance mutations concurrently. Drug resistance is thought to evolve primarily at drug concentrations below the MPC but above the MIC. This region is termed as the MSW

11
and the size of the MSW is one measurement of the potential to evolve resistance. The larger the MSW, the greater the potential for the evolution of drug resistance [4].
To test for MPC, the test bacteria will be cultured in LB broth and incubated in a shaker at 37°C until it attains absorbance of between 0.5 and 0.7. The suspension will then be centrifuged using an Eppendorf 5810R centrifuge at 4000 rpm to yield a supernatant with a concentration of 1010 colony forming unit (CFU)/mL. The inocula will further be confirmed through the serial dilution and plating of 100mL samples on drug free medium as positive control. MATLAB R2011b (2011) application software will be used to determine two fold MIC concentrations of drugs to be used in various MPC experiments. Then, agar petri dishes with two-fold increases of MICs (2X MIC_, 4X MIC_, 8X MIC_, 16X MIX_, etc.) which will be followed by more intermediate concentrations (narrow concentration increments) will be tested to obtain more precise values of MPCs [26,32]. Agar plates will then be incubated for 48 h to 72 hours at 37°C and screened visually for growth and colonies counted [32].
The MPC 109 will be reported as the lowest integer coefficient concentration of MIC at which only 109 times or fewer as many CFU formed as compared to the control plates. MPC and MIC ratios (MSW) will help detect presence of drug resistant mutants. MSWs for single drug and multi-drug combinations to determine which ones have the potential for evolution of drug resistance will be determine and compared [4, 11, 42]. Uninoculated plates with no drugs for each drug concentration will be prepared and used as negative controls.
3.9 Statistical analysis A laboratory-based study has already been conducted to evaluate the performance of two sampling methods (pour plate and streak plate techniques) for recovery of Staphylococci. Results indicated that overall, there were no statistically significant correlation differences between pour plate and streak plate method (r2= 0.534). Streak plate method was chosen for this study because of its field replication advantage over the pour plate method. One-way ANOVA will be used to determine if the colony forming units (cfu) per plate are significantly different among sampling sites. Two way ANOVA will be performed to determine temporal differences between various train lines and sampling sites. Computational phylogenetics will be used to construct phylogenies for 16S rRNA gene.
3.10 Expected Results I expect to obtain bacterial abundances from public train transportation system and determine if there are any temporal differences between to the time or seasons of sampling. Clearly, knowledge of the existence of certain strains of Staphylococcus aureus including MRSA) on public trains will be of critical importance from a public health perspective. This study will also determine which isolates will have high potential for the evolution of drug resistance.

12
TIMELINE
Year ACTIVITY
1 Research training, literature review, to help refine research question. Continue to make contacts and get established into research, Collect preliminary data in field and lab. Learn Matlab and begin analyzing data and making figures.
2 Further development of research tools, continue collecting of data. 3 Main research phase: continue collecting of data. 4 Finish collecting data. Analysis, supplementary research activities, literature
review 5 Complete writing up

13
REFERENCES
1. Baquero et al., 2011. Ecology and Evolution as Targets: the need for Novel Eco-Evo
Drugs and Strategies to fight antibiotic resistance. Antimicrobial Agents and Chemotherapy. 55 (8): 3649-3660.
2. Svara, F. and Rankin, D.J. 2011. The evolution of plasmid- carried antibiotic resistance. BMC Evolutionary Biology. 11:130.
3. Zhang et al., 2011. Acceleration of Emergence of Bacterial Antibiotic resistance in Connected Microenvironments. Science. 333: 1764-1767.
4. Drlica, K. 2003. The mutant selection window and antimicrobial resistance. Journal of Antimicrobial Chemotherapy. 52: 11-17.
5. Oancea, S., Stoia, M. 2010. Antibiotic resistance of bacterial pathogens: the magnitude of the problem from two perspectives - Romanian and worldwide. Romanian Biotechnological Letters. 15 (5): 5519-5529.
6. Clardy, J., Fischbach, M.A., Walsh, C.T. 2006. New antibiotics from bacterial natural products. Nature Biotechnology. 24(12): 1541-1550.
7. Martinez, J.L. 2009. Environmental pollution by antibiotic resistance determinants. Environmental pollution. 157: 2893-2902.
8. Andrews, J.M. 2006. Determination of Minimum Inhibitory Concentrations. Birmingham: City Hospital NHS Trust. pp. 1-19.
9. Smith, D.L., Dushoff, J. Morris, J.G. 2005. Agricultural Antibiotics and Human Health: Does antibiotic use in agriculture have a greater impact than hospital use? PLoS Medicine. 2(8): 0731-0735.
10. Drlica, K., Perlin, D.S. 2011. Antibiotic Resistance: Understanding and Responding to Emerging Crisis. New Jersey: Pearson Education inc. pp. 73-117.
11. Wright, G.D. 2010. Antibiotic resistance in the environment: a link to the clinic? Current Opinion in Microbiology. 13:589-594.
12. Smith, D.L., Harris, A.D., Johnson, J.A., Silbergeld, E.K., Morris, J.G. 2002. Animal antibiotic use has an early but important impact on the emergence of antibiotic resistance in human commensal bacteria. PNAS. 99(9):6434-6439.
13. Lipsitch, M., Singer, R.S., Levin, B.R. 2002. Antibiotics in agriculture: When is it time to close the barn door? PNAS. 99(9): 5752-5754.
14. Villaescusa et al., 2010. A close link between bacterial community composition and environmental heterogeneity in maritime Antarctic lakes. International Microbiology. 13:67-77.
15. Davies, J. Davies, D. 2010. Origins and Evolution of Antibiotic Resistance. Microbiology and Molecular Biology Reviews. 74 (3): 417-433.
16. Fischbach, M.A., Walsh, C.T. 2009. Antibiotics for Emerging Pathogens. Science. 325: 1089-1093.
17. Alvarez, C.A., Yomayusa, N., Leal, A.L., Moreno, J., Mendez-Alvarez, S., Ibanez, M., Vanegas, N. 2010. Nosocomial infections caused by community-associated methicillin-resistant Staphylococcus aureus in Colombia. American Journal of Infection Control. 38: 316-318.
14
18. Asensio, A., Canton, R., Vaque, J., Rossello, J., Calbo, F., Garcı´a-Caballero, J., Domı´nguez,, V., Herna´ndez, A., Trilla, A. 2006. Nosocomial and community-acquired meticillin-resistant Staphylococcus aureus infections in hospitalized patients (Spain, 1993-2003). Journal of Hospital Infection. 63: 465-471.
19. Fritschea, T.R., Sader, H.S., Stilwell, M.G., Dowzicky, M.J., Jones, R.N. 2005. Antimicrobial activity of tigecycline tested against organisms causing community-acquired respiratory tract infection and nosocomial pneumonia. Diagnostic Microbiology and Infectious Disease. 52: 187-193.
20. Simon et al., 2008. Nosocomial infection: A risk factor for a complicated course in children with respiratory syncytial virus infection – Results from a prospective multicenter German surveillance study. International Journal of Hygiene and Environmental Health. 211:241-250.
21. Allen, G.P., Deshpande, LM. 2010. Determination of the mutant selection window for clindamycin, doxycycline, linezolid, moxifloxacin and trimethoprim-sulfamethoxazole against community-associated meticillin-resistant Staphylococcus aureus (MRSA). International Journal of Antimicrobial Agents. 35: 45-49.
22. D’Costa, V.M. et al., 2011. Antibiotic resistance is ancient. Nature. 477: 457-461. 23. Canton, R., and Morosini, M. 2011. Emergence and spread of antibiotic resistance
following exposure to Antibiotics. Federation of European Microbiological Societies. 35: 977-991.
24. Andrews, J.M. 2001. Determination of minimum inhibitory Concentrations. Journal of Antimicrobial Chemotherapy. 48: Suppl. S1- 5-16.
25. Rodriguez, J.C., Cebrian, L., Lopez, M., Ruiz, M., Royo, G. 2004. Mutant prevention concentration: a new tool for choosing treatment in nontuberculous mycobacterial infections. International Journal of Antimicrobial Agents. 24: 352-356.
26. Zhao, X., Drlica, K. 2001. Restricting the Selection of Antibiotic-Resistant Mutants: A General Strategy Derived from Fluoroquinolone Studies. Clinical Infectious Diseases. 33(3): S141-S146.
27. Credito, K., Kosowska-Shick, K., Appelbaum, P.C. 2010. Mutant Prevention Concentrations of Four Carbapenems against Gram-Negative Rods. Antimicrobial Agents and Chemotherapy. 54 (6): 2692-2695.
28. Dong, Y., Zhao, X., Domagala, J., Drlica, K. 1999. Effect of Fluoroquinolone Concentration on Selection of Resistant Mutants of Mycobacterium bovis BCG and Staphylococcus aureus. Antimicrobial Agents and Chemotheraphy. 43(7): 1756-1758.
29. Chen, C. Fischbach M.A., Walsh, C.T. 2009. Antibiotics for Emerging Pathogens. Science. 325: pp. 1089-1093.
30. Skov et al., 2011. Update on the prevention and control of community-acquired meticillin-resistant Staphylococcus aureus (CA-MRSA). International Journal of Antimicrobial Agents. ANTAGE-3745.
31. Michel, J., Yeh, P.J., Chait, R., Moellering, R.C., Kishony, R. 2008. Drug interactions modulate the potential for evolution of resistance. PNAS 105 (39): 14918-14983.
32. Gebru, E., Damte, D., Choi, M., Lee, S., Kim, Y., Park, S.C. 2011. Mutant prevention concentration and phenotypic and molecular basis of fluoroquinolone resistance in

15
clinical isolates and in vitro-selected mutants of Escherichia coli from dogs. Veterinary Microbiology. 154:384-394.
33. Otter, J.A., French, G.L. 2009. Bacterial contamination on touch surfaces in the public transport system and in public areas of a hospital in London. Letters in Applied Microbiology ISSN 0266-8254.
34. Kinge, C.N.W., Ateba, C.N., Kawadza, D.T. 2010. Antibiotic resistance profiles of Escherichia coli isolated from different water sources in the Mmabatho locality, North-West Province, South Africa. South African Journal of Science. 106 (1/2): 1- 6.
35. Heuer et al., 2002. Gentamicin resistance genes in environmental bacteria: prevalence and transfer. FEMS Microbiology Ecology. 42: 289-302.
36. Keen, P.L., Montforts, M.H.M.M. 2012. Antimicrobial Resistance in the Environment. New Jersey: Black-well synergy. pp. 15-123.
37. Allen, H.K., Donato, J. Wang, H.H., Cloud-Hansen, K.A. Davies, J. Handelsman, J. 2010. Call of the wild: antibiotic resistance genes in natural environments. Macmillan Publishers Limited. 8: 251-259.
38. Ajiboye, R.M., Solberg, O.D., Lee, B.M., Raphael, E., DebRoy, C., Riley, L.W. 2010. Global Spread of Mobile Antimicrobial Drug Resistance Determinants in Human and Animal Escherichia coli and Salmonella Strains Causing Community-Acquired Infections. Clinical Infectious Diseases. 49:365-71
39. Boone, J.E., Popa, R. 2010. Molecular Techniques in Microbiology. 3rd Edition. Portland city: Fountainhead Press. pp. 51-52.
40. Russell, P.J. 2010. iGenetics: A molecular Approach. 3rd Edition. San Francisco: Benjamin Cummings. (Kindle Edition).
41. Yeh, P.J., Simon, D.M., Millar, J.A., Alexander, H.F. 2011. A Diversity of Antibiotic-resistant Staphylococcus spp. in a public Transportation System. Public Health and Research Perspectives. 2(3): 202-209.
42. Drlica, K. Zhao, X. Blondeau, J.M., Hesje, C. 2006. Low Correlation between MIC and Mutant Prevention Concentration. Antimicrobial Agents and Chemotherapy. 5 (1): p. 403-404.





























