Embed Size (px)
Citation preview
Cheryl Cashin, R4D/JLN
Peter Smith,
Imperial College
EVOLUTION OF HEALTH
PURCHASING, PROVIDER
PAYMENT SYSTEMS AND
RBF
Interagency Working Group on Results-Based Financing
Meeting – Geneva, Switzerland
November 12, 2012
OUTLINE OF THE PRESENTATION
Summary of results and main conclusions from the
OECD/European Observatory study on supply-side
Pay-for-Performance Programs in 11 OECD Countries
(Peter Smith)
Implications for the role of RBF in health purchasing
and provider payment—initial thoughts on a
conceptual framework (Cheryl Cashin)
Peter
Smith
OECD/EUROPEAN OBSERVATORY
STUDY ON P4P IN OECD COUNTRIES
SUMMARY OF RESULTS AND MAIN
CONCLUSIONS
A DEFINITION OF P4P (FORTHCOMING)
“the deliberate adaptation of provider payment mechanisms
explicitly to promote the pursuit of health system quality
objectives”.
The key elements of any P4P programme should usually be:
a statement of the quality objectives it seeks to promote;
definition of quality metrics that will influence reimbursement;
formulation of the associated rules for reimbursement that make
some element conditional on measured levels of attainment;
rules for providers regarding provision of information and other
standards;
governance arrangements that ensure that the system is working as
intended.
Source: Borowitz, Cashin, Chi, Smith,
and Thompson (forthcoming) for
Observatory and OECD
WHAT SHOULD BE REWARDED?
Structure
Provision of service
Accreditation
Information provision
Process
Adherence to guidelines
Outcomes
Biomedical status
Avoidable admissions
Health status
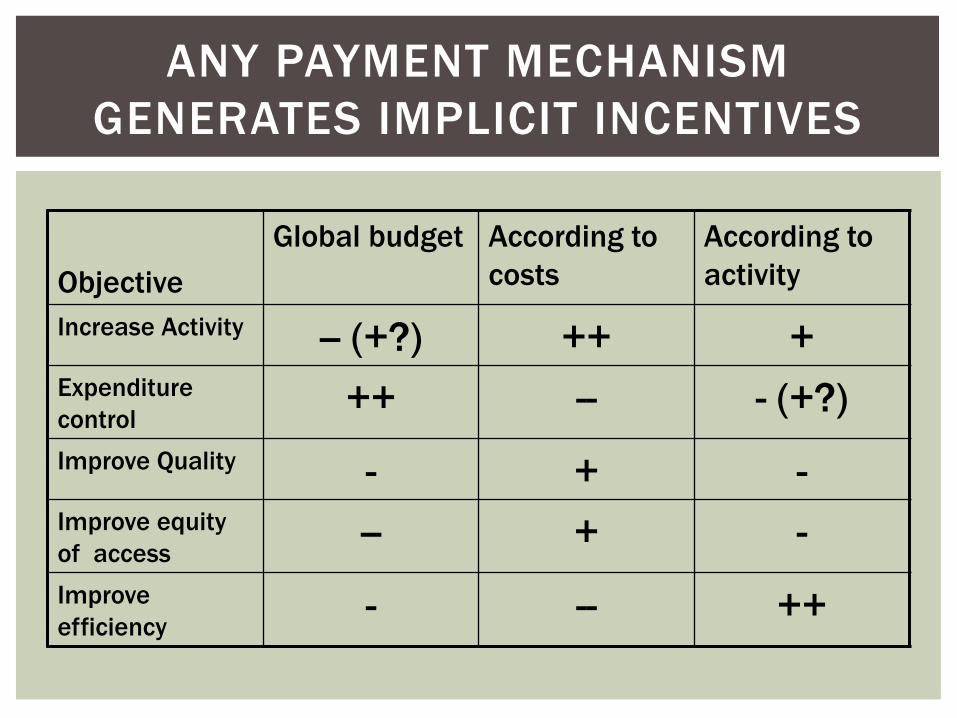
ANY PAYMENT MECHANISM
GENERATES IMPLICIT INCENTIVES
Objective
Global budget According to
costs
According to
activity
Increase Activity -- (+?) ++ + Expenditure
control ++ -- - (+?)
Improve Quality - + - Improve equity
of access -- + -
Improve
efficiency - -- ++
ANY PERFORMANCE REPORTING
GENERATES INCENTIVES FOR QUALITY
Reputational incentive
Commercial incentive
Direct financial incentive
Note the key role of comparative performance
information
Increasing recognition that indirect reputational and
commercial incentives are inadequate
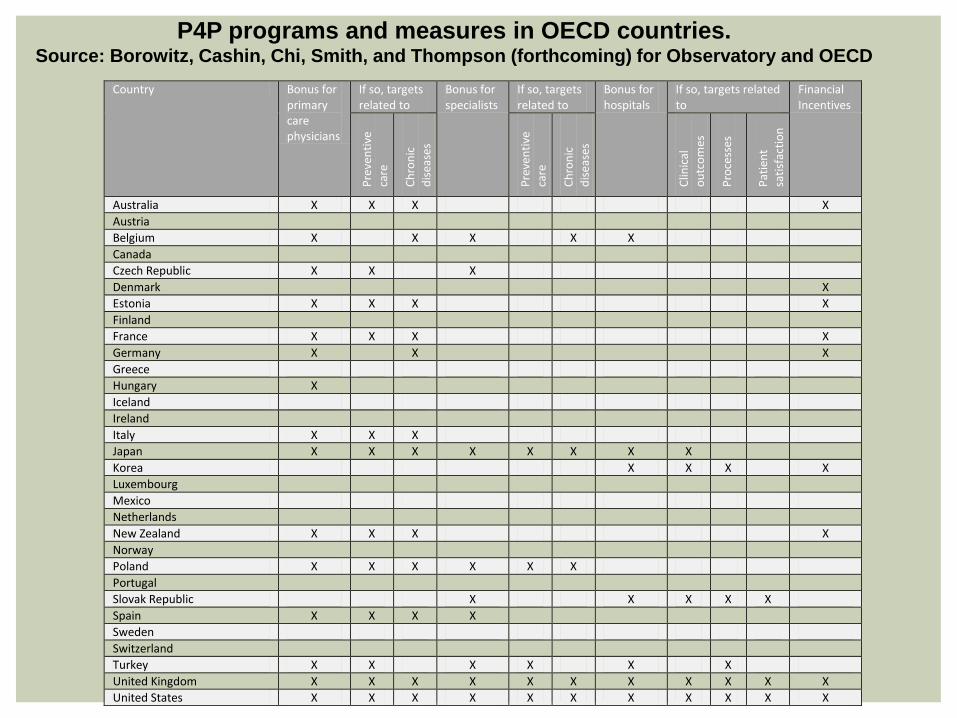
P4P programs and measures in OECD countries. Source: Borowitz, Cashin, Chi, Smith, and Thompson (forthcoming) for Observatory and OECD
Country Bonus for primary care physicians
If so, targets related to
Bonus for specialists
If so, targets related to
Bonus for hospitals
If so, targets related to
Financial Incentives
Pre
ven
tive
care
Ch
ron
ic
dis
ease
s
Pre
ven
tive
care
Ch
ron
ic
dis
ease
s
Clin
ical
ou
tco
mes
Pro
cess
es
Pat
ien
t sa
tisf
acti
on
Australia X X X X
Austria
Belgium X X X X X
Canada
Czech Republic X X X
Denmark X
Estonia X X X X
Finland
France X X X X
Germany X X X
Greece
Hungary X
Iceland
Ireland
Italy X X X
Japan X X X X X X X X
Korea X X X X
Luxembourg
Mexico
Netherlands
New Zealand X X X X
Norway
Poland X X X X X X
Portugal
Slovak Republic X X X X X
Spain X X X X
Sweden
Switzerland
Turkey X X X X X X
United Kingdom X X X X X X X X X X X
United States X X X X X X X X X X X
Primary care (and disease management) :
Australia: Per formance Improvement Program
United Kingdom: Quality and Outcomes Framework (QOF)
New Zealand: Primary Health Organization (PHO) Per formance Program
Brazi l : Program for Per formance Improvement (PIMESF) in Pir ipir i
France: Contracts to Improve Individual Practice (CAPI)
Germany: Disease management
Hospital care
United States: Hospital Quality Incentive Demonstration (HQID) in the Medicare System
United States: Cal ifornia Hospitals Init iat ive
Korea: Value Incentive Program
CASE STUDIES
UK QUALITY AND OUTCOMES FRAMEWORK
(QOF): SUMMARY OF FINDINGS TO DATE
Quality was improving rapidly before the QOF was introduced
The QOF may have led to a further small, but possibly transient,
increase in quality
In general, the targets seem to have been set at too low a level
The rewards associated with the QOF appear to have been excessive
Only modest evidence that ‘unmeasured’ quality is suffering relative to
measured quality
Evidence of some modest ‘gaming’ to achieve improved scores
Side-benefits of QOF include:
computerization;
better information flow;
more informed patients;
better focus for GPs;
more informed debate on what GPs should do.
Scope of scheme
Comprehensive (QOF)
Piecemeal
Who can enter the scheme?
Voluntary or compulsory? Choice of performance
measures
Structure, process, outcome
Power and size of incentives
Rewards for incremental improvements in quality
Difficulty of targets
Absolute attainment or improvement
External benchmark or relative to other providers
Risk adjustment for disadvantaged populations and other contextual factors
Exception reporting
Avoidance of gaming and other adverse outcomes
Information systems
Audit and penalties
Governance and accountability
Reporting requirements
Monitoring and evaluation
P4P DESIGN ISSUES
Immense variety of P4P schemes, with subtle design
variations and differences in setting
Rarely set up with evaluation in mind
Generally small measured effects
However, benefits in terms of:
Clarifying objectives
Information systems
Accountability
Dialogue between purchasers and providers
Broader public debate
Key issue is to move towards better purchasing, in
which quality plays a more prominent role
SUMMARY OF KEY FINDINGS
Cheryl
Cashin
IMPLICATIONS FOR THE ROLE OF
RBF IN HEALTH PURCHASING AND
PROVIDER PAYMENT
TOWARD A CONCEPTUAL
FRAMEWORK
Indicator/target-based incentive programs have not led to
“breakthrough” improvements in performance and quality
in higher resource settings
where strategic purchasing approaches are already in place.
So, RBF is not an endpoint.
RBF programs can, however, help build the elements of more
strategic health purchasing:
Stronger governance
More focus on specific objectives—clarified output
Better information generation and use
Improved accountability mechanisms
What do the results of the study tell us about
the role of RBF in health purchasing?
Better defined contracts
Stronger purchasing function
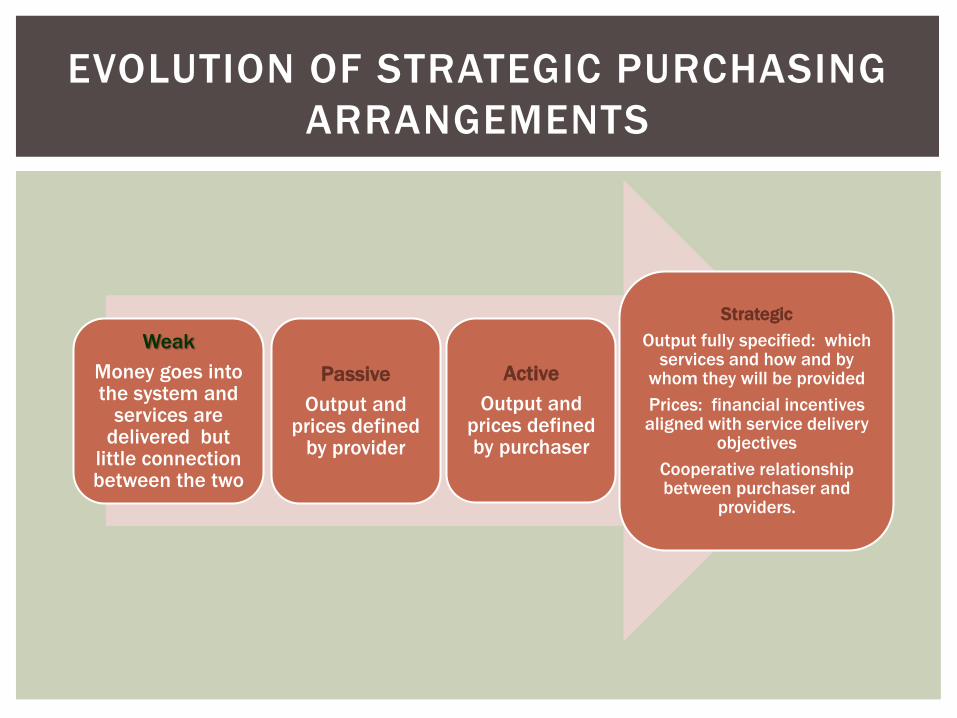
Passive
Output and prices defined
by provider
Active
Output and prices defined by purchaser
Strategic
Output fully specified: which services and how and by
whom they will be provided
Prices: financial incentives aligned with service delivery
objectives
Cooperative relationship between purchaser and
providers.
Weak
Money goes into the system and
services are delivered but
little connection between the two
EVOLUTION OF STRATEGIC PURCHASING
ARRANGEMENTS
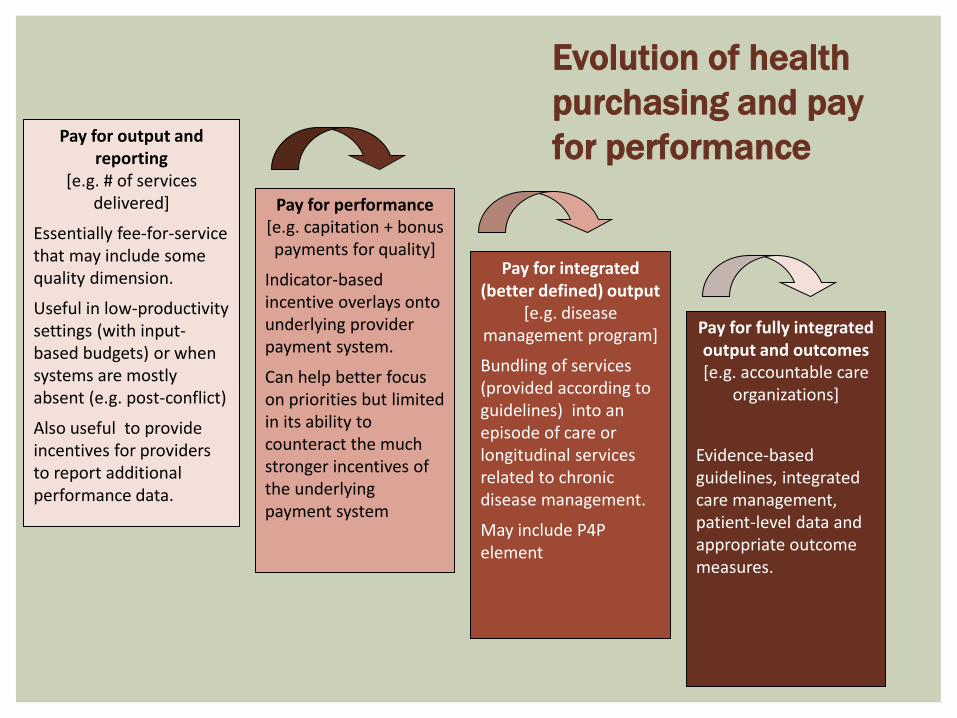
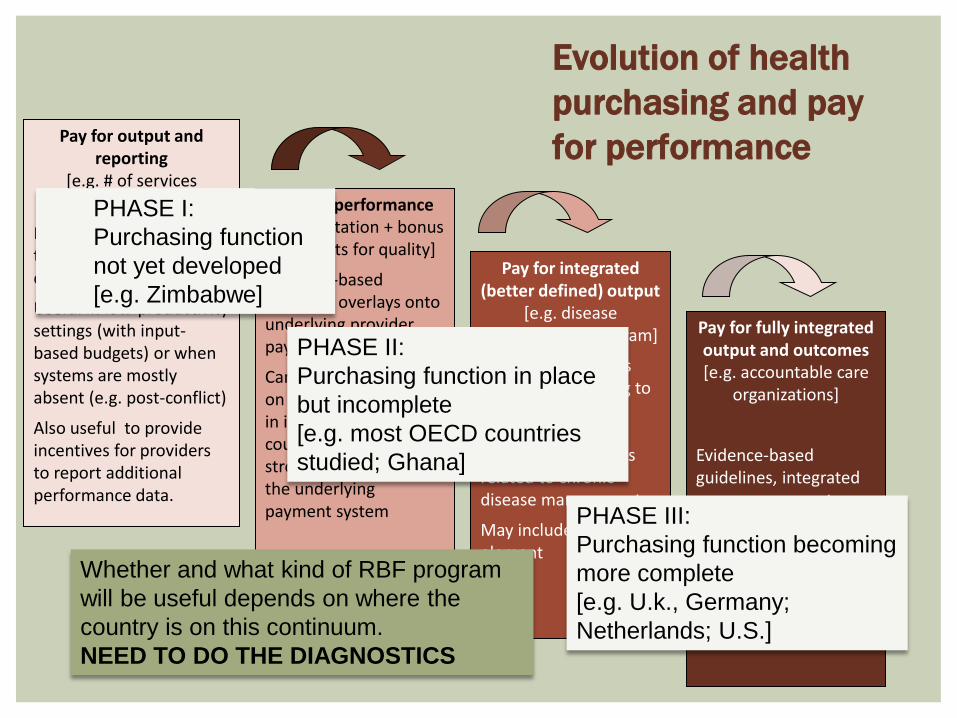
Pay for output and reporting
[e.g. # of services delivered]
Essentially fee-for-service that may include some quality dimension.
Useful in low-productivity settings (with input-based budgets) or when systems are mostly absent (e.g. post-conflict)
Also useful to provide incentives for providers to report additional performance data.
Pay for performance
[e.g. capitation + bonus payments for quality]
Indicator-based incentive overlays onto underlying provider payment system.
Can help better focus on priorities but limited in its ability to counteract the much stronger incentives of the underlying payment system
Pay for integrated (better defined) output
[e.g. disease management program]
Bundling of services (provided according to guidelines) into an episode of care or longitudinal services related to chronic disease management.
May include P4P element
Pay for fully integrated output and outcomes
[e.g. accountable care organizations]
Evidence-based guidelines, integrated care management, patient-level data and appropriate outcome measures.
Evolution of health
purchasing and pay
for performance
Pay for output and reporting
[e.g. # of services delivered]
Essentially fee-for-service that may include some quality dimension.
Useful in low-productivity settings (with input-based budgets) or when systems are mostly absent (e.g. post-conflict)
Also useful to provide incentives for providers to report additional performance data.
Pay for performance
[e.g. capitation + bonus payments for quality]
Indicator-based incentive overlays onto underlying provider payment system.
Can help better focus on priorities but limited in its ability to counteract the much stronger incentives of the underlying payment system
Pay for integrated (better defined) output
[e.g. disease management program]
Bundling of services (provided according to guidelines) into an episode of care or longitudinal services related to chronic disease management.
May include P4P element
Pay for fully integrated output and outcomes
[e.g. accountable care organizations]
Evidence-based guidelines, integrated care management, patient-level data and appropriate outcome measures.
Evolution of health
purchasing and pay
for performance
Whether and what kind of RBF program
will be useful depends on where the
country is on this continuum.
NEED TO DO THE DIAGNOSTICS
PHASE I:
Purchasing function
not yet developed
[e.g. Zimbabwe]
PHASE II:
Purchasing function in place
but incomplete
[e.g. most OECD countries
studied; Ghana]
PHASE III:
Purchasing function becoming
more complete
[e.g. U.k., Germany;
Netherlands; U.S.]
ZIMBABWE
The “Diagnostics”—what are the
main performance problems? Economic and political crises between
2000-2008
35% ↓ in GDP; collapse of basic social
services; ↓ coverage of priority MCH
services; ↓ in health outcomes
Under-utilization and low productivity
RBF program
Performance-based contracts between
NGO (purchaser) and public facilities to
deliver package of priority services
Fee-for-service payments replace user
fees
External verifier for quantity and quality
indicators reported by providers
Example of
“Phase I ”
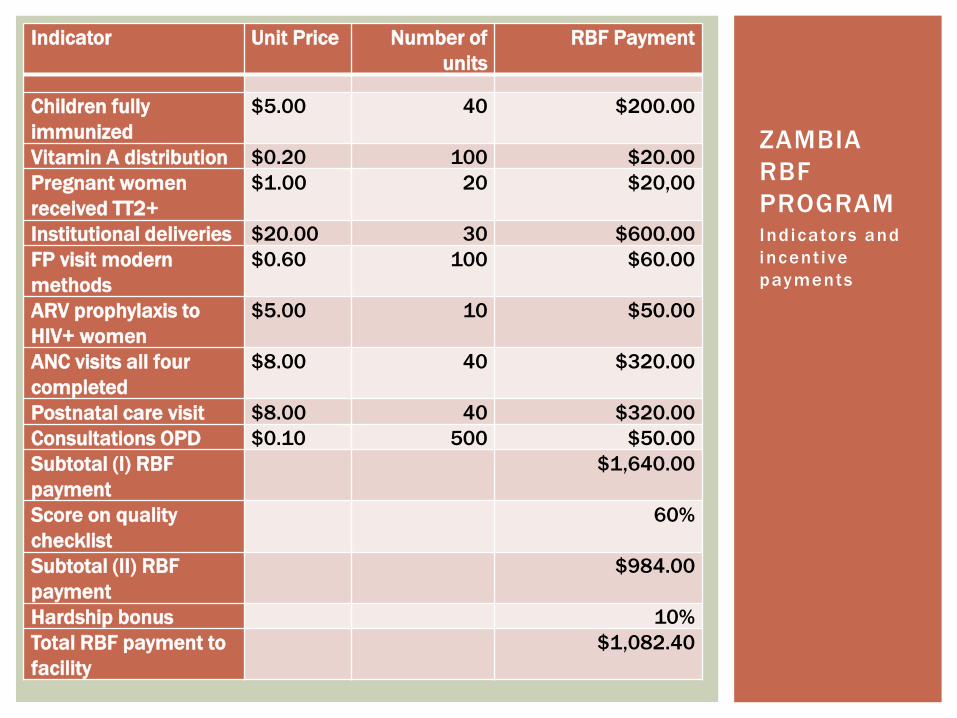
Ind icators and
incent ive
payments
ZAMBIA
RBF
PROGRAM
Indicator Unit Price Number of
units
RBF Payment
Children fully
immunized
$5.00 40 $200.00
Vitamin A distribution $0.20 100 $20.00
Pregnant women
received TT2+
$1.00 20 $20,00
Institutional deliveries $20.00 30 $600.00
FP visit modern
methods
$0.60 100 $60.00
ARV prophylaxis to
HIV+ women
$5.00 10 $50.00
ANC visits all four
completed
$8.00 40 $320.00
Postnatal care visit $8.00 40 $320.00
Consultations OPD $0.10 500 $50.00
Subtotal (I) RBF
payment
$1,640.00
Score on quality
checklist
60%
Subtotal (II) RBF
payment
$984.00
Hardship bonus 10%
Total RBF payment to
facility
$1,082.40
ZIMBABWE
How is RBF building a strategic purchasing function? District Health Executives (DHEs)
supervise outputs and services linked to the package of services
Provincial Health Executives (PHEs) supervise outputs and quality of care at District Hospitals and provide in-service support and mentoring.
Training and capacity-building
What next?—How will Zimbabwe move to Phase II?
The Government sees the need to develop a health financing strategy, which may include social health insurance and innovative instruments like demand side RBF.
Where will the purchasing function “live”?
Example of
“Phase I ”
Example of
“Phase I I ”
GHANA
The “Diagnostics”—what are the main
performance problems?
Strategic purchasing function has been
established in the National Health Insurance
Authority (NHIA)
New output-oriented provider payment systems
(mainly fee-for-service)
Cost escalation (claims/beneficiary)
not bringing the most value for money
Threats to the sustainability of the NHIA
Capitation pilot—but concerns about effect of
incentives on quality and utilization
Quality concerns remain—although salaries have
increased significantly in recent years
How could RBF strengthen the
strategic purchasing function?
Different approaches to RBF are
under discussion
Where RBF could be helpful:
Clarify the output in the contract—which
services and how should they be delivered
Fine-tune incentives of underlying payment
systems
Strengthen the generation and use of
information
Example of
“Phase I I ”
GHANA
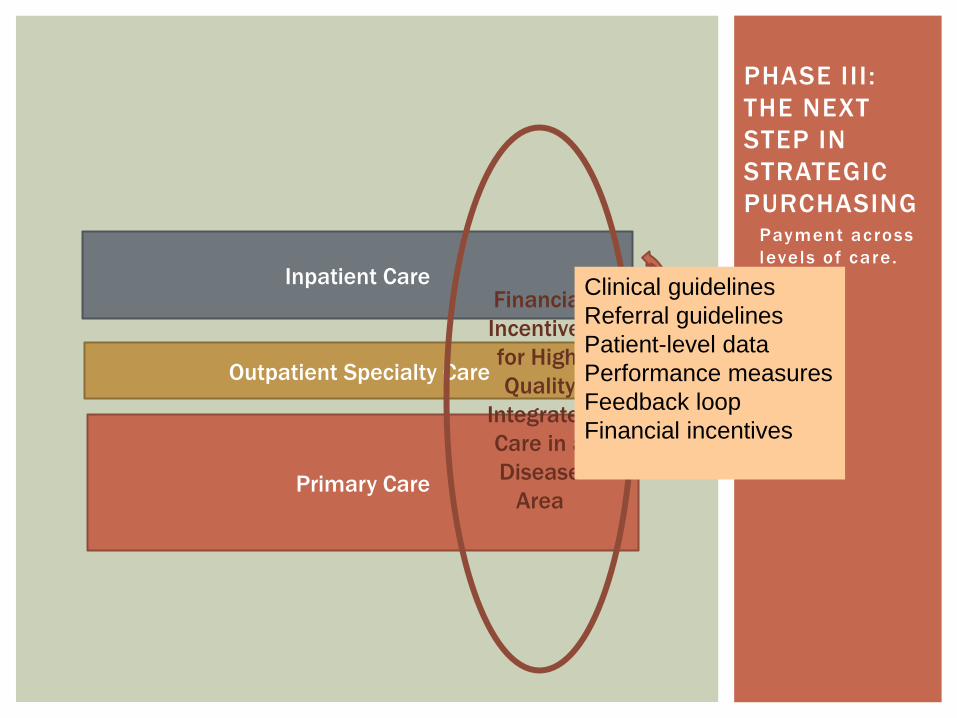
Payment across
levels of care .
PHASE III :
THE NEXT
STEP IN
STRATEGIC
PURCHASING
Primary Care
Outpatient Specialty Care
Inpatient Care Financial
Incentives
for High-
Quality
Integrated
Care in a
Disease
Area
Clinical guidelines
Referral guidelines
Patient-level data
Performance measures
Feedback loop
Financial incentives
Greater
accountability
for results
requires more
integrated
service
delivery
Toward
Strategic
Purchasing
Germany—Disease management programs
place primary care physicians as care
coordinators for patients with chronic
conditions, using financial incentives to
reward better care quality
Netherlands— new “care groups” receive
bundled payments to manage chronic
conditions
U.S.—new “Value -Based Purchasing”
initiatives accompanied by Accountable Care
Organizations and Medical Home models
New Zealand—group practices formed into
Primary Health Organizations to better
address population health needs;
accompanied by P4P for chronic disease
management
RBF programs can be helpful to star t the development of a strategic
purchasing function where none exists
RBF programs can strengthen an existing strategic purchasing
function
E.g. complement traditional payment systems with incentives targeted directly
at specific objectives, such as higher quality processes of care that follow
evidence-based guidelines
But, RBF programs are not an endpoint
The programs should explicitly strengthen strategic health
purchasing to allow continued evolution Do the diagnostics
Build on existing health purchasing and provider payment systems —or have a
plan for where the health purchasing function eventually will “live”
Ensure that governance, information, and accountability mechanisms are
strengthened
KEY ISSUES GOING FORWARD

THANK YOU





























