Embed Size (px)
Citation preview

Ewing’s tumor of the jaw R. E. Wood, DDS, KG,” C. J. Nortje , BChD, PhD,b P. Hesseling, MB, ChB MMed (Paed), MD,’ and F, Grotepass, BChD,d Capetown, Republic of South Africa, and Toronto, Ontario, Canada
UNIVERSITY OF STELLENBOSCH AND ST. MICHAEL’S HOSPITAL
Previous reports have focused on the fact that laminar periosteal new bone is a common radiologic sign of
Ewing’s sarcoma of the jaws. Critical analysis of the literature does not lead to this conclusion. A case is
reported and radiologic appearances described. A review of the literature shows striking clinical and
radiologic similarities to osteogenic sarcoma of the jaws. A differential radiologic interpretation of Ewing’s
sarcoma of the jaws is offered.
(ORALSURG ORALMED ORAL PATHOL 1990;69:120-7)
J ames Ewing in 1921 described a new malignant tumor of endothelial origin.’ This tumor, which bears his name, is now thought to arise from immature reticulum cells or primitive mesenchymal cells of bone marrow.2 It accounts for 4% to 7% of all primary tumors of bone.2 Fifty-six percent of lesions originate in long bones, and two thirds of all lesions are of the lower skeleton.2v3 Bones frequently involved include the femur, ilium, and fibula.3 Occurrence in the jaw bones is comparatively rare, with the jaws accounting for 1 .2%,4 1.3%,5 2.3%,3 2.8%,6 3.8%,7 4%,8 9%,9 and 13%” of all sites. In a survey of primary malignant tumors of the jaw bone, 2 of 19 were Ewing’s tumors.”
Periosteal lamination or “onion-skinning” of the periosteum is said to be a characteristic sign of Ewing’s lesions of long bones.5s’2 In critical reviews of the radiologic features of Ewing’s sarcoma, this has not been borne out. Periosteal onion-skinning was seen in only 4 of 25 patients examined by Swenson.13 Vohra7 stated that onion-skinning was seen in a minority of the 156 cases he reviewed. He also said that in the mandible, the periosteal reaction took the form of sun-ray spicules7 Even in long bones, laminar periosteal reactions were not seen in the absence of other changes suggestive of malignan-
“Oral and Maxillofacial Radiologist, St. Michael’s Hospital, Toronto, Ontario, Canada. bProfessor and Head. Oral and Maxillofacial Radiology: ‘Profes- sor and Head, Pediatrics; and dProfessor and Head, Maxillofacial Surgery, Faculties of Dentistry and Medicine, University of Stellenbosch, Capetown, Republic of South Africa. 7/16/11630
120
CY.~ Modern orthopedic radiology textbooks have recognized this fact. z I4 McCormack and coworkers5 called Ewing’s sarcoma the great imitator of bone pathosis because almost the entire gamut of changes that can occur in bone may be seen. Spjut and coworkers2 state that Ewing’s sarcoma of flat bones has no specific radiologic characteristics. Despite this rather damning evidence to the contrary, text- books of oral pathology and radiology’5-‘7 still main- tain that an onion-skin pattern of periosteal reaction is typical of Ewing’s sarcoma in the jaws. Some dissenting authors have stated that onion-skinning is either uncommon’8~‘9 or excessively rare*O in the jaws.
Although there have been excellent reviews7~2’~22 and case reports, 23-25 no author has examined in detail the reported radiologic features of Ewing’s sarcoma of the jaws. The problem is more than academic since Ewing’s sarcoma is an important differential diagnosis for periostitis reaction associated with mandibular infections.26 The purpose of this review is to examine the literature for reported radiologic features of Ewing’s sarcoma of the jaw bones and present a case that may serve to illustrate some radiologic signs associated with this condition.
MATERIALS AND METHODS
The literature pertaining to Ewing’s sarcomas of the jaws and other bones was reviewed. Specific radiologic observations associated with jaw tumors as stated by authors were recorded, and other find- ings evident in illustrative radiographs were also noted. The literature analyzed consisted of a large series of cases3-9~2'vZ27-30 and caSe reports.",20,23-25.31-5S

Volume 69 Number 1
Ewing’s tumor of jaw 121
Table I. Breakdown of reported sites of Ewing’s sarcoma of the jaws
Mandible Posterior Anterior Unspecified Total
Maxilla Posterior Anterior Unspecified Total
Posterior jaws Anterior jaws Nasal fossa Zygomatic bone Temporal bone Buccai mucosa
No. of sites % of total
30 29.4 5 4.9
31 30.3 66 64.6
12 1 1.8
5 4.9 14 13.7 31 30.4 42 41.1 10 9.8 2 2.0 1 1.0 1 1 .o 1 1.0
Unspecified site in 3 of 105 cases.
The literature was analyzed and cross-indexed to ensure that cases were not counted twice. Informa- tion with respect to clinical, radiologic, and survival features of these patients was tabulated. To this group we add our case report.
CASE REPORT
An 8-year-old white female patient came to her pedia- trician with an 18-day history of facial swelling (Fig. 1). A biopsy performed at that time was interpreted as indicating Burkitt’s lymphoma. Findings from blood studies and chest radiographs were normal. The patient was subsequently referred to the pediatric oncology service at Tygerberg Hospital for consultation. Clinical examination revealed an 8 X 9 cm hard tumor attached to the left side of the mandible. Enlarged firm submandibular lymph nodes were also present.
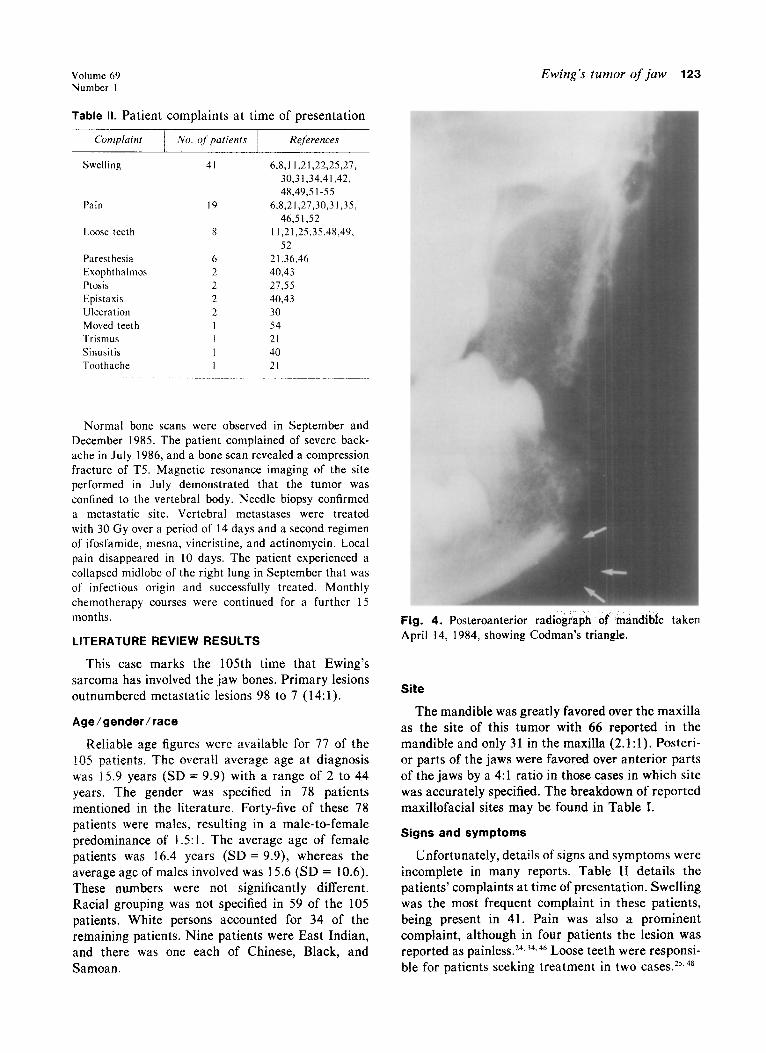
Radiographs taken in April 1984 showed an expansile, permeative, destructive lesion extending from the region of the mandibular left first molar to the condylar neck (Figs. 2 to 4). The lesion was poorly demarcated and uncorticated at its periphery. Its internal structure consisted of multiple discrete polymorphous radiolucent areas ranging in size from 1 m to several millimeters. These zones in turn were surrounded by thin sclerotic margins. The cortex of the follicle of the left second molar was destroyed, and this tooth was pushed anteriorly and superiorly. Cortical destruction was evident at the lower and posterior borders of the left side of the mandible and in the cortex of the mandibular neurovascular canal. The periosteal reaction consisted of sun-ray type spicules emanating from the inferior border of the mandibular body and suggestion of Codman’s triangle at the anterior edge of this site.
In addition to the radiographic examination, further testing was performed. Technetium bone scan revealed that osseous changes were limited to the mandible. Bone
Fig. 1. Clinical photograph of patient at time of presen- tation. Note swelling evident in mandibular angle is on patient’s left.
marrow aspirate, cerebrospinal fluid, abdominal ultra- sound, circulating blood count, skeletal survey, chest radiographs, and liver function studies were all normal. Screening for Epstein-Barr virus was negative. A second biopsy was performed. The tumor consisted of small round closely packed cells somewhat larger than lymphocytes. These cells were arranged in dense sheets although some areas showed nests of cells. Mitotic figures were present but not abundant. The histologic diagnosis was Ewing’s sarcoma. Confirmation of the diagnosis was obtained by means of electron microscopy, which demonstrated char- acteristic changes.
Chemotherapy consisting of sequential vincristine, cyclophosphamide, and doxorubicin hydrochloride (Adria- mycin) as proposed by Chan and coworkersS6 was initiated. In addition to chemotherapy, the patient received 57.5 Gy of cobalt 60 radiation over a period of 4 weeks. Intercur- rent problems consisted of radiation mucositis, abscess of right knee, septicemia, depression, abdominal pain, and measles, which were all successfully treated.
Intratreatment radiographs revealed some resolution in the bone pattern of the mandible (Fig. 5). This was especially evident in the cancellous bone at the angle of the jaw. The inferior and posterior borders of the mandible

122 Wood et al. ORAL SURG ORAL MED ORAL PATHOL January 1990
we] tuti left to 1
198
Fig. 2. Panoramic radiograph of April 14, 1984. Note extent of lesion, its poor definition, and the relative increase in eruption of the second molar tooth on the affected side (arrows).
Fig. 3. Panoramic radiograph of April 14, 1984. The lesion is made up of multiple polymorphous radiolucent areas surrounded by sclerotic margins (small arrows). The large arrow illustrates the sun-ray spiculation. Note also the destruction of the follicular cortex on the right mandibular second molar.
-e better defined at this time. There was some reconsti- resolution of normal internal mandibular architecture ion of the follicular cortex of the second molar, but the normal mandibular shape largely restored. There side of the mandible was still slightly expanded relative complete resolution of the follicular cortex of the se
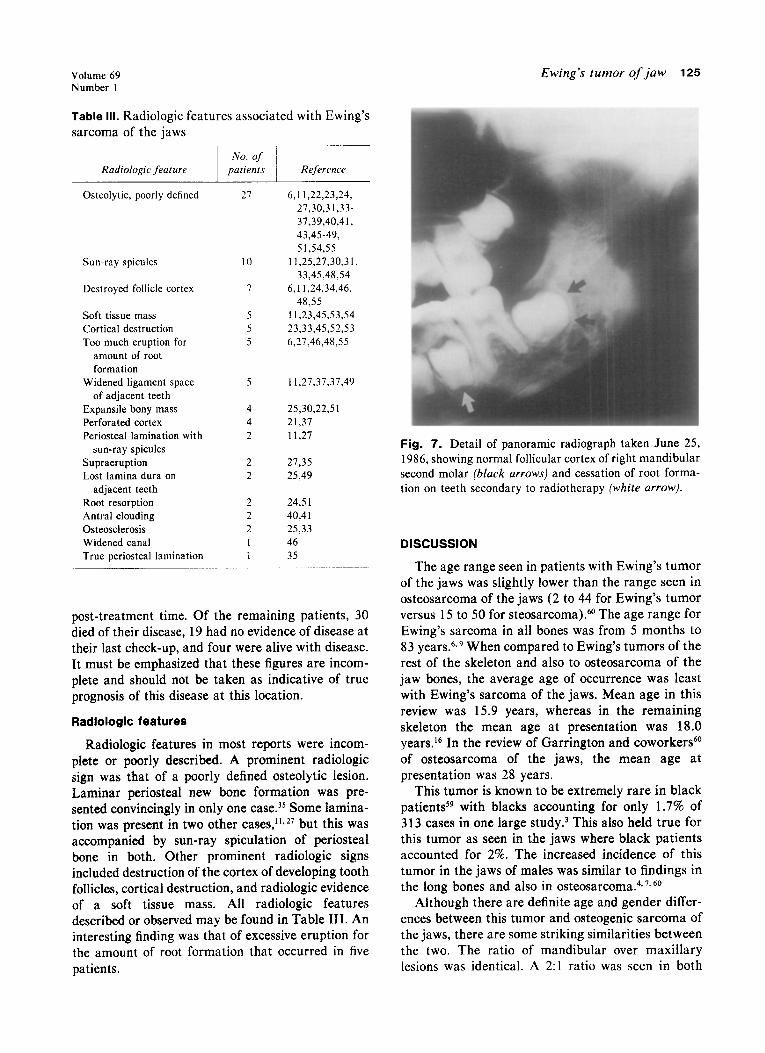
.he patient’s right side. molar and a more normal appearance to the inf The tumor was no longer clinically visible in March mandibular cortex. Root formation on posterior teeth 15. Further radiographs taken in April (Fig. 6) showed halted as seen on radiographs of June 1986 (Fig. 7).
with was
cond erior was
Volume 69 Number 1
Ewing’s tumor of jaw 123
Table II. Patient complaints at time of presentation
Complain1
Swelling
Pain
Loose teeth
Paresthesia Exophthalmos Ptosis Epistaxis Ulceration Moved teeth Trismus Sinusitis Toothache
,Vo. ofpatients References
41 6,8,11,21,22,25,27, 30,31,34,41,42, 48,49,5 1-55
19 6.8,21,27,30,31,35. 46,5 1,52
8 11,21,25.35,48,49. 52
6 21336.46 2 40,43 2 27355 2 40,43 2 30 I 54 I 21 1 40 I 21
Normal bone scans were observed in September and December 1985. The patient complained of severe back- ache in July 1986, and a bone scan revealed a compression fracture of T.5. Magnetic resonance imaging of the site performed in July demonstrated that the tumor was confined to the vertebral body. Needle biopsy confirmed a metastatic site. Vertebral metastases were treated with 30 Gy over a period of 14 days and a second regimen of ifosfamide, mesna, vincristine, and actinomycin. Local pain disappeared in 10 days. The patient experienced a collapsed midlobe of the right lung in September that was of infectious origin and successfully treated. Monthly chemotherapy courses were continued for a further 15 months.
LITERATURE REVIEW RESULTS
This case marks the 105th time that Ewing’s sarcoma has involved the jaw bones. Primary lesions outnumbered metastatic lesions 98 to 7 (14:l).
Age/gender/race
Reliable age figures were available for 77 of the 105 patients. The overall average age at diagnosis was 15.9 years (SD = 9.9) with a range of 2 to 44 years. The gender was specified in 78 patients mentioned in the literature. Forty-five of these 78 patients were males, resulting in a male-to-female predominance of 1.5:1. The average age of female patients was 16.4 years (SD = 9.9), whereas the average age of males involved was 15.6 (SD = 10.6). These numbers were not significantly different. Racial grouping was not specified in 59 of the 105 patients. White persons accounted for 34 of the remaining patients. Nine patients were East Indian, and there was one each of Chinese, Black, and Samoan.
Fig. 4. Posteroanterior radiograph of mandible taken April 14, 1984, showing Codman’s triangle.
Site
The mandible was greatly favored over the maxilla as the site of this tumor with 66 reported in the mandible and only 31 in the maxilla (2.1:1). Posteri- or parts of the jaws were favored over anterior parts of the jaws by a 4:l ratio in those cases in which site was accurately specified. The breakdown of reported maxillofacial sites may be found in Table I.
Signs and symptoms
Unfortunately, details of signs and symptoms were incomplete in many reports. Table II details the patients’ complaints at time of presentation. Swelling was the most frequent complaint in these patients, being present in 41. Pain was also a prominent complaint, although in four patients the lesion was reported as painless. 24, 34. 46 Loose teeth were responsi- ble for patients seeking treatment in two cases.25,48

124 Wood et al. ORAL SURG ORAI MED ORAL PATHOL
January 1990
Fig. 5. Panoramic radiograph of August 29, 1984, showing partial resolution of normal mandibular architecture.
Fig. 6. Panoramic radiograph of June 25, 1986. Note relative sclerosis of bone on affected side and reconstitution of normal size.
Treatment Survival
TIGLIL~UCIIL iIlc;iu&J burger-y, chemotherapy, and The range of survivai in patients reviewed in this radiotherapy alone, and in varying combinations. report was from 12 days to 17 years.4, 25 There were Discussion of the treatment modalities is beyond the no follow-up data provided on 50 patients, and two scope of this article. patients were lost to follow-up after a specified
Volume 69 Number 1
Table III. Radiologic features associated with Ewing’s sarcoma of the jaws
Radiologic feature No. of
patients Reference
Osteolytic, poorly defined
Sun-ray spicules
Destroyed follicle cortex
Soft tissue mass Cortical destruction Too much eruption for
amount of root formation
Widened ligament space of adjacent teeth
Expansile bony mass Perforated cortex Periosteal lamination with
sun-ray spicules Supraeruption Lost lamina dura on
adjacent teeth Root resorption Antral clouding Osteosclerosis Widened canal True periosteal lamination
21
10
I
5
5
5
5
4
4
2
2
2
2
2
2
1
1
6,l I ,22,23,24, 27,30,31,33-
37,39,40,41,
43,45-49,
51.54.55
11.25,27,30.3 I. 33,45,48,54
6,11,24,34,46,
48,55
11,23,45,53,54 23,33,45,52,53
6,27,46,48,55
11,27,37,37,49
25,30,22,51
21,37
11,27
27,35
25,49
24.51
40.41
25.33
46
35
post-treatment time. Of the remaining patients, 30 died of their disease, 19 had no evidence of disease at their last check-up, and four were alive with disease. It must be emphasized that these figures are incom- plete and should not be taken as indicative of true prognosis of this disease at this location.
Radiologic features
Radiologic features in most reports were incom- plete or poorly described. A prominent radiologic sign was that of a poorly defined osteolytic lesion. Laminar periosteal new bone formation was pre- sented convincingly in only one case.3’ Some lamina- tion was present in two other cases,11+27 but this was accompanied by sun-ray spiculation of periosteal bone in both. Other prominent radiologic signs included destruction of the cortex of developing tooth follicles, cortical destruction, and radiologic evidence of a soft tissue mass. All radiologic features described or observed may be found in Table III. An interesting finding was that of excessive eruption for the amount of root formation that occurred in five patients.
Ewing’s tumor of jaw 125
Fig. 7. Detail of panoramic radiograph taken June 25, 1986, showing normal follicular cortex of right mandibular second molar (black arrows) and cessation of root forma- tion on teeth secondary to radiotherapy (white arrow).
DISCUSSION
The age range seen in patients with Ewing’s tumor of the jaws was slightly lower than the range seen in osteosarcoma of the jaws (2 to 44 for Ewing’s tumor versus 15 to 50 for steosarcoma).60 The age range for Ewing’s sarcoma in all bones was from 5 months to 83 years.6,g When compared to Ewing’s tumors of the rest of the skeleton and also to osteosarcoma of the jaw bones, the average age of occurrence was least with Ewing’s sarcoma of the jaws. Mean age in this review was 15.9 years, whereas in the remaining skeleton the mean age at presentation was 18.0 years.r6 In the review of Garrington and coworker@” of osteosarcoma of the jaws, the mean age at presentation was 28 years.
This tumor is known to be extremely rare in black patients5q with blacks accounting for only 1.7% of 313 cases in one large study.3 This also held true for this tumor as seen in the jaws where black patients accounted for 2%. The increased incidence of this tumor in the jaws of males was similar to findings in the long bones and also in osteosarcoma.4,7*60
Although there are definite age and gender differ- ences between this tumor and osteogenic sarcoma of the jaws, there are some striking similarities between the two. The ratio of mandibular over maxillary lesions was identical. A 2:l ratio was seen in both
126 Wood et al.
tumors.60 The localization of this tumor in the posterior portion of the mandible may be an indica- tion of its genesis from marrow constituents. Another common denominator between osteosarcoma and Ewing’s tumor would be the symptoms at presenta- tion. Both lesions presented with almost exactly the same symptoms. Swelling was seen most commonly followed by pain, loose teeth, and paresthesia.60 Pain was more common than swelling in long bone lesions, which may be the result of associated weight-bearing stresses on these bones.37
Table III shows that laminar periosteal response by itself is not a feature of this disease in the jaw bones. This agrees with statements of Ewing’s tumor’s effects on flat bones as outlined by Spjut and coworkers.2 A report of jaw lesions having laminated type of periosteal reaction contains no convincing case of this appearance. 27 We stated that periosteal laminations are difficult to demonstrate in the jaws because of complex anatomy. This does not seem to be the case in most instances.26 This is not to say that laminar periosteal reaction never occurs but rather that it is not common. What is a common radiologic presentation is that of a poorly defined osteolytic lesion, which may have associated sun-ray spicules of periosteal bone. Other common radiologic signs include presence of a soft tissue mass adjacent the destructive site and destruction of cortices of follicles of unerupted teeth. It is always dangerous to rely on a single radiologic sign in the interpretation of radiographs. All of the radiograph must be examined in detail, all observations recorded, and consideration given to the significance of these observations. Sun- ray type radiographic appearance is seen in eight other conditions, multiple ill-defined radiolucent areas in at least five, destroyed follicular cortices in eleven, soft tissue masses adjacent destruction in fourteen, and widened periodontal ligaments in at least nineteen.61
A differential diagnosis listing of this condition in the long bones is offered by Wilmer.12 Conditions of the jaws that from a radiologic point of view may be mistaken for this condition include osteogenic sarco- ma, neuroblastoma, lymphosarcoma, histiocytosis X, rhabdomyosarcoma, pyogenic osteomyelitis, and metastatic carcinoma.
The prognosis of patients with isolated Ewing’s sarcoma is not good. Chan and coworkers56 state that a significant increase in local control of the lesions is afforded by a combination of chemotherapy and ra~;n+hpr~n~~ hl~+ the main problem in this lesion is 1 r the management of distant metastases. Five-year survival rates are not good.58
ORAL SURC ORAL MED ORAL PATHOL January 1990
We thank the photography department of the Faculty of
Dentistry, University of Stellenbosch, and Ms. J. Murray- Wood and Ms. S. Roberts for preperation of the manu-
script.
REFERENCES
1.
2.
3.
4.
5.
6.
I.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
Ewing J. Diffuse endothelioma of bone. Proc NY Path01 Sot 1921;21:17-24. Spjut HJ, Dorfmann HD, Fechner RF, Ackerman LV. AFIF fascicle 5: tumors of bone and cartilage. Bethesda, Maryland: American Forces Institute of Pathology, 1970:216-22.. Kissawe JM. Askin FB. Foulkes M. Stratton LB. Shirlev SF. Ewing’s sarcoma of bone. Hum Paihol 1983;14:?73-9. ’ Dahlin DC, Coventry MB, Scanlon PW. Ewing’s sarcoma: a critical analysis of 165 cases. J Bone Joint Surg 1961; 43(A):185-92. McCormack LJ, Dockerty MB, Ghormley RK. Ewing’s sarcoma. Cancer 1952;5:85-99. Bhansali SK, Desai PB. Ewing’s sarcoma: observations on 107 cases. J Bone Joint Surg 1963;45(A):541-53. Vohra VG. Roentgen manifestations in Ewing’s sarcoma. Cancer 1967;20:727-33. Wang CC, Schulz MD. Ewing’s sarcoma. N Engl J Med 1957;248:571-5. Falk S, Alpert M. The clinical and roentgen aspects of Ewing’s sarcoma. Am J Med Sci 1965;250:492-508. Geschickter CF, Copeland M. Tumors of bone. 2nd ed. Philadelphia: JB Lippincott, 1936:381-440. Burford WN, Ackerman LV. Symposium on nineteen cases of benign and malignant lesions from the oral cavity from the Ellis Fischel State Cancer Hospital, Columbia Missouri- Vol. II. Am J Orthod 1945;31:541-74. Wilmer D. Radiology of bone tumors and allied disorders. Philadelphia: WB Saunders, 1982:225 1. Swenson PC. The roentgenologic aspects of Ewing’s tumor of bone marrow. AJR 1943;50:343-54. Edeiken J, Hodes PJ. Roentgen diagnosis of diseases of bone. 3rd ed. Baltimore: Williams & Wilkins, 1983:280-2. Goaz PW, White SC. Oral radiology: principles and interpre- tation. St. Louis: CV Mosby, 198%li2. . Shafer WG. Hine MK. Levv BM. A textbook of oral Dathol- ogy. 4th ed. Philadelphia: GB Saunders, 1983:177-S.’ Lucas RB. Pathology of tumours of the oral tissues. 3rd ed. London: Churchill Livingstone, 1976:260. Pindborg JJ, Hjorting-Hansen E. Atlas of diseases of the jaws. Philadelphia: WB Saunders, 1974:36.
19. Worth HM. Principles and practice of oral radiologic inter- pretation. Chicago: Year Book Medical Publishers, 1963: 580-l.
20. Baker CG, Tishler JM. Malignant disease in the jaws. J Can Assoc Radio1 1977;28:129-41.
21. Arafat A, Ellis GL, Adrian JC. Ewing’8 sarcoma of the jaws. ORAL SURG ORAL MED ORAL PATHOL 1983;55:589-96.
22. Rota AN. Smith JL. MacComb WS. Jine B. Ewing’s Y - - -0 -
sarcoma of the maxilla and mandible. ORAL SURG ORAL MED ORAL PATHOL 1968;25:194-203.
23. Bacchini P, Marchetti C, Mancini L, Present D, Bertoni F. Ewing’s sarcoma of the mandible and maxilla. ORAL SURG ORAL MED ORAL PATHOL 1986;61:278-83.
24. Hardy P, Gibbs AR. Ewing’s sarcoma of the mandible. Br J Oral Surg 1984;22:287-94.
25. Oehlers FAC. A case of Ewing’s tumor with primary lesion in the mandible. Br Dent J 195&88:146-50. - _
26. Eversole LR. Leider AS. Corwin JO. Karian B. Proliferative periostitis of GarrB: its differentiation from other neoperios- toses. J Oral Surg 1979;37:725-3 1.
27. de Santos LA, Jing BS. Radiographic findings of Ewing’s sarcoma of the jaws. Br J Radio1 1978;51:682-7.

Volume 69 Number I
28.
29.
30.
31.
32.
33.
34.
35.
36.
31.
38.
39.
40.
41.
42.
43.
44.
4s.
46.
41.
Lindberg R. Unusual malignant tumors of the head and neck. Radiology 1966;86:1090-5. Macintosh DJ, Price G, Jeffree GM. Ewing’s tumour: a study of behaviors and treatment in 47 cases. J Bone Joint Surg 1975;57(B):331-40. Potdar GG. Ewing’s tumors of the jaws. ORAL SURG ORAL MED ORAL PATHOL 1970;29:505-1 2. Bernstein PE, Bone RC, Feldman PS. Ewing’s sarcoma of the mandible. Ann Otol Rhino1 Laryngol 1979;88:105-8. Blakemore JR, Stein M. Primary Ewing’s sarcoma of the mandible: report of case. J Oral Sure 1975:33:376-9. Borhelli RF,‘Barros RE, Zampieri J-Ewing’s sarcoma of the mandible: report of case. J Oral Surg 1978;36:423-5. Brownson RJ, Cook RP. Ewing’s sarcoma of the maxilla. Ann Otol Rhino1 Laryngol 1969;78: l299- 1304. Carl W, Schaaf NC, Gaeta J, Sinks LF. Ewing’s sarcoma. ORAL SURG ORAL MED ORAL PATHOL 197 1;31:472-8. Crowe WW. Ewing’s sarcoma with primary lesion in mandi- ble: report of case. J Oral Surg 1965;23: 156-6 1. Damm DD, White DK, Drummond JF, Ferretti GA. Ewing’s tumor of the jaws. Pediatr Dent 1985;7:57-60. Dehner LP. Tumors of the mandible and maxilla in children. Cancer 1973;32:112-20. Dieckmann J, Fischedick 0. Zur Klinik, Diagnostik und Terapie, des Ewing-Sarkom in Gesichtsshadelbereich. Dtsch Zahnaerztl Z 1976;31:254-6. Ferlite A. Primary Ewing’s sarcoma of the maxilla: a clinico- pathological study of the cases. J Laryngol Otol 1978; 92:1007-24. Hunsuck EE. Ewing’s sarcoma of the maxilla. ORAL SURG ORAL MED ORAL PATHOL 1968;25:923-8. Khanna S, Khann NN. Primary tumors in the jaws in children. J Oral Surg 1979;37:800-4. Konray RR, Crissman JD. Pathologic quiz case 2. Arch Otolaryngol 1979;105:108-9. Prowisionato A. Reticula-sarcoma e Sarcoma di Ewing Primitivi dell Osso Mandibolare. Arch Ital Pat Tumori 1958; 11:248-64. Rapoport A, Sobrinho J, Carvalho M, Magrin J, Costa F, Quadros J. Ewing’s sarcoma of the mandible. ORAL SURG ORAL MED ORAL PATHOL 1977;44:89-94. Salman 1, Darlington G. Rare (unusual) malignant tumors of the jaws. Am J Orthod 1944;30:725-40. Schill W, Eschler J. Bijsartge Kiefertumoren bei Kindern und Jugendlichen. Dtsch Zahnaerztl Z 1969;24:286-8.
48
49
50
51
52
53
54.
55.
56.
57.
58.
59.
60.
61.
Ewing’s tumor of jaw 127
Som PM, Hermann G, Krespi Y, Shugar J. Ewing’s sarcoma of the mandible. Ann Otol Rhino1 Laryngol 1980;89:20-3. Weir JC, Amorett MR, Krolls SO. Tumorous conditions of the fibula, supraorbital area, and mandible. J Oral Pathol 1979;8:313-8. Wiederhold A, Carmona I. Un Caso de Tumor de Ewing de Los Maxilares en ei Nino. Rev Med Cordoba. 1952;40:97- 102. Sidu SS, Parkash H, Subherwal GL. Ewing’s sarcoma of the mandible. J Dent 1976;4:227-30. Zamor J. Ewing’s sarcoma of the mandible. Mt Sinai J Med (NY) 1982;49:352-4. Lam KH, Wong J. Lim STK, Ong GB. Primary sarcomas of the jaw. Aust NZ J Surg 1979;49:668-75. Smith F. Ewing’s sarcoma of the mandible. NZ Med J 1958;57:465-7. Kelly JR, Barr ES. Ewing’s sarcoma with involvement of the head and neck. J Dent Child 1976;43:423-6. Chan RC, Sutow WW, Lindberg RD, Samuels ML, Murray JA, Johnston DA. Management and results of localized Ewing’s sarcoma. Cancer 1979;43:1001-6. Mahoney JP, Alexander RW. Ewing’s sarcoma--a light and electron microscopic study of 21 cases. Am J Surg Pathol 1978;2:283-98. Falk S, Alpert M. Five-year survival rates of patients with Ewing’s sarcoma. Surg Gynecol Obstet 1967;124:319-24. Fraumeni JF, Glass AC. Rarity of Ewing’s sarcoma among U.S. Negro children. lancet 1970;1:366-7. Garrington GE, Scofield HH, Cornyn J, Hooker SP. Osteo- sarcoma of the jaws: analysis of 56 cases. Cancer 1967; 20:377-91. Wood RE, Pharoah MJ, Nortje CJ, Stoneman DW, Farman AC. Handbook of signs in dental and maxillofacial radiolo- gy. Toronto; Warthog Publications, 1988.
Reprint requests to:
Dr. R. E. Wood Dental Clinic St. Michael’s Hospital 30 Bond St. Toronto, Ontario, Canada M5B 1 W8