Embed Size (px)
Citation preview
Therapeutics, Targets, and Chemical Biology
Ex Vivo Explant Cultures of Non–Small Cell LungCarcinoma Enable Evaluation of Primary TumorResponses to Anticancer TherapyEllie Karekla1,Wen-Jing Liao1, Barry Sharp2, John Pugh2, Helen Reid2,John Le Quesne1,3, David Moore1, Catrin Pritchard1, Marion MacFarlane3,and James Howard Pringle1
Abstract
To improve treatment outcomes in non–small cell lung cancer(NSCLC), preclinical models that can better predict individualpatient response to novel therapies are urgently needed. Usingfreshly resected tumor tissue, we describe an optimized ex vivoexplant culture model that enables concurrent evaluation ofNSCLC response to therapy while maintaining the tumor micro-environment. We found that approximately 70% of primaryNSCLC specimens were amenable to explant culture with tissueintegrity intact for up to 72 hours. Variations in cisplatin sensi-tivity were noted with approximately 50% of cases responding exvivo. Notably, explant responses to cisplatin correlated signifi-cantly with patient survival (P ¼ 0.006) irrespective of tumor
stage. In explant tissue, cisplatin-resistant tumors excluded plat-inum ions from tumor areas in contrast to cisplatin-sensitivetumors. Intact TP53 did not predict cisplatin sensitivity, but apositive correlation was observed between cisplatin sensitivityand TP53 mutation status (P ¼ 0.003). Treatment of NSCLCexplants with the targeted agent TRAIL revealed differential sen-sitivity with the majority of tumors resistant to single-agent orcisplatin combination therapy. Overall, our results validated arapid, reproducible, and low-cost platform for assessing drugresponses in patient tumors ex vivo, thereby enabling preclinicaltesting of novel drugs and helping stratify patients using bio-marker evaluation. Cancer Res; 77(8); 2029–39. �2017 AACR.
IntroductionNon–small cell lung cancer (NSCLC) is a leading cause of
cancer death worldwide. Patients with stage I–III tumors aresurgically resected and given adjuvant chemotherapy or radio-therapy. Patients with stage IV disease receive palliative chemo-therapy only unless they can be stratified for targeted therapy.Most patients receive combination chemotherapy based on clin-ical parameters of cisplatin or carboplatin with at least one otherdrug such as vinorelbine, gemcitabine, or paclitaxel. Unfortunate-ly, only approximately 5% of patients receiving adjuvant therapyshow 5-year average survival benefit (1, 2). Therefore, moreaccurate methods for predicting chemotherapeutic benefit areurgently required to improve clinical outcomes.
The era of personalized medicine has heralded the develop-ment of targeted therapies for NSCLC, some of which rely onpreselection of cancers according to genetic mutation. Forexample, selective EGFR inhibitors gefitinib and erlotinib pro-vide clinical benefit over standard chemotherapy for NSCLCtumors bearing EGFR mutations (3, 4), whereas the ALK inhib-itor crizotinib benefits ALK-mutated cases (5). A global industryis centered on assessing additional mono- or combinatorialtreatments in NSCLC clinical trials. Despite this momentum,late-stage failures are a reality and there is less than 11% successin bringing a drug to market (6), attributable in part to non-predictive preclinical drug platforms (7, 8). The incorporationof patient-derived xenograft (PDX) mouse models (9, 10) intopreclinical studies has improved predictive accuracy somewhat(11, 12). However, PDX efficacy studies are expensive, requiringlarge numbers of mice. Furthermore, not all primary humantumors generate PDXs and, of those that do, serial propagationcan select tumors that adapt to grow in an immunocompro-mised environment.
An alternative approach is to use 3-dimensional ex vivo cul-ture of fresh human tumors. Methods for ex vivo culture ofhuman tumors have been available for many years, and evi-dence shows that they can reliably reflect tumor growth in vivo(13–19). Here, we have developed and perfected an ex vivoculture method for NSCLC tumor samples that is both simpleand reproducible. We have optimized culture conditions andshow that tumor and stroma are retained intact and are viable.As proof-of-concept, NSCLC explant response to the standard-of-care chemotherapy drug cisplatin was examined, as well asresponse to the targeted agent TRAIL. We also illustrate how
1Department of Cancer Studies, University of Leicester, Leicester, United King-dom. 2Centre for Analytical Science, Department of Chemistry, LoughboroughUniversity, Loughborough, Leicestershire, United Kingdom. 3MRC ToxicologyUnit, Leicester, United Kingdom.
Note: Supplementary data for this article are available at Cancer ResearchOnline (http://cancerres.aacrjournals.org/).
C. Pritchard, M. MacFarlane, and J.H. Pringle contributed equally to this article.
Corresponding Authors: Catrin Pritchard, Department of Cancer Studies, Uni-versity of Leicester, Lancaster Road, Leicester LE1 9HN, United Kingdom. Phone:4411-6229-7061; Fax: 4411-6229-7018; E-mail: [email protected]; and Marion Mac-Farlane, MRC Toxicology Unit, Hodgkin Building, Lancaster Road, Leicester LE19HN, United Kingdom. E-mail: [email protected]
doi: 10.1158/0008-5472.CAN-16-1121
�2017 American Association for Cancer Research.
CancerResearch
www.aacrjournals.org 2029
on January 20, 2020. © 2017 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 15, 2017; DOI: 10.1158/0008-5472.CAN-16-1121

explants can be used to inform mechanisms of drug action byevaluating biomarkers of drug response. Together, our datashow that the explant platform can effectively predict patientresponse to therapy and can be used for monitoring clinicallyrelevant biomarkers.
Materials and MethodsEx vivo explant culture
Fresh NSCLC tumors were collected from consented patientsundergoing lung surgery (Ethical approval: LREC: 07/MRE08/ 07).Patients had no prior exposure to chemotherapy. Viable tumorareas were identified by frozen tissue sectioning and hematoxylinand eosin (H&E) staining. Tissue was placed inHank balanced saltsolution and cut into fragments of 2 to 3 mm3 using 2 skin graftblades on a dental wax surface. These were placed in fresh culturemedia (DMEM with 4.5 g/L glucose þ 0%–5% FCS and 1% pen/strep); 9 fragmentswere randomly selected andplacedona 0.4-mmculture insert disc (Millipore) floated on 1.5 mL of media in a6-well dish. Explants were incubated at 37�Cand 5%CO2 for 16 to20 hours. Discs were then transferred to new wells containing1.5-mL freshmedia, anddrugsor carrier controlwere added toeachwell in a volume of 1.5 mL for 24 hours. Cisplatin (Sigma) wasutilized over a dose range of 0 to 50 mmol/L (dissolved indimethylformamide). TRAIL (20, 21) was utilized at 1 mg/mL,diluted inDMEMmedia from a stock of 1mg/mL. After treatment,explants were washed with PBS and transferred to new wellscontaining 1 mL of 4% (w/v) paraformaldehyde for 20 hours.Explants were transferred onto sponges, pre-soaked in 70% (v/v)ethanol, and placed in histology cassettes. They were embeddedinto paraffin blocks from which 4-mm sections were generated.
Histologic analysisH&E staining of formalin-fixed, paraffin-embedded (FFPE)
material sections was generated by standard approaches and, forimmunohistochemistry (IHC), sections were processed asdescribed (22). The Novolink Polymer Detection System Kit(Leica Microsystems) was used according to the manufacturer'sinstructions. Primary antibodies were: cleaved PARP [E51]:Abcam 1:6,000, Ki67 Clone MIB-1: DAKO 1:2,000, p53 DO1:gift from David Lane 1:1,000, cytokeratin clone MNF116: DAKO1:5,000. Antibodies were diluted in blocking solution made with3% (w/v) BSA, 0.1% (v/v) Triton X-100 (Fisons) in TBS. Stainingwas visualized under a LEICA DM 2500 microscope and photo-graphed with a LEICA DFC 420 camera.
Quantitation of IHC stainingImages of the tumor explants were taken at 10�magnification
and merged using Adobe Photoshop CS5.1, generating a singleimage of one explant. Tumor area was determined using ImageJanalysis (23), excluding areas of necrosis and stroma. The labelingindex was determined using ImmunoRatio (24), and a singlevalue was obtained for all 9 explants derived from one treatmentthat was expressed as a percentage of the total tumor area.
Laser ablation inductively coupled plasma mass spectrometrySections of explants treated with cisplatin were subjected to
Laser ablation inductively coupled plasma mass spectrometry(LA-ICP-MS) to produce elemental maps showing the spatialdistribution of platinum in tissue sections (25). The method isdescribed in Supplementary Fig. S1.
Statistical analysisSignificance of proliferation/death indices was determined
by Wilcoxon matched pairs test and Jonckheere–Terpstra trendtest, respectively. Unpaired data were compared by the Mann–Whitney U test or Kruskal–Wallis one-way ANOVA. Paired datawere analyzed by the Page L test (Unistat Statistical Package,version 5.0, Unistat), and interrelationships were investigatedby Spearman rank correlation (SPSS, version 22, IBM). Theoptimal cutoff point to determine the relationship betweenexplant response and patient survival was examined using aplot of sensitivity against 1 � specificity as a receiver operatorcharacteristic (ROC) curve (SPSS). Survival was investigated byKaplan–Meier analysis (SPSS) of cell indices, which were com-pared by the log-rank Mantel–Haenszel (Peto) test, and byunivariate and multivariate Cox regression (SPSS). P < 0.05 wasconsidered statistically significant.
ResultsHistopathology of NSCLC tumors used for explants
Table 1 provides a summary of patient demographics, tumortype, and stage for all 45 samples utilized for this study. Thehistologic types and stages were broadly consistent with theknown distribution of NSCLC cases in the United Kingdom(26). A proportion of NSCLC tumors is known to be necrotic(27), and an important first step was to exclude such tumors fromanalysis using H&E assessment. This led to the identification of13 tumors (�29%) that were excluded from explant generation.Supplementary Fig. S2 indicates the histologic type (Supplemen-tary Fig. S2A) and stage (Supplementary Fig. S2B) of viable andnonviable tumors. The highest proportion of nonviable tumorswas within the adenocarcinoma subtype [�36% compared with�25% of squamous cell carcinoma (SCC) cases]. However, therewas no correlation between tumor stage and viability.
Thirty-two viable tumors were processed for explant culture.Intrinsic levels of cell proliferation and cell death were firstassessed in uncultured samples by Ki67 or cleaved PARP (cPARP)
Table 1. Summary of patients' characteristics and tumors used for this study
Characteristic Number (%) of patients/tumors
SexMale 25 (55.6)Female 20 (44.4)
AgeMedian 70Range 54–85
HistologyAdenocarcinoma 22 (48.9)SCC 20 (44.4)Large cell carcinoma 0 (0)Atypical carcinoid 3 (6.7)
StageIA 7 (15.6)IB 8 (17.8)IIA 8 (17.8)IIB 9 (20)IIIA 11 (24.4)IIIB 1 (2.2)IV 1 (2.2)
NOTE: Tumor samples were collected from consented patients undergoinglung surgery at Glenfield Hospital, Leicester. Clinical data, histology, andstage were provided by official histopathologic reports submitted by con-sultant pathologists at University Hospitals of Leicester, Leicester, UK.
Karekla et al.
Cancer Res; 77(8) April 15, 2017 Cancer Research2030
on January 20, 2020. © 2017 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 15, 2017; DOI: 10.1158/0008-5472.CAN-16-1121

immunostaining (Fig. 1A and B). SCC tumors displayed signif-icantly higher levels of proliferation than adenocarcinoma,whereas atypical carcinoid tumors were essentially indolent (Fig.1A). These observations are consistent with several previousreports (28–30). With regard to cPARP staining, the majority ofsamples showed less than20%of staining, indicating low levels ofintrinsic cell death (Fig. 1A and B).
Optimization of explant cultureOur approach for the NSCLC explant culture system was based
on previous experience with breast cancer samples (MacFarlane,unpublished observations; ref. 31; ). As a first step in implement-ing protocols forNSCLC, we first investigated the effects of culturetime and FCS concentration.
Explants were routinely allowed to recover for a period of16 to 20 hours after their initial generation; viability wasassessed over a time range of 24 to 72 hours after recovery for5 tumors. As shown in Fig. 2A, a trend of decreasing cellproliferation and increasing cell death with increasing time ofculture was observed, suggesting ex vivo explant cultures aremore viable in short-term culture. Varying FCS concentration,from 0% to 5%, at 24 hours of culture after the initial 16 to20 hours of culture recovery showed no statistically significantdifference in levels of proliferation or cell death (Fig. 2B).
The data from above suggest that the 24-hour time point givesthe greatest viability but that FCS concentration is not a signi-ficant factor. Subsequent analyses of drug responses were there-fore performed for 24 hours, using 1% as the standard FCS
B
cPARPKi67
LT103
LT98
LT104
A%
Lab
elin
g in
dex
Ki67 +ve cPARP +ve0
20
40
60
80
100
L
M
H
% K
i67
+ve
ACSCCADC0
20
40
60
80
100
P = 0.003
% c
PAR
P +v
e
ACSCCADC0
20
40
60
80
100
Figure 1.
Intrinsic levels of proliferation and apoptosis in the tumors used for explants. A, Proliferation was assessed by quantitating Ki67 IHC staining and celldeath by quantitating cPARP staining. Left, percentage of intrinsic proliferation and cell death in tumors. A single dot represents a single tumor sample. Forthe Ki67 staining, the samples were grouped into 1 of 3 groups: H, high (>40%); M, medium (20%–40%); L, low (0%–20%). The samples all had lowintrinsic levels of cPARP staining. Middle and right, percentage of Ki67 and percentage of cPARP staining for tumors with adenocarcinoma (ADC), SCC,and atypical carcinoid (AC) histologies. The SCC samples had significantly higher levels of intrinsic proliferation compared with the adenocarcinomasamples whereas, the atypical carcinoid samples were indolent. Cell death levels were consistent across the histologies. B, Representative images of Ki67(left) and cPARP (right) IHC staining of high (LT103; top), medium (LT98; middle), and low (LT104; bottom) proliferative tumors. IHC stains werecounterstained with hematoxylin. LT103 (high proliferative tumor) and LT98 (medium proliferative tumor) represent SCC samples, whereas LT104 (lowproliferative tumor) is an adenocarcinoma. Scale bars, 100 mm.
Assessing Tumor Drug Response with a Novel Ex Vivo Platform
www.aacrjournals.org Cancer Res; 77(8) April 15, 2017 2031
on January 20, 2020. © 2017 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 15, 2017; DOI: 10.1158/0008-5472.CAN-16-1121
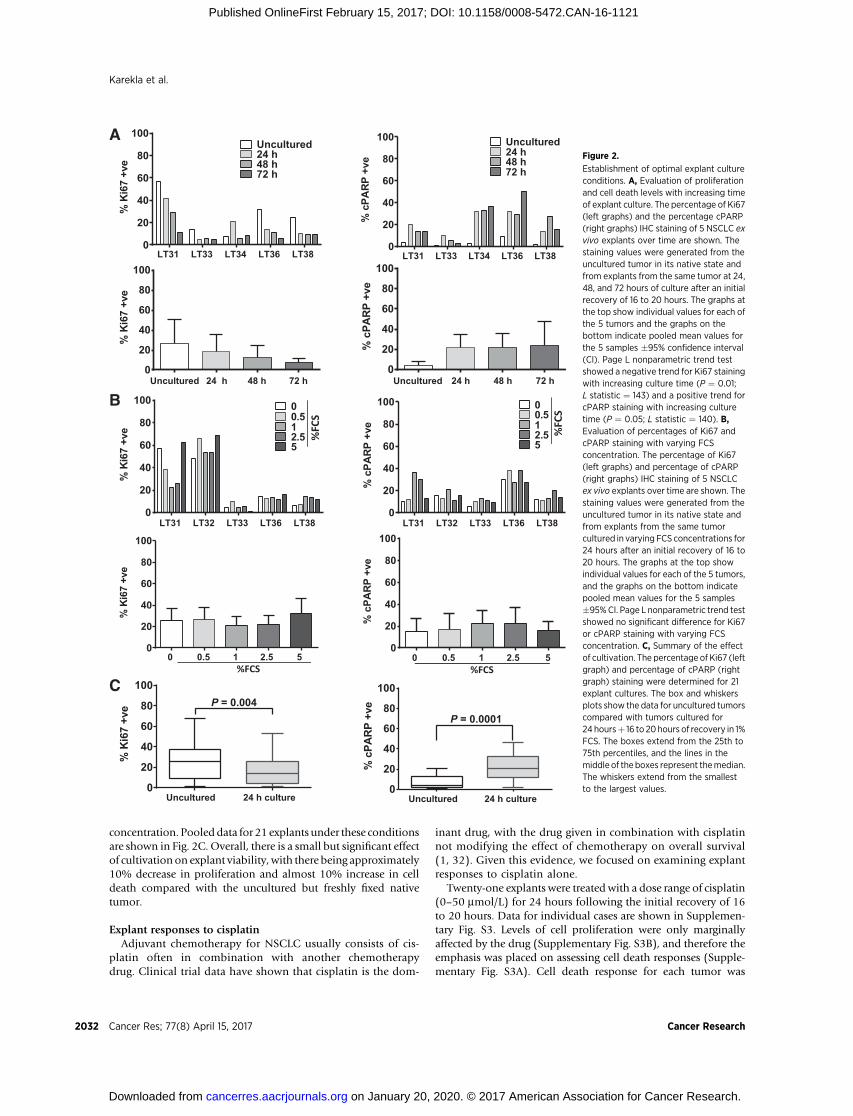
concentration. Pooled data for 21 explants under these conditionsare shown in Fig. 2C. Overall, there is a small but significant effectof cultivation on explant viability, with there being approximately10% decrease in proliferation and almost 10% increase in celldeath compared with the uncultured but freshly fixed nativetumor.
Explant responses to cisplatinAdjuvant chemotherapy for NSCLC usually consists of cis-
platin often in combination with another chemotherapydrug. Clinical trial data have shown that cisplatin is the dom-
inant drug, with the drug given in combination with cisplatinnot modifying the effect of chemotherapy on overall survival(1, 32). Given this evidence, we focused on examining explantresponses to cisplatin alone.
Twenty-one explants were treated with a dose range of cisplatin(0–50 mmol/L) for 24 hours following the initial recovery of 16to 20 hours. Data for individual cases are shown in Supplemen-tary Fig. S3. Levels of cell proliferation were only marginallyaffected by the drug (Supplementary Fig. S3B), and therefore theemphasis was placed on assessing cell death responses (Supple-mentary Fig. S3A). Cell death response for each tumor was
% K
i67
+ve
LT38LT36LT34LT33LT310
20
40
60
80
100Uncultured24 h48 h72 h
% K
i67
+ve
LT38LT36LT33LT32LT310
20
40
60
80
100 00.512.55
% K
i67
+ve
5 2.5 1 0.50 0
20
40
60
80
100
% K
i67
+ve
24 h cultureUncultured0
20
40
60
80
100P = 0.004
% c
PAR
P +v
e
24 h cultureUncultured0
20
40
60
80
100
P = 0.0001
% c
PAR
P +v
e
52.5 1 0.50 0
20
40
60
80
100
% c
PAR
P +v
e
LT38LT36LT33LT32LT310
20
40
60
80
100 00.512.55
A
B
C%FCS %FCS
%FCS
%FCS
% K
i67
+ve
72 h48 h24 hUncultured0
20
40
60
80
100
% c
PAR
P +v
e
LT38LT36LT34LT33LT310
20
40
60
80
100 Uncultured24 h48 h72 h
% c
PAR
P +v
e72 h48 h24 hUncultured
0
20
40
60
80
100
Figure 2.
Establishment of optimal explant cultureconditions. A, Evaluation of proliferationand cell death levels with increasing timeof explant culture. The percentage of Ki67(left graphs) and the percentage cPARP(right graphs) IHC staining of 5 NSCLC exvivo explants over time are shown. Thestaining values were generated from theuncultured tumor in its native state andfrom explants from the same tumor at 24,48, and 72 hours of culture after an initialrecovery of 16 to 20 hours. The graphs atthe top show individual values for each ofthe 5 tumors and the graphs on thebottom indicate pooled mean values forthe 5 samples �95% confidence interval(CI). Page L nonparametric trend testshowed a negative trend for Ki67 stainingwith increasing culture time (P ¼ 0.01;L statistic ¼ 143) and a positive trend forcPARP staining with increasing culturetime (P ¼ 0.05; L statistic ¼ 140). B,Evaluation of percentages of Ki67 andcPARP staining with varying FCSconcentration. The percentage of Ki67(left graphs) and percentage of cPARP(right graphs) IHC staining of 5 NSCLCex vivo explants over time are shown. Thestaining values were generated from theuncultured tumor in its native state andfrom explants from the same tumorcultured in varying FCS concentrations for24 hours after an initial recovery of 16 to20 hours. The graphs at the top showindividual values for each of the 5 tumors,and the graphs on the bottom indicatepooled mean values for the 5 samples�95%CI. Page L nonparametric trend testshowed no significant difference for Ki67or cPARP staining with varying FCSconcentration. C, Summary of the effectof cultivation. The percentage of Ki67 (leftgraph) and percentage of cPARP (rightgraph) staining were determined for 21explant cultures. The box and whiskersplots show the data for uncultured tumorscompared with tumors cultured for24 hoursþ 16 to 20hours of recovery in 1%FCS. The boxes extend from the 25th to75th percentiles, and the lines in themiddle of the boxes represent themedian.The whiskers extend from the smallestto the largest values.
Karekla et al.
Cancer Res; 77(8) April 15, 2017 Cancer Research2032
on January 20, 2020. © 2017 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 15, 2017; DOI: 10.1158/0008-5472.CAN-16-1121

calculated as fold induction relative to the control over the doserange (Fig. 3A). Of 21 tumors, 9 (43%) showed less than 2-foldinduction in cell death in response to the drug, whereas theremaining 12 of 21 (57%) showed cell death induction rangingfrom 2- to 25-fold. The majority of these tumors only showed aresponse at high levels of cisplatin (50 mmol/L), with only 2tumors responding at the lower dose of 10 mmol/L.
In addition to the 21 explants treated with a dose range ofcisplatin, a further 9 were treated with a single dose of 50 mmol/Lcisplatin.Weobtained clinical and histopathologic information onall 30 patients and their tumors (Supplementary Table S1). Celldeath difference compared with control in response to cisplatin isincluded alongside this information. One tumor was excludedfrom the analysis due to complex histopathology and 3 atypicalcarcinoids were excluded because of their different biologic behav-ior compared to adenocarcinomas and SCCs. For the remaining26,a ROC curve was used to determine the threshold for resistance/sensitivity to cisplatin and this analysis gave an area under the curveof 0.6485 � 0.1122 SE, a likelihood ratio of 3.30 and identified28.45% as the optimal cutoff (Supplementary Fig. S4A).
We then categorized each explant into being either sensitive orresistant to cisplatin (Supplementary Fig. S4B and SupplementaryTable S1). Using clinical information on corresponding patients(Supplementary Table S1), the relationship of cisplatin sensitiv-ity/resistance in explant culture to patient survival post-surgerywas determined (Fig. 3B). The data show a statistically significantrelationship (P ¼ 0.006) with sensitive cases demonstrating amean survival time (MST) of 28 months and resistant cases anMST of 14 months. To rule out an effect of tumor stage, weseparated stage I/IIA and IIB/III cases (Fig. 3C). There is a statis-tically significant relationship between cisplatin sensitivity andpatient survival for both stage I/IIA cases (P¼ 0.02) and for stageIIB/III cases (P ¼ 0.05), indicating the correlation is independentof stage; importantly, this relationship was also shown to beindependent of stage in a multivariate Cox survival analysis. Ofthe 26 patients, 12 received adjuvant therapy (SupplementaryTable S1), 8 received platinum-based chemotherapy, 3 receivedradiotherapy, and 1 received taxane-based chemotherapy. Inthose cases receiving any form of adjuvant therapy, there is asignificant correlation with survival of patients and response tocisplatin in explants (P ¼ 0.01; Fig. 3D, left). However, there wasno relationship between cisplatin sensitivity in explants andsurvival for patients reported to have lymph node involvement(P ¼ 0.13; Fig. 3D, right). Overall, the data show a strongrelationship between patient survival and explant sensitivity tocisplatin, indicating that the explant platform is predictive ofdisease recurrence and response to adjuvant therapy.
Cisplatin sensitivity in explants was also correlated with tumorstage andhistologic type (Fig. 3E). Therewas a significant negativetrend between difference in percentage of cPARP staining com-pared with control in response to cisplatin and increasing tumorstage (P¼0.007), suggesting thatmore advanced tumors aremoreresistant to the drug. There was also a significant correlationbetween cisplatin sensitivity and tumor type (P ¼ 0.0004), withSCC cases demonstrating greater cisplatin sensitivity than adeno-carcinoma subtypes (Fig. 3E).
Cisplatin sensitivity is linked to drug accumulation intumor areas
A number of mechanisms have been reported to render cellsresistant to cisplatin including reduced drug uptake, enhanced
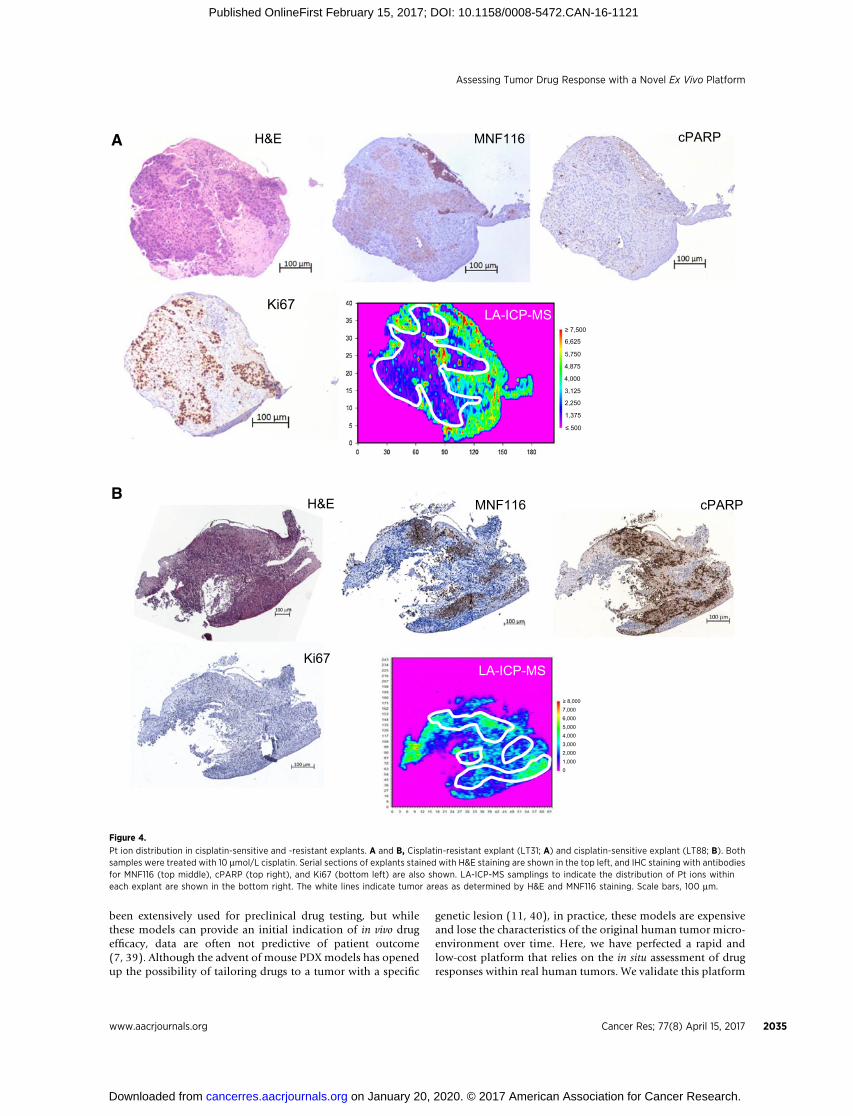
export, drug deactivation, increased repair of DNA damage, oralterations in apoptosis (33, 34). To examine drug uptake/export,we investigated Pt ion distribution across explant tissue using LA-ICP-MS (see Supplementary Fig. S1) imaging (Fig. 4 and Supple-mentary Fig. S5). For resistant cases, Pt ions were depleted fromareas corresponding to tumor cells but were present in the stroma(Fig. 4A and Supplementary Fig. S5). In contrast, for sensitivecases, Pt ions were present throughout the tumor and stromalareas of the explant, indicatingwidespread cisplatin uptake (Fig. 4Band Supplementary Fig. S5). Thus, while cisplatin is available tothe resistant explants, there is decreased intracellular drug concen-tration in tumor cells.
TP53 expression in the explantsThe TP53 gene is frequently mutated in NSCLC (35). Wild-
type TP53 protein is induced by DNA-damaging agents such ascisplatin, whereas mutated TP53 is either not expressed or isconstitutively expressed. We utilized IHC to gain an indicationof TP53 function in the 30 tumors, identifying 3 categories:(i) WTTP53 tumors (12 tumors), (ii) MUTTP53 tumors withconstitutively high TP53 levels (16 tumors), and (iii) MUTTP53tumors expressing undetectable TP53 (2 tumors). IHC TP53staining of positive and negative tumors is shown in Fig. 5A,whereas Fig. 5B indicates induction of TP53 following treat-ment of a WTTP53 tumor with a dose range of cisplatin andquantitation of the staining. Overall, 40% of tumors wereWTTP53 and 60% MUTTP53 based on IHC criteria (Supplemen-tary Table S1). This is approximately consistent with the knownmutation rate of TP53 in human NSCLC (34).
As expected, TP53MUT tumors had significantly higher intrin-sic levels of proliferation compared with TP53WT tumors(Fig. 5C), and the majority of TP53MUT cancers were of the SCCsubtype (Fig. 5D). In terms of response to cisplatin, TP53MUT
samples had significantly higher levels of cell death inductioncompared with TP53WT samples (Fig. 5D, left) and significantlyhigher levels of suppression of cell proliferation (Fig. 5D, right).These data counteract the view that TP53MUT tumors are defec-tive in their apoptotic response to DNA damage induced bycisplatin.
Explant responses to TRAILTRAIL is a death receptor ligand that has been developed for
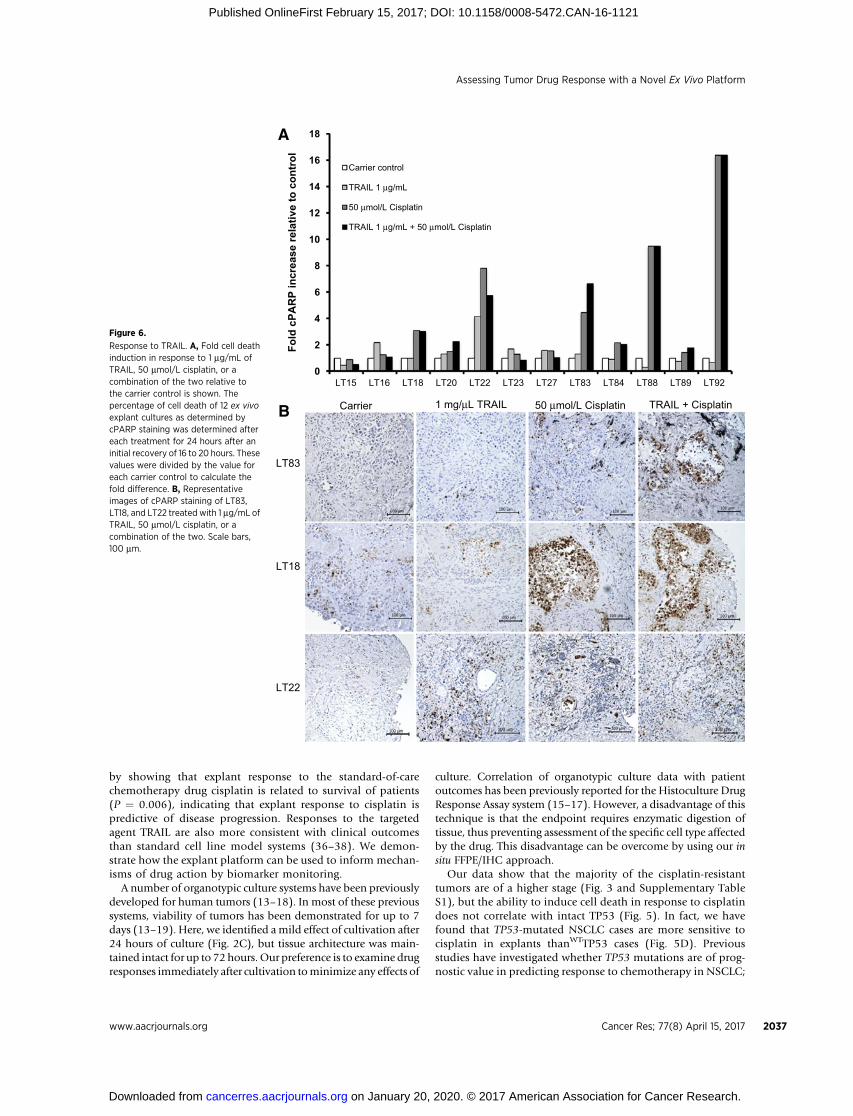
therapy, although clinical trials have been disappointing (36).It is thought that preclinical in vitro studies using cell lines havenot faithfully represented the clinical situation. This is sup-ported by data demonstrating that the majority of primaryhuman tumor cells are resistant to TRAIL receptor agonists(36–38). To investigate TRAIL sensitivity in NSCLC, 12 explantswere treated with TRAIL either as a single agent or in combi-nation with cisplatin (Fig. 6A). TRAIL alone did not elicit astrong response, except for one case (LT22) that demonstratedapproximately 4-fold induction of cell death. Similarly, TRAILdid not enhance the effects of cisplatin in the majority of cases,except for one tumor (LT83) for which slightly greater cell deathinduction (6-fold) than cisplatin alone (4-fold) was detected(Fig. 6A and B).
DiscussionPredicting drug response in patients with cancer is a major
challenge in the clinic. Cell line xenograft mouse models have
Assessing Tumor Drug Response with a Novel Ex Vivo Platform
www.aacrjournals.org Cancer Res; 77(8) April 15, 2017 2033
on January 20, 2020. © 2017 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 15, 2017; DOI: 10.1158/0008-5472.CAN-16-1121

Months elapsed806040200
0
50
100
P = 0.02
Cis SensCis Res
Months elapsed806040200
0
50
100
P = 0.05
Cis SensCis Res
Months elapsed403020100
0
50
100
P = 0.13
Cis SensCis Res
Months elapsed806040200
0
50
100 Cis SensCis Res
P = 0.01
0
5
10
15
20
25
30
501010
A B
Cisplatin dose (mmol/L)
E
Stage IIB+III
Lymph node involvement
All cases
Adjuvant therapy
Stage I+IIA
Fold
cPA
RP
incr
ease
rela
tive
to c
ontr
ol
C
D
Diff
eren
ce o
f % c
PAR
Pfr
om c
ontr
ol
Months elapsed
% S
urvi
val
% S
urvi
val
% S
urvi
val
% S
urvi
val
% S
urvi
val
8060402000
50
100
P = 0.006
Cis SensCis Res
SCCADC0
50
100
Tumor type
P = 0.0004
I II III0
50
100
Stage
Diff
eren
ce o
f % c
PAR
Pfr
om c
ontr
ol
Figure 3.
NSCLC explant response to cisplatin. A, Fold cell death relative to control of 21 NSCLC explant cultures treated with a dose range (0–50 mmol/L) of cisplatin. Thepercentage of cPARP staining of each sample was quantitated within explants from the same tumor cultured in carrier control (DMF) or increasing cisplatinconcentrations (1, 10, and 50 mmol/L) for 24 hours after an initial recovery of 16 to 20 hours. The value for each treatment was divided by the carrier control to obtain afold change.B,Kaplan–Meier patient survival for all cases correlatedwith sensitivity of explants to cisplatin at 50 mmol/L. Datawere evaluated for 26 patients/explants(Supplementary Table S1). The threshold of sensitivity/resistance to the drugwas determined using an ROC curve (Supplementary Fig. S4A). TheMantel–Cox log-ranktest identified a statistically significant relationship (P ¼ 0.006) between patient survival and cisplatin sensitivity. C, Kaplan–Meier patient survival according tostage correlated with sensitivity of explants to cisplatin at 50 mmol/L. Left graph, stage I/IIA samples (n ¼ 14, P ¼ 0.02). Right graph, stage IIB/III samples (n ¼ 12,P ¼ 0.05). D, Kaplan–Meier patient survival according to adjuvant chemotherapy or lymph node involvement correlated with sensitivity of explants to cisplatinat 50 mmol/L. Left graph, subgroup of patients receiving adjuvant therapy (n ¼ 12), including platinum-based chemotherapy (n ¼ 8), radiotherapy (n ¼ 3),and taxane-based chemotherapy (n ¼ 1). The Mantel–Cox log-rank test identified a statistically significant relationship between survival of patients andresponse to cisplatin in explants (P ¼ 0.01) Right graph, subgroup of patients with lymph node involvement (n ¼ 10) for which the Mantel–Cox log-rank test did notidentify a statistically significant relationship (P ¼ 0.13) between patient survival and cisplatin sensitivity. E, Correlation of response to cisplatin in explantculture with tumor stage (left) and histology (right). The box and whiskers plots show data for difference in percentage of cPARP staining in response to 50 mmol/Lcisplatin compared with control treatment for each explant relative to tumor stage/histology. The box extends from the 25th to 75th percentiles, and the lines inthe middle of the boxes represent the median. The whiskers extend from the smallest to the largest values. The Jonckheere–Terpstra test for orderedalternatives showed a significant negative trend (P ¼ 0.007) between increasing stage and cisplatin response. Correlation of tumor histology with cisplatin responsedemonstrated statistically significant differences between SCC samples and adenocarcinoma (ADC) types with a Mann–Whitney test of P ¼ 0.0004.
Karekla et al.
Cancer Res; 77(8) April 15, 2017 Cancer Research2034
on January 20, 2020. © 2017 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 15, 2017; DOI: 10.1158/0008-5472.CAN-16-1121
been extensively used for preclinical drug testing, but whilethese models can provide an initial indication of in vivo drugefficacy, data are often not predictive of patient outcome(7, 39). Although the advent of mouse PDX models has openedup the possibility of tailoring drugs to a tumor with a specific
genetic lesion (11, 40), in practice, these models are expensiveand lose the characteristics of the original human tumor micro-environment over time. Here, we have perfected a rapid andlow-cost platform that relies on the in situ assessment of drugresponses within real human tumors. We validate this platform
A MNF116H&E cPARP
Ki67LA-ICP-MS
BMNF116
Ki67
cPARPH&E
LA-ICP-MS
≥ 7,500
≥ 8,000
≤ 500
6,625
7,0006,0005,0004,0003,0002,0001,0000
5,750
4,875
4,000
3,125
2,250
1,375
Figure 4.
Pt ion distribution in cisplatin-sensitive and -resistant explants. A and B, Cisplatin-resistant explant (LT31; A) and cisplatin-sensitive explant (LT88; B). Bothsamples were treated with 10 mmol/L cisplatin. Serial sections of explants stained with H&E staining are shown in the top left, and IHC staining with antibodiesfor MNF116 (top middle), cPARP (top right), and Ki67 (bottom left) are also shown. LA-ICP-MS samplings to indicate the distribution of Pt ions withineach explant are shown in the bottom right. The white lines indicate tumor areas as determined by H&E and MNF116 staining. Scale bars, 100 mm.
Assessing Tumor Drug Response with a Novel Ex Vivo Platform
www.aacrjournals.org Cancer Res; 77(8) April 15, 2017 2035
on January 20, 2020. © 2017 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 15, 2017; DOI: 10.1158/0008-5472.CAN-16-1121

A
C
ADCACSCC
LT27LT18
LT23 LT116
Carrier control 1 µmol/L cisplatin
50 µmol/L cisplatin10 µmol/L cisplatin
B
D
Cisplatin dose (mmol/L)
ADCACSCC
%D
ecre
ase
of K
i67
com
pare
d w
ith c
ontr
ol
Noninducible p53Inducible p53–60
–40
–20
0
P = 0.00610
% In
crea
se o
f cPA
RP
com
pare
d w
ith c
ontr
ol
Noninducible p53Inducible p530
50
100 P = 0.003
% K
i67
+ve
TP53 +veTP53 -ve0
20
40
60
80
100
P = 0.002
100 µm 100 µm 100 µm100 µm
100 µm100 µm100 µm100 µm
100
80
60
40
20
00 1 10 50
% L
abel
ing
inde
x of
p53
Figure 5.
TP53 expression. A, IHC staining of explants treated with cisplatin demonstrating tumors with constitutively high levels of nuclear TP53 in tumor cells (LT18,LT27, and LT23) or low levels of TP53 (LT116). Scale bars, 100 mm. B, IHC staining and quantitation of nuclear p53 staining in a TP53WT explant sampledemonstrating dose-dependent TP53 expression following cisplatin treatment. The graph shows the percentage of mean labeling index of TP53 �SDfollowing treatment of the tumor sample with increasing doses of cisplatin (P ¼ 0.0001). Scale bars, 100 mm. C, Correlation of intrinsic proliferationindex with TP53 IHC staining. The graph shows the percentage of Ki67 staining of tumors classified according to TP53 IHC staining. Each circlerepresents one sample. D, Induction of cell death, as assessed by cPARP staining (left graph), and reduction of proliferation (right graph), as assessedby Ki67 staining, upon 50 mmol/L cisplatin treatment of 30 NSCLC ex vivo explants stratified according to their ability to induce TP53 expressionupon treatment with the drug. The data show that TP53-inducible tumors have a significantly reduced (P ¼ 0.003) ability to undergo cell death in responseto cisplatin compared with TP53-noninducible tumors. The majority of these tumors are of the SCC subtype.
Karekla et al.
Cancer Res; 77(8) April 15, 2017 Cancer Research2036
on January 20, 2020. © 2017 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 15, 2017; DOI: 10.1158/0008-5472.CAN-16-1121
by showing that explant response to the standard-of-carechemotherapy drug cisplatin is related to survival of patients(P ¼ 0.006), indicating that explant response to cisplatin ispredictive of disease progression. Responses to the targetedagent TRAIL are also more consistent with clinical outcomesthan standard cell line model systems (36–38). We demon-strate how the explant platform can be used to inform mechan-isms of drug action by biomarker monitoring.
A number of organotypic culture systems have been previouslydeveloped for human tumors (13–18). In most of these previoussystems, viability of tumors has been demonstrated for up to 7days (13–19). Here, we identified amild effect of cultivation after24 hours of culture (Fig. 2C), but tissue architecture was main-tained intact for up to 72 hours. Our preference is to examine drugresponses immediately after cultivation tominimize any effects of
culture. Correlation of organotypic culture data with patientoutcomes has been previously reported for the Histoculture DrugResponse Assay system (15–17). However, a disadvantage of thistechnique is that the endpoint requires enzymatic digestion oftissue, thus preventing assessment of the specific cell type affectedby the drug. This disadvantage can be overcome by using our insitu FFPE/IHC approach.
Our data show that the majority of the cisplatin-resistanttumors are of a higher stage (Fig. 3 and Supplementary TableS1), but the ability to induce cell death in response to cisplatindoes not correlate with intact TP53 (Fig. 5). In fact, we havefound that TP53-mutated NSCLC cases are more sensitive tocisplatin in explants thanWTTP53 cases (Fig. 5D). Previousstudies have investigated whether TP53 mutations are of prog-nostic value in predicting response to chemotherapy in NSCLC;
0
2
4
6
8
10
12
14
16
18
LT92LT89LT88LT84LT83LT27LT23LT22LT20LT18LT16LT15
Fold
cPA
RP
incr
ease
rela
tive
to c
ontr
ol
Carrier control
TRAIL 1 µg/mL
50 µmol/L Cisplatin
TRAIL 1 µg/mL + 50 µmol/L Cisplatin
A
Carrier 1 mg/µL TRAIL 50 µmol/L Cisplatin TRAIL + Cisplatin
LT83
LT18
LT22
B
Figure 6.
Response to TRAIL. A, Fold cell deathinduction in response to 1 mg/mL ofTRAIL, 50 mmol/L cisplatin, or acombination of the two relative tothe carrier control is shown. Thepercentage of cell death of 12 ex vivoexplant cultures as determined bycPARP staining was determined aftereach treatment for 24 hours after aninitial recovery of 16 to 20 hours. Thesevalues were divided by the value foreach carrier control to calculate thefold difference. B, Representativeimages of cPARP staining of LT83,LT18, and LT22 treated with 1 mg/mL ofTRAIL, 50 mmol/L cisplatin, or acombination of the two. Scale bars,100 mm.
Assessing Tumor Drug Response with a Novel Ex Vivo Platform
www.aacrjournals.org Cancer Res; 77(8) April 15, 2017 2037
on January 20, 2020. © 2017 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 15, 2017; DOI: 10.1158/0008-5472.CAN-16-1121

the results are controversial (41). In a 35-patient study, thepresence of mutant TP53 was highly indicative of resistance tocisplatin (P ¼ 0.002) (42), while in a study involving 253patients, TP53-positive patients had a significantly greater sur-vival benefit from adjuvant chemotherapy compared withTP53-negative patients (43). Another report in the Internation-al Adjuvant Lung Cancer Trial (IALT), a randomized trial ofadjuvant cisplatin-based chemotherapy, found no correlationbetween TP53 mutation and outcome in 524 patients (44).Overall, it will be important to extend analysis to a greaternumber of explants/patients to robustly determine the prog-nostic value of TP53 mutation. Lack of response to cisplatindoes, however, correlate with exclusion of the drug from tumorareas (Fig. 4). Cisplatin import is mediated by the coppertransporter CTR1, whereas the copper transporters ATP7A andATP7B regulate the efflux of cisplatin (45). Resistance to cis-platin has been associated with alterations in the expressionstatus of these transporters (46) and so it will also be importantto evaluate these transporters in the explant system used here.
In summary, the explant platform provides a patient-relevantmodel system for the preclinical evaluation of novel anticanceragents. When combined with tumor stratification approaches,the platform has the potential for personalizing drug treatment.The technology is low-cost, rapid, and achievable within anintegrated cancer translational research setting. An importantnext step will be to conduct a clinical study aimed at deter-mining which patients would best respond to chemotherapyprospectively; such a study is currently being developed withinour center.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
Authors' ContributionsConception and design: B. Sharp, C. Pritchard, M. MacFarlane, J.H. PringleDevelopment of methodology: E. Karekla, B. Sharp, J. Le Quesne, C. Pritchard,M. MacFarlane, J.H. PringleAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): E. Karekla, W.-J. Liao, J. Pugh, M. MacFarlaneAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): E. Karekla, B. Sharp, J. Pugh, H. Reid, J. Le Quesne,D. Moore, C. Pritchard, M. MacFarlane, J.H. PringleWriting, review, and/or revision of the manuscript: E. Karekla, B. Sharp,J. Pugh, H. Reid, C. Pritchard, M. MacFarlane, J.H. PringleAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): E. Karekla, H. Reid, J.H. PringleStudy supervision: C. Pritchard, M. MacFarlane, J.H. PringleOther (histopathologicinterpretation): J. Le Quesne
AcknowledgmentsWe thank Andrew Wardlaw for providing the ethical framework for this
project; Hilary Marshall and Will Monteiro for support in tissue collection;thoracic surgeons atGlenfieldHospital, Leicester, for providing clinical samples;and Chris Baines for providing clinical data. We also thank Angie Gillies forassistance with histology.
Grant SupportThis work was supported by a Medical Research Council (MRC) Doctoral
Training Grant to E. Karekla, the MRC Toxicology Unit (MC A/600), and theLeicester Experimental CancerMedicineCentre (C325/A15575Cancer ResearchUK/UK Department of Health). C. Pritchard was supported by a Royal Society-Wolfson merit award.
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received April 18, 2016; revised January 10, 2017; accepted January 30, 2017;published OnlineFirst February 15, 2017.
References1. Pignon JP, Tribodet H, Scagliotti GV, Douillard JY, Shepherd FA, Stephens
RJ, et al. Lung adjuvant cisplatin evaluation: a pooled analysis by theLACE Collaborative Group. J Clin Oncol 2008;26:3552–9.
2. Douillard JY, Tribodet H, Aubert D, Shepherd FA, Rosell R, Ding K, et al.Adjuvant cisplatin and vinorelbine for completely resected non-small celllung cancer: subgroup analysis of the Lung Adjuvant Cisplatin Evaluation.J Thorac Oncol 2010;5:220–8.
3. Mok TS, Wu YL, Thongprasert S, Yang CH, Chu DT, Saijo N, et al. Gefitinibor carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med2009;361:947–57.
4. Rosell R, Molina MA, Serrano MJ. EGFR mutations in circulating tumourDNA. Lancet Oncol 2012;13:971–3.
5. Solomon BJ, Mok T, Kim DW, Wu YL, Nakagawa K, Mekhail T, et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N Engl JMed 2014;371:2167–77.
6. Kola I, Landis J. Can the pharmaceutical industry reduce attrition rates?Nat Rev Drug Discov 2004;3:711–5.
7. Johnson JI, Decker S, Zaharevitz D, Rubinstein LV, Venditti JM, Sche-partz S, et al. Relationships between drug activity in NCI preclinicalin vitro and in vivo models and early clinical trials. Br J Cancer 2001;84:1424–31.
8. Fricker J.Time for reform in the drug-development process. Lancet Oncol2008;9:1125–6.
9. Tentler JJ, Tan AC, Weekes CD, Jimeno A, Leong S, Pitts TM, et al. Patient-derived tumour xenografts as models for oncology drug development. NatRev Clin Oncol 2012;9:338–50.
10. Siolas D, Hannon GJ. Patient-derived tumor xenografts: transformingclinical samples into mouse models. Cancer Res 2013;73:5315–9.
11. Hidalgo M, Bruckheimer E, Rajeshkumar NV, Garrido-Laguna I, De Oli-veira E, Rubio-Viqueira B, et al. A pilot clinical study of treatment guided by
personalized tumorgrafts in patients with advanced cancer. Mol CancerTher 2011;10:1311–6.
12. Bertotti A, Migliardi G, Galimi F, Sassi F, Torti D, Isella C, et al. Amolecularly annotated platform of patient-derived xenografts ("xenopa-tients") identifies HER2 as an effective therapeutic target in cetuximab-resistant colorectal cancer. Cancer Discov 2011;1:508–23.
13. Pampaloni F, ReynaudEG, Stelzer EH. The third dimensionbridges the gapbetween cell culture and live tissue. Nat Rev Mol Cell Biol 2007;8:839–45.
14. Freeman AE, Hoffman RM. In vivo-like growth of human tumors in vitro.Proc Natl Acad Sci U S A 1986;83:2694–8.
15. Yoshimasu T, Oura S, Hirai I, Tamaki T, Kokawa Y, Hata K, et al. Dataacquisition for the histoculture drug response assay in lung cancer. J ThoracCardiovasc Surg 2007;133:303–8.
16. Kubota T, SasanoN,AbeO,Nakao I, Kawamura E, Saito T, et al. Potential ofthe histoculture drug-response assay to contribute to cancer patient sur-vival. Clin Cancer Res 1995;1:1537–43.
17. Furukawa T, Kubota T, Hoffman RM. Clinical applications of the histo-culture drug response assay. Clin Cancer Res 1995;1:305–11.
18. Vaira V, FedeleG, Pyne S, Fasoli E, ZadraG, BaileyD, et al. Preclinicalmodelof organotypic culture for pharmacodynamic profiling of human tumors.Proc Natl Acad Sci U S A 2010;107:8352–6.
19. Majumder B, Baraneedharan U, Thiyagarajan S, Radhakrishnan P, Nara-simhan H, Dhandapani M, et al. Predicting clinical response to anti-cancer drugs using an ex vivo platform that captures tumour heterogeneity.Nat Commun 2015;6:6169.
20. Harper N,MacFarlaneM. Recombinant TRAIL and TRAIL receptor analysis.Methods Enzymol 2008;446:293–313.
21. MacFarlane M, Ahmad M, Srinivasula SM, Fernandes-Alnemri T, CohenGM, Alnemri ES. Identification and molecular cloning of two novelreceptors for the cytotoxic ligand TRAIL. J Biol Chem 1997;272:25417–20.
Karekla et al.
Cancer Res; 77(8) April 15, 2017 Cancer Research2038
on January 20, 2020. © 2017 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 15, 2017; DOI: 10.1158/0008-5472.CAN-16-1121
22. Caramel J, Papadogeorgakis E, Hill L, Browne GJ, Richard G, Wierinckx A,et al. A switch in the expression of embryonic EMT-inducers drives thedevelopment of malignant melanoma. Cancer Cell 2013;24:466–80.
23. Schneider CA, Rasband WS, Eliceiri KW. NIH Image to ImageJ: 25 years ofimage analysis. Nat Methods 2012;9:671–5.
24. Tuominen VJ, Ruotoistenmaki S, Viitanen A, Jumppanen M, Isola J.ImmunoRatio: a publicly available web application for quantitative imageanalysis of estrogen receptor (ER), progesterone receptor (PR), and Ki-67.Breast Cancer Res 2010;12:R56.
25. Koppen C, Reifschneider O, Castanheira I, Sperling M, Karst U, CiarimboliG. Quantitative imaging of platinum based on laser ablation-inductivelycoupled plasma-mass spectrometry to investigate toxic side effects ofcisplatin. Metallomics 2015;7:1595–603.
26. Baldwin DR, White B, Schmidt-Hansen M, Champion AR, Melder AM;Guideline Development Group. Diagnosis and treatment of lung cancer:summary of updated NICE guidance. BMJ 2011;342:d2110.
27. Swinson DE, Jones JL, Richardson D, Cox G, Edwards JG, O'Byrne KJ.Tumour necrosis is an independent prognostic marker in non-small celllung cancer: correlation with biological variables. Lung Cancer 2002;37:235–40.
28. Mehdi SA, Etzell JE, Newman NB, Weidner N, Kohman LJ, Graziano SL.Prognostic significance of Ki-67 immunostaining and symptoms inresected stage I and II non-small cell lung cancer. Lung Cancer 1998;20:99–108.
29. Nguyen VN,Mirejovsky P,Mirejovsky T,Melinova L,Mandys V. Expressionof cyclin D1, Ki-67 and PCNA in non-small cell lung cancer: prognosticsignificance and comparison with p53 and bcl-2. Acta Histochem 2000;102:323–38.
30. Warth A, Cortis J, Soltermann A, Meister M, Budczies J, Stenzinger A, et al.Tumour cell proliferation (Ki-67) in non-small cell lung cancer: a criticalreappraisal of its prognostic role. Br J Cancer 2014;111:1222–9.
31. Twiddy D, Edwards J, Walker RA, Cohen GM, MacFarlane M. A TRAIL-R1-specific ligand in combination with doxorubicin selectively targetsprimary breast tumour cells for apoptosis. Breast Cancer Res 2010;12Suppl 1:17–8.
32. Cortes J, Rodriguez J, Calvo E, Gurpide A, Garcia-Foncillas J, Salgado E,et al. Paclitaxel, cisplatin, and vinorelbine combination chemotherapy inmetastatic non-small-cell lung cancer. Am J Clin Oncol 2004;27:299–303.
33. Kelland LR.Preclinical perspectives on platinum resistance. Drugs 2000;59Suppl 4:1–8; discussion 37–8.
34. Cosaert J, Quoix E. Platinum drugs in the treatment of non-small-cell lungcancer. Br J Cancer 2002;87:825–33.
35. Le Calvez F, Mukeria A, Hunt JD, Kelm O, Hung RJ, Taniere P, et al. TP53and KRAS mutation load and types in lung cancers in relation to tobaccosmoke: distinct patterns in never, former, and current smokers. Cancer Res2005;65:5076–83.
36. Amarante-Mendes GP, Griffith TS. Therapeutic applications of TRAILreceptor agonists in cancer and beyond. Pharmacol Ther 2015;155:117–31.
37. Dyer MJ, MacFarlane M, Cohen GM. Barriers to effective TRAIL-targetedtherapy of malignancy. J Clin Oncol 2007;25:4505–6.
38. MacFarlane M, Kohlhaas SL, Sutcliffe MJ, Dyer MJ, Cohen GM. TRAILreceptor-selective mutants signal to apoptosis via TRAIL-R1 in primarylymphoid malignancies. Cancer Res 2005;65:11265–70.
39. Kung AL.Practices and pitfalls of mouse cancer models in drug discovery.Adv Cancer Res 2007;96:191–212.
40. Aparicio S, Hidalgo M, Kung AL. Examining the utility of patient-derivedxenograft mouse models. Nat Rev Cancer 2015;15:311–6.
41. Toyooka S, Tsuda T, Gazdar AF. The TP53 gene, tobacco exposure, and lungcancer. Hum Mutat 2003;21:229–39.
42. Kandioler D, Stamatis G, Eberhardt W, Kappel S, Zochbauer-Muller S,Kuhrer I, et al. Growing clinical evidence for the interaction of the p53genotype and response to induction chemotherapy in advanced non-smallcell lung cancer. J Thorac Cardiovasc Surg 2008;135:1036–41.
43. TsaoMS, Aviel-Ronen S, Ding K, LauD, Liu N, Sakurada A, et al. Prognosticand predictive importance of p53 and RAS for adjuvant chemotherapy innon small-cell lung cancer. J Clin Oncol 2007;25:5240–7.
44. Ma X, Rousseau V, Sun H, Lantuejoul S, Filipits M, Pirker R, et al.Significance of TP53 mutations as predictive markers of adjuvant cisplat-in-based chemotherapy in completely resected non-small-cell lung cancer.Mol Oncol 2014;8:555–64.
45. Safaei R, Howell SB. Copper transporters regulate the cellular phar-macology and sensitivity to Pt drugs. Crit Rev Oncol Hematol 2005;53:13–23.
46. Kuo MT, Chen HH, Song IS, Savaraj N, Ishikawa T. The roles of coppertransporters in cisplatin resistance. Cancer Metastasis Rev 2007;26:71–83.
www.aacrjournals.org Cancer Res; 77(8) April 15, 2017 2039
Assessing Tumor Drug Response with a Novel Ex Vivo Platform
on January 20, 2020. © 2017 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 15, 2017; DOI: 10.1158/0008-5472.CAN-16-1121

2017;77:2029-2039. Published OnlineFirst February 15, 2017.Cancer Res Ellie Karekla, Wen-Jing Liao, Barry Sharp, et al. TherapyEnable Evaluation of Primary Tumor Responses to Anticancer
Small Cell Lung Carcinoma− Explant Cultures of NonEx Vivo
Updated version
10.1158/0008-5472.CAN-16-1121doi:
Access the most recent version of this article at:
Material
Supplementary
http://cancerres.aacrjournals.org/content/suppl/2017/02/15/0008-5472.CAN-16-1121.DC1
Access the most recent supplemental material at:
Cited articles
http://cancerres.aacrjournals.org/content/77/8/2029.full#ref-list-1
This article cites 46 articles, 14 of which you can access for free at:
Citing articles
http://cancerres.aacrjournals.org/content/77/8/2029.full#related-urls
This article has been cited by 4 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/77/8/2029To request permission to re-use all or part of this article, use this link
on January 20, 2020. © 2017 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 15, 2017; DOI: 10.1158/0008-5472.CAN-16-1121










![Inflammation and cancer: How hot is the link? · carcinoma [30], colon carcinoma, lung carcinoma, squamous cell carcinoma, pancreatic cancer [31,32], ovarian carcinoma biochemical](https://img.pdfslide.net/doc/110x75/5fcdd6c81c76a34db570e7e6/iniammation-and-cancer-how-hot-is-the-link-carcinoma-30-colon-carcinoma.jpg)


















