Embed Size (px)
DESCRIPTION
exam
Citation preview

EXAM 4 PEDS STUDY GUIDE
CARDIAC Cardiac Assessment
o Normal pediatric vital signs HRo Newborn
100-180o 1 wk-3 mo
100-220o 2 mo- 2 yr
60-150o 2-10 yr
70-110o 10 yr-adult
55-90 Cardiovascular disease has 2 major groups
o Congenital heart disease (CHD) Primarily anatomic abnormalities present at birth that result in
abnormal cardiac function 2 types
Heart failure (HF) Hypoxemia
o Acquired cardiac disorders Disease processes or abnormalities that occur after birth and can be
seen in normal heart or the presence of genital heart defects Various factors:
Infection Autoimmune responses Environmental factors Familial tendencies
History & physical examo HISTORY HISTORY HISTORY!!!! o Inspection
Nutritional state- failure to thrive or poor weight gain is associated with heart disease
Color- cyanosis –common feature of CHD Pallor associated with poor perfusion
Chest deformities- enlarged hears distorts chest configuration Unusual pulsations- visible pulsations of the neck veins are seen
sometimes Respiratory excursion- refers to ease or difficulty of respiration Clubbing of fingers- associated with cyanosis
o Palpation and Percussion Chest- maneuvers help discern heart size and other characteristics Abdomen – hepatomegaly or spenomegaly
1

Peripheral pulses- rate, regularity, and amplitudeo Auscultation
Heart rate and rhythm- listen for fast heart rates, slow, and irregular rhythms
Character of heart sounds- listen for distinct or muffled sounds, murmurs, and additional heart sounds
o Diagnostic Electrocardiogram
Nurse should assess the patient, not the monitor Echocardiography
Most frequently used tests for detecting cardiac dysfunction Involves use of ultra-high-frequency sound waves to produce
an image of heart’s structure Transducer placed directly on chest wall delivers repetitive
pulses of ultrasound and processes the returned signals
Cardiac Catheterization Invasive diagnostic procedure in which a radiopaque catheter is inserted thru a
peripheral blood vessel into the heart Catheter is guided thru the heart with aid of fluoroscopy After tip of catheter is within a heart chamber, contrast material is injected, and
films are taken of the dilution and circulation of the material (angiography) Types:
o Diagnostic catheterizations: Used to diagnose congenital cardiac defects- particularly in
symptomatic infants & before surgical repair Divided into right-sided catheterizations, in which cateheter is
introduced through a vein & threaded into right atrium Left-sided catheterization- catheter is threaded thru an artery into
aorta and into the hearto Interventional catheterizations:
Therapeutic catheterization A balloon catheter or other device is used to alter the cardiac anatomy Interventions:
Balloon atrioseptostomyo Transposition of great arterieso Some complex single-ventricle defects
Balloon dilationo Valvular pulmonic stenosiso Branch pulmonary artery stenosiso Congenital valvular aoritic stenosiso Rheumatic mitral stenosiso Recurrent coarctations of aortao Congential mitral stenosis
Coil occlusion
2
o PDA (<4mm( Transcatheter device closure
o ASD Amplatzer septal occluder
o ASD VSD devices
o VSDs Stent placement
o Pulmonary artery stenosiso Coarctation of the aorta in adolescentso Use to treat other lesions
RF ablationo Some tachydysrthymias
o Electrophysiology studies Catheters with tiny electrode that record the impulses of the heart
directly from conduction system are used to evaluate dysrthymias & sometimes destroy accessory pathways that cause some tachydsrthmias
Possible side effects:o Acute hemorrhage from entry siteo Low-grade fevero Nauseao Vomitingo Loss of pulse in catheterized extremeo Transient dysrhythmias
Rare risks:o Strokeo Seiureo Tamponadeo Death
Preprocedural care:o Prepare child & fam for procedureo Use developmentally appropriate materials o Assess & mark pulseso Basline O2 satso NPO for 4-6 hours before procedure
Postprocedural:o Observe of the following for signs of complications:
Pulses Temp & color of affected extremity Vital signs- q 15 minutes Blood pressure Dressing Fluid intake
3

Bloog glucose levels- for hypoglycemia Postpericardiotomy syndrome
o Symptoms: Fever Pericardial friction rub Pericardial & pleural effusion
o Occurs immediate post opo Also can occur later (day 7-21)o Cause=unknown
CONGENTIAL HEART DISEASE (CHD) Incidence:
o 5-8 per 1000 live birthso 2-3 are symptomatic in 1st year of lifeo CHD=major cause of death in first year of life (after prematurity)o Most common anomaly= ventricular septal defect
Causes:o Chromosomal/genetic 10-12%o Maternal/environmental 1-2%
Maternal drug use Infants that have FAS- 5-% have CHD
Maternal illness Rubella infection PDA & pulmonary branch stenosis Cytomegalovirus, toxoplasmosis, other viral illness Infants of diabetic mothers (IDMs)
o Multifactorial 8%% Normal fetal circulation changes
o When newborn takes 1st breath, the fetal vascular system undergoes abrupt changes
Umbilical vein & umbilical arteries Before birth, umbilical vein delivers O2 and nutrients to a fetus
Foramen ovale Closes as pressure in left atrium exceed pressure in right
atrium Ductus arteriosus
Starts to close in presence of increased O2o The following are NO LONGER NEEDED:
Foramen ovale Shunts highly oxygenated blood from RA to LA & supplies
upper extremities and head Ductus venosus
Fetal blood vessel connecting UV to IVC Umbilical vessels
o WITH THE FIRST BREATH… Lungs expand causing dramatic fall in pulmonary vascular resistance
4

Market increase in pulmonary blood flow (raising LA pressure above that of IVC)
A progressive thinning of the walls of pulmonary arteries occurs Blood pressure is now high in the aorta & the baby’s systemic
circulation is well established The ductus arteriosus contstricts at birth, but there is often a small
shunt of blood from the aorta to the Left Pulmonary Artery for a few days
This decreases with increases PO2 which stimulates bradykinin release
Umbilical arteries constrict functionally, later become fibrous o
o History indicators of cardiac dysfunction Symptoms may appear 4-12 weeks after birth Failure to thrive, poor weight gain, activity intolerance Developmental delays Positive prenatal history Positive family history of cardiac disease
o Physical indicators of cardiac dysfunction: Poor feeding Tachypnea, tachydardia Diaphoresis Crackles
5

Hepatomegaly Cyanosis Murmur Sternal lift Impaired myocardial function
Tachycardia Fatigue Weakness Restlessness Pale Cool extremities Decreased BP Decreased output
Pulmonary congestion Tachypnea Dyspnea Respiratory distress Exercise intolerance Cyanosis
Systemic venous congestion Peripheral & periorbital edema Weight gain Hepatomegaly Neck vein distention
Goals of management o Support maximal growth & nutritiono Reduce cardiac workloado Prevent & treat congestive heart failureo Maintain optimal cardiac outputo Provide palliative procedures to protect lungs from too much bloow flow, or
too little blood flowo Correct the underlying defecto Maintain fluid & electrolyte balanceo Prevent secondary complications (failure to thrive, cardiogenic shock,
infection, respiratory compromise, cardiac dysrthythmia, thromboembolism) Diagnostic tests:
o H&Po Chest x-rayo Echocardiogram, EKGo Labs:
ABG’s CNC Electrolyte panel Therapeutic & diagnostic cardiac catheterization
Therapeutic nursing managemento Avoid situations that increase cardiac demands (fever, pain, agitation)
6

o Avoid unnecessarily disturbing the infanto Monitor weightso Small frequent feedings (increased calorie formula as needed)o O2 as neededo Administer pharmacologic agents as ordered; evaluate patient response to
treatmento Portect from infectiono Accurate I&O
Pharmacology:o Depends on defect & MOST IMPORTANTLY patient’s clinical condition
Digoxin Diuretics Prostaglandin
Keep PDA open Indomethacin
Close PDA Vasopressors Vasodilators Vaccinations as indicated
Complications:o Heart failureo Postpericardiotomy syndrome
Post-op period: fever, pericardial friction rub, pleural effusiono Cerebral thrombosiso Failure to thriveo Death
Older Classifications of CHDo Acyanotic
May become cyanotico Cyanotic
May be pink May develop congestive heart failure
Newer classification of CHDo Hemodynamic characteristics (blood flow patterns within the heart):
1. Increased pulmonary blood flow2. Decreased pulmonary blood flow3. Obstruction of blood flow out of the heart4. Mixed blood flow
Increased Pulmonary Blood Flow Defects Abnormal connection between the 2 side of the heart
o Either the septum or great vessels Increase blood volume on RIGHT side of heart Increased pulmonary blood flow
7

Decreased systemic blood flow Defects:
o Atrial Septal Defect (ASD) Acyanotic Hole between two atria
Allowing blood from higher pressure left atrium to follow into the lower pressure right atrium
Closes naturally, with therapeutic catheterization of surgery
Loud, harsh murmur With fixed split second heart sound
Enlarged right side of heart Increased oxygen saturiation in right atrium Mild congestive heart failure May be asymptomatc Surgical patch closure
o Ventricular Septal Defect (VSD) Acyanotic Hole between right & left ventricles Most common cardiac defect Closes naturally or with surgical
correction Loud, harsh murmur that begins at
about 4-8 weeks of age O2 saturation is higher that normal in
right ventricle Congestive heart failure Failure to thrive Dysrthymias Small defects may be asymptomatic
o Atrioventricular canal defect Combo of ASD & VSD Acyanotic Incomplete fusion of endocardium creating
a large central AV valve that allows blood to flow between all four chambers of the heart
Most common cardiac defect in children with Down syndrome
Flow is determined by pulmonary and systemic resistance
8

Surgical repair required CHF Loud systolic murmur Cyanosis increases with crying Pulmonary vascular obstructive disease Increased blood volume is pumped into the lungs, which may
eventually result in increased pulmonary vascular resistance o Patent Ductus Arteriosus (PDA)
Acyanotic Fetal vessel between the pulmonary
artery and the aorta that fails to close
PDA is common in premature infants
Closure occurs naturally, with Indomethacin, therapeutic catherization, or surgery
Machinery-like murmur Patients at risk for BE and
pulmonary vascular obstructive disease later in life from chronic excessive pulmonary blood flow
Tachycardia Enlargement of left ventricle Wide pulse pressure Bounding pulses Tachypnea
OBSTRUCTIVE DEFECTS Blood exiting the heart meats an area of anatomic narrowing (stenosis) causing
obstruction to blood flow The pressure in ventricle and in great artery before obstruction is increased, and the
pressure in the area beyond the obstruction is decreased Location of narrowing is usually near the valve:
o Vavlular- at site of valveo Subvalvular- narrowing in the ventricle below the valve (ventricular outflow
tract)o Suprvalvular- narrowing in great artery above valve
There is a pressure load on the ventricle and decreased cardiac output Clinically exhibit signs of HF Defects:
o Coarctation of the Aorta Acyanotic Narrowing of the aorta due to a
constricting band
9

Increased blood pressure and oxygen saturation in the upper extremities as compared with the lower extremities
Headaches Vertigo Nosebleeds Absence of femoral pulses High blood pressure Leg pain Decreased cardiac output CHF Surgical repair & reconstruction
is usually needed Cool lower extremities
o Aortic Stenosis Acyanotic Narrowing of aortic valve
Causing resistance to blood flow in left ventricle, decreased cardiac output, left ventricular hypertrophy, & pulmonary vascular congestion
Left ventricular enlargement Systolic ejection murmur Faint pulses, hypotension, tachycardia, poor feeding Exercise intolerance, chest pain, and dizziness Decreased cardiac output Opened with balloon procedure or surgery Risk for:
o BE, coronary insufficiency, & ventricular dysfunction o Pulmonic Stenosis
Acyanotic Narrowing of the pulmonary valve or pulmonary artery Resistance to blood flow causes right ventricular hypertrophy &
decreased pulmonary blood flow Right ventricular enlargement Systolic ejection murmur Exercise intolerance CHF, cyanosis Opened with balloon procedure or surgery
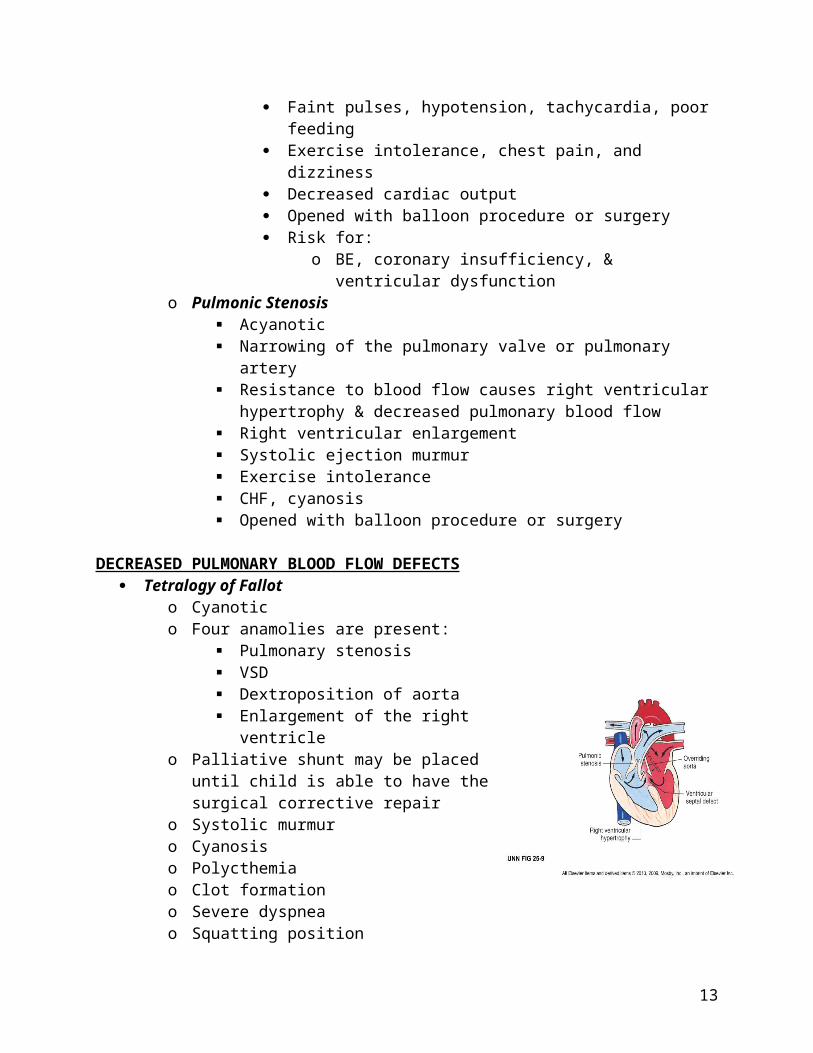
DECREASED PULMONARY BLOOD FLOW DEFECTS Tetralogy of Fallot
o Cyanotico Four anamolies are present:
10

Pulmonary stenosis VSD Dextroposition of aorta Enlargement of the right ventricle
o Palliative shunt may be placed until child is able to have the surgical corrective repair
o Systolic murmuro Cyanosiso Polycthemiao Clot formationo Severe dyspneao Squatting positiono Hypercyanotic spells (“Tet Spells”)o Acidosiso Clubbing of the fingerso Growth retardationo Failure to thrive
Tricuspid Atresiao Cyanotico Tricuspid valve is completely closedo Generally requires several complex
surgerieso Incompatible with life if there is
inadequate pulmonary blood flowo PGE infusion is used until an emergency
shunt procedure can be performedo The Fontan procedure is the surgical
repairo No blood flow from right atrium to right
ventricleo Severe cyanosis within hours after birth (Increased as the PDA closes)o CHFo Failure to thrive
MIXED DEFECTS Transposition of the great arteries or transposition of the great vessels
o Cyanotico Aorta arises from the right ventricle instead of the left, and the pulmonary
artery arises from the left instead of the righto Incompatible with life if there is no
connection between right and left sideso Emergency septostomy is performed to
create a connection between the right and left sides
11

o The surgical repair is the atrial switch procedureo Severe cyanosis hours to days after birth (as PDA closes)o Various murmurso Presence of ASD and VSDo CHF
Total anomalous pulmonary venous connectiono Cyanotico Total anomalous pulmonary venous
returno Rare defect characterized by failure
of pulmonary veins to join the left atrium; instead are connected with the venous system
o Repaired surgically o Cyanosis (inversely related to
amount to pulmonary blood flow)o May initially be asymptomatico CHF, cardiac failure, death
Truncus Arterioususo Cyanotico Failure of normal separation in development of the pulmonary artery and
aorta, resulting in a single vessel that overrides both ventricles; mixing pulmonary & systemic circulations
o Repaired in first few months of life (closing VSD and hemographs- modified Rastelli procedure)
o CHFo Cyanosiso Poor growtho Activity intoleranceo Murmuro Brain abscesso Bacterial endocarditis
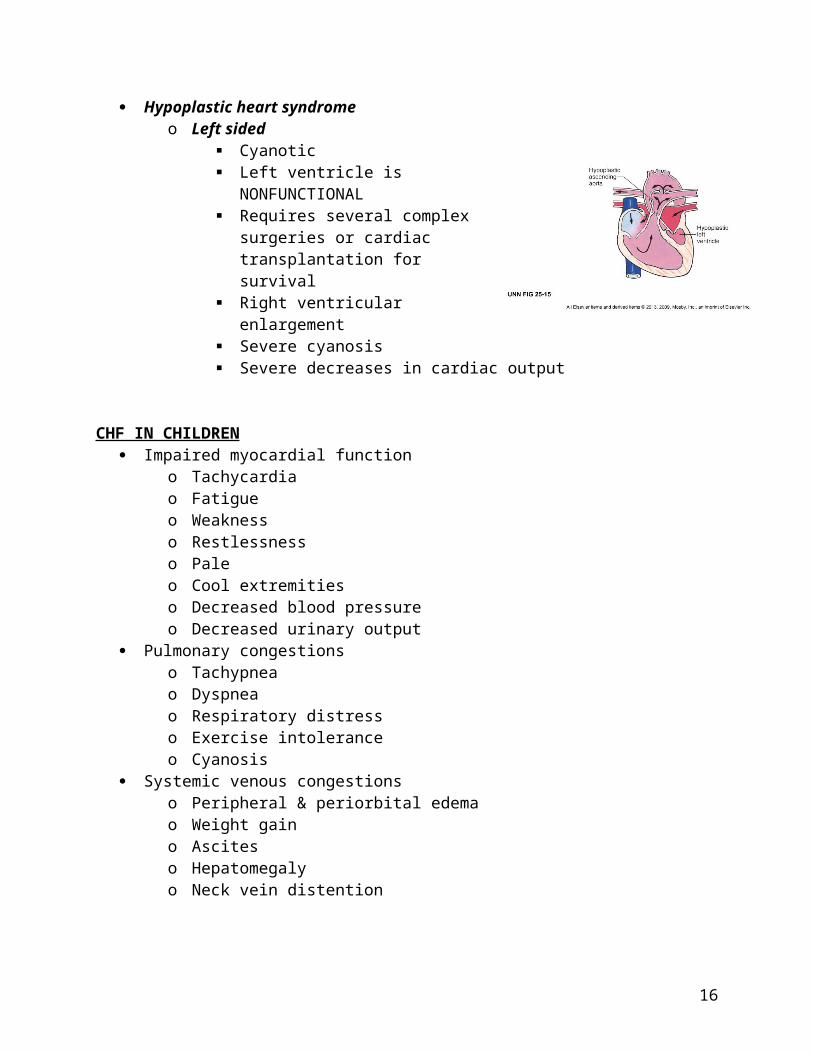
Hypoplastic heart syndromeo Left sided
Cyanotic Left ventricle is NONFUNCTIONAL Requires several complex surgeries
or cardiac transplantation for survival
Right ventricular enlargement Severe cyanosis Severe decreases in cardiac output
12
CHF IN CHILDREN Impaired myocardial function
o Tachycardiao Fatigue o Weaknesso Restlessnesso Paleo Cool extremitieso Decreased blood pressureo Decreased urinary output
Pulmonary congestionso Tachypneao Dyspneao Respiratory distresso Exercise intoleranceo Cyanosis
Systemic venous congestionso Peripheral & periorbital edemao Weight gaino Asciteso Hepatomegalyo Neck vein distention
ENDOCARDITIS Bacterial endocarditis (BE) and subacute endocarditis (SBE) are now referred to as
infective endocarditis (IE) Often a sequela of bacteremia in children with CHD or AHD Most common causative agents:
o Streptococcus viridans or Staphylococcus aureuso Fungal agents such as Candida albicans
Prophylaxis for 1 hour before procedures (IV) or may use PO in some caseso Antibiotics
Clinical manifestations:o Onset usually insidiouso Unexplained fevero Anorexiao Malaiseo Weight losso Characteristic findings caused by extracardiac emboli formation
Splinter hemorrhage (think black lines) under the nails Osler nodes
13

Janeway lesions Petechiae on oral mucous membranes
o May be present: Heart failure Cardiac dysrthmias New murmur
RHEMATIC FEVER (RF) & RHEMATIC HEART DISEASE (RHD) Rheumatic Fever
o Inflammatory disease occurring after group A B-hemolytic stremptococcal pharyngitis (GABHS)
o Infrequently seen in USo Self-limiting
Affects joints, skin, brain, serous surfaces, & heart Rheumatic heart disease
o Most common complication of RFo Damage to valves as a result of RF
Clinical manifestations:o Jones criteria (Presence of 2 major manifestations or one major
manifestation & two minor manifestations) Carditis Polyarthritis Erythema Marginatum Subcutaneous Nodes Chorea (St. Vitus Dance, Sydenham Chorea)
Treatmento Prevention of GABHSo Tx of streptococcal tonsillitis and pharyngitis
Penicillin G IM once Penicillin V by mouth for 10 days Sulfa by mouth for 10 days Erythromycin (if patient is allergic to the above agent) by mouth for
10 dayso Tx of recurrent RF
Same as above
KAWASAKI DISEASE (KD); Mucocutaneous lymph node syndrome An acute systemic vasculitis of unkown cause 75% of cases, the child is younger than 5 years of age 3 phases:
o Acute phase Sudden high fever, unresponsive to antipyretics & antibiotics
o Subacute phase Lasts from end of fever thru end of all KD clinical signs
14

o Convalescent phase: Clinical signs have resolved, but laboratory values have not returned
to normal Ends when normal values have returned (6-8 weeks)
Diagnostic criteria for Kawasaki diseaseo Changes in extremities
In acute phase: edema, erythema of palms and soles Subacute: periungual desquamation (peeling) of hands & fet
o Bilateral conjuctival injection (inflammation) without exudationo Changes in the oral mucous membraneso Polymorphous rasho Cervical lymphadenopathy
Treatment of KDo Acetylsalicyclic acid (ASA) 80-11 mg/kg/day for fevero IV immunoglobulin (IVIG)o Then 3-5 mg/kg/day antiplatelet
Hyperlipidemia Identify kids at risk & treat early Tx is lifestyle modifcation
o Restrict intake of cholesterol & fatso Increase intake of whole grains, fruits, & veggieso Exercies for 60 min a day 5 days a weeko Stop smoking and avoid second-hand smoke
If there is no response to diet changes & meds:o Colestipol (Colestid)o Cholestyramine (Questran)
Systemic Hypertension Essential hypertension has no known cause Secondary has an identifiable cause Pediatric hypertension is generally secondary to structural abnormality or an
underlying pathologic conditiono Renal diseaseo Cardiovascular diseaseo Endocrine or neurologic disorders
Pharmacologic treatment:o B-blockerso Calcium channel blockerso Angiotensin-converting enzyme (ACE) inhibitorso Angiotensin receptor blockerso Diuretics
15
MS
Immobilized patient Atrophy Joint contracture Major musculoskeletal consequences of immobilization are:
o Significant decrease in muscle size, strength, and enduranceo Bone demineralization leading to osteoporosiso Contractures and decreased joint mobility
DVT
Developmental Dysplasia of the Hip (DDH)x Wide range of abnormal development of the hip leading to hip instability 1 per 100 live births 80% are female Lift hip affected most commonly Caucasion children most often affected Degrees of DDH
o Acetabular dysplasia Acetabular rool shallow; mildest form
o Subluxation Head of femur is partially displaced Flattened socket; most common form
o Dislocation Femoral head not in contact with acetabulum
Clinical manifestations of DDHo Infant:
Shortened limb on affected side Restricted abduction of hip on affected side Unequal gluteal folds when infant prone Positive Ortolani test Positive Barlow test
o In older infant & child Affected leg shorter than other Telescoping or piston mobility of joint Trandelenburg sign Trandelenburg gait Greater tochanter is prominent and appears above line from
anterosuperior iliac spine to tuberosity of ischium Marked lordosis if bilateral dislocations Waddling gait if bilateral disclocations Sign of gluteus medius weakness or relative inhibition
Sign is elicited by asking patient to stand on involved leg
16

If sign is positive, the pelvis will drop on uninvolved side Ortolani & Barlow tests
o Barlow test shows that hip has potential to dislocateo Ortolani test confirms its dislocation
oo Never do at the same time; do one knee then the other
Diagnosiso Newborn assessment tools most reliable in early infancyo X-ray not reliable in infancy due to incomplete ossification of femoral heado Ultrasound as adjunct to abnormal physical findings
Therapeutic management of DDHo Importance of early interventiono Newborn to age 6 months:
Palvik harness for abduction of hipo Age 6-18 months:
Dislocation unrecognized until child begins to stand and walk; use traction and cast immobilization (spica)
o Older child: Operative reduction Tenotomy (muscle contracture) Osteotomy (rebuild acetabular roof) Difficult after 4 years
Management: 0-6 monthso Splinting: Palvik harness
Worn continuously x 3-5 months until hip stable Straps checked q 1-2 weeks for adjustment
o 95% effective if hips reducible at birtho prevent adductiono Nursing care of child in palvik harness
Newborn hip assessment
17

Management of reduction device Teaching application/use of harness
o Removal, adjustment discouraged Prevent skin breakdown
o Clothing, diaper under strapso Check for reddening under straps often
Management: 6-18 monthso Gradual reduction by traction x 3 weekso Closed/open reduction under anesthesiao Hip spica cast x 3 months
Management: Older childo Operative reductiono Construction of acetabular roofo Post-operative castingo Successful reduction difficult after 4 years
TALIPES: Congenital Clubfoot Includes multiple foot, ankle deformity and malposition, and soft tissue
contractures Incidence: 1-2: 1000 live births Male: female= 2:1 50% are bilateral increase risk of hip dysplasia Etiology
o Not well identified o Strong family disposition
Q:10 if parent affectedo Possible arrested fetal development of skeletal & soft tissue (9-10 weeks
gestation)o Associated with other syndrome (myelomeningocele)o Idiopathic clubfoot most common form
18

oo Talipes varus: inversion, or bending inwardo Talipes valgus: eversion, or bending outo Talipes equinus: plantar flexion with toes lower than the heelo Talipes calcaneus: dorsiflexion with toes higher than the heelo Talipes equinovarus: when the foot turns inward and downward; most
common form Classification of clubfoot
o Mild or postural May correct spontaneously or require passive exercise or serial
castingo Tetralogic
Associated with other congenital anomalies Usually requires surgical correction with high incidence or
recurrence o Idiopathic
Bony abnormality almost always requiring surgical intervention Treatment
o Started as a neonate
19

o Serial casting of affected leg(s)o Recasting frequent until maximum correction achieved (~8-12 weeks) o X-Ray to evaluate efficacy of castingo If casting unsuccessful, surgery @6-12 months & casting/brace after surgery
Metatasus Adductus Most common Treatment usually not needed Due to abnormal intrauterine positioning Associated with pigeon toed gait Different from Talipes deformities because foot has full ROM
20

Kyphosiso Abnormally increased convex angulation of the curvature of the thoracic
spineo Most common form is posturalo Can result from tuberculosis, arthritis, osteodystrophy, or compression
fracture o PT w/ strengthening excerciseso Not associated with pain
Lordosiso Accentuation of the cervical or lumbar curvature beyond physiologic limitso May be idiopathic or secondary complication or traumao May occur with flexion contractures of hip, congenital dislocated hipo In obese children, abdominal fat alters center of gravity, causing lordosiso Treat cause ie excess weight and manage pain; associated with pain
Scoliosiso Most common spinal deformityo Complex spinal deformity in 3 planes:
Lateral curvature Spinal rotation causing rib asymmetry Thoracic kyphosis
o Congenital or develop during childhood
21

Congenital associated w/ myelomeingoceleo Idiopathic scoliosis during growth spurt of early adolescence most common
form o Early manifestations of Idiopathic scoliosis
Seldom apparent before preadolescent growth spurt May be picked up in school screening Uneven pants length Rarely painful Right curvature is usually scoliosis Left curvature often associated with disorders and have a neurologic
componento Diagnosis
Physical exam Asymmetry of shoulder, hip height; flank, scapular shape when
standing Asymmetry of ribs & flanks with bend at waist Stand & twist to evaluate flexibility of curve
X-Ray of spine to measure curve magnitude MRI if indications of other spinal abnormalities
Spinal curvature and treatmento 10 degree normal postural variationo 10-20 – mild, no treatment if no progressiono 20-40- bracingo >40 surgery
Bracing/exerciseo Bracing can slow or stop progression of curvatureo TLSO (thoracolumbarsacral orthosis)
Wear 16-23 hours per day; adjusted periodically Milwaukee brace; Boston brace (less visible)
o Daily exercises to prevent atrophy of spinal and abdominal muscle Operative management
o Curves >40, difficult sitting, breathing, pain require surgeryo Realignment and internal fixation with bony fusion or realigned spineo Harrington rod system
Immobilized postoperatively Post-Op Nursing care
o Pain management Considerable pain 2-3 days post-op
o Neurologic dysfunction Post-op paralysis a risk
o GI dysfunction Paralytic ileus
o GU dysfunction Urine retention & hypoperfusion possible
22

o Respiratory dysfunction Anesthesia & immobility atelectasis
o Immobility consequences High potential for skin breakdown Potential for phlebitis
Discharge educationo Recommended physical activityo Pn meds & side effectso Psychological adjustment to brace, altered body imageo Assess family, peer supporto Schoolingo National Scoliosis Foundation
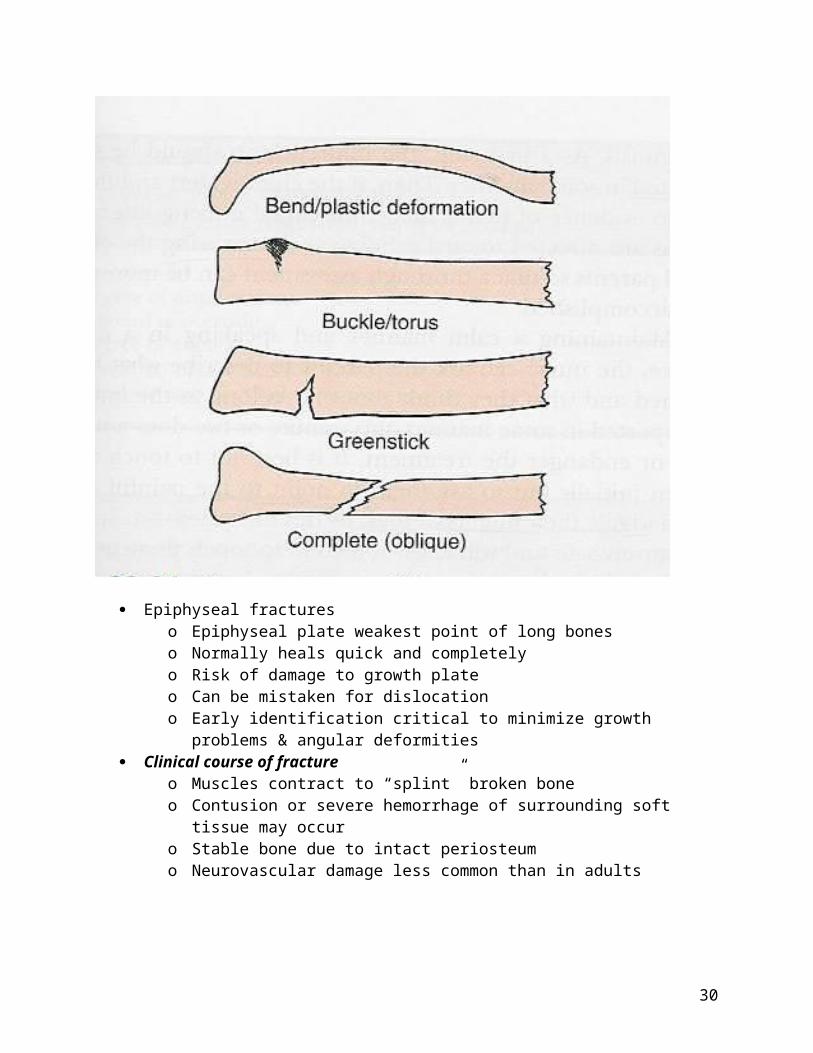
Fractures Bone structure in a child
o Ossification incomplete until 18-21 yearso Epiphyseal plate
Growth plateo Periosteum
Vascular membrane Critical for growth and healing of bone
Bone healing in childreno Generally faster in children due to thick vascular periosteumo Healing of bone
Neonate: 2-3 weeks Early childhood: 4 weeks Later childhood: 5-8 weeks Adolescence: 8-12 weeks Adult: 10-16 weeks
o Remodeling Fractures in infant & small child:
o Infancy: Birth trauma MVA Child abuse (twisting, rough handling, pulling) Periosteal bleeding not visible on x-ray for weeks after injury
o Small child: Multiple fractures at varied stages of healing warrants investigation
for abuse Causes:
o Breaking a fall- clavicle, forearmo Auto vs peds- femoral neck or femur
Most commonly seen in 4-7 years old Triad of auto vs peds injuries:
23
Femur fracture Trunk trauma Head injury
Epiphyseal fractureso Epiphyseal plate weakest point of long boneso Normally heals quick and completelyo Risk of damage to growth plateo Can be mistaken for dislocationo Early identification critical to minimize growth problems & angular
deformities Clinical course of fracture
o Muscles contract to “splint” broken boneo Contusion or severe hemorrhage of surrounding soft tissue may occuro Stable bone due to intact periosteumo Neurovascular damage less common than in adults
24

oo 5 P’s of ischemia from vascular injury:
Pain Pallor Pulselessness Paresthesia Paralysis
o Slight rise in WBC due to inflammation & hgb decreases Management
o Usually closed reduction & castingo Femur, humerus fractures may require hospitalization and traction o Internal fixation more quickly stabilizes injury (ORIF)o Casting
Bone will grown in the direction in which stress is placed on it- Wolff’s law
Critical to check for skin injury prior to application of cast Check for neurovascular compromise
TRACTIONo Primary goals of traction
To fatigue involved muscle and reduce muscle spasm To realign distal and proximal bone ends to promote satisfactory bone
healing To immobilize fracture until realignment has occurred and boen has
healed well enough to cast or splint o Complications of fractures
Circulatory impairment Nerve compression Compartment syndrome Epiphyseal damage Non union or malunion of bone Osteomyelitis Pulmonary emboli
25

Sprains & Strains Sprain:
o Ligament stretched or torn by force created as joint twisted Vessel, tendon, nerve damage common Joint laxity best indicator of severity of sprain
Strain:o Microscopic tear of tendon
Painful & swollen Usually do not occur immediately but over time
Management of soft tissue injurieso RICE
Rest Ice (some controversy about icing) Compression Elevation First 6-12 hours critical for treatment
Shin Splints Extensive running pressure on tibia Ligaments tear away from shaft of tibia Painful but rarely serious
Nursemaid’s elbow Most common dislocation in young children Usually <5 Sudden jerk and pull of arm Tx: pop back into place just like a shoulder
Osgood-Schlatter disease Painful inflammatory disorder of proximal tibia at point of insertion of patellar
tendon Repeated stress and overuse of quadriceps causes irregularities of growth Presentation:
o Knee pain, inflammation at tibial tubercleo Prominent tibial tubercleo Pn exacerbated by activity, improved with resto Hip examination necessary to rule out hip abnormalitieso Knee x-ray findings variable
Treatment:o Self-limitingo When growth of proximal tibia ceases, pain disappearso Rest, avoiding activity that contract quadriceps
26

Osteogenesis Imperfecta (OI) Group of heterogenous inherited disorders of connective tissue Characterized by excessive fragility and bone defects Defective periosteal bone formation and reduced cortical thickness of bones Hyperextensibility of ligaments Therapeutic management
o Primarily supportive careo Drugs of limited benefito May rule out OI if multiple fractures occuro Nursing care management:
Caution with handling to prevent fractures Fam education Occupational panning and genetic counseling
Legg-Calve-Perthes disease Self-limiting, idiopathic, occurs in juveniles ages 3-12 , more cmmon in males 4-8 yo Avascular necrosis of femoral head 10-15% of cases have bilateral hip involvement Most have delayed bone age Pathophysiology:
o Cause is unkown but involved disturbed circulation to the femoral head with ischemic aseptic necrosis
Treatment goal:o Keep head of femur in acetabulumo Containment with various appliances/deviceso Rest, no weight bearing initiallyo Surgery in some caseso Home traction in some cases
Prognosiso Self-limitingo Outcome has wide variations due to multiple factors
Nursing care management:o Identification of affected children & referral teaching care and managemento Compliance issues with child and family
OSTEOMYELITIS Inflammation and infection of bony tissue May be caused by exogenous or hematogenous sources Signs and symptoms begin abruptly, resemble symptoms of arthritis and leukemia Marked leukocytosis Bone cultures obtained from biopsy or aspirate Early x-rays may appear normal Bone scans for diagnosis
27
Exogenous Osteomyelitiso Infectious agent invades bone following penetrating wound, open fracture,
contamination in surgery, or secondary from extension from abscess or burn Hematogenous osteomyelitis
o Preexisting infectiono Source may be furuncles, skin infections, upper respiratory tract infection,
abscessed teeth, pyelonephritiso Any organism can cause osteomyelitiso Infective emboli travel to artiers in bone metaphysis, causing abscess
formation and bone destruction Therapeutic management of osteomyeleitis
o May have subacute presentation with walled off abscess rather than spreading infection
o Prompt, vigorous IV antibiotics for extended period (3-4 weeks or up to several months)
o Monitor hematologic, renal, hepatic responses to treatment Nursing care:
o COMPLETE bed rest & immobility of limbo Pn management concernso Long-term IV access (for antibiotic administration)o Nutritional considerationso Long-term hospitilzation, therapyo Psychosocial needs
Juvenile Idiopathic Arthritis (JIA) AKA juvenile rheumatoid arthritis, juvenile chronic arthritis, or idiopathic arthritis
of childhood Possible causes Peak ages: 1-3 years and 8-10 years Often undiagnosed Actually a heterogenous group of diseases:
o Pauciarticular onset – involves 4 or more jointso Polyarticular onset- involves 5 or more jointso Systemic onset- high fever, rash, hepatosplenomegaly, pericarditis, pleuritis,
lymphadenopathy) Symptoms may “burn out” and become inactive Chronic inflammation of synovium with joing effusion, destruction of cartilage, and
ankylosis of joints as disease progresses Symptoms:
o Stiffnesso Swellingo Loss of mobility in affected jointso Warm to touch, usually without erythemao Tender to touch in some caseso Symptoms increase with stressors
28
o Growth retardation Diagnostic evaluation of JIA
o No definitive diagnostic testso Elevated sedimentation rate in some caseso Antinuclear antibodies common, but not specific for JIAo Leukocytosis during exacerbationso Diagnosis based on criteria of American College of Rheumatology
Their diagnostic criteria: Age of onset <16 years 1 or more affected joints Duration of arthritis >6 weeks Exclusion of other forms of arthritis
Therapeutic management:o No cureo Goals of therapy:
Preserve function Prevent deformities Relieve symptoms
o Iridocyclitis, uveitis: Inflammation of iris & ciliary body Unique to JIA Requires opthalmologist
MEDSo NSAIDso SSARDso Corticosteroidso Cytotoxic agentso Immunologic modulators
Management of JIAo Therapy individualized to childo Physical & occupational therapyo Nutrition, exerciseo Splinting deviceso Pn managemento Prognosis
Systemic Lupus Erythematosus (SLE) A chronic, multisystem, autoimmune disease of the CT and blood vessels characterized
by inflammation on potentially any body issue Course and symptoms: unpredictable, mild to life threatening complications
o Clinical manifestations of systemic lupus erythematosus related to tissues involved:
Constitutional - fever, fatigue, weight loss, anorexia
29
Cutaneous - erythematous butterfly rash over bridge of nose and across cheeks, discoid rash, photosensitivity, mucocutaneous ulceration, alopecia, periungual telangiectasias
Musculoskeletal - arthritis, arthralgia, myositis, myalgia, tenosynovitis Neurologic- headache, seizure, forgetfulness, behavior change, change
in school performance, psychosis, chorea, stroke, cranial and peripheral neuropathy, pseudotumor cerebri
Pulmonary and cardiac- pleuritis, basilar pneumonitis, atelactasis, pericarditis, myocarditis, endocarditis
Renal- Glomerulonephritis, nephritic syndrome, hypertension GI- abdominal pain, NV, blood in stool, abdominal crisis, esophageal
dysfuntion, colitis Hepatic, splenic, and nodal- hepatomegaly, splenomegaly,
lymphadenopathy Hematologic- anemia, cytopenia Ophthalmologic- cotton wool spots, papilledema, retinopathy Vascular- Raynaud phenomenon, thrombophleitis, livedo reticularis
o Diagnostic Criteria for SLE:1. Malar rash- fixed malar erythema2. Discoid rash- patchy erythematous lesions3. Photosensitivity- pain with sun exposure4. Oronasal ulcers- painless ulcers in mouth or nose5. Arthritis- swelling, tenderness, or effusion in two or more peripheral
joints (nonerosive)6. Serositis- pleuritis, pericarditis7. Renal disorder- proteinuria, casts8. Neuro disorder- psychosis, seizures9. Hematologic disorder- hemolytic anemia, thrombocytopenia,
leucopenia, lymphopenia10. Immunologic disorder- anti double stranded DNA, anti Sm,
antiphospholipid antibodiesl lupus anticoagulant; false positive syphilis test (rapid plasma reagin [RPR])
11.Antinuclear antibodies Neonatal lupus: another form of lupus, which occurs when maternal auto antibodies cross the placenta and cause transient lupus like symptoms in a newborn, with
potential complications of heart block Therapeutic management
o Ensure child’s health by balancing meds necessary to avoid exacerbation and complications while preventing or minimizing treatment associated morbidity.
o MEDS Corticosteroids-to control inflammation administered in doses
sufficient to control and then taper to lowest suppressive dose Antimalarial (rash and arthritis) NSAIDS (relieve muscle and joint inflammation)
30

Immunosuppressive agents such as cyclophosphamide- renal and CNS disease mycophenolate, azathioprine, and methotrexate-effective, may
be used to control SLE and allow steroids to be reduced Antihypertensives, aspirin, antibiotics, may be needed to treat or
avoid complications General supportive care: sufficient nutrition, sleep and rest, exercise.
o Limit exposure to sun and ultraviolet B (UVB) light is limited bc of association with SLE exacerbation
Sunscreens, wearing sun resistant clothes, and altering outdoor activities; must be provided with great sensitivity to ensure compliance while minimizing the associated feeling of being different from peers
Nursing Care Managemento Principal nursing goal: help child and fam positively adjust to disease and
therapyo Learn S/S of exacerbationo Key issues:
Therapy compliance, body-image problems associated with rash, hair loss, and steroid therapy; school attendance; vocational activities, social relationships; sexual activity; and pregnancy.
Maintain reg med supervision, seek attention quickly when ill, or before elective surgical procedures, such as dental extraction, bc of potential needs for increasd steroids or prophylactic antibiotics
o Carry ID for disease and steroid dependence
31

![New Years Poster [Peds] 8 - FFF Enterprises · Title: New Years Poster [Peds] 8.5x11 Subject: New Years Poster [Peds] 8.5x11 Keywords: New Years Poster [Peds] 8.5x11 Created Date:](https://img.pdfslide.net/doc/110x75/5fd6db4c8a000945d6684aca/new-years-poster-peds-8-fff-title-new-years-poster-peds-85x11-subject-new.jpg)



























