Embed Size (px)
Citation preview

Examination of Exercise Effects on KneeOsteoarthritis Outcomes: Why Should the LocalMechanical Environment Be Considered?LEENA SHARMA
IntroductionOsteoarthritis (OA) is the most common form of humanarthritis. Almost every older adult has some evidence ofradiographic OA: 905 of 1,040 participants aged 55–65years in the Rotterdam study had definite radiographic OAin the hands, knees, hips, or spine (1). Although lessprevalent than radiographic OA, symptomatic OA is aleading cause of chronic disability. It is estimated that12% of Americans between ages 25 and 75 years haveclinical signs and symptoms of OA (2).
Disability due to OA is largely a result of knee or hipinvolvement. The risk of disability attributable to knee OAalone is as great as that due to cardiovascular disease andgreater than that due to any other medical condition inelderly persons (3). Beyond its direct effect, knee OA syn-ergistically increases the risk of disability originating fromother medical conditions (4).
Exercise is widely used in the management of knee OA,based on the results of predominantly short-term trials thatdemonstrate a clear beneficial effect on both symptomsand physical function. Less is known about the effect ofexercise on structural outcome—i.e., new OA develop-ment and progression of established OA—or on risk ofchronic disability.
Buckwalter and Lane propose that exercise (especiallyexercise that involves repetitive impact or torsion) mayhave a more deleterious effect in joints that have a localanatomic or physiologic impairment (5). From the per-spective of the local environment, OA knees are heteroge-
neous. Local mechanical factors may be thought of asfactors that have a clinically important biomechanical ef-fect, may be linked to joint anatomy or physiology, and arespecific to joint site. In published investigations, exerciseeffects have commonly been examined in samples nar-rowed to include subjects with OA predominantly at thejoint site of interest, e.g., the knee. To date, minimal atten-tion has been devoted to the examination of whether ex-ercise effects differ between subsets of OA knees basedupon local mechanical factors.
Statement of the ProblemIn studies of arthritis that deal with the effect of specificexercise programs, investigators have endeavored to exam-ine homogeneous samples of subjects. It is generally be-lieved that homogeneity has been achieved when the sam-ple includes subjects with a single type of arthritis, at asingle joint site of predominant involvement. These crite-ria for homogeneity are essential but may not be sufficient:a single type of arthritis (i.e., OA) even at a single joint site(the knee) is a heterogeneous condition in terms of thelocal joint-organ environment.
The same exercise program may have a dissimilar effecton different knee subsets based on local mechanical envi-ronment. Such variation in effect would dilute the de-tected impact of the intervention on study outcomes intherapeutic trials that consider the gamut of OA kneestogether, and may explain in part the relatively modestimpact of exercise interventions on physical function inmany trials. Ultimately, exercise interventions for thosewith knee OA may be more effective if they are tailored toknee subset.
Review of the LiteratureThere is increasing awareness that the profiles of determi-nants of symptoms, physical function, and structural dis-ease outcomes are not identical in OA; the effect of anyintervention on each of these outcomes needs to be spe-cifically examined. In the exercise literature dealing withknee OA, several studies demonstrate a beneficial effect ofexercise on symptoms and on patient-centered physicalfunction. In terms of structural outcome, there is minimal
Presented at the International Conference on Health Pro-motion and Disability Prevention for Individuals and Pop-ulations with Rheumatic Disease: Evidence for Exercise andPhysical Activity, St. Louis, MO, September 2001.
Leena Sharma, MD: Northwestern University MedicalSchool, Chicago, Illinois.
Address correspondence to Leena Sharma, MD, AssociateProfessor, Division of Rheumatology, Northwestern Uni-versity Medical School, 303 E. Chicago Avenue, Ward Build-ing 3-315, Chicago, IL 60611. E-mail: [email protected].
Submitted for publication May 17, 2002; accepted in re-vised form August 14, 2002.
Arthritis & Rheumatism (Arthritis Care & Research)Vol. 49, No. 2, April 15, 2003, pp 255–260DOI 10.1002/art.11006© 2003, American College of Rheumatology
SPECIAL ARTICLE
255

information on either risk of incident or progressive OA.Nonoccupational physical activity in general (with theexception of certain elite athletic activities) was not asso-ciated with an increase in the risk of newly occurring, kneeOA in most studies in which this has been examined (6).
The lack of attention to the effect of exercise on diseaseprogression is multifactorial. Even with x-ray acquisitionand measurement protocols that increase the ability todetect change, the study duration required to gauge theeffect of an exercise intervention on radiographic diseaseprogression may be prolonged and the necessary samplesize large. Magnetic resonance imaging (MRI)-based out-come measures may be superior in terms of reducing studyduration and sample size but are expensive. Ensuring com-pliance with any intervention in a therapeutic trial over along followup is challenging; this challenge can be evengreater with exercise interventions.
Despite these challenges, the effect of exercise on inci-dent OA, OA disease course, and disability each warrantfurther study. In theory, specific exercise programs mighthave some disease-modifying effect (i.e., delay progressionor worsening of OA) via beneficial actions on joint tissuesand the potential to enhance joint-protective mechanisms.Manipulating the local mechanical environment is rela-tively untapped as a strategy to delay disease progression.In addition, specific exercise programs may differ in theirimpact on physical function and on disability risk.
It is unlikely that a single exercise program will servethe heterogeneous process labeled “knee OA.” In the eval-uation of exercise intervention on structure and disabilityoutcomes, the local mechanical environment needs to beconsidered for at least 2 reasons: To stratify response tobroadly applied exercise approaches according to pres-ence/absence or severity of local impairment; and to de-velop exercise interventions that are tailored to knee OAsubset.
The biomechanics literature and clinical OA literatureoffer insight into which local factors to consider in thederivation of subsets of OA knees. Malalignment and lax-ity are local impairments that are common in knee OAthough of variable severity, influence load distribution atthe knee, and can be measured relatively easily in clinicalsettings. This is not equivalent to subsetting according toOA disease stage or severity. In many individuals, abnor-malities in alignment and/or laxity may be present prior toor at early stages of OA. Also, specific features of OAdisease may have opposing effects on a given local impair-ment (e.g., as described for laxity below).
It is likely that the effect of an exercise intervention willdiffer between knees that are malaligned versus closer toneutral in alignment, between lax versus stable knees.These are subsets that differ in structural vulnerability tothe forces that develop during exercise or physical activ-ity.
Examining exercise interventions according to kneealignment. Alignment (i.e., the hip-knee-ankle angle) is akey determinant of load distribution at the knee. In theory,any shift from a neutral or collinear alignment of the hip,knee, and ankle affects load distribution at the knee (7). Ina varus knee, the load-bearing axis passes medial to the
knee, and a moment arm is created that increases forceacross the medial compartment. In a valgus knee, the load-bearing axis passes lateral to the knee, and the resultingmoment arm increases force across the lateral compart-ment. Biomechanical studies support that varus and val-gus alignment increase medial and lateral load, respec-tively (7–9). Also, severity of varus alignment correlateswith the ratio of medial to lateral bone mineral density inpatients with OA, i.e., greater density in the higher load-bearing region (10).
During gait, disproportionate transmission of load to themedial compartment results from a stance-phase adduc-tion moment (11). The adduction moment reflects themagnitude of intrinsic compressive load on the medialcompartment (12). Varus-valgus alignment is a key deter-minant of this moment. Varus alignment further increasesmedial load during gait (13). Valgus alignment is associ-ated with an increase in lateral compartment peak pres-sures (9); however, more load is still borne medially untilmore severe valgus is present (14,15).
In theory, varus and valgus alignment may each be botha cause and result of progressive knee OA. Varus or valgusalignment that predates knee OA may be due to genetic,developmental, or posttraumatic factors. Animal modeldata support a link between preexisting varus or valgusalignment and OA development (7). Knee alignment thatresults from knee OA may be due to loss of cartilage andbone height.
A large body of literature gives evidence that preopera-tive alignment is a determinant of the outcome of surgicalprocedures involving the knee (e.g., arthroplasty, osteot-omy, complete or partial meniscectomy, meniscal debride-ment). In the operated knee, the development or progres-sion of OA is linked to several factors not at play in theexamination of natural progression (e.g., nature of surgery,stage of OA at time of surgery, complications). Consider-ably less attention has been paid to the role of knee align-ment in the nonsurgical, natural evolution of knee OA.Few longitudinal studies have dealt with alignment andthe natural history of OA.
Schouten et al found that subject recollection of bowlegs or knock knees in childhood was associated with a5-fold increase in the risk of OA progression (odds ratio[OR] 5.13, 95% confidence interval [95% CI] 1.14–23.1)over a 12-year period, after adjusting for age, sex, and bodymass index (BMI) (16). In another study involving patientsfrom a hospital practice who had not undergone surgery,and in whom alignment was considered at the end offollowup, 50% of 35 varus knees had progressive jointspace narrowing (17).
We recently reported on the effect of varus and valgusalignment measured at baseline on subsequent progressionof medial and lateral tibiofemoral OA, respectively, in 240community-recruited subjects with knee OA (with definiteosteophyte presence and at least a little difficulty withphysical function) (18). Alignment was measured as theangle made by the intersection of the femoral and tibialmechanical axes from a full-limb radiograph. Knees withgrade 3 (most severe) joint space narrowing at baselinewere excluded.
First, the relationship between baseline varus alignment
256 Sharma

(varus in degrees as a positive value, neutral 0, and valgusin degrees as a negative value) and magnitude of decreasein medial joint space width (from baseline to 18 months onsemiflexed, fluoro-confirmed knee radiographs correctedfor magnification error), each as a continuous variable, wasexamined in the dominant knee of each subject usinglinear regression. Severity of varus alignment correlatedwith the magnitude of loss of medial joint space width(R � 0.52, P � 0.0001). Similarly, the relationship betweenbaseline valgus alignment and magnitude of decrease inlateral joint space width was examined. Severity of valgusalignment correlated with the magnitude of loss in lateraljoint space width (R � 0.35, P � 0.0001). These relation-ships persisted in analyses adjusted for age, sex, and BMI.
Second, the relationship between baseline alignmentand compartment-specific progression, defined as a 1grade increase in grade of severity of joint space narrowingwas examined. Odds ratios were calculated using logisticregression and generalized estimating equations method-ology to include data from one or both knees of eachsubject.
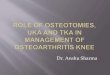
As shown in Figure 1, varus versus nonvarus at baselinewas associated with a 4-fold increase in the odds of medialprogression after adjusting for age, sex, and BMI. In calcu-lating risk in varus versus nonvarus knees, we recognizedthat medial OA may be associated with varus, valgus, orneutral alignment. Therefore, the risk associated with va-rus alignment was compared with the risk conferred byany other possible alignment for a given knee. To deter-mine the progression risk associated with varus alignmentwhen the comparison group had neutral or nearly neutralknees, we repeated the analysis with a referent groupconsisting of neutral (0°) or mildly valgus (�2°) knees.Varus alignment was still associated with a 3-fold increase
in risk of medial progression in adjusted analyses (Figure1).
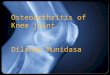
Valgus versus nonvalgus (referent) alignment at baselinewas associated with an almost 4-fold increase in the oddsof lateral progression during the subsequent 18 months(Figure 2). This relationship persisted after adjustment forage, sex, and BMI. When the referent group had neutral ornearly neutral (�2° varus) knees, valgus alignment wasassociated with a more than 3-fold increase in the odds ofsubsequent lateral OA progression (Figure 2). It is likelythat malalignment and OA progression are in a viciouscycle. The results of this study support the concept that,whether a given alignment precedes or results from OAdisease, malalignment may contribute to subsequent pro-gression.
The burden of malalignment at baseline also predicteddeterioration in physical function between baseline and 18months (18). Subjects were classified into 1 of 3 groups,i.e., subjects who had no knees with alignment �5°; 1 kneewith alignment �5°; both knees with alignment �5°. Phys-ical functional outcome was analyzed as a continuousvariable, i.e., baseline to 18 month change in chair standrate (time required to complete 5 chair stands, converted toa rate or number of stands per minute). As shown in Table1, change did not differ between the first 2 groups. How-ever, a significantly greater deterioration in chair standperformance was found in subjects having both knees ver-sus no knees with alignment �5°. The difference betweenthese groups persisted after adjusting for age, sex, BMI,and pain.
We also explored the relationship between burden ofmalalignment and functional decline, designating declineas �20% worsening in rate of chair stand performance.Thirty-four subjects (16% of the 215 subjects able to per-form the test at baseline) experienced functional decline
Figure 2. The odds of lateral progression conferred by valgusalignment are presented for 2 reference groups: nonvalgus kneesand neutral/mild varus knees (i.e., neutral or � 2° varus). Theunadjusted odds ratio (OR) for valgus versus nonvalgus (referent)was 3.88, 95% confidence interval (95% CI) 1.82–8.24; and forvalgus versus neutral/mild varus (referent) 3.23, 95% CI 1.30–8.05. The adjusted (for age, sex, and body mass index [BMI]) ORfor valgus versus nonvalgus was 4.89, 95% CI 2.13–11.20; and forvalgus versus neutral/mild varus 3.42, 95% CI 1.31–8.96. Kneeswith grade 3 (most severe grade) joint space narrowing in eitherthe medial or lateral compartment at baseline were excluded. Thenumber for analysis involving the first reference group was 381knees. The number for analysis involving the second referencegroup was 278 knees. —●— � valgus versus nonvalgus; ��●��� valgus versus neutral/mild varus.
Figure 1. The odds of medial progression conferred by varusalignment are presented for 2 reference groups: nonvarus kneesand neutral/mild valgus knees (i.e., neutral or � 2° valgus). Theunadjusted odds ratio (OR) for varus versus nonvarus (referent)was 5.00, 95% confidence interval (95% CI) 2.77–9.02; and forvarus versus neutral/mild valgus (referent) 3.54, 95% CI 1.85–6.77. The adjusted (for age, sex, and body mass index [BMI]) ORfor varus versus nonvarus was 4.09, 95% CI 2.20–7.62, and forvarus versus neutral/mild valgus 2.98, 95% CI 1.51–5.89. Kneeswith grade 3 (most severe grade) joint space narrowing in eitherthe medial or lateral compartment at baseline were excluded. Thenumber for analysis involving the first reference group was 381knees. The number for analysis involving the second referencegroup was 281 knees. —●— � varus versus nonvarus; ��●�� �varus versus neutral/mild valgus.
Mechanical Environment and Knee OA 257

by this definition. The proportion of subjects experiencingdecline steadily rose as the burden of malalignment in-creased from none to 1 to 2 knees. The odds of functionaldecline were doubled (OR 2.33, 95% CI 0.97–5.62) byhaving one knee with alignment �5° versus no knee withalignment �5°, and were tripled by having both kneeswith alignment �5° versus no knee with alignment �5°(OR 3.22, 95% CI 1.28–8.12).
In summary, there is biomechanical evidence that align-ment influences load distribution and longitudinal evi-dence that this biomechanical effect is clinically relevantin knee OA structural and functional outcome.
Examining exercise interventions according to kneelaxity. Stability is an important component of the me-chanical environment of any joint. Knee laxity may bebroadly defined as abnormal displacement or rotation ofthe tibia with respect to the femur (19). In the unloadedstate, knee stability is provided by the ligaments, capsule,and other soft tissues, and in the loaded state by interac-tions between these tissues, condylar geometry, and con-tact forces generated by muscle activity and gravitationalforces (19). Dynamic stability also depends upon proprio-ceptive input and reflex and centrally driven muscle ac-tivity (20). During normal motion, ligament stiffness islow. In the setting of large forces, soft tissue stiffnessincreases to limit displacement between the femur andtibia, protecting cartilage and other tissues from injury(21).
As clinically assessed, joint laxity represents an impair-ment for which muscle activity may or may not be able tocompensate. Laxity results in more abrupt joint motionwith larger displacements. Deleterious effects of laxity in-clude alteration of the congruence and regions of contactof the opposing articular surfaces, and an increase in shearand compression forces on some regions of the articularcartilage (22). Bruns et al demonstrated that ligament di-vision in cadaver knees resulted in further increases inpeak articular pressure, even in the presence of severemalalignment (9). Such alterations in pressure may lead tocartilage damage, lessening the subsequent ability of car-tilage to withstand stress (21).
In individuals without arthritis, frontal plane or varus-valgus laxity may reflect primary capsuloligamentous lax-ity (related to genetic factors or aging-related soft tissuechanges) or prior injury. In knees with moderate to severeOA, laxity may be due to loss of cartilage and/or boneheight, chronic capsuloligamentous stretch, or combina-
tions of ligamentous, meniscal, muscular, and capsularpathology. The ligaments and the menisci of the OA kneedevelop fraying and cracking similar to what is seen inarticular cartilage (23).
The paucity of clinical information on varus-valgus lax-ity in knee OA relates in part to the absence of measure-ment systems. In clinical settings, varus-valgus laxity ismost commonly assessed by physical exam, an unreliableapproach (24,25). Sources of variation during the physicalexam test have been identified as inadequate immobiliza-tion of the thigh and ankle, incomplete muscle relaxation,variation of the knee flexion angle, variation of load ap-plied, and imprecise measures of rotation with load appli-cation (24–26). Devices to measure anterior-posterior (AP)laxity are commercially available.
Aging is associated with alterations in ligament proper-ties. Ligament stiffness and ultimate load decreased sub-stantially with specimen age in a study of human femur-anterior cruciate ligament (ACL)-tibia complex involving 3groups, i.e., younger (22–35 years), middle (40–50 years),and older (60–97 years) (28). Ultimate load was more than300% higher in the younger group than in the older group.In subjects without clinical or radiographic evidence ofOA, a modest correlation between varus-valgus laxity andage has been described (27). Such age-related changes maybe intensified by anatomic factors, by patterns of use, andby comorbid conditions.
The knee injury literature provides some evidence of theclinical importance of laxity. OA develops in a caninemodel by inducing an unstable joint via complete ACLtransection. Lundberg and Messner found that while themajority of those with isolated medial collateral ligament(MCL) injuries (grades I–II) did not develop OA by 10years, combined injury to the MCL and the ACL led to OAin close to 50% of patients (29). Kannus reported that 50%of those with a grade III sprain of the lateral collateralligament developed OA within 8 years of injury, and that63% of those with grade III sprains of the MCL developedOA within 9 years (30,31). Attention to concomitant injuryto tissues other than ligaments varies between injury stud-ies.
There is evidence that a portion of the varus-valguslaxity present in OA knees predates the development offull-blown disease. In support of this concept, we foundthat varus-valgus laxity was greater in subjects with kneeOA—even in their uninvolved knee or their mildly in-volved knee—than in older subjects without any clinicalor radiographic evidence of knee OA (27). These differ-
Table 1. Alignment group differences in the baseline to 18-month change in chair stand performance*
Groups based onmalalignment burden
Difference between groups (95% CI)
UnadjustedAdjusted for age,
sex, and BMIAdjusted for age,
sex, BMI, and pain
One knee �5° versus no knee �5° 0.48 (�1.40, 2.36) 0.43 (�1.44, 2.31) 0.17 (�1.66, 2.01)Two knees �5° versus no knee �5° 2.88 (0.75, 5.01) 2.73 (0.52, 4.94) 2.23 (0.05, 4.41)
* 95% confidence interval (95% CI) that excludes 0 represents a significant difference between groups. Subjects with 2 knees with alignment �5° hadsignificantly greater deterioration in chair stand rate between baseline and 18 months versus subjects with 0 knees with alignment �5°, in unadjustedand adjusted analyses. BMI � body mass index.
258 Sharma

ences persisted after adjusting for age and sex. AlthoughBrage et al did not statistically compare the knees withmild OA with the knees of older control subjects, mildlyarthritic knees in their study appear to be more lax thanthe knees of the control subjects (32).
Although some portion of the varus-valgus laxity ofidiopathic OA appears to predate the development of full-blown disease, specific aspects of the disease itself exac-erbate the problem. Varus-valgus laxity increased as jointspace decreased, and was greater in knees with evidence ofbony attrition (27). This is presumably related to the pointsof ligamentous attachment to the femur and tibia movingcloser together as a result of loss of bone and cartilageheight.
It is likely that osteophytes prevent laxity to some ex-tent, as demonstrated by Pottenger et al, who measuredvarus-valgus laxity before and after intraoperative osteo-phyte removal in patients with advanced knee OA (33).Given their findings, it is possible that, at earlier stages ofOA, osteophytes make some contribution to varus-valgusstability. With progressive disease, loss of cartilage andbone height appear to override this stabilizing effect. Atadvanced stages, although osteophytes continue to havesome stabilizing activity, they cannot prevent further in-creases in varus-valgus laxity. The opposing effects ofspecific features of OA on varus-valgus laxity may havecontributed to the mixed results seen when studies haverelied on global radiographic assessment of OA status.
Using a KT1000 arthrometer, no relationship betweenAP laxity and age or sex in subjects without OA wasdetected (27). The AP laxity did not differ between sub-jects with OA and controls, and was not associated withspecific features or global grade of OA severity. In studiesusing the Genucom computerized measurement system,AP laxity declined with increasing severity of OA. In onestudy including arthroscopic examination, the decline inAP translation was noted in spite of the fact that amongthose with severe OA, ACLs were absent or torn in themajority of subjects (34). The ACL type did not predict APtranslation. Joint stiffness due to capsular changes or os-teophytic growth may override the cruciate ligament in-sufficiency that can occur in progressive knee OA.
We have found that varus-valgus laxity, i.e., the sum ofright and left knees, was associated with physical functionin cross-sectional analyses (35). Physical function wasworse in subjects with high laxity (Western Ontario andMcMaster Universities Osteoarthritis Index physical func-tion score 26.5 � 13.3) than low laxity (20.8 � 13.8; P �0.008). There is evidence that varus-valgus laxity maymediate in the relationship between muscle strength andphysical functioning in patients with knee OA (35). Laxitynecessitates that greater muscular work be directed towardjoint stabilization. We found that greater laxity was con-sistently associated with a weaker relationship betweenstrength (quadriceps or hamstring) and physical function(self reported or observed). These results raise the possi-bility that muscle strengthening may have less impact onphysical function in high laxity than low laxity knees, andthat addressing varus-valgus laxity may improve the out-come of strengthening intervention.
In summary, there is biomechanical evidence and cross-
sectional clinical evidence that varus-valgus laxity is a keylocal factor in the course of knee OA.
ConclusionsKnees with OA are heterogeneous in terms of the localmechanical environment. Differences in the local environ-ment explain, in part, interindividual variation in the rateof OA disease progression. The same exercise programmay have a dissimilar effect on different knee subsetsbased upon local environment. Malalignment and laxityare local factors to consider in the derivation of subsets ofOA knees. These factors are suggested as a first step; thelist of relevant mechanical factors to apply toward devel-oping subsets will extend beyond the factors describedhere.
There is evidence that alignment influences load distri-bution at the knee, is a determinant of surgical outcomes,increases the risk of natural progression of knee OA in theexpected compartment-specific fashion, and increases therisk of functional decline in persons with knee OA. Thereis evidence that varus-valgus laxity has deleterious biome-chanical effects that may lead to cartilage damage, in-creases with age, is associated with a greater risk of OA inthe setting of ligament injury, is present in OA patients tosome extent before full-blown disease, is made worse byspecific aspects of OA disease, is associated with worsephysical function, and alters the strength/function rela-tionship.
The effect of exercise or physical activity may differbetween knees that are malaligned versus closer to neutralin alignment, between lax versus more stable knees. Mal-alignment and laxity may reduce the impact of genericexercise programs on functional outcome, and may changethe effect of exercise on structural outcome.
These findings point to areas for future research. A pro-file of key local mechanical factors for each joint siteshould be identified. In exercise trials of knee OA, inves-tigators should consider stratifying results according toalignment (if feasible considering both direction and se-verity of malalignment) and varus-valgus laxity, as well asother key mechanical factors. Certain knee subsets (e.g.,malaligned knees or lax knees) are likely to benefit froma more tailored approach; exercise interventions shouldbe developed for these subsets. Exercise trials shouldstrive to include structure and disability outcomes. In-terventions (e.g., orthotics) directed towards laxity- andmalalignment-associated stresses on the knee should befurther developed and studied. Methods to assess laxityand alignment in clinical settings should be developed.
REFERENCES
1. Meulenbelt I, Bijkerk C, de Wildt SCM, Miedema HS, Valk-enburg HA, Breedveld FC, et al. Investigation of the associa-tion of the CRTM and CRTL-1 genes with radiographicallyevident osteoarthritis in subjects from the Rotterdam study.Arthritis Rheum 1997;40:1760–5.
2. Lawrence RC, Helmick CG, Arnett FC, Deyo RA, Felson DT,Giannini EH, et al. Estimates of the prevalence of arthritis andselected musculoskeletal disorders in the United States. Ar-thritis Rheum 1998;41:778–99.
3. Guccione AA, Felson DT, Anderson JJ, Anthony JM, Zhang Y,
Mechanical Environment and Knee OA 259

Wilson PWF, et al. The effects of specific medical conditionson the functional limitations of elders in the FraminghamStudy. Am J Public Health 1994;84:351–7.
4. Ettinger WH, Davis MA, Neuhaus JM, Mallon KP. Long-termphysical functioning in persons with knee osteoarthritis fromNHANES I: effects of comorbid medical conditions. J ClinEpidemiol 1994;47:809–15.
5. Buckwalter JA, Lane NE. Current concepts: athletics and os-teoarthritis. Am J Sports Med 1997;25:873–81.
6. Sharma L. Physical activity and injury and their relationshipwith knee osteoarthritis in epidemiologic studies. In: GarretW, Lester G, McGowan J, Kirkendahl D, editors. Women’shealth in sports and exercise. Rosemont (IL): American Acad-emy of Orthopedic Surgeons; 2001.
7. Tetsworth K, Paley D. Malalignment and degenerative ar-thropathy. Orthop Clin North Am 1994;25:367–77.
8. McKellop HA, Llinas A, Sarmiento A. Effects of tibial mal-alignment on the knee and ankle. Orthop Clin North Am1994;25:415–23.
9. Bruns J, Volkmer, M, Luessenhop S. Pressure distribution atthe knee joint: influence of varus and valgus deviation with-out and with ligament dissection. Arch Orthop Trauma Surg1993;133:12–9.
10. Wada M, Maezawa Y, Baba H, Shimada S, Sasaki S, Nose Y.Relationships among bone mineral densities, static align-ment, and dynamic load in patients with medial compartmentknee osteoarthritis. Rheumatology 2001;40:499–505.
11. Andriacchi TP. Dynamics of knee malalignment. Orthop ClinNorth Am 1994;25:395–403.
12. Schipplein OD, Andriacchi TP: Interaction between activeand passive knee stabilizers during level walking. J OrthopRes 1991;9:113–9.
13. Hsu RWW, Himeno S, Conventry MB, Chao EYS. Normalaxial alignment of the lower extremity and load-bearing dis-tribution at the knee. Clin Orthop 1990;255:215–27.
14. Johnson F, Leitl S, Waugh W. The distribution of load acrossthe knee: a comparison of static and dynamic measurements.J Bone Joint Surg Br 1980:62B:346–9.
15. Harrington IJ. Static and dynamic loading patterns in kneejoints with deformities. J Bone Joint Surg Am 1983;65A:247–59.
16. Schouten JSAG, van den Ouweland FA, Valkenburg HA. A 12year follow up study in the general population on prognosticfactors of cartilage loss in osteoarthritis of the knee. AnnRheum Dis 1992;51:932–7.
17. Miller R, Kettelkamp DB, Laubenthal KN, Karagiorgos A,Smidt GL. Quantitative correlations in degenerative arthritisof the knee. J Bone Joint Surg Am 1973;55A:956–62.
18. Sharma L, Song J, Felson DT, Cahue S, Shamiyeh E, DunlopDD. The role of knee alignment in disease progression andfunctional decline in knee osteoarthritis. JAMA 2001;286:188–95.
19. Markolf KL, Bargar WL, Shoemaker SC, Amstutz HC. The roleof joint load in knee stability. J Bone Joint Surg Am 1981;63A:570–85.
20. Solomonow M, D’Ambrosia R. Neural reflex arcs and musclecontrol of knee stability and motion. In: Scott WN, editor. Theknee. St. Louis (MO): Mosby; 1994.
21. Woo SL-Y, Fenwick JA, Kanamori A, Gil JE, Saw SSC, VogrinTM. Biomechanical considerations of joint function. In: Mos-kowitz RM, Howell DS, Altman RD, Buckwalter JA, GoldbergVM, editors. Osteoarthritis: diagnosis and medical/surgicalmanagement. Philadelphia: W.B. Saunders; 2001.
22. Buckwalter JA, Lane NE, Gordon SL. Exercise as a cause ofosteoarthritis. In: Kuettner KE, Goldberg VM, editors. Osteo-arthritic disorders. Rosemont (IL): American Academy of Or-thopedic Surgeons; 1995. p. 405–17.
23. Hough AJ. Pathology of osteoarthritis. In: Moskowitz RM,Howell DS, Altman RD, Buckwalter JA, Goldberg VM, editors.Osteoarthritis: diagnosis and medical/surgical management.Philadelphia: W.B. Saunders; 2001.
24. Cushnaghan J, Cooper C, Dieppe P, Kirwan J, McAlindon T,McCrae F. Clinical assessment of osteoarthritis of the knee.Ann Rheum Dis 1990;49:768–70.
25. Noyes FR, Cummings JF, Grood ES, Walz-Hasselfeld KA,Wroble RR. The diagnosis of knee motion limits, subluxa-tions, and ligament injury. Am J Sports Med 1991;19:163–71.
26. Markolf KL, Graff-Radford A, Amstutz HC. In vivo knee sta-bility, a quantitative assessment using an instrumented clin-ical testing apparatus. J Bone Joint Surg Am 1978;60A:664–74.
27. Sharma L, Lou C, Felson DT, Dunlop DD, Kirwan-Mellis G,Hayes KW, et al. Laxity in healthy and osteoarthritic knees.Arthritis Rheum 1999;42:861–70.
28. Woo SL, Hollis JM, Adams DJ, Lyon RM, Takai S. Tensileproperties of the human femur-anterior cruciate ligament-tibia complex: the effects of specimen age and orientation.Am J Sports Med 1991;19:217–25.
29. Lundberg M, Messner K. Ten-year prognosis of isolated andcombined medial collateral ligament ruptures. Am J SportsMed 1997;25:2–6.
30. Kannus P. Nonoperative treatment of grade II and III sprainsof the lateral ligament compartment of the knee. Am J SportsMed 1989;17:83–8.
31. Kannus P. Long-term results of conservatively treated medialcollateral ligament injuries of the knee joint. Clin Orthop1988;226:103–12.
32. Brage ME, Draganich LF, Pottenger LA, Curran JJ. Knee laxityin symptomatic osteoarthritis. Clin Orthop 1994;304:184–9.
33. Pottenger LA, Phillips FM, Draganich LF. The effect of mar-ginal osteophytes on reduction of varus-valgus instability inosteoarthritic knees. Arthritis Rheum 1990;33:853–8.
34. Wada M, Imura S, Baba H, Shimada S. Knee laxity in patientswith osteoarthritis and rheumatoid arthritis. Br J Rheumatol1996;35:560–3.
35. Sharma L, Hayes KW, Felson DT, Buchanan TS, Kirwan-Mellis G, Lou C, et al. Does laxity alter the relationship be-tween strength and physical function in knee osteoarthritis?Arthritis Rheum 1999;42:25–32.
260 Sharma