Embed Size (px)
Citation preview

EXAMINING THE WILBARGER’S DEEP PRESSURE AND PROPRIOCEPTIVE
TECHNIQUE FOR TREATING CHILDREN WITH SENSORY DEFENSIVENESS
USING A MULTIPLE SINGLE CASE STUDY APPROACH
By Anoo Bhopti
Thesis submitted for the Degree of Master of Biomedical Science Part 1
Department of Occupational Therapy
Faculty of Medicine, Nursing and Health Sciences
Monash University
August 2010

Copyright Notices Notice 1 Under the Copyright Act 1968, this thesis must be used only under the normal conditions of scholarly fair dealing. In particular no results or conclusions should be extracted from it, nor should it be copied or closely paraphrased in whole or in part without the written consent of the author. Proper written acknowledgement should be made for any assistance obtained from this thesis. Notice 2 I certify that I have made all reasonable efforts to secure copyright permissions for third-party content included in this thesis and have not knowingly added copyright content to my work without the owner's permission.

2
Acknowledgements
I would like to acknowledge several people who have assisted me during the two
years of my study and for producing this thesis. Firstly, I would like to thank my family,
my all time rock – my husband, Behram, who always encouraged me to follow my dreams,
and my cheer leader daughter, Nikita, who makes me laugh; to my wonderful parents,
Sushma and Jeet, who always believe in me and made me who I am. Then, I would like to
thank all the families that worked with me and their children, for their commitment and
enthusiasm and for the wonderful conversations that we had that helped me understand
many aspects in my work and in my study.
I would also like to thank Yooralla, for their continued support and trust and for
allowing me the time and encouragement that is so much needed at such times. All my co-
workers have been very supportive and excited about this study and I thank you all. I would
like to thank the Department of Education and Early Childhood Development for their
generous scholarship that they awarded me to assist me in completing this study.
Most important of all, I would like to thank my supervisor, Dr. Ted Brown. I am so
grateful for your encouragement, for always being there, even across the seas, and for being
so vigilant and making me a better occupational therapist and a researcher. Your assistance
with my drafts, your insights and constant words of wisdom have kept me motivated and
your relaxed but critical attitude has allowed me to reach the end of my thesis with little
doubt and loads of self esteem. I would also like to thank Monash University faculty and all
the staff (especially Carissa Lyons, for that very timely phone assistance) that have been so
helpful. And lastly, I would like to thank my all time companion, Keanu, my dog who sat
and listened to all my drafts and frustrations with patience and love.

3
Candidate’s Statement of Originality
I declare that the work presented in this thesis, to the best of my knowledge and
belief, is original and my own work, except as acknowledged in the text. I hereby declare
that I have not submitted this material either in whole or part, for a degree at this or any
other university.
Anoo Bhopti
August 2010

4
Abstract
Background
The need for occupational therapy services has risen exponentially (Royeen, 2010)
especially in paediatrics, and the sensory integration framework is used commonly when
working with children. A variety of intervention approaches are used within this
framework. The Wilbargers’ approach is one such approach that is known to be used by
occupational therapists for children presenting with sensory defensiveness or over
responsivity. However, lack of sufficient research in this area leads to a need for examining
this approach.
Purpose
The purpose of this study was to examine the Wilbargers’ Deep Pressure and
Proprioceptive Technique (DPPT) in children presenting with sensory defensiveness and to
investigate parent/carer perspectives on the effectiveness of DPPT.
Method
A prospective multiple single case design was used with convenient sampling. Five
children eligible for early childhood intervention services were recruited for this study and
three tools were used to collect data, namely the Sensory Profile (Dunn, 1999), sensory
interviews and parent questionnaire at the end of the study. Goals were drawn with the
parent/carer, and Goal Attainment Scaling (GAS), (Kiresuk & Shermann, 1968) was used as
an outcome measure.
Each child participated in a six week regime involving the Wilbargers’ DPPT every two
hours along with sensory diet activities concurrently at least three times per day (Wilbarger
& Wilbarger, 2007). Participants were reviewed weekly using GAS.

5
Results
The results indicated a significant statistical difference in scores on Sensory Profile
scores and GAS scores. The parent questionnaires also indicated that the parents rated
‘importance’ as highest indicating that it is very important for them to reduce their child’s
sensory defensive behaviours and 4 out of 5 parents reported that they felt the intervention
was effective for their child.
Implications
Implications for future research include completing similar studies using larger
sample sizes and over larger geographical regions. Also including children with varying
diagnostic groups (such as child and adolescent mental health, paediatric neurology,
paediatric genetic disorders and from school aged population) where sensory defensive
behaviours may be interfering with school function is suggested.
Conducting randomised control studies and qualitative studies investigating the
parents/caregivers experiences of implementing the DPPT regime with their child is
recommended. Conducting more studies within Australian context is required as the
majority of studies are from the United States.
Conclusion
The results from the Sensory Profile scores and GAS scores in this study seem to
support the use of the DPPT in children presenting with sensory defensiveness. The
comments and results from parent questionnaires and interviews support the use of DPPT
and most parents found it conducive to family centred practice principles of providing
information and empowerment to them as well as increased participation of their children
in everyday routines and settings.

6
Table of contents
Acknowledgements 2
Candidate’s statement of originality 3
Abstract 4
Chapters 6
List of Tables 9
List of Figures 10
List of abbreviations 11
List of Appendices 13
Chapter 1: Introduction to thesis 14
1.1 Introduction 14
1.2 Clinical application 15
1.3 Thesis overview 15
1.4 Search strategy 16
Chapter 2: Literature Review 18
2.1 Introduction 18
2.2 Occupational therapy practice 18
2.2.1 Scope 18
2.2.2 Theoretical framework 19
2.2.3 Paediatrics 20
2.3 An overview of sensory integration and sensory processing theory 21
2.3.1 Models and terminology in sensory-based theory 22
2.3.1. a Sensory integration and sensory processing 27
2.3.1. b Sensory modulation and responsivity 28
2.3.2 Disorders of sensory systems 30

7
2.3.3 Intervention approaches 34
2.3.3. a The Wilbargers’ ‘Deep Pressure and Proprioceptive
Technique’ (DPPT) 38
2.4 Evidence based practice and research in sensory- based occupational
therapy intervention approaches 41
2.4.1 Summary of research available on the Wilbargers’ DPPT 43
2.5 Summary 55
Chapter 3: Methodology 56
3.1 Introduction 56
3.2 Research aims 56
3.3 Design 56
3.4 Participants 57
3.4.1 Inclusion and exclusion criteria 57
3.5 Ethical considerations 58
3.6 Instrumentation 60
3.6.1 The Sensory Profile (Dunn, 1999) 60
3.6.2 Sensory history/ interview 62
3.6.3 Parent Questionnaire 63
3.6.4 Goal Attainment Scaling 64
3.7 Procedures and data collection 66
3.8 Data analysis 68
3.8.1 Paired samples t- tests 68
3.8.2 Goal Attainment Scaling 68
3.8.3 Sensory Profile 69
3.9 Summary 70
Chapter 4: Results 71

8
4.1 Introduction 71
4.2 Participant demographics 71
4.3 Results from analysis 72
4.3.1 Descriptive statistics 72
4.3.1.1 Sensory Profile – descriptive statistics 72
4.3.1.2 GAS – descriptive statistics 77
4.3.2 Paired samples t-tests 82
4.3.2.1 Sensory Profile results 82
4.3.2.2 GAS results 85
4.3.2.3 Parent questionnaire results 86
4.4 Summary 86
Chapter 5: Discussion 87
5.1 Introduction 87
5.2 Sensory Profile 87
5.3 Goal Attainment Scaling (GAS) 88
5.4 Wilbargers’ DPPT 91
5.5 Family-Centred Practice and sensory-based interventions 93
5.6 Summary 95
Chapter 6: Limitations, Future Research, Implications, and Conclusion 96
6.1 Introduction 96
6.2 Limitations 96
6.3 Recommendations for future research 96
6.4 Implications for future research and for the profession 97
6.5 Conclusions 98
References 100
Appendices 115

9
List of Tables
Table
number
Title Page
Number
Table 1 Models of occupational therapy practice 20
Table 2 Sensory systems 22
Table 3 Definition of terms commonly used in a sensory –based model of practice
25
Table 4 Some intervention approaches within sensory – based occupational therapy
36
Table 5 Oxford Centre for Evidence based medicine 44
Table 6 Summary of research papers on the Wilbargers’ Deep Pressure and Proprioceptive Technique
45
Table 7 GAS goals (Kirusek et al., 1994) 65
Table 8 A sample of GAS 69
Table 9 Quadrant definitions, Sensory Profile 70
Table 10 Descriptive statistics, Sensory Profile, Time 1(T1) 72
Table 11 Descriptive statistics, Sensory Profile, Time 2(T2) 72
Table 12 Section raw scores, Sensory Profile, T1 v/s T2 75
Table 13 Sum of scale scores, GAS, time 1 to time 7 79
Table 14 Average scale scores, GAS, time 1 to time 7 80
Table 15 t-scores, GAS, time 1 to time 7 81
Table 16 Paired samples statistics – quadrant scores, Sensory Profile
83
Table 17 Paired samples test – quadrant scores, Sensory Profile
84
Table 18 Paired samples statistics, GAS 85
Table 19 Paired samples tests, GAS 85
Table 20 Descriptive statistics, parent questionnaire 86

10
List of Figures
Figure Number Table/Figure Name Page
Number
Figure 1
Relationship between behavioural responses and neurological thresholds (Dunn, 1999)
30
Figure 2 Classification of SPD Patterns and subtypes (Miller, 2006; Henry, 2007)
31
Figure 3 Sensory Profile – Quadrant raw scores, T1 v/s T2 73
Figure 4 Sensory Profile – section raw scores T1 v/s T2 74
Figure 5 GAS – Sum of scale scores, average scale scores & t-scores from T1 to T7 for all 5 participants
79
Figure 6 Sum scale scores GAS, time 1 to time 7 80
Figure 7 Average scale scores, GAS, time 1 to time 7
81
Figure 8 Mean t-scores, GAS, time 1 to time 7 82

11
List of Abbreviations
AJOT – American Journal of Occupational Therapy
ASD – Autism Spectrum Disorder
CAOT – Canadian Association of Occupational Therapists
CNS – Central Nervous System
DPPT – Deep Pressure and Proprioceptive Technique
DSM-IV – Diagnostic Statistical Manual -IV
ECIS – Early Childhood Intervention Services
EDR – Electro Dermal Responses
GAS – Goal Attainment Scaling
ICF – International Classification of Function
OT/SI – Occupational Therapy / Sensory Integration
SI – Sensory Integration
SMD – Sensory Modulation Disorder
WFOT – World Federation of Occupational Therapists
WHO – World Health Organization

12
List of Appendices
Appendix
No
Description Page
number
Appendix 1 Evolution of sensory integration theory 115
Appendix 2 Treatment implementation Plan 116
Appendix 3 Ethics approval letter from Monash University 118
Appendix 4 Ethics approval letter from DEECD 119
Appendix 5 Yooralla permission letter 120
Appendix 6 Consent form 121
Appendix 7 Sensory Profile 122
Appendix 8 Sensory interview/ history 124
Appendix 9 Parent questionnaire 125
Appendix 10 Sample of GAS goals for a participant. 127
Appendix 11 Handout: sensory defensiveness 129
Appendix 12 The Deep Pressure Proprioceptive Technique/ DPPT 132
Appendix 13 Pictures of demonstration page 2. 133
Appendix 13 Comments from parent/carers 134

13
Chapter 1. Introduction to thesis
1.1 Introduction
Sensation is everywhere. The world around us makes sounds, provides textures, and
offers tastes and smells. We use sensory words to describe most physical characteristics of
our homes, workplaces, shops and other settings (Dunn, 2008), for example, a bright, noisy
playground, or a soft and cuddly teddy. According to DeGangi (2000), parents and
professionals have been puzzled over the importance of sensory processing issues and self-
regulatory problems in children. Babies learn to suck and swallow, cry for attention, and
respond to touch and warmth for comfort. The early regulation of arousal and the
physiological state are critical for successful adaptation to the environment (DeGangi,
2000). Homeostasis is important in modulation of the physiological states and is needed for
mastery of sensory functions and for learning self-calming. Infants with problems
associated with regulating sensorimotor systems (e.g., hypersensitivity to stimulation) tend
to develop emotional difficulties in the school-aged years (Fish & Dixon, 1978; Walker &
Emory, 1983).
Sensory issues are often unrecognised and can be associated with parenting issues
or ‘colic’ in babies, therefore do not warrant further monitoring. However, according to
Ayres (2005), sensory stimulation and motor activity during the years of childhood mould
the neurons and interconnections to form sensory and motor processes that will remain
relatively stable for the rest of a person’s life.
Occupational therapists work with children and the need for occupational therapy
services has risen exponentially with the increase in adverse conditions affecting children’s
health including disease, poverty, birth complications and autism (Royeen, 2010).
Occupational therapists are challenged to provide services to a wide range of children and
their families, including children with sensory processing difficulties in an ethical,

14
professional and efficacious manner (Royeen, 2010) and assist children and families to
increase their participation in their everyday activities like play, going out in the
community and self care skills. A variety of frameworks and approaches are used within
occupational therapy and will be mentioned later in the chapter 2, however one of the
approaches that is used is a sensory based approach or a sensory integration frame of
reference (Ayres, 1972). A variety of intervention approaches are used within this
framework and the Wilbargers’ approach is one such approach that is known to be used by
occupational therapists for children presenting with sensory defensiveness or over
responsivity.
1.2 Clinical Application:
The Wilbargers’ approach to treating sensory defensiveness is used extensively
within occupational therapy. According to a survey done in New York in 2001, out of 64
occupational therapists, 78 % used the Wilbarger’s Deep Pressure and Proprioceptive
Technique (DPPT) to treat tactile defensiveness (Sudore, 2001). If the effectiveness and
usefulness of the DPPT as an intervention strategy can be recognised, then it will provide
valuable information to therapists for intervention, goal setting and parent involvement and
empowerment. Therefore, building a body of evidence related to the efficacy of
intervention approaches such as DPPT is important for therapists and clients alike.
1.3 Thesis overview
It is unclear with the current literature review whether the Wilbargers’ DPPT is an
effective intervention due to the small number of studies and small sample sizes. This study
will examine the effectiveness of the DPPT by using a multiple single case study design
and add to the current knowledge base of research within sensory based interventions in
particular the Wilbargers’ DPPT. This thesis has 6 chapters. In chapter 2, a literature
review including a brief overview of occupational therapy is given following information
regarding sensory integration theory, intervention approaches and a summary of research.

15
In chapter 3, the methodology and ethical considerations of the current study follows and
chapter 4 discusses the results of the study. Chapter 5 presents a discussion of the study
findings while chapter 6 includes study limitations, suggestions for future research,
implications for professional practice, and a general conclusion.
1.4 Search Strategy
Comprehensive search strategies were used in the following electronic databases:
MEDLINE (1966 to present), CINAHL (1954 to present), OT Seeker, AMED, OVID and
Google scholar. The search strategies included the following medical subject headings
keywords:
• Sensory defensiveness
• Wilbargers’ Protocol
• Deep pressure and proprioceptive technique
• Sensory processing
• Sensory integration
• Sensory modulation
• Tactile defensiveness
• Occupational therapy and sensory integration
• Models of practice and occupational therapy
• Sensory Profile and Winnie Dunn
• Sensory Integration Quarterly
• Anxiety and sensory defensiveness
• Family centred practice
• Early childhood intervention
• Goal attainment scaling
• Goal setting in occupational therapy

16
In an effort to identify further published and unpublished research–related material, the
following strategies were used:
1. Scanning the reference lists of identified studies and reviews
2. Identifying unpublished research by searching dissertation abstracts and attempting
to contact the key researchers
3. Liaising with authors of the technique being examined and keeping abreast of the
latest published research
4. Hand searching of relevant occupational therapy and other related journals
including:
• American Journal of Occupational Therapy
• Australian Occupational Therapy Journal
• Canadian Journal of Occupational Therapy
• Physical and Occupational Therapy in Paediatrics
• Journal of Autism and Developmental Disorders

17
Chapter 2: Literature Review
2.1 Introduction
This chapter provides a general introduction to sensory integration theory. It
includes an overview of occupational therapy practice and models of practice used. This is
followed by an overview of the terminology used within sensory-based occupational
therapy and a background for sensory modulation leading to sensory defensiveness and the
Wilbarger’s Deep Pressure and Proprioceptive Technique (DPPT). Finally, a brief
summary of the current available research is presented.
2.2 Occupational Therapy Practice
Occupational therapy is a profession primarily concerned with enabling people to
participate in activities of daily living by promoting health and well-being through
occupation (World Federation of Occupational Therapists [WFOT], 2004). Over the years,
even though the essence of occupational therapy has remained the same, the definitions and
practice have evolved. Occupational therapists use a systematic approach based on
evidence and professional reasoning to enable individuals, groups and communities to
develop the means and opportunities to identify, engage in and improve their function in
the occupations of life (Canadian Association of Occupational Therapists [CAOT], 2008).
2.2.1 Scope
Based on the above definitions by WFOT (2004) and CAOT (2008), the main
outcome within occupational therapy is to increase participation, restore occupation and
improve quality of life through optimum independence in everyday occupations that
include self-care, leisure and productivity.
Occupational therapy is practiced in a variety of settings including paediatrics,
psychiatry and mental health, geriatrics, general medicine and surgery, neurology and
rehabilitative medicine. Therapists can work individually or within groups, within

18
integrated health care teams with other professionals, within community settings, as
consultants, and in private practice. From developmental issues to acquired conditions,
occupational therapy has an important place in treatment of children with additional needs.
Occupational therapy fits in with the principles of best practice when working with children
and families, some of the aspects being; family-centred practice; play, as an important
occupation in children; increasing independence and performance to increase participation
and evidence-based practice by integrating research findings into practice and using
research evidence in clinical reasoning (Dunst & Bruder, 2002; Dunn, 2000).
Occupational therapy applies clinical and scientific reasoning to assess, plan and
provide intervention and ethical reasoning to weigh the risks and benefits of intervention
techniques and considers multiple perspectives of the child and family including their
values, interests, priorities and contexts (Radomski & Trombly, 2008). Occupational
therapy respects cultural diversity and this means that successful outcomes depend on
being culture-specific (Kielhofner, 2008). For example, independent feeding may not be a
goal for a family until the age of 6 years from one culture, whereas in a different culture, it
is important to achieve independent feeding by the age of 3 years.
2.2.2 Theoretical framework
The traditional approach to medical care was based on World Health Organization’s
(WHO) old model (1980) that focused on impairments, disabilities and handicaps. The
WHO has since changed the definitions and structures on disabilities and the new
International Classification of Function, Disability and Health (ICF; WHO 2001) puts
forwards a conceptual framework of body function and structure, activity, participation,
and personal and environmental factors (Law & Baum, 2005). Occupational therapy
practice models have also since then evolved and are used in a client-centred approach,
focussing on the client goals and client occupational needs (Law & Baum, 2005). Table 1
illustrates these models of practice.

19
Table 1. Models of occupational therapy practice
Model Description
The Ecology of Human Performance
Model (EHP), (Dunn, Brown & McGuigan, 1994, Dunn, Brown, & Youngstrom, 2003
The EHP is built around four constructs: person, task, context and the performance. This framework describes a three-dimensional model in which the person can only be seen if observed in the context. Within the EHP model, performance cannot be understood outside the environmental context (Dunn et al., 1994).
The Canadian Model of
Occupational Performance (CAOT 1997, 2002).
The Canadian Model of Occupational Performance was first presented in Enabling occupation: an occupational therapy
perspective (CAOT 1997, 2002). This model placed particular emphasis on occupational performance. The Canadian Model of
Occupational Performance and Engagement (CMOP-E), later added engagement to the CMOP. The construct on human engagement captures the broadest perspectives on occupation. The central person is depicted to have four performance components namely cognitive, affective and physical, with spirituality at the core. The person is embedded within the environment to indicate that each person lives within a unique environmental context.
The Person-Environment-Occupation model (PEO) (Law et al., 1996; CAOT, 1997a, 2002).
Six constructs are identified namely person, environment, activity, task, occupations and occupational performance (Law et al., 1996). Occupation is a part of hierarchical structure and outcomes occur when the fit among the person, occupation and environment is maximised.
2.2.3 Paediatrics
Within paediatrics, occupational therapy uses a variety of models of practice and
can be classified into two types namely, occupation–based models and neuromaturation–
based models (Law, Missiuna, Pollock & Stewart, 2005). Occupation–based models are
based primarily on contemporary theoretical approaches such as systems theory and
integrative models of development. They include cognitive approaches, compensatory and
environmental approaches, psychosocial approaches, social skills development, motor
learning and sensory processing approach (Law et al., 2005).

20
Neuromaturation approaches are based on a hierarchical staged development of the
nervous system and are based primarily on developmental theories. They include
neurodevelopmental approach, sensory integration and other developmental approaches
(Law et al., 2005). Over the past 30 years, sensory integration has been a major approach
used by occupational therapists within paediatrics in conjunction with other approaches
(Koomar et al., 2004).
2.3 Overview of sensory integration and sensory processing theory.
Sensory integration and the more recently coined term sensory processing (Dunn,
1997, 2001) are both used by occupational therapists working with children.
‘Sensory’ means different things to different people but can include vision, hearing,
smelling, tasting and touching. It is an area that is expansive and inclusive of all of the
above senses, and more. It includes vestibular, proprioceptive and auditory systems (Ayres,
2005). Table 2 describes the different sensory systems.

21
Table 2. Sensory systems
System Description Individual occupational
performance
Impacts on occupational
performance
Visual system The receptors are in the retina and are sensitive to light waves, sending visual sensory input to the visual processing centres in the brain stem and then to other parts of the cerebellum to be integrated with motor messages going to muscles that move the eyes and neck.
Ability to see and move eyes from one object to another. This helps one to see moving objects, or pages of a book.
Difficulties with eye contact, puzzles, reaction to light, reading, writing, figure-ground and attention
Auditory system The receptors are in the inner ear and are sensitive to sound waves in the air, sending these auditory impulses via the brain stem auditory nuclei along with impulses from the vestibular system and the muscles and the skin to several parts of the cerebral hemispheres. Auditory impulses also travel to the cerebellum and a great deal of integration is required at each level of the brain to make meaning of what one hears.
Ability to hear and develop speech and language. The most intricate and complicated part is the refinement of sounds into meaningful syllables and words.
Difficulties with tolerating noises, understanding language, speech, following complex instructions
The gustatory system or taste
The receptors are in the tongue
ability to taste four different tastes namely sweet, sour, bitter and salty.
Difficulties with oral skills like feeding, picky eaters, over filling mouth
The olfactory system or smell
The receptors are in the nose. Smell is processed directly through projections to the limbic system without travelling through the brain stem. Thus smell activates emotions directly and one can like or dislike what one encounters by the way it smells.
Ability to smell and differentiate smells
Unusual responses to smell, smelling non – foods, unaware of smells
The tactile system or touch The receptors are in the skin layers and it is the largest sensory system playing a vital role in human behaviour, both physical and psychological. There are several types of receptors for receiving touch, pressure, temperature and pain. The nuclei are in the brain stem that process tactile inputs. Many of these impulses never reach those parts of the cerebral cortex that make one aware of sensation, instead are used at the lower levels to adjust the reticular arousal system, to influence
Tactile system is the first to develop in the womb and is very important for overall neural organisation. Tactile inputs make one aware of pain, cold or hot, wet or sticky and vibration.
Difficulties with touch tolerance, tactile defensiveness, dislike for certain textures and grooming activities like hair brushing, unusual responses to touch, over touching, difficulties with tactile discrimination.

22
emotions and to give meaning to sensory information. Processing is required at the cerebral cortex to understand the location of the stimulus on the skin.
The proprioceptive system or position and movement
the receptors are located in the muscles and joints. The term proprioception comes from the Latin word proprius meaning “one’s own”. The sensations from one’s own body occur especially during movement. Most proprioceptive input is processed in areas of the brain that do not require conscious awareness and therefore one rarely notices the sensations of muscles and joints during movement.
Proprioception helps one to move and without adequate proprioception it would be difficult to perform everyday simple tasks like buttoning, opening jars, getting in and out of a chair or from an escalator. One would have to rely on visual information to assist with these skills.
Difficulties with maintaining body positions, early fatigue, poor motor planning, clumsy and low muscle tone for activities, poor gross motor abilities
The vestibular system or gravity, head movement and balance
the receptors are within the membranous labyrinth in the inner ear. There are two types of receptors. The first is a pair of saclike swellings called the utricle and the saccule and lies in the vestibule of the inner ear and responds to the accelerated movement of the head, or to changes in acceleration resulting from an altered position of the head. The second is the three directionally sensitive semicircular ducts within the semicircular canals and they detect angular acceleration of the head in any of these directions. Information from both sets of vestibular receptors is relayed to the vestibular part of the eighth nerve, to the vestibular nuclei in the brain stem and to the cerebellum and the motor nuclei of the extraocular muscles.
This helps to keep the body balanced, to coordinate head and body movements and most remarkably to keep the eyes fixed on a point in space even when the head is moving.
Difficulties with movement, may be excessive movement seekers, cannot sit still, spinning or rocking behaviours, or over sensitive to movement and may cry if moved, anxiety
Visceral Input or input from the internal organs of the body
the receptors are in the internal organs and in major blood vessels. Other sensory systems like vestibular and tactile can affect the autonomic system for example spinning can upset digestion.
Visceral input assists in regulating blood pressure, digestion, breathing and other functions of the autonomic nervous system.
Difficulties with digestion, regulation of bodily functions
Note: (Ayres, 2005; Kandel et al., 1991)

23
2.3.1 Models and terminology in sensory–based theory
Within sensory-based approaches, a number of terms are used by occupational
therapists. Table 3 provides a definition of commonly used terms with some examples. In a
recent issue of American Journal of Occupational Therapy, Schaaf and Davies, (2010) did
a review of evolution of sensory integration theory and terminology and reported that when
appropriate, the problem should be described (i.e., children and adolescents with difficulty
processing and integrating sensory information) rather than naming a disorder (sensory
integrative dysfunction or sensory processing disorder). This decision was made after much
reflection, discussion, and analysis of the literature. Schaaf and Davies, (2010) stated that
at this time no critical mass of research supports the naming of a disorder; thus, it would be
presumptuous and assumptive to suggest it at this time. They recommend describing the
problem rather than naming a disorder until there is more research to guide terminology.
Based on the literature review, and the author’s interpretation, Appendix 1 provides
a flow chart of the evolution of sensory-based occupational therapy approaches.

24
Table 3. Definition of terms commonly used in a sensory–based model of practice
Term Definition Example
Sensory Integration is the organisation of sensations for use. (Ayres, 2005) When a child walks through an obstacle course and at the same time is able to listen and respond to his mother’s voice telling him to come and get a drink, then it can be said that sensory integration is occurring and all systems are working together in an integrated way. In this case the child’s visual and vestibular system are assisting him to climb without losing balance, the tactile and proprioceptive system are giving him information about where his body is and where to place his hands and legs next and his auditory system is assisting in filtering all the sounds from the environment and respond to his mother’s voice. This is called sensory integration.
Sensory modulation is a dynamic CNS process that is subject to the ebb and flow of continual input over multiple channels. Behaviourally, it is reflected in sensory seeking and sensory avoiding (Dunn 1999; McIntosh et al., 1999; Parham & Mailloux, 1996)
Seeking input all the time, cannot sit still or avoiding sensations like messy play or swings
Detection
If the stimulus is seen as novel or important or potentially harmful or dangerous, the brain increases transmission and lowers the threshold thus causing sensitisation or detection. The nervous system identifies this stimulus as one requiring heightened attention and more neurons can be recruited to make the message more powerful and generate an immediate and powerful response.
Children develop and use detection to remain active within their surroundings while engaged in play and other learning e.g. responding to the school bell after lunch break and move towards the classrooms.
Habituation When a familiar stimulus is presented to the brain it recognises this and decreases transmission. This raises the threshold over a period of time and thus causes habituation.
Children need habituation otherwise they would be continually distracted by each new stimulus, including how their clothes feel, background noise in a shopping centre, or eating the same fresh fruit at lunch time.

25
Term Definition Example
Sensory discrimination refers to be able to take in information, interpret what’s going on in the environment and develop skills by making adaptive responses (Koomar, 2004).
Koomar (2004) compared this to the effect of having novocaine in your body after a dental visit; when the effect is wearing off one knows where the mouth is but it feels vague and on attempt to eat one may feel insecure about where the mouth is even though one knows where the mouth is, and may have trouble biting or chewing and may drool. Children with poor discrimination may bump into things have a vague sense of their bodies and may bump into people due to a poor understanding of where their body ends (e.g., dyspraxia)
Sensory processing is a broad term that encompasses all that goes on with a sensory signal, including its reception in the periphery, our central detection of this information, its transformations between electrical and chemical signals and its interaction with other activity within the nervous system (Lane et al., 2000).
When we see a red light, our visual system registers this and the brain processes the meaning of the signal, leading to our whole body getting ready to respond by stopping.
Sensory registration is a term that has been used clinically to describe the behaviour of noticing sensory stimuli in the environment (Lane, 2000).
Registering a sound e.g. ambulance or touch e.g. spider crawling on our back, noticing it. Is related to our state of arousal.
Sensory detection is defined as the first step that occurs centrally. Incoming sensory information is recorded at multiple levels within the CNS so that it can affect ongoing neural activity by influencing the overall level of activity in the CNS (Lane, 2002).
Detecting the signal is the first step and takes a fraction of a second, however is an important step for registration
Sensory defensiveness is a constellation of symptoms related to aversive or defensive reactions to non – noxious stimuli across one or more sensory systems. It is an overreaction of our normal protective responses. There may be patterns of avoidance, sensory seeking, fear, anxiety or aggression (Wilbarger & Wilbarger 2002, 2007)
A child may be sensitive to light touch and have difficulty standing close to other children in a line at school or not tolerate hair washing.

26
2.3.1a Sensory integration and sensory processing
Dr. Ayres was a visionary occupational therapist and was responsible for pioneering
the development of sensory integration theory, research, assessment, intervention and
therapeutic equipment since the 1960s (Roley et al. , 2001). She first used the words
sensory integration (SI) in 1963 and then refined her theory as a result of many empirical
studies proposing in 1989 that the neurobehavioural process of processing and integrating
sensory inputs strongly affects development (Henry, 2007). Ayres’ theory was based on
the hierarchic model of the central nervous system (CNS). Hierarchic models view the
nervous system in terms of vertically arranged levels with the spinal cord at the bottom and
the cerebral hemispheres at the top with the brain stem in between. These levels are
interdependent yet reflect a trend of ascending control and specialisation. The cerebral
cortex assumes a directive role over the lower levels through inhibition and is highly
specialised, analysing precise details of sensory information (Parham & Mailloux, 2005).
The lower levels have less specialised functions yet potentially more pervasive in influence
and filter and refine sensory information before relaying it to the cerebral cortex. Thus the
cortical centres are interdependent on the lower levels for receiving well – organised
sensory information to plan action (Parham & Mailloux, 2005).
One of the tenets of Ayres theory is that because of the dependence of higher
structures on lower structures, increased efficiency at the levels of the brain stem and
thalamus enhance higher-order functioning (Parham & Mailloux, 2005). This hierarchic
approach to the CNS led Ayres to emphasise the more primitive vestibular and
somatosensory systems in young children. She reasoned that primitive functions such as
postural control, balance and tactile perception provide a sensorimotor foundation for
higher order functions like academic learning, behavioural self regulation and complex
motor skills (Parham & Mailloux, 2005). Ayres hypothesised that by providing enriched

27
sensory opportunities processed at the level of the brain stem, and by stimulating the
child’s motivation via the limbic system with the ‘just–right’ sensory and motor challenges,
the child would make higher level adaptive responses and be more willing to tackle
challenges in daily life (Parham & Mailloux, 2005).
Ayres also noted that each level of the CNS can function as a self-contained sensory
integration system and the sensory integrative process involves the brain working as a
whole, not simply a series of hierarchically controlled messages. She was ahead of her time
in suggesting the heterarchic ability of the CNS (Parham & Mailloux, 2005).
2.3.1b Sensory modulation and responsivity
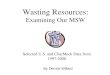
Dunn (1997) generated a new conceptual model that proposed that there is an
interaction between neurological thresholds and behavioural responses. This model (see
Figure1) presents the neurological thresholds and behavioural responses as continua that
interact with each other. This interaction provides a method for explaining how sensory
information is processed and provides guidance for intervention planning. This model is
based on the assumption of a heterarchic CNS rather than a hierarchic and is most
contemporary to the current theories of CNS functioning.
According to Dunn (2000) the neuroscience concepts that sensory integration
theory is built upon are: that sensory input is necessary for the brain to function; sensory
information gets combined and reorganised as it travels to the cortex; and the CNS has
many interdependent circuits and different areas of the brain share information and rely on
each other for function; and the nervous system is plastic at the cellular, system and
organism level and learning in the CNS is represented by changes in the cell structure and
organisation, changes in system connections and changes in efficiency of operations. The
neurological threshold refers to the amount of stimuli required for a neuron or neuron
system to respond (Dunn, 2000). Behavioural response refers to the way people act in
consideration of their thresholds. The entire nervous system operates based on excitation

28
and inhibition. When neurons are more likely to respond or activated excitation occurs, and
when responses are blocked, inhibition occurs. The balance between these two operations
determines responses; this process of continual balance of the neurological continuum is
termed as modulation (Dunn, 2000). When modulation is intact, the child generates an
appropriate adaptive response to the situation.
Sensory modulation is the process by which the brain adjusts and organises itself
through habituation or sensitisation (Dunn, 2002) (see Table 3 and Figure 1). These are the
extreme ends of the neurological threshold continuum. In either of these cases, the
thresholds for action are extremely important for responses to occur in a way that is
appropriate; and this is critical to maintain one’s ability to engage in daily occupations. If
the thresholds are raised excessively then it could lead to low arousal states and under
responsivity, however if the thresholds are lowered markedly, then it could lead to a
heightened state of arousal and over responsivity.
This is the basis for sensory modulation (Dunn, 2002). Individuals with high
thresholds acting in accordance with those thresholds may appear passive or non-
responsive. Dunn classified these individuals as having low-registration. Individuals with
high thresholds may also seek out additional sensory input to counteract that threshold;
Dunn classified these individuals as sensory seeking. Similarly, individuals who have a low
threshold and act in accordance with their threshold would be considered sensory sensitive.
Yet individuals who act to position themselves away from potentially noxious stimuli
would be classified as sensory avoiders (Reynolds & Lane, 2008). Filtering of sensations
and attending to those relevant; maintaining attention to task, all require modulation. When
modulation is adequate, attention maybe continually diverted to ongoing changes in the
sensory environment.

29
Behavioural Response Continuum Neurological
Threshold
Continuum Acting in
ACCORDANCE
With Threshold
Acting to
COUNTERACT
threshold
HIGH
(habituation)
Poor
Registration Sensation
Seeking
LOW
(sensitization)
Sensitivity
to Stimuli
Sensation
Avoiding
Figure 1: Relationship between behavioural responses and neurological thresholds (Dunn,
1999)
2.3.2 Disorders of sensory systems
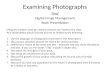
After years of exploration and research, a new classification for the diagnosis of
sensory problems (see Figure 2) has been introduced as Sensory Processing Disorder
(SPD) with the long term goal being inclusion of SPD into the upcoming revision of the
Diagnostic and Statistical Manual of Mental Disorders IV –TR (DSM IV) of the American
Psychiatric Association due out in 2012 (Henry et al., 2007). “Sensory processing disorder
exists when sensory signals don’t get organised into appropriate responses and a child’s
daily routines and activities are disrupted as a result” (Miller, 2006, p. 5, cited in Henry et
al., 2007).

30
Figure 2. Classification of SPD patterns and subtypes, (Miller, 2000, p. 13, cited in Henry et
al., 2007). Sensory Modulation Disorder and Overresponsivity are highlighted to provide an
understanding of where sensory defensiveness sits within the classification
Sensory Modulation Disorder (SMD):
Sensory modulation refers to the ability to filter, screen incoming information so
that we can respond appropriately to the situation (Koomar et al., 2004). Cermak (1988)
and Royeen (1989) hypothesised that there is a continuum of sensory responsivity with
hyporesponsiveness at one end and hyperresponsiveness at the other. An optimal level of
SPD patterns and subtypes
Sensory Modulation
Disorder
Sensory-Based Motor
Disorder
Sensory
Perception/Discrimin
ation Disorder
Sensory Over-
Responsivity
Sensory Under-responsivity
Sensory seeking
/Craving Dyspraxia Postural
Disorder
Visual (eye)
Auditory (ear)
Tactile (touch)
Vestibular (Movement)
Proprioception (Muscle)
Taste/Smell (Mouth/Nose)

31
arousal and orientation lies in the centre and most activity falls here for most individuals.
Sensory Modulation Disorder is a problem in the capacity to regulate and organise the
degree, intensity and nature of response to sensory input in a graded manner (Lane et al.,
2000). According to Dunn (2000), it is characterised by behaviours of extreme
responsivity. These behaviours interfere with daily function. There may be patterns of
avoidance, sensory seeking, fear, anxiety or even aggression. Over-responsivity manifests
by noticing every stimulus in the environment (easily distractible or irritable). These
children manifest with sensory defensiveness. Under responsivity manifests by lack of
noticing stimuli and appearing “dull” or “slow”.
In an article by Reynolds and Lane (2008), by considering under- or over-
responsiveness as separate aspects of the construct of Sensory Modulation Dysfunction
(SMD), researchers may be better able to understand the sensory related behavioural
patterns as a whole (Liss et al., 2006), and the essential links between neurological
mechanisms and observable behaviour. Physiological differences between children with
over-responsivity and under-responsivity have been identified, providing preliminary
evidence of behavioural–physiological correlations in SMD (McIntosh et al., 1999). Over-
responsivity has been identified as the more common form of SMD (approximately 80%)
based on referrals to research programs (Schaaf et al., 2003). Over-responsivity is also
referred to as sensory defensiveness, in which individuals maybe overly sensitive to one or
more incoming sensations (Wilbarger & Wilbarger, 2007).
Sensory defensiveness is a constellation of symptoms related to aversive or
defensive reactions to non-noxious stimuli across one or more sensory systems (Wilbarger
& Wilbarger, 1991). It is an overreaction of our normal protective responses. Ayres (1964)
initially described this phenomenon in the literature in the 1960s. Sensory defensiveness is
considered the behavioural manifestation of over-responsivity.

32
According to Wilbarger and Wilbarger (2007), a number of cases treated for sensory
defensiveness over more than forty years have provided valuable information about this
condition and its treatment. Patricia Wilbarger (1984) was particularly interested in the use
of intensive, natural sensory based activity and the latency effects of activity. After 1975, a
long term follow-up of infants treated in an intensive care nursery began and after
successful outcomes were documented, the scope and significance of sensory defensiveness
was obvious (Wilbarger & Wilbarger, 2007).
Wilbarger and Wilbarger (1991) promoted the concept of sensory defensiveness as
consistent with normal defensive responses. They propose that sensory defensiveness is on
a continuum of approach and avoidance behaviours and that sensory defensiveness is one
of a subset of sensory modulation disruptions. Several researchers have been working to
understand further the nature of sensory defensiveness. This collection of work is
beginning to verify long held clinical opinions that disruptions in sensory modulation are
identifiable phenomenon that affect the daily lives of individuals (Kinnealey et al., 1998).
Kinnealey et al., (1998) have been studying the phenomenology of sensory
defensiveness in adults. They have also explored treatment of sensory defensiveness using
a sensory diet model, in the tradition of the Wilbarger approach. Baranek et al., (1997) and
Baranek, (1999), conducted a series of studies to understand the role of sensory
defensiveness in individuals with developmental disabilities and autism. Between 3-30 %
of their sample of individuals with developmental disabilities had sensory defensiveness.
These studies are adding to the body of understanding that sensory defensiveness may be a
unique disruption of sensory modulation. As such, it appears to be a legitimate
phenomenon and not necessarily a by-product of another disorder (Wilbarger &
Stackhouse, 2006).

33
Sensory based motor disorders and sensory discrimination disorders
The vestibular and proprioceptive systems are usually responsible for processing
information from the movement senses and body position in space. Individuals may lack
sensory–based abilities (praxis) for motor activities, may have inadequate balance and may
get frustrated because they feel stuck. They may not be able to figure out how to move their
bodies for gross motor skills like jumping, for fine motor skills like colouring-in or oral
motor skills like talking or eating (Henry, 2007).
Sensory discrimination refers to being able to take in information, interpret what is
going on the environment and develop skills, by making appropriate adaptive responses
(Ayres, 2005). Most of us can put our hands in our pocket and tell the difference between a
dollar coin and a fifty cent piece without looking at it. An example of sensory
discrimination disorder may be seen when a child shows reduced awareness of his/her body
from the sense of touch, or tactile discrimination or from their muscles and joints, the
proprioception system and maybe unable to tell differences in objects by touching or
appear clumsy (Henry, 2007).
A common form of sensory based motor disorders is dyspraxia, a disorder of motor
planning and smooth movement (Henry, 2007). Another common form is disorders in
vestibular bilateral integration, characterised by clumsiness, incoordination and poor
postural control (Dunn, 2000), for example, during handwriting and ball skills.
2.3.3 Intervention approaches:
Sensory integration intervention approach was derived and grew from the work of
Jean Ayres (1969, 1972a, 1972b). Ayres indicated that the theory of sensory integration is
constantly evolving and is informed and modified as new research is generated (Ayres,
1972a). Participation in self care, leisure and academic social activities is the final outcome
of sensory integration process and interventions (Schaaf et al. 2010). This is also the final

34
outcome within occupational therapy philosophy. Over the years, best practice demands
that occupational therapy profession not only act in accordance with the knowledge,
principles and philosophies of their own profession, but also with a larger set of beliefs in
mind (Dunn, 2000). Family-centred care has become more central to practice with children
and families and therapists have recognised that the principles of sensory integration can be
used within the daily routines as a critical part of the intervention (Dunn, 1999). Some
sensory-based intervention approaches are described in Table 4.

35
Table 4: Some intervention approaches within sensory based occupational therapy
Intervention Approach Description
Classical Sensory Integration treatment (Ayres) This refers to the therapy that Jean Ayres started in the early seventies specifically to remediate sensory integrative dysfunction. Classical sensory integrative therapy provides and controls sensory input through the sensory systems in such a way that the child forms adaptive responses that integrate these sensations. It is always applied on an individual basis to address the child’s interest and response in the activity and altered as the child adapts from moment to moment (Bundy, 2002). The emphasis is on the inner drive and active participation of the child. Another key characteristic is the setting in which it takes place. Specialised therapeutic equipment and a sensory-rich environment is an important aspect of classical sensory integration treatment (Clark et al., 1989; Koomar & Bundy, 2002). The therapeutic activities are neither predetermined nor are they simply free play. It is an intensive long-term intervention. A typical schedule involves two sessions per week lasting for 45 minutes to an hour and the course lasts for two years.
The Wilbargers’ Deep Pressure and Proprioceptive Technique (DPPT)
It is a popular type of intervention to treat clients with sensory modulation dysfunction of which the most consistent manifestation is over responsiveness or sensory defensiveness to sensory stimuli. The Wilbargers’ protocol to treating sensory defensiveness involves a comprehensive, intensive and individualised programme (Wilbarger & Wilbarger 1991). This technique is described in detail in next section.
The Alert Program for Self – Regulation This is a step by step method by which adults (preferably a team) determine which sensory strategies support children’s optimal performance and identify sensory hypersensitivities that hinder their performance (Shellenberger & Williams, 1996). This program is designed to improve awareness of self-regulation through charts, worksheets and activities. Adults guide children to recognise their alertness levels and help them learn strategies to change their levels of alertness or arousal (Shellenberger & Williams, 1996). This program was initially designed for children aged 8 – 12 years, but later adapted for preschoolers through to high school age and for adults.

36
Intervention Approach Description
Auditory Integration Training (AIT) .
Auditory integration training (AIT) is based on the concept that electronically modulated/ filtered music provided through earphones maybe helpful in remediating hypersensitivities and overall auditory processing ability that is thought to be problematic in children with sensory processing disorders (Baranek, 2002). The exact neurological mechanisms underlying AIT are not known, however various hypotheses have been proposed, like improved functioning of the reticular activating system, reorganisation of the cerebellar vestibular system, modification of brain serotonin levels. AIT is said to massage the middle ear and enhance auditory perception
Berard method of auditory training A modulating and filtering device, audiokinetron or audio tone enhancer accepts music input from CDs and transforms sounds by randomly modulating high and low frequencies and filtering out selected frequencies in accordance with the child’s performance on an audiogram. Treatment is usually provided individually in a small sound-quiet room for 30 minutes, 2 times per day for 10 to 20 days by a trained professional and fees can range from $1000 to $3000 for 2 week treatment, (Baranek, 2002).
The Tomatis method The Tomatis method is similar, but integrates a psychodynamic with a psychophysiological perspective (Baranek, 2002). In the passive phase the individual listens to filtered sounds of the maternal voice, as well as prepared music and in the active phase, is introduced to language and audio vocal exercises that provide feedback of his/ her own voice through headphones to reinforce more normal auditory perception and overall quality of life. The treatment is performed in ways similar to the Berard method, but often with repeated blocks of intervention with overall durations, sometimes over a few years (Baranek, 2002).
Therapeutic Listening Therapeutic Listening provides individualised programs in the form of electronically altered music using the organised sound patterns inherent in music (Frick, 2009). It is based on ideas from Tomatis, Berard and Steinbach and uses a variety of modification techniques (Frick, 2009). Equipment requirements are headphones with a frequency range of 20 Hz – 23000 Hz with impedance of 150 ohms. The cost of the headphones range between $250 - $300 and the CDs cost $ 70 approximately. The child needs to listen to the music twice a day for 30 minutes (Frick, 2009). The child engages in activities during the programme however not cognitively demanding tasks.

37
2.3.3.a The Wilbargers’ ‘Deep Pressure and Proprioceptive Technique’ (DPPT)
The Wilbargers’ protocol or “brushing” is the commonly used term for
describing Wilbargers’ Deep Pressure and Proprioceptive Technique. It is also referred
to as the Therapressure protocol. It is considered to be a complementary and alternative
treatment used within a broader context of occupational therapy intervention with a
sensory integration framework (Bundy & Murray, 2002). It is a popular type of
intervention to treat clients with sensory modulation dysfunction of which the most
consistent manifestation is over responsiveness to sensory stimuli. Brushing has been
used as a preparatory method of intervention by occupational therapists for decades.
The use of the surgical brush to systematically provide deep pressure was promoted in
the Wilbarger protocol (Wilbarger & Wilbarger, 1991).
The Wilbargers’ protocol to treating sensory defensiveness involves a
comprehensive, intensive and individualised programme (Wilbarger & Wilbarger
1991). Wilbarger and Wilbarger, (2007) stated that social emotional disorders related to
sensory defensiveness result in patterns of learned behaviours, habits and interaction
styles that are protective and defensive in nature. The behaviours are related to stress
and anxiety and appear as controlling or obsessive compulsive in nature. They are a
result of sensory defensiveness or coping strategies. Kinnealey et al. (1995) also
identified avoidance as a coping mechanism for adults with sensory defensiveness.
Wilbarger and Wilbarger, (2007) recognised critical issues in sensory defensiveness for
example that sensory defensiveness is a unique and identifiable phenomenon; it is
present from birth and can interfere with typical development and disrupts all areas of
function; it can produce a number of secondary effects and coping styles that are also
present in many other conditions like social/ emotional behaviours, subtle postural
problems, discriminatory issues, stress and anxiety.

38
Sensory defensiveness can affect arousal and lead to poor habituation,
unpredictable behaviour, increased responsivity and changing behavioural states
(Wilbarger & Wilbarger, 2007). The cause of sensory defensiveness is unknown.
Sensory defensiveness presents in a wide range of symptoms and severity from mild to
moderate to severe. In mild sensory defensiveness the following symptoms can be
observed like an overreaction to a few sensory experiences, near normal behaviour
(e.g., ‘picky’, ‘oversensitive’, ‘touchy’ mild irritations to labels, smells, crowds, noisy
gatherings). According to Wilbarger and Wilbarger, (2007) these symptoms may go
undetected, as individuals can adapt to demands of life; however, intervention brings
reduced stress, and a feeling of freedom.
In moderate sensory defensiveness, the symptoms can range within two or more
areas of life e.g. social relations, eccentricities in self – care and defensive against
sensory events, controlling behaviours, compulsive tendencies and disorganisation with
change. Intervention brings new choices to an individual’s life style (Wilbarger &
Wilbarger, 2007). In severe sensory defensiveness symptoms can disrupt every aspect
of an individual’s life, due to rigid and restricted behaviours and frequent existence of
other problems and diagnoses. Intervention provides options for an individual and
allows other therapy to be more effective (Wilbarger & Wilbarger, 2007). In summary,
sensory defensiveness is a sensory modulation disorder resulting in a negative or
avoidant response to non-noxious stimuli, not just being distracted by it. Sensory
defensiveness can be tactile, oral, motor (postural), auditory, vestibular, visual,
olfactory and proprioceptive.
A detailed assessment includes a clinical interview, clinical observations and
any questionnaires or checklists may be used as an adjunct (Wilbarger & Wilbarger,
2007, 2009). The family reports on events that occur across two days; one typical day
may include a school day, and one non- typical may include a weekend. Goals of the

39
assessment are mainly to identify symptoms of sensory defensiveness, inform the
family about the extent and impact of sensory defensiveness and gain information for
treatment planning (Wilbarger & Wilbarger, 2007).
The Wilbarger approach to the treatment of sensory defensiveness is comprised
of three components. These include education and increasing awareness of sensory
defensiveness and its symptoms, individualised sensory diet and an individualised
professionally guided treatment program (Wilbarger & Wilbarger, 2007).
Education implies that when implementing the Wilbarger approach, the therapist
provides information and awareness; to clients, families, educators and other
caregivers; regarding what sensory defensiveness is, what effect it may have on the
client and those close to the client, what behaviours may be present when sensory
defensiveness occurs and how this relates to the client’s challenges (Wilbarger &
Wilbarger, 2007).
A sensory diet is a form of home program intervention plan that incorporates organising
sensory input, or utilises already existing sensory input, into everyday life in order to
assist the person to maintain a regulated behavioural state (Wilbarger & Wilbarger,
2006; Williams & Shellenberger, 1994; Cool, 1990). Sensory diet strategies may be
implemented at regular intervals throughout the day.
Professionally guided treatment (DPPT) is planned based on the findings of clinical
interviews, sensory history checklists such as the Sensory Profile (Dunn, 1999),
observations and standardized assessment tools where appropriate. Collaborative
treatment plans, developed with clients and families, should be individualised to the
specific needs of the client and should be monitored and adjusted where appropriate
Treatment involves application of deep pressure and proprioception every two
hours for a period of six to eight weeks and a strict adherence to the protocol. It
includes both direct treatment and the design and monitoring of precise, intensive,

40
individual treatment programs. Oral defensiveness is treated with an oral tactile
technique involving touch contact to portions of the mouth at specific intervals during
the day (Wilbarger & Wilbarger, 2007).
Sensory diets are an important aspect of the treatment plan and are always
prescribed along with the direct intervention. Patricia Wilbarger (1984) developed the
concept of ‘sensory diets’ to integrate and expand the theories to the use of sensory
experiences and to enhance occupational performance in any individual and contribute
to the remediation of developmental and sensory processing disruption. DPPT should
not be an isolated treatment method but rather one part of a treatment plan focusing on
all activities of daily living (Wilbarger & Wilbarger, 2002; Wilbarger & Wilbarger,
2006).
A treatment plan is created for every individual based on the findings of the assessment
(Wilbarger & Wilbarger, 2007). (See Appendix 2).
2.4 Evidence based practice and research in sensory-based occupational
therapy intervention approaches:
“Evidence-based medicine is the integration of best research evidence with
clinical expertise and patient values” (Sackett et al., 2000, p. 656). It links theory to
clinical practice, stimulates clinically relevant research, accountability, helps to ensure
cost effectiveness and efficacy to funding bodies and payers, improves client outcomes
and client care, improves clinician’s knowledge and communicates a profession’s
research base.
Ayres researched sensory integration based on brain research and neuroscience,
in the 1960s and 1970s. Since then many researchers are studying the efficacy of
sensory- based approaches especially with children with learning difficulties. All of the
studies of the efficacy of intervention that followed in the early years after Ayres
published her theory have been criticised for various design – related issues.

41
Ottenbacher, (1982) was able to identify eight studies published between 1972 and
1981 that were included in a meta-analysis due to having sufficient rigor. He found
sufficient evidence to suggest that intervention based on sensory integration principles
was effective. However as these studies were not comparative, the analysis drew
criticism. Vargas and Camilli, (1999) also used meta-analysis to examine studies in the
same period and supported Ottenbacher’s results. From the 1980s up to 1993 many
studies were conducted to validate intervention based on sensory integrative principles,
however these were less successful. Some of these studies had procedural faults;
however most were conducted in a rigorous manner.
Many of the researchers wanted to find that this intervention was effective
(Vargas & Camilli, 1999). Children receiving this intervention did make gains,
however the gains were so few and unpredictable that Wilson et al. (1992) concluded
after reviewing seven studies between 1982 and 1992 that there were no statistical
evidence to support the claim that sensory integration treatment improved academic
performance in children with learning disabilities more than a placebo. Polatajko et al.
(1992) concluded that with respect to sensory or motor performance, the results of the
review of studies are not consistent, but did suggest that statistically, overall sensory
integration therapy may be similar to perceptual motor training.
In a recent systematic review, ( May-Benson & Koomar, 2010), twenty-seven
studies were systematically reviewed to identify, evaluate, and synthesize the research
literature on the effectiveness of sensory integration (SI) intervention on the ability of
children with difficulty processing and integrating sensory information to engage in
desired occupations and to apply these findings to occupational therapy practice.
Results suggested that the SI approach may result in positive outcomes in sensorimotor

42
skills and motor planning; socialization, attention, and behavioural regulation; reading-
related skills; participation in active play; and achievement of individualized goals
(May-Benson & Koomar, 2010).
Current research with populations comprised of individuals with Sensory
Modulation Disorder (SMD) has been questioned since SMD is not yet recognised as
an ICD-10 or DSM-IV diagnosis. However, the Diagnostic Classification of Mental
Health, Developmental Disorders of Infancy and Early Childhood: Revised Edition
(DC:0-3R) (Zero to Three 2005) and the Diagnostic Manual for Infancy and Early
Childhood (DMIC) and Interdisciplinary Council for Developmental and Learning
disorders [ICDL 2005] have included Regulatory Sensory Processing Disorders as a
diagnostic category, with overresponsive sensory modulation identified as a specific
type of SMD associated with the fearful/ cautious or anxious behaviour pattern and the
negative/defiant or stubborn behaviour pattern.
Validity for the existence of SMD has been enhanced by measurement of
physiological responses associated with sensory stimulation. McIntosh and colleagues
(1999) studied electro dermal responses (EDR) patterns in 19 children clinically
diagnosed with SMD and without conditions such as cerebral palsy, foetal alcohol
syndrome, or autism. The children with SMD showed larger and more frequent EDR
than typical controls and slower habituation to repeat stimuli, suggesting an
overresponsive pattern in approximately 79% of the experimental sample.
2.4.1 Summary of research available currently on the effectiveness of the
Wilbarger’s DPPT: Reviewing the evidence
Articles were searched using comprehensive search strategies in the following
electronic databases: MEDLINE (1966 to present), CINAHL (1954 to present), OT
Seeker, AMED, OVID and Google scholar. After completing the search for and
retrieval of articles, a review of each article’s quality, rigor and impact on outcomes is

43
required (Koh, 2008). According to the Oxford Centre for Evidence-Based Medicine
(2009), levels of evidence are presented in Table 5 below. Table 6 summarises the
studies completed that investigate the use of the Wilbargers’ DPPT to date.
Table 5: Oxford Centre for Evidence-based medicine – Evidence for therapy/ Prevention/ Etiology/ Harm:
1a: Systematic reviews (with homogeneity ) of randomized controlled trials
1a Systematic review of randomized trials displaying worrisome heterogeneity
1b Individual randomized controlled trials (with narrow confidence interval)
1b Individual randomized controlled trials (with a wide confidence interval)
1c All or none randomized controlled trials
2a Systematic reviews (with homogeneity) of cohort studies
2a Systematic reviews of cohort studies displaying worrisome heterogeneity
2b Individual cohort study or low quality randomized controlled trials (<80% follow-up)
2b
Individual cohort study or low quality randomized controlled trials (<80% follow-up /
wide confidence interval)
2c 'Outcomes' Research; ecological studies
3a Systematic review (with homogeneity) of case-control studies
3a Systematic review of case-control studies with worrisome heterogeneity
3b Individual case-control study
4 Case-series (and poor quality cohort and case-control studies)
5
Expert opinion without explicit critical appraisal, or based on physiology, bench
research or 'first principles'

44
Study Design Sample Tools/
instruments
Results Level
Foss, A., Swinth, Y., McGruder, J., & Tomlin, G. (2003). Sensory modulation dysfunction and the Wilbarger Protocol: An Evidence Review. OT
Practice, 8(12), CE1– CE8.
This is an article that reviews relevant literature, provides an overview of some issues surrounding the application of the Wilbargers’ technique and provides strategies for applying this material to clinical practice. Two rigorous studies addressing sensory modulation dysfunction (SMD) using electrodermal responses are discussed where psychophysiological evidence supports the validity of SMD in children. 4 studies are reviewed to study the efficacy of the Wilbarger protocol.
N/A Literature reviews According to the authors, emerging evidence supports the use of a brushing intervention, such as the Wilbarger Protocol, specifically for persons who present with over responsiveness. Because of the limited empirical evidence supporting or refuting the effectiveness of the Wilbarger Protocol, it should be applied with caution. The protocol should always be used within the context of a comprehensive occupational therapy intervention, and data should be collected to ensure that the brushing results in improved occupational performance.
Narrative review
Strengths:
• pertinent information and definitions provided
• clear understanding of what is existing and implications provided
• extensive reviews done Weakness:
• More terminology added to an already highly worded sensory integration area e.g. SMD (Sensory Modulation Dysfunction), Over-responsiveness, DSI (Sensory Integration Dysfunction)
Table 6: Summary of research papers available on the Wilbargers’ DPPT. (Adapted from T. May-Benson, 2008. Contributions from abstracts and from Foss, et al (2003).

45
Segal, R., & Beyer, C. (2006). Integration and application of a home treatment program: A study of parents and occupational therapists. American Journal of
Occupational Therapy,
60, 500–510.
Qualitative exploratory study 6 parents (of children between 4 – 7 yrs), and 8 occupational therapists (with 4 – 12 years of experience, learnt about Wilbarger’s approach in academic educational programmes)
One to two 45 – 90 minute interviews, transcribed verbatim, with open ended questions and data analysis by constant comparison method
Children’s positive responses, parental observation of the immediate effects of treatment were critical to maintaining adherence. The frequency of treatment was identified as an inconvenience for parents and was not flexible with daily routines. All occupational therapists agreed that it was challenging and would not fit all families and that the adherence was poor.
Level 4
Strengths:
• Qualitative project with quotes made it an interesting read
• Involved parents to make it family centred
• Tried to eliminate bias through participant selection Weaknesses:
• Quotations from interviews do not coincide with the results as the quotes appear positive for the use of the protocol, however results indicate poor adherence. Maybe another interview was required at the end of stopping the protocol or needed to be cited.
• Most of the participants did not follow through with the protocol every two hours
• Small sample size

46
Stagnitti, K., Raison, P., & Ryan, P. (1999). Sensory defensiveness syndrome: A paediatric perspective and case study. Australian Occupational
Therapy Journal 46, 175-187
Single case study – case report
One boy aged 5 years with a query of Aspergers syndrome (Specialist children’s services, Victoria)
Millers Assessment for Preschoolers (MAP); sensory checklist; observations at home and kindergarten, parent interview
Results from repeating the sensory checklist and MAP indicated favourable results and reduction in sensory defensiveness, to the use of the Wilbarger’s brushing protocol, in association with behavioural strategies. It also recommended that the severity levels of sensory defensiveness syndrome be categorised to assist with diagnosis and prognosis.
Level 3b - 4
Strengths:
• Classification of sensory defensiveness syndrome suggested for diagnosis and prognosis
• Detailed observations done for precise case report
• Functional skills were assessed
Weaknesses:
• Single case sample
• No statistical analysis could be used
• No standardised sensory assessment or checklist used
• Introduced behavioural intervention along with the sensory intervention and this could lead to a bias in results Kimball, J., Lynch, K., Stewart, K., Williams, N., Thomas, M., & Atwood, K. (2007). Using Salivary Cortisol to measure the effects of a Wilbarger Protocol-based procedure on sympathetic arousal: A pilot study; American
Journal of Occupational
Therapy, 61(4), 406-413.
Single-subject design across participants
4 boys with sensory defensiveness ages 3 – 5 years, 1 out of 4 had pervasive developmental disorder and 1 had autism, University of New England
Saliva sample collected pre and post (after 15 min of quiet time) administration of the Wilbarger protocol and analysed for Cortisol using ELISA(enzyme-linked immunosorbent assay)
Changes in the salivary cortisol levels in all 4 boys indicated that the procedure used, modulated the cortisol levels and there was an association between sympathetic nervous system response and the Wilbarger protocol-based procedure.
Level 3a

47
Strengths:
• Rigorous method, pre and post intervention used to reduce bias
• 4 cases used Weaknesses:
• Post intervention results were only taken at one time post brushing, rather than at the end of 6 – 8 weeks as suggested for using the Wilbarger’s protocol, therefore cannot contribute to results of using the intervention technique for sensory defensiveness
Zbytniewski, R. (2002). The effects of sensory integration's Wilbarger technique on engaging behaviours. Bay Shore, NY: Touro College. (unpublished master's project)
Quasi-experimental design Subjects serving as own case control
Seven participants: 2 girls, 5 boys with sensory integration dysfunction
Participants were observed in a preschool classroom for five minutes pre-brushing treatment and five minutes post-brushing treatment.
The data from this research project was unable to support the Wilbarger Protocol as it was not significant; boys may show a greater response to the Wilbargers’ technique than girls.
Level 3b - 4
Strengths:
• 7 participants used
• Quasi experimental design used Weaknesses:
• Results recorded five minutes post brushing rather than at the end of 6 – 8 weeks as suggested for using the Wilbarger’s protocol, therefore cannot contribute to results of using the intervention technique for sensory defensiveness
• Assessment tools not specified

48
Moore, K & Henry, A. (2002) Treatment of Adult Psychiatric Patients using the Wilbarger Protocol. Occupational Therapy
in Mental Health, 18(1), 43-63.
Pilot study; Qualitative study .
3 women with histories of self-injurious behaviours
Data collected through interview, the 50-item Sensory Defensiveness Screening for Adults and patient journals. Wilbarger brushing and joint compression protocol lasted approximately 1 month. Symptoms and patterns of role engagement and self-injury were compared before and nine months after treatment.
At follow-up all participants were re-engaged in valued roles with no incidents of self-injury. Respective items endorsed by participants on the Sensory Defensiveness Screening for Adults dropped from 58% to 54%, 43% to 18%, and 72% to 36%. This treatment approach appeared to have some positive influence on sensory defensive symptoms.
Level 4
Strengths:
• Followed the Wilbarger protocol as required
• Used standardised assessment screening tool
• Pre – post study was done with detail Weaknesses:
• Small sample size
• Sensory defensiveness screening is not a standardised tool for measuring sensory defensiveness Reisman, J. & Gross, A. (1992). Psychophysiological measurement of treatment effects in an adult with sensory defensiveness. Canadian Journal of
Occupational Therapy,
59, 248-257.
Single subject case study 1 Adult with sensory defensiveness
Autonomic responsiveness to touch and visual and auditory stimulation were assessed by psycho physiological measurements. The treatment was self administered firm tactile input which was expected to have a calming effect.
Changes in respiration rate, hand temperature and amplitude of skin conductance reflected reduced autonomic arousal. The study supports the relationship to autonomic arousal, the potential for effective therapy and the use of psychophysiological measures of sensory defensiveness.
Level 3b-4

49
Strengths:
Strengths: Rigorous techniques used for instrumentation; Weaknesses: Complex instrumentation precludes replication by clinical therapists. Lack of regularity between treatment times and sessions does not allow for replication of treatment. Intervention technique is not clearly defined. Small sample size Not indicative of the effect of the Wilbargers’ protocol Snyder-Stonebraker, D. (2001). The effects of a Wilbarger-based brushing protocol: A single subject study. Unpublished master’s thesis. University of Puget Sound, Tacoma, WA.
Single subject case study Boy with sensory defensiveness
Miller Assessment Tool for Preschoolers; Sensory Profile
The effectiveness of the sensory summation technique was confirmed. Effective behavioural strategies are explained and differential diagnosis between sensory defensiveness syndrome and other disorders such as autism spectrum disorders is emphasized. Participant demonstrated functional improvements in group participation at school, decreases in incidence of tantrums, and social participation at home and in the community
Level 3b-4
Strengths:
• Used standardised tools for measurement.
• Functional outcomes were assessed and reassessed
• The study was conducive to participation and the ecological model of occupational therapy Weaknesses:
• Small sample size
• intervention technique not defined clearly
• Outcomes measured not clear regarding change in sensory defensiveness

50
Sudore, K. (2001). Tactile defensiveness and the Wilbarger brushing protocol in system management. Unpublished master’s thesis. D’Youville College, Buffalo, New York.
Qualitative study: Survey conducted in American Occupational
Therapy Association (AOTA), Sensory Integration Special
Interest Section (SISIS)
64 occupational therapists randomly chosen from a list of the members of the (AOTA) and who were registered for SISIS the in the year 2000
78% of respondents use the Wilbarger Protocol in the intervention of tactile defensiveness.
Level 5
Strengths:
• Supports the use of the protocol by occupational therapists
• Participants selected randomly Weaknesses:
• Low rigor of study due to survey only
• Does not lead to the efficacy of the intervention technique, but its frequency of use. Stratton, J. & Gailfus, D. (1998). A new approach to substance abuse treatment in adolescents and adults with ADHD. Journal of Substance
Abuse, 15(2), 89-94.
Qualitative study: Anecdotal article
Adolescent aged 16 years
Sensory checklist, quick neurological screening test, VMI, TVPS, Client interviews and observations
Article discussed positive outcomes from sensory integration based treatment and the Wilbarger Protocol when it was administered to an adolescent with attention deficit disorder in substance abuse treatment.
Level 4 - 5
Strengths:
• Descriptive case presentation
• Standardised tools used Weaknesses:
• Literature review not sound
• No clear intervention strategy defined
• Small sample size

51
Kinnealey, M. (1998). Princess or tyrant: A case report of a child with sensory defensiveness Occupational Therapy
International, 5(4), 293–303.
Case report Child aged 3 ½ years with no diagnosis
Sensory history, behavioural style questionnaire (McDevitt & Carrie, 1974), and observations
Article presents a case report of a child with sensory defensiveness and outcomes following a sensory integration treatment programme, including the Wilbarger’s brushing technique.
Level 5
Strengths:
• Detailed case report provided
• The DPPT intervention technique was used Weaknesses:
• Non standardised assessments for measuring sensory issues,
• Low rigor study,
• No clear intervention strategy defined

52
Mora L., & Chapparo, C., (2008). The impact of the sensory protocol on the functional behavioural responses of children with intellectual disability, sensory defensiveness and behaviour support needs. Australian
Society of Study of
intellectual disability
(ASSID) Conference,
Melbourne, VIC.
Randomised controlled study experimental (group 1, sensory intervention) and control group (behavioural intervention); random allocation
16 children 11 male; 5 female; 4 – 10 years; mean 5.8 with developmental delay/ intellectual disability
Developmental behaviour checklist (Enfield and Tonge,1995); Goal attainment scale; Parent sensory protocol diary;
-Statistically significant change on total GAS t scores in both groups; -Statistically significant change in overall GAS scores was found between the sensory and behaviour groups indicating more positive outcomes for the sensory group. - no difference between intervention groups on functional GAS scores indicating sensory and behavioural interventions were equally effective in changing functional behaviour - a statistically significant difference in behavioural GAS scores between sensory and behavioural interventions in favour of sensory intervention.
Level 2b
Strengths:
• Randomised control trial
• Good sample size
• Standardised tools used for measurement
• Rigorous statistical analysis used Weakness:
• Expensive to replicate study
• Requires large work force

Most of the studies listed above have small sample sizes ranging from single case
studies to a maximum of 16 children. No studies have used randomised control trials
except one (Mora & Chapparo, 2008), and a variety of non-standardised assessment tools
have been used in most studies. Most studies are difficult to replicate due to the
methodology used or cost involved and in most of the studies the Wilbargers’ DPPT is
not carried out as specified, to measure its true efficacy. Overall most research in this
field has been at the level 4 or 5 except for two studies that were at Levels 1b and 3b. All
studies available, however, present positive findings on the effectiveness of the Wilbarger
Protocol.
In a paper by Baranek (2002) the efficacy of sensory and motor interventions for
children with autism was reported and even though it did not mention the Wilbargers’
DPPT directly, a sensory summation approach was reviewed that involved sensory diets
in the home or classroom and a schedule of frequent and systematically applying somato-
sensory stimulation with a brush and joint compressions. The paper concluded that
findings from the studies reported were often mixed. Several studies in the area of SI,
sensory stimulation, auditory integration training, prism lenses, and physical exercise
yielded some positive, albeit modest outcomes; however, methodological constraints
(e.g., use of small and convenience samples, weak/uncontrolled designs, observer bias,
etc.) limit conclusive statements and generalisibility of much of this work (Baranek,
2002).
While this level of evidence is not conclusive or rigorous enough to support the
efficacy of this technique, the preliminary emerging evidence does provide a starting
point. Additional well-controlled studies are needed.

54
2.5 Summary
This chapter presented an overview of sensory integration, disorders associated
with sensory-based intervention and how sensory defensiveness fits into the classification
of sensory processing disorders under sensory modulation disorders. It outlined
intervention approaches used within a sensory-based approach and presented a review of
research studies in the area. It provided detail about Wilbargers’ DPPT, its use and the
need for further research in this area. The next chapter describes methodology used for
this study.

55
Chapter 3: Methodology
3.1 Introduction
According to the literature review in Chapter 2, it is unclear whether sensory
integration intervention, specifically the Wilbargers’ Deep Pressure and Proprioceptive
Technique (DPPT) has enough supporting evidence to be used within occupational
therapy practice contexts. The present study will attempt to add to the current knowledge
base. This chapter will present the methodology for the proposed study.
3.2 Research aims
The aims of the present study were:
1) To evaluate the effectiveness of the Wilbarger’s Deep Pressure and
Proprioceptive Technique (DPPT) in children presenting with signs of
sensory defensiveness.
2) To investigate parent / carer perspectives on the effectiveness of DPPT
3.3 Design:
A prospective multiple single case design was used with convenient sampling.
Single subject research methods are useful for answering questions regarding the
effectiveness of specific interventions for specific individuals by providing experimental
control and contributing to clear and precise clinical documentation (Deitz, 2006). Some
of the reasons why this design was selected to undertake the study were that low
incidence diagnoses or impairment can be researched (e.g., sensory defensiveness),
withholding of treatment from children is not required like in control groups, it is more
realistic for practice settings due to small sample sizes and the findings can be used to
inform large settings (Deitz, 2006).
In a multiple baseline design, one behaviour is treated across participants, (in this study,
that is sensory defensiveness) and the results are used for drawing conclusions. A

56
multiple case study enables the researcher to explore differences within and between
cases. The goal is to replicate findings across cases (Yin, 2003). The advantage is that the
internal validity is better as it is done at different times for each individual setting or
behaviour and it is useful when behaviours are not reversible. The weaknesses in this
design approach are that it requires more data collection, more time and the behaviours
stay for longer at baseline (Deitz, 2006).
Case study methodology allows the researcher to explore individuals or
organisations, simple through complex interventions, relationships, communities, or
programs (Yin, 2003). This approach is valuable for health science research to develop
theory, evaluate programs, and develop interventions because of its flexibility and rigor
(Baxter & Jack, 2008).
3.4 Participants:
Data collection took place in the Melbourne metropolitan area at a community
based organisation called Yooralla. Yooralla is a not for profit organisation and
participants were selected from Yooralla’s Early Childhood Intervention Services (ECIS)
sites. Yooralla’s ECIS caters for children from birth to 6 years of age and are developed
on a strengths based, family–centred approach. Eligibility into the service requires a child
to present with two or more areas of developmental delay, or have a recognised disability.
Five children were recruited for this study from across Yooralla’s nine ECIS between
August 2009 and March 2010. Boys and girls were eligible to participate in this study,
subject to informed parental/carer consent.
3.4.1 Inclusion and Exclusion criteria
The inclusion criteria were:
1. Parents/carers having a working knowledge of English for completion of sensory
questionnaires (Sensory Profile, sensory histories and interviews).

57
2. Children recruited either attending or eligible for ECIS
3. Age group between 3 – 8 years
4. Children to present with signs of sensory defensiveness which include difficulties
with tolerating certain everyday activities like hair washing, loud noises, and certain
movements.
5. Providing informed parental consent to take part in the study. The consent forms were
signed by parent/ carer on behalf of the child before participating in the study.
The exclusion criteria for study participants were:
1. Children who have received this treatment previously were excluded.
2. Children with skin conditions like eczema, burns, fragile bone conditions
wherein joint compressions are contraindicated (e.g. in osteogenesis imperfecta),
with physical neurological conditions like cerebral palsy or with Down syndrome
were excluded.
3. Parents/ carers who are not able to meet the requirements of the protocol (not
able to follow frequency of treatment for time period of six weeks) at the outset
were excluded; however they were given all the information material and an
option of returning to the therapists to avail the treatment programme in the
future.
3.5 Ethical Considerations
Ethics committee approval was granted from Monash University in August 2009
and by Victorian Department of Education and Early Childhood Development (DEECD)
in July 2009. Permission from Yooralla to collaborate with participants was granted prior
to the commencement of the study. (Ethics approval documents are attached in
Appendices 3, 4 and 5).

58
Parental/carer consent was sought in writing prior to taking part in the study. To
enable informed consent, parents/ carers were given information packs explaining the
purpose of the study, extent of involvement including length of time for completing
Sensory Profile and interviews and time frame for the Wilbargers’ DPPT. (See Appendix
6 for copy of consent forms). Privacy policies, consent forms, and explanatory sheets
were handed over to the parents/carers. Signed consent forms were collected prior to
commencement of the study. The researcher did the pre and post assessments and follow
up phone calls and the treating therapist followed up the treatment. Parents also had
access to the researcher via telephone during the six week period of administering the
treatment protocol to provide support and avoid cessation of treatment. The researcher
took written permission from the parent/carer to stay in touch over the phone every week
to ascertain adherence and provide support.
Parents had the freedom to withdraw from the study at any time during the study
without any reason and this would not affect their general programmes in any way. The
parents/carers were assured in writing that information collected for the study would be
held in confidence and access to data would be highly secured. To avoid feelings of
coercion parents/carers were recruited on a voluntary basis and the researcher did not
request participation from the parents verbally. Letters to request participation were
distributed to Yooralla’s nine ECIS centres and the occupational therapists working at the
specific site disseminated these letters to the families to assist the researcher in
distribution and to avoid power relationships with the researcher therapist.
All the data was stored in locked filing units and in secure password protected
computer programmes in accordance with privacy policies. All records will be
maintained in archives for a period of 5 years. All staff is covered through public liability
insurance within Yooralla. Yooralla follows quality assurance programmes and grievance

59
procedures are available to all families if they are dissatisfied with any aspect of the
programme. Debriefing is available to families through their family service coordinators
and programme coordinators and a counsellor at certain sites, in case of any unforseen
incidents.
It was clarified in writing to all families participating in the research, that they
would continue in their respective programmes and everyday activities before, during and
after the research and their daily routines/ participation in any programmes will be
maintained and not altered by participating in this study. All participating parents/carers
will receive a follow up phone call from the researcher after three months and six months
post cessation of the treatment to maintain connections and provide opportunities for
further discussion relating to the treatment protocol.
3.6 Instrumentation:
Three tools were used to collect data, namely the Sensory Profile (Dunn, 1999),
sensory interviews and a parent questionnaire at the end of the study. Clinical
observations including one hour at the child’s home or at the child’s group setting (e.g.,
kindergarten, childcare, Yooralla centre) were recorded at the start of the study.
Based on the results from the parent interviews, Sensory Profile and parental concerns,
sensory defensive issues were potentially identified. Three to five goals were drawn to be
measured pre and post administration of the intervention. Goal Attainment Scale (GAS)
was used as a standardised and valid tool to measure the goals pre, during, and post
treatment.
3.6.1 The Sensory Profile (Dunn, 1999):
The Sensory Profile provides a standard method for professionals to measure a
child’s sensory processing abilities and to profile the effect of sensory processing on
functional performance in the daily life of a child (Dunn, 1999). The Sensory Profile is a

60
judgement – based caregiver questionnaire. It can be used for children between 3 – 10
years of age (Dunn, 1999). It consists of 125 items grouped into three main sections
namely sensory processing, modulation, and behavioural and emotional responses (Dunn,
1999). (Refer Appendix 7).
The caregiver who has daily contact with the child completes the questionnaire by
reporting the frequency with which these behaviours occur namely always, frequently,
occasionally, seldom or never. Once scored, certain patterns of performance on the
Sensory Profile are indicative of difficulties with sensory processing and performance
(Dunn, 1999). A Sensory Profile manual (Dunn, 1999) provides a framework for
interpreting the caregiver’s responses.
The reliability of the Sensory Profile was estimated using Cronbach’s alpha
(Dunn, 1999). The internal consistency indicates the extent to which the items in each
section measure a single construct. The values for the alpha coefficient for the various
sections ranged from .47 to .91. The Standard Error of Measurement (SEM) is an index
of the degree to which obtained scores differ from true scores. The Sensory Profile
provides a standard error of measurement value for each section and factor raw score
between 0.92 to 2.89 (Dunn, 1999).
Validity refers to evidence that establishes the extent to which a test measures
what it was designed to measure (Dunn, 1999). Content validity was established during
the development of the Sensory Profile through a national study using 155 occupational
therapists (Dunn, 1999) and results indicated that 80% of therapists agreed on the
category placement on 63% of the items (78 out of 125). To determine construct validity,
various scores on the Sensory Profile were compared with different functional tasks as
measured by the School Function Assessment (Coster et al., 1998) and the data supported

61
the hypothesised correlations, demonstrating both convergent and discriminant validity
(Dunn, 1999).
A contextually relevant evaluation of the impact of sensory experiences on
children's ability to function within their environment (i.e., home, school, community) is
an important part of an occupational therapy assessment (Ermer & Dunn, 1998). The
Sensory Profile has been used extensively in clinical practice and research in the United
States and in Australia. Recent studies have incorporated the use of the Sensory Profile
(Dunn & Westman, 1995) in the diagnostic evaluation of sensory behaviours in children
with and without disabilities (Ermer & Dunn, 1998) as a potential method for including
sensory data in the diagnostic process. An Australian study was conducted (Brown et al.,
2008) that studied the discriminant validity of the Sensory Profile in Australian Children
with Autism Spectrum Disorder comparing 26 children with Autism and 26 typically
developing children and found that the children with ASD had significantly lower
sensory processing scores on all fourteen categories, eight out of nine factors, and all four
quadrants of the Sensory Profile. The results also provide evidence of discriminant
validity of Sensory Profile scores between children with ASD and children with typical
development. In addition, the study findings indicate that the Sensory Profile can be used
with confidence in cross-cultural contexts, such as Australia.
3.6.2 Sensory history / interview
This interview technique is designed to go beneath the obvious and detect the
unique individual differences that are important in evaluating and treating sensory
defensiveness (Wilbarger & Wilbarger, 2007). This format for this interview is not
standardised. A sensory history format was presented to participants who attended the
training course over two days in March 2007, by Wilbarger and Wilbarger. This format is
available in the course manual (Wilbarger & Wilbarger, 2007).

62
A short schedule with typical events that take place each day is recorded to
provide a structure for focussing on the key events focussing on the beginning and end of
the day. Examples of questions would include, “What time does your child wake up? Is
he/she cheerful and alert or is he/she slow to wake up? What does he wear to bed? What
did it take to get her to sleep the night before?” (Wilbarger & Wilbarger, 2007). This line
of questioning needs to be completed for one typical workday and one non-structured or
weekend day. The parent needs to also be asked to describe incidents when the child had
major difficulties and other times when they are particularly organised.
Every sensory area is covered through the interview namely tactile, pain, oral,
temperature, audition, visual, vestibular, proprioception, vibration, olfaction, taste and
other non-specific qualities of sensation like intensity, novelty, unexpected and the
cumulative effect of sensations. All recording is done in terms of functions like self care,
play/leisure, school/work and considering all environments like family routines,
interactions, childcare, kindergarten, etc (Wilbarger & Wilbarger, 2007).
The objectives of the interview are to detect the symptoms of sensory
defensiveness, question about each sensory system, record aversive, avoiding and seeking
behaviours and to get more specific information about the events, environments and
interactions that promotes the escalation of symptoms, to visualise behaviour within a
time frame, and to increase the parent/ carer’s awareness and depth of understanding of
sensory defensiveness (Wilbarger & Wilbarger, 2007). It provides descriptive and
qualitative data of symptoms and behaviours that can be used along with the standardised
Sensory Profile. (Refer Appendix 8)
3.6.3 Parent Questionnaire
At the end of eight weeks of intervention parent/carers were given a questionnaire
consisting of six items using a five-point Likert-type rating scale to measure parent

63
perspectives of participating in the DPPT intervention. This questionnaire was designed
with a view to gaining insights and opinions from parents about their experiences during
the intervention period and to find out if the DPPT intervention fitted in with features of
Family Centred Practice (FCP) which is considered a best practice approach in ECIS
settings. The questions addressed the following points from the parents’ perspective:
information provided, inconvenience caused, impact on daily routine, empowerment,
importance and effectiveness of the DPPT intervention. (Refer appendix 9)
3.6.4 Goal Attainment Scaling
Goals were drawn with the parent/carer, post data gathering and translated into
Goal Attainment Scaling (GAS) (see Table 7). GAS is an individualised, criterion
referenced measure of change, using goals (King et al., 1999). GAS was first described
by Kiresuk and Sherman (1968) as a general method to evaluate the outcome of mental
health treatment.
Because of its ability to assess change brought about by any form of intervention,
GAS has many applications in education, rehabilitation and medicine (Kirusek et al.,
1994). GAS not only can serve to organise and focus treatment, it can by openly
communicating the goals, marshal the help of others for example members of the family,
in reaching these goals (Kirusek et al., 1994). This facilitates parent involvement and
adheres to principles of family–centred practice.
GAS methodology is congruent with the client-centered occupational therapy
philosophy because GAS provides a means to identify intervention outcomes that are
specifically relevant to individuals and their families. Through the use of interviews
during goal-setting, during and post treatment sessions, the GAS process captures
functional and meaningful aspects of a person’s progress that are challenging to assess
using available standardised measures (Mailloux et al., 2007). Recent studies have found

64
that, although parents value observable sensory and motor changes traditionally reflected
in standardised tests, they place greater value on those aspects of functioning that are not
readily measured by traditional outcome measures (Cohn, 2001 ; Cohn, et al., 2000).
Because GAS captures individualised progress that is meaningful to the family, it is an
appealing methodology for measuring change during and after occupational therapy-
sensory integration (OT-SI), both in clinical and research applications (Mailloux et al.,
2007).
The advantages of using the GAS is that it is a responsive outcome measure that
accurately detects clinically meaningful change, detects difference, reflects clients’ and
clinicians’ priorities, facilitates client problem-solving, increases inter-disciplinary
agreement and goal-setting and improves clarity of goals (Forbes, 1998). The GAS is not
bound to any treatment approach and goals are individualised for every client
(Ottenbacher & Cusick, 1993).
Table 7. GAS goals (Kirusek et al., 1994)
Translating goals to GAS goals
• Goals should be observable, repeatable and measurable criteria for success (Palisano et al., 1992).
• Goals should be specified for performance and have a time frame for achievement (Novak, 2008).
• A number of individually tailored intervention goals or objectives should be specified in relation to a set of graded scale points, ranging from the least to the most favourable outcomes considered likely.
• Each outcome/goal should be transformed into an approximate random variable, thus allowing the overall attainment of the specific goal to be treated as standard scores. (Dziegielewski & Powers, 2000).
The disadvantages of GAS are that some clinicians view it as evaluating their
ability to predict change, setting goals that are too easy to attain and not comparing an
absolute level of adjustment or disability in relation to individuals, because it is criterion-

65
referenced and not norm-referenced (Forbes, 1998; Ottenbacher & Cusick, 1993).
Appendix 10 provides an example of GAS goals used in this study (names have been
changed for identity purposes)
3.7 Procedures and data collection
All nine ECIS centres within Yooralla were provided with information and
explanatory notes regarding the study. Therapists trained in the Wilbargers’ DPPT were
identified within the nine centres to carry forward the treatment aspect of the study if
needed. Recruitment of children was done with assistance from the occupational
therapists working directly at the service, who identified children exhibiting sensory
defensive issues based on their clinical expertise, scores from the Sensory Profile
(children with majority of the sensory processing behaviours falling under the ‘definite
difference’ category) and a history of sensory defensiveness based on information
obtained from the sensory history interviews and observations.
A single-subject design was used for this study involving five children. Based on
scores from the Sensory Profile scores, children with the majority of the behaviours
falling under ‘definite difference’ sensory processing rating categories and a history of
sensory defensiveness (elicited from the sensory interviews and observations completed
with parents) were recruited for the study.
Over a period of six months the potential participants were identified and
assessments were carried out by the direct therapist to ascertain whether the inclusion
criteria were met. The parent/carers of the child were then informed about the study and
their informed consent was sought and once received, they were recruited for the study.
Once recruited, a list of the participant’s routine across two days was recorded (e.g., one
typical day, a weekday and one atypical day, on a weekend), a Sensory Profile was done
and a sensory interview was done by the investigator.

66
Treatment implementation plans (Wilbarger & Wilbarger, 2007) including
sensory diets were planned in accordance with the daily routines of the children and their
families as far as possible to fit into their daily routines and within the principles of
inclusion, using naturalistic environments and family–centred practice by the investigator
along with the direct therapist. Natural environments are the home, community, and early
childhood settings where children learn and develop everyday abilities and skills (Dunst
& Bruder, 2002).
Each parent/carer received a therapressure brush, handout on sensory
defensiveness, written instructions, pictures and demonstrations on how to use the
Wilbargers’ DPPT (Wilbarger & Wilbarger, 2007) and an individually prepared
implementation plan (refer to Appendices 11, 12 & 13.). DPPT was demonstrated on the
child and on the parent/carer to ascertain the correct application of pressure by the
investigator. The parent/carer repeated the procedure on their child and on the
investigator. Sensory diet activities were explained and demonstrated if required. A daily
record form was given to keep records and to report any comments during the
intervention if possible. If other service providers were involved, then a visit to their
centre was organised by the investigator and the same procedure was demonstrated to
them for follow up.
Each child participated in a six week regime involving the Wilbargers’ Deep
Pressure and Proprioceptive Technique (DPPT). The DPPT was completed with the
children by their parents/carers every two hours along with sensory diet activities
concurrently at least three times per day (Wilbarger & Wilbarger, 2007). Participants
were reviewed weekly using GAS, (Kiresuk & Shermann, 1968) based on goals drawn
earlier by the investigator via a phone call. As well, the parents/carers were responsible
for follow-up of the intervention program at home and reported to the direct therapist

67
involved every two weeks. The investigator did the follow-up and recording of
observations and the therapist had opportunities to provide any feedback via the phone or
e mail.
Data was collected at the start of the study, and at the end of six weeks, the DPPT
was terminated and data was recorded again. Every week a follow-up phone call or visit
was carried out by the investigator and the goals were reviewed using the GAS tool. The
Sensory Profile was administered again at the end of eight weeks by the investigator. The
DPPT record was maintained optionally by the parent/carer and change was recorded on
an informal documentation form provided (Wilbarger & Wilbarger, 2007). The
assessments pre and post, DPPT intervention demonstration, follow–up, recording of data
and data analysis was done by the investigator for uniformity and to avoid bias.
3.8 Data Analysis:
The Statistical Package of Social Sciences Version 17 (SPSS; Pallant, 2005) was
used for data entry, storage, retrieval and generation of descriptive statistics. SPSS is a
data management system designed for statistical analysis and production of graphs and
tables.
Descriptive statistics were derived using the SPSS and paired samples t-tests were
used to analyse pre- and post-intervention data for GAS scores and Sensory Profile
scores.
3.8.1 Paired-samples t-test
Paired-samples t-tests are used when data is collected from one group of
participants on two different occasions. Pre-test/post-test designs are an example where
this technique is appropriate (Pallant, 2005). If the probability value is less than .05, then
it is concluded that there is a significant difference between the scores. The effect size
(eta squared) value determines that the scores were unlikely to occur by chance. To

68
interpret the eta squared values the guidelines were used: .01=small effect, .06 =
moderate effect, and 0.14= large effect (Pallant, 2005).
3.8.2 Goal Attainment Scaling
Goals were reviewed using the Goal Attainment Scale (GAS) tool, pre, during and
post intervention and were recorded. The GAS uses five possible outcomes (refer to Table
8).
Table 8: A sample of the GAS
Level of expected
outcome
Goal 1
Decision making
Goal 2
Self esteem
Goal 3
Isolation
Review date
Much more than expected (+2)
Makes plans, follows through, modifies if needed, and reaches goal
Expresses realistic positive feelings about self
Actively participates in group or social activities
More than expected (+1)
Makes plans, follows through without assistance unless plan needs changing
Expresses more positive than negative feelings about self
Attends activities, sometimes initiates contact with others
Most likely outcome (0)
Makes plans and follows through with assistance/reminders
Expresses equally both positive and negative feelings about self
Leaves house and attends community centre. Responds if approached
Less than expected outcome (-1)
Makes plans but does not take any action to follow through
Expresses more negative than positive feelings about self
Leaves house occasionally, no social contact
Much less than expected (-2)
Can consider alternatives but doesn't decide on a plan
Expresses only negative feelings about self
Spends most of time in house except for formal appointments
Source: www.socsci.flinders.edu.au/fippm/consult/gasuse.html
The expected level is 0 with 2 possible levels of less/more favourable and it can
determine progress despite the goal not being reached. The GAS computes change for
multiple goals and the composite score is a T-score (Mean=50, SD=10). It quantifies
change over time and across individuals. The weighting enables the composite score to
reflect emphasis for each goal (Palisano et al., 1992).

69
3.8.3 Sensory Profile
At the end of eight weeks the Sensory Profile (Dunn, 1999) was repeated for
comparison. Sensory Profile raw scores were summed into four quadrant scores. The four
quadrants are registration, seeking, sensitivity and avoiding. Table 9 provides an
explanation of the four Sensory Profile quadrants as defined by Dunn (2000). Pre- and
post–intervention scores were compared using the quadrant raw scores and paired t- test
analyses.
Table 9: Quadrant definitions, Sensory Profile, (Dunn, 2000)
Quadrant definitions
Registration The degree to which a child misses sensory input. A child with a ‘much more than others’ score in this pattern, misses sensory input at a higher rate than others.
Seeking The degree to which a child obtains sensory input. A child with a ‘much more than others’ score in this pattern, seeks sensory input at a higher rate than others.
Sensitivity The degree to which a child detects sensory input. A child with a ‘much more than others’ score in this pattern, notices sensory input at a higher rate than others.
Avoiding
The degree to which a child is bothered by sensory input. A child with a ‘much more than others’ score in this pattern, moves away from sensory input at a higher rate than others.
The Sensory Profile scores were plotted for week one and week eight and the GAS
scores were plotted weekly for weeks 0 – 6 during the DPPT intervention period. Scores
were graphed and descriptive statistics (e.g., mean and standard deviation) were
calculated.
3.9 Summary
Chapter 3 outlined the methodology used to collect the data for this study. In
chapter 4 the findings will be presented.

70
Chapter 4: Results
4.1 Introduction.
This chapter will describe the results obtained from descriptive statistics, and pre-
and post-intervention comparisons of the Sensory Profile, Goal Attainment Scaling
(GAS) goals and descriptive statistics from the parent questionnaires.
4.2 Participants demographics
Participants were aged between 3–4 years of age, with a mean of 3.4 years (SD=
0.3). All participants were male and 4/5 had a given diagnosis of Autism Spectrum
Disorder (ASD). The mother was the main carer for the follow-up phone calls (100%). In
3/5 (60%) of the cases, the mother followed through with the Deep Pressure and
Proprioceptive Technique (DPPT) with her child, in 1 (20%) instance the DPPT was
carried through by both the child’s mother and father while in the last case, the DPPT
was completed by child’s mother and another person (childcare staff member). Three
children were from Yooralla’s Endeavour Hills site, one was from Narre Warren and one
from Pakenham. All three of these sites are located within the Melbourne metropolitan
region.
Four out of 5 (80%) of the children’s parents followed through on conducting the
DPPT as required. For one child (ID= 5), the intervention was modified after two weeks
and the parent reported that she had to reduce the frequency of the ‘brushing’ part of the
DPPT intervention. The family was able to follow up all sensory diet activities; however
the child refused the DPPT intervention with the brush every two hours. However the
mother did not want to drop out of the study as she had some days when she was able to
follow up better than others and she reported that she enjoyed completing the DPPT with
her child. Therefore, the child was not excluded from the study.

71
4.3 Results from analysis
The results from the data analysis are presented in this section.
4.3.1 Descriptive statistics:
4.3.1.1 Sensory Profile- descriptive statistics: The mean quadrant scores are
reported in Tables 10 and 11. Figure 3 compares the raw quadrant scores and Figure 4
compares the section raw scores for all five participants from Time 1 (T1) to Time 2 (T2)
and Table 12 presents the section raw scores from the Sensory Profile, Time1 versus
Time 2 for all 5 participants and highlights typical performance and definite difference.
Table 10. Descriptive Statistics – Sensory Profile Time 1
Quadrant Minimum Maximum Mean Std. Deviation
registration 3.27 4.27 3.87 .38
seeking 2.42 4.04 3.15 .65
sensitivity 2.00 3.40 2.92 .56
avoiding 2.59 3.17 2.98 .25
Table 11. Descriptive Statistics – Sensory Profile Time 2
Quadrant Minimum Maximum Mean Std. Deviation
registration 3.60 4.40 4.05 .32
Seeking 3.42 4.31 3.92 .33
Sensitivity 2.95 4.15 3.76 .48
Avoiding 3.17 4.24 3.90 .43

72
Figure 3. Sensory Profile, Quadrant raw scores, Time 1 versus Time 2
(Reg= registration, seek= seeking, sens = sensitivity, avoid = avoiding); Typical scores for registration =between 64-72, seeking = between 103-123, sensitivity = 81-94 and avoiding = between 113 – 133, Sensory Profile, (Dunn 1999).
Quadrant raw scores T1,T2
0
20
40
60
80
100
120
140
participants
raw scores
Reg T1 Reg T2 SeekT1 seek T2 sensT1 sens T2 avoidT1 avoidT2
Reg T1 57 64 62 46 61
Reg T2 66 57 64 52 63
SeekT1 63 68 85 105 81
seek T2 103 100 106 108 89
sensT1 68 55 63 65 39
sens T2 79 81 79 74 57
avoidT1 90 84 91 92 75
avoidT2 117 121 123 112 93
1 2 3 4 5

73
Section Raw Scores Sensory Profile T1,T2
0
10
20
30
40
50
60
70
80
90
1 2 3 4 5
aud1
aud2
vis1
vis2
ves1
ves2
touch1
touch2
multi1
multi2
oral1
oral2
tone1
tone2
movt1
movt2
activ1
activ2
modemo1
modemo2
modvis1
modvis2
emosoc1
emosoc2
behav1
behav2
thresh1
thres2
Figure 4. Sensory Profile, Section raw scores, Time 1 versus Time 2
KEY: (aud=auditory processing, vis=visual processing, ves=vestibular processing, touch= touch processing, multi= Multisensory processing, oral= oral sensory processing, tone= sensory processing related to endurance/tone, movt= modulation related to body position and movement, activ=modulation of movement affecting activity level, modemo= modulation of sensory input affecting emotional responses, modvis= modulation of visual input affecting emotional responses and activity level, emosoc= emotional/social responses, behave= behavioural outcomes of sensory processing, thresh= items indicating thresholds for response) Sensory Profile, (Dunn,1999)

Table 12: Section raw scores, Sensory Profile, Time1 versus Time 2. (Typical scores provided in last row for comparison); * indicates typical scores
of participants, red highlight indicates definite difference, yellow highlight indicates typical performance; all other scores are probable difference.
ID Aud1 aud2 vis1 vis2 ves1 ves2 touch1 touch2 multi1 multi2 oral1 oral2
1 20 29 41* 38* 42 49* 52 78* 18 29* 26 46*
2 27 30* 29 38* 37 50* 46 74* 24 23 30 47*
3 30* 35* 32* 42 46* 52* 67 79* 22 27* 22 39
4 20 31* 36* 38* 45 49* 62 73* 17 25 35 47*
5 16 16 28 27 36 37 51 71 22 27* 34 34
Typical 30-38 32-41 48-55 73-88 27-33 45-59
ID tone1 tone2 movt1 movt2 activ1 activ2 modemo1 modemo2 modvis1 modvis2
1 44* 41* 32 40 17 26* 10 16* 11 15*
2 41* 37* 35 40 11 30* 18* 17* 14 14
3 38 42* 38 46* 23* 20 17* 17* 12 18*
4 25 28 41 48* 22 29* 9 15 13 15*
5 43* 45* 31 32 23* 23* 4 13 14 18*
Typical 39-45 41-49 23-40 16-20 15-19

75
ID emosoc1 emosoc2 behav1 behav2 thresh1 thres2
1 52 64* 12 17 7 14*
2 56 56 21 20 7 11
3 47 75* 21 30 9 11
4 63* 51 16 14 5 13*
5 49 60* 18 23* 8 10
Typical 63-79 22-26 12-15
(Note that aud 1 = auditory processing time 1 ; aud 2 = auditory processing time 2; vis 1 = visual processing time 1, vis 2 = visual processing time 2 and so on. Refer figure 4 for key

4.3.1.2. GAS - descriptive statistics:
Refer Table 13, Table 14 and Table 15 for descriptive statistics and graphs in Figures 5,
6, and 7 for graphs in this section.
Participant ID 1
-20
-10
0
10
20
30
40
50
60
70
80
90
w k 0 Wk 1 Wk 2 Wk 3 Wk 4 Wk 5/6
time in weeks
sco
res
sum of scale scores average scale score t - score
Participant ID 2
-20
-10
0
10
20
30
40
50
60
70
80
90
Wk 0 Wk 1 Wk 2 Wk 3 Wk 4 Wk 5 w k 6
Time in weeks
score
s
sum of scale scores average scale score t - score

77
Participant ID 3
-20
-10
0
10
20
30
40
50
60
70
80
90
Wk 0 Wk 1 Wk 2 Wk 3 Wk 4 Wk 5 w k 6
Time in weeks
sco
res
sum of scale scores average scale score t - score
Participant ID 4
-20
-10
0
10
20
30
40
50
60
70
80
Wk 0 Wk 1 Wk 2 Wk 3 Wk 4 Wk 5 w k 6
Time in weeks
sc
ore
s
sum of scale scores average scale score t - score

78
Figure 5: GAS - Sum of scale scores, average scale scores and t-scores from Time 1
– Time 7 (Week 0 – Week 6) for all 5 participants (N=5; ID=1 to ID=5)
Table 13: Sum of scale scores, GAS, Time 1 to Time 7, (N=5)
Time Minimum Maximum Mean Std. Deviation
Week 0 -12.00 -10.00 -10.40 .89
Week 1 -9.00 -1.00 -4.80 3.49
Week 2 -6.00 4.00 .00 4.18
Week 3 -5.00 8.00 3.40 5.03
Week 4 -5.00 10.00 4.60 5.81
Week 5 -5.00 10.00 6.20 6.30
Week 6 -5.00 10.00 6.60 6.50
Participant ID 5
-20
-10
0
10
20
30
40
Wk 0 Wk 1 Wk 2 Wk 3 Wk 4 Wk 5 wk 6
Time in weeks
scores
sum of scale scores average scale score t - score

79
gaswk6gaswk5gaswk4gaswk3gaswk2gaswk1gaswk0
Mean
10
0
-10
-20
Figure 6. Sum Scale Scores GAS, Time1 to Time7
Table 14: Average scale scores, GAS, from Time 1 to Time 7, (N=5)
Time Minimum Maximum Mean Std. Deviation
Week 0 -2.00 -1.67 -1.80 .18
wk1 -1.50 -.17 -.82 .57
wk2 -1.00 .67 -6.00 E-03 .70
wk3 -.83 1.33 .59 .83
wk4 -.83 1.67 .79 .97
wk5 -.83 1.80 1.09 1.09
wk6 -.83 1.80 1.16 1.12

80
gasw k6gasw k5gasw k4gasw k3gasw k2gasw k1gasw k0
Me
an
1.5
1.0
.5
0.0
-.5
-1.0
-1.5
-2.0
Figure 7: Average scale scores, GAS, from Time 1 to Time 7
Table 15 : t- scores, GAS, Time 1 to Time 7, (N=5)
Time Minimum Maximum Mean Std. Deviation
wk0 19.02 24.18 22.28 2.61
wk1 26.76 47.42 37.34 8.87
wk2 34.51 60.33 49.91 10.83
wk3 37.09 70.66 59.04 12.97
wk4 37.09 75.82 62.22 14.99
wk5 37.09 77.14 66.79 16.79
wk6 37.09 77.14 67.82 17.24

81
Mean gas t-scores time1 to time 7
gasw k6tscore
gasw k5tscore
gasw k3tscore
gasw k2tscore
gasw k1tscore
gasw k0tscore
Me
an
80
70
60
50
40
30
20
10
Figure 8. Mean t-scores, GAS, Time 1 to Time 7
4.3.2 Paired samples t-tests
4.3.2.1 Sensory Profile results:
A paired samples t-test using the Statistical Package of Social Sciences Version 17
(SPSS; Pallant, 2005) was conducted to evaluate the impact of the DPPT on the five
participants’ scores on the four quadrant scores namely, registration, sensory seeking,
sensitivity and sensory avoiding. Tables 16 and 17 report the paired sample scores and tests for
the Sensory Profile.
Registration:
There was a slight difference in scores from time 1 to time 2, however this was not a
statistically significant difference [M=4.05, SD = 0.3, t(4) = -1.13, p=0.3]. The eta squared
statistic (0.2) indicated a large effect size.

82
Seeking
There was a statistically significant difference in scores from time 1 to time 2 on
sensory seeking [M=3.92, SD = 0.32, t(4) = -2.97, p=0.04]. The eta squared statistic (0.68)
indicated a large effect size.
Sensitivity
There was a statistically significant difference in scores from time 1 to time 2 on
sensory sensitivity [M=3.76, SD = 0.48, t(4) = -5.65, p=0.005]. The eta squared statistic (0.88)
indicated a large effect size.
Avoiding
There was a statistically significant difference in scores from time 1 to time 2 on
sensory sensitivity [M=3.89, SD = 0.43, t(4) = -7.30, p=0.002]. The eta squared statistic (0.93)
indicated a large effect size.
Table 16: Paired Samples Statistics – Quadrant scores, Sensory Profile
(N=5)
Quadrants (Q) Pairs Mean Std. Deviation Std. Error Mean
Q 1 Time1 registration 3.85 .38 .17
Time2 registration 4.05 .32 .14
Q 2 Time 1 seeking 3.15 .65 .29
Time2 seeking 3.92 .33 .15
Q 3 Time1 sensitivity 2.92 .56 .25
Time2 sensitivity 3.76 .48 .21
Q 4 Time1 avoiding 2.98 .25 .11
Time2 avoiding 3.90 .43 .19

83
Table 17: Paired Samples Test, Quadrant scores, Sensory Profile, (N=5)
Paired Difference
s
t df Sig. (2-tailed)
Mean Std. Deviatio
n
Std. Error Mean
95% Confidence Interval of the Difference
Lower Upper
Pair 1 registration (T1,T2)
-.19 .37 .16 -.64 .27 -1.13 4 .32
Pair 2 seeking (T1,T2)
-.78 .58 .26 -1.50 -5.0776E-02
-2.97 4 .04
Pair 3 Sensitivity (T1,T2)
-.84 .33 .15 -1.25 -.43 -5.65 4 .00
Pair 4 avoiding (T1,T2)
-.92 .28 .12 -1.26 -.57 -7.30 4 .00
In summary, there was a significant statistical difference in mean scores of three quadrants out
of four and the highest statistically significant differences were on ‘sensitivity’(p=.0005) and ‘
avoiding’(p=.0002).
4.3.2.2 GAS results
A paired samples t-test was conducted to evaluate the impact of the DPPT on the goals
and a comparison was done between mean t-scores on GAS at Time1 (week 0) and Time 7
(week 6) for the five participants. There was a statistically significant difference in scores from
Time 1 to Time 7 on the GAS goals [M=67.82, SD = 17.24, t(4) = -5.538, p=0.005]. The eta
squared statistic (0.88) indicated a large effect size (refer Tables 17, and 18 for paired samples
test statistics).

84
Table 18: Paired Samples Statistics, GAS, (N=5)
t-score
Mean
Std. Deviation
Std. Error Mean
wk0 22.28 2.61 1.17
wk6 67.82 17.24 7.71
Table 19: Paired Samples Test, GAS, (N=5)
4.3.2.3 Parent/Carer questionnaire results
Descriptive statistics (mean and standard deviation) on the parent/carer questionnaire
were calculated to identify parents’ opinions on the DPPT intervention (see table 20) questions
were listed on a Likert scale and the parents were given a questionnaire at the end of 8 weeks
of commencing the intervention. (refer appendix 9 & 14…)
Paired
Differe
nces
t df Sig. (2-
tailed)
Mean Std.
Deviati
on
Std.
Error
Mean
95%
Confidence
Interval of the
Difference
Lower Upper Pair 1 t-scores,
wk0 -wk6 -45.54 18.39 8.22 -68.37 -22.71 -5.54 4 .005

85
Table 20: Descriptive data for parent questionnaire (1=strongly agree, 2=agree,
3=neutral, 4=disagree, 5=strongly disagree)
Scale
Minimum
Maximum
Mean
Std. Deviation
1. information satisfaction
1.00 2.00 1.20 .45
2. inconvenience
2.00 4.00 3.60 .89
3a. positive impact on daily routine
1.00 4.00 2.40 1.14
3b. negative impact on daily routine
3.00 5.00 4.00 .71
4. empowerment
1.00 2.00 1.40 .55
5. importance
1.00 1.00 1.00 .00
6. effectiveness 1.00 5.00 1.80 1.79
4.4 Summary
This chapter presented the results from the three tools namely the Sensory Profile, GAS
and parent questionnaire. The results indicated a significant statistical difference in scores on
Sensory Profile scores and GAS scores. Descriptive data from the parent questionnaires was
also outlined. The next chapter will present a discussion of the results.

86
Chapter 5: Discussion
5.1 Introduction
Sensory-defensiveness or ‘over-responsivity’ (Henry, 2007) has many implications for
children and families. This study examined the effectiveness of the Wilbargers’ Deep Pressure
and Proprioceptive Technique (DPPT), an intervention approach being used under the umbrella
of occupational therapy since the 1970s. The findings from this study indicated that DPPT was
effective for the five children involved in this study.
5.2 Sensory Profile
The comparative results from time 1(T1) and time 2(T2) from the raw quadrant scores
in the Sensory Profile, indicated that there was a reduction in sensory sensitivity and avoiding
as the total raw scores on these two quadrants increased for all children, indicating that the
children exhibited less sensitive and less avoiding behaviours than before. This indicated that
as a group, the scores for the five children moved towards the Sensory Profile normative scores
or from definite difference to typical performance (registration = between 64-72, seeking =
between 103-123, sensitivity = 81-94 and avoiding = between 113 – 133; Sensory Profile,
Dunn 1999). The highest statistically significant differences in mean scores were on
‘sensitivity’ (p=.0005) and ‘avoiding’ (p=.0002), and these two areas strongly determine
sensory defensiveness or over-responsivity (e.g., items like ‘responds negatively to loud
noises’, ‘avoids getting messy’, and ‘dislikes head upside down’) (Reynolds & Lane, 2008).
Four out of the 5 participants had a formal diagnosis of Autism in this study, even
though this was not a specified inclusion or exclusion criteria. The Sensory Profile was
developed by Dunn (1999) to assess the responses of both children with disabilities and
children without disabilities to a variety of commonly occurring sensory experiences based on
parent/caregiver report (Ermer & Dunn, 1998). Studies by Kientz and Dunn (1997), Ermer and
Dunn (1998), Watling et al. (2001), Kern et al. (2006b), Rogers et al., (2003), and Tomchek

87
and Dunn (2007) provide evidence of sensory processing differences between children with
and without Autism Spectrum Disorder (ASD).
The results from this study were consistent with a previous study by Brown et al.
(2008), which compared Australian children with ASD and typically developing children. In
Brown’s study (2008), the children with ASD had lower average responsiveness quadrant
scores in relation to poor registration, sensation seeking, sensitivity to stimuli, and sensation
avoidance than their typically developing peers. In this study all 5 participants scored lower in
three out of the four Sensory Profile quadrants (5 out of 5 scored lower on sensitivity and
avoiding, 4 out of 5 scored lower on seeking, and 2 out of 5 scored lower on registration). The
section score results from this study indicated that 10 out of the 14 Sensory Profile category
areas (auditory processing, vestibular processing, touch processing, multisensory processing,
oral sensory processing, modulation of movement, emotional responses, social emotional
behaviours, behavioural outcomes to sensory processing and thresholds for response) had
significantly lower scores (e.g., in the definite difference category), which is again consistent
with Brown’s study (2008) that indicated that children with ASD had low scores on all 14
categories.
5.3 Goal Attainment Scaling (GAS)
The GAS paired t-tests results in this study indicated that there were significant
differences in the goals identified and rated by the children’s parents (p=.005). As well, the
large effect size (.88) demonstrated that the changes were not likely to occur by chance
(Pallant, 2005).
GAS methodology has been successfully applied in previous occupational therapy
effectiveness studies in paediatric settings, including rehabilitation (Lannin, 2003; Mitchell &
Cusick, 1998) and school systems (Dreiling & Bundy, 2003; King et al., 1999).

88
The first known application of GAS in a research protocol for children with sensory
integration dysfunction occurred in two pilot studies conducted between 1997 and 2005
(Mailloux et al., 2007). The studies examined the effectiveness of Occupational Therapy-
Sensory Integration (OT-SI) for children ages 4 to 12 years who were identified as having
atypical responsiveness to sensation. In these pilot studies, the children participated in OT-SI
for 20 sessions over a 10-week period. Effectiveness of the intervention was measured by
examining pretest and posttest changes in behavioural responses using traditional standardised
assessments. Additionally, parents were interviewed at the initiation of the study to establish
objectives written according to the GAS process to reflect potential intervention outcomes that
were meaningful to the parents and family and that were not typically reflected in the
standardised and physiological measures. This methodology was consistent with that used in
this study.
GAS measures in the study by Mailloux et al. reflected the most significant gains with a
pre-treatment and post-treatment difference score (M = 25.31, SD = 11.71, p < .0001) and a
large effect size of 2.16. Thus, scaling goals using GAS appeared to be the most sensitive
means to reflect change in individual children. This was again consistent with the current study
[M=67.82, SD = 17.24, t(4) = -5.538, p=0.005] with a large effect size of 0.88.
Further, their study demonstrated that GAS could capture individual changes in daily
life occupations that are functional, meaningful alterations in occupational performance over a
short intervention period in a small sample (Mailloux et al. 2007) consistent in this study (see
appendix 14 for parent comments)
When developing a GAS process for use with children who have sensory integration
dysfunction, the collaborative team (Mailloux et al., 2007) recommended a number of steps be
used in their study that were consistent to the methodology used in this current study, for
example:

89
• the occupational therapist who was trained to write the GAS goals should review
the child’s records, including evaluation and sensory history;
• the GAS goal-writing therapist and the therapist providing the OT-SI
intervention should not be the same person.
• the parent goal-setting meeting should take place using a semi-structured
interview format with consistent structure across clinical sites (if more than one site is
involved);
• the GAS goal-writing therapist should review the scaled goals with the parents
to validate the expected level of performance; and
• after a standard designated intervention period, a follow-up meeting should be
conducted with the parents to determine the child’s progress on the scaled goals.
The study by Mailloux et al. (2007) concluded that considering the potential value of
this method, especially in the application to children with sensory integration disorders in
which outcomes of intervention are typically diverse and highly individualised, GAS offers
therapists a unique method of capturing outcomes that are truly meaningful to children and
families.
Other studies published that have used GAS as an outcome measure in paediatric
studies including Turner-Stokes et al. (2010) (in children – use of Botulinum toxin), Cusick et
al. (2006) (comparing GAS with COPM in paediatrics), Klepper et al. (2007) (children with
minor motor difficulties). These studies are consistent with the consensus that GAS is a valid
tool for use in studies that evaluate the effectiveness of clinical interventions such as the DPPT.
Mora and Chapparo’s unpublished study (2008) also used GAS as an outcome measure for
studying the impact of the Wilbargers’ DPPT protocol.

90
5.4 Wilbargers’ Deep Pressure and Proprioceptive Technique (DPPT).
The study results indicate that the Wilbargers’ DPPT appeared to be effective for the
five case studies involved in this study. The effect size statistics indicated the magnitude of the
intervention’s effect and was not just whether the difference could have occurred by chance
(Pallant, 2005). The large effect size (0.88) in this study (.01=small effect; .06 = moderate
effect; .14= large effect [Pallant, 2005]) indicated that the DPPT intervention was effective, as
no other variables were changed from the daily routines of the participants and the passage of
time pre- and post-intervention was only 6 weeks which cannot fully account for significant
developmental changes in the five children.
The previously completed DPPT effectiveness studies (that are summarised in Table 6)
have had mixed findings.
In a study by Kimball et al. (2007), salivary cortisol was tested pre and post one session
of the Wilbargers’ DPPT. This was similar to this study because a single subject case design
across 4 participants with sensory defensiveness was used and two of the participants had ASD
and PDD (pervasive development disorder). The results were that changes in the salivary
cortisol levels in all 4 boys indicated that the procedure used modulated the cortisol levels and
there was an association between sympathetic nervous system response and the Wilbarger
protocol-based procedure. It did not clearly state the effectiveness of the intervention technique
for sensory defensiveness and the term used was ‘Wilbarger protocol- based procedure’.
In a study by Snyder and Stonebraker (2001), a single subject with sensory
defensiveness was used, and the results indicated that the effectiveness of the sensory
summation technique (Wilbargers’ DPPT) was confirmed. The participant demonstrated
functional improvements in group participation at school, decreases in incidence of tantrums,
and social participation at home and in the community. However this was a small sample and
was never published.

91
In an Australian study by Stagnitti et al. (1999), a single subject with sensory
defensiveness was used and results from repeating the sensory checklist and Millers
Assessment for Preschoolers, indicated favourable results and reduction in sensory
defensiveness, to the use of the Wilbarger’s brushing protocol, in association with behavioural
strategies. This study was done in an Australian context and the results were similar to this
study.
Another Australian study by Mora and Chapparo, 2008, used 16 participants with
developmental delay or intellectual disability and was a randomised controlled study with the
experimental group receiving sensory intervention (DPPT) and the control group receiving a
behavioural intervention with random allocation. GAS was used as one of the outcome
measures in the study. The results demonstrated a statistically significant difference (p=.001) in
GAS scores between sensory and behavioural interventions in favour of sensory intervention
(Mora & Chapparo, 2008). The result is similar to this study which demonstrated a score of
p=.005 on the GAS t-scores for the DPPT intervention.
However, in most of the above studies reported except for one (unpublished, Mora &
Chapparo, 2008), the DPPT was not specifically carried out as proposed by Wilbarger and
Wilbarger. They propose to follow the DPPT every two hours over minimum 6 weeks, for its
effectiveness (Wilbarger & Wilbarger, 1991, 2007, 2009) and therefore the studies may not be
a true measure of the effectiveness of the DPPT.
A study by Segal and Beyer (2006) observed that children’s positive responses and
parental observation of the immediate effects of DPPT were critical to maintaining adherence
which is consistent with the comments received from parents of children involved in this study
(See appendix 14). However their study reported that the frequency of treatment was identified
as an inconvenience for parents and was not flexible with daily routines whereas in this study 4
out of 5 parents reported that they did not find the frequency of completing the DPPT regime

92
inconvenient. They reported that they fitted it in with their daily routines, as per the parent
questionnaire. Segal and Beyer, (2006) studied the parental observations and most of their
families did not follow the DPPT protocol where it needed to be completed every two hours.
5.5 Family-Centred Practice and Sensory-Based Interventions
Occupational therapists have an important role in working with children and families
with additional needs. According to an Australian study by SCOPE, (2005) families want
balance in their life, and want their lives to be more than just about their child’s disability.
They want to be respected, valued and confirmed for the choices they make. Evidence in the
literature (SCOPE, 2005) suggests that children do better where goal setting is collaborative
between practitioners and families, and where goals reflect needs and priorities in the context
of the child’s natural environments.
Family-centred practice is considered best practice when working with children and
whatever input is provided to the children and family should be within this context. Family-
centred practice is synonymous with client-centred practice which is now a hallmark of
occupational therapy service provision. All elements of occupational therapy should bring joy
and increased participation in the lives of children and families. Using a family-centred
approach in paediatric rehabilitation results in greater parental satisfaction with services,
enhanced parental psychosocial wellbeing, and improves the psychological adjustment of
children (King, Law, King, & Rosenbaum, 1998). In a meta-analysis by Dunst et al. (2007), on
family centred helpgiving practices research, the results from a meta-analysis of 47 studies
indicated that the use of family-centered practices seems both warranted and indicated, in
programs working with children and their parents and other family members.
With the continued use of sensory-based intervention techniques like the Wilbargers’
DPPT, occupational therapists believe that they are providing children and their families with a
tool that can increase their participation and provide better access to their local programmes

93
and within the community. DPPT is not meant to be provided in isolation and has to be
presented within the context of the family and the community. Therefore sensory diets are
usually recommended along with the DPPT and the child’s everyday routines are taken into
consideration while preparing a suitable home programme for the child and family (Wilbarger
& Wilbarger, 2007).
When the DPPT regime was suggested as an intervention strategy for the five
participants in this study, everyday routines and daily living tasks were severely impacted upon
by behaviours (such as inability to go near escalators, near hairdryers and lawn mowers,
distress going into the shower, on a swing, in shopping centres, eating more than a few food
textures, wearing particular textured clothes, and many other such everyday experiences) were
taken into account. Four out of five participants followed up the intervention technique as
prescribed and parents reported significant changes to their everyday routines due to the
marked reduction of the sensory defensive behaviours exhibited by their children.
GAS and parent questionnaires were used to actively involve families in goal setting,
goal scoring and providing their valued opinions and comments as is conducive to family-
centred practice. Based on parent questionnaire results and comments from parents/carers, in
their opinion, they found the intervention to be effective for their children and all five parents
felt empowered and that they had benefited from the information that they received during the
course of the DPPT intervention. Parent/carer perspective was given utmost important
throughout the course of this study and parents reported that they enjoyed receiving follow up
phone calls and giving scores to the goals for their children.
5. 6 Summary
Based on earlier studies completed, it is inconclusive whether the DPPT regime has
demonstrated therapeutic efficacy. The previously completed studies had a number of
methodological weaknesses including small sample sizes, failure to follow the DPPT

94
intervention as specified by the Wilbargers’, use of multiple assessment methods, and no
standardised tools (such as the Sensory Profile or the Sensory Processing Measure) available
for measuring outcomes. More rigorously executed studies with larger randomly selected
samples and sound methodology are required. However the results of this study from the
Sensory Profile and GAS scores appear to indicate that the DPPT regime was effective for the
five participants. The next chapter will present the study conclusions.

95
Chapter 6: Limitations, Future Research, Professional Implications,
and Conclusion
6.1 Introduction
This chapter will include the limitations to the study, suggestions for future research,
professional implications and general conclusions.
6.2 Limitations
A number of limitations to this study should be acknowledged. This was a pre – post
study using a series of single case studies with participants from multiple sites, assessed at
baseline and at intervals. The study results indicated that there was a significant difference in
Sensory Profile and GAS scores; however some limitations need to be mentioned.
The number of participants was small (N=5) and ideally this study should be repeated
with a larger sample and with children in different settings and presenting with other
diagnoses. A matched control group of children was not included therefore comparative
participant data was not obtained. Participants were not selected randomly and were recruited
from one geographical region. This limits generalising the results.
The investigator carried out the assessments, pre and post, and the follow up with the
GAS goals and recorded the observations based on parent scores and this can be considered a
limitation in the study as the aims were known to the investigator.
6.3 Recommendations for future research
Recommendations for future research include completing similar studies using larger
sample sizes and over larger geographical regions. Also including children with varying
diagnostic groups (such as child and adolescent mental health, paediatric neurology, paediatric
genetic disorders and from school aged population) where sensory defensive behaviours may
be interfering with school function is suggested. Also conducting randomised control studies
where one group receives the DPPT and the other is a control group that can avail of the

96
intervention post the 6 weeks of the study if they desire will allow for meaningful comparisons.
Finally, completing a qualitative study investigating the parents/caregivers experiences of
implementing the DPPT regime with their child is recommended given that it requires
diligence and commitment on the part of family members.
6.4 Implications for future research and for the profession
The Wilbargers’ Deep Pressure and Proprioceptive Technique (DPPT) is a popular
intervention approach used by occupational therapists for treating over- responsiveness or
sensory defensiveness. Based on a survey completed by Sudore (2001), in New York, 78 % of
the 64 occupational therapists registered with American Occupational Therapists Association,
who responded, used the Wilbargers’ DPPT to treat tactile defensiveness. According to
Kimball et al. (2007), more than 15,000 healthcare professionals have received specialised
training in DPPT and 20,000 brushes used as part of the DPPT regime are ordered every year.
This study makes a small contribution to the body of empirical data related to the DPPT
promoted by the Wilbargers’; however more studies using valid and sensitive measures, larger
samples and in a variety of settings are needed especially in school-aged children, where it is
extremely difficult to follow through with such intervention techniques that demand time and
repetition. According to Bourke–Taylor et al. (2010), service provision within educational
settings tends to require interventions that facilitate the student role and opportunities to
communicate and accommodate family goals and concerns may positively impact the child’s
education, as well as ease the difficulties experienced by children and caregivers in the home
environment.
Occupational therapy has been approved since November 2008 as an essential service
for children with ASD. Medicare in Australia will fund up to 20 sessions per year for children
with ASD and up to five sessions per year for children with a chronic illness to access
occupational therapy services. Sensory processing and defensive issues are a commonly

97
presenting issue in clinical practice. Occupational therapy using a sensory integrative approach
(OT/SI) is one of the most frequently used intervention approaches within occupational therapy
(Mulligan, 2002). Many occupational therapists are using the Wilbarger’s DPPT as one method
to assist with sensory processing and defensive issues that children present with. The lack of
evidence supporting clinical practice and the continued use of the Wilbarger’s DPPT regime as
an intervention strategy for sensory defensiveness by occupational therapists warrants further
investigation to clearly establish its efficacy.
6.5 Conclusions
Sensory-based interventions have always been met with scepticism due to the paucity
of rigorous research, overlap with behavioural issues and limited valid quantitative measuring
tools. Yet in clinical practice especially with children, sensory issues seem to interfere with
daily functional performance for many children. Despite the varied findings related to sensory
integration research, sensory integration therapy is a widely used intervention method in
occupational therapy. Many healthcare and educational professionals have expressed concerns
regarding the lack of empirical support for sensory integration theory and practice (McWilliam,
1999; Shaw, 2002). Recent research has also included parents’ perceptions of change in their
children and in themselves as a result of occupational therapy that used sensory integration
approaches (Cohn, 2000; Miller et al. 1999). Research based on rigorous methodology and
sensitive outcome measures has provided some evidence documenting the existence of sensory
modulation dysfunction (SMD) (Mangeot et al., 2001; McIntosh et al., 1999; Miller et al.,
1999).
In this study, the Wilbargers’ DPPT regime for treating children presenting with
sensory defensiveness was examined using a multiple single case study approach. The results
appear to support the use of the DPPT with children presenting with signs of sensory
defensiveness. The parent questionnaires also indicated that the parents rated ‘importance’ as

98
highest, indicating that it is very important for them to reduce their child’s sensory defensive
behaviours and 4 out of 5 parents reported that they felt the intervention was effective for their
child. This fits with the principles of client-centred practice where therapists and clients and
families work together collaboratively. In summary, the findings of the study support the use of
DPPT but further ongoing investigations are needed.

99
References
Ayres, A. J. (1964). Tactile functions: Their relation to hyperactive and perceptual motor
behaviour. American Journal of Occupational Therapy, 18, 6-11.
Ayres, A. J. (1969). Relation between Gesell developmental quotients and later perceptual-motor
performance. American Journal of Occupational Therapy, 23(1), 11-17.
Ayres, A. J. (1972a). Sensory integration and learning disorders. Los Angeles, CA: Western
Psychological services.
Ayres, A. J. (1972b). Types of sensory integrative dysfunction among disabled learners. The
American Journal of Occupational Therapy, 26(10), 13-18.
Ayres, A. J. (2005). Sensory integration and the child (25th Anniversary Edition.). Los Angeles,
CA: Western Psychological Services.
Baranek, G. T., Foster, L. G. & Berkson, G. (1997). Tactile defensiveness and stereotyped
behaviours. American Journal of Occupational Therapy, 51, 91-95.
Baranek, G. T. (1999). Autism during infancy: a retrospective video analysis of sensory-motor
and social behaviours at 9 -12 months of age. Journal of Autism and Developmental Disorders,
29, 213-224.
Baranek, G. (2002). Efficacy of sensory and motor interventions for children with Autism.
Journal of Autism and Developmental Disorders, 32(5), 397-421.
Baxter, P., & Jack, S. (2008). Qualitative case study methodology: study design and
implementation for novice researchers. The Qualitative Report, 13(4) 544-559
Bourke-Taylor, H., Howie, L., & Law, M. (2010). Impact of caring for a school-aged child with
a disability: Understanding mothers’ perspectives. Australian Occupational Therapy
Journal,57(2),127-36.

100
Brown, T., Leo, M., & Austin, D. W. (2008). Discriminant validity of the Sensory Profile in
Australian Children with Autism Spectrum Disorder. Physical and Occupational therapy in
pediatrics, 28(3), 253-266.
Bundy, A. C., Lane, S., J., Murray, E., A. (2002). Sensory integration theory and practice (2nd
ed.). Philadelphia: F. A. Davis Company.
Campbell, R., & Ahrens C. (1998). Innovative community services for rape victims: An
application of multiple case study methodology. American Journal of Community Psychology,
26, 537-571.
Canadian Association of Occupational Therapists (1997). Enabling occupation: an occupational
therapy perspective. Ottawa, Ontario: CAOT Publications
Canadian Association of Occupational Therapists (2002). Enabling occupation: an occupational
therapy perspective. Ottawa, Ontario: CAOT Publications ACE
Canadian Association of Occupational Therapists (2008). Enabling occupation: an occupational
therapy perspective. Ottawa, Ontario: CAOT Publications
Case – Smith, J. (2005). Occupational therapy for children (5th Ed.). St. Louis: Elsevier Inc.
Cermak, S. (1988). The relationship between attention and sensory integration Dysfunction
(part1), Sensory integration special interest section newsletter, 11, 1-4.
Clark, G. & Ward, S. (1999). Charting results: Evaluating progress of children with sensory
processing disorder. OT Practice, 4(10), 12-16.
Cohn, E., Miller, L. J., & Tickle-Dengen, L. (2000). Parental hopes for therapy outcomes:
Children with sensory modulation disorders. American Journal of Occupational Therapy, 54, 36-
43.
Cohn, E. (2001). Parent perspectives of occupational therapy using a sensory integration
approach. American Journal of Occupational Therapy, 55, 285–294.

101
Cool. S., (1990). Use of a surgical brush in treatment of sensory defensiveness: Commentary and
exploration. Sensory Integration Special Interest Section Quarterly, 13(4), 4-6.
Coster, W., Deeney, T., Haltiwanger, J., & Haley, S. (2008) School Function Assessment user's
manual. San Antonio, TX: Therapy Skill Builders.
Cusick, A., & Ottenbacher, K. (1994). Goal attainment scaling: Continuing education evaluation
tool. Journal of Continuing Education in Health Professionals, 14(3), 141-154.
Cusick, A., McIntyre, S., Novak,I., Lannin, N., & Lowe, K. (2006). A comparison of goal
attainment scaling and the Canadian Occupational Performance Measure for paediatric
rehabilitation research. Developmental Neurorehabilitation, 9(2), 149-157.
DeGangi, G. (2000). Pediatric disorders of regulation in affect and behaviour. San Diego, CA:
Elsevier.
Deitz, J. C. (2006). Single – Subject Research. In G. Kielhofner (ed), Research in Occupational
Therapy: Methods of inquiry for enhancing Practice. Philadelphia: F. A. Davis Company.
Diagnostic and Statistical Manual of Mental Disorders (DSM IV) (1994). American
Psychological Association.
Dreiling, D. S., & Bundy, A. C. (2003). Brief Report—A comparison of consultative model and
direct–indirect intervention with preschoolers. American Journal of Occupational Therapy, 57,
566–569.
Dunn, W., Brown, C., & McGuigan, A. (1994). The ecology of human performance: a
framework for considering the effect of context. The American Journal of Occupational
Therapy, 48(7), 595-607.
Dunn, W., & Westman, K. (1995). The Sensory Profile. Unpublished manuscript, University of
Kansas Medical Center, Kansas City.

102
Dunn, W. (1997). A conceptual model for considering the impact of sensory processing abilities
on the daily lives of young children and their families. Infants and young children, April,10, 23-
25.
Dunn, W. (1999). Sensory Profile: User’s Manual. San Antonio TX: The Psychological
Corporation.
Dunn, W. (2000). Best practice occupational therapy. Thorofare, NJ: SLACK incorporated
Dunn, W. (2002). The Sensory Profile: Administration and interpretation, participant’s
handbook. Melbourne, VIC: Scope.
Dunn, W., Brown, C., & Youngstrom, M. J. (2003). Ecological model of occupation, in
Perspectives in human occupation participation in Life. Philadelphia, Pennysylvania: Lippincott
Williams & Wilkins.
Dunn, W. (2008). Technical report: Sensory Profile. San Antonio TX: The Psychological
Corporation.
Dunst, C. J., & Bruder, M. B. (2002). Valued outcomes of service coordination, early
intervention, and natural environments. Exceptional Children, 68, 361-375.
Dunst, C. J., Trivette, C. M., & Hamby, D. W. (2007). Meta-analysis of family centred
helpgiving practices research. Mental Retardation and Developmental Disabilities Research
Review, 13, 370-378
Dziegielewski, S., & Powers, G. (2000). Designs and procedures for evaluating crisis
intervention in Roberts’(ed) Crisis intervention handbook. NY, US: Oxford University Press
Einfeld, S. L., & Tonge, B. J. (1995). The Developmental Behaviour Checklist: The
development and validation of an instrument to assess behavioural and emotional
disturbance in children and adolescents with mental retardation. Journal of Autism and
Developmental Disorders, 25(2), 81-104.

103
Ermer, J.,& Dunn, W. (1998). The Sensory Profile: A discriminant analysis of children with and
without disabilities. American Journal of Occupational Therapy, 52, 283–290.
Field, T. (1981). Gaze behaviour of normal and high-risk infants and during early interactions.
Journal of the American Academy of Child Psychiatry, 20, 308-317.
Fish, B., & Dixon, W. J. (1978). Vestibular hyporeactivity in infants at risk for schizophrenia.
Archives of General Psychiatry, 35, 963-971.
Forbes, D. A. (1998). Goal Attainment Scaling. A responsive measure of client outcomes.
Journal of Gerontology and Nursing, 24(12) 34-40.
Foss, A., Swinth, Y., McGruder, J., & Tomlin, G. (2003). Sensory modulation dysfunction and
the Wilbarger protocol: an evidence review. OT Practice, 8, CE-1-CE8.
Frick, S. (2009). Therapeutic Listening®: Listening with the whole body (course manual),
Madison, WI: Vital Links
Hanshu, B. (2003). Evaluation and treatment of sensory processing disorders. Presented at
developmental concepts, the ready approach conference, Boise, ID.
Henry, D.A., Kane-Wineland, M., & Swindeman, S. (2007). Tools for Tots, Glendale, Arizona:
Henry OT Services Inc.
Hopkins, H. (1978) Current basis for theory and philosophy of occupational therapy (1978). In.
(5th ed.) Willard and Spackman’s Occupational therapy. Philadelphia: Lippincott Company.
Interdisciplinary Council on Developmental and Learning Disorders, (2005). Diagnostic manual
for infancy and early childhood: mental health, developmental, regulatory-sensory processing,
and language disorders and learning challenges (ICDL-DMIC). Bethesda, MD: Author.
International Classification of Diseases (ICD 10) (1992). World Health Organization.
Kandel, E., Schwartz, J., & Jessel, T. (1991). Principles of neural science (3rd ed.). Connecticut:
Appleton & Lange.

104
Kelly, J. (1991) The sense of balance. In Kandel et al., (Eds.) Principles of neural science.
Connecticut: Appleton & Lange
Kempermann, G., & Gage, F. H. (1999). Experience-dependent regulation of adult hippocampal
neurogenesis: Effects of long-term stimulation and stimulus withdrawal. Hippocampus, 9, 321–
332.
Kern, J.K., Trivedi, M.H., Garver, C.R., Grannemann, B.D., Andrews, A.A., Savla, J.S.,
Johnson, D.G., Mehta, J.A., & Schroeder, J.L. (2006b). The pattern of sensory processing
abnormalities in autism. Autism, 10, 480–494.
Kielhofner, G. (2008) Model of Human Occupation: Theory and application (4th ed.).
Philadelphia: Lippincott Williams & Wilkins.
Kielhofner, G., (2006) Research in occupational therapy: Methods of inquiry for enhancing
practice. Philadelphia: F. A. Davis Company.
Kientz, M.A., & Dunn, W. (1997). A comparison of the performance of children with and
without autism on the Sensory Profile. American Journal of Occupational Therapy, 51, 530–537.
Kimball, J., Lynch, K., Stewart, K., Williams, N., Thomas, M., Atwood, K. (2007). Using
salivary cortisol to measure the effects of a Wilbarger Protocol-based procedure on sympathetic
arousal: A pilot study. American Journal of Occupational Therapy, 61(4), 406-413
Kinnealey, M., Oliver, B., & Wilbarger, P. (1995). A phenomenological study of sensory
defensiveness in adults. American Journal of Occupational Therapy 49(5), 444-451.
Kinnealey, M., (1998). Princess or tyrant: A case report of a child with sensory defensiveness.
Occupational Therapy International, 5 (4), 293 – 303.
King, G., Law, M., King, S., & Rosenbaum, P. (1998). Parents’ and service providers’
perceptions of the family-centredness of children’s rehabilitation services. Physical &
Occupational Therapy in Pediatrics, 18(1), 21-40.

105
King, G. A., McDougall, J., Palisano, R. J., Gritzan, J., & Tucker, M. A. (1999). Goal attainment
scaling: Its use in evaluating paediatric therapy programs. Physical and Occupational Therapy in
Paediatrics, 19(2), 31-52.
King, G. A., McDougall, J., Tucker, M. A., Gritzan, J., Malloy-Miller, T., Alambets, P. (1999).
An evaluation of functional, school-based therapy services for children with special needs.
Physical and Occupational Therapy in Pediatrics, 19, 5–29.
Kirusek, T. J., & Sherman, R. E. (1968). Goal Attainment Scaling: a general method for
evaluating comprehensive community mental health programs. Community Mental Health
Journal. 4(6), 443-453.
Kirusek, T. J., Smith, A., & Cardillo, J. E. (1994). Goal Attainment Scaling: Applications, theory, and
measurement. Hillsdale, NJ: Lawrence Erlbaum Associates.
Klepper, K., Burns, Y. R. and Watter, P. (2007). Goal attainment scaling as an outcome measure
in Australian children with minor motor difficulties. In World Physical Therapy 2007: 15th
International Congress of The World Confederation for Physical Therapy: Moving Physical
Therapy Forward, 2-6 June 2007, (S354-S354), Vancouver, Canada.
Koh, C. (2008). Australian occupational therapists’ practice in cognitive rehabilitation for
clients after stroke: Congruent with current research evidence. Unpublished Master of
Philosophy dissertation, University of Queensland, Queensland, Australia.
Koomar, J., Szklut, S. & Cermak, S. (2004). Making sense of sensory integration (Compact
Disk). Las Vegas, NV: Sensory Resources
Lane, S. J., Miller, L. J., & Hanft, B. E. (2000). Towards a consensus in terminology in sensory
integration theory and practice: Part 2 sensory integration patterns of function and dysfunction.
Sensory Integration special interest quarterly, 23(2), 1-3
Lane, S. J., (2002). Sensory Modulation, in Bundy, A.C., Lane, S. J., & Murray, E. A. (Eds).
Sensory Integration: theory and practice (2nd ed.). Philadelphia, PA: FA Davis and Company.

106
Lane, S. J., & Schaaf, R. C. (2010).Examining the neuroscience evidence for sensory-driven
neuroplasticity: implications for sensory-based occupational therapy for children and
adolescents. American Journal of Occupational Therapy, 64(3), 375-390.
Lannin, N. (2003). Goal attainment scaling allows program evaluation of a home-based
occupational therapy program. Occupational Therapy in Health Care, 17, 43–54
Law, M., Cooper, B., Strong, S., Stewart, D., Rigby, P., & Letts, L. (1996). The Person-
Environment-Occupation Model: A transactive approach to occupational performance. Canadian
Journal of Occupational Therapy, 63(1), 9-23.
Law, M., Baum, C., & Dunn W. (2005). Measuring occupational performance, supporting best
practice in occupational therapy (2nd ed). Thorofare, NJ: SLACK Incorporated.
Law. M., Missiuna, C., Pollock, N., & Stewart, D. (2005). Foundations for occupational therapy
practice with children, in Occupational therapy for children (5th ed.). St. Louis: Elsevier Inc.
Liss, M., Saulnier, C., Fein, D., & Kinsbourne, M. (2006). Sensory and attention abnormalities in
autistic spectrum disorders. Autism, 10(2), 155–172.
Lynch E., & Hanson, M. (1993). Changing demographics: Implications for training in early
intervention. Infants and Young Children, 6 (1), 50 – 55.
Mailloux, Z., May-Benson, T. A., Summers, C. A., Miller, L.J., Brett-Green, B., Burke, J. P.,
Cohn, E. S., Koomar, J., Parham, D., Roley, S. S., Schaaf, R. C., & Schoen, S. A. (2007). Goal
attainment scaling as measure of meaning outcomes for children with sensory integration
disorders. American Journal of Occupational therapy, 61(2), 254-259.
Mangeot, S. D., Miller, L. J., McIntosh, D. N., McGrath-Clarke, J., Simon, J., Hagerman, R. J.,
& Goldson, E., (2001). Sensory modulation dysfunction in children with attention deficit
hyperactivity disorder. Developmental Medicine and Child Neurology, 43, 399-466.

107
May- Benson, T. A., & Koomar, J. A. (2010). Systematic review of the research evidence
examining the effectiveness of interventions using a sensory integrative approach for children.
American Journal of Occupational Therapy, 64(3), 403-114
McDevitt, S. C., & Carey, W. . (1978). The measurement of temperament in 3-7 year old
children. Journal of Child Psychology, 19, 245-253.
McIntosh, D. N., Miller, L. J., Shyu, V., & Hagerman, R. J. (1999). Sensory-modulation
disruption, electrodermal responses, and functional behaviours. Developmental Medicine and
Child Neurology, 41, 608–615.
McWilliam, R. (1999). Controversial practices: The need for a reacculturation of early
intervention fields. Topics in Early Childhood Special Education, 19(3), 177-188.
Miller, L. J., McIntosh, D. N., McGrath, J., Shyu, V., Lampe, M., Taylor, A. K., Tassone, F.,
Neitzel, K., Stackhouse, T., & Hagerman, R., (1999). Electrodermal responses to sensory
stimulation in individuals with fragile X syndrome: A preliminary report. American Journal of
Medical Genetics, 83, 268-279.
Miller, L. J. (2006). Sensational kids: Hope and help for children and adolescents with sensory
processing disorder (SPD). New York, NY: G.P. Putnam’s Sons.
Miller, L. J., Anzalone, M. E., Lane,S. J., Cermak, S. A., & Osten, E.T. (2007). Concept
evolution in sensory integration: A proposed nosology for diagnosis, American Journal of
Occupational Therapy, 61,135-140.
Miller, L. J., Schoen, S. A., James, K., & Schaaf, R. C. (2007). Lessons learned: A pilot study of
occupational therapy effectiveness for children with sensory modulation disorder. American
Journal of Occupational Therapy, 61, 161–169.
Mitchell, T., & Cusick, A. (1998). Evaluation of a client-centered pediatric rehabilitation
programme using goal attainment scaling. Australian Occupational Therapy Journal, 45, 7-17.

108
Moore, K. & Henry, A. (2002). Treatment of adult psychiatric patients using the Wilbarger
Protocol, Occupational therapy in mental health, 18(1), 43-63.
Mora L., & Chapparo, C. (2008). The impact of the sensory protocol on the functional
behavioural responses of children with intellectual disability, sensory defensiveness and
behaviour support needs, Australian Society for Study of Intellectual Disability (ASSID)
Conference, Melbourne, Nov 2008(unpublished) retrieved on 16 July, 2009, from
http://www.assid.org.au/ConferencePapers/
Mulligan, S. (2002). Advances in sensory integration research. In A. C. Bundy, S. J.
Lane, & E. A. Murray (Eds.), Sensory integration theory and practice (2nd ed.,
pp. 397–411). Philadelphia: F. A. Davis
Novak, I. (2008). Notes from training workshop, Goal Attainment Scaling, held at Yooralla,
Melbourne.
Ottenbacher, K. J. (1982). Sensory integration therapy: affect or effect. American Journal of
Occupational Therapy, 36, 571-578.
Ottenbacher, K. & Cusick, A. (1993). Discriminative versus evaluative assessment: some
observations on Goal Attainment Scaling. American Journal of Occupational Therapy, 47(4),
349-354.
Oxford Centre for EBM evidence, (2009). Retrieved on July 13, 2010 from http://www.cebm.net
Palisano, R. J., Haley, S. M., & Brown, D. A. (1992). Goal Attainment Scaling as a measure of
change in infants with motor delays. Physical Therapy, 72(6), 432-437.
Pallant, J., (2005). SPSS survival manual: A step by step guide to data analysis using SPSS (2nd
Ed.). Crows Nest, NSW: Allen & Unwin.
Parham, D., & Mailloux, Z. (1996). Sensory integration and children with learning disabilities. In
P. N. Pratt & Allen, A. S. Occupational therapy in children (3rd ed.). 307-355.

109
Parham, D., & Mailloux, Z. (2005). Sensory integration. In J. Case Smith (Eds.), Occupational
therapy for children (5th ed.). St. Louis, MO: Mosby.
Polatajko, H. J., Kaplan, B., 7 Wilson, B. (1992). Sensory integration treatment for children with
learning disabilities: Its status 20 years later. Occupational Therapy Journal of Research, 12,
323-341.
Radomski M., & Trombly Latham C. (2008). Occupational therapy for physical dysfunction (6th
ed.). Baltimore, MD: Wolters Kluwer/ Lippincott Williams & Wilkins
Reisman, J., & Gross, A. (1992). Psychophysiological measurement of treatment effects in an
adult with sensory defensiveness. Canadian Journal of Occupational Therapy, 59, 248-257.
Reynolds, S., & Lane, S. J. (2008). Diagnostic validity of sensory over-responsivity: A review of
the literature and case reports. Journal of Autism and Developmental Disorders, 38, 516 – 529.
Rodger, S. & Ziviani, J. (2006). Occupational therapy with children. Oxford, UK: Blackwell
Publishing Ltd.
Rogers, S.J., Hepburn, S., & Wehner, E. (2003). Parent reports of sensory symptoms in toddlers
with autism and those with other developmental disorders. Journal of Autism and Developmental
Disorders, 33, 631–642.
Roley, S., Blanche, E. I., & Schaaf, R, C. (Eds.) (2001). Understanding the nature of sensory
integration with diverse populations. San Antonio, TX: Therapy skill builders.
Royeen, C. (1989). Commentary of ‘Tactile functions in learning disabled and normal children:
reliability and validity considerations’. Occupational therapy journal of research, 9, 16-23.
Royeen, C. (2010). Preface in Kramer and Hinojosa’s Frames for pediatric occupational therapy
(3rd ed.). Philadelphia, Pennsylvania: Lippincott Williams & Wilkins.
Sackett, D. L., Strauss, S. E., Richardson, W. S., Rosenberg, W. M. C., & Haynes, R. (2000).
Evidence-based Medicine: How to practice and teach EBM (2nd ed.). Edinburgh, UK: Churchill
Livingstone

110
Schaaf R. C., Miller L. J., Seawell D., & O'Keefe S. (2003). Children with disturbances in
sensory processing: a pilot study examining the role of the parasympathetic nervous system.
American Journal of Occupational Therapy, 57(4), 442-9.
Schaaf, R. C., & Davies, P. L. (2010). Evolution of the sensory integration frame of reference.
American Journal of Occupational Therapy, 64(3), 364-367
Schaaf, R. C., Schoen, S. A., Roley, S. S., Lane, S. J., Koomar, J., & May-Benson, T. A. (2010).
A frame of sensory integration in Kramer and Hinojosa’s Frames of reference for pediatric
occupational therapy (3rd ed.). Philadelphia, Pennsylvania: Lippincott Williams & Wilkins.
Scope, Statewide Specialist Service (2005). Family-centred practice: an evaluation of an early
childhood intervention service, Bulletin ,7, 15-17
Segal, R., & Beyer, C. (2006). Integration and application of a home treatment programme: A
study of parents and occupational therapists. American Journal of Occupational Therapy, 60(5),
500–510.
Shaw, S. (2002). A school psychologist investigates sensory integration therapies: promise,
possibility, and the art of placebo. National Association of School Psychologists Communique,
31(2). Retrieved on May 5, 2003 from http://www.naspoline.org/publications/cq3I2si.html.
Shellenberger S., & Williams, M. S. (1996). How does your engine run?, Albuquerque, NM:
Therapy works, Inc.
Snyder-Stonebraker, D. (2001). The effects of a Wilbarger-based brushing protocol: A single
subject study. Unpublished master’s thesis. University of Puget Sound, Tacoma, WA.
Stagnitti, K., Raison, P., & Ryan, P. (1999). Sensory defensiveness syndrome: A paediatric
perspective and case study. Australian Occupational Therapy Journal, 46, 175-187.
Stratton, J. & Gailfus, D. (1998). A new approach to substance abuse treatment in adolescents
and adults with ADHD. Journal of Substance Abuse, 15(2), 89-94.

111
Sudore, K. (2001). Tactile defensiveness and the Wilbarger brushing protocol in system
management. Unpublished master’s thesis. D’Youville College, Buffalo, New York.
Tomchek, S.D., & Dunn, W. (2007). Sensory processing in children with and without autism: a
comparative study using the Short Sensory Profile. American Journal of Occupational Therapy,
61(2), 190–200.
Townsend, E. & Polatajko, H. (2007). Enabling occupation II: Advancing an occupational
therapy vision for health, well- being, & justice through occupation. Ottawa, ON: Canadian
Association of Occupational Therapists.
Tronick, E. Z. (1989). Emotions and emotional communication in infants. American
Psychologist, 44(2), 112-119.
Turner-Stokes, l., Baguley, A. J., De Graff, S., Katrak, P., Davies, L., McCrory, P. & Hughes, A.
(2010). Goal attainment scaling in the evaluation of treatment of upper limb spasticity with
botulinum toxin: a secondary analysis from a double-blind placebo-controlled randomized
clinical trial. Journal of Rehabilitation and Medicine, 42, 81-89
Vargas, S., & Camilli, G. (1999). A meta-analysis of research on sensory integration treatment.
American Journal of Occupational Therapy, 53(2), 189-198.
Walker, E., & Emory, E. (1983). Infants at risk of psychopathology: Offspring of schizophrenic
parents. Child Development, 54, 1269 -1285.
Watling, R., Deitz, J., & White, O. (2001). Comparison of Sensory Profile scores of young
children with and without autism spectrum disorders. American Journal of Occupational
Therapy, 55, 416–423.
Wilbarger, P. (1984). Planning a “sensory diet”: Application of sensory processing theory during
the first year of life. Zero to three, 5(1), 7-12.
Wilbarger, J., & Stackhouse T. (2006). Sensory modulation: A review of the literature. retrieved
on January 16, 2009 from http:// www.OT –Innovations.com.

112
Wilbarger, P., & Wilbarger, J. (1991). Introduction to sensory defensiveness. (Audio tape), Van
Nuys, CA: Avanti Educational programs
Wilbarger, J. L., & Wilbarger, P. L. (2002). Wilbarger approach to treating sensory
defensiveness and clinical application of the sensory diet in Bundy, A. C., Murray, E. A., &
Lane, S. (eds.) Sensory Integration in theory and practice (2nd ed.). Philadelphia: F. A. Davis
Company
Wilbarger, P., & Wilbarger, J. (2007). Sensory defensiveness: A comprehensive treatment
approach. Panorama, CA: Avanti Educational Programs.
Wilbarger, P., & Wilbarger, J. (2009). Sensory defensiveness: Treatment Level II. Panorama,
CA: Avanti Educational Programs.
Williams, M.S., & Shellenbarger, S. (1996). “How does your engine run?”. Albuquerque, NW :
Therapy Works.
Wilson, B. N., Kaplan, B. J., Fellowes, S., Gruchy, C., & Faris, P. (1992). The efficacy of
sensory integration compared to tutoring. Physical and occupational therapy in pediatrics, 12(1),
1-36.
World Federation of Occupational Therapists (WFOT) (2004). What is occupational therapy?
Retrived on January 16, 2009 from http:// wfot.org/information.asp
World Health Organization (WHO) (1980). International classification of impairments,
disbilities and handicaps. Geneva: World Health Organization.
World Health Organization (WHO) (2001). International Classification of functioning, disability
and health: ICF (Short Version ed.). Geneva: World Health Organization.
Yin, R. K. (2003). Case study research: design and methods (3rd ed.). Newbury Park, CA: Sage.
Zbytniewski, R. (2002). The effects of sensory integration's Wilbarger technique on engaging
behaviours. Bay Shore, NY: Touro College. (Unpublished Master's project)

113
Zero to Three. (2005). Diagnostic classification: 0-3-revised. Arlington, VA: National centre for
clinical infant programs.

114
List of Appendices
Appendix
No
Description Page
number
Appendix 1 Evolution of sensory integration theory 115
Appendix 2 Treatment implementation Plan 116
Appendix 3 Ethics approval letter from Monash University 118
Appendix 4 Ethics approval letter from DEECD 119
Appendix 5 Yooralla permission letter 120
Appendix 6 Consent form 121
Appendix 7 Sensory Profile 122
Appendix 8 Sensory interview/ history 124
Appendix 9 Parent questionnaire 125
Appendix 10 Sample of GAS goals for a participant. 127
Appendix 11 Handout: sensory defensiveness 129
Appendix 12 The Deep Pressure Proprioceptive Technique/ DPPT 132
Appendix 13 Pictures of demonstration page 2. 133
Appendix 13 Comments from parent/carers 134

115
Appendix 1: The evolution of the sensory based occupational therapy
Sensory – based
Occupational therapy
Classical Sensory Integration
Ayres (1960s – 1989) Paediatric therapy network (2005)
Sensory Modulation/
processing
Winnie Dunn, Cemark, Royleen, Miller, Reisman, McIntosh & Simon (2001)
Based on a hierarchical model of CNS A classic SI includes the idea that the treatment must be child-directed, with the therapist guiding the just right challenge in order to facilitate adaptive responses (Wilbarger& Stackhouse, 2006).
Based on a systems model (heterarchic) of CNS Utilises the principle that there is a continuum of sensory responsivity with
hyporesponsiveness at one end and hyperresponsiveness at the other
(Parham & Mailloux, 2005)
Assessments
SCSIT(1972a), SIPT(1989) Bruninks-Osterstsky Test of Motor Profiency(1978), Miller Assessment for prechoolers(1988), School Function Assessment(1998)
Assessments
Sensory Profile (Dunn, 1999) Evaluation of sensory Processing, ESP,
(Parham &Ecker 2002) The Sensory Rating Scale (Provost, 1991) Touch Inventory for Elementary school-
aged children (Royeen & Fortune,
Commonly defined terms
Sensory integration, adaptive response, bilateral integration, ideation, praxis,
sequencing, somatosensory, perception, sensory systems, sensory registration
Commonly defined terms
Hyperresponsivity, hyporesponsivity, over/ underresponsiveness, sensory processing, sensory modulation, sensation seeking, sensory defensiveness, sensory discrimination, registration, thresholds for response
Intervention principles (Parham&Mailloux 2005)
Remediation of sensory integrative dysfunction Individual basis
Inner drive and child-centred and requires child – therapist interplay
Specialised equipment needed
Intervention principles (Dunn, 2000) Follows best practice and focuses on society and environment. Needs to be provided in the child’s context and environment. Supports participation and activity and applies the principles of sensory integration to daily life routines as a critical part of the intervention process.
Classical Sensory Integration treatment
Sensory-based interventions Providing tactile, poprioceptive, vestibular inputs Treating sensory defensiveness
Sensory based programs
Wilbarger’s protocol
Therapeutic listening
Alert Program
Sensory Diets

116
Appendix 2. Treatment Implementation Plan for Sensory Defensiveness
Name: ________________________________________Age: ___________
Time Key Events in The Day
DPPT OTT Other Sensory Diet Activities
Comments
Wake Up
Breakfast
Lunch
Dinner
Bedtime
DPPT = Deep Pressure and Proprioceptive Technique & OTT = Oral tactile Technique
Treatment Implementation plan : An example

117
Name: Danny X Age: 3.4 years
Time Key Events in
The Day
DPPT OTT Other Sensory Diet
Activities
5.45 – 6.30 Wakes up Leave toys or drawing out for Danny to be able to access and play
7:00
Wake Up Eat rice crackers Offer Weetbix regularly
X X Jump and Crash – 5 times/ bounce on trampoline or ball/ Row row your boat Use firm touch when dressing Danny. Watching TV after one activity
9.00 If at home If at kinder can engage in some deep pressure activities or climbing outdoors or blowing games.
X X Deep pressure with ball – 2 – 3 minutes Blowing games eg bubbles, whistles Include games/ songs which include jumping and crashing (humpty dumpty, bounce and sway, row row your boat etc) – 10 minutes max; If school drop off use a fidget toy
Choose any one activity for 5 mins
11.00 X X
1:00 – 2:00 Lunch X X Play outdoors
3.00 School Pick up X X Use fidget toys or favourite toy to hold during this time
5.00 Dinner X X Rolling over big ball with head and hands down. Roll ball over the top of Danny while he is lying on his tummy on the floor Body hugs Squeezes
7.00 Play with dad X X Rolling up in a towel and
unrolling –Sausage roll game Rough housing play. Ball pushes, somersaults, rolling ball, piggy backs, arm wrestles, sitting on ball/ air cushion for watching TV

118
Appendix 3: Ethics Monash University
Human Ethics Certificate of Approval
Date: 4 August 2009
Project Number: CF09/1623 - 2009000888
Project Title: The efficacy of using the Wilbarger’s Deep Pressure and Proprioceptive
Protocol on children with sensory defensiveness
Chief Investigator: Dr Ted Brown
Approved: From: 4 August 2009 to 4 August 2014
Terms of approval 1. The Chief investigator is responsible for ensuring that permission letters are obtained, if relevant, and a copy forwarded to MUHREC before any data collection can occur at the specified organisation.
Failure to provide permission letters to MUHREC before data collection commences is in breach of the National Statement on Ethical Conduct in Human Research and the Australian Code for the Responsible Conduct of Research. 2. Approval is only valid whilst you hold a position at Monash University. 3. It is the responsibility of the Chief Investigator to ensure that all investigators are aware of the terms of approval and to ensure the project is conducted as approved by MUHREC. 4. You should notify MUHREC immediately of any serious or unexpected adverse effects on participants or unforeseen events affecting the ethical acceptability of the project. 5. The Explanatory Statement must be on Monash University letterhead and the Monash University complaints clause must contain your project number. 6. Amendments to the approved project (including changes in personnel): Requires the submission of a Request for Amendment form to MUHREC and must not begin without written approval from MUHREC. Substantial variations may require a new application. 7. Future correspondence: Please quote the project number and project title above in any further correspondence. 8. Annual reports: Continued approval of this project is dependent on the submission of an Annual Report. This is determined by the date of your letter of approval. 9. Final report: A Final Report should be provided at the conclusion of the project. MUHREC should be notified if the project is discontinued before the expected date of completion. 10. Monitoring: Projects may be subject to an audit or any other form of monitoring by MUHREC at any time. 11. Retention and storage of data: The Chief Investigator is responsible for the storage and retention of original data pertaining to a project for a minimum period of five years.
Professor Ben Canny Chair, MUHREC Cc: Ms Anoopama Bhopti
Research Office Postal – Monash University, Vic 3800, Australia Building 3E, Room 111, Clayton Campus, Wellington Road, Clayton Telephone +61 3 9905 5490 Facsimile +61 3 9905 3831 Email [email protected] www.monash.edu/research/ethics/human/index/html ABN 12 377 614 012 CRICOS Provider #00008C

119
Appendix 4: Ethics, Department of Education and Early Childhood Development
Department of Education and Early Childhood Development
Department of Education and Early Childhood Development GPO Box 4637 Melbourne Victoria 3001 23 July 2009 Ms Anoo Bhopti Department of Occupational Therapy Monash University-Peninsula Campus PO Box 527 Frankston 3199 Dear Ms Bhopti, RE: Application to undertake research involving the Department of Education and Early Childhood Development I write to you concerning your application to the Early Childhood Research Committee (ECRC) to undertake research entitled “The efficacy of the Wilbarger’s Deep Pressure and Proprioceptive Protocol with children presenting with signs of
sensory defensiveness” I am pleased to inform you that the Department of Education and Early Childhood Development ECRC will support the research subject to the following conditions:
The research is conducted in accordance with the documentation you provided to the ECRC; The provision of a copy of the Monash University Human Research Ethics Committee approval letter; The provision of a final report to the ECRC at the completion of the research; The provision of a one page summary of the outcomes of the research and how this relates to the Department of Education and Early Childhood Development; That you provide the ECRC with the opportunity to review and provide comment on any materials generated from the research prior to formal publication. It is expected that if there any differences of opinion between the ECRC and yourself related to the research outcomes, that these differences would be acknowledged in any publications, presentations and public forums; That you acknowledge the support of the Department of Education and Early Childhood Development in any publications arising from the research; and The project is commenced within 12 months of this approval letter, after this time the approval lapses and extensions will need to be considered by the ECRC. If you have any further enquiries, please don’t hesitate to contact the ECRC Secretariat on 03 9947 1849 or via email [email protected]. The ECRC wishes you the best in your research and we look forward to seeing the results in due course. Yours sincerely Joyce Cleary Chair, Early Childhood Research Committee

120
Appendix 5: Approval from Yooralla
Permission Letter for Research Project “The efficacy of using the Wilbarger’s
Deep Pressure and Proprioceptive Protocol on children with sensory
defensiveness”. 2nd June, 2009 Dear Anoo, Thank you for your request to recruit participants from Yooralla Early Childhood services for the above-named research. I have read and understood the Explanatory Statement regarding the research and hereby give permission for this research to be conducted. I confirm Yooralla requires that written parental consent is obtained for children under the age of 18 to participate in the research. For students aged 16 to 18 it is preferable (but not obligatory) that the consent of both the parent and of the student is obtained. The consent must be informed consent, meaning that the person giving consent can comprehend the information provided and can make a voluntary choice whether to participate or not. It is a condition that any person conducting the research and who may have unsupervised access to a child must have a current Working with Children Check. Where the person conducting the research is supervised (at all times) by a Yooralla staff member who has a current Working With Children Check, this requirement does not apply. Yours Sincerely, Kathryn Finemore/ Sue Bray Managers Early Childhood Services Yooralla

121
Appendix 6: Consent Form
Consent Form - Families/ Caregivers of children attending Yooralla Early
Childhood Intervention Services
Title: Effectiveness of the Wilbarger’s Deep Pressure and Proprioceptive Technique / Deep
Brushing Program
NOTE: This consent form will remain with the Monash University researcher for their records
I agree that ________________________________________ may take part in the Monash University research project specified above. I have had the project explained to me, and I have read the Explanatory Statement, which I keep for my records. I understand that agreeing to take part means that: I agree to complete questionnaires asking me about my child’s sensory processing issues and sensory defensiveness and complete the Sensory Profile questionnaire.
I understand that agreeing to take part means that I am willing to follow up the programme with my child, ______________________________ and be available for the follow up appointments with the researcher. I understand that my participation is voluntary, that I can choose not to participate in part or all of the project, and that I can withdraw at any stage of the project without being penalised or disadvantaged in any way. I understand that any data that the researcher extracts from the questionnaire / survey for use in reports or published findings will not, under any circumstances, contain names or identifying characteristics. Participant’s name
Signature
Date

122
Appendix 7: Sensory Profile

123

124
Appendix 8: Sensory interview format, page1
Integrated Treatment Approach Assessment - 124 -
Sensory Area and Quality of sensation most likely to produce a defensive response
Performance Areas likely to be disrupted
Questions How does _______respond to: ?
Touch/ Tactile
Pain
Oral Tactile

125
Appendix 9 : Parent questionnaire
Questionnaire for Parents/ Caregivers
Families/ Caregivers of children attending Yooralla Early Intervention Services
Title: Effectiveness of the Wilbarger’s Deep Pressure and Proprioceptive Technique/ Deep
Brushing program
Date: _______ Dear parent/ caregiver, Thank you for continuing to participate in this research study. Please take a few minutes to complete this questionnaire as it will assist us in understanding your valuable experiences with this programme. Scale 1 – 5 1- STRONGLY AGREE; 2 – AGREE; 3 – NEUTRAL; 4 – DISAGREE; 5 STRONGLY DISAGREE 1 The information presented to me about the research study and the intervention programme was satisfactory 1---------- 2----------- 3-------------- 4---------------- 5-------------
2. This intervention protocol is labour intensive and causes inconvenience 1---------- 2----------- 3-------------- 4---------------- 5-------------
3. This intervention impacted on my daily routine - In a positive way? 1---------- 2----------- 3-------------- 4---------------- 5-------------

126
- In a negative way? 1---------- 2----------- 3-------------- 4---------------- 5-------------
4. This information/ assessment and follow up assisted me in increasing my understanding of my child’s sensory behaviours? 1---------- 2----------- 3-------------- 4---------------- 5-------------
5. It is very important to me to reduce my child’s sensory defensive behaviours 1---------- 2----------- 3-------------- 4---------------- 5-------------
6. This intervention was effective for my child 1---------- 2----------- 3-------------- 4---------------- 5-------------
Please place in the sealed envelope provided and return to your centre occupational therapist or to: Anoo Bhopti, Occupational therapist/ Researcher, 68 Kingston Rd, Heatherton 3202

127
Appendix 10 Sample of GAS goals for a participant (name changed)
Level of expected outcome
Goal 1 For Danny to tolerate messy play at kinder
Goal 2 For Danny to be able to use escalators in shopping centres
Goal 3 For Danny to tolerate loud noises better
Goal 4 To increase the variety of foods Danny eats and not gag
Much more than expected +2
Danny will join in messy play when led without any hesitation for more than 5 minutes
Danny will be able to board and ride the escalator without demonstrating any anxious behaviours (eg pushing, tantrums)
Danny will not cover his ears when the blender or hairdryer is on
Danny will eat a small piece of fruit 50 % of the times offered
More than expected +1
Danny will not resist approaching the messy play table and participate in messy play when led for 5 minutes
Danny will be able to board the escalator without demonstrating anxious behaviours (eg crying, tantrums) but then begins to demonstrate anxious behaviours (eg pushing, tantrums) whilst riding the escalator
Danny will not cover his ears for 10 - 30 secs when the blender or hair dryer is on
Danny will tolerate fruit pieces in his juice 50% of the times or more
Most likely outcome 0
Danny will try to run away, however will participate in messy play when led for 30 seconds - 1 minute
Danny will demonstrates anxious behaviours (eg pushing tantrums) when approaches an escalator but able to board the escalator
Danny will cover his ears 50% or more of the time when the hairdryer or blender is on
Danny will tolerate a tiny lump of fruit in his juice without spitting it out < 50% of the time
Less than expected outcome -1
Danny will run away up to 90% of the times when led to messy play and not participate in the activity
Danny will demonstrate anxious behaviours (eg pushing, tantrums) up to 90% of the time when approaches an escalator and unable to board the
Danny will cover ears every time the blender or hairdryer is on
Danny will tolerate thicker fruit juice

128
escalator
Much less than expected outcome -2
Danny will run away > 90% of the times when led to messy play and not participate in the activity
Danny will demonstrate anxious behaviours (eg pushing, tantrums) >90% of the time when approaches an escalator and unable to board the escalator
Danny will cover his ears in anticipation on the sight of blender or hairdryer going on
Danny will tolerate fruits in the form of fruit juice

129
Appendix 11: Handouts to parents
What is it?
Each of us has the ability to sense potential danger. Our senses tell us if a spider is creeping on our back, if we are at risk of falling, or when there is smoke in the air. At such times we can respond appropriately to protect ourselves from harm. Some people have a tendency to over protect or defend themselves. They respond to certain harmless sensations as if they were irritating, dangerous or even painful. This is called “Sensory Defensiveness”. Sensory defensiveness shows itself in an array of symptoms across one or more sensory systems as a result of the brain reacting to non-noxious stimuli. Sensory Defensiveness is in fact the over reaction of our normal protective senses. Each individual with sensory defensiveness has their own response style or a way of coping. These may be patterns of movement (extending arms and back), seeking out sensory experiences (unconscious attempt to process sensations more), physical avoidance, control, sensory seeking, fear, anxiety or even aggression.
There is a cost for the individual with Sensory Defensiveness. In its mildest form the person will not enjoy all of life’s activities to the full and will create routines and coping strategies to avoid sensory events or they may need time after an event to recover. In a child this may be seen in the child sleeping a lot more than normal, or seeking certain types of sensory input eg trampolining. In the most
severe form, the individual with sensory defensiveness will find all areas of life are impacted in a negative way so that interactions with others and the environment are so frightening and demanding that they may completely avoid them. In the young child fear limits their exploration of play and as a result physical, emotional and social development may be delayed.
SENSORY DEFENSIVENESS

130
Why does it happen?
Each sensation we experience in our bodies is perceived by the brain and assessed for it’s value or relevance in relation to the need to be ready for action (emotional or motor response). Before the brain initiates a response a decision is made: Do I need to respond to this stimulus? And if so, how much? The group of nerves responsible for this are called the Evaluative Sensory System, which are located deep in the brain. Sensory defensiveness occurs when the Evaluative Sensory System misinterprets the non noxious sensory stimuli and rather than disregarding the sensation or turning the sensation off, the brain initiates an anxiety reaction, to fight, fright or flight. FIGHT FRIGHT FLIGHT
Each of us have optimum level of alertness and when we have an event or experience that is more confronting, upsetting or scary our level or alertness is increased however we evaluate it, respond to it and then recover. In the person with Sensory Defensiveness each sensory event builds on the previous one and the individual’s level of alertness/reactivity increases without time for recovery, finally causing a physical response which may include: an increased heart rate, sweating, increased respiration, bodily withdrawal, crying, screaming, thrashing, anger or aggression.
How do you discover if you have Sensory Defensiveness?
When Sensory Defensiveness is suspected a thorough evaluation of the individual is made by interview and observation. As we mature, the individual with Sensory Defensiveness learns to tolerate or cope better with sensory experiences but the defensiveness never actually goes away. The interview therefore seeks information on early life experiences that signal the evidence of the condition. After the interview, therapists discuss the results to determine if it is truly Sensory Defensiveness as there are a large number of people in the normal population, and particularly children with additional

131
needs who have difficulties with one or more areas of sensory integration but do not have Sensory Defensiveness. Two particular areas of behaviour that signpost defensiveness diagnoses are
1. Coping styles and the recovery time an individual programs into his life. For a child this may be indicated by more sleep than normal or unable to stop/ shutdown.
2. Unusually high threshold to pain or very sensitive.
Can something be done? Once an individual has been diagnosed help is available. However the individual or family need to be willing to embark on an intensive treatment program. The intervention includes the application of a Therapressure program and Oral technique (Wilbarger protocol) and Sensory diet as prescribed by therapists. The protocol is simple in application but it is imperative that it is learnt properly and applied as directed, which is frequent and consistent approximately every 2 hours during waking hours or 8 times per day. The Sensory diet is supplementary sensory activities aimed at assisting the child to maintain their optimum alert state and avoid reactive behaviour. Generally intervention is ceased after a max of 4-6 weeks. Intervention is designed specifically for each individual and can significantly reduce or even eliminate the symptoms in many individuals. The intervention techniques have a scientific basis directly impacting the areas of our brain responsible for evaluating sensations. Years of clinical practice has shown that with a wide range of people and of all ages the program is very beneficial. The goal of treatment is not to simply “desensitize” but to assist the brain in correctly evaluating sensory information. The opposite of Sensory Defensiveness is a “joyful, jubilant exploration of sensation” which so many of us take for granted. Adapted from Wilbarger and Wilbarger (2007).

132
Appendix 12: The Deep Pressure Proprioceptive Technique/ DPPT
The DPPT which includes deep pressure input using a therapressure brush and joint proprioception/compression, is used for all children and adults. The oral technique is only used for some individuals. Before you start, prepare:
• It is preferable to have your child seated with access around his/her body
• Remove jewellery (bracelets/necklaces)
• Prepare clothing. Without causing irritation to the child pull up sleeves and if possible trouser legs.
• Remove shoes and socks
• Apply the DPPT (brushing) 6 - 8 times daily as directed, 1. Brush as demonstrated and practiced to the body - hands, arms, back, legs and feet. 2. Use only the therapressure brush given and keep pressure firm and consistent. 3. Immediately follow with joint compressions input as shown to shoulders, elbows, hands,
fingers, hips, knees, ankles and chest 4. if prescribed use oral techniques as shown at appropriate times
• Apply the oral technique if required directly before each meal/snack 1. using moderate touch sweep upper palette as shown 2. apply gentle proprioception down through the lower jaw as shown
• The protocol does not cause pain, if your child complains of pain check with your therapist before continuing.
• Do not brush over skin where there are cuts, sores or bites
• Never brush over stomach, groin or face
• If your child shows any unusual behaviour or symptoms please contact your therapist immediately (redness of the skin caused by skin pressure should go away in 10 minutes)
• Daily complete as many of the sensory diet activities as possible
• Complete daily record form as provided. Most interesting to note will be changes in behaviours related to alerted sleep patterns, ability to cope with changes in day to day schedules, more comfort moving around, ability to perform sensory activities without irritation or upset.
• Once you have begun the procedure do not stop, if you are interrupted start again from the beginning. Warning
� It is better not start the intervention than apply it incorrectly or less than the prescribed number of times.
� In some cases the child’s behaviour has got worse before it has got better. This generally occurs in the first 2 weeks of treatment. If this is the pattern for your child please persist as the long term benefits will be worth it. (Please speak to your therapist)
� Often, when a child’s coping pattern is to sleep more, expect that with recovery your child will sleep less, or in an age-appropriate way.
Contact Anoo Bhopti, Occupational Therapist, 0434317429 if any queries . References Therapressure Program ™ for treating Sensory Defensiveness. Patricia Wilbarger M.Ed. OTR. FAOTA Sensory Defensiveness A Comprehensive Treatment Approach Patricia Wilbarger and Julia Wilbarger PhD, OTR

133
Appendix 13: Pictures of demonstration page 2.
Brush along inside and outside of arm from shoulder to wrist x 10
Brush palm of hand x 10
Brush vertically from nape of neck to small of back x 10
Brush horizontally from nape of neck to small of back x 10

134
Appendix 14: Comments from parent/carers
Daily activities/routines Behaviours Family/
community
From questionnaire
Picked up clippers and put in hair
Seems a lot happier Allowed family to watch a new movie and shared the TV; would never do that
“The brushing has
allowed me to take
‘John’ to the shops and
other places which I
would avoid. But now
these activities have
become stress free”
Playing more sensibly with dolls
Lots of singing and dancing
Was very quiet at airport and Vic roads;....can’t believe it
“Information provided
was presented
thoroughly and I was
comfortable that I
understood the
program”
Can sit in stroller in shops for an hour and escalators are no problem now
No tantrums and listens to negotiations like, ‘if you want a boost juice you need to sit in the trolley’
Grandma noticed that he is much calmer
“I found having the day
run with a two hour
structure handy. It
reminded me to include
things for him to do in
regular blocks.”
Is using more words in Hindi and English
No tantrums during transitions
Changed his bedroom and both of us(parents) were dreading this as he loves his bed, but there was no fuss
“I found the follow up
and constant
communication very
reassuring.”
Doing really well at shopping centres
Seems more confident and less anxious
People have commented at kinder on “wow, what’s going on?”
“Unfortunately
‘Johnny’s’ cooperation
dwindled fairly quickly
and it became a battle to
have him participate”
Had a haircut on barber’s chair not my lap
Is tolerating other children and plays beside them at kinder
His speech pathologist was amazed at his eye contact
Is leaving clothes on, not running naked
He was wonderful on our holiday
Will spit out hot food and is recognising that it is hot
Sat on the swing with two other children at kinder
Talking more Sat for story time and all throughout ‘Old MacDonald had a farm’ song
Was scared of motorbikes, but last week got onto one
This week not so good, not allowing me to complete it

135
Loves the compressions and diet activities
No poo smearing at all after brushing
Doing a lot more pretend play
Knows hot/cold now
Is playing with play dough for 10 minutes
Not seeking his dummy
Sat in a mud puddle and was happy