Embed Size (px)
Citation preview

Excimer phototherapeutic keratectomy for corneal subepithelial cryoglobulin deposits
Israel Kremer, MD, Michael Blumenthal, MD
ABSTRACT
A 64-year-old man with a history of cryoglobulinemia and repeated scraping of immunoglobulin deposits from both superficial corneas presented with gradual decrease in vision and progressive hyperopia caused by circumferential redeposition of the cryoglobulins in his corneas. He had debridment of the deposits combined with phototherapeutic keratectomy to smooth the corneal surface. Visual acuity and reading capacity markedly improved, and hyperopia regressed by 5.75 diopters (D) in the right eye and 5.25 0 in the left. Follow-up was 3 years. J Cataract Refract Surg 1997; 23:1119-1121
Bilateral corneal immunoglobulin deposits in pa
tients with paraproteinemias and raised serum
level of a specific immunoglobulin fraction have been
recognized, albeit rarely, for many years·. l-4 Palm3 was
the first to report on superficial corneal deposits of
crystalline appearance in a case of cryoglobulinemia.
No surgical or medical treatment was suggested in these
two reports. l -4 We report the results of bilateral photo
therapeutic keratectomy (PTK) in a patient with cryo
globulin corneal deposits recurring several years after
mechanical keratectomy.
Case Report
A 64-year-old man presented with gradually decreasing vision, photophobia, and progressive hyperopia. On examination, uncorrected visual acuity (UCVA) was 6/120 in both eyes. Best corrected visual acuity (BCVA) was 6115( -) with a correction of +7.00 +2.00 X 45 in the right eye and 6/15( +) with a correction of +6.00 + 1.50 X 170 in the left
From Ein Tal Eye Center, Tel Aviv, Israel.
Reprint requests to Israel Kremer, MD, Department of Ophthalmology, Beilinson Medical Center, Petach Tikvah 49100, Israel.
eye. In both eyes, his reading capacity was J3, with a + 3.00 diopter (D) addition.
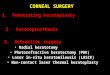
Two years before this examination, his BCVA was 61 12( +) with a correction of + 3.50 + 1.50 X 40 in the right eye and + 3.00 + 1.50 X 170 in the left eye. Slitlamp examination of both corneas showed gelatinous gray-white elevated subepithelial deposits, extending through 360 degrees. These confluent nodular masses also extended toward the center of the cornea in finger-like projections (Figure 1). They were much more elevated and their projections were closer to the visual axis than 2 years previously. The deeper corneal stroma, Descemet's layer, and endothelium appeared normal. The anterior and posterior segments were completely normal.
The patient had a history of essential monoclonal kappa-immunoglobulin G (IgG) cryoglobulinemia, and the corneal deposits were histologically proven to be subepithelial rod-shaped aggregates ofIgG.5 Eight years previously, he had had superficial keratectomy to remove all subepithelial deposits. 5 During the following years, these deposits recurred, increased in height, and extended toward the visual axis. Concurrently, the patient became hyperopic; the hyperopia gradually progressed while BCVA decreased.
In 1993, the patient had debridment of the subepithelial deposits and keratectomy with a Beaver blade after removal of the epithelium from all affected areas of the right cornea. Subsequently, several drops of artificial tears were applied to smooth the irregular stromal surface. A circular mode PTK
J CATARACT REFRACT SURG-VOL 23, SEPTEMBER 1997 1119

CASE REPORTS: KREMER
Figure 1. (Kremer) Slitlamp photograph of the patient's cornea showing elevated subepithelial opaque deposits extending from the periphery to the center.
was performed with multiple confluent rones of 4.0 mm diameter ablation while the patient's head was moved in a circular manner to obtain a circumferential, smooth, doughnut-like ablation. The estimated ablation depth through the entire treated area was 20 Jlm. The epithelium at the central 3.5 mm diameter rone of the cornea was left intact and was not ablated. The same procedure was repeated in the left eye.
One month after PTK in both eyes, the patient's UCVA improved to 6/12(-) in both eyes. His BCVA was 6/10(-) in the right eye with a correction of + 1.50 + 1.00 X 30 and 6/10( +) in the left eye with a correction of + 1.25 + 1.00 X
140. Twelve months after surgery, the patient's UCVA had slightly improved to 6112( +) in each eye; BCVA was 6/9( -) in the right eye with a correction of + 1.00 + 2.50 X 35 and 6/9( +) in the left eye with a correction of + 1.00 + 1.00 X
160. His reading capacity was J1 with an addition of +3.00 D.
Slitlamp biomicroscopy revealed a smooth epithelial surface with subepithelial, superficial stromal opacities occupying the circumferential zone where the IgG deposits were located and treated. The central corneal rone of 3.5 mm was clear. Two years later, the UCVA and BCVA were not changed, and the patient was free of symptoms.
Discussion
The therapeutic success of superficial excimer laser keratectomy relies on the cornea's ability to remain
smooth without subsequent iatrogenic scarring affecting the visual axis and to allow adequate epithelial regeneration and adherence to the new stromal surface.6-8 In patients in whom superficial corneal pathology decreases corneal clarity and causes surface irregu-
larity, the smoothing technique appears effective in increasing visual acuity and decreasing light scattering and ocular surface discomfort. These benefits appear to result from regularization of the corneal surface and restoration of central corneal clarity. 8
In corneal disorders in which the superficial pathologic tissue is resistant to excimer laser ablation9 or there are dense deposits of abnormal material such as in band keratopathy9.10 or in paraproteinemia, PTK must be
combined with mechanical superficial keratectomy. Mter epithelial removal, the cleavage plane between the abnormal tissue and superficial stroma must be identified by blunt dissection. The abnormal tissue can then be dissected from the stroma and PTK subsequently performed.
With regard to the effect of treatment on our patient's hyperopia induced by the circumferential IgG deposits, PTK in general has the potential to induce refractive errors after removal of anterior corneal pathology. Relatively greater ablation of the abnormal tissue in the central cornea will cause central flattening and refractive shift in the hyperopic direction, which may at times reach 7.00 0. 10
In contrast, greater ablation in the peripheral and pericentral cornea will induce relative central steepening and a refractive change in the myopic direction, as we find in hyperopic PRK.ll If the preoperative refractive error is hyperopic, as in our patient, the refractive
shift may reach emmetropia. Our patient had progressive hyperopia within a period of several years during which the peripheral and midperipheral subepithelial IgG deposits increased in volume, elevating the overlying epithelium so that they created a central surface concavity within a midperipheral and peripheral circumferential elevation. Thus, the dioptric power of the patient's central cornea decreased significantly, and he developed progressive hyperopia up to a spherical equivalent of 8.000 in the right eye and 6.75 D in the left.
Mechanical keratectomy, followed by circular midperipheral PTK of 20 /Jffi of the underlying stroma, created relative central corneal steepening and resulted in a marked decrease in the patient's hyperopia. This refractive effect of PTK lasted for 3 years, and penetrating or lamellar keratoplasty could be deferred for several years. If these IgG deposits recur in the future and the patient becomes symptomatic, PTK may be repeated. In the future, we may also consider using plasmapher-
1120 J CATARACT REFRACT SURG-VOL 23. SEPTEMBER 1997

CASE REPORTS: KREMER
esis or low-dosage chemotherapy to reduce the high level of serum IgG, preventing further deposition of the cryoglobulin in the superficial corneal stroma.
References
1. Allansmith MR, McClellan BH. Immunoglobulins in the human cornea. Am J Ophthalmol 1975; 80:123-132
2. Ormerod LD, Collin HB, Dohlman CH, et al. Paraproteinemic crystalline keratopathy. Ophthalmology 1988; 95:202-212
3. Palm E. A case of crystal deposits in the cornea. Precipitation of a spontaneously crystallizing plasma globulin. Acta Ophthalmol 1947; 25:165-174
4. Oglesby RB. Corneal opacities in a patient with cryoglobulinemia and reticulohistiocytosis. Arch Ophthalmol 1961; 65:63-66
5. Kremer I, Wright P, Merin S, et al. Corneal subepithelial
monoclonal kappa IgG deposits in essential cryoglobulinaemia. Br J Ophthalmol 1989; 73:669-673
6. Stark Wl, Chamon W, Kamp MT, et al. Clinical followup of 193-nm ArF excimer laser photokeratectomy. Ophthalmology 1992; 99:805-812
7. Gartry 0, Kerr Muir M, Marshall J. Excimer laser treatment of corneal surface pathology: a laboratory and clinical study. Br J Ophthalmol 1991; 75:258-269
8. Talamo JH, Steinert RF, Puliafito CA. Clinical strategies for excimer laser therapeutic keratectomy. J Refract Corneal Surg 1992; 8:319-324
9. McOonnellJM, GarbusJJ, McDonnell PJ. Unsuccessful excimer laser photo therapeutic keratectomy; clinicopathologic correlation. Arch OphthalmoI1992; 110:977-979
10. Fagerholm P, Fitzsimmons TO, Orndahl M, et al. Phototherapeutic keratectomy: long-term results in 166 eyes. Refract Corneal Surg 1993; 9(suppl):S76-S81
11. Oausch 0, Klein R. Schroder E. Excimer laser photorefractive keratectomy for hyperopia. Refract Corneal Surg 1993; 9:20-28
J CATARACf REFRACf SURG-VOL 23, SEPTEMBER 1997 1121






![Fu abutment stabilization technique (FAST): A simple ...Subepithelial connective tissue graft (CTG) [24-27] Subepithelial Connective Tissue Graft (CTG) is commonly harvested from the](https://img.pdfslide.net/doc/110x75/601a275155ed9c309b1586a7/fu-abutment-stabilization-technique-fast-a-simple-subepithelial-connective.jpg)





















