Embed Size (px)
Citation preview
The PDF of the article you requested follows this cover page.
This is an enhanced PDF from The Journal of Bone and Joint Surgery
2007;89:979-986. doi:10.2106/JBJS.F.00440 J Bone Joint Surg Am.Patrick J. O'Neill, Brent G. Parks, Russell Walsh, Lucia M. Simmons and Stuart D. Miller
Ankle SprainExcursion and Strain of the Superficial Peroneal Nerve During Inversion
This information is current as of May 11, 2007
Reprints and Permissions
Permissions] link. and click on the [Reprints andjbjs.orgarticle, or locate the article citation on
to use material from thisorder reprints or request permissionClick here to
Publisher Information
www.jbjs.org20 Pickering Street, Needham, MA 02492-3157The Journal of Bone and Joint Surgery
COPYRIGHT © 2007 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED
979
Excursion and Strain of the Superficial Peroneal Nerve
During Inversion Ankle SprainBy Patrick J. O’Neill, MD, Brent G. Parks, MSc, Russell Walsh, BSc,
Lucia M. Simmons, BSc, and Stuart D. Miller, MD
Investigation performed at the Department of Orthopaedic Surgery, Union Memorial Hospital, Baltimore, Maryland
Background: Traction is presumed to be the mechanism of injury to the superficial peroneal nerve in an inversion an-kle sprain, but it is not known whether the amount of strain caused by nerve traction is sufficient to cause nerve in-jury. We hypothesized that the superficial peroneal nerve would experience significant excursion and strain during asimulated inversion sprain, that sectioning of the anterior talofibular ligament would increase excursion and strain,and that an impact force would produce strain in a range that can structurally alter the nerve.
Methods: Differential reluctance transducers were placed in the superficial peroneal nerve in sixteen lower-extremitycadaver specimens to measure excursion and strain in situ. Static weight was applied to the foot in increments start-ing at 0.454 kg and ending at 4.54 kg. The anterior talofibular ligament was sectioned, and the measurements wererepeated. A final impact force of 4.54 kg was applied to each specimen. Two-way repeated-measures analysis of vari-ance was used to evaluate differences in excursion and strain.
Results: The mean excursion and strain of the superficial peroneal nerve increased with increases in the appliedweight in both the group with the intact anterior talofibular ligament and the group in which it had been sectioned.Nerve excursion was greater in the sectioned-ligament group than in the intact-ligament group with all applied weights(p < 0.05). The mean nerve strain was greater in the sectioned-ligament group (range, 5.5% to 12.9%) than in the in-tact-ligament group (range, 3.0% to 11.6%) with application of the 0.454, 0.908, 1.362, and 1.816-kg weights (p <0.05). With the ligament sectioned, the 4.54-kg impact force produced significantly higher mean nerve excursion andstrain than did the 4.54-kg static weight (p < 0.05).
Conclusions: The magnitude of strain with the impact force was in the lower range of values that have been shownto structurally alter peripheral nerves. The superficial peroneal nerve is at risk for traction injury during an ankle inver-sion sprain and is at additional risk with more severe sprains or with an insufficient anterior talofibular ligament.
Clinical Relevance: Nerve injury may contribute to the high rate of residual morbidity after inversion ankle sprains.
nversion ankle sprains are extremely common, estimatedto occur once per 10,000 people every day1-3, and they arethe most common injuries in sports4-6. Up to 40% of pa-
tients who sustain an inversion ankle sprain have residualsymptoms7-11. A potential cause of chronic morbidity is in-jury to the tibial nerve or to the common peroneal nerve or
its branches12-22. Clinical manifestations of nerve injury in-clude gastrocnemius or peroneal weakness, paresthesias, an-terolateral ankle pain, instability, and local tenderness withburning13,15,19,20,23-25.
Electrophysiologic studies that have shown nerve ab-normalities after inversion ankle sprains have substantiated
I
Disclosure: The authors did not receive any outside funding or grants in support of their research for or preparation of this work. Neither they nor amember of their immediate families received payments or other benefits or a commitment or agreement to provide such benefits from a commercialentity. No commercial entity paid or directed, or agreed to pay or direct, any benefits to any research fund, foundation, division, center, clinical prac-tice, or other charitable or nonprofit organization with which the authors, or a member of their immediate families, are affiliated or associated.
J Bone Joint Surg Am. 2007;89:979-86 • doi:10.2106/JBJS.F.00440
ONeill.fm Page 979 Wednesday, April 11, 2007 2:44 PM
980
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LU M E 89-A · NU M B ER 5 · MAY 2007EXCU RS I ON A N D ST R AI N OF T H E SU P E R F I CI A L PE RO N E A L NER VE DUR I N G INVERS I ON AN K LE SP R A I N
the clinical findings17,20,22,26. Using electromyographic measure-ments, Nitz et al. found that 86% of patients with a more se-vere ankle sprain had a peroneal nerve injury and 83% had atibial nerve injury20. Other studies have demonstrated markedelectromyographic or nerve-conduction abnormalities in thedeep peroneal nerve, superficial peroneal nerve, or commonperoneal nerve after inversion ankle sprains17,19,22,26.
The mechanism of nerve injury around the ankle maybe traction, as has been suggested by previous investiga-tors17,20,21,25. However, we are not aware of any biomechanicalstudies that have established that nerves around the ankle ex-perience strain during an ankle inversion sprain. Also, it is notknown whether the amount of strain produced by an ankle in-version sprain would reach a threshold level sufficient to resultin nerve injury. Additionally, there is a lack of evidence regard-ing the amount of excursion experienced by the nerves aroundthe ankle during inversion sprains. Previous studies of periph-eral nerves have shown histological or functional alterationsoccurring at between 6% and 50% strain27-33. Loading studieshave determined that the elastic limit of peripheral nerves isreached with strains of 8% to 21%28,32,34.
Because of its anterolateral position, the superficial per-oneal nerve appears to be vulnerable to excursion and stretchinjury during an inversion ankle sprain. Furthermore, moresevere ankle sprains often include injury to the anteriortalofibular ligament, an important lateral stabilizing structure.Rupture of the anterior talofibular ligament would be ex-pected to lead to increased ankle motion with an increase inexcursion and strain in the superficial peroneal nerve withequal forces applied to the foot.
The purpose of this study was to evaluate excursion andstrain of the superficial peroneal nerve during simulated in-version ankle sprains. The hypotheses were that the nervewould experience significant excursion and strain, sectioningof the anterior talofibular ligament would increase excursionand strain, and an impact force would produce strain in arange that has been shown to structurally alter peripheralnerves.
Materials and Methodsixteen lower extremities from fresh-frozen cadavers wereused for the study. None of the samples had signs of previ-
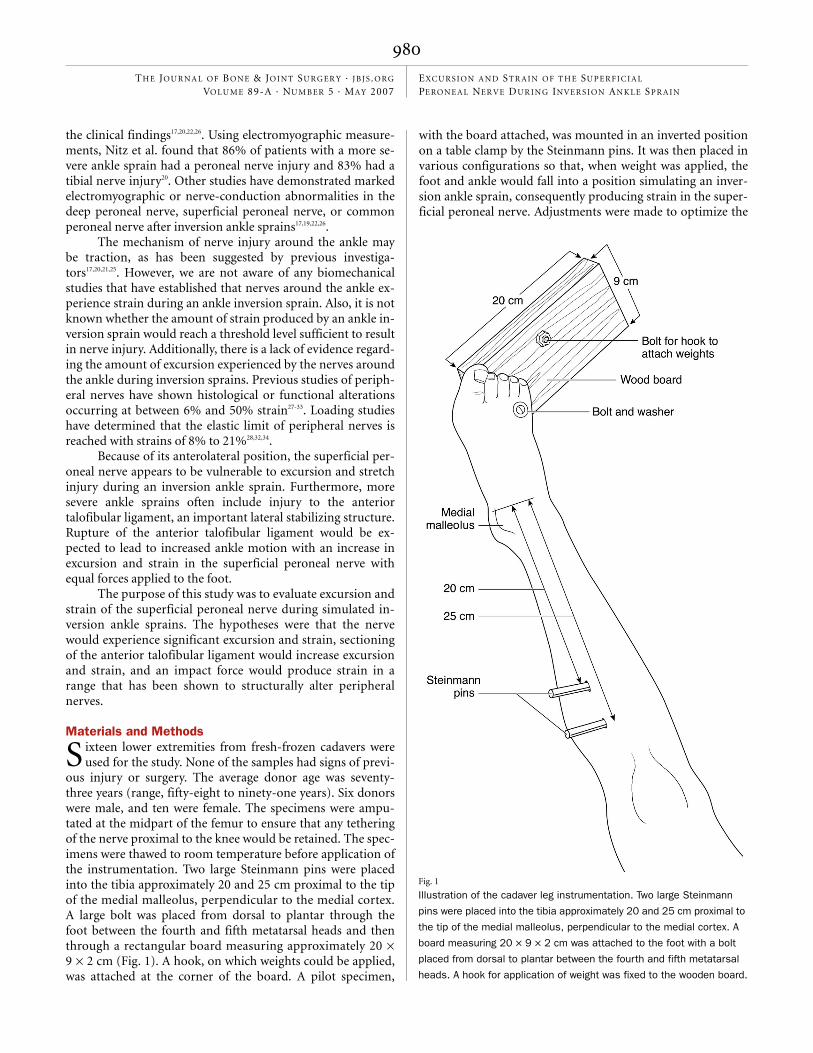
ous injury or surgery. The average donor age was seventy-three years (range, fifty-eight to ninety-one years). Six donorswere male, and ten were female. The specimens were ampu-tated at the midpart of the femur to ensure that any tetheringof the nerve proximal to the knee would be retained. The spec-imens were thawed to room temperature before application ofthe instrumentation. Two large Steinmann pins were placedinto the tibia approximately 20 and 25 cm proximal to the tipof the medial malleolus, perpendicular to the medial cortex.A large bolt was placed from dorsal to plantar through thefoot between the fourth and fifth metatarsal heads and thenthrough a rectangular board measuring approximately 20 ×9 × 2 cm (Fig. 1). A hook, on which weights could be applied,was attached at the corner of the board. A pilot specimen,
with the board attached, was mounted in an inverted positionon a table clamp by the Steinmann pins. It was then placed invarious configurations so that, when weight was applied, thefoot and ankle would fall into a position simulating an inver-sion ankle sprain, consequently producing strain in the super-ficial peroneal nerve. Adjustments were made to optimize the
S
Fig. 1
Illustration of the cadaver leg instrumentation. Two large Steinmann
pins were placed into the tibia approximately 20 and 25 cm proximal to
the tip of the medial malleolus, perpendicular to the medial cortex. A
board measuring 20 × 9 × 2 cm was attached to the foot with a bolt
placed from dorsal to plantar between the fourth and fifth metatarsal
heads. A hook for application of weight was fixed to the wooden board.
ONeill.fm Page 980 Wednesday, April 11, 2007 2:44 PM
981
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LU M E 89-A · NU M B ER 5 · MAY 2007EXCU RS I ON A N D ST R AI N OF T H E SU P E R F I CI A L PE RO N E A L NER VE DUR I N G INVERS I ON AN K LE SP R A I N
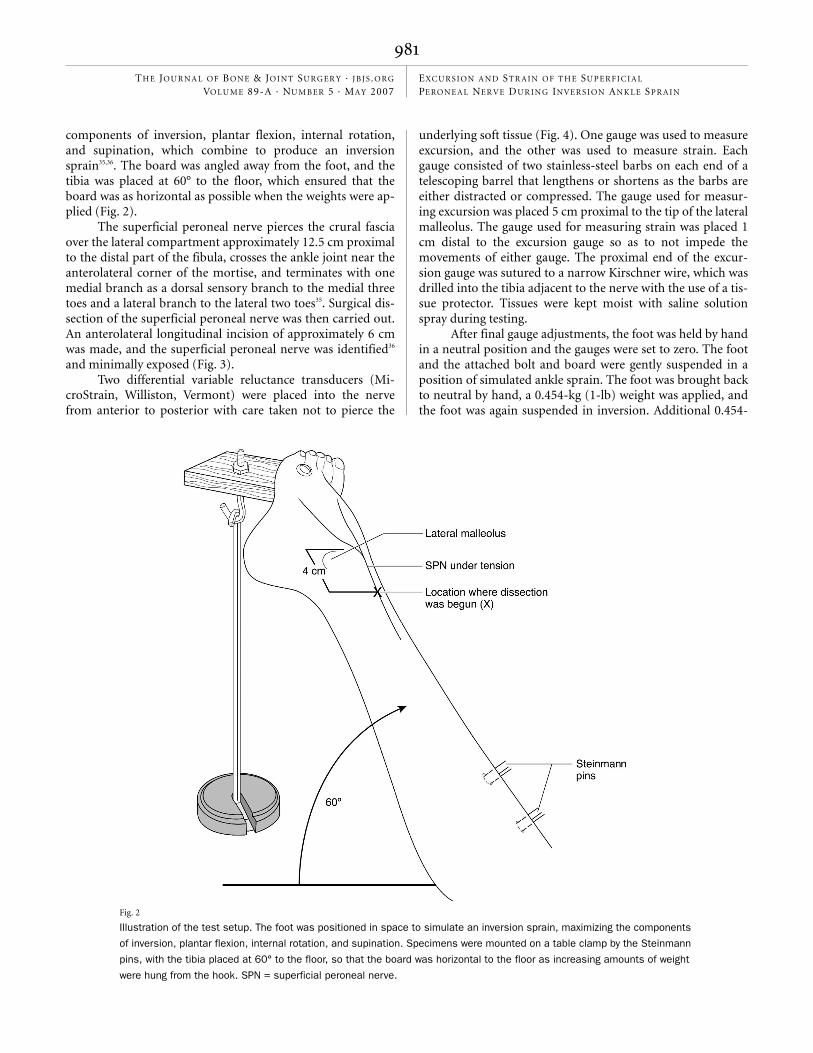
components of inversion, plantar flexion, internal rotation,and supination, which combine to produce an inversionsprain35,36. The board was angled away from the foot, and thetibia was placed at 60° to the floor, which ensured that theboard was as horizontal as possible when the weights were ap-plied (Fig. 2).
The superficial peroneal nerve pierces the crural fasciaover the lateral compartment approximately 12.5 cm proximalto the distal part of the fibula, crosses the ankle joint near theanterolateral corner of the mortise, and terminates with onemedial branch as a dorsal sensory branch to the medial threetoes and a lateral branch to the lateral two toes35. Surgical dis-section of the superficial peroneal nerve was then carried out.An anterolateral longitudinal incision of approximately 6 cmwas made, and the superficial peroneal nerve was identified36
and minimally exposed (Fig. 3).Two differential variable reluctance transducers (Mi-
croStrain, Williston, Vermont) were placed into the nervefrom anterior to posterior with care taken not to pierce the
underlying soft tissue (Fig. 4). One gauge was used to measureexcursion, and the other was used to measure strain. Eachgauge consisted of two stainless-steel barbs on each end of atelescoping barrel that lengthens or shortens as the barbs areeither distracted or compressed. The gauge used for measur-ing excursion was placed 5 cm proximal to the tip of the lateralmalleolus. The gauge used for measuring strain was placed 1cm distal to the excursion gauge so as to not impede themovements of either gauge. The proximal end of the excur-sion gauge was sutured to a narrow Kirschner wire, which wasdrilled into the tibia adjacent to the nerve with the use of a tis-sue protector. Tissues were kept moist with saline solutionspray during testing.
After final gauge adjustments, the foot was held by handin a neutral position and the gauges were set to zero. The footand the attached bolt and board were gently suspended in aposition of simulated ankle sprain. The foot was brought backto neutral by hand, a 0.454-kg (1-lb) weight was applied, andthe foot was again suspended in inversion. Additional 0.454-
Fig. 2
Illustration of the test setup. The foot was positioned in space to simulate an inversion sprain, maximizing the components
of inversion, plantar flexion, internal rotation, and supination. Specimens were mounted on a table clamp by the Steinmann
pins, with the tibia placed at 60° to the floor, so that the board was horizontal to the floor as increasing amounts of weight
were hung from the hook. SPN = superficial peroneal nerve.
ONeill.fm Page 981 Wednesday, April 11, 2007 2:44 PM
982
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LU M E 89-A · NU M B ER 5 · MAY 2007EXCU RS I ON A N D ST R AI N OF T H E SU P E R F I CI A L PE RO N E A L NER VE DUR I N G INVERS I ON AN K LE SP R A I N
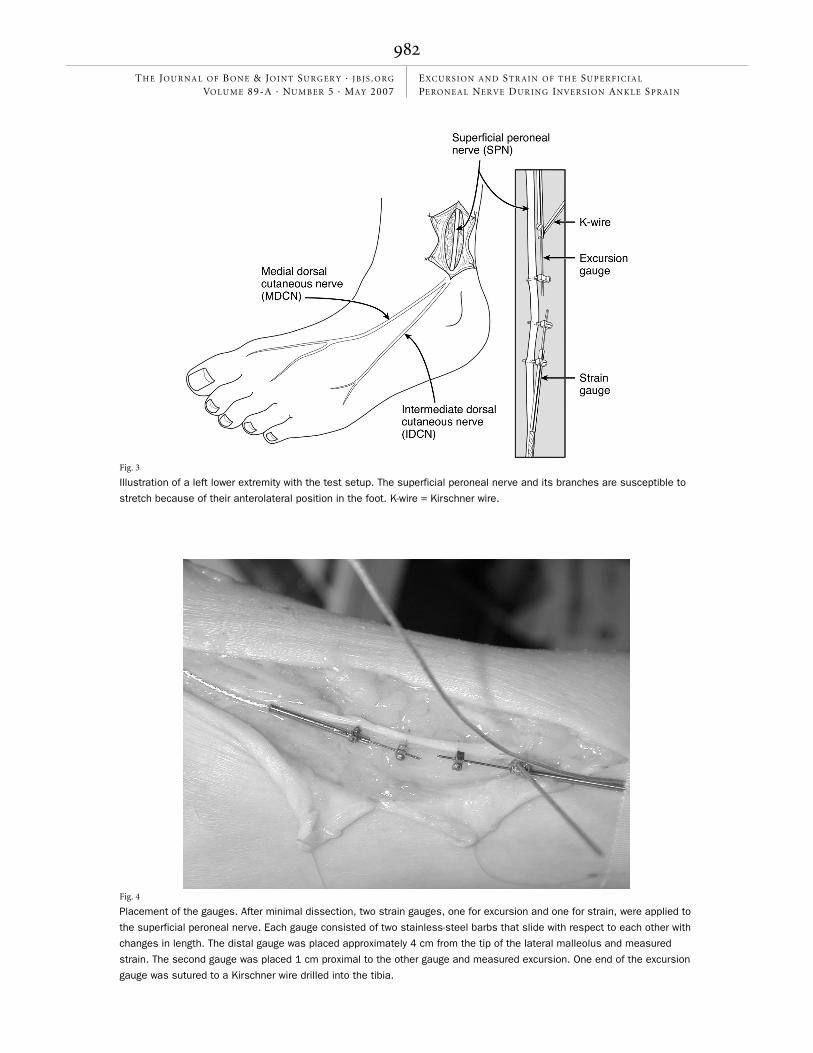
Fig. 3
Illustration of a left lower extremity with the test setup. The superficial peroneal nerve and its branches are susceptible to
stretch because of their anterolateral position in the foot. K-wire = Kirschner wire.
Fig. 4
Placement of the gauges. After minimal dissection, two strain gauges, one for excursion and one for strain, were applied to
the superficial peroneal nerve. Each gauge consisted of two stainless-steel barbs that slide with respect to each other with
changes in length. The distal gauge was placed approximately 4 cm from the tip of the lateral malleolus and measured
strain. The second gauge was placed 1 cm proximal to the other gauge and measured excursion. One end of the excursion
gauge was sutured to a Kirschner wire drilled into the tibia.
ONeill.fm Page 982 Wednesday, April 11, 2007 2:44 PM
983
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LU M E 89-A · NU M B ER 5 · MAY 2007EXCU RS I ON A N D ST R AI N OF T H E SU P E R F I CI A L PE RO N E A L NER VE DUR I N G INVERS I ON AN K LE SP R A I N
kg weights were applied successively at intervals of approxi-mately five seconds, up to 4.54 kg (10 lb). Gauge lengths wereelectronically recorded continuously throughout the testing ofeach specimen with use of LabVIEW software (National In-struments, Austin, Texas). The position of each gauge was alsodisplayed on a computer monitor. After each weight was re-moved and the foot was brought back to neutral by hand, thecomputer display was used to ensure that the gauges had re-turned to the zero starting point. This first set of data for eachspecimen represented the intact-ligament group. The amountsof weight that were used were based on pilot testing of theconstruct. Using approximately 15% strain as the elastic limitof peripheral nerves28,32,34, we chose a maximum test weight(4.54 kg) that produced a strain of approximately 10% to 12%to avoid injuring the nerve after repeated measures.
The anterior talofibular ligament was then surgicallysectioned, and the weights were again applied in 0.454-kg in-crements up to 4.54 kg. This group of data represented thesectioned-ligament group. Finally, the foot was again broughtback to neutral, the 4.54-kg weight was attached to the hook,and the construct was released in a free fall until it wasstopped by the structures of the ankle. This relatively largesudden force was applied to more closely approximate themechanism of a true ankle sprain. The impact force was nottested with the anterior talofibular ligament intact to avoid ir-reversible deformation of the nerve before testing with the an-terior talofibular ligament sectioned.
Excursion and strain data were analyzed with SPSS sta-
tistical software (SPSS, Chicago, Illinois). Two-way repeated-measures analysis of variance was used to compare the meanexcursion and strain between all ankles with the anteriortalofibular ligament intact and all ankles with the anteriortalofibular ligament sectioned in each weight group. In addi-tion, in the sectioned-ligament group, the mean excursion andstrain caused by the 4.54-kg impact were compared with themean excursion and strain caused by the 4.54-kg static weight.
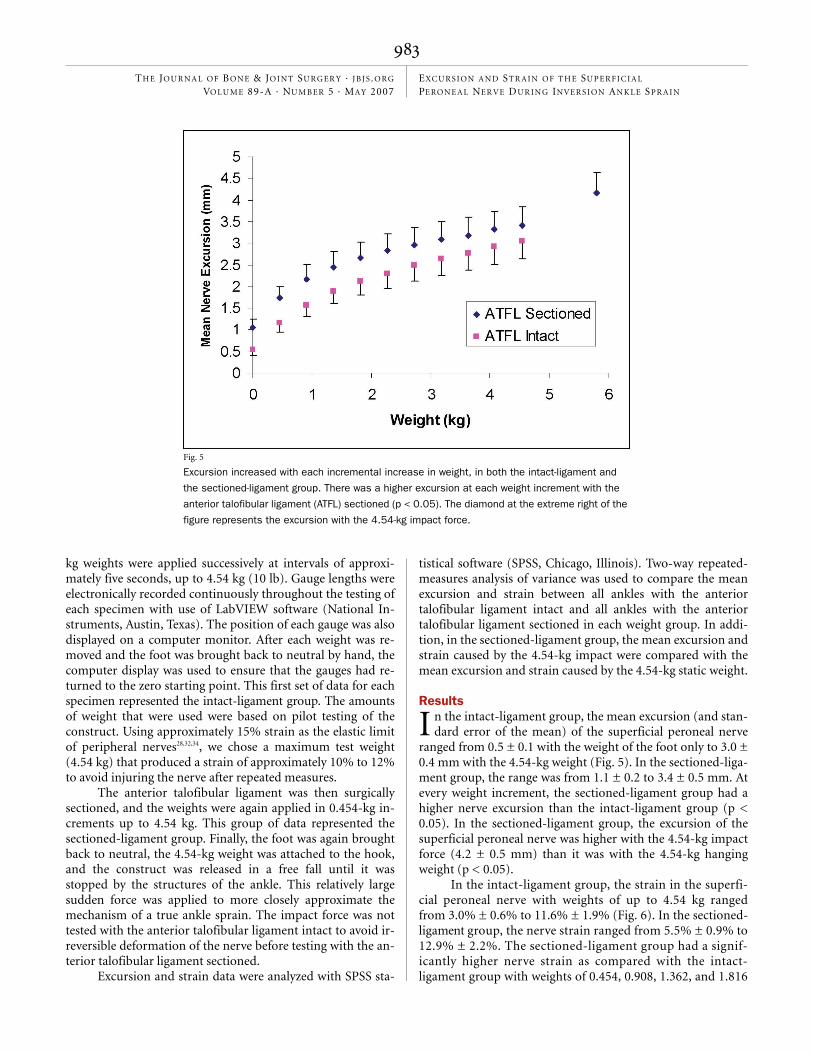
Resultsn the intact-ligament group, the mean excursion (and stan-dard error of the mean) of the superficial peroneal nerve
ranged from 0.5 ± 0.1 with the weight of the foot only to 3.0 ±0.4 mm with the 4.54-kg weight (Fig. 5). In the sectioned-liga-ment group, the range was from 1.1 ± 0.2 to 3.4 ± 0.5 mm. Atevery weight increment, the sectioned-ligament group had ahigher nerve excursion than the intact-ligament group (p <0.05). In the sectioned-ligament group, the excursion of thesuperficial peroneal nerve was higher with the 4.54-kg impactforce (4.2 ± 0.5 mm) than it was with the 4.54-kg hangingweight (p < 0.05).
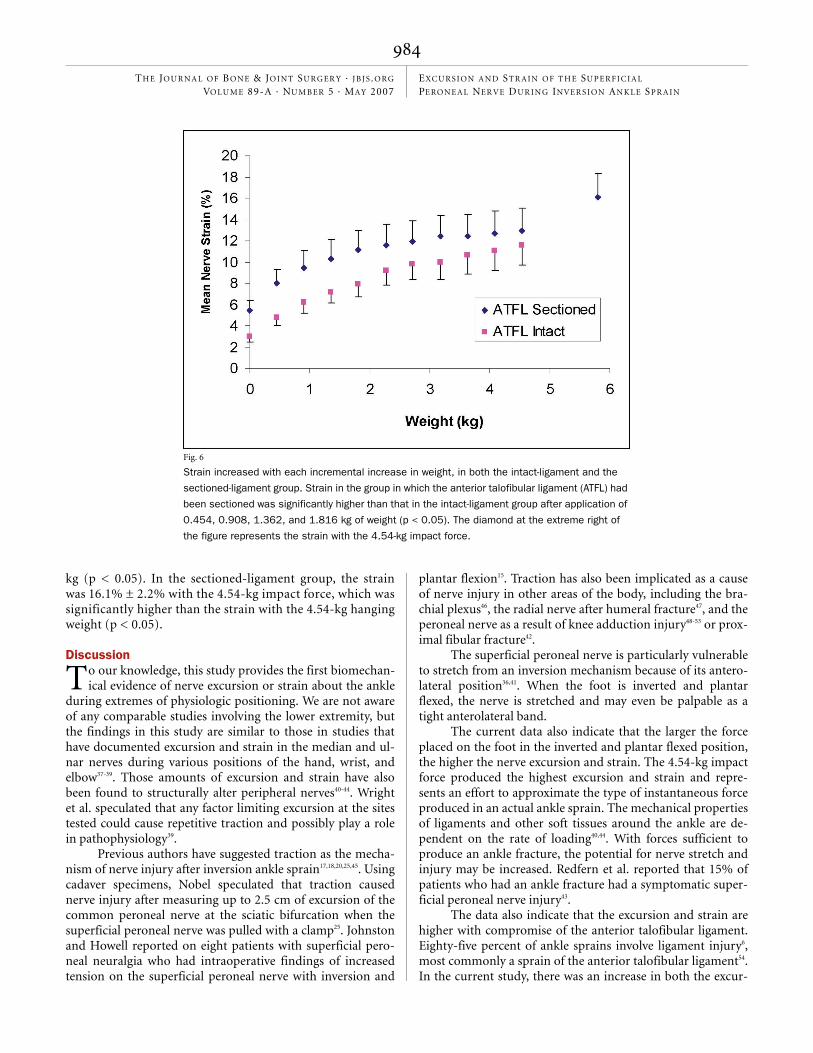
In the intact-ligament group, the strain in the superfi-cial peroneal nerve with weights of up to 4.54 kg rangedfrom 3.0% ± 0.6% to 11.6% ± 1.9% (Fig. 6). In the sectioned-ligament group, the nerve strain ranged from 5.5% ± 0.9% to12.9% ± 2.2%. The sectioned-ligament group had a signif-icantly higher nerve strain as compared with the intact-ligament group with weights of 0.454, 0.908, 1.362, and 1.816
I
Fig. 5
Excursion increased with each incremental increase in weight, in both the intact-ligament and
the sectioned-ligament group. There was a higher excursion at each weight increment with the
anterior talofibular ligament (ATFL) sectioned (p < 0.05). The diamond at the extreme right of the
figure represents the excursion with the 4.54-kg impact force.
ONeill.fm Page 983 Wednesday, April 11, 2007 2:44 PM
984
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LU M E 89-A · NU M B ER 5 · MAY 2007EXCU RS I ON A N D ST R AI N OF T H E SU P E R F I CI A L PE RO N E A L NER VE DUR I N G INVERS I ON AN K LE SP R A I N
kg (p < 0.05). In the sectioned-ligament group, the strainwas 16.1% ± 2.2% with the 4.54-kg impact force, which wassignificantly higher than the strain with the 4.54-kg hangingweight (p < 0.05).
Discussiono our knowledge, this study provides the first biomechan-ical evidence of nerve excursion or strain about the ankle
during extremes of physiologic positioning. We are not awareof any comparable studies involving the lower extremity, butthe findings in this study are similar to those in studies thathave documented excursion and strain in the median and ul-nar nerves during various positions of the hand, wrist, andelbow37-39. Those amounts of excursion and strain have alsobeen found to structurally alter peripheral nerves40-44. Wrightet al. speculated that any factor limiting excursion at the sitestested could cause repetitive traction and possibly play a rolein pathophysiology39.
Previous authors have suggested traction as the mecha-nism of nerve injury after inversion ankle sprain17,18,20,25,45. Usingcadaver specimens, Nobel speculated that traction causednerve injury after measuring up to 2.5 cm of excursion of thecommon peroneal nerve at the sciatic bifurcation when thesuperficial peroneal nerve was pulled with a clamp25. Johnstonand Howell reported on eight patients with superficial pero-neal neuralgia who had intraoperative findings of increasedtension on the superficial peroneal nerve with inversion and
plantar flexion15. Traction has also been implicated as a causeof nerve injury in other areas of the body, including the bra-chial plexus46, the radial nerve after humeral fracture47, and theperoneal nerve as a result of knee adduction injury48-53 or prox-imal fibular fracture42.
The superficial peroneal nerve is particularly vulnerableto stretch from an inversion mechanism because of its antero-lateral position36,41. When the foot is inverted and plantarflexed, the nerve is stretched and may even be palpable as atight anterolateral band.
The current data also indicate that the larger the forceplaced on the foot in the inverted and plantar flexed position,the higher the nerve excursion and strain. The 4.54-kg impactforce produced the highest excursion and strain and repre-sents an effort to approximate the type of instantaneous forceproduced in an actual ankle sprain. The mechanical propertiesof ligaments and other soft tissues around the ankle are de-pendent on the rate of loading40,44. With forces sufficient toproduce an ankle fracture, the potential for nerve stretch andinjury may be increased. Redfern et al. reported that 15% ofpatients who had an ankle fracture had a symptomatic super-ficial peroneal nerve injury43.
The data also indicate that the excursion and strain arehigher with compromise of the anterior talofibular ligament.Eighty-five percent of ankle sprains involve ligament injury6,most commonly a sprain of the anterior talofibular ligament54.In the current study, there was an increase in both the excur-
T
Fig. 6
Strain increased with each incremental increase in weight, in both the intact-ligament and the
sectioned-ligament group. Strain in the group in which the anterior talofibular ligament (ATFL) had
been sectioned was significantly higher than that in the intact-ligament group after application of
0.454, 0.908, 1.362, and 1.816 kg of weight (p < 0.05). The diamond at the extreme right of
the figure represents the strain with the 4.54-kg impact force.
ONeill.fm Page 984 Wednesday, April 11, 2007 2:44 PM

985
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LU M E 89-A · NU M B ER 5 · MAY 2007EXCU RS I ON A N D ST R AI N OF T H E SU P E R F I CI A L PE RO N E A L NER VE DUR I N G INVERS I ON AN K LE SP R A I N
sion and the strain of the nerve after the anterior talofibularligament was sectioned. Previous studies have documentedthe importance of the anterior talofibular ligament as a stabi-lizer against inversion injury41,55. Thus, injury to this importantstabilizing structure may lead to higher nerve strain and in-creased morbidity.
Peripheral nerves may be injured when they are stretchedbeyond their physiologic limits. Previous studies have shownfunctional impairment, arrest of blood flow, and structuraldamage with as little as 15% strain27,28,30,31,49,56,57. A study of humanperipheral nerves by Sunderland and Bradley showed the elasticlimit to be at 8% to 21% strain with mechanical failure occur-ring at 10% to 32% strain34. Other studies have documentednerve damage with strains of 12% to 50%29,32,33. The mean strainof 16% produced by the relatively small 4.54-kg impact force inthe current study is in the lower range of values that have beenshown to structurally alter peripheral nerves40-44. The weightsplaced in this study were small compared with those experi-enced in a traumatic inversion ankle sprain with full bodyweight. This suggests that the superficial peroneal nerve may beat risk during actual ankle sprains.
Given the substantial strain measured in this study andthe fact that 90% of ankle sprains are caused by an inversionmechanism54,58, it is interesting that nerve injury is not morecommonly reported. This may be due to anatomic variationsor to the lack of active muscular protection in cadaver speci-mens. Alternatively, as previous authors have suggested19,20,50,59,nerve injury may actually be relatively common. The true in-cidence of nerve injuries may be underestimated if they aremasked by the acute pain of an ankle sprain or the longer-term morbidity of a ligament injury19,50,59. Nitz et al. observedelectrophysiologic changes in the peroneal nerve in >80% ofpatients with a severe ankle sprain20. Kleinrensink et al. foundthat the mean conduction velocity of the superficial peronealnerve was acutely decreased after an inversion ankle sprain butreturned to normal in five weeks17. Slowed conduction velocitymay contribute to functional instability, a common cause ofmorbidity after an inversion ankle sprain17,20,22,60 that is foundin up to 40% of patients13,61. Functional instability may becaused by a loss of proprioceptive reflexes or decreased sensa-tion, which may result from nerve injury20,22,60-62. Chronic dis-ability may also be caused by weakness resulting from injuryto the superficial or deep peroneal nerve13,14,19.
Normal peripheral nerve function may be compromisedif excursion is not adequate during normal motion. Decreasedexcursion due to tethering may result in higher strains. Severalprevious studies have demonstrated improved excursion andclinical findings following surgical release of nerve fibrosis orsoft-tissue tethers in patients with superficial peroneal neural-gia due to an inversion ankle sprain12,15,16,21,63,64. In the upper ex-tremity, it was found that ulnar nerve strain at the elbow withflexion ranged from 0% to 14% and that increased ulnar nervestrain at the elbow was caused by various amounts of tether-ing65. In the current study, some nerves appeared qualitativelyto be much more naturally tethered than others, and addi-tional study of this phenomenon may be warranted.
Weaknesses of this study include the use of fresh-frozencadaver limbs, in which the properties of the nerves and softtissues may differ from those of in vivo specimens. In addi-tion, although dissection of the nerves was held to a mini-mum, the exposure could have altered their behavior. Also, thespecimens were created by midfemoral amputation, whichmay alter the amount of excursion or strain. The specimensused were from elderly donors, whose anatomy or soft-tissuemechanical properties may differ from those of younger indi-viduals. The biomechanical model of the current study alsomay not precisely recreate the biomechanics of a true injurywith regard to either the magnitude or the direction of forcesapplied. Finally, sectioning of only the anterior talofibular lig-ament may not simulate the actual injury pattern of a severeinversion ankle sprain.
This study provided biomechanical evidence of excur-sion and strain produced in a nerve around the ankle in an ex-treme physiologic position. The observation of strain supportsthe possibility that superficial peroneal nerve injury could becaused by an inversion ankle sprain.
Patrick J. O’Neill, MDBrent G. Parks, MScRussell Walsh, BScLucia M. Simmons, BScStuart D. Miller, MDUnion Memorial Orthopaedics, The Johnston Professional Building, #400, 3333 North Calvert Street, Baltimore, MD 21218. E-mail address for S.D. Miller (c/o Lyn Camire, Editor): [email protected]
References
1. Brooks SC, Potter BT, Rainey JB. Treatment for partial tears of the lateral ligament of the ankle: a prospective trial. Br Med J (Clin Res Ed). 1981;282:606-7.
2. McCulloch PG, Holden P, Robson DJ, Rowley DI, Norris SH. The value of mobili-sation and non-steroidal anti-inflammatory analgesia in the management of inver-sion injuries of the ankle. Br J Clin Pract. 1985;39:69-72.
3. Ruth CJ. The surgical treatment of injuries of the fibular collateral ligaments of the ankle. J Bone Joint Surg Am. 1961;43:229-39.
4. Kannus P, Renstrom P. Treatment for acute tears of the lateral ligaments of the ankle. Operation, cast, or early controlled mobilization. J Bone Joint Surg Am. 1991;73:305-12.
5. Sammarco GJ, DiRaimondo CV. Surgical treatment of lateral ankle instability syndrome. Am J Sports Med. 1988;16:501-11.
6. Garrick JG, Requa RK. The epidemiology of foot and ankle injuries in sports. Clin Sports Med. 1988;7:29-36.
7. Anderson ME. Reconstruction of the lateral ligaments of the ankle using the plantaris tendon. J Bone Joint Surg Am. 1985;67:930-4.
8. Freeman MA. Instability of the foot after injuries to the lateral ligament of the ankle. J Bone Joint Surg Br. 1965;47:669-77.
9. Gerber JP, Williams GN, Scoville CR, Arciero RA, Taylor DC. Persistent dis-ability associated with ankle sprains: a prospective examination of an ath-letic population. Foot Ankle Int. 1998;19:653-60.
10. Schaap GR, de Keizer G, Marti K. Inversion trauma of the ankle. Arch Orthop Trauma Surg. 1989;108:273-5.
11. Staples OS. Result study of ruptures of lateral ligaments of the ankle. Clin Orthop Relat Res. 1972;85:50-8.
ONeill.fm Page 985 Wednesday, April 11, 2007 2:44 PM
986
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LU M E 89-A · NU M B ER 5 · MAY 2007EXCU RS I ON A N D ST R AI N OF T H E SU P E R F I CI A L PE RO N E A L NER VE DUR I N G INVERS I ON AN K LE SP R A I N
12. Acus RW 3rd, Flanagan JP. Perineural fibrosis of superficial peroneal nerve complicating ankle sprain: a case report. Foot Ankle. 1991;11:233-5. Comment in: Foot Ankle. 1991;11:414.
13. Bosien WR, Staples OS, Russell SW. Residual disability following acute ankle sprains. J Bone Joint Surg Am. 1955;37:1237-43.
14. Hyslop GH. Injuries to the deep and superficial peroneal nerves compli-cating ankle sprain. Am J Surg. 1941;51:436-8.
15. Johnston EC, Howell SJ. Tension neuropathy of the superficial peroneal nerve: associated conditions and results of release. Foot Ankle Int. 1999;20:576-82.
16. Kernohan J, Levack B, Wilson JN. Entrapment of the superficial peroneal nerve. Three case reports. J Bone Joint Surg Br. 1985;67:60-1.
17. Kleinrensink GJ, Stoeckart R, Meulstee J, Kaulesar Sukul DM, Vleeming A, Snijders CJ, van Noort A. Lowered motor conduction velocity of the peroneal nerve after inversion trauma. Med Sci Sports Exerc. 1994;26:877-83.
18. MacIver DA, Letts FL. Paralysis of the peroneal nerve in association with a plantar flexion inversion injury of the ankle. Med Serv J Can. 1966;22:285-7.
19. Meals RA. Peroneal-nerve palsy complicating ankle sprain. Report of two cases and review of the literature. J Bone Joint Surg Am. 1977;59:966-8.
20. Nitz AJ, Dobner JJ, Kersey D. Nerve injury and grades II and III ankle sprains. Am J Sports Med. 1985;13:177-82.
21. Seckler MM, DiStefano V. Peroneal nerve palsy in the athlete: a result of indirect trauma. Orthopedics. 1996;19:345-8.
22. Stoff MD, Greene AF. Common peroneal nerve palsy following inversion ankle injury: a report of two cases. Phys Ther. 1982;62:1463-4.
23. Banerjee T, Koons DD. Superficial peroneal nerve entrapment. Report of two cases. J Neurosurg. 1981;55:991-2.
24. Mizel MS, Hecht PJ, Marymont JV, Temple HT. Evaluation and treatment of chronic ankle pain. Instr Course Lect. 2004;53:311-21.
25. Nobel W. Peroneal palsy due to hematoma in the common peroneal nerve sheath after distal torsional fractures and inversion ankle sprains. J Bone Joint Surg Am. 1966;48:1484-95.
26. Streib EW. Traction injury of peroneal nerve caused by minor athletic trauma: electromyographic studies. Arch Neurol. 1983;40:62-3.
27. Brown R, Pedowitz R, Rydevik B, Woo S, Hargens A, Massie J, Kwan M, Garfin SR. Effects of acute graded strain on efferent conduction properties in the rabbit tibial nerve. Clin Orthop Relat Res. 1993;296:288-94.
28. Highet WB, Sanders FK. The effects of stretching nerves after suture. Br J Surg. 1943;30:355-69.
29. Hoen TI, Brackett CE. Peripheral nerve lengthening. I. Experimental. J Neuro-surg. 1956;13:43-62.
30. Kwan MK, Wall EJ, Massie J, Garfin SR. Strain, stress and stretch of periph-eral nerve. Rabbit experiments in vitro and in vivo. Acta Orthop Scand. 1992;63:267-72.
31. Liu CT, Benda CE, Lewey FH. Tensile strength of human nerves. Arch Neurol Psychiatry. 1948;59:322-36.
32. Rydevik BL, Kwan MK, Myers RR, Brown RA, Triggs KJ, Woo SL, Garfin SR. An in vitro mechanical and histological study of acute stretching on rabbit tibial nerve. J Orthop Res. 1990;8:694-701.
33. Wall EJ, Massie JB, Kwan MK, Rydevik BL, Myers RR, Garfin SR. Experimental stretch neuropathy. Changes in nerve conduction under tension. J Bone Joint Surg Br. 1992;74:126-9.
34. Sunderland S, Bradley KC. Stress-strain phenomena in human peripheral nerve trunks. Brain. 1961;84:102-19.
35. Blair JM, Botte MJ. Surgical anatomy of the superficial peroneal nerve in the ankle and foot. Clin Orthop Relat Res. 1994;305:229-38.
36. Adkison DP, Bosse MJ, Gaccione DR, Gabriel KR. Anatomical variations in the course of the superficial peroneal nerve. J Bone Joint Surg Am. 1991;73:112-4.
37. Wilgis EF, Murphy R. The significance of longitudinal excursion in peripheral nerves. Hand Clin. 1986;2:761-6.
38. Wright TW, Glowczewskie F, Wheeler D, Miller G, Cowin D. Excursion and strain of the median nerve. J Bone Joint Surg Am. 1996;78:1897-903.
39. Wright TW, Glowczewskie F Jr, Cowin D, Wheeler DL. Ulnar nerve excursion and strain at the elbow and wrist associated with upper extremity motion. J Hand Surg [Am]. 2001;26:655-62.
40. Attarian DE, McCrackin HJ, De Vito DP, McElhaney JH, Garrett WE Jr. Biomechanical characteristics of human ankle ligaments. Foot Ankle. 1985;6:54-8.
41. Colville MR, Marder RA, Boyle JJ, Zarins B. Strain measurement in lateral ankle ligaments. Am J Sports Med. 1990;18:196-200.
42. Platt H. On the peripheral nerve complications of certain fractures. J Bone Joint Surg. 1928;10:403-14.
43. Redfern DJ, Sauve PS, Sakellariou A. Investigation of incidence of super-ficial peroneal nerve injury following ankle fracture. Foot Ankle Int. 2003;24:771-4.
44. Self BP, Harris S, Greenwald RM. Ankle biomechanics during impact landings on uneven surfaces. Foot Ankle Int. 2000;21:138-44.
45. Hayes DW Jr, Mandracchia VJ, Webb GE. Nerve injury associated with plantarflexion-inversion ankle sprains. Clin Podiatr Med Surg. 2000;17:361-9, vi-vii.
46. Naraka A. Traumatic brachial plexus lesions. In: Dyck PJ, Thomas PK, Lambert EH, Bunge MB, editors. Peripheral neuropathy. 2nd ed. Philadelphia: WB Saunders; 1984. p. 1394.
47. Pollock FH, Drake D, Bovill EG, Day L, Trafton PG. Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am. 1981;63:239-43.
48. Mansoor IA. Delayed incomplete traction palsy of the lateral popliteal nerve. Clin Orthop Relat Res. 1969;66:183-7.
49. Ogata K, Naito M. Blood flow of peripheral nerve effects of dissection, stretching and compression. J Hand Surg [Br]. 1986;11:10-4.
50. Lerman BI, Gornish LA, Bellin HJ. Injury of the superficial peroneal nerve. J Foot Surg. 1984;23:334-9.
51. Watson-Jones R. Styloid process of the fibula in the knee joint with peroneal palsy. J Bone Joint Surg. 1931;13:258-60.
52. White J. The results of traction injuries to the common peroneal nerve. J Bone Joint Surg Br. 1968;50:346-50.
53. Novich MM. Adduction injury of the knee with rupture of the common pero-neal nerve. J Bone Joint Surg Am. 1960;42:1372-6.
54. Balduini FC, Tetzlaff J. Historical perspectives on injuries of the ligaments of the ankle. Clin Sports Med. 1982;1:3-12.
55. Renstrom P, Wertz M, Incavo S, Pope M, Ostgaard HC, Arms S, Haugh L. Strain in the lateral ligaments of the ankle. Foot Ankle. 1988;9:59-63.
56. Lundborg G, Rydevik B. Effects of stretching the tibial nerve of the rabbit. A preliminary study of the intraneural circulation and the barrier function of the perineurium. J Bone Joint Surg Br. 1973;55:390-401.
57. Lundborg G. Structure and function of the intraneural microvessels as re-lated to trauma, edema formation, and nerve function. J Bone Joint Surg Am. 1975;57:938-48.
58. Lee MS, Hofbauer MH. Evaluation and management of lateral ankle injuries. Clin Podiatr Med Surg. 1999;16:659-78.
59. Sidey JD. Weak ankles. A study of common peroneal entrapment neuropathy. Br Med J. 1969;3:623-6.
60. Hertel J. Functional instability following lateral ankle sprain. Sports Med. 2000;29:361-71.
61. Freeman MA, Dean MR, Hanham IW. The etiology and prevention of func-tional instability of the foot. J Bone Joint Surg Br. 1965;47:678-85.
62. Konradsen L, Ravn JB. Ankle instability caused by prolonged peroneal reac-tion time. Acta Orthop Scand. 1990;61:388-90.
63. Lemont H. Perineural fibrosis of the superficial peroneal nerve complicating ankle sprain: a case report. Foot Ankle. 1991;11:414.
64. Styf J. Entrapment of the superficial peroneal nerve. Diagnosis and results of decompression. J Bone Joint Surg Br. 1989;71:131-5.
65. Toby EB, Hanesworth D. Ulnar nerve strains at the elbow. J Hand Surg [Am]. 1998;23:992-7.
ONeill.fm Page 986 Wednesday, April 11, 2007 2:44 PM





























