Embed Size (px)
Citation preview

Exercise Is Medicine—Putting Science in to Clinical Practice
Preventive Medicine 2010Arlington, VA
February 18, 2010
Steven N. BlairDepartments of Exercise Science &
Epidemiology/BiostatisticsUniversity of South Carolina

DisclosuresDisclosures Medical/Scientific Advisory BoardsMedical/Scientific Advisory Boards
• Jenny Craig, IncJenny Craig, Inc• AlereAlere• TechnogymTechnogym
Research FundingResearch Funding• NIHNIH• Body MediaBody Media• Coca ColaCoca Cola• Swimming Pool FoundationSwimming Pool Foundation

Exercise Is Medicinewww.exerciseismedicine.org
Exercise Is Medicine World Congress
Baltimore, MDJune 1-3, 2010

Dr. & Mrs. Jerry Morris with Brad Pitt

Aerobics Center Longitudinal Study

Design of the ACLS
1970 More than 80,000 patients 2005
Mortality surveillance to 2003More than 4000 deaths
Cooper Clinic examinations--includinghistory and physical exam, clinical tests,body composition, EBT, and CRF
1982 ‘86 ‘90 ‘95 ’99 ‘04Mail-back surveys for case finding and monitoring habits and other characteristics

All-Cause Death Rates by CRF Categories—3120 Women and
10 224 Men—ACLS
0
10
20
30
40
50
60
70
Ag
e ad
j dea
th r
ate/
10,0
00 P
Y
Low Moderate High
Women
Men
Blair SN. JAMA 1989

Cardiorespiratory Fitness, Risk Factors and All-Cause Mortality, Men,
ACLS
0
10
20
30
40
50
60
De
ath
s/1
0,0
00
MY
*
Low Mod High
01
2 or 3
# of risk factors
Risk Factorscurrent smokingSBP >140 mmHgChol >240 mg/dl
Cardiorespiratory Fitness Groups*Adjusted for age, exam year, and other risk factors
Blair SN et al. JAMA 1996; 276:205-10

CRF and Risk of Incident Hypertension, ACLS Women
4,884 healthy women 4,884 healthy women examined at the Cooper examined at the Cooper Clinic, 1970-1998Clinic, 1970-1998
157 women developed 157 women developed hypertension during hypertension during average follow-up of 5 average follow-up of 5 yearsyears
Risk adjusted for age, exam Risk adjusted for age, exam year, alcohol intake, year, alcohol intake, smoking, BP, family history smoking, BP, family history of hypertension, waist girth, of hypertension, waist girth, glucose, & triglyceridesglucose, & triglycerides
FitnessGroups
Risk of Developing Hypertension
Barlow CE et al. Am J Epidemiol 2006; 163:142-50
P for trend <0.01

CRF and Digestive System Cancer Mortality
•38,801 men, ages 20-88 38,801 men, ages 20-88 yearsyears•283 digestive system 283 digestive system cancer deaths in 17 years cancer deaths in 17 years of follow-upof follow-up
CRF was inversely CRF was inversely associated with death after associated with death after adjustment for age, adjustment for age, examination year, body examination year, body mass index, smoking, mass index, smoking, drinking, family history of drinking, family history of cancer, personal history of cancer, personal history of diabetesdiabetes•Fit men had lower risk of Fit men had lower risk of colon, colorectal, and liver colon, colorectal, and liver cancer deathscancer deaths
High Fit
Moderately Fit
Low Fit
Peel JB et al. Cancer Epidemiol Biomarkers Prev 2009; 18:1111

CRF and Breast Cancer Mortality
•14,551 women, ages 20-83 14,551 women, ages 20-83 yearsyears•Completed exam 1970-2001Completed exam 1970-2001•Followed for breast cancer Followed for breast cancer mortality to 12/31/2003mortality to 12/31/2003•68 breast cancer deaths in 68 breast cancer deaths in average follow-up of 16 yearsaverage follow-up of 16 years•Odds ration adjusted for age, Odds ration adjusted for age, BMI, smoking, alcohol intake, BMI, smoking, alcohol intake, abnormal ECT, health status, abnormal ECT, health status, family history, & hormone usefamily history, & hormone use
Odds Ratio
p for trend=0.04
Sui X et al. MSSE 2009; 41:742

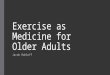
Activity, Fitness, and Mortality in Older Adults

Cardiorespiratory Fitness and All-Cause Mortality, Women and Men ≥60 Years of Age
4060 women and men 4060 women and men ≤60 years≤60 years
989 died during ~14 989 died during ~14 years of follow-upyears of follow-up
~25% were women~25% were women Death rates adjusted Death rates adjusted
for age, sex, and exam for age, sex, and exam yearyear
0
5
10
15
20
25
30
35
40
45
60-69 70-79 80+
Low
Moderate
High
All-Cause death rates/1,000 PY
Age Groups
Sui M et al. JAGS 2007.

Cardiorespiratory Fitness and Risk of Dementia, ACLS
59,960 women and men Followed for 16.9 years
after clinic exam 4,108 individuals died
• 161 with dementia listed on the death certificate
Hazard ratio adjusted for age, sex, exam yr, BMI, smoking, alcohol, abnormal ECG, history of hypertension, diabetes, abnormal lipids, and health status
00.10.20.30.40.50.60.70.80.9
1
Low Moderate High
Fitness Categories
Hazard Ratio
P for trend=0.002
Lui R et al. Research in progress

Multivariate + % Body Fat adjusted HR of Multivariate + % Body Fat adjusted HR of All-Cause Mortality by Fitness Groups, All-Cause Mortality by Fitness Groups,
ACLS, 2603 Adults 60+ACLS, 2603 Adults 60+
0
0.2
0.4
0.6
0.8
1
1.2
Q1 Q2 Q3 Q4 Q5
Adjusted HR
p for trend <0.001
Cardiorespiratory Fitness
106 deaths
98 deaths95 deaths
90 deaths61 deaths
*Adjusted for age, exam year, smoking, abnormal exercise ECG, baseline health conditions, and percent body fat Sui M et al. JAMA 2007; 298:2507-16

Cardiorespiratory Fitness and Health Outcomes in Various
Population SubgroupsSuch as People Who Are
Overweight or Obese

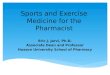
CVD Mortality Risk* by Fitness and BMI Categories, 2316 Men with Diabetes, 179 CVD Deaths
0
1
2
3
4
5
6
7
8
9
10
Ris
k o
f C
VD
Mo
rta
lity
18.5 < BMI <25.0 25.0 ≤ BMI <30.0 30.0 ≤ BMI < 35.0
Re
fere
nc
e
Church TS et al. Arch Int Med 2005; 165:2114
*Adj for age and examination year
p for trend <0.0001p for trend <0.0001 p for trend <0.002

Joint Associations of CRF and % Body Fat Joint Associations of CRF and % Body Fat with All-cause Mortality, ACLS Adults 60+with All-cause Mortality, ACLS Adults 60+
0
10
20
30
40
Fit Unfit
Normal
Obese
Death rate/1,000 person-years
Rates adjusted for age, sex and exam year
Deaths 151 190 29 72
Sui M et al. JAMA 2007; 298:2507-16

Muscular Strength and Mortality

Strength, Adiposity, and Cancer Mortality•8,677 men, 20-82 years•18.8 years of follow-up, 211 cancer deaths•Muscular strength assessed by 1-RM bench press and leg press •Significant trend across strength categories remained after further adjustment for BMI, % body fat, waist circumference, and cardiorespiratory fitness Thirds of Strength
Odds of Cancer Death*
*Adj for age, exam yr, smokingalcohol intake, and health status
P for trend=0.003
Ruiz J et al. Cancer Epidemiol Biomarkers Prev 2009; 18:1468

Yes, But Those Are Observational Studies, and
We Require Randomized Clinical Trial Evidence

Change in Physical Health
3.05
7.35
8.56
10.35
0
2
4
6
8
10
12
Control 72 minutes 136 minutes 192 minutes
Study Groups
SP
H
Martin CK et al. Arch Int Med 2009; 169:269-78

Change in Mental Health
3.32
8.41 8.55
11.86
0
2
4
6
8
10
12
14
Control 72 minutes 136 minutes 192 minutes
Study Groups
SM
H
Martin CK et al. Arch Int Med 2009; 169:269-78

Change in Energy
5.21
12.2511.58
14.42
0
2
4
6
8
10
12
14
16
Control 72 minutes 136 minutes 192 minutes
Study Groups
VT
Martin CK et al. Arch Int Med 2009; 169:269-78

Reduction in Risk of Developing Diabetes in Comparison with Controls,
DPP
58%
31%
0
20
40
60
80
100
Ris
k re
du
ctio
n (
%)
*Moderate intensity exercise of 150 min/week; low calorie, low fat diet
Lifestyle Intervention* Metformin
DPP Research Group. NEJM 2002; 346:393-403

Cost Effectiveness of Diabetes Prevention-DPP
The lifestyle and metformin groups cost $2,250 more/year than placebo
As implemented in the DPP and from a societal perspective, lifestyle was more cost effective than metformin
$0$10,000$20,000$30,000$40,000$50,000$60,000$70,000$80,000$90,000
$100,000P
er Case
Delayed
/Prev
Per Q
AL
YG
ained
Lifestyle
Metformin
DPP Res Group. Diab Care 2003; 26:2518

Summary

Gain in Longevity for a 45-Year Old Male
5.8 years
8.7 years
0
2
4
6
8
10
Low vs Moderate Low vs High
Years of added life
Comparison of Low, Moderate, and High Fitness Levels

Health Care Overview Medical care costs in the U.S are
~17% of GNP, by far the highest in the world
By traditional public health markers such as longevity, chronic disease rates, infant mortality, etc; the U.S. ranks far behind many other countries
Most health problems are the result of unhealthy lifestyles
We must be more aggressive in integrating lifestyle interventions into medical practice and public health programs

Behavioral Approaches to Physical Activity Interventions
Theoretical foundations• Social Learning Theory• Stages of Change Model• Environmental/Ecological Model
Methods• Problem solving• Self-monitoring• Goal setting• Social support• Cognitive restructuring• Incremental changes• Manipulating the environment

Lessons Learned from Physical Activity Intervention Studies
Individuals who use cognitive and behavioral strategies are more likely to be active at 24 months than individuals who do not use these strategies
Approximately 25-30% of initially sedentary persons who participate in Active Living will be meeting consensus public health guidelines for physical activity at 24 months

How to Achieve Lifestyle Change
Counseling by a PhD level behavioral psychologist
Counseling by B.A. level health educators
Counseling by mail and telephone
Counseling by electronic communications

Lifestyle Interventions Integrated with Electronic
Health Records—Kaiser Permanente

Within the Visit Navigator, you will now see the “Exercise Vitals” section immediately following the “Vitals” section.
Exercise as a Vital SignKaiser Permanente

When you click on the “Exercise Vitals” the section opens up to display the two exercise intake questions that can be completed in a quick manner. The date and time this data was captured will also be noted/stored.
Exercise as a Vital SignKaiser Permanente

Telehealth and Weight Change•87 participants (73 women & 14 men)•Mean age 50 years•Treatment groups (Quasi-experimental design)
•Traditional class•Telehealth—interaction with RD via web and email•Control
•No difference in satisfaction between traditional and telehealth•Telehealth more convenient than traditional (p<0.0001)
Kg change at 6 mo
Traditional Telehealth Control
p <0.05
Haugen HA et al. Obes 2007; 15:3067-77

Promoting PA via PDAA 37 healthy, inactive adults, ≥50 years
of age 8-week RCT PDA intervention (93% had not used
PDAs)• Questions about amount and type of PA • Alerted at 2 PM and 9 PM to complete PA
assessment• Gave motivational and behavioral tips
Controls—standard written materials
King AC et al. Am J Prev Med 2007; 34:138-42

Promoting PA via PDA
Intervention participants completed 68% of the 112 PDA entries available
After adjusting for baseline differences• PDA group reported 310.6 minutes of
moderate to vigorous PA/week• Control group reported 125.5
minutes/week• p=0.048 for group comparison
78.6% of PDA group reported enjoying using the device
King AC et al. Am J Prev Med 2007; 34:138-42

Summary Unhealthful lifestyles are the major
cause of chronic disease morbidity and mortality
Lifestyle interventions have demonstrated efficacy and effectiveness in a variety of populations
Our challenge now is to develop translational interventions, using modern technology, to reach large numbers of individuals at a low cost.

Thank you