Embed Size (px)
Citation preview
Expanding Your Assessment Toolbox
Bradley Jackson, Ph.D.
The Children’s Hospital
Aurora, CO
Robert Stadolnik, Ed.D.
FirePsych, Inc/Brandon School
Medway, MA
May 14, 2009
3rd Annual Northeast Juvenile FireseOng IntervenPon Conference
Worcester, MA
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
Evidenced Based Assessments
Avoid clinical judgment alone which is a poor and inconsistent method. (Mills, 2005)
Encourage frameworks that promote systemizaPon and consistency, yet are flexible enough to adapt to individual needs. (Doyle and Dolan, 2002)
Allow for integraPon of science and pracPce. (Borum, 2006)
Collect, structure, and usually quanPfy the impressions of child, caregivers, and professionals. (Hunt and Johnson, 1990)
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
Evidence Based Assessment of Conduct Problems McMahon and Frick (2005)
EB Assessment requires use of a mulPple methods strategy Interviews (Parent, Child, Family) Behavioral Measures Behavioral Observa=ons Evaluate Co-‐Morbid Adjustment Problems (ADHD, Anxiety, Depression, Social Rejec=on, Substance Abuse, Learning Disability)
Issues Relevant to Assessment 1) Severe CP’s cover a broad range of anPsocial and aggressive behaviors.
ODD vs. CD, CD: overt-‐covert, destrucPve-‐nondestrucPve
2) Youth’s with CP’s oben have a number of adjustment problems.
3) There are a large number of risk factors that can have addiPve or interacPve effects.
4) Impact of risk factors can differ across subgroups of youths with CP.
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
Evidenced Based Assessments and FireseOng
Previous authors have reported on importance of a comprehensive diagnosPc approach. (Kolko and Kazdin, 1989; Fineman, 1995; Sakheim and Osborn, 1994; Stadolnik, 2000; Wilcox, 2006)
Assessment is the combinaPon of both scienPfic process and arPsPc endeavor. (Stadolnik, 2000)
Evaluator must embrace a diverse array of data with increased need for collateral contacts. (Wilcox, 2006)
Evaluator must collect and analyze data from mulPple domains. (Fineman, 1995; Humphreys and Kopet, 1996; Kolko, 1999; Stadolnik, 2000; Wilcox, 2006)
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
ConstrucPng Your Assessment Protocol
Factors: 1) PopulaPon Served 2) Funding/Insurance, etc. 3) Service Delivery Model 4) Prior Training and Experience
5) Supervision and Training OpportuniPes
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
StaPsPcs 101
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
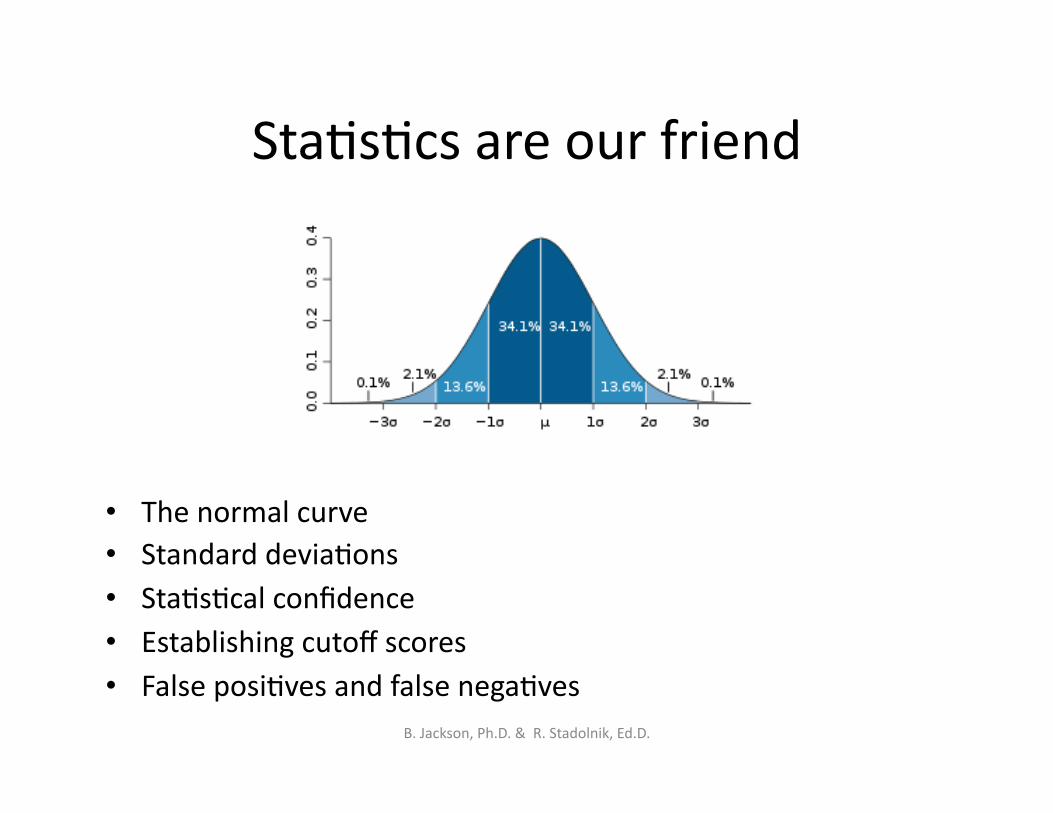
StaPsPcs are our friend
• The normal curve • Standard deviaPons • StaPsPcal confidence • Establishing cutoff scores • False posiPves and false negaPves
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
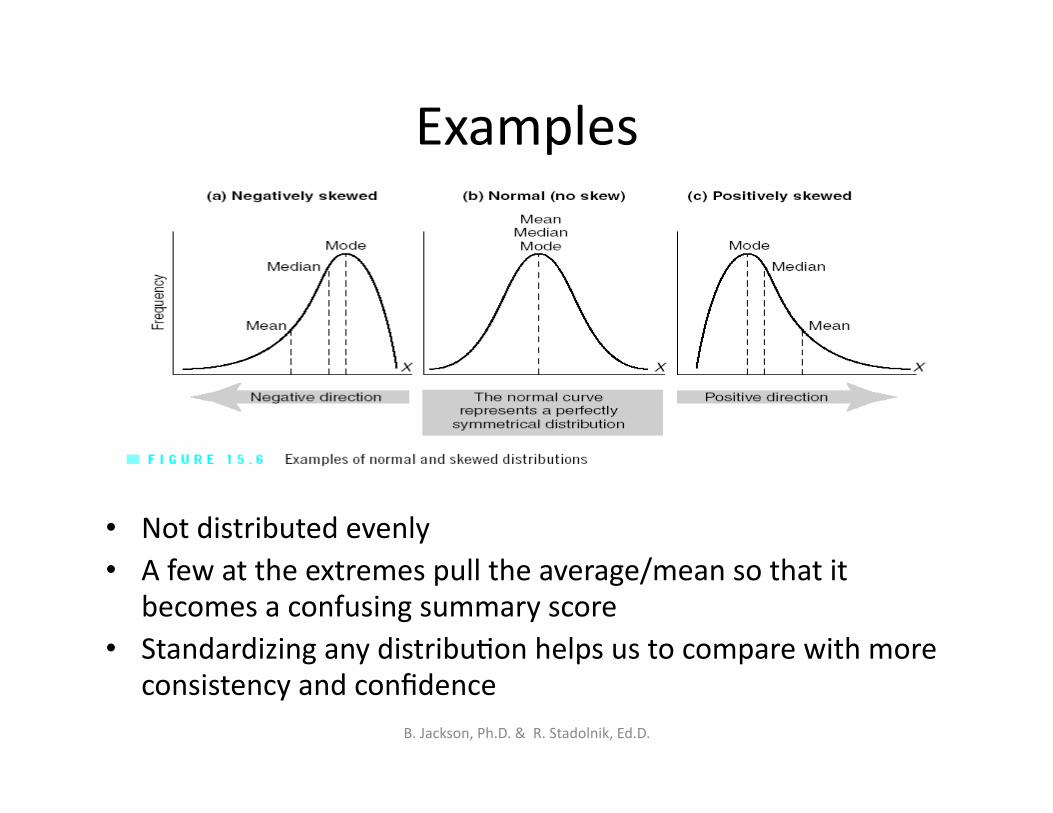
Examples
• Not distributed evenly • A few at the extremes pull the average/mean so that it
becomes a confusing summary score • Standardizing any distribuPon helps us to compare with more
consistency and confidence B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
Standardized scores
• Mathematically transforming a raw score (or any score) into a standard score allows us to use what we know about the normal curve
• Here are some more well-known standard scores
IQ scores (mean = 100, std dev = 15)
GRE/SAT score (mean = 500, std dev = 100)
T scores (mean = 50, std dev = 10)
• For all of these transformations, equal differences between people will result in equal differences between the scores, so now we can actually compare test scores and know what the differences mean.
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
PercenPle
• The percentile of a score tells you what proportion of the population received that score or lower.
• The mean of percentiles is 50% and the range is 0% to 100%.
• The scores do not have to follow any particular distribution so be sure to use a program or chart that standardizes the percentiles.
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
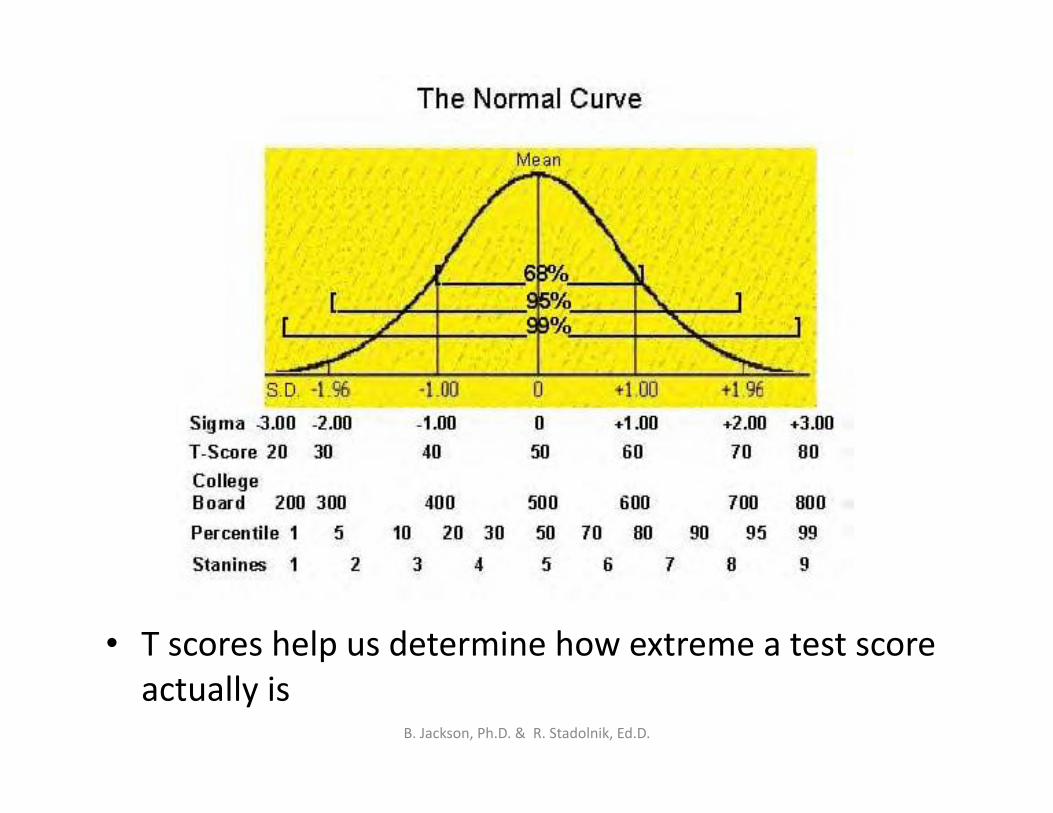
• T scores help us determine how extreme a test score actually is
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.

ReporPng test results
• Raw score • T score • PercenPle • Total score • Scale score • Special score • CriPcal item
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
FireseOng Assessment Domains Stadolnik, R. (2000)
Behavioral FuncPoning Social/EmoPonal FuncPoning
Parent/Family FuncPoning School/CogniPve FuncPoning
FireseOng Behavior History
Fire Scene Evidence
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
Behavioral Func1oning
Assessment Prac<ce Methods:
Record review
Clinical and Collateral Interviews ObservaPon reports Standardized measures
Ques<ons to answer:
Are behaviors acute or chronic?
What is the rate of progression?
Consensus among reporters?
Is impulsivity present?
Criminal charges or police contact?
Direct aggression to people or animals?
Periods of improved behavior?
Current behavior?
Behavioral Measures • Achenbach CBCL, TRF, and YSR
• Behavioral Assessment System for Children (BASC)
• Connor’s RaPng Forms
Aggression Measures • Aggression QuesPonnaire
• Novaco Anger Scale and Provoca=on Inventory
• Overt Aggression Scale
• Interview for AnP Social Behavior
• Others
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
Child Behavior Checklist (Achenbach)
• Self Report Format
• Parent, Teacher, and Youth Versions
• Ages 6 -‐ 18 • Takes 15 -‐ 20 minutes to complete
• Computerized scoring and reports
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
CBCL/Achenbach Subscales
• Competence Scales (20 items, 2 open-‐ ended quesPons) – AcPviPes – Social relaPons – School performance – Total
(e.g., list your child’s sports and rate how oben and how well they do each one compared to other same-‐age children)
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
Child Behavior Checklist
• Behavior Problems Scales (118 items, plus 2 open-ended items)
• Parents rate their child for how true each item is now or within the past 6 months using the following scale: – 0 = not true (as far as you know) – 1 = somewhat or sometimes true – 2 = very true or often true
• Example items -‐ argues a lot; impulsive or acts without thinking; sets fires; unusually loud; unhappy, sad, or depressed
• Internalizing, Externalizing, and Total Problem Scales
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
Child Behavior Checklist
Cross Informant Syndromes: • Anxious/Depressed • Withdrawn/Depressed • Somatic Complaints • Social Problems • Thought Problems • Attention Problems • Rule-Breaking Behavior • Aggressive Behavior
DSM-oriented scales: • Affective Problems • Anxiety Problems • Somatic Problems • Attention Deficit/ Hyperactivity Problems • Oppositional Defiant
Problems • Conduct Problems
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
Novaco Anger Scale and ProvocaPon Inventory Novaco, R. (2003)
Two-‐part, self report measure with 85 total items
Ages 9 to 84 For use in research,
individual assessment, and outcome evalua1on
Designed to assess anger as a problem of psychological func1oning and physical health
Hand Scored
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
Novaco Anger Scale and ProvocaPon Inventory (NAS-‐PI)
NAS-‐PI Scores Cogni<ve (COG)-‐thoughts of jusPficaPon,
suspicion and hosPlity. Arousal (ARO)-‐elevated physiological response
to anger. Behavior (BEH)-‐confrontaPonal and
antagonisPc behaviors or verbalizaPons. Anger Regula<on (REG)-‐suggests effecPve
regulaPon skills, potenPal strength.
NAS Total-‐overall levels of angry behaviors and thoughts.
Provoca<on Inventory PI Total-‐an index score of anger intensity
across a range of provocaPons: disrespect, unfairness, frustaPon, annoyances.
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.

The Aggressive Adolescent
Cogni<ve Characteris<cs Narrow bands of imaginaPon (concrete-‐operaPonal), habitually ruminate
on violent self percepPons, and appraise all situaPons in a hosPle manner. Affec<ve Characteris<cs Narrow band of emoPonal expression, frequently seen as unhappy or
unwell (dysphoric), dichotomous expression of anger from overcontrolled to undercontrolled.
Behavioral Coping Skills Lack basic social skills and have low asserPveness skills. Poor
negoPators and unable to delay graPficaPon. Need to be taught how to avoid conflicts.
Davis, D. (2000). The Aggressive Adolescent: Clinical and Forensic Issues. New York. Haworth Press.
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
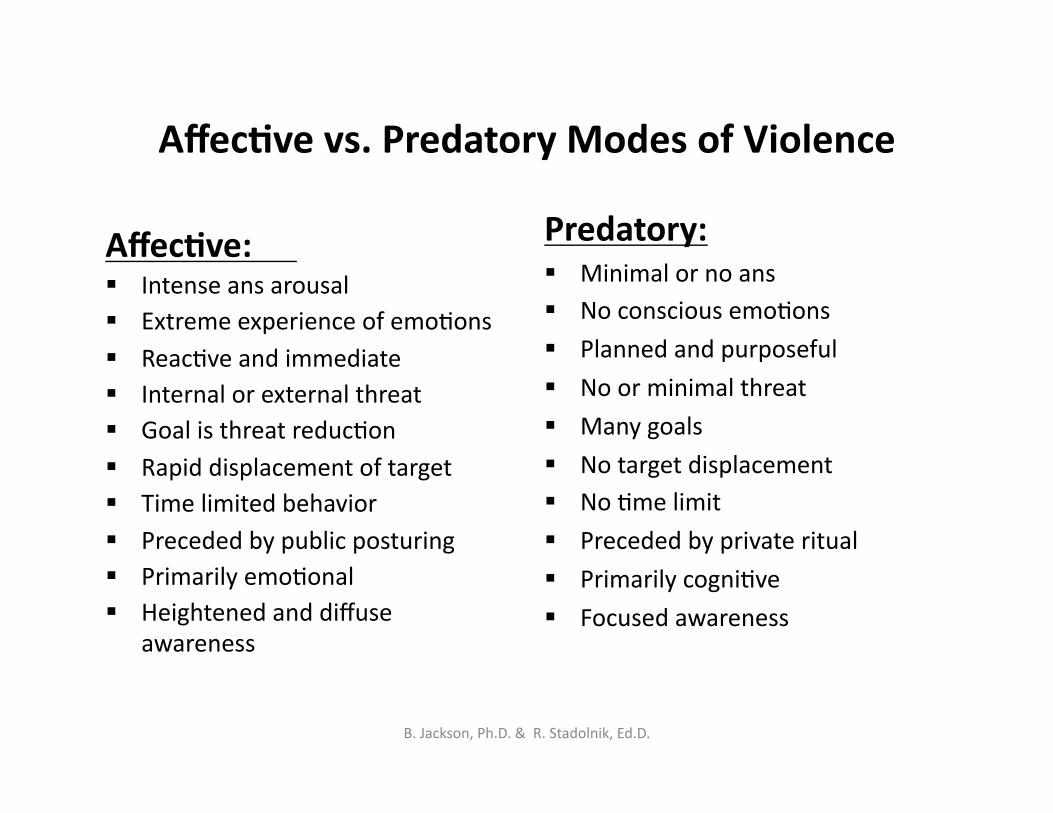
Affec<ve vs. Predatory Modes of Violence
Affec<ve: Intense ans arousal Extreme experience of emoPons ReacPve and immediate Internal or external threat Goal is threat reducPon Rapid displacement of target Time limited behavior Preceded by public posturing Primarily emoPonal Heightened and diffuse
awareness
Predatory: Minimal or no ans No conscious emoPons
Planned and purposeful
No or minimal threat
Many goals
No target displacement No Pme limit
Preceded by private ritual
Primarily cogniPve
Focused awareness
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
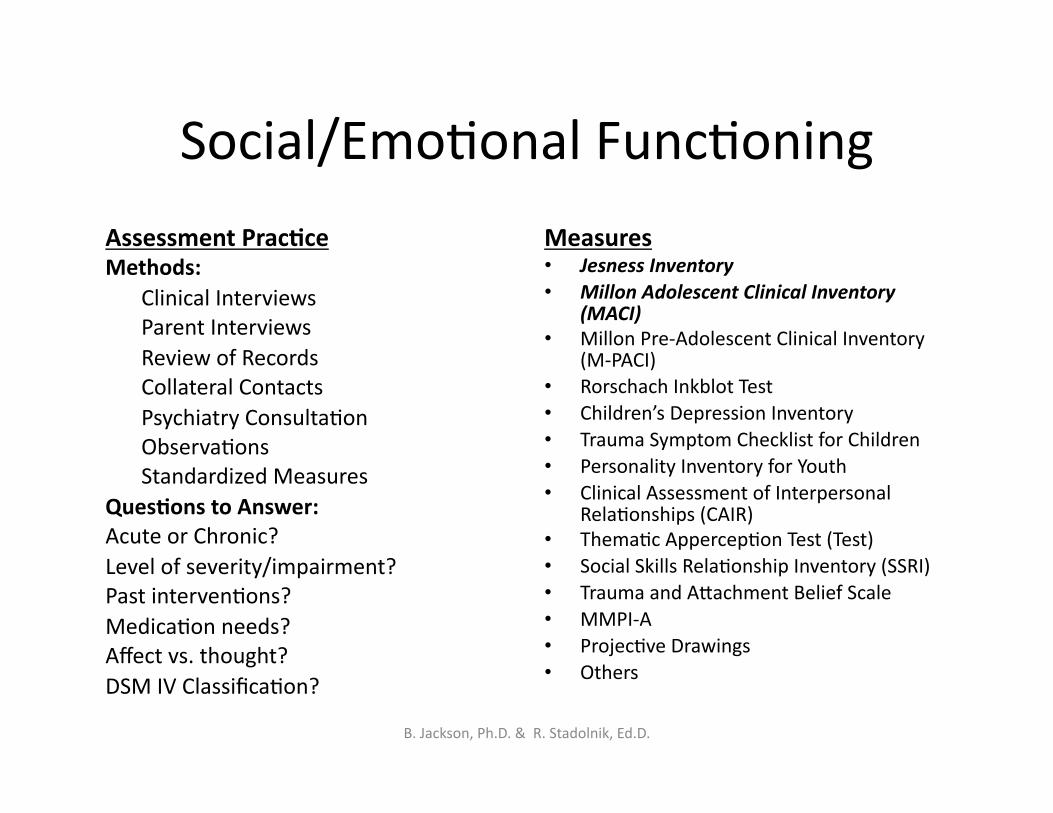
Social/EmoPonal FuncPoning
Assessment Prac<ce Methods: Clinical Interviews Parent Interviews Review of Records Collateral Contacts Psychiatry ConsultaPon ObservaPons Standardized Measures Ques<ons to Answer: Acute or Chronic? Level of severity/impairment? Past intervenPons? MedicaPon needs? Affect vs. thought? DSM IV ClassificaPon?
Measures • Jesness Inventory • Millon Adolescent Clinical Inventory
(MACI) • Millon Pre-‐Adolescent Clinical Inventory
(M-‐PACI) • Rorschach Inkblot Test • Children’s Depression Inventory • Trauma Symptom Checklist for Children • Personality Inventory for Youth • Clinical Assessment of Interpersonal
RelaPonships (CAIR) • ThemaPc AppercepPon Test (Test) • Social Skills RelaPonship Inventory (SSRI) • Trauma and Amachment Belief Scale • MMPI-‐A • ProjecPve Drawings • Others
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
Jesness Inventory-‐ Revised (JI-‐R)
• Youth self-‐report • 160 true/false items • Ages 8 yrs and older • Computerized scoring, hand-‐
scoring templates, online administraPon
• 30 – 45 minutes
DSM-‐IV Scales • Conduct Disorder • OpposiPonal Defiant Disorder
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
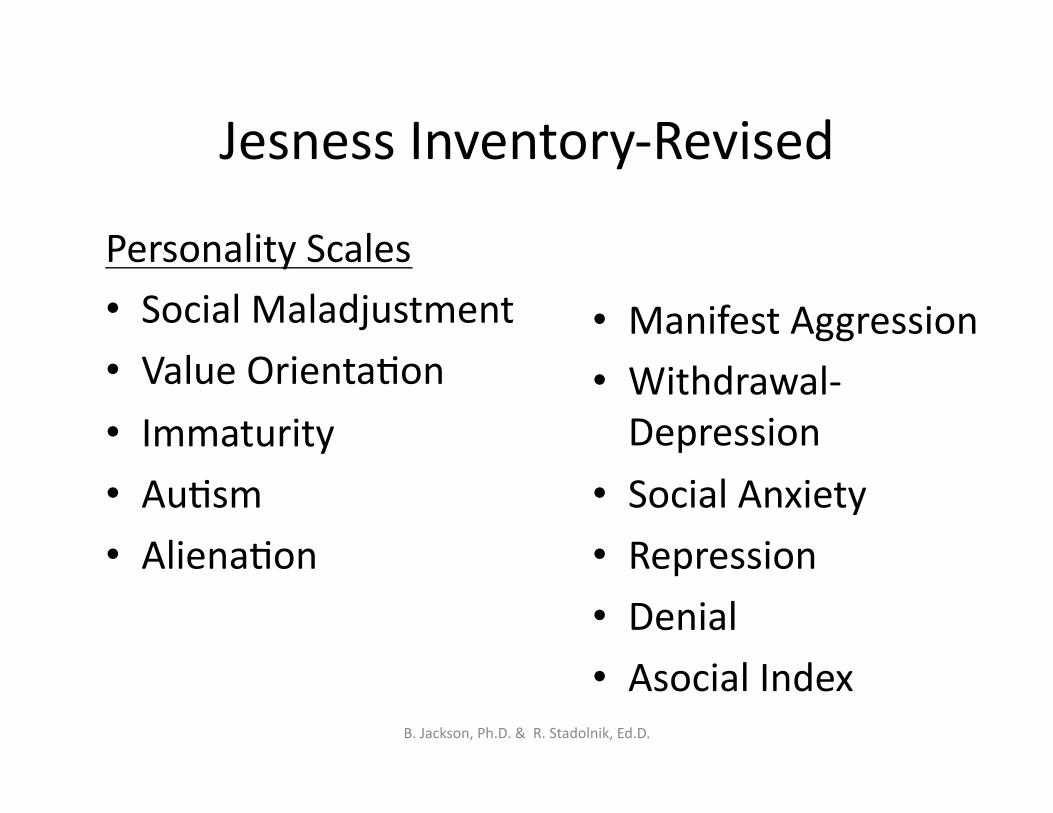
Jesness Inventory-‐Revised
Personality Scales • Social Maladjustment
• Value OrientaPon • Immaturity
• AuPsm
• AlienaPon
• Manifest Aggression • Withdrawal-‐Depression
• Social Anxiety • Repression • Denial • Asocial Index
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
Jesness Subtype Profiles
• Undersocialized, AcPve • Undersocialized, Passive • Conformist
• Group-‐Oriented • PragmaPst
• PragmaPst
• Autonomy-‐Oriented
• IntrospecPve • Inhibited • AdapPve
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
Trauma Symptom Checklist (TSCC)
• Youth self-‐report measure of post-‐traumaPc distress
• 54 items
• Ages 8 – 16 • Hand Scored • Profile Form
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
TSCC
Validity Scales
• Underresponse • Hyperresponse
Clinical Scales
• Anxiety • Depression • Anger • PosmraumaPc Stress • DissociaPon (3) • Sexual Concerns (3) • CriPcal Items
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
Millon Adolescent Clinical Inventory (MACI) Millon, T. (2006)
MACI Features 160 items, True/False, self report measure
Ages 13-‐19 Summarized in computer generated narra1ve reports
Examines three dis1nct categories: Personality PaOerns, Expressed Concerns, and Clinical Syndromes B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
Millon Adolescent Clinical Inventory (MACI)
Base Rate (BR) Interpreta=ons
MACI raw scores are transformed into BR scores
BR scores are a measure of the rate at which a characteris1c is present in the norm popula1on.
For each MACI scale BR scores are anchored at 75 and 85.
85= represents adolescents for whom this trait is most prominent 75= represents adolescents for whom the trait is prominent or present
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
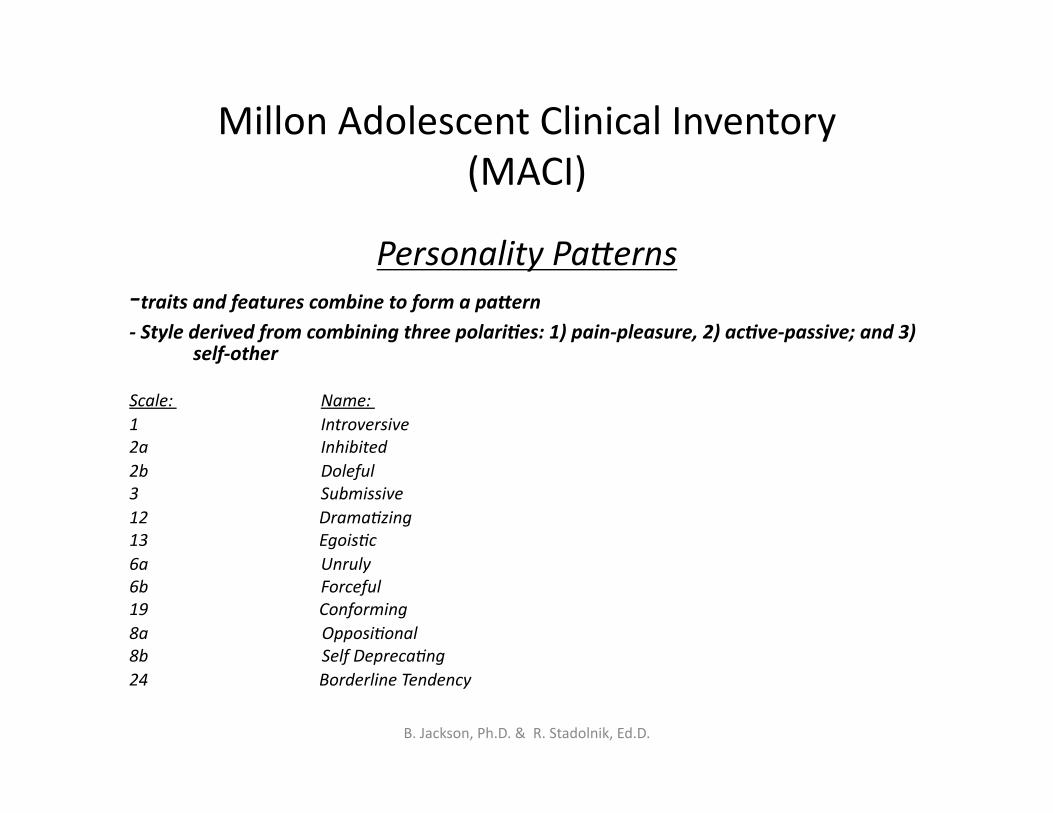
Millon Adolescent Clinical Inventory (MACI)
Personality PaVerns -‐traits and features combine to form a paOern -‐ Style derived from combining three polari=es: 1) pain-‐pleasure, 2) ac=ve-‐passive; and 3)
self-‐other
Scale: Name: 1 Introversive 2a Inhibited 2b Doleful 3 Submissive 12 Drama1zing 13 Egois1c 6a Unruly 6b Forceful 19 Conforming 8a Opposi1onal 8b Self Depreca1ng 24 Borderline Tendency
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
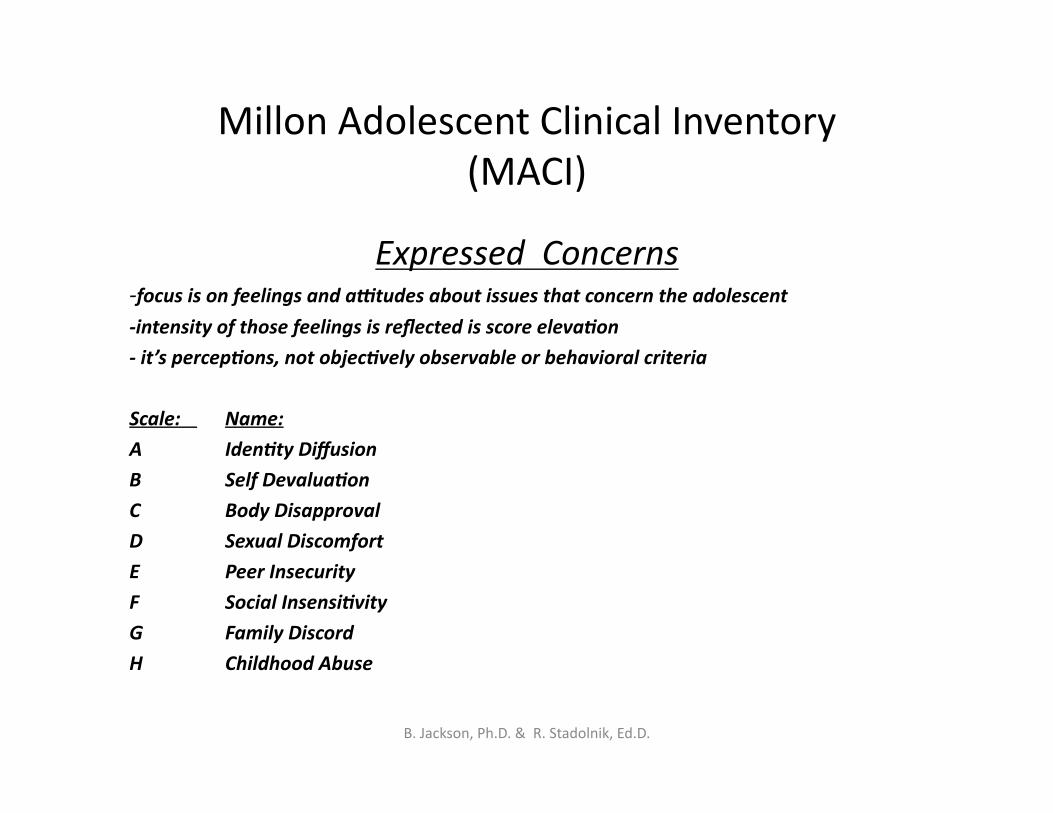
Millon Adolescent Clinical Inventory (MACI)
Expressed Concerns -‐focus is on feelings and aVtudes about issues that concern the adolescent
-‐intensity of those feelings is reflected is score eleva=on
-‐ it’s percep=ons, not objec=vely observable or behavioral criteria
Scale: Name:
A Iden=ty Diffusion
B Self Devalua=on
C Body Disapproval
D Sexual Discomfort
E Peer Insecurity
F Social Insensi=vity
G Family Discord
H Childhood Abuse
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
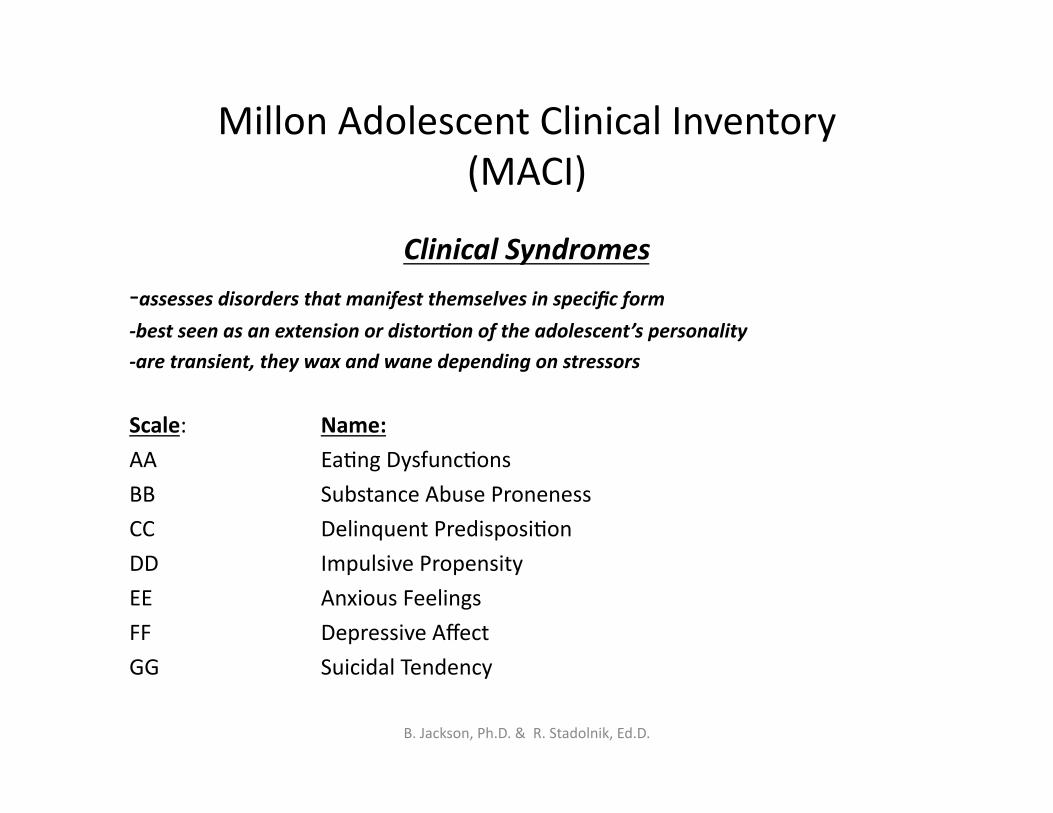
Millon Adolescent Clinical Inventory (MACI)
Clinical Syndromes
-‐assesses disorders that manifest themselves in specific form
-‐best seen as an extension or distor=on of the adolescent’s personality
-‐are transient, they wax and wane depending on stressors
Scale: Name:
AA EaPng DysfuncPons
BB Substance Abuse Proneness
CC Delinquent PredisposiPon
DD Impulsive Propensity
EE Anxious Feelings
FF Depressive Affect
GG Suicidal Tendency
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
Parent /Family Func=oning
Assessment Prac<ce: Methods:
Direct interview
Data from collateral reporters
Home visit
Milieu observaPon reports
Standardized measure
Ques<ons to answer:
Overall emoPonal climate?
RelaPonship/amachment quality?
Discipline pracPces?
Family resources?
Parent mental health?
Marital strength?
Measures:
ParenPng Stress Index Family Conflict Scale
Parent-‐Child RelaPonship Inventory
Family Assessment Measure III
Alabama Parent QuesPonnaire
Others
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
Family Assessment Measure-‐Version 3 Skinner, B., Steinhauer, P., and Santa-‐Barbara, J. (1995)
FAM III Features Self report measure, takes
30-‐40 minutes to complete Ages 10 and older Provides a quan1ta1ve
descrip1on of family strengths and weaknesses
Can be completed by all members of the family
3 Scales: General Scale, Dyadic Rela1onship Scale, Self-‐Ra1ng Scale
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
Family Assessment Measure-‐Version 3 FAM III
FAM III Subscales Task Accomplishment-‐ basic tasks met, flexible, alterna=ve solu=ons are explored
Role Performance-‐family understands expecta=ons of roles, and agrees, adapt to new roles
Communica=on-‐ direct, clear, open, sufficient
Affec=ve Expression-‐full range of affect when appropriate and with correct intensity
Involvement-‐ empathic involvement, concern for others, nurturing
Control-‐ paOerns of influence, adaptable, predictable yet flexible, construc=ve Values and Norms-‐consistent with family subgroup, explicit and implicit rules are
consistent
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
Family Assessment Measure-‐Version 3 FAM III
Interpre=ve Guidelines: Elevated scores (T>60) must be interpreted for alterna=ve
explana=ons (Ex: Involvement)
The more family members who indicate and elevated score in a par=cular area, the more likely it is problema=c.
Total number of elevated scores correlates to overall family pathology.
Greater discrepancies among spouse profiles suggest marital discord
Different scores elevated for different members of the family suggest percep=on differences.
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
FireseOng Behavior History
Assessment Prac<ce
Methods: Fire History Interview-Child Parent Interview Structured Interview Tools Record Review Collateral Reports Questions to Answer: When ? How? Where? Who? What? Why?
Structured Interview Tools: Children’s Firesetting Interview Firesetting Risk Interview Graphing Technique Oregon Screening Tool FIRE Protocol Fire Risk Interviews (Child, Parent,
Family)-FEMA Others
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
Drawings
Use of drawings during the assessment interview can help to:
• Immerse the child in the memory
• Engage the child in mulPple modaliPes of sharing (verbal, visual)
Types of drawings
• Self • Tree • Family doing something
• Safe fire • Unsafe fire
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
Individual fire graphs
• From a list of all firesets/fireplay, the child selects a significant fire incident and details the sequence of events before, during and aber the fire
• Cartoon or panel technique for fire drawings • Wrimen graph encourages child/teen to link thoughts and feelings to the sequence of events
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
Wrimen Fire Graph • Describe the situaPon & the sequence of events • Usually aware of events occurring during the fireset and aber
• Focus on the events before fireset • Slow down the descripPon • Ask clarifying quesPons • Focus on possible precipitaPng triggers earlier in the day/week/month
• Add corresponding thoughts and feelings
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.
Bibliography
Achenbach, T. (2001) Manual for the Achenbach System for Empirical Behavior Analysis. University of Vermont. Burlington, VT.
Borum, R. (2006). Assessing risk for violence among juvenile offenders. In Forensic Mental Health Assessment of Children and Adolescents (Sparta, S and Koocher, G. Eds.). Oxford University Press. London. (pgs190-‐203).
Doyle, M. and Dolan, M.(2002). Violence risk assessment: combining actuarial and clinical informaPon to structure clinical judgments for the formulaPon and management of risk. Journal of Psychiatric and Mental Health Nursing. 9. 649-‐657.
Fineman, K. (1995). A model for the qualitaPve analysis of child and adult fire deviant behavior. American Journal of Forensic Psychology. 13(1). 31-‐60.
Humphreys, J. and Kopet, T. (1996). Manual for the Juvenile FireseVer Needs Assessmnet Protocol. Oregon State Fire Marshal. Portland, OR.
Hunt, F. and Johnson, C. (1990). Early intervenPon for severe behavior problems: the use of judgment based assessment procedures. Topics in Early Childhood Special Educa1on. 10(3). 111-‐122.
Jesness, C. (2003). Jesness Inventory-‐Revised Manual. MulP-‐Health Systems. North Tonowanda, NY.
Kolko, D. (1999). FireseOng in children and youth. In V Van Hasselt & M. Hersen (Eds.), Handbook of Psychological Approaches with Violent Offenders: Contemporary Strategies and Issues. 95-‐115. Kluwar Academic/Plenum Publishers. New York.
Kolko, D. and Kazdin, A. (1989). Assessments of dimensions of childhood fireseOng among paPents and nonpaPents: the FireseOng Risk Interview. Journal of Abnormal Child Psychology. 17(2). 157-‐176.
McMahon, R. and Frick, P. (2005). Evidence-‐based assessment of conduct problems in children and adolescents. Journal of Clinical Child and Adolescent Psychology. 34(3). 477-‐505.
Millon, T. (2006). Millon Adolescent Clinical inventory Manual. NCS Pearson Inc. Minneapolis, MN.
Mills, J. (2005). Advances in the assessment and predicPon of interpersonal violence. Journal of Interpersonal Violence. 20(2). 236-‐241. Novaco, R. (2003). The Novaco Anger Scale and Provoca1on Inventory Manual. Western Psychological Associates. Los Angeles, CA.
Skinner, H., Steinhauer, P. and Santa-‐Barbara, J. (1995). Family Assessment Measure Version III Technical Manual. MulP-‐Health Systems. North Tonowanda, NY.
Stadolnik, R. (2000). Drawn to the Flame: Assessment and Treatment of Juvenile Fireseang Behavior. Professional Resource Press. Sarasota, FL.
Wilcox, D. (2006). Assessing Fireseang Behavior in Children and Adolescents. In Forensic Mental Health Assessments of Children and Adolescents (Sparta, S. & Koocher, G. Eds.). Oxford University Press, New York, NY.
B. Jackson, Ph.D. & R. Stadolnik, Ed.D.