Embed Size (px)
Citation preview

Experience with family based intervention against overweight Carl-Erik Flodmark
Childhood Obesity UnitDept of Pediatrics in Malmö, Sweden16th Nordic Congress of General PracticeCopenhagen 15th May 2009
The problems
Childhood obesity is increasing The first step
Nutrition Epidemiology: Bogalusa study: Total consumption of low-quality
foods were positively associated with overweight status Nicklas TA, Yang SJ, Baranowski T, Zakeri I & Berenson G (2003) Eating patterns
and obesity in children. The Bogalusa Heart Study. Am J Prev Med 25, 9-16
Treatment: Calori intake more important than “fashion diets” Nordmann AJ, Nordmann A, Briel M, Keller U, Yancy WS, Jr., Brehm BJ &
Bucher HC (2006) Effects of low-carbohydrate vs low-fat diets on weight loss and cardiovascular risk factors: a meta-analysis of randomized controlled trials. Arch Intern Med 166, 285-93

The problems, cont.
The first step cont Nutrition cont
In children there is no conclusive evidence regarding diets using low glycemic index or high-protein diets although reduction of soft-drinks seems to be efficient in prevention Nowicka P (2005) Dietitians and exercise professionals in a childhood
obesity treatment team. Acta Paediatr Suppl 94, 23-9 Physical acitivity
Systematic review of RCTs of physical activity treatment showed that an aerobic exercise prescription of 155-180 min/weeks at moderate-to-high intensity is effective for reducing body fat Atlantis E, Barnes EH & Singh MA (2006) Efficacy of exercise for treating
overweight in children and adolescents: a systematic review. Int J Obes (Lond) 30, 1027-40
The problems, cont
The second step Change of lifestyle
Professional conversation Drugs
No licensed drugs in Europe Not recommended
Surgery No controlled trials Not recommended
Prevention Flodmark CE, Marcus C & Britton M (2006) Interventions to prevent
obesity in children and adolescents: a systematic literature review. Int J Obes (Lond) 30, 579-89.
Family based interventions
Seeing a family – group encounter Interacting with a family – socio-environmental
therapy Treating a family
Behavioural therapy Cognitive behavoural therapy Family therapy
The reasons for this model
Behavioral therapy Using behavioral performance based procedures to
induce changes in behavior (re-learning) Cognitive behavioral therapy
Using behavioral performance based procedures and cognitive interventions to produce changes in thinking, feeling and behavior
Psychological models cont
Family (systems) therapy Using the encounter with a family to improve the
members health by observing and analyzing interactions between family members but also with the therapists and improving the family’s ability to use their own resources
Group therapy Review
Flodmark CE. Childhood Obesity. Clinical Child Psychology and Psychiatry 1997;2: 283-
295

BackgroundBackgroundChildhood Obesity Unit Childhood Obesity Unit
The board for health and hospital care started 2001 The board for health and hospital care started 2001 a project of three years for establishing a knowledge a project of three years for establishing a knowledge and treatment centre for obese children in the and treatment centre for obese children in the Region Skåne. Region Skåne.
Childhood obesity unit Regional centre in 2004
A regional assignment for coordinating actions against childhood obesity by:
Informing about the disease childhood obesity and its health consequences
Establishing a dialogue with child health care, school health care and other present of future collaborating bodies.
Making this evidence based therapy based on family therapy available in the Region Skåne
Treating children with overweight including obesity
Multi-disciplinary approach
Medical (pediatric) Nutrition Physical activity Psychological/social
Co-operation within a team is necessary to offer a Co-operation within a team is necessary to offer a treatment specially designed for the familytreatment specially designed for the family
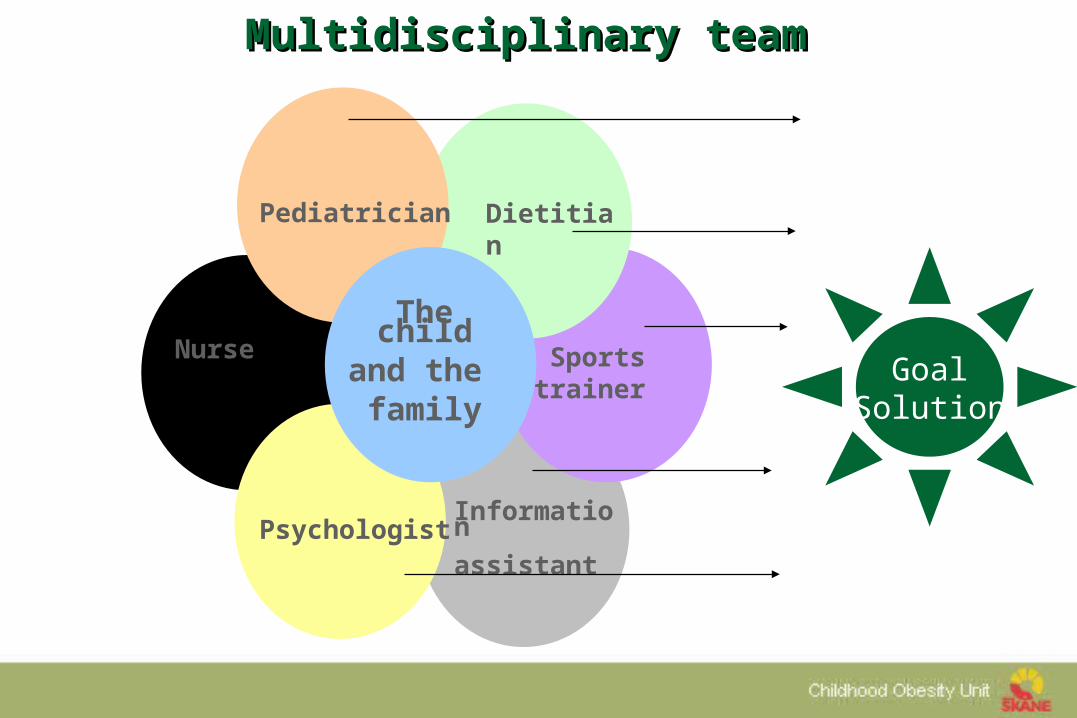
Nurse
Pediatrician
The childand the family
Dietitian
Psychologist
Sports trainer
Information
assistant
GoalSolution
Multidisciplinary team Multidisciplinary team
Treatment modelsSOFT
Standardised Obesity Family TherapySingle family treatment:
First visit includes– Full team
– Investigation– Evaluation
– Goals for this family
Follow-up is done using smaller teams
Flodmark, CE. Pediatrics (1993) 91:880-884Nowicka, P. International Journal of Pediatric Obesity (2007) 2:211-217
Results
Eighty-one percent of the children and their parents participated in the follow-up.
Eleven children were treated for 6-12 months, and 33 for more than 12 months.
Families received 3.8 family therapy sessions.
International Journal of Pediatric Obesity (2007) 2:211-217
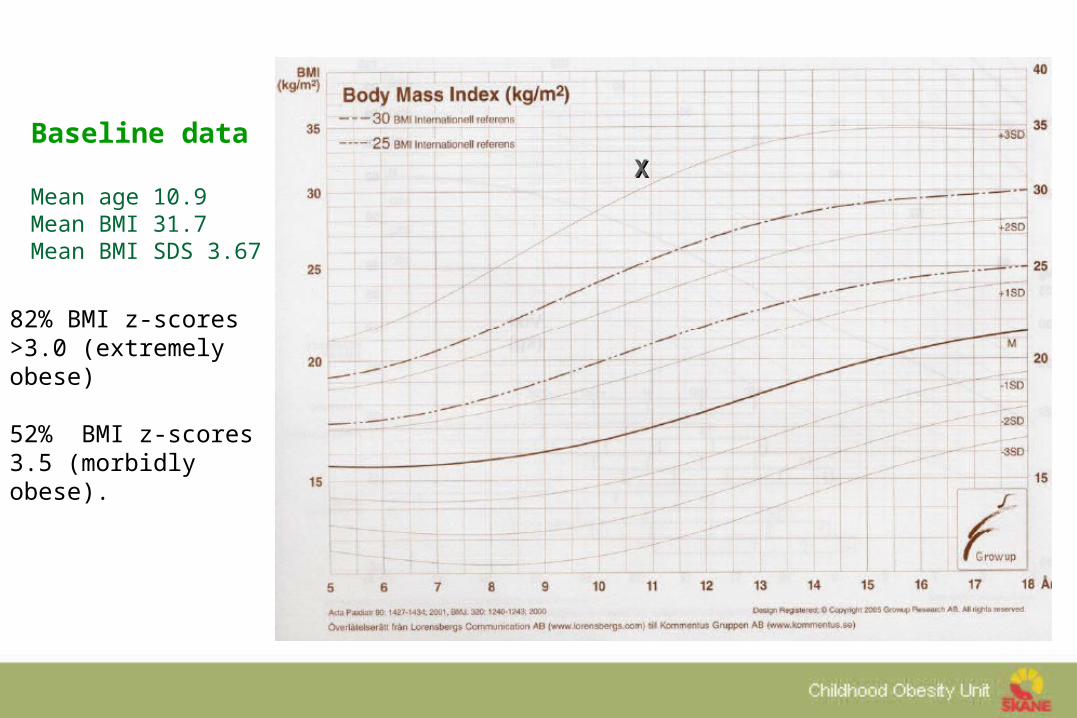
XX
Baseline data
Mean age 10.9Mean BMI 31.7Mean BMI SDS 3.67
82% BMI z-scores >3.0 (extremely obese)
52% BMI z-scores 3.5 (morbidly obese).

ResultsBMI z-score changes
6 8 10 12 14 16 18
23
45
Age
BM
I z-s
co
re
GirlsBoys
International Journal of Pediatric Obesity (2007) 2:211-217
Intervention resulted in a mean decrease in BMI z-score of 0.12 (p=0.0001).
Family therapy
Ref. Flodmark CE et al Prevention of progression to severe
obesity in a group of obese schoolchildren treated with family therapy Pediatrics 1993;91:880-884
Background Tomm K: Interventive interviewing. Part III. Intending to
ask linear, circular, strategic and reflexive questions? Fam Process 1988;27, 1-45
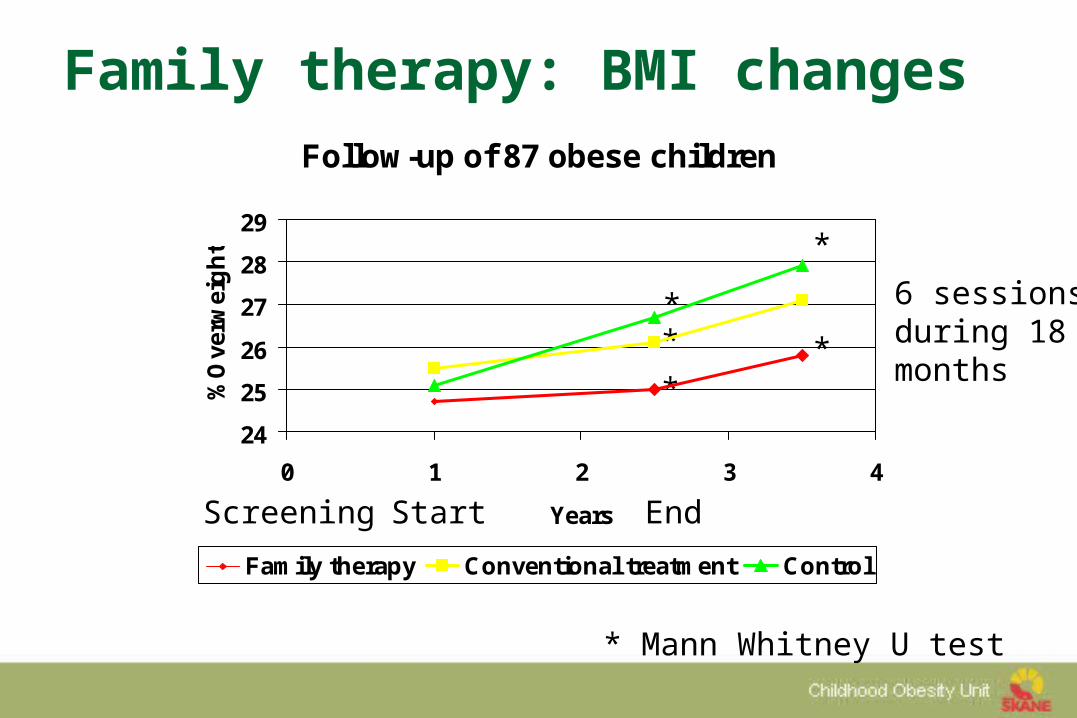
Family therapy: BMI changes
Screening Start End
**
*
**
* Mann Whitney U test
6 sessionsduring 18months
Follow-up of 87 obese children
24
25
26
27
28
29
0 1 2 3 4
Years
%O
verw
eig
ht
Family therapy Conventional treatment Control
Reflexions
Non-blaming approach showing respect (requires training)
Realistic goals (biological knowledge) Small steps Age adjusted strategies (requires understanding of
psychological development)
Behavioural therapy
Ref. Epstein L. H., Valoski A., Wing R. R. &
McCurley J. Ten-year follow-up of behavioral, family-based treatment for obese children. Jama 1990;264:2519-2523.
Background Stuart R. B. Behavioral control of overeating.
Behav Res Ther 1967;5:357-365.
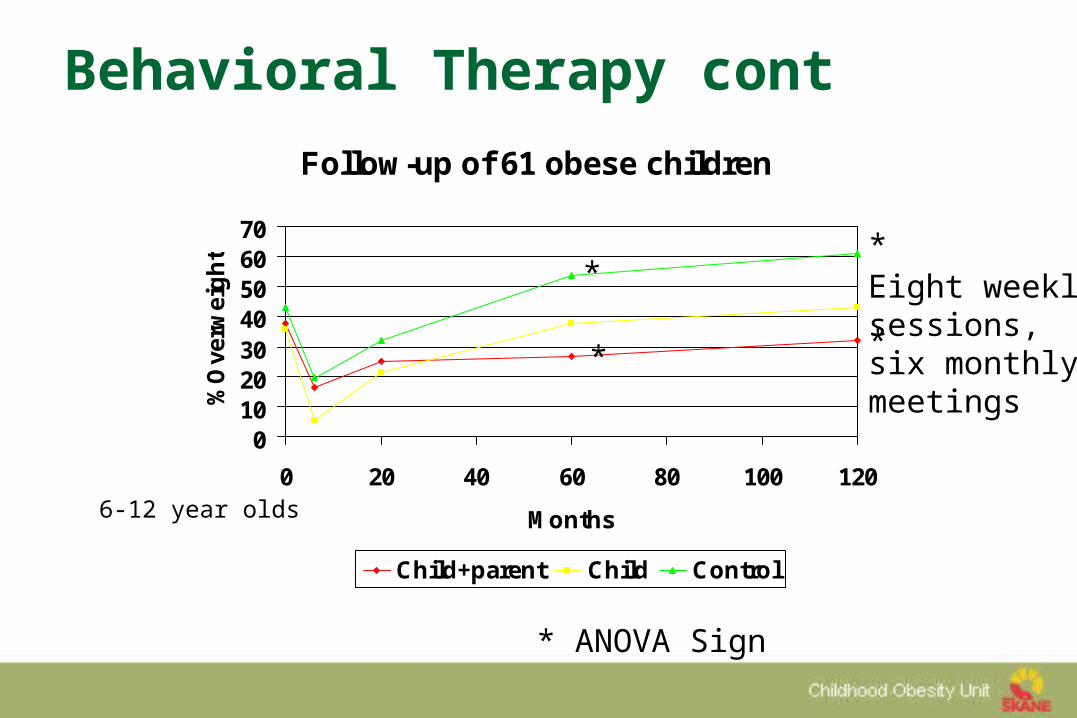
Behavioral Therapy contFollow-up of 61 obese children
010203040506070
0 20 40 60 80 100 120
Months
%O
verw
eig
ht
Child+parent Child Control
*
*
*
*
* ANOVA Sign
Eight weeklysessions,six monthlymeetings
6-12 year olds
Cognitive behavior therapy
Ref. Braet C. & Van Winckel M. Long-term follow-
up of a cognitive behavioral treatment program for obese childr. Behavior Therapy 2000;31:55-74.
Braet C., Van Winckel M. & Van Leeuwen K. Follow-up results of different treatment programs for obese children. Acta Paediatr 1997;86:397-402
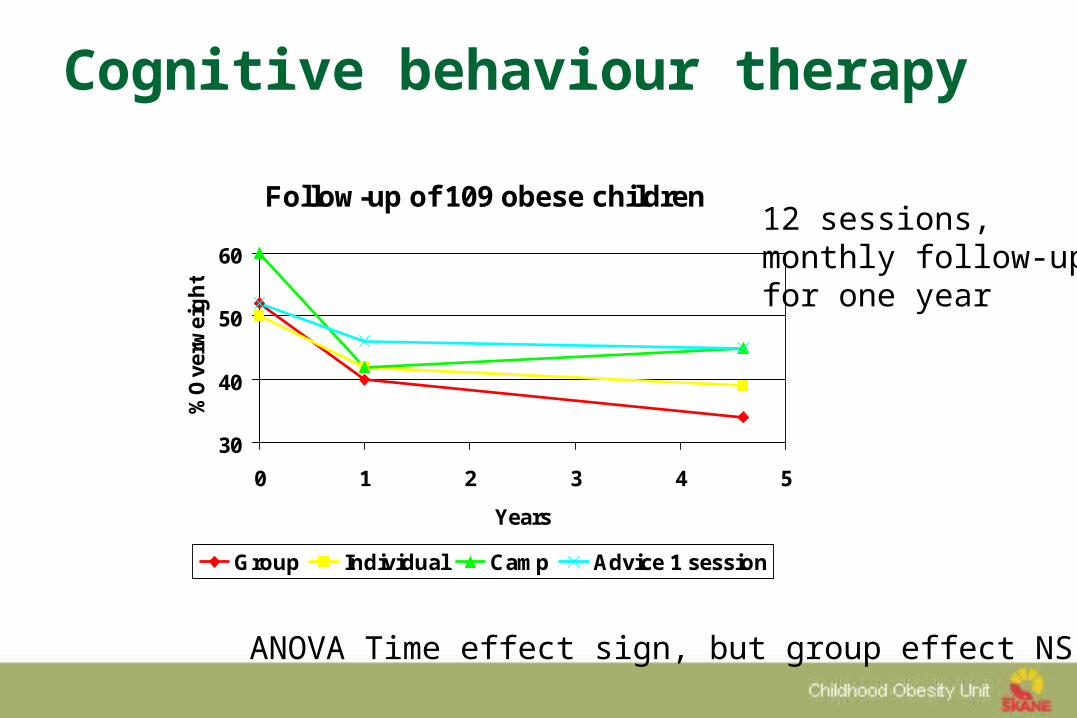
Cognitive behaviour therapy
ANOVA Time effect sign, but group effect NS
12 sessions,monthly follow-upfor one year
Follow-up of 109 obese children
30
40
50
60
0 1 2 3 4 5
Years
%O
verw
eig
ht
Group Individual Camp Advice 1 session
Future possibilities
Surgery – Not yet Drugs – Not yet Pedagogical and conversational treatments
combined Family weight school
Family weight school
Multiple family treatment Education and conversational treatment for the
teenagers 12-19 years of age and the family 72 families were treated for one year Evaluation regarding BMI, quality of life, diet and
physical activity
Nowicka P.Nowicka P. International Journal of International Journal of Pediatric Obesity (2008) 3:141-147Pediatric Obesity (2008) 3:141-147
BMI SDS (-0. 09, p=0.039) decreased in all children ≤ BMI z-scores 3.5, as compared with the control group.
ResultsThe follow-up one year after study start
Family Weight School Cost of treatment
Intensity of treatment
Braet C et al (Belgium) 30 visits per patient per year
Epstein L et al (USA) 14 visits
Single Family Treatment 3.8 visits
Family Weight School 3.4 visits
Cost of treatment
Single Family Treatment 3 000 € per family
Family Weight School 1 300 € per family
A professional conversation
How do you do it?
Is it effective?
Is it cost-effective?
Is it safe?
How to start?
Use psychological based treatments
Better long-term results than in adults
The method chosen might be important
No indication of increased eating disorders
Karl Tomm Systemic interviewing Fam Process 1988;27, 1-45
More information
SPOC 9-10 July 2010
Scandinavian Pediatric Obesity ConferenceSPOC official satellite of ICO Stockholm 2010, Sweden
www.childhoodobesity.info
The web page for Childhood Obesity Unit Region Skåne (publicerat=publication list):
www.bravikt.info

Thank you!