Embed Size (px)
Citation preview
ON THE RISK vol.31 n.4 (2015) 1
JOURNAL OF THE ACADEMY OF LIFE UNDERWRITING
December 2015Volume 31 Number 4www.ontherisk.com
ISSN 0885-4416Copyright 2015Printed in U.S.A.
OTR Cardiac Stress Tests | 54 M. Wetzel US Age and Amount Requirements & Preferred Classification Criteria Trends | 37 D. Davis / M. Privett Highlights of the 2015 CLIMOA Annual Conference | 26 T. Trachenko Avoiding Material Misrepresentation and Fraud in Life Insurance | 43 K. Brown And More ...
IN THIS ISSUE
www.alu-web.com
www.ciu.ca
www.ahou.org
OTR is a benefit of membership in
and
ON THE RISK vol.31 n.4 (2015)2
The One Stop Solution for all your Underwriting and Claims Requirements
Outsourced/Remote Underwriting• Tele-Underwriting• Quick Quotes• Objective Analysis & Decisions• Full STP Capabilities
Exam Solutions• Unparalleled National Coverage• Presets Welcome• Highest Rated Examiners• Real-Time Status Updates
APS Retrievals• Daily Updates• 9 Calendar Day Average• Fully Automated• Dedicated CRM
114 Mowbray Drive • Kew Gardens, NY 11415 • 888-766-3999 • www.parameds.com
© 2007 Parameds.com, Inc.
Making Your ‘Life’ Easier!™For a FREE Demo or trial, please contact Stuart Levy at 888-766-3999 x 2769 or [email protected].
APS Summaries• Experienced, U.S. based underwriters• Health history synopsis that chronologically details tobacco use, medications, prior conditions and lab tests• Paperless, secure environment
Backlogged with Cases? Ask PDC about a FREE demo of our
APS Summary Service today!
Ad_8_31.indd 1 11/8/07 11:38:01 AM
ON THE RISK vol.31 n.4 (2015) 3
®
Impossible demands for time service? •
Shuffling paper instead of underwriting? •
Overloaded by APS page counts? •
Complicated health histories? •
Here’s your cure:
Contact us today to find out how to qualify for our 24 Hour APS Summary Service!Stuart [email protected]
www.parameds.com
24Hour
APS SummaryService!
114 Mowbray Drive • Kew Gardens, NY 11415 • 888-766-3999 • www.parameds.com
© 2008 Parameds.com, Inc.
Making Your ‘Life’ Easier!™
For a FREE Demo or trial, please contact Stuart Levy at 888-766-3999 x 2769 or [email protected]
EXPERIENCING THESE SYMPTOMS?
xray_ad.indd 1 11/4/08 2:51:13 PM

ON THE RISK vol.31 n.4 (2015)4
JOURNAL OF THE ACADEMY OF LIFE UNDERWRITING
ON THE RISK is the Journal of the Academy of Life Underwriting. It is published under the direction of the Board of Directors of the Academy of Life Underwriting (ALU) comprising representatives of the Association of Home Office Underwriters (AHOU), the Canadian Institute of Underwriters (CIU), the ALU and OTR. It is published quarterly and printed by The Marek Group, Inc., Milwaukee, WI. Permission to reproduce articles must be obtained from the Editor-in-Chief unless copy-right is clearly indicated to be held by an author and/or a third party.
EDITOR-IN-CHIEFKevin Cunningham, FALUJohn Hancock Life218 Harmony DriveDelaware, OH 43015Phone (614) [email protected]
EXECUTIVE EDITORNancy AtkinsMetLife18210 Crane Nest DriveTampa, FL 33647Phone (813) [email protected]
ADMINISTRATIVE EDITORBrendan Paradis, FALUMetLife11215 North Community House RoadCharlotte, NC 28277Phone (980) [email protected]
ADVERTISING MANAGERDeb Wesenberg, FALURoyal Neighbors of America230 16th StreetRock Island, IL 61201-8645Phone (309) [email protected]
EXECUTIVE AND BUSINESS OPERATIONS ASSOCIATE EDITORS INTERNATIONAL EDITORS
ACTUARIAL CONSULTANT Richard L. Bergstrom, FSAConsulting [email protected]
MEDICAL CONSULTANTClifton P. Titcomb Jr., MDHannover Life [email protected]
DisclaimerON THE RISK is a professional journal devoted to the continuing education of its readers and to the exchange of infor-mation and ideas that serve those professionals. Opinions expressed within the correspondence and articles published in ON THE RISK do not represent official opinions of ON THE RISK. Such expressions only represent the views of authors or persons quoted. Publication of articles discussing products, services or methods offered by vendors does not represent endorsement by OTR. Such information is published only for its value as business knowledge.
Vera F. Dolan, FALUVFD Consulting, [email protected]
Barbara J. Lutz, FALUCUNA Mutual [email protected]
Jodi Przybyl McDonald, FALUHannover Life [email protected]
Tanya Trachenko, MD, FALUWawanesa [email protected]
LEADERSHIPMarv Reber, [email protected]
CONTRIBUTING EDITORS
Rochelle Fernandes, FALUThe Canada Life Assurance [email protected]
Jeanne Hollinger, [email protected]
Jennifer Johnson, [email protected]
Namita Joshi, [email protected]
Jane Mattson, [email protected]
Michelle Privett, FALUSwiss [email protected]
Clifton P. Titcomb Jr., MDHannover Life [email protected]
Michael Wetzel, MDPrudential Insurance [email protected]
Asia EditorDr. Himanshu BhatiaGenRe AsiaMumbai, [email protected]
Canada EditorLaura Brandson, AALUWestern Life Assurance CompanyWinnipeg, [email protected]
Caribbean EditorRafael R. ShabetaiPan-American Life Insurance Grp.New Orleans, [email protected]
Latin America EditorFreddy Velasco-A., AALUL&H Underwriting ConsultantMiami, [email protected]
United Kingdom EditorYunus (Pip) PiperdyRGA UK Services LtdLondon, United [email protected]

ON THE RISK vol.31 n.4 (2015) 5
Subscription Information: Members of the Association of Home Office Underwriters (AHOU) and the Canadian Institute of Underwriters (CIU) receive OTR as a benefit of membership. Direct subscriptions are also available. One-year subscription rate: Electronic only version (global rate) - $35.00; Print version - North America (USA, Canada and Mexico): $40.00; Outside North America: $55.00. Back issues - North America: $15.00; Outside North America: $25.00. Subscribe by credit card at the website - www.ontherisk.com. Otherwise, please make all checks payable to ON THE RISK. Please send change of address forms and all subscription correspondence to: OTR Publishing Services, P.O. Box 2990, Binghamton, NY 13902-2990; Telephone (607) 724-3992; Fax (607) 724-0041; E-mail address: [email protected]; Website: www.ontherisk.com.
IMPORTANT: Under current copyright laws protecting OTR’s digital rights, a subscription is a personal subscription for one person only and cannot be shared with others at your company. It is illegal to share the username and password or to post the downloaded e-version PDF on a company’s intranet or to e-mail a copy to others as a means of avoiding the purchase of additional subscriptions.
TABLE OF CONTENTSThe Underwriting Quiz .............................................................FALU Club of RGA 8
OTR News ............................................................................................................. 10Calendar of Coming Events .................................................................................... 14From the President: Academy of Life Underwriting ..............................F. Goetz 16From the President: Association of Home Office Underwriters – AHOU 2016 - “Capture the Magic” ......................................................C. Johns 22
Highlights of the 2015 CLIMOA Annual Conference: Athlete’s Heart; Prognosis of
Patients with Cardioverters-Defibrillators: Are They Insurable?; Fibromyalgia
& Disability: What’s New in 2015?; The Pulmonary Nodule in the Era of Scans
and Screens; Breast Cancer: What’s New?; Prostatic Cancer: New
Developments ............................................................................. T. Trachenko 26
US Age and Amount Requirements &
Preferred Classification Criteria Trends ..........................D. Davis / M. Privett 37
Avoiding Material Misrepresentation and Fraud in Life Insurance
(Overview, Application Design and Red Flags) ..................................K. Brown 43
The Simplified Issue Conundrum ................................................ D. Dombrosky 46
Management vs. Leadership .................................................................M. Reber 52
Cardiac Stress Tests ..............................................................................M. Wetzel 54
Understanding the Complete Blood Count ............................................O. Telfer 59
Low Cholesterol and Low Albumin Levels:
Alerts to Hidden Mortality Risk .........................................M. Fulks / R. Stout 65
Mature Age Underwriting .................................................................J. Morrison 70
Chikungunya – A New Tropical Disease in Latin America .............F. Velasco-A. 74
Index to Advertisers ...............................................................................................78
Follow OTR on Facebook Twitter and

ON THE RISK vol.31 n.4 (2015)6 ON THE RISK vol.31 n.3 (2015)6
www.alu-web.com
THE ACADEMY OF LIFE UNDERWRITING
EXAMINATION 101COORDINATORLori Boucher, FALULiberty Life of Boston
Lynn Dreist, FALULincoln Financial Group
Kayla Grigsby-Bailey, FALUNew York Life
Zera Langley, FALULincoln Financial Group
Pamela Lewis, FALUNorthwestern Mutual Life
Brendan Paradis, FALUMetLife
Danni Pedigo, FALUDavis Life/Innovative UW Solutions
EXAMINATION 201COORDINATORAnn Day, FALUWestern Fraternal Life Assoc.
Rick Dawson, FALUFBL Financial
Gay Kemmis, FALUSecurian Financial Group
Libby Limoni, FALUVOYA Financial
Donna Melfi, FALUSecurity Mutual Life of NY
Carol Steckel, FALUAmerican Family Life
Oana Telfer, MD, FALUSun Life Financial
EXAMINATION 202COORDINATORCatie Muccigrosso, FALURGA Reinsurance Group
Christine Klein, FALUUnited Life Insurance
Joyce Jess, FALUGreat West Financial
Joanne Kay, FALUSun Life Financial
Marcel Padilla, FALUIndustrial Alliance Insurance
Aubree Pham, FALUAmerican Income Life
Amy Rider, FALUOptimum Re Insurance
EXAMINATION GROUPS
PRESIDENTFrank Goetz, FALUPacific Life Insurance Company
PAST PRESIDENTMargaret Taff, FALUVantis Life Insurance
SECRETARYJodie Hofmaier, FALUUnited of Omaha Life Insurance Co.
TREASURERJean Everhart, FALUWoodmen Life
DIRECTOR OF CONTINUING EDUCATIONSharon Garner, FALUAmerican National Insurance Co.
DIRECTOR OF CURRICULUMJodi McDonanld, FALUHannover Life Re
DIRECTOR OF EXAMSJoseph Keown, FALULincoln Financial Group
DIRECTOR OF MARKETINGJennifer Dahl, FALURBC Insurance
MEETING PLANNERMark McPheronCincinnati Life Insurance Co.
WEBSITE MANAGERCarolyn Goshorn, FALUSwiss Re
CONSULTANTSMEDICAL CONSULTANTSSusan Sokoloski, MDAXA
Cathy Percival, RN, BSN, FALU
EDITORMarty Meyer, FALU
MANAGING DIRECTORRichard SchmidtAcademy of Life [email protected]
EXECUTIVE GROUP
EXAMINATION 301COORDINATORDoreen Brynga, FALUVOYA
Debbie Dias, FALUCanada Life Reinsurance
Stephanie Helle, FALUAegon / Transamerica
Michael Hill, FALURGA Reinsurance Company
Sandy Jenum, FALURiverSource Life Insurance
Stacey Jung, FALUCincinnati Life Insurance Co.
Cynthia Landry, FALUSwiss Re America
Lisa Gutierrez, FALUAccordia Life
Jeanne Hollinger, FALUMetLife
Joanne Lackenbauer, FALUSun Life
Angela Read, FALULegal & General America
Vicky Sheehan, FALULincoln Financial Group
Peter Trivella, FALUJohn Hancock
Elise Walter, FALUTexas Life Insurance
Michael Waterhouse, FALULincoln Financial Group
Roland Paradis, FALUAXA Equitable
Paula Romano, FALU
Angela Read, FALULegal & Gerneral America
EXAMINATION GROUPS
CURRICULUM GROUP
Hope Adams, FALU Transamerica Life Insurance
Roy Davis, FALUNFP
John Duff, FALUBMO Life Assurance
Tim Miller, FALUMunich American Reassurance
Sue Swenson, FALUPrudential
Nancy Thorpe, FALURBC Insurance
COORDINATORKathleen Alfano, FALU
Sherri Boyda, FALUBerkshire Hathaway Group Rein.
Cindy Mitchell, FALUSCOR Global Life Americas
Carla Martin, FALUExamOne
William Dumpman, FALUGenworth Financial
COORDINATORKristin Ringland, FALUSCOR Global Life Americas
Carol Flanagan, FALUJohn Hancock
Roberta Scott, FALUWoodmen Life
John Sherman, FALUAIG Global Consumer Insurance
FORUM GROUP
MARKETING GROUP
SURVEY GROUP
MEDICAL UNDERWRITING TASK FORCE
UNDERWRITING DEVELOPMENT AND CONTINUING EDUCATION
ON THE RISK vol.31 n.4 (2015) 7
hr|Ascent is a trusted source of credible, evidence-based ratings on over 500 medical conditions
Hannover Life Reassurance Company of America
200 South Orange Avenue, Ste. 1900 Orlando, Florida 32801 USA
[email protected] www.hannover-re.com Member of the Hannover Re Group
Practical underwriting solutions from Hannover Life Reassurance Company of America•Facultative underwriting – Highly experienced
underwriting staff specializing in competitive, timely offers combined with capacity of USD 20 million plus
• Consulting – Underwriting requirements and preferred guideline analysis
• Research – Diverse team of underwriting and mortality-related research experts
• hr|Ascent – The most user-friendly and comprehensive underwriting manual in the industry
• Alternative underwriting solutions – Simplified Issue, Merica US™ and COLI / BOLI
150717_hrv_advert_ascent.indd 1 17.07.15 16:01
ON THE RISK vol.31 n.4 (2015)8
FALU Club of RGA
THE UNDERWRITING QUIZ
Executive Summary ON THE RISK is known for its scholarly articles on insurance topics. In keeping with this, the FALU Club of RGA offers a fun and challenging addition to OTR in the form of the underwriting quiz. This regular feature is meant to challenge the underwriting knowledge of you, the reader, encourage ALU class enrollment and promote ongoing professional education in general. If you would like to submit quiz questions of your own, or if you have any comments, suggestions or questions, please contact the FALU Club of RGA at [email protected]. We look forward to hearing from you.
So now we invite you to test your wits on this quiz. Are you smarter than a FALU?
The Academy of Life Underwriting will offer four ALU examinations on April 19, 2016. ALU 101 ALU 201ALU 202 ALU 301
The registration period for all ALU examinations opened September 1, 2015. Exam registrations are accepted through March 1, 2016; registration forms received February 2 – March 1, 2016, require payment of a late registration fee in addition to the regular exam fee.
Answers on page 77
ON THE RISK vol.31 n.4 (2015) 9
Traditional inspection reports can offer tremendous insight, but the time and expense of obtaining them—not to mention the inconvenience to customers—means they aren’t always used.
Now you can maintain high underwriting standards and provide exceptional customer service at the same time. Get immediate access to a proposed insured’s public records footprint, such as properties, criminal records history, professional licenses, bankruptcies, liens, judgments and more with LexisNexis® Life Electronic Inspection Report. This single report provides the critical information your underwriters need to evaluate risk and independently confirm information disclosed on applications—efficiently and effectively.
To learn more: Call 800.458.9197, email [email protected] or visit lexisnexis.com/risk/life
LexisNexis Life Electronic Inspection Report is a consumer reporting agency product provided by LexisNexis Risk Solutions, Inc. and may only be accessed in compliance with the Fair Credit Reporting Act, 15 U.S.C. 1681, et seq. Due to the nature of the origin of public record information, the public records and commercially available data sources used in reports may contain errors. Source data is sometimes reported or entered inaccurately, processed poorly or incorrectly, and is generally not free from defect. This product or service aggregates and reports data, as provided by the public records and commercially available data sources, and is not the source of the data, nor is it a comprehensive compilation of the data. Before relying on any data, it should be independently verified. LexisNexis and the Knowledge Burst logo are registered trademarks of Reed Elsevier Properties Inc., used under license. Other products and services may be trademarks or registered trademarks of their respective companies. Copyright © 2015 LexisNexis. All rights reserved.
Get a more holistic view of your proposed insured in one real-time report.
Risk SolutionsInsurance

ON THE RISK vol.31 n.4 (2015)10
Metlife for 7 years and has been in the insurance in-dustry for 15 years. In his current position, Brendan has responsibility for the underwriting team that services the MetLife Premier Client Group Southeast Region. He is directly involved in efficiency and best practice initiatives for the overall life underwriting and new business teams, and has played a role in MetLife’s relocation strategy to Charlotte, NC. Prior to Brendan’s current role, he served as the manager of the Jet Issue Underwriting Unit that underwrote all lower face amount, younger age cases in both broker-age and career underwriting channels.
Congratulations, Brendan!
Donna Daniells, FALU, FLMI, MBA, has completed her 3-year term as an Executive Team member–serv-ing as 2013 Administrative Editor, 2014 Executive Editor and 2015 Editor-in-Chief.
During Donna’s term, OTR introduced several inno-vations including “Key Point” icons within articles, themed recurring sections such as “Leadership,” and encouragement of short, narrowly focused articles of 1000 words or less.
Beginning in mid-2016, she will serve as OTR’s del-egate on the Academy of Life Underwriting Board of Directors.
Congratulations and thank you, Donna!
OTR NEWS - INTRODUCING THE 2016 EXECUTIVE TEAM; DEPARTING EDITOR-IN-CHIEF IS THANKED FOR HER SERVICE
AtkinsCunningham
OTR is proud to announce the succession of Kevin Cunningham, FALU, FLMI, ACS, CLU, ChFC, as Editor-in-Chief effective January 1,
2016, after serving as 2015 Executive Editor. Kevin will be responsible for overall management of the quarterly editorial content of OTR, and will work with the Executive Editor and Administrative Editor on developing valuable editorial content for readers from the Associate, Contributing and International Editors in addition to independent authors. He will also assist the Advertising Manager in the delivery of excellent service to advertisers in each issue. Kevin has served as the Associate Manager for Publishing and Circulation with OTR since 2010.
Congratulations, Kevin!
OTR is also proud to announce the appointment of Nancy Atkins as Executive Editor effective January 1, 2016, after serving as 2015 Administrative Editor. Nancy will be directly responsible for management of the Associate and Contributing Editor teams and monitor preparation of the financial and manage-ment reports. Nancy will assist the Editor-in-Chief and Publisher with management of the quarterly publication process, review of editorial content, and management of article inventory and online content. Congratulations, Nancy!
OTR is also proud to announce the appointment of Brendan Paradis, as Administrative Editor effective January 1, 2016. Brendan will be directly responsible for management of the International Editor team. In addition, he will assist the Executive Editor with management of the OTR Policies and Procedures guidelines, review of editorial content, and manage-ment of article inventory and online content.
Brendan is currently a Life Underwriting Director, Metlife Retail Life & Disability. He has worked at
Paradis
Daniells
ON THE RISK vol.31 n.4 (2015) 11
AU RA is more than one of the most widely used automated underwriting tools in the world. It is a powerful decision engine that saves time and money and gathers vital data so you can grow your business. And AU RA is the only automated underwriting solution backed by RGA's award-winning expertise, experience and customer focus.
Superior underwriting rules, fast decisions and business insights. Get it all with AURA.

ON THE RISK vol.31 n.4 (2015)12
OTR NEWS - OTR WELCOMES NEW CONTRIBUTING EDITOR
OTR is pleased to announce the appointment of Jeanne Hollinger, FALU, FLMI, as a Contributing Editor. Jeanne is an Associate Chief Underwriter with MetLife, and has been with the company since 2005. She is also entering her fifth year as a member of the ALU Curriculum Group, and authored the “Life Claims” chapter in the ALU 202 textbook and “Life
Hollinger
Claims - What the Underwriter Needs to Know” in the December 2014 issue of OTR. Jeanne has more than 30 years’ experience as a brokerage underwriter and 25 years in management. She worked with Prudential, Executive Life, and the North American Company for Life and Health prior to joining MetLife.
Welcome aboard, Jeanne!
(Left) From the September 2015 Annual Meeting of the Academy of Life Underwriting in Portland, OR - members of the ALU Executive Group: (left to right) ALU Board Chair and Past President Margaret Taff, Vantis Life; ALU President Frank Goetz, Pacific Life; ALU Treasurer Jean Everhart, Woodmen Life; ALU Secretary Jodie Hofmaier, United of Omaha Life.
(Right) ALU Executives at the Annual Meeting of the Academy of Life Underwriting: (left to right) Meeting Planner Mark McPheron, Cincinnati Life; Website Manager Carolyn Goshorn, Swiss Re; Director of Continuing Education Sharon Garner, American National; Director of Marketing Jenni-fer Dahl, RBC Insurance; Director of Curriculum Jodi McDonald, Hannover Life Re; Director of Exams Joseph Keown, Lincoln Financial.
ON THE RISK vol.31 n.4 (2015) 13EIUWOTR 1215
emsinet.com/Insurance
THE MOST TALENTED UNDERWRITERS CHOOSE EMSIThere’s a reason talented Individual Life Insurance Underwriters choose to work with EMSI. With flexible hours, the ability to work from home and the potential to underwrite business for the most respected carriers in the industry, we’re fast becoming the underwriter employer of choice.
Learn more at emsinet.com
Underwriting Services
Decode data analytics and take risk assessment to the next level EMSI’s structured APS Summaries provide a compelling ROI and unprecedented insight into impairment risk.
Structured APS Summaries: Crack the Code
Partner with EMSI and unlock the secret to improved underwriting decision making.
Structured APS Summaries: Crack the Code
Comprehensive risk assessment capabilities you can rely on We deliver an insightful APS summarization - a reliable risk assessment tool that covers everything from clinical, ICD10 and MIB coding to impairments, vitals and lab trends. With the ability to incorporate EHRs, the structured data we provide on individuals and populations holds infinite possibilities for data analysis, directly contributing to rapid and informed policy decisions.
For nearly 20 years, EMSI has been a leading provider of APS summaries. Our underwriting professionals are highly trained and come from home office environments giving them the expertise our customers demand.
SEE IT FOR YOURSELFContact us at
underwriting-sales@ emsinet.com
for a sample APS Summary
ON THE RISK vol.31 n.4 (2015)14
OTR CALENDAR OF COMING EVENTS
January 18-19 CIU Winter Education Seminar at the St. Andrew’s Club & Conference Centre, Toronto, ON. For more information visit www.ciu.ca.
January 24-26 MUD (Metropolitan Underwriting Discussion Group) Annual Conference at the InterContinental Hotel, New York, NY. For more information visit www.mudgroup.com.
March 3 CHOLHUA (Chicago Home Office Life and Health Underwriters Association) Spring Conference at the Allstate Financial Campus, Northbrook, IL. For more information contact [email protected].
April 4-6 ACLI Life Insurance Conference at the Bellagio, Las Vegas, NV. For more information visit www.acli.com.
April 19 ALU Annual Examination. For more information visit www.alu-web.com.
May 1 XIIIth IUSG (International Study Group) at the Marriott World Center, Orlando, FL. For more information contact Rafael Shabetai at [email protected].
May 1-4 AHOU Annual Conference at the Marriott World Center, Orlando, FL. For more informa-tion visit www.alu-web.com.
May 4 FHOUA (Fraternal Home Office Under-writers Association) Annual Meeting at the Marriott World Center, Orlando, FL. For in-formation contact [email protected].
June 2-3 CIU Annual General Meeting at the Marriott Yorkville - Bloor in Toronto, ON. For more information visit www.ciu.ca.
June 5-8 CLIMOA (Canadian Life Insurance Medi-cal officers Association) 71st Annual Scien-tific Meeting at the Ivey Spencer Leadership Centre, London, ON. For more information visit www.climoa.com.
2016
June 22-24 SEHOUA (Southeastern Home Of-fice Underwriters Association) 2016 Annual Meeting at the Naples Grande Beach Resort in Naples, FL. For more information contact Kim Lancaster at [email protected].
September 12-14 ALU Annual Underwriting Fo-rum at the Hyatt Regency O’Hare, Chicago, IL. For more information visit www.alu-web.com.
September 21–23 LIMRA DI & LTC Insurers’ Forum at The Roosevelt, New Orleans, LA. For more information visit www.limra.com/conferences/.
September 25-28 ELHUA (European Life and Health Underwriters Association) Confer-ence at the Husa Princesa Hotel, Madrid, SP. For more information visit www.elhua.eu.
October 14 NEHOUA (NorthEast Home Office Underwriters Association) Annual Confer-ence at the Sheraton, Portsmouth, NH. For more information visit www.nehoua.org.
October 16-18 ACLI Annual Conference at the J.W.Marriott, Washington, DC. For more information visit www.acli.com.
October 20-22 ALUCA (Australasian Life Under-writing and Claim Association) Conference at the Adelaide Hilton, Adelaide, SA. For more information contact [email protected].
October 23-26 SOA (Society of Actuaries) Annual Meeting at the Cosmopolitan of Las Vegas, Las Vegas, NV. For more information visit www.soa.org.
Regional, national and international underwriting association meetings and non-profit educational events of direct interest to underwriters can be promoted in OTR’s Calendar of Coming Events and at the ALU website - www.alu-web.com. Notify OTR of your meeting details by e-mail to [email protected].
ON THE RISK vol.31 n.4 (2015) 15
Together, we see risk clearly.MIB sheds light on fraud so that members can offer — and consumers
can purchase — affordable life and health insurance. With products like
the MIB Checking Service, Plan-F Follow-up Service, Insurance Activity
Index and the Disability Income Record Service, we help improve
underwriting effectiveness and profitability. Exactly what the industry
needs to…Issue with Confidence.
781.751.6000 ❚ www.mibgroup.comMIB, Inc. provides MIB’s Underwriting Services to members of the MIB Group, Inc.
ON THE RISK vol.31 n.4 (2015)16
FROM THE PRESIDENT: ACADEMY OF LIFE UNDERWRITING
Frank Goetz, FALU, FLMIPresident, ALU
Pacific LifeAliso Viejo, CA
Executive Summary This report updates and summarizes the 2015 activities and accomplish-ments of the Academy of Life Underwriting.
The Academy of Life Underwriting had another pro-ductive year in 2015, serving the educational needs of life underwriters and advancing our profession. I appreciate the opportunity to share with you some of these events and accomplishments.
The current voting members of the ALU Board of Directors are:
• Margaret Taff, Board Chair and Past President, ALU
• Norm Leblond, Treasurer and Past President, AHOU
• Jo-Ann Joliffe, Secretary and CIU representative• Frank Goetz, President, ALU• Tanya Trachenko, OTR representative
OTRAs of January 1, 2016, Kevin Cunningham will be the Editor-in-Chief, with Nancy Atkins as Executive Edi-tor, and Brendan Paradis the Administrative Editor.
The editors, managers and the consultants for ON THE RISK put many hours of work into producing a consistently high quality underwriting journal.
ON THE RISK and the ALU share a mission of provid-ing continuing education to professional home office underwriters, as well as encouraging underwriters to pursue the FALU designation.
2015 Exams and FALUsThe enrollment for the four examinations this year was 1,222 students. The following numbers show students registered and passing for each exam:
There were 728 students from the United States, 148 students from Canada, and 346 students from other countries, including 76 from the Philippines, 50 from the Republic of Korea, and 38 from the People’s Republic of China. In all, exams were written in 29 countries, the newest being Thailand.
The top six companies (worldwide and aggregated) in numbers of students for 2014 were:Manulife Financial – 91, MetLife – 67, New York Life – 58, State Farm – 52, Sun Life – 46, and Pru-dential – 45.
There are 87 new Fellows so far in the Class of 2015: 56 from the United States, 11 from Canada, and 20 from eight other countries. Congratulations to all of the new FALUs!
The Charles A. Will Award is presented annually to the new FALU having the highest average score on all four exams. The 2015 Charles A. Will Award recipient was Kathy Gieryn from Northwestern Mu-tual Life, who was honored at the AHOU meeting in Washington, DC.
For more information about our exams, please visit www.alu-web.com and check out the 2016 examina-tion program. We are currently accepting registra-tions for the April 19, 2016, examinations.
Working Groups – 2015 AccomplishmentsThe ALU groups have been busy with the activities for which they have responsibility: creating new exams, updating textbooks, hosting webinars and an under-writing forum for chief underwriters, communicating the benefits of our programs and conducting surveys.
The Academy of Life Underwriting, the ALU Board
Exam Number registered Number passing
ALU 101 436 303
ALU 201 301 196
ALU 202 249 178
ALU 301 238 157
ON THE RISK vol.31 n.4 (2015) 17
IBU is the market leader in providing solutions that simplify underwriting for the life insurance industry. We put the expertise of experienced professional underwriters to work in a variety of ways that improves turnaround time and reduces costs.
Simplified Issue Underwriting Telephone underwriting for simplified and super-simplified issue products streamlines point-of-sale and non-point-of-sale applications.
Telephone Interviews by Underwriters IBU interviews by underwriters are proven to save time and reduce cost without compromising risk for conditions such as high blood pressure, asthma, diabetes and depression.
APS Summary Solutions Increase production capacity by carving out large APS’s. All IBU underwriters are former home office professionals who write and document as if they were underwriting the cases themselves.
Custom Underwriting Solutions IBU is a nimble, innovative underwriting service provider with the capacity to respond quickly to client needs. Let us put our underwriting talent to work for you.
Contact IBU today!
Call Lincoln Tedeschi directly at 860.295.1190email: [email protected]
IBU, Inc. • 100 Pearl Street, 14th Floor • Hartford, CT 06103
Underwriting Made Easy
Simplifying Life Insurance Underwriting
Improve Time Service
Expand Underwriting
Capacity
Minimize Anti-Selection
Reduce Costs
simpleibuinc.com

ON THE RISK vol.31 n.4 (2015)18
and the editorial team of ON THE RISK recently held our annual planning meeting in Portland, OR. This meeting brought all our group members together to work diligently in preparation for the upcoming year.
There is one group of question writers for each of the four ALU exams. During the annual meeting, each group edits the questions they’ve created during the summer prior to the meeting. One of the objectives of this review process is to ensure the questions are clear in meaning.
The Curriculum Group is responsible for reviewing the textbooks and having authors update or write new chapters. This year the primary focus was providing updates to the ALU 202 and 301 textbooks, along with expanding the review question sections at the end of each chapter to provide additional study aids to our students.
All four of the ALU textbooks are available online at no cost to registered students. They are also free to FALUs accessing the ALU website–alu-web.com. Though the textbooks are available online, hard-copy textbooks are also available; and based on our sur-veys, most students indicate they still prefer to study from a hard-copy book.
The Underwriting Development and Continuing Education Group has been busy this past year, re-sponsible for four webinars on medical topics and a special EKG series.
The Webinars continue to be a popular and cost-effec-tive means of providing continuing education, where one annual payment covers all regular webinars for all underwriters in a company, whether working in the home office or remotely. Individual subscriptions are also available. Seventy-six companies have sub-scribed to the webinar program this year, including 105 registrants for the EKG series.
The 10th Underwriting Forum was held September 13-14, 2015, at the Hyatt Regency O’Hare in Chicago, organized by the Forum Group. This meeting provides a venue for underwriting leaders of direct, reinsur-ance and retrocession companies to discuss risk selec-tion and management issues in a round-table format.
The Marketing Group continued its work of provid-ing information about ALU and its programs to the underwriting and insurance communities. Among other tasks, this included creating ALU brochures, a PowerPoint presentation, and ads and flyers.
The Survey Group conducted a survey regarding underwriter training and continuing education, high-lighted in the September edition of OTR. It provided useful information regarding the training activities industry-wide that will assist chief underwriters and insurance executives in planning for future need as the 23% of underwriters retiring within the next 5 years create a growing void of expertise in need of replacement.
Our Website Manager worked closely with our Managing Director to bring new functionality to our website that we hope you will find helpful. Please check it out at www.alu-web.com!
Retiring Members of the Academy of Life UnderwritingI want to acknowledge all of the contributions made by the members of the ALU who have or will complete their terms at the end of the 2015-2016 academic year:
• Jo-Ann Joliffe – Aurigen Reinsurance – Board Secretary
• Tanya Trachenko – Wawanesa Life – OTR Board Representative
• Jodie Hofmaier – United of Omaha – Secretary• Carolyn Goshorn – Swiss Re America – Website
Manager• Joe Keown – Lincoln Financial – Director of
Exams• Ann Day – Western Fraternal Life – Coordina-
tor, Exam 201• Kayla Grigsby-Bailey – New York Life – Exam
101• Brendan Paradis – MetLife – Exam 101• Dr. Oana Telfer – Sun Life Financial – Exam 201• Joyce Jess – Great West Financial – Exam 202• Michael Hill – RGA Reinsurance – Exam 301• Stacey Jung – Cincinnati Life – Exam 301• Elise Walter – Texas Life – Curriculum Group• Michael Waterhouse – Lincoln Financial – Cur-
riculum Group• Kathleen Alfano – Risk Management Consultant
– Forum Group• Carla Martin – ExamOne – Marketing Group• Tim Miller – Munich American Reinsurance
– Underwriting Development and Continuing Education Group
• Sue Swenson – Prudential – Underwriting De-velopment and Continuing Education
These individuals have served at least 3 years, if not more, working many hours to ensure the success of the ALU program. Thank you for all of your dedica-tion and contributions.
ON THE RISK vol.31 n.4 (2015) 19
Current Members of the Academy of Life UnderwritingI also want to recognize the current members of the Academy of Life Underwriting, which includes those listed above as well as the following whose terms continue beyond 2016, and thank them for their hard work and continued commitment to the education of their fellow underwriters.
Executives • Frank Goetz, FALU – President – Pacific Life
Insurance Company • Margaret Taff, FALU – Past President – Vantis
Life Insurance• Jean Everhart, FALU – Treasurer – Woodmen
of the World • Mark McPheron, FALU – Meeting Planner –
Cincinnati Life Insurance Company• Jodi McDonald, FALU – Director of Curriculum
– Hannover Life Reinsurance• Jennifer Dahl, FALU – Director of Marketing –
RBC Insurance• Sharon Garner, FALU – Director of Continu-
ing Education – American National Insurance Company
Coordinators• Lori Boucher, FALU – Exam 101 Coordinator –
Liberty Life of Boston• Catie Muccigrosso, FALU – Exam 202 Coordina-
tor – RGA Reinsurance Group• Doreen Brynga, FALU – Exam 301 Coordina-
tor – VOYA• Kristin Ringland, FALU – Survey Group Coor-
dinator – SCOR
Exam 101 Group• Lynn Dreist, FALU – Lincoln Financial Group• Zera Langley, FALU – Lincoln Financial Group• Pamela Lewis, FALU – Northwestern Mutual
Life• Danni Pedigo, FALU – Davis Life/Innovative
Underwriting Solutions Exam 201 Group
• Rick Dawson, FALU – FBL Financial• Gay Kemmis, FALU – Securian Financial Group• Libby Limoni, FALU – VOYA Financial• Donna Melfi, FALU – Security Mutual Life of NY• Carol Steckel, FALU – American Family Life
Insurance Company
Exam 202 Group• Christine Klein, FALU – United Life Insurance• Aubree Pham, FALU – American Income Life• Amy Rider, FALU – Optimum Re Insurance
• Joanne Kay, FALU – Sun Life Financial• Marcel Padilla, FALU – Industrial Alliance
Insurance
Exam 301 Group• Debbie Dias, FALU – Canada Life Reinsurance• Stephanie Helle, FALU – Transamerica Life• Sandy Jenum, FALU – River Source Life• Cynthia Landry, FALU – Swiss Re
Curriculum Group• Lisa Gutierrez, FALU – Accordia Life• Jeanne Hollinger, FALU – MetLife• Joanne Lackenbauer, FALU – Sun Life• Vicky Sheehan, FALU – Lincoln Financial Group• Peter Trivella, FALU – John Hancock
Forum Group
• Sherri Boyda, FALU – Berkshire Hathaway Group
• Cindy Mitchell, FALU – SCOR Global Life Americas
Marketing Group• William Dumpman, FALU – Genworth Financial
Medical Underwriting Task Force
• Roland Paradis, FALU – AXA Equitable• Angela Read, FALU – Legal & General America• Paula Romano, FALU
Survey Group• Carol Flanagan, FALU – John Hancock• Roberta Scott, FALU – Woodmen Life• John Sherman, FALU – AIG Global Consumer
Insurance
Underwriting Development and Continuing Education Group
• Hope Adams, FALU – Transamerica Life• John Duff, FALU – BMO Life Assurance• Roy Davis, FALU – Nationwide Financial• Nancy Thorpe, FALU – RBC Insurance
Consultants• Susan R. Sokoloski, MD, DBIM – Medical Con-
sultant – AXA• Cathy Percival, RN, BSN, MBA – Medical Con-
sultant • Marty Meyer, FALU – Editor and Educational
Consultant• Stan Meyer – ALU/OTR Photographer and Cul-
tural Attache’
Administration• Richard Schmidt – Managing Director – Risk
Selection Resources, LLC

ON THE RISK vol.31 n.4 (2015)20
How to Become a Member of the Academy of Life UnderwritingIf you have your FALU designation and are interested in working as a member of the ALU, please send me an e-mail at [email protected] and I can pro-vide more information about what would be involved.
Thank YouFirst, I want to again thank all the members of the Academy of Life Underwriting. The work of all our groups is done by underwriters who volunteer their time outside of their regular work hours. Thank you to everyone for a great job!
The ALU also wants to recognize the many companies that provide support to these underwriters in attend-ing the meetings. This generous support is essential to our organization and is very much appreciated.
Finally, we want to thank the Association of Home Office Underwriters and the Canadian Institute of Underwriters for the support they provide to the Academy of Life Underwriting.
(Left) The ALU Examination 101 Group (left to right): Zera Langley, Lincoln Financial; Pamela Lewis, Northwestern Mutual; Kayla Grigsby-Bailey, New York Life; Lynn Dreist, Lincoln Financial; Danni Pedigo, Davis Life/Innovative UW Solutions; Brendan Paradis, MetLife; Exam 101 Coordinator Lori Boucher, Liberty Life.
(Right) The ALU Examination 201 Group at the ALU Annual Meeting (left to right): seated - Gay Kemmis, Securian Financial; Coordinator Ann Day, Western Fraternal Life; Rick Dawson, FBL Financial; standing - Donna Melfi, Security Mutual Life of NY; Libby Limoni, VOYA Financial; Oana Telfer, MD, Sun Life Financial; Carol Steckel, American Family Life.
ON THE RISK vol.31 n.4 (2015) 21
The Underwriting Development and Continuing Education Committee of the Academy of Life Underwriting announces ……
2016 Webinar Series Line Up February 9: Echocardiograms
Speaker: TBD
May 10: Sleep Apnea
Rod Richie, MD
Texas Life Insurance Co August 9: Predictive Data Analytics and Its Application to Underwriting
Chris Stehno
Deloitte
October 11: Advanced Cancer Underwriting
Steven Rigatti, MD
Mass Mutual
The company annual membership fee for 2016 is based on the number of underwriters in the company:
Company with up to 50 underwriters: $350 Company with more than 50 underwriters: $700 Individual Memberships also available: $100
Membership includes ALL of these benefits: Access to All Previous Webinars Access to Basic Medical Tutorials on ALU’s website, including topics covering seizures, mental illness, heart, hematuria, respiratory, esophagus, pancreas, foreign risks, liver function tests and cancer For more information contact: Sharon Garner at [email protected] or visit the ALU website at www.alu‐web.com An Affordable Option for companies to Provide Employees with Quality Continuing Education

ON THE RISK vol.31 n.4 (2015)22
FROM THE PRESIDENT: ASSOCIATION OF HOME OFFICE UNDERWRITERS – AHOU 2016 – “CAPTURE THE MAGIC” – CHANGE. CHALLENGE. OPPORTUNITY
Executive Summary This article provides an overview of the AHOU’s strategic planning ac-tivities and previews the 2016 AHOU Annual Conference in Orlando, FL.
www.ahou.org
Happy Anniversary, AHOU! In 2016, the Association of Home Office Underwriters will celebrate 15 years as an association serving our underwriting profession. Many of the volunteers who were involved back in the beginning are still working relentlessly to ensure the AHOU remains relevant and adds value for today’s underwriting professional. Part of the value proposition that we provide is educational, through the delivery of our 2016 an-nual conference. The 15th Annual Conference of the AHOU will be held at the Marriott World Center in Orlando, FL. This is a premier facility that promises to offer “a world of possibilities.” The resort is near Walt Disney World and many other Orlando area at-tractions. There is a fantastic pool oasis, featuring two 200-foot winding waterslides, a 90-foot speed slide, kid’s splash park, and multiple pools and hot tubs. It is surrounded by a beautiful 18-hole championship golf course and is home to several award-winning restaurants, a full-service spa and state-of-the-art fitness center.
The Executive Council and Program Committee met on September 27-29, 2015, in Orlando to kick off the planning for this year’s program. Our conference theme is “Capture the Magic – Change. Challenge. Opportunity.” The Program Committee, led by Pro-gram VP Bob Cicchi and AVP Amy Prestegaard, is working on finalizing a program that’s full of inter-esting, relevant and meaningful topics. Our primary focus will be on the future of underwriting–with a little magic thrown in.
On Sunday morning we will be resurrecting a chari-table event that had been organized by Re-Run at past AHOU conferences. This year we will be doing a Relay for Life event on the grounds of the hotel to
raise funds in support of the American Cancer Soci-ety. Plan to join us on Sunday evening and Monday afternoon of the conference for our newly renovated AHOU Marketplace. This event takes the place of the ever-popular Expo. As the name implies, the layout and design have undergone a major renovation and we are sure that you will truly enjoy the change! The Marketplace is a great opportunity for you to meet with your business partners and learn about leading-edge products and services. As always, Monday afternoon and all-day Tuesday workshops will cover a mix of medical, non-medical, financial and manage-ment topics. Monday evening, get ready for a casual outdoor Everglades experience, complete with an airboat! Wednesday morning will see the return of the Study Groups, but these will be complemented by a few concurrent workshops to provide attendees with an educational alternative to the interactive study groups. On Wednesday, our closing speaker is certain to create some buzz and excitement. So please, make plans now to join us in Orlando, May 1 – 4, 2016. We have made a commitment to build a conference that will be educational and FUN!
In preparing for the annual conference this year, I’ve been doing a little research and wanted to share some facts regarding where we have been, where we are and where we are going. Does anyone remember the old “proceedings” books? Yep, we used to print paper books that contained all of the information from our annual conferences. In looking back at these publi-cations from 2001, I found a few interesting tidbits about our history:
Cheryl Johns, FALUPresident, AHOU
AAA Life Insurance CompanyLivonia, MI
ON THE RISK vol.31 n.4 (2015) 23
Capture the Magic
Change.Challenge.Opportunity
May 1 – 4, 2016Marriott World Center
Orlando, Florida
15thAnnual ConferenceAHOU 2016
Knowledge and networKing for today’s underwriting professional
AHOU_OTR_AD_2016.indd 1 10/1/2015 7:18:27 AM
ON THE RISK vol.31 n.4 (2015)24
• The Association of Home Office Underwriters (AHOU) came into existence as of May 1, 2001, and held its inaugural meeting in Seattle, WA, November 10-13, 2002. The Association was formed upon the closure of two predecessor or-ganizations–the Home Office Life Underwriters Association (HOLUA) and the Institute of Home Office Underwriters. (IHOU). The Steering Com-mittee working to create the new combined orga-nization consisted of: Barb Lutz, Linda Shumilas, Nancy Manning and Brian Baxter.
• Officers for the new AHOU were nominated for election at the IHOU meeting October 15, 2001, at the Westin Century Plaza Hotel in Los Angeles. The 2001-2002 officer team: John Krinik, Paul Howman, Daniel Clark, Brian Baxter, Sandy Kelly, Dennis Fagan, Jo Simonetti, Roland Para-dis, Elizabeth Reinhart, Sharon Smith and Gloria Flattum.
• The Home Office Life Underwriters Association (HOLUA) was formed in 1930 and held its first meeting that year in New York. Its final meeting was held in 2001 in Orlando, closing out 71 years in existence. The original charter membership consisted of 24 individuals representing 21 US and three Canadian companies–primarily in the northeast United States.
• The Institute of Home Office Underwriters (IHOU) was formed in 1937 and held its first meeting that year in Birmingham, AL. The char-ter membership consisted of 42 companies, a cross-section of every type and size, throughout the US, Canada and several other countries. Its 65th, and final, meeting was held in Los Angeles in October 2001.
As I looked back through these proceedings, here are a few other interesting things to ponder:
• Our membership numbers have decreased since original inception. We are currently at 1100 members–390 shy of the original 1490 in 2001.
• The importance of volunteers and dedication to the profession hasn’t changed; we need more people who are willing to give of their time to make a difference.
• The number of FALUs walking across the stage has grown–in 2001, 19 were recognized at the HOLUA and IHOU meetings combined. This year we expect close to 75 or more will walk across the stage in Orlando.
I must say, though, the AHOU is so much more than just an annual conference. Over the last few years, we have been working on our strategic plan, built from survey data collected directly from our membership.
To refresh your memory, our four primary strategic focus areas are:
1. Increasing networking opportunities for mem-bers.
2. Expanding educational and professional develop-ment opportunities for members.
3. Increasing member engagement.4. Communicating the value of the underwriting
profession.
Over the past year we have completed a full audit and have published our financials in our efforts to ensure transparency to our membership. We have continued to grow our presence on social media and encourage you to follow us on Twitter, Facebook and Linked-In. Our website and AHOU Connection communications continue to evolve and change in order to better meet the feedback that we receive from our members.
We are currently working on the formal process of filing for incorporation and expect that effort to be completed in 2016. We are also working to further enhance our relationships with local and regional underwriting organizations, AAIM and ALU. Signifi-cant focus on how we can better collectively move our profession forward in a meaningful way has begun and will continue. We look forward to sharing more on this initiative with you in Orlando.
AHOU has identified education and professional de-velopment as one of the key initiatives for potentially providing additional value to our members. As the underwriting environment is rapidly changing, it is important that our profession has access to resources which can support the development of skills and expertise in this ever-increasing data world. Cur-rently, there are limited options in the marketplace. The Executive Committee is evaluating the options available to AHOU by commissioning a feasibility study. An Educational Task Force is being formed to serve as the primary industry information source and manage the feasibility study. This effort is being led by our VP of Marketing, Bill Moore.
I invite you all to join us in Orlando to learn more about the progress that is being made on our strategic plan efforts, to help you prepare for change, challenge, opportunity, and to “Capture the Magic.”
See you in Orlando!
ON THE RISK vol.31 n.4 (2015) 25
Innovative Underwriting Solutions seamlessly blends well trained, competent and producer savvy underwriters into your department without the difficult and expensive hiring, training and management process.
No time and money spent searching for qualified candidates
No backlogs because of too few underwriters for current caseloads
No upset producers due to slow turn around time
No additional fixed or benefit costs (e.g., relocation expenses, matching social security, recruiter fees, vacation etc.)
Experienced, well trained and ready-to work underwriters
Solutions for your immediate, developing and or long-term needs
Senior staff represents nearly 100 years experience in underwriting, product development and distribution
“ I was in need of additional underwriters and IUS provided me with the perfect solution. Their underwriters are highly skilled, experienced, efficient, and professional. They were able to assimilate my company’s underwriting guidelines and philosophy in a very short period of time and immediately made a positive impact. I highly recommend IUS contract underwriters to any company that is in need of acquiring additional staff. ” – B.O.

ON THE RISK vol.31 n.4 (2015)26
Executive Summary The 2015 Annual Scientific Meeting of the Canadian Life Insurance Medical Officers Association (CLIMOA) was held June 7-10 in Québec City. Highlights from the 2015 CLIMOA meeting include a presentation on the differentiation of normal and abnormal ECG findings in athletes; a talk on prognosis of pa-tients with cardioverters-defibrillators; an over-view of fibromyalgia and disability; an update on pulmonary nodules diagnosis and follow-up; and new developments in breast and prostate cancer management.
Tanya Trachenko, MD, FALUOTR Associate EditorWawanesa [email protected]
AN OTR SPECIAL REPORT: HIGHLIGHTS OF THE 2015 CLIMOA ANNUAL SCIENTIFIC MEETING
ATHLETE’S HEARTPaul Poirier, MD, FRCPC, FACC, FAHA, Professor, Faculty of Pharmacy, Quebec Heart and Lung Insti-tute, Université Laval, Québec City, Québec, gave a talk on the differentiation of normal and abnormal ECG findings in athletes and the evolution of screen-ing recommendations designed to prevent sudden cardiac deaths during sport activities.
Dr. Poirier began his presentation by identifying normal cardiovascular adaptations in athletes that include lower blood pressure, bradycardia, left ven-tricular hypertrophy, normal left ventricular diastolic function, and unchanged individual maximal heart rate or maximal blood pressure over the years of training.
According to the Race-Associated Cardiac Arrest Event Registry for the period from Jan. 1, 2000, to May 31, 2010, of 10.9 million runners, 59 had cardiac arrest (0.54 per 100,000 participants). The incidence rate was significantly higher during marathons (1.01 per 100,000) than during half-marathons (0.27 per 100,000) and among men (0.90 per 100,000) than among women (0.16 per 100,000). Only 7% of run-ners younger age than 40 survived the cardiac arrest (2 out of 27). Survival rate for athletes over age 40 was higher at 47% (15 out of 32). Younger participants died mostly from hypertrophic cardiomyopathy, whereas coronary artery disease was the main cause of death in the older athletes.
Dr. Poirier continued his talk by stating that ECG evaluation increases the ability to detect potentially dangerous diseases such as hypertrophic cardiomy-opathy, AV accessory pathways, right ventricular cardiomyopathy, Brugada syndrome and Long QT syndrome. European Society of Cardiology (ESC) classifies changes found on the athlete’s ECG into two groups.
Group 1 represents common and training-related changes:
• Sinus bradycardia• First-degree atrioventricular block• Incomplete right bundle-branch block • Early repolarization• Isolated QRS voltage criteria for left ventricular
hypertrophy
Group 2 lists uncommon and training-unrelated ECG changes:
• T-wave inversion• ST-segment depression• Pathological Q-waves• Left atrial enlargement• Right atrial enlargement• Left axis deviation• Right axis deviation• Right ventricular hypertrophy• Ventricular pre-excitation• Left bundle-branch block• Right bundle-branch block• Long-QTc interval (>440 ms in men; >460 in
women)• Short-QTc interval (<380 ms)• Brugada-like early repolarization

ON THE RISK vol.31 n.4 (2015)28
In 2012, an international panel held in Seattle pro-vided a revision to the above criteria to facilitate the development of universally accepted guidelines for ECG interpretation in young athletes that may also be applicable to black athletes.
Seattle criteria abnormal ECG findings in athletes:• T-wave inversion beyond V2 in white athletes and
V4 in black athletes• ST segment depression• Pathologic Q-waves• Complete left bundle branch block• Intraventricular conduction delay (QRS ≥140 ms)• Left axis deviation• Left atrial enlargement• Right atrial enlargement• Right ventricular hypertrophy patterns• Ventricular pre-excitation• Long QT interval ≥470 ms in men• Long QT interval ≥470 ms in women• Short QT interval ≤320 ms• Brugada-like ECG pattern• Profound sinus bradycardia (< 30 beats/min)• Atrial tachyarrhythmias• Premature ventricular contractions• Ventricular arrhythmias
Dr. Poirier commented that the evolution of ECG abnormality criteria improves the specificity of the ECG in detecting pathology without compromising its sensitivity.
About 9% of athletes will require further investiga-tions based on their symptoms, relevant family his-tory, results of physical examination, ECG or echocar-diogram. The investigations may include a maximal exercise tolerance test, 24-hour Holter monitor, electrophysiology study, cardiac catheterization and a cardiac MRI.
Despite the ongoing debate between the American Heart Association and European Society of Cardiol-ogy concerning routine use of 12-lead ECGs, the vast majority of professional sporting organizations in the United States and Europe incorporate an ECG in their screening protocols. The Canadian Academy of Sport and Exercise Medicine recommendation for all national team athletes is to have screening ECGs done and interpreted by a designated cardiologist trained in athlete-specific ECG interpretation.
In conclusion Dr. Paul Poirier noted that while ECG screening in athletes increases the diagnosis of potentially dangerous diseases, it remains debat-able whether an ECG does more good than harm. False-positive results are often reported due to lack
of ability to accurately interpret athlete-specific pat-terns. Consequently, this leads to inappropriate fur-ther noninvasive and invasive studies, needless use of defibrillators, unnecessary ablations of accessory pathways, as well as inappropriate athletic restriction and unnecessary anxiety.
PROGNOSIS OF PATIENTS WITH CARDIOVERTERS-DEFIBRILLATORS: ARE THEY INSURABLE?Jean-François Sarrazin, MD, FRCPC, FACC, FHRS, Cardiologist/Electrophysiologist, Electrophysiology Fellowship Program, Director, Institut Universitaire de Cardiologie et Pneumologie de Québec (IUCPQ), Université Laval, Québec City, Québec, discussed conditions associated with the risk of a sudden cardiac death and the benefits of the implantable cardioverter-defibrillator treatment.
Sudden cardiac death (SCD) is an unexpected death from a cardiac cause within a short time period, generally within 1 hour from the onset of symptoms. The incidence of SCD in the general population (20-75 years) is 1 in 1,000 and accounts for 18.5% of all deaths. Incident rate amongst competitive athletes is lower and accounts for 0.4 - 0.6/100,000 persons-years. Most of the deaths occur in the low -risk population subgroups with no prior symptoms. SCD is 6 to 10 times more frequent in persons with an underlying cardiomyopathy, in older individu-als, and in men. Dr. Sarrazin added that LVEF (left ventricular ejection fraction) is a reliable predictor of 1-year SCD mortality.
An implantable cardioverter-defibrillator (ICD) is a device able to detect an abnormal heart rhythm and deliver an electric shock to restore a normal heart-beat. Michel Mirowski (1924-1990) was the inventor of a miniaturized defibrillator. He came up with the idea in 1966 after his mentor died suddenly following symptoms of ventricular tachycardia. Levi Watkins performed the first human ICD implantation in 1980. By comparison to the early devices, today’s defibril-lator is much smaller in size. It is associated with low perioperative mortality risk and lasts up to 9 years.
The ICD is implanted for secondary and primary prevention of SCD. Primary prevention refers to pa-tients who have not suffered a life-threatening cardiac episode but are at risk for SCD. Patients resuscitated from a cardiac arrest receive ICD therapy for sec-ondary prevention. Clinical trials showed improved survival rates for patients with ICD in both groups. Patients with multiple risk factors, such as advanced age, history of AF, LVEF < 20% or renal insufficiency, are at higher risk for early mortality after ICD implan-tation; therefore, they must be carefully evaluated for

ON THE RISK vol.31 n.4 (2015) 29
“Consulting Leaders in Latin America for Insurance Companies”
::: Inspections ReportsTelephone Inspections in Spanish, Portuguese,
English and French
::: Simpli�ied Inspection ReportsLow cost alternative for lower face amounts
::: Audit SurveysMeasures client experience , payment methods,
consent to the product o�ered, medical requirements
and more
::: Due diligence for Prospective AgentsIncludes a complete pro�le of the individual that
your company plans to hire
:::
Visit www.iusolutions.com/movil24/7 online follow-up of each casefrom your smartphone and/or tablet
Misiones 1371 4th �oor Montevideo I Uruguay I Tel. (+54-11) 6385.5463 I 6385.5487 [email protected] I www.iusolutions.com
We are leaders in Latin American market: 90 per cent of the life insurance companies request our service
IUSolutions powered by ibu for Tele-Underwriting in spanish communities Helps you improve time service and minimize costs. Powered by the latest secure web-based technologies
New!

ON THE RISK vol.31 n.4 (2015)30
the benefits of ICD prior to implantation.
Dr. Sarrazin then moved to explore the most common conditions for primary prevention of SCD in patients with preserved LVEF.
Hypertrophic Cardiomyopathy (HCM) is character-ized by unexplained cardiac hypertrophy, fibrosis and myocardial disarray. It is the most frequent cause of sudden death in young adults. Its prevalence is 1/500. Annual mortality varies from 1% in the majority of patients to 6% in the selected high-risk group. A recent study by Maron BJ et al. published in 2015 in the Journal of the American College of Cardiology showed historical 50-year reduction in HCM-related mortality to the current rate of 0.5% per year with contemporary management strategies, including ICDs.
Long QT Syndrome is primary an electrical disease. It is characterized by the prolongation of the QT interval on ECG (men - QTc > 440 msec; women - QTc > 460 msec), and a predisposition to syncope, convulsions and sudden death. Its prevalence is 1/2,500. Up to 50% of patients with long QT syndrome have a normal or borderline QT interval at rest. Long QT syndrome accounts for 7-23% of unexplained sudden death and lifetime risk of SCD of 3-5%. Main treatment for LQT1 and LQT2 is β-blocker. Patients with syncope on β-blocker are candidates for ICD primary prevention due to a high risk of SCD.
Brugada Syndrome is characterized by the presence of ST-segment elevation with a negative T-wave in the right precordial leads (V1-V2) without underly-ing structural heart disease. Its prevalence is 0.012 - 0.26% in North America and Europe and accounts for 9% of all cases of unexplained sudden death. Brugada syndrome is usually autosomal dominant with variable penetrance. History of syncope with spontaneous Brugada pattern on ECG is a predictor of an increased risk of sudden death.
Arrhythmogenic Right Ventricular Dysplasia is a genetic form of cardiomyopathy characterized by fibrofatty replacement of the right ventricle myocar-dium. Its prevalence is 1/1,000. Cardiac MRI is a gold standard for the diagnosis of this condition.
Adult Congenital Heart Disease is responsible for sudden cardiac death of 0.1 - 0.2% a year. SCD is mainly associated with tetralogy of Fallot, D-trans-position of great arteries with Mustard or Senning baffles, congenitally corrected transposition of the great arteries, left-sided obstructive lesions, cyanotic Eisenmenger syndrome or Ebstein anomaly.
Patients with high risk of SCD are carefully evaluated to determine the level of risk for SCD based on their medical condition, history of syncope, LVEF, symp-toms including VT, and family history.
Dr. Sarrazin concluded that improvements in primary and secondary prevention have resulted in substantial declines in overall coronary heart disease mortality over the past 30 years. ICDs can prevent sudden car-diac death in different groups of patients, including patients with preserved LVEF.
FIBROMYALGIA & DISABILITY: WHAT’S NEW IN 2015?Mary-Ann Fitzcharles, MD, FRCP (C), Rheumatolo-gist, McGill University Health Centre, Montréal, Qué-bec, provided an overview of fibromyalgia (FM) in-cluding causation, severity, outcome and disability, as well as the highlights of the Canadian FM guidelines.
Dr. Fitzcharles started her presentation by stating that fibromyalgia is a valid condition that is over-diagnosed. She asked her audience to remember the 30% rule and explained that about one-third of the patients report onset of diffuse pain syndrome follow-ing a trigger. Fibromyalgia is responsible for about 30% of disability rates in North America; that is much higher than for rheumatoid arthritis or scleroderma. She added that about 30% of FM patients may be feigning or amplifying symptoms.
Fibromyalgia is believed to be a dysregulation of pain processing in the peripheral and central nervous systems. Its prevalence is 2-5%. FM mostly affects middle-aged women and is often poorly recognized in men, children or the elderly. On average, it takes 5 to 7 years to diagnose.
2012 Canadian FM guidelines introduced three new concepts. Firstly, FM patients are best managed in a primary care setting. Secondly, multimodal treat-ments are ideal with only modest effect from medi-cations. And finally, it is important for the patients to maintain function and remain in the workforce. Dr. Fitzcharles explained that diagnosis of FM and chronic pain conditions is based on the clinical pre-sentation and the report of symptoms that are en-tirely subjective, without any identifiable biomarker. Chronic widespread pain is the defining feature in the FM diagnosis, often accompanied by fatigue, sleep disturbance, mood disorder, cognitive dysfunction and other somatic symptoms. Fibromyalgia is a clini-cal diagnosis based on the careful assessment of the patient’s history and physical examination which is within normal limits. Investigations should be limited to simple laboratory testing, including CBC, ESR, CK,
ON THE RISK vol.31 n.4 (2015) 31
CANADIAN INSTITUTE OF UNDERWRITERS
HARNESS THE PAST ....
UNLEASH THE FUTURE!
Join us June 2 & 3, 2016!Toronto Marriott Bloor-Yorkville
Of 30thAnniversary
AnnualGeneralMeeting
2016
Stacey Grant-Thompson
Dr. Brian GoldmanCBC
Kelly Peters
… are just a few Main Stage
Speakers secured for CIU’s AGM
CIU 2016 30th AGM Program Details &
Registration Package
Available: Spring 2016
Visit us @: www.ciu.ca

ON THE RISK vol.31 n.4 (2015)32
TSH and simple biochemistry. Any additional testing should be dependent on the specific characteristics that may raise a question of some other diagnosis.The tender point count is no longer used to confirm the diagnosis of fibromyalgia. FM is not a homog-enous condition. It is a syndrome that may have an identifiable initiating factor and symptoms, and their severity may be variable. Differential diagnosis includes endocrine conditions (disorders of thyroid and parathyroid), neurological diseases (MS, myas-thenia gravis, neuropathy), musculoskeletal disorders (early inflammatory arthritis, SLE, myositis, PMR, hypermobility), psychiatric conditions (depression, borderline personality, drug-seeking behaviours, so-matization and even feigning of symptoms), as well as effects of some drugs (statins, aromatase inhibitors, PPI’s, bisphosphonates and chemotherapy).
What causes fibromyalgia? About one-third of FM patients are believed to have a genetic predisposition. Persons with a fragile stress response system that is orchestrated by the hypothalamo-pituitary-adrenal axis may be more susceptible to onset of FM when exposed to some adverse event such as psychosocial trauma or physical illness, especially when young. About 30% of the patients experienced an alleged precipitating event.
Dr. Fitzcharles then moved on to discuss the manage-ment of fibromyalgia that is focused on symptom-based treatments and patient-tailored approach to improve symptoms and optimize function. Patients are encouraged to develop self-management strate-gies and be active participants in their health care management. The guidelines for pharmacological treatments include using lowest doses of medications with gradual dose increase and the expectation of modest response to treatment. Using combinations of drugs with different mechanisms of action is often more effective with the caution not to overmedicate. Patients who are passive with external locus of control or untreated prominent mood disorders have poorer outcomes. To measure the progress of treatment, clinicians rely on the individual’s global impression of change, as well as improvement in specific symp-toms associated with FM, such as sleep disturbance, fatigue and mood disturbance. Questionnaires to assess status are not currently used in the clinical setting and should not be used in the insurance or medico-legal settings, as responses may be framed by the patient to emphasize clinical severity. Dr. Fitzcharles asserted that tender points count should not be used for outcome evaluation.
Can patients with fibromyalgia work? Disability rates for fibromyalgia in Canada and the US are 30 to 40%.
Dr. Fitzcharles emphasized that the diagnosis of fibromyalgia should not infer disability entitlement. Since FM symptoms are purely subjective, they can be feigned by patients seeking disability benefits. Neu-ropsychologists believe that about one-third of the FM patients are feigning. In this context, physicians should be cautious and assess function pertaining to daily activities, including leisure and health-related activities, rather than only focusing on the subjective report of severity of symptoms. Fibromyalgia patients are encouraged to remain in the workforce, and if not currently working, should participate in the ap-propriate rehabilitation program with the objective to return to the workforce.
THE PULMONARY NODULE IN THE ERA OF SCANS AND SCREENSAntoine Delage, MDCM, FRCPC, Respirology and Critical Care Medicine, Institut Universitaire de Car-diologie et Pneumologie de Québec, Québec, covered the topic of the pulmonary nodules, including the differential diagnosis, the value of diagnostic exams in the investigation and follow-up, and estimating the probability of a nodule to be malignant.
A solitary pulmonary nodule is a rounded opacity that is less than 3 cm in diameter and is surrounded by a normal lung parenchyma. Neoplasia risk ranges between 5 and 69% depending on the presence of risk factors. A lung nodule that is over 3 cm in diameter is a lung mass and is considered a malignancy until proven otherwise. About 90% of solitary nodules are incidental findings on the chest radiographs. The widespread utilization of the chest computed tomography (CT) scans has greatly increased the incidence of the pulmonary nodules in the past 2 decades. A proper differentiation of benign nodules from malignant is very important due to the fact that an early diagnosis and surgical treatment of pulmo-nary neoplasia are associated with a high survival rate (80% at 5 years). Most common lung malignancies are primary lung carcinoma (non small cell or small cell carcinoma), metastatic cancer (originating as melanoma, breast, digestive or genitourinary tract cancers) and carcinoid tumours. Benign nodules include lesions that are infectious (granuloma, pneu-monia, abscess, mycotic), inflammatory (rheumatoid nodules, Wegener granulomatosis, sarcoidosis), vas-cular (arteriovenous malformations) and congenital (bronchopulmonary sequestration, bronchogenic cysts), as well as hamartoma. Due to the high level of the false-positive results, up to 25% of surgically resected nodules are benign.
Dr. Delage continued by discussing the main risk factors for malignancy that include older age, smok-

ON THE RISK vol.31 n.4 (2015) 33

ON THE RISK vol.31 n.4 (2015)34
ing history, previous neoplasia and occupational exposure to asbestos. During the diagnostic process, clinicians must consider the presence of the follow-ing important symptoms: cough, hemoptysis, fever, night sweats and weight loss. The discovery of the enlarged lymph nodes or clubbing on physical exam is suggestive of neoplasia.
A CT scan with thin (1-3 mm) cuts is necessary in the evaluation of a pulmonary nodule. Dr. Delage examined important radiologic characteristics of the lung nodules including their size, location, calcifica-tions, growth rate, contour and aspect, as well as the importance of these characteristics in the diagnosis.
The size of a nodule measured by the diameter and, even more importantly, by volume directly correlates with the risk of malignancy. Of nodules over 3 cm in diameter, 93 to 97% are malignant. Lesions that are under 1 cm are malignant in less than 15% of cases. However, there is no minimal size to exclude malignancy.
Lung nodules in the upper lobes have a higher prob-ability of malignancy as most primary lung cancers are in the upper portion of the lung. The presence and the pattern of the calcifications can suggest the etiology but rarely can rule out a malignant cause. Organized calcification patterns such as diffuse, central, laminary or popcorn are usually benign but could also be associated with malignancy.
Tumour growth rate is one of the most valuable radio-logical signs that determine an underlying etiology. The volume of the nodule is much more important than the diameter. Lesions with the doubling time of less than 20 days are usually of infectious etiol-ogy. Nodules that double in volume over 400 days are likely benign. Lesions that are stable for over 2 years are also likely benign, with the exception of the nodules with a ground-glass component, which can represent a low-grade malignancy.
The other important characteristic is the contour of the nodule. Pulmonary nodules with spiculated con-tour or nodules that are lobulated are highly suspi-cious for malignancy. Nodules with smooth edges are usually benign but over 30% of them are malignant.
Positron emission tomography (PET) is a useful adjunct in the investigation of indeterminate lung nodules. However, its sensitivity is not adequate for nodules under 8 mm in diameter. PET is also considered more and more as the gold standard in lung cancer staging. Complementary investigations include bronchoscopy with or without endobron-
chial ultrasound and trans-thoracic needle aspiration. Trans-thoracic needle aspiration is usually performed in patients who are deemed inoperable.
Dr. Delage concluded his presentation by providing an overview of the indicated radiological follow-up of pulmonary nodules:
• Stable or benign nodules do not need a longer follow-up than 2 years except for the ground-glass lesions.
• Nodules 8 mm or less should be followed ac-cording to the Fleishner Society guidelines that are based on the presence of three risk factors (smoking history, age and history of neoplasia).
• Indeterminate nodules that are over 8 mm or growing lesions warrant referral to a specialist.
BREAST CANCER: WHAT’S NEW?Brigitte Poirier, MD, FRCSC, Surgical Oncologist, Centre des Maladies du Sein, Hôpital du Saint-Sacre-ment, Centre Hospitalier Universitaire de Québec, Québec City, Québec, provided an overview of the modern breast cancer management based on the new pathologic determinants of survival, the role of treat-ment profiling, and the impact of different treatment modalities on morbidity and return to work times.
Historically, breast cancer prognosis was determined by the size of the tumour and the lymph node involve-ment. The surgical approach was “bigger is better.” In the 1970s and 1980s, NSABP research group questioned the necessity of the total mastectomy. The results of the NSABP B-06 study showed that there is no difference in survival between total mastectomy and partial mastectomy with radiotherapy.
The AJCC Cancer Staging Manual, Seventh Edition (2010) uses TNM classification (T: tumor size, N: lymph node size and number, and M: metastasis) and the staging from I to IV. Dr. Poirier noted that most studies showed that the role of staging in prognosis determination has decreased over time. For example, some patients with the lymph node metastasis have better prognosis than patients who are free from the lymph node involvement.
Current decisional process for cancer treatment includes an evaluation of different elements of the tumour and the response to the treatment. The fol-lowing criteria play an important role in determina-tion of prognosis and treatment selection:
● Tumour morphology● Tumour histological grade● Presence of lymphovascular invasion● Tissue markers (hormonal receptor and Her
2NEU expression)● Tumour gene profile
ON THE RISK vol.31 n.4 (2015) 35
Tumoral morphology is a prognostic factor. For example, the prognosis is different for ductal and lobular invasive carcinomas. Lobular carcinoma has lower recurrence rate in the first 6 years but the recur-rence rate increases after the 6-year mark. Patients with positive hormone receptors have better overall survival. Tumors with HER 2NEU overexpression show the worst prognosis. Breast cancer gene pro-filing provides a classification of the breast cancer subtypes and, as a result, a more refined estimate of survival.
Current knowledge of the multiple prognostic criteria with the variety of combinations for each individual allows for a personalized treatment approach. For example, hormonal treatment is effective in patients with positive receptors, but the choice of treatment is different for premenopausal patients (tamoxifen or Zoladex and aromatase inhibitor) and during meno-pause (Tamoxifen and Aromatose inhibitor). The benefit of the medication use is weighed against the risk of the side effects. For patients with a very good
prognosis, the hormonal treatment is not necessarily given due to a minimal improvement in survival and the importance of side effects for a patient.
Chemotherapy can be given for all kinds of tumours. The decision to give chemotherapy depends on the prognosis and the response to treatment. Genomic techniques that measure gene expression help in identification of the biology-based prognosis profiles and the potential benefit of the chemotherapy. The 21-gene Recurrence Score (oncotype Dx) is used in the US and Canada. It calculates tumour scores based on the tissue analysis and classifies them into three categories. If the score is less than 18, the addition of chemotherapy seems not to improve the prognosis. The benefit of the chemotherapy is equivocal for pa-tients with the score between 18 and 30. The addition of chemotherapy improves the prognosis for women with the score over 30.
Chemotherapy is an aggressive treatment that causes multiple side effects (nausea, vomiting, diarrhea,
FIRST FINANCIAL UNDERWRITING SERVICES, INC. “Inspection Reports Should Answer Questions NOT Raise More Questions”©
20+ Years of EXCELLENCE www.firstfin.com
ONE SHOP FOR ALL YOUR INSPECTION RELATED NEEDS
Specializing in Electronic Inspection Reports (Filtered EIR)
MOST DETAILED FINANCIAL INSPECTIONS MOST ACCURATE CRIMINAL RECORDS, SPECIAL SSN TRACE REPORTS, SPECIALTY COURT RECORD SEARCHES
BUSINESS BENEFICIARY REPORTS WITH FULL FINANCIAL DETAILS
FULL IN‐HOUSE SPANISH SERVICES WHICH INCLUDES CRIMINAL COURT RECORDS AND CREDIT REPORTS IN MEXICO
THIRD PARTY REPORTS & EIRS ON LOWER AMOUNTS FOR FILTERED IDENTITY AUTHENTICATION AND FOR FRAUD DETECTION
FULL INSPECTION / APS TRANSLATION SERVICES IN HONG KONG & THE ORIENT
TAILOR MADE QUESTIONNAIRE AVAILABLE ON REQUEST
RECORDED INTERVIEWS AT NO ADDITIONAL COST
TELEPHONE INTERVIEW REPORTS ENCRYPTED ORDERING AND TRACKING SYSTEM INTERVIEWS IN LANGUAGE OF CHOICE CUSTOMIZED ELECTRONIC BILLING DETAILED PFQ & STOLI QUESTIONNAIRE FOREIGN LANGUAGE APS TRANSLATIONS
(SPANISH, MANDARIN, CANTONESE, etc.) CREDIT CHECKS MOTOR VEHICLE REPORTS We invite you to call our office to discuss your basic, intermediate, specialty, complex, international cases, APS translation and filtered EIR needs. Live agents available from 8:00 AM to 8:00 PM Eastern Monday through Friday. With over 200 years of combined experience, we can help you assess the risk at hand.
Contact Information EMAIL: [email protected]
TELEPHONE NUMBER: 1 (800) 570 3477 FAX NUMBER: 1 (800) 571 3477

ON THE RISK vol.31 n.4 (2015)36ON THE RISK vol.31 n.4 (2015)36
constipation, febrile neutropenia, TVP-embolism, hair and nail loss), as well as during and post-treatment (physical and mental fatigue, neuropathy, menopause, cardiac risks, secondary neoplasia and musculoskeletal pain).
Hormonal therapy also causes side effects including hot flashes, joint pain, insomnia, vaginal dryness and decrease in bone density. Fatigue is a common side effect of the radiation treatment that can continue for months after the treatment is finished. Differ-ent drugs cause different side effects. Doctors and scientists are continually working on selecting new drugs and combinations of existing treatments that have fewer side effects.
Dr. Poirier concluded her presentation by noting that the effects of the cancer treatment, as well as the patient’s emotional response to the cancer diag-nosis, impact their return to work time. Some cancer patients will continue working while receiving treat-ment, but others will stop working because of the challenging situation.
PROSTATIC CANCER: NEW DEVELOPMENTSYves Fradet, MD, FRCS(c), President and Chief Medical Officer, DiagnoCure, Québec City, Québec, explored the rationale of the recommendations by the Canadian Task Force on Preventive Health Care (CTFPHC) on screening for prostate cancer with the PSA test, new developments in screening and prog-nostic tests, as well as clinical approaches to prostate cancer treatments.
Dr. Fradet started his presentation by comparing recommendations by the Canadian Task Force on Preventive Health Care for prostate and breast can-cers for ages 50 to 70. He indicated that the screening with the PSA test is not recommended for men aged 55-69 years (weak recommendation; moderate qual-ity evidence). However, for women aged 50-69 years, CTFPHC recommends a routine screening with mam-mography every 2 to 3 years (weak recommendation; moderate quality evidence). Dr. Fradet questioned the rationale for the breast cancer screening recom-mendations, based on the current evidence indicating that screening mammography has led to a substantial over-diagnosis with only marginal reduction of the advanced breast cancer rate detection, yet the recom-mendation for the screening mammography stands. The PSA testing has also produced a higher rate of cancer diagnosis, but at the same time it has led to a decline in the prostate cancer mortality evidenced by the studies conducted mostly in Europe.
Dr. Fradet then moved on to compare the watchful waiting approach in prostate cancer management to active surveillance. There is no intention to cure with the watchful waiting follow-up. The only treatment that might be used is the palliative treatment and the treatment for the metastasis. Active surveillance is a close monitoring with the intention to cure. It often results in a delayed surgery if the person’s cancer is growing or becoming more aggressive. Radical pros-tatectomy reduces the absolute mortality risk for the early prostate cancer cases when compared with the watchful waiting approach by 12.7%. The 25.5% risk reduction is observed in younger men (< 65 years). Remarkably, patients with low-risk tumours benefit from the prostatectomy in a way of reducing the absolute mortality risk by 15.6%. Had it not been for the PSA testing, Dr. Fradet noted, more than 30% of men would be diagnosed with prostate cancer at the metastatic stage.
In the absence of a reliable imaging test for prostate cancer, physicians use TRUS (trans-rectal ultra-sound) with the biopsy resulting in a cancer detection rate of 20 to 30% for a 6-core biopsy and 27 to 40% rate for a 12-core biopsy. This procedure, however, carries a risk of infection and post-procedure bleeding often requiring hospitalization. MRI could be used for the non-invasive prostate cancer surveillance but the cost of this investigation is high.
Considering that about half of the new prostate cancer cases are low-grade tumours, the current goal is to develop a test or an algorithm that would allow ac-curate risk prediction of an aggressive prostate cancer for an individual patient. One of the examples, PCA3 testing, proves to be a reliable and cost-effective way for risk calculation. Another challenge is to choose the risk-appropriate treatment by carefully weighing the benefits and the side effects. Prostatectomy, radio-therapy and brachytherapy have different recovery times, risk of incontinence, risk of impotence and risk of developing secondary cancers.
Dr. Fradet concluded his presentation by predicting that we might see an increase in the number of newly diagnosed advanced prostate cancer cases as a result of following the CTFPHC recommendations for PSA screening. Given the exponential cost of treating metastatic prostate cancer patients who will still die from the disease, dropping the early detection of prostate cancer by PSA testing may not be a sound economic decision.
Opinions expressed within this article published in ON THE RISK do not represent official opinions of CLIMOA. Such expressions only represent the views of the author or the speakers whose presentation remarks are herein summarized.

ON THE RISK vol.31 n.4 (2015) 37
US AGE AND AMOUNT REQUIREMENTS & PREFERRED CLASSIFICATION CRITERIA TRENDS
Executive Summary Data from companies in the US life insurance marketplace was analyzed to identify trends in routine age and amount re-quirements and preferred classification. Compa-nies included in the analysis were top competitors in the term life and universal life markets based on industry sales volume reports and other com-petitive intelligence gathering measures. This article summarizes the changes at a high level.
Dee Davis, AALU, FLMI Michelle Privett, FALU, RN [email protected] [email protected]
Swiss Re American Holding CorporationFort Wayne, IN
Industry Trends• Companies with teleunderwriting programs were
more likely to make changes to their guidelines by introducing lower testing thresholds for certain requirements or by adding (or discontinuing) requirements at certain age and amounts.
• Fewer companies rely on the full scope of paramed and medical exams, and the use of prescription profiles and elderly functional and cognitive test-ing has increased.
• Companies modified the types of laboratory re-sults required by increasing their use of hemo-globin A1c, NT pro-BNP and PSA.
• Preferred criteria showed a mix of tightening and loosening of criteria.
• Changes in both areas of age and amount require-ments as well as preferred classification criteria reflected the need to stay competitive in the US life insurance market.
Trends were analyzed regarding age and amount requirements and preferred classification criteria for fully underwritten business, looking at ages 25 and older. More than 30 companies in the US life insurance marketplace were included in the study.
Age and Amount Requirement Trends Age and amount guidelines used on a routine basis from 2010 to 2014 were compared to assess changing patterns of use over time. There was an equal mix of companies with a teleunderwriting process and tra-ditional application process. Numerous noteworthy trends were found across a variety of requirements. There was a slight increase in the use of physical measurements (also called vitals, vital signs or ab-breviated paramedical exam) over the use of full para-medical examinations. The percentage of companies
using MD exams also declined.
Drill-down interviews were highly favored over less invasive questions for both traditional and teleun-derwriting processes. Additionally, teleunderwriting interviews that included both Part 1 and Part 2 of the application were more popular than interviews which included Part 2 history only.
Laboratory testing showed several trends. Fewer com-panies were using oral fluids as a requirement. More companies used hemoglobin A1c, NT pro-BNP and PSA to assess risk, especially at older ages. There was limited use of C-reactive protein (CRP) and complete blood cell counts (CBC).
Companies relaxed their use of treadmill stress tests at age 75 and older. Treadmill testing has been declin-ing for several years. Cost of the test, inconvenience for the applicant and turnaround time are defining factors on why companies choose to remove treadmill testing from their age and amount requirements. Companies also relaxed their use of electrocardio-grams at the younger ages (ages 35 and 55).
Very few companies were found to require chest X-rays (CXR), and overall use declined at older ages.

ON THE RISK vol.31 n.4 (2015)38
However, some companies still continued to see the value of the CXR for smokers and tobacco users.
Prescription profiles increased in popularity. More companies used the profile as a routine age and amount requirement, and testing thresholds were lower across all ages.
Attending physician statements (APS) continued to be important in risk assessment. There was a general increase in the number of companies with published rules for APS requirements. More companies required the APS on all applicants at age 75 and over, and testing thresholds tightened up (were lower) for this age bracket.
In addition to obtaining APS requirements for the elderly, companies demonstrated a greater use of functional and cognitive testing. There was a dramatic increase in the use of this testing by the examiner and less reliance on self-reported information provided by the applicant or taken over the phone.
Non-medical requirements also demonstrated some notable trends. More companies required financial justification through the use of a financial question-naire or via third party financials. This increase was seen across the board at all ages. A small percentage of companies were using the federal tax form 4506T in order to obtain tax returns from the federal gov-ernment.
Trends for inspections and MVR (motor vehicle records) were also observed. Although there was a slight decline in the use of commercial inspection reports, a moderate percentage of companies used background checks across all age groups in contrast to commercial inspection reports that require third-party interviews to confirm applicant history and financials. Background checks are electronic database queries that confirm the applicant’s identity, criminal activity, medical, financial or employment records. A small percentage of companies continued to see value in obtaining face-to-face inspection reports for the larger cases. Motor vehicle records were also shown to have a greater use at all age groups.
Preferred Classification and Criteria Trends The number of non-tobacco (NT) preferred rate class-es and preferred criteria for the best NT preferred class were also reviewed for the years 2010 and 2014. Companies appeared to be taking more of a stream-lined approach in determining the number of NT classes to offer on products. Most companies offer-ing term insurance had three NT preferred classes.
Although most companies offering permanent insur-ance only had two NT preferred classes, there was an increase in the number of companies with three NT preferred classes for permanent coverage.
The analysis showed no change in regards to how companies look at nicotine use. The 5-year look-back period remained the gold standard when it came to preferred classification for best non-tobacco rates.
Build continued to be an important part of preferred criteria. Obesity maximum ranges measured by body mass index (BMI) were only slightly looser in 2014, demonstrating that companies appeared to remain concerned with the effect of obesity on mortality. A notable change was the increase in companies with thresholds for underweight or low BMI as preferred criteria.
The analysis noted systolic blood pressure thresholds were slightly more conservative on average than in the past. This movement was mostly driven by changes at the younger ages. Diastolic thresholds remained unchanged on average, although there was loosening at the older ages among a few outlying companies.
Several trends were noted regarding cholesterol us-age. The use of cholesterol/HDL ratio as preferred criteria increased, while the use of total cholesterol declined slightly. Thresholds for total cholesterol were slightly higher (looser), which was in contrast to prior trends where companies were tightening their numbers. There was also an increase in the number of companies with preferred risk criteria for low total cholesterol.
Criteria for treated blood pressure and cholesterol also demonstrated some relaxation as key criteria. More companies allowed treatment for both high blood pressure and high cholesterol into their best preferred rate class. This finding for treated blood pressure contrasted with prior trends where compa-nies were moving to exclude treatment for the best preferred rate class.
Family history criteria tightened in some areas and loosened in others. Fewer companies were disregard-ing family history of stroke, but an increasing number of companies were disregarding family history of diabetes. There was also a relatively large increase in the number of companies who disregard family history altogether for applicants age 75 and older.
On the non-medical side, preferred driving criteria were also reviewed. There was a near 50-50 split in the number of companies allowing one violation vs.

ON THE RISK vol.31 n.4 (2015) 39
two violations in the best preferred rate classes. There was an increase in the use of a 3-year look-back period on motor vehicle reports (MVR), but the 5-year look-back period remained the gold standard for driving under the influence (DUI) violations.
Changes in the handling of private aviation and avocation risk were also noted. Nearly 60% of the companies did not allow ratable activity in their best preferred rate class. A flat extra premium or exclusion rider may be required. In regards to avocations, the most common practice was to exclude all forms of hazardous activity in the best class. However, there was an increase in companies that allowed a flat extra premium or exclusion rider.
Other notable findings included criteria to qualify for best NT preferred rates. Most companies maintained a look-back period that was 7 years or longer for personal histories of alcohol and drug abuse. Where it concerned personal cancers, most companies al-lowed applicants with a history of non-melanoma skin cancer to qualify in the best NT preferred class.
SummaryThe trend analysis on age and amount requirements showed a number of interesting findings. There was less use of full paramedical examinations, and slight increase in the use of physical measurements and drill-down interviews. Prescription profile use increased as did elderly functional and cognitive test-
ing. Fewer resting ECGs were required at the younger ages and fewer treadmills at the older ages. Use of NT pro-BNP and hemoglobin A1c grew in popularity, and MVR use remained strong. Companies required more financial justification for insurance, increased the use of the 4506T tax return forms, and switched to back-ground checks from traditional inspection reports.
Preferred classification trends showed an increase for the number of non-tobacco rate classes for permanent products. Changes to best class NT preferred criteria were just as interesting. There was no change for how companies look at nicotine use. Companies began adding low BMI as criteria, tightened blood pressure criteria at younger ages, and actually loosened criteria for blood pressure at older ages on permanent plans. An increased use of criteria for low total cholesterol was seen, and more companies allowed treatment for both high blood pressure and high cholesterol in the best preferred class. Companies paid more attention to family history of stroke, less attention to family history of diabetes, and disregarded family history for applicants age 75 and older. In the non-medical arena, more companies used a 3-year look-back pe-riod for moving violations, but the 5-year look-back remained the gold standard for DUIs.
US life insurance companies continue to work dili-gently to refine their underwriting guidelines and pre-ferred risk categories to maintain a competitive edge.
The ALU Examination 202 Group at the 2014 ALU Meeting (left to right): seated - Joanne Kay, Sun Life; Co-ordinator Catie Muccigrosso, RGA Reinsurance; Aubree Pham, American Income Life; standing - Joyce Jess, Great West Financial; Amy Rider, Optimum Re; Christine Klein, United Life; Marcel Padilla, Industrial Alliance.
ON THE RISK vol.31 n.4 (2015)40
• Provides risk-based scoring of all laboratory results in combination with build and blood pressure
• Identifies high-risk cases requiring review and stratifies standard or better risks into appropriate preferred categories, based on their mortality risk and your underwriting classes
• Accounts for age and gender so that the relative mortality for each applicant, compared to peers, is correctly identified
• Scores every component of the lab profile, including reflexive tests and drugs of abuse
• Delivers an applicant report that includes the risk (in debits or credits) for each test, as well as the total score, enabling explanation of your decisions
• Underlying science and scoring based on years of CRL published research (Journal of Insurance medicine)
Smart Score®changes that!
Q.
Smart Score® will improve your bottom line with better mortality and allow your underwriters to focus on cases where they add maximum value.
Greater Insights. Better Outcomes.®
Based on early-claims file review of several respected insurers,
far too many!
How many early claims are caused by
missed lab results? A.
Clinical Reference Laboratory | 800.882.1922 | www.CRLcorp.com/insurance

ON THE RISK vol.31 n.4 (2015) 41
These numbers tell a story. One we both can be proud of. A story ofhardwork, determination and commitment. Working together wehave helped millions of families. But our work isn’t done. We canstill help 95 million more Americans without life insurance protecttheir families. We are committed to this challenge by providingyou with innovative tools and simplified processes — resulting in amore satisfied applicant.
Committed everyday, with:• High-quality, cutting-edge laboratory results for all applicants.• More applicant choices for communication, exam locations andscheduling options.
• The nation’s largest network of paramedical service centersand dedicated mobile examiners.
• Proud supporter of LIFE Happens and Life InsuranceAwareness Month.
We are committed to you, our industry and helping every familybe protected with life insurance. Stronger together.
ExamOne.com I 855-324-7468*Based on applicants from July 2014-June 2015. To learn more about hidden healthy contact ExamOne.
Quest, Quest Diagnostics, ExamOne, any associated logos, and all associated Quest Diagnostics registered or unregistered trademarks are the property of Quest Diagnostics. All third partymarks - ® and ™ - are the property of their respective owners. ©2014 Quest Diagnostics Incorporated. All rights reserved.
Hidden Healthyapplicants identified*
applicants have accessedlaboratory results online
95 Millionuninsured Americans (LIMRA)
Billionvalue of policies ExamOne isentrusted with every year
#Committed2tell us how you are committed toour industry on social media.
800K
663K
$844
X1 Commit Ad 3.qxd:Layout 1 9/1/15 2:49 PM Page 1
ON THE RISK vol.31 n.4 (2015)42
About the AuthorsDeatra (Dee) Davis, AALU, FLMI, is Vice President, Manager and Researcher, Applied R&D, with Swiss Re America Holding Corporation, where she helps clients understand the value of requirements used during the underwriting process, and how those requirements compare to industry benchmarks. Her work includes conducting competitive intelligence and protective value studies to support the Life Mortality System, a com-ponent of Swiss Re’s Integrated Costing Environment, and she developed a cost benefit tool that measures underwriting and mortality costs.
Dee’s life insurance career spans 30 years and includes underwriting guide development and various leader-ship positions as a life insurance underwriter and researcher at Hawkeye National Life Insurance Company and Lincoln Re. She graduated with honors from Indiana Wesleyan University with a Bachelor in Manage-ment degree, is an Associate of the Academy of Life Underwriting, and earned the Fellow, Life Management Institute designation from The American College.
Michelle Privett, FALU, RN, MS, FLMI, PCS, is a master’s prepared registered nurse with over 15 years of underwriting experience and 20 years of nursing experience. She has worked in the areas of emergency medicine, urology, nephrology, cardiac telemetry, public health and intensive care with a current interest in hospice care. Prior to entering the profession of underwriting, Michelle served as chief kidney transplant coordinator for two large academic medical centers in West Virginia and Chicago. She achieved certifica-tions as a nationally certified Nephrology Nurse and a nationally certified Clinical Transplant Coordinator (solid organ). She is a Fellow of the Academy of Life Underwriting (FALU), a Fellow of the Life Management Institute (FLMI), and has obtained her Professional in Customer Service designation from LOMA. She cur-rently serves as an OTR Contributing Editor and has published in ON THE RISK and Life Insurance Selling magazine. Michelle served on the Academy of Life Underwriting Curriculum Committee and has presented for various nursing and underwriting groups.
(Right) The ALU Examination 301 Group at the ALU Annual Meeting (left to right): seated - Stephanie Helle, Ae-gon/Transamerica; Michael Hill, RGA Reinsurance; Sandy Jenum, Ameriprise/RiverSource Life; standing - Coordina-tor Doreen Brynga, ING; Stacey Jung, Cincinnati Life Insurance Co.; Debbie Dias, Canada Life Re; Cynthia Landry, Swiss Re America.
(Left) The ALU Forum Group at the ALU Annual Meeting (left to right): Cindy Mitchell, SCOR Global Life; Website Manager Carolyn Goshorn, Swiss Re; Sherri Boyda, Berkshire Hathaway Group Reinsurance; (not pic-tured - Coordinator Kathleen Alfano, National Life Group).

ON THE RISK vol.31 n.4 (2015) 43
AVOIDING MATERIAL MISREPRESENTATION AND FRAUD IN LIFE INSURANCE (OVERVIEW, APPLICATION DESIGN AND RED FLAGS)
Executive Summary The negative financial im-pact of material misrepresentation and fraud on life insurance companies is daunting. In this article we’ll revisit definitions of anti-selection and fraud, discuss the role of application design in combating material misrepresentation and fraud, review MIB and application-related red flags, and help readers reduce their companies’ financial exposure in these areas.
Keith Brown, FALURisk Management & Chief UnderwriterGen ReStamford, [email protected]
In my role as Chief Underwriter at a reinsurance com-pany, the more I travel, visit clients, meet potential clients and attend industry meetings, the more I am surprised to hear so many companies express concern about dealing with material misrepresentation and fraud during the application and underwriting pro-cesses. Insurance industry meetings routinely have sessions on fraud. I’ve heard estimates regarding the percentage of new business applications affected by material misrepresentation or fraud ranging from 10% to 50%, depending upon company. These are frightening percentages, especially when we take the numbers a step further and consider the potential death benefit risk involved. For example, even if the percentage is as low as 10%, writing $1 billion of face amount volume in a year could mean that as much as $100 million of that risk involves material misrepre-sentation or fraud.
Anti-Selection and FraudAnti-selection is a term used to describe situations, either medical, non-medical or financial, where an applicant, proposed insured or agent conceals, falsi-fies or materially misrepresents information at the time of application, in a way that financially injures an insurance carrier. This term includes simple avoid-ance of detection where one party has information that another party doesn’t have.
In legal terms, fraud is generally defined as an in-tentional misrepresentation of existing material fact made by one person to another with knowledge of its falsity, and made for the purpose of inducing the other person to act — a misrepresentation upon which the other person relies with resulting injury or damage. Fraud may also be made by an omission or purpose-ful failure to state material facts, a nondisclosure that makes other statements misleading.1
Anti-selection and fraud appear in several forms or patterns of opportunity. These can involve a customer
acting alone, an agent acting alone, or multiple parties acting in collusion with one another. Collusion is a secret agreement to cheat or deceive others, especially for fraudulent or treacherous purposes. Collusion can occur at any time during the sales process, so the underwriter must not only be alert but have the imagination needed to make the associations and connections that reveal anti-selection practices.
Application DesignApplication question design is essential in helping avoid material misrepresentation and fraud. If your application forms have not been updated in recent years, they may be full of holes that attract anti-selection. Some quick tips:
• Consider checking with the state departments of insurance (DOIs) with whom your company works to see if they would consider approving an additional question along the lines of “Within the past 10 years, have you had or used a different name or names other than that indicated in Ques-tion _____ above? If yes, please list all names and dates used.” This would enable companies to avoid fraud by obtaining underwriting informa-tion for each name as appropriate (e.g., running checks on MIB, pharmacy databases and order-ing additional attending physician statements, etc.). To illustrate this vulnerability, I have seen cases where individuals changed their names in an effort to hide criminal history. We also saw
ON THE RISK vol.31 n.4 (2015)44
an inquiry recently on someone in her 30s who had coverage under five different names due to multiple marriages. The inquiring company was only aware of the current name.
• Be specific in designing application questions. For example, some companies ask if someone “abused” alcohol or drugs. “Abused” is not specific enough, as one individual’s abuse may simply represent another’s enjoyment. Make your questions quantitatively precise.
• Consider partnering with a behavioral economist to help you design your forms. A behavioral economist may be able to help frame questions optimally to minimize anti-selection and fraud. In working with state DOIs and a behavioral economist, you may discover that placing the sig-nature/attestation in a different section of an ap-plication may be a stronger fraud deterrent than requiring signatures and attestations at the end of a document, as is the common practice in the life, disability and critical illness industries. The use of a behavioral economist may be of particular help to companies considering expansion into the accelerated (simplified) underwriting market.
Note: LabCorp announced an initiative to let consumers order their own tests.2
As of this writing, approximately 35 states allow consumers to order some (or all types) of tests without a physician order. In view of this, companies may want to also check with the state DOIs with whom they work to see if they will approve an addi-tional question along the lines of “Within the past 5 years, has the proposed insured had any other diagnostic tests, such as an electrocardiogram (EKG), X-ray or lab work, other than those related to the Human Immunode-ficiency Virus (AIDS virus)?” For any “yes” answer, details may be requested, such as name, address and telephone number of the place where the tests were performed, and/or name, address and telephone number of the medical professional or facility pre-scribing the tests, and dates of the tests.
Extensive MIB ActivityApplicants with extensive MIB histories should be underwritten very conservatively, both medically and financially. Underwriters should be especially vigilant concerning three specific MIB red flag patterns:
1. Concealment of an undisclosed impairment.2. Stacking of coverage to include the avoidance of
additional underwriting requirements.3. Early lapse, churning or possible rebating sce-
narios.
Stacking of coverage is the planned purchase of multiple policies for smaller face amounts from nu-merous carriers rather than one policy for a larger face amount from one carrier. Stacking can be done concurrently or over a number of months or years to avoid requirements or the development of negative risk assessment information that would be uncov-ered if a proposed insured were to apply for a higher face amount. To do it concurrently, for example, a proposed insured and/or agent may indicate that he is applying for $100,000 from each of five different companies but will only choose one policy for a maxi-mum of $100,000. After placing the first policy, little if anything can prevent the applicant from placing other policies that were also approved.
An underwriter who suspects this activity should be sure to check with the other carriers noted in the 30 to 60 days following to see whether or not additional
policies were placed. If stacking is discovered, the underwriter should work with his legal department on the appropriate action, which may involve rescission and/or termination of the agent’s selling contract. Applicants who stack coverage can be expected to have knowledge of adverse non-medical, medical or financial history that would negatively impact insur-ability and that remains unknown to the insurance carrier(s).
To avoid underwriting requirements that would detect adverse information, an individual may apply for coverage amounts below which additional under-writing requirements would be necessary. This sce-nario occurs with guaranteed and simplified issues,
Additional Red Flags> Applicants haven’t listed any other coverage being applied for, but the
“lab slip” or “lab ticket” notes multiple companies. > A company’s analytics for producers and agencies indicate face
amounts that consistently fall just below the threshold for certain financial and/or medical requirements. If not running such analytics, it is likely your company is experiencing some degree of anti-selection. For companies that lack the technology to implement such analysis, consult with your vendors for possible solutions.
> A producer repeatedly fights providing third-party verification of finances.

ON THE RISK vol.31 n.4 (2015) 45
as well as on fully underwritten business, when the applicant wants to avoid published age and amount requirements, such as paramedical exams, lab work, avocation questionnaires, MVRs, inspection reports, credit reports, and 1040 Federal Income Tax verifica-tion of income on higher face amount applications.
It takes a lot of detailed work by multiple departments to reduce a company’s financial exposure to insurance fraud. But the payoff could be huge. In future articles
I will address topics such as reinstatement challenges, lack of medical history at older ages, underwriting foreign nationals, rebating and churning, as well as underwriting the self-employed. Stay tuned.
Notes1 definitions.uslegal.com/f/fraud.2 www.lifehealthpro.com/2015/04/20/the-doctor-is-out-labcorp-
to-let-consumers-order-o?eNL=5535a9c5150ba03557e78bd7&utm_source=LifeHealthProDaily&utm_medium=eNL&utm_campaign=LifeHealthPro_eNLs&_LID=97625306.
About the AuthorKeith Brown, FALU, MSM, CLU, ChFC, FLMI, RHU, joined Gen Re in 2014 and is responsible for assisting in the development and implementation of the Individual Products Division strategy for ceded life, disability income and critical illness reinsurance.
Keith has over 30 years’ experience in the insurance industry. Prior to Gen Re, Keith was most recently Vice President and Chief Underwriter at Western & Southern Financial Group in Cincinnati, OH. Previously, he worked as Vice President of Underwriting and New Business at Security Mutual Life of NY, and he began his career as an underwriter at Mass Mutual in Springfield, MA.
He currently is a member of the Impaired Risk Underwriters Association, serves on the ACLI Genetic Testing Task Force, and is a member of the AHOU Planning Committee. Keith earned his BA in English from Bow-doin College in Brunswick, ME, and his MS in Management from the American College in Bryn Mawr, PA.
The ALU Curriculum Group at the 2015 ALU Annual Meeting (left to right): seated - Vicky Sheehan, Lincoln Financial; Joanne Lackenbauer, Sun Life; Director of Cur-riculum Jodi McDonald, Hannover Life Re; Lisa Gutierrez, Accordia Life; standing - Peter Trivella, John Hancock; Michael Waterhouse, Lincoln Financial; Elise Wal-ter, Texas Life; Jeanne Hollinger, MetLife.
The Medical Task Force at the ALU Annual Meeting: (left to right) Paula Romano, (retired-Prudential); Angela Read, Legal & General America; (not pictured - Roland Paradis, AXA).

ON THE RISK vol.31 n.4 (2015)46
THE SIMPLIFIED ISSUE CONUNDRUM
Executive Summary Conundrum: noun; any-thing that puzzles. For years insurers have been looking to simplify the life insurance purchase experience. From ease of sale to hassle-free un-derwriting, the goal is to make the sale a simple financial transaction. Many compare simplified issue life insurance sales to the purchase of mu-tual funds or 100 shares of Apple stock. The pro-ducer “drops a ticket” and the stock certificate is delivered within days rather than weeks. But how simple should the life insurance purchase process be? It can be a large, complicated financial and health-related process with significant financial implications for the consumer as well as the in-surer. This article will explore the issues associ-ated with simplifying the issue and underwriting process. Driving forces behind this development, implications for risk selection, pricing and our industry will be explored. It truly is a conundrum.
Darren M. Dombrosky, FLMI, ACSSenior Vice President, National AccountsExamOneLenexa, [email protected]
Background: Introduction to the Conundrum of Simplified Issue (SI)One goal of SI insurance is to enable companies to further penetrate the middle market. Numerous surveys have shown that a significant percentage of middle market consumers, sometimes defined by annual household income of $35,000-$75,000, are uninsured or underinsured. They may not be as financially savvy as more affluent customers and may be intimidated by the entire life insurance purchase process.
Problematic as well is selling to the “millennials,” (in-dividuals born between the early 1980s and the early 2000s). Millennials don’t conform to the purchasing habits of their parents. They want to purchase on their own terms. They may not value an agent. They are computer-savvy and may choose to purchase financial products online at midnight. They want to control the process.
For insurers, an additional goal may be to enhance utilization of underwriting engines by further auto-mating the underwriting process. Simplified issue may offer opportunities to reduce acquisition ex-penses by spending less on traditional underwriting requirements and potentially reducing staff.
The industry is seeing renewed interest in SI prod-ucts, but this time with a few twists. Unlike traditional simplified issue products that reduce face amounts for the same premium as a fully underwritten policy or adjust mortality assumptions, agent compensa-tion, product profitability or a combination of these and other factors, the new generation of SI products may claim to have the same mortality assumptions as fully underwritten products while paying “full” agent compensation and yielding similar ROEs as full underwriting. These products may cause some to ask:
How is this possible? Can you eliminate traditional underwriting requirements with no impact on mortal-ity, compensation and profitability? Every company must decide what level of underwriting works for it. Each needs to evaluate which underwriting levers can be pushed and pulled and the consequences associ-ated with every change.
The rest of this paper provides a blueprint for items that companies must consider when developing, marketing and underwriting this next generation of SI products. Data is the key. Companies must measure the impacts of changes from start to finish, and share this data across the underwriting, actuarial, financial and marketing operations of the company. Without data, companies may be flying blind, and unintended, adverse financial consequences will be looming years down the road.

ON THE RISK vol.31 n.4 (2015) 47
Companies must break down the entire sales process, from reviewing the application questions through the underwriting final decision. Included in this review is the actual sales process including the preferred distribution channel and the application. We’ll ex-amine each aspect of the insurance transaction and the essential items that must be measured.
The Simplified Issue Sales ProcessWill agents/brokers sell the policy? Will policies be sold face-to-face? Over the Internet? Over the phone? If a company sells coverage from a call center, will it utilize its own employees or outsource the work? There are pluses and minuses to each of these sce-narios.
Face-to-face sales provide some comfort that the proposed insured is who he claims to be and is in relatively good health. But we also need to keep in mind that the producer in face-to-face sales has a strong financial interest in getting the policy issued, and there are small minorities of agents who may be inclined to coach the applicant. “Mr. Jones, you have never used tobacco, right?”
Internet sales sometimes reduce or eliminate agent compensation, but companies must feel comfortable the customer understands application questions and will be able to provide the level of detail required in response to “yes” answers. Multiple signatures for the application, authorizations, disclosures and consents can often stymie the Internet sales process.
When sales are completed by agents, will telephone sales be allowed? Agent-completed telephone sales may create mortality issues that need to be considered in product pricing.
Sales conducted from call centers may reduce anti-selection. If companies haven’t already done so, they should measure the quality of application declara-tions provided by agents compared to call center personnel. This includes not only the quantity of information but also the quality of information. This data can then be used to estimate the mortality im-pacts associated with each sales method. Companies should be aware that there are mortality differences based on who completes the application and by what means it was completed.
The ApplicationSimplified issue sales almost always incorporate a short-form application. However, the question remains: How short can you go? Companies must measure the potential mortality impacts of short-form applications.
Assuming that regulators would ever approve a single-question application (they won’t!), you might just ask, “In the past 10 years, detail all visits to a physician or medical professional including date of visit, reason for visit, findings, medications prescribed and full name and address for each medical provider.”
We have learned over decades of underwriting that a certain number of application questions are required to elicit information sufficient to properly underwrite and price the risk. Each question is intended to provide underwriting value. Some companies tout a limited number of application questions but bundle multiple medical conditions into each question. Other companies ask a larger number of questions, but shorter questions. There is no right or wrong answer. The key is to get the necessary information.
With simplified issue products, the number and scope of application questions are reduced. But what questions can be eliminated without impacting mortality? Remember, we’re considering the new generation of simplified issue products that assume the same mortality as fully underwritten products. Do you eliminate the questions about epilepsy and nervous system disorders? Do you reduce the scope of the questions related to heart or coronary artery disease? If there were no underwriting or mortality impacts associated with those questions, why were they included on the full underwriting application in the first place? If there are mortality implications, companies need to measure the impact of each elimi-nated question and factor that into the final financial analysis. Do you have questions about the potential mortality impact of eliminated questions? Reinsurers may be able to help.
Underwriting RequirementsCritical to the success of any simplified issue product are the underwriting requirements. To achieve ex-pected mortality and profitability goals, the require-ments must be thoroughly studied. This includes conducting appropriate cost/benefit analyses to fully understand the impact of reducing or adding under-writing requirements.
MIB/Insurance Activity IndexThere is no questioning the value of the MIB/IAI in simplified issue underwriting. The MIB helps reduce anti-selection. The same is true for the IAI as it helps identify rewrites of non-issued policies by the issuing company, as well as “stacking” of simplified issue or guaranteed issue policies. Eliminating either will have devastating financial consequences.

ON THE RISK vol.31 n.4 (2015)48
Medical ExamCompanies need to understand the protective value of the medical exam questions. While frequently duplicative of application questions, there may be additional questions not covered by the application. Additionally, insurers have long recognized the value of a disinterested third party asking the questions and fully recording the applicant’s responses. Simi-lar to the application question asked earlier, if the exam questions are assumed to add no underwriting value, why were they required in the first place? In fact, medical history questions may be even more important now as consumers know more about their health than ever before.
Conversely, well-crafted application and drill-down questions completed by a tele-app provider or call center can mitigate the loss of examination Part 1 protective value.
Vital MeasurementsDo most applicants accurately report their weight on the non-medical Part 1? For those who don’t provide a reasonably accurate weight, do they most often overstate or understate their true height and weight? With the exam and vital measurements off the table for SI underwriting, will the level of understatement of weight be exacerbated?
Blood PressureThere will be some level of anti-selection related to blood pressure, but a portion of this may be mitigated with prescription drug checks (see below). Of greater concern are those applicants with elevated blood pressure who are first made aware of their condition by the insurance exam. Mortality from those with previously undiagnosed elevated blood pressure will increase. Companies need to account for this in their overall mortality calculations.
Perhaps the most interesting feature of the new gen-eration of SI products is total elimination of blood and urine (except for cases with significant MIB information). For companies assuming SI mortality will match full underwriting mortality, this will be the one area that needs to be thoroughly measured through cost/benefit analyses.
Tobacco UseThe biggest issue with elimination of fluids is tobacco misrepresentations. One client reported the percent-age of admitted tobacco users on its SI product was significantly smaller than the percentage of confirmed tobacco users in its fully underwritten book of busi-ness.
How prevalent/significant is “smoker’s amnesia” with SI underwriting? The only way to establish a baseline is by measuring tobacco misrepresentation on fully underwritten products. Companies must do a robust review of recently processed applications, including issued, declined and incomplete files. Select a statistically significant sample of applications and focus on the tobacco use question on the non-medical Part 1. Ignore any exam, inspection or APS tobacco disclosures, as none of these will be required with SI underwriting.
Focus the cost/benefit analysis on applications where the applicant denies tobacco use. Then review the cotinine result on the urine specimen. Companies that have done this work report mid-single digit to low-double digit percentages of tobacco misrepre-sentations.
The next step is to calculate the mortality impact of tobacco misrepresentation. Assume that during the initial application review the company finds 95% of applicants declare themselves non-tobacco users. As-sume further the urine specimen review shows 5% of these applicants were actually tobacco users. Overall, the tobacco misrepresentation for the company’s full underwriting book of business is 4.75% (.95 x .05.) Most companies assume tobacco use mortality is twice (Table 4) “standard” mortality. Then ask the actuaries to calculate the overall mortality/profit-ability impact if 3.8% of business is underpriced by four tables. This result must be incorporated into the SI product design and pricing.
It is relatively simple to calculate tobacco use anti-selection on fully underwritten products. Companies can be absolutely sure to experience even greater levels of tobacco use anti-selection on simplified issue products. Short of an MIB “hit” for recent tobacco use, there is virtually no way to identify misrepre-senters on SI products. Producers know this, and so do customers.
Glucose/A1cWe’re in a “diabesity crisis” in the United States. The overall and insured population has a much greater average BMI than just 20 years ago, and the incidence of glucose intolerance and diabetes has skyrocketed during the same time period. Diabetes.org, the official website of the American Diabetes Association, reports that in 2012 there were 29.1 million Americans with diabetes, of which 8.1 million (27.8%) were undiag-nosed. Additionally, there are 86 million Americans age 20 and older with “pre-diabetes,” up from 79 million just 2 years earlier.

ON THE RISK vol.31 n.4 (2015) 49
Traditional insurer blood glucose testing is rapidly being replaced industry-wide with routine A1c screen-ing. Routine A1c screening allows insurers to keep pace with the explosion in diabetes and pre-diabetes, but this protective value is lost with SI underwriting. A number of companies have found nearly 20% of applicants have elevated A1c levels (5.7% and higher) and 3%-5% of these are truly protective test results. (No known indication of glucose intolerance and dia-betes from any other underwriting source, including the application.) Again, insurers are wise to calculate the lost protective value from eliminating routine glucose and A1c screening.
HIVThe HIV epidemic identified in the early 1980s led to almost universal blood testing. Few if any applicants who were HIV-positive admitted their status on the insurance application. Additionally, the vast majority of HIV-infected individuals were unaware of their sta-tus adding further value to the insurance blood test.Companies need to review their last several years of blood test results (ask your lab) and determine the number and percent of HIV-positive applicants. Until proven otherwise, 100% of these individuals are generally uninsurable and at least some will now slip through to the SI insured population. Also, one ExamOne client company that tracked simplified issue HIV experience reported significant levels of HIV anti-selection.
Liver Function Tests (LFT)Elimination of blood testing also means loss of the LFTs. This is particularly important for HCV-positive applicants with abnormal liver enzymes. Approxi-mately 60%-65 % of HCV-infected applicants have abnormal LFTs. Client companies have reported that similar to HIV-positive applicants, few HCV-positive applicants admit their status and the vast majority are unaware of their HCV status. And with overall HCV rates of infection nearly three times the HIV positive rate, the mortality impacts are significant. How significant?
Asymptomatic, untreated HCV infection conveys a moderate mortality risk. At best, these applicants require a mild to moderate substandard under best-case scenarios. Only a small percentage of these applicants will spontaneously clear the virus. With an approximate .15% insured population infection rate and average mortality approximately two times “standard” the mortality implications are significant. Once again, a review of fully underwritten applica-tions will yield a rough estimate of LFT protective value for HCV-positive individuals.
The same is true for alcohol abusers. Loss of blood testing will allow a number of these applicants to slip into the SI pool.
Other Blood/Urine ResultsThe concerns expressed above also hold true for other blood/urine test results, but the mortality impacts are generally somewhat smaller. In any event, com-panies need to take these into account when pricing the new product.
Attending Physician Statements (APS) and Electronic Medical RecordsAPSs are also virtually eliminated on the new genera-tion SI products except where the MIB or a prescrip-tion drug check discloses significant, unadmitted information. Similar to the concerns expressed above, companies need to measure and understand the im-pact of fewer APSs.
Does the company order a significant number of age/amount APSs? Virtually 100% of their protective value may be lost on SI products. For APSs ordered “for cause,” are companies comfortable these APSs only infrequently reveal significant, non-disclosed medical impairments? Accessing electronic medical records and use of services that extract prescription histories, lab and pathology reports can help offset the elimination of the traditional APS.
Anti-SelectionIt is impossible to accurately calculate the adverse mortality impacts of anti-selection. But we know we have a very efficient life insurance marketplace. Producers spreadsheet companies and products and will most certainly gravitate to SI products if they perceive a “bargain” for their client while generating full compensation.
Prescription (Rx) Drug ChecksPrescription checks provide an excellent opportunity to recapture at least a portion of the “lost” mortality detailed above. But how much?
Companies utilizing prescription drug checks on a screening or reflex basis should already have a rough estimate of their protective value. If not, adding rou-tine prescription checks for the SI product without a cost/benefit analysis is just a shot in the dark.
Go back to the tobacco misrepresentation example from above. Remember the 4.75% of business un-derpriced by four tables? How much of that mortality can the company reasonably expect to recapture with prescription checks? Ask/answer the same question for the mortality lost through the short form applica-

ON THE RISK vol.31 n.4 (2015)50
tion, loss of exam, and loss of vital measurements, APSs and various blood/urine tests.
On the flip side, routine prescription checks may produce some mortality savings not captured by tra-ditional underwriting requirements. Companies may learn of significant medical conditions that routine exams, APSs and blood/urine tests won’t uncover. Will these be sufficient to further close the mortal-ity gap? The pricing actuaries and finance folks will need this data.
Companies may also consider ordering prescription checks by both the industry providers to help close gaps in available PBM data. Not all similar data is available to each of the major prescription data providers. If companies are relying on prescrip-tion screening to offset mortality from eliminated requirements, they need to understand the quantity and quality of the prescription data they will be us-ing. New data sources are becoming available to the industry that extract prescription, lab and pathology reports from medical records.
ExpensesReduced expenses. Significantly reduced expenses. We have discussed potential reductions in sales commissions if products are sold over the Internet or through call centers. The new generation of SI prod-ucts eliminates virtually all medical exams, blood/urine and APSs. Can we assume lower lost business rates due to faster policy issue? Greater placement ratios reduce per policy costs. Greater placement rates translate to increased profitability.
Increased Sales Is one of the goals of SI underwriting to increase sales and “placed” business? If so, a post-implementation study to validate achievement of this goal is essential. Too often, the promised “plus” sales fail to material-ize. Why mention plus sales? There is always a risk SI sales will cannibalize fully underwritten business. Companies may achieve their SI sales goals only to find sales of fully underwritten business tail off. Sales goals need to be defined and measured.
ReinsuranceDon’t have the time/resources/inclination to com-plete cost/benefit analyses to measure the financial impacts of each step of the SI process? Companies might want to tap into reinsurance expertise. Re-insurers must obviously be involved in each step of the SI process if they reinsure any portion of the risk. This is especially true if the direct writer prices the product for “standard” mortality. However, even if a company retains 100% of the SI risk, it would be wise
to engage its reinsurer(s) in discussions regarding its underlying assumptions. It is best to identify potential mortality/profitability issues prior to product launch rather than have to react to adverse experience years down the road.
Actuaries, Claims and SalesIntroduction of a simplified issue product, especially if “standard” or better mortality is assumed, requires total transparency with the actuarial, finance, claim and distribution channels. Actuaries have historic data measuring actual to expected mortality experi-ence on fully underwritten products. They need to understand and embrace the tradeoffs involved in SI underwriting. This means sharing objective data related to what requirements are being eliminated and added, and the underwriting department’s mor-tality assumptions related to each change. If fully underwritten mortality is tracking much better than pricing assumptions, an aggressive SI underwriting policy may make sense. If actual to expected is on target the actuaries must agree the recommended SI protocol will not skew current experience.
Once actuarial approval is secured, the finance de-partment must join the conversation to fully under-stand how underwriting acquisition expenses and financial targets will be impacted.
The claims department will need to understand the underwriting changes and assumptions in order to conduct appropriate contestable claim investigations, and not panic when claims must be paid because the application and underwriting requirements may not disclose significant information that has traditionally been readily available on fully underwritten business.The sales team will be showering their underwrit-ing brethren with copious praise for simplifying the process and eliminating all those burdensome and unnecessary requirements. But they also need to understand their responsibility to provide a full and complete SI application and to fulfill any sales com-mitments required to achieve the desired corporate results.
ConclusionThe simplified issue conundrum. It may not be quite a conundrum if companies break down the entire process from start to finish, conduct appropriate cost/ benefit analyses, and complete post-implementation validation studies. Assuming “standard” mortality on SI business can be a game changer provided com-panies can adequately answer the questions posed above.
ON THE RISK vol.31 n.4 (2015) 51
About the AuthorDarren M. Dombrosky, FLMI, ACS, serves as Senior Vice President, National Accounts, for ExamOne. In this role, he oversees the development, marketing and operations of the company’s national sales efforts. Before leading sales, Darren developed and introduced ExamOne’s Teleunderwriting (EDC) services in 2000 and led that area for several years. Prior to joining ExamOne, Darren was in underwriting at the Principal Financial Group, where he worked as a life and disability underwriter for 8 years. Darren earned his bachelor’s degree in Finance and International Business from the University of Iowa.
The ALU Underwriting Development and Continuing Education Group at the ALU Annual Meeting (left to right): Roy Davis, NFP; Sue Swenson, Prudential; Director of Continuing Education Sharon Garner, American National; Nancy Thorpe, RBC Insurance; Hope Adams, Transamerica Life; Tim Miller, Munich American Re; (not pictured) John Duff, BMO Life.
The Survey Group at the ALU Annual Meeting: (left to right) John Sherman, AIG Global; Roberta Scott, Wood-men Life; Carol Flanagan, John Hancock; Coordinator Kristin Ringland, SCOR Global Life.

ON THE RISK vol.31 n.4 (2015)52
MANAGEMENT VERSUS LEADERSHIP
Executive Summary This article explores the differences between management and leadership, two terms which are often used together or as synonyms. Definitions of each term are offered followed by a conversation on some practical differentiators. Management is presented as a constellation of skills, with leadership as a subset and a more focused skill. Leadership is then ad-dressed in greater detail as the concepts of vision, role modeling and empowerment are discussed.
Marv Reber, FALUOTR Contributing EditorMassMutualScottsdale, [email protected]
IntroductionThe terms management and leadership are often used interchangeably. Some people might say they recognize a leader, even if they can’t explain why. Asked to name a great leader, we often hear the names Gandhi, Abraham Lincoln, Nelson Mandela or Martin Luther King, Jr. These are certainly great leaders, but what differentiates them as leaders vs. managers? This article identifies and explores these differences and offers some insight on the skills and characteristics of a great leader.
DefinitionsManagement can be defined as “the process of deal-ing with or controlling people or things, the skill of making decisions in business, or the act of conducting or supervising something.” As a number of defini-tions are reviewed, the word “controlling” appears frequently.
A good definition of leadership is difficult to find because leadership is often described as “the act of leading.” One example defines the activity of leading as “the ability to establish a clear vision, sharing the vision, and then providing information, knowledge and methods to realize the vision.”
“Management is doing things right; leadership is doing the right things.” Peter Drucker
DifferentiatorsManagement books consider managing as having four basic functions: planning, organizing, influencing and controlling, where influencing is often replaced with leading. In the management context, leading is described as “being a motivator of people through understanding of personalities and use of communi-cation techniques to find success.” Thus leadership concepts can be considered a subset of management, with management being more concrete, involving
planning, organizing, coordinating, providing struc-ture and rules, and finding solutions for problems. Leadership is about having vision, living certain val-ues or being a role model, working with strategy and empowering. Management skills tend to be learned first by new managers, whereas leadership is a dis-cipline aligned to established and tenured managers who become involved with strategy.
• Management is reactive while leadership is pro-active.
• Management is telling while leadership is com-municating and listening.
• Management is tactical or transactional, focused on tasks while leadership is strategic or transfor-mational, focused on people.
• Leaders have followers.
“I suppose leadership at one time meant muscles; but today it means getting along with people.”Mahatma Gandhi
VisionHaving vision seems to be a contributing factor to the highly regarded leadership qualities of Lincoln, King and Gandhi, et al. John F. Kennedy is often regarded as a great leader for his vision to put a man on the moon before the end of the decade of the 1960s.
ON THE RISK vol.31 n.4 (2015) 53
Vision is the ability to create a future view of a situ-ation, organization or process which often takes us a giant leap forward, rather than just a small step. But it isn’t just that, as many a politician or business leader has outlined a vision, without thought or realization, and never to come to fruition. For success, it is the ability to communicate a vision, inspiring people to buy in and support it, to provide details and insight to the vision’s challenges, and eventually create the motivation to implement and realize the vision.
Having vision involves seeing the big picture and your place in it. A vision is established by knowing the setting, the situation, the timing, the historical aspects, and literally trying to predict or create the future. For leaders to be visionaries they must be knowledge experts, really knowing their business and its regulations, understanding how it operates, how it has been run historically, and then thinking three steps ahead. Vision is about thinking big, setting the tone and never giving up.
“Four score and seven years ago ... dedicated to the great task remaining before us ... this nation ... shall have a new birth of freedom, and that the government of the people, by the people, for the people, shall not perish from the earth.” Abraham Lincoln
“Leadership and learning are indispensable to each other.” John F. Kennedy
Role Model Leaders are role models. They model the behaviors that they wish others to emulate. Their behaviors, actions and words will determine how successful they are. They are consistent and establish a manner that supports their vision. For a vision to be successful, the architect and sponsor of that vision must be all in, practicing what they preach.
Leaders must be bold and confident, yet humble, real-izing it is people who will make their vision happen.
Leaders create a culture involving individuals, not only for their work skill, but for their ideas and tal-ents, all for the greater good. A strong leader is a good listener, an active listener, who strives to understand others, who learns from them and creates a trust.
“A genuine leader is not a searcher for consen-sus but a molder of consensus.” Martin Luther King, Jr.
EmpowermentLeadership is the ability to guide others without force into a direction or decision that leaves them still feel-ing empowered and accomplished. It is helping others rise to their full potential, understanding the talents and temperament of each person. It is an art of serv-ing and preparing others, giving them the appropriate tools, time and energy to realize their potential. Good leaders can take an average team and transform them into stars. They also know when to lead and when to step back and let others take the lead. They challenge individuals to walk beside them rather than behind.
“It is better to lead from behind and to put others in front, especially when you celebrate victory when nice things occur. You take the front line when there is danger. Then people will appreci-ate your leadership.” Nelson Mandela
ConclusionGood managers will keep organizations at the status quo or move them forward slowly. Strong leaders will take individuals and companies to places they would not have been able to reach alone. Leaders will get people to accomplish more than they ever would. They will not rely on a title or positional power, but rather a personal skill or power to influence. They will set a vision, model positive behaviors, and empower team members to reach the vision.
“There are those who look at things the way they are and ask why ... I dream of things that never were and ask why not?” Robert Kennedy
OTR thanks Stan Meyer for his photos of the 2015 ALU Annual Meeting which appear in this issue.

ON THE RISK vol.31 n.4 (2015)54
CARDIAC STRESS TESTS
Executive Summary An underwriter will encoun-ter various cardiac stress test results while re-viewing medical records. This article will review the different tests and discuss how a physician determines which test to order.
Michael Wetzel, MDOTR Contributing EditorPrudential Insurance CompanyMaple Grove, [email protected]
While reviewing the file of a 57-year-old man, you come across a stress test. It is an exercise treadmill test performed following an overnight hospital stay for chest pain. Later that same day you review an exercise echocardiogram performed on a 50-year-old woman with increased shortness of breath. The next file you review has a pharmacologic myocardial per-fusion scan performed on an obese 75-year-old man. He has cardiac risk factors of hypertension, diabetes and hyperlipidemia, and there is mention of severe osteoarthritis of the knees. Looking at these tests you may wonder why are there different types and how does a physician decide which test to order.
A physician needs to answer several questions when determining which test is the appropriate one to order. What is the indication for the test? Can the person exercise enough to obtain a reliable result? Are there any baseline abnormalities seen on the EKG? Is it important to evaluate the structure of the heart? What is the person’s body habitus?
IndicationsThere are several indications to perform a cardiac stress test. The most common is for the evaluation of suspected ischemia. For example, a person may present with symptoms concerning for ischemic car-diac disease, such as exertional chest pain, increased shortness of breath, increased fatigue or reduced exercise tolerance. To confirm or rule out the cause being ischemia, a stress test is performed.
Other indications include the following:• A person has known coronary artery disease
(CAD), but has a change in his status, such as new or worsening symptoms.
• Someone with newly diagnosed heart failure or cardiomyopathy to rule out ischemia as the cause. Usually this person would have an angiogram, but a stress test may be performed to determine
if the myocardium is viable and to plan revascu-larization.
• A pre-op evaluation for non-cardiac, non-emer-gent surgery.
• Someone with recently diagnosed acute coronary syndrome who is managed medically. A stress test may be performed after 3 months to determine the effectiveness of the treatment and for risk assessment.
• A person who has had prior revascularization. A stress radionuclide myocardial perfusion imaging test may be done once–5 years after a CABG or 2 years after a PTCA. Otherwise it is not recom-mended to routinely perform stress tests on this population in the absence of new symptoms.
A stress test is not indicated for someone who has atypical or non-cardiac type chest pain if he is at low risk for CAD. It should not be used to screen asymp-tomatic people. The reason for this is as the probabil-ity of cardiac disease in a person decreases, the risk of a false-positive result increases. Some exceptions are those who are at a very high risk of CAD based on risk factors and those in high-risk occupations, such as a commercial airline pilot or a professional firefighter.
Test selectionOnce a physician decides a stress test is indicated, the provider needs to determine the appropriate test. Two main questions need to be answered:
1. How to stress the heart?2. How to evaluate the stressed heart?
The factors taken into consideration include:
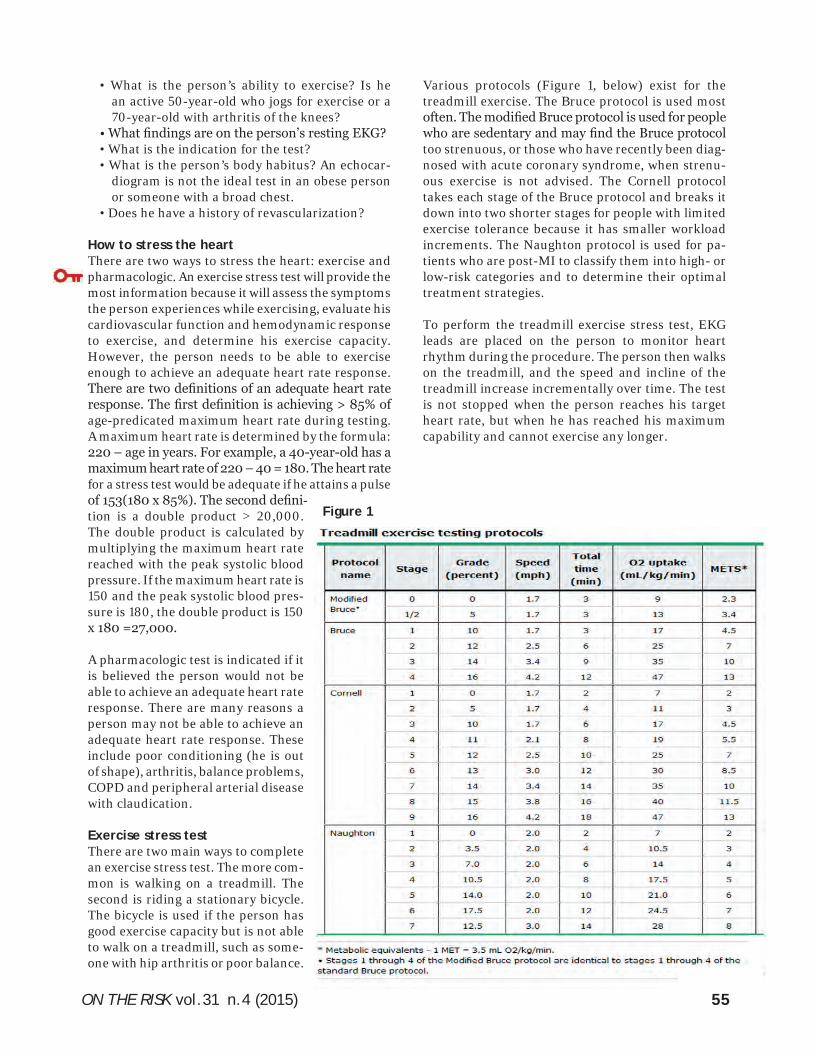
ON THE RISK vol.31 n.4 (2015) 55
• What is the person’s ability to exercise? Is he an active 50-year-old who jogs for exercise or a 70-year-old with arthritis of the knees?
• What findings are on the person’s resting EKG? • What is the indication for the test?• What is the person’s body habitus? An echocar-
diogram is not the ideal test in an obese person or someone with a broad chest.
• Does he have a history of revascularization?
How to stress the heartThere are two ways to stress the heart: exercise and pharmacologic. An exercise stress test will provide the most information because it will assess the symptoms the person experiences while exercising, evaluate his cardiovascular function and hemodynamic response to exercise, and determine his exercise capacity. However, the person needs to be able to exercise enough to achieve an adequate heart rate response. There are two definitions of an adequate heart rate response. The first definition is achieving > 85% of age-predicated maximum heart rate during testing. A maximum heart rate is determined by the formula: 220 – age in years. For example, a 40-year-old has a maximum heart rate of 220 – 40 = 180. The heart rate for a stress test would be adequate if he attains a pulse of 153(180 x 85%). The second defini-tion is a double product > 20,000. The double product is calculated by multiplying the maximum heart rate reached with the peak systolic blood pressure. If the maximum heart rate is 150 and the peak systolic blood pres-sure is 180, the double product is 150 x 180 =27,000.
A pharmacologic test is indicated if it is believed the person would not be able to achieve an adequate heart rate response. There are many reasons a person may not be able to achieve an adequate heart rate response. These include poor conditioning (he is out of shape), arthritis, balance problems, COPD and peripheral arterial disease with claudication.
Exercise stress testThere are two main ways to complete an exercise stress test. The more com-mon is walking on a treadmill. The second is riding a stationary bicycle. The bicycle is used if the person has good exercise capacity but is not able to walk on a treadmill, such as some-one with hip arthritis or poor balance.
Various protocols (Figure 1, below) exist for the treadmill exercise. The Bruce protocol is used most often. The modified Bruce protocol is used for people who are sedentary and may find the Bruce protocol too strenuous, or those who have recently been diag-nosed with acute coronary syndrome, when strenu-ous exercise is not advised. The Cornell protocol takes each stage of the Bruce protocol and breaks it down into two shorter stages for people with limited exercise tolerance because it has smaller workload increments. The Naughton protocol is used for pa-tients who are post-MI to classify them into high- or low-risk categories and to determine their optimal treatment strategies.
To perform the treadmill exercise stress test, EKG leads are placed on the person to monitor heart rhythm during the procedure. The person then walks on the treadmill, and the speed and incline of the treadmill increase incrementally over time. The test is not stopped when the person reaches his target heart rate, but when he has reached his maximum capability and cannot exercise any longer.
Figure 1
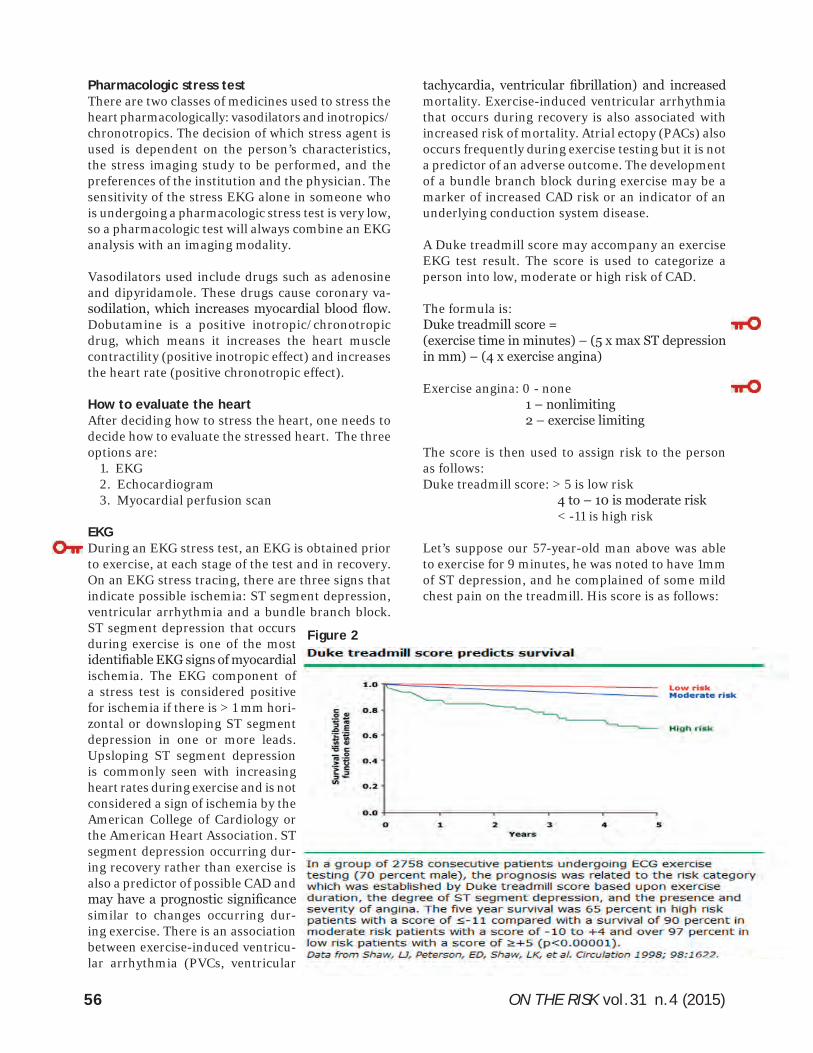
ON THE RISK vol.31 n.4 (2015)56
Pharmacologic stress testThere are two classes of medicines used to stress the heart pharmacologically: vasodilators and inotropics/chronotropics. The decision of which stress agent is used is dependent on the person’s characteristics, the stress imaging study to be performed, and the preferences of the institution and the physician. The sensitivity of the stress EKG alone in someone who is undergoing a pharmacologic stress test is very low, so a pharmacologic test will always combine an EKG analysis with an imaging modality.
Vasodilators used include drugs such as adenosine and dipyridamole. These drugs cause coronary va-sodilation, which increases myocardial blood flow. Dobutamine is a positive inotropic/chronotropic drug, which means it increases the heart muscle contractility (positive inotropic effect) and increases the heart rate (positive chronotropic effect).
How to evaluate the heartAfter deciding how to stress the heart, one needs to decide how to evaluate the stressed heart. The three options are:
1. EKG2. Echocardiogram3. Myocardial perfusion scan
EKGDuring an EKG stress test, an EKG is obtained prior to exercise, at each stage of the test and in recovery. On an EKG stress tracing, there are three signs that indicate possible ischemia: ST segment depression, ventricular arrhythmia and a bundle branch block. ST segment depression that occurs during exercise is one of the most identifiable EKG signs of myocardial ischemia. The EKG component of a stress test is considered positive for ischemia if there is > 1 mm hori-zontal or downsloping ST segment depression in one or more leads. Upsloping ST segment depression is commonly seen with increasing heart rates during exercise and is not considered a sign of ischemia by the American College of Cardiology or the American Heart Association. ST segment depression occurring dur-ing recovery rather than exercise is also a predictor of possible CAD and may have a prognostic significance similar to changes occurring dur-ing exercise. There is an association between exercise-induced ventricu-lar arrhythmia (PVCs, ventricular
tachycardia, ventricular fibrillation) and increased mortality. Exercise-induced ventricular arrhythmia that occurs during recovery is also associated with increased risk of mortality. Atrial ectopy (PACs) also occurs frequently during exercise testing but it is not a predictor of an adverse outcome. The development of a bundle branch block during exercise may be a marker of increased CAD risk or an indicator of an underlying conduction system disease.
A Duke treadmill score may accompany an exercise EKG test result. The score is used to categorize a person into low, moderate or high risk of CAD.
The formula is: Duke treadmill score = (exercise time in minutes) – (5 x max ST depression in mm) – (4 x exercise angina)
Exercise angina: 0 - none 1 – nonlimiting 2 – exercise limiting
The score is then used to assign risk to the person as follows:Duke treadmill score: > 5 is low risk 4 to – 10 is moderate risk < -11 is high risk
Let’s suppose our 57-year-old man above was able to exercise for 9 minutes, he was noted to have 1mm of ST depression, and he complained of some mild chest pain on the treadmill. His score is as follows:
Figure 2
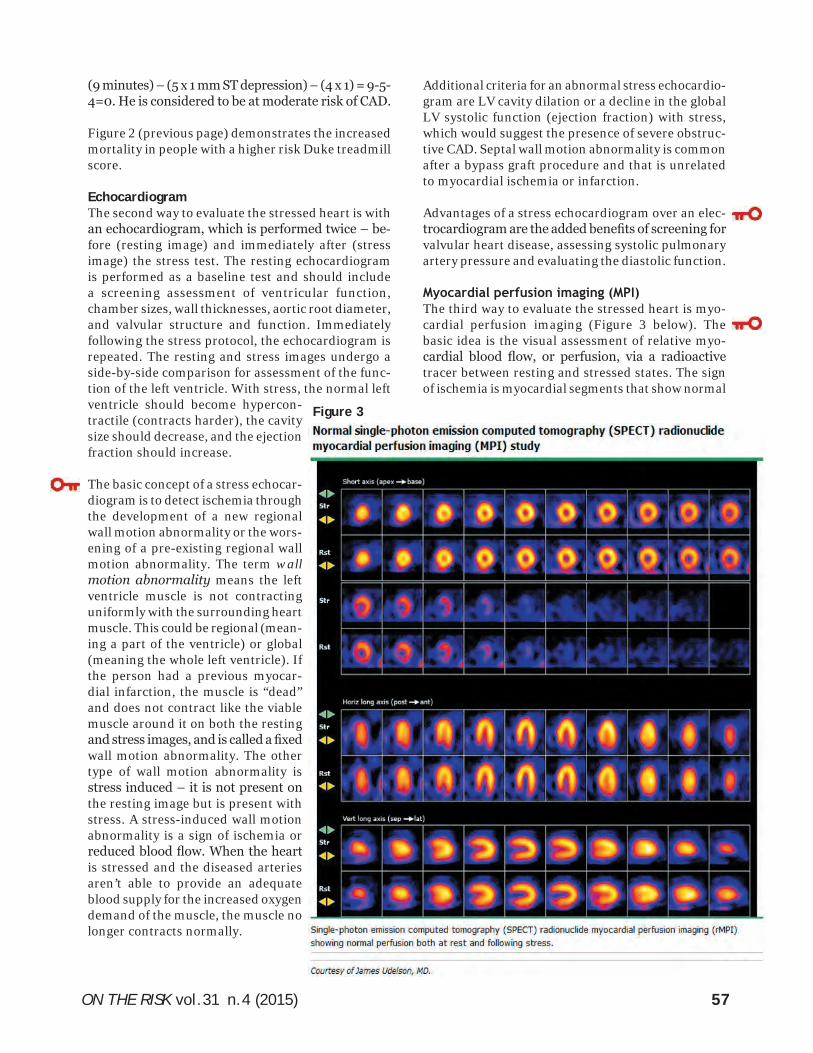
ON THE RISK vol.31 n.4 (2015) 57
(9 minutes) – (5 x 1 mm ST depression) – (4 x 1) = 9-5-4=0. He is considered to be at moderate risk of CAD.
Figure 2 (previous page) demonstrates the increased mortality in people with a higher risk Duke treadmill score.
EchocardiogramThe second way to evaluate the stressed heart is with an echocardiogram, which is performed twice – be-fore (resting image) and immediately after (stress image) the stress test. The resting echocardiogram is performed as a baseline test and should include a screening assessment of ventricular function, chamber sizes, wall thicknesses, aortic root diameter, and valvular structure and function. Immediately following the stress protocol, the echocardiogram is repeated. The resting and stress images undergo a side-by-side comparison for assessment of the func-tion of the left ventricle. With stress, the normal left ventricle should become hypercon-tractile (contracts harder), the cavity size should decrease, and the ejection fraction should increase.
The basic concept of a stress echocar-diogram is to detect ischemia through the development of a new regional wall motion abnormality or the wors-ening of a pre-existing regional wall motion abnormality. The term wall motion abnormality means the left ventricle muscle is not contracting uniformly with the surrounding heart muscle. This could be regional (mean-ing a part of the ventricle) or global (meaning the whole left ventricle). If the person had a previous myocar-dial infarction, the muscle is “dead” and does not contract like the viable muscle around it on both the resting and stress images, and is called a fixed wall motion abnormality. The other type of wall motion abnormality is stress induced – it is not present on the resting image but is present with stress. A stress-induced wall motion abnormality is a sign of ischemia or reduced blood flow. When the heart is stressed and the diseased arteries aren’t able to provide an adequate blood supply for the increased oxygen demand of the muscle, the muscle no longer contracts normally.
Additional criteria for an abnormal stress echocardio-gram are LV cavity dilation or a decline in the global LV systolic function (ejection fraction) with stress, which would suggest the presence of severe obstruc-tive CAD. Septal wall motion abnormality is common after a bypass graft procedure and that is unrelated to myocardial ischemia or infarction.
Advantages of a stress echocardiogram over an elec-trocardiogram are the added benefits of screening for valvular heart disease, assessing systolic pulmonary artery pressure and evaluating the diastolic function.
Myocardial perfusion imaging (MPI)The third way to evaluate the stressed heart is myo-cardial perfusion imaging (Figure 3 below). The basic idea is the visual assessment of relative myo-cardial blood flow, or perfusion, via a radioactive tracer between resting and stressed states. The sign of ischemia is myocardial segments that show normal
Figure 3
ON THE RISK vol.31 n.4 (2015)58
myocardial perfusion at rest but reduced myocardial perfusion with stress. A matched reduction in perfu-sion seen at rest and with stress indicates a previous myocardial infarction – there is no blood flow at rest or with stress. Other information that can be obtained with a myocardial perfusion scan is cardiac size and function.
Soft tissue attenuation is a term frequently encoun-tered in a myocardial perfusion report and is one of the more common causes of artifact on a perfusion scan. The heart is surrounded by tissues of varying densities including air, bone, fat and muscle, which will cause non-uniform photon activity. Soft tissue attenuation is caused by these intervening structures such as the chest wall, diaphragm, lungs and breasts.
Similar to the echocardiogram, a septal wall motion abnormality may be seen after a bypass graft and does not indicate myocardial ischemia or infarction.
Let’s put it all togetherHere are the options for cardiac stress testing:
• Exercise EKG• Exercise echocardiogram• Exercise MPI• Pharmacologic echocardiogram• Pharmacologic MPI
ConclusionThere are different cardiac stress tests that an un-derwriter will frequently encounter while reviewing medical records. A physician takes into account vari-ous factors when deciding which test to order. The indication for the test is reviewed. The person’s ability to exercise is evaluated and the EKG is examined. The physician determines if an evaluation of the structure of the heart is important. After careful consideration of these points, the physician is able to select the ap-propriate test to order.
[Life insurance is issued by The Prudential Insurance Company of America, Newark, NJ, and its affiliates.
This article is not intended to provide medical advice. Diagnosis and treatment should be left to the patient’s physician.
The availability of coverage and rates will vary based on company underwriting criteria including, but not limited to, age, sex, health history, smoking status and residency.]
Have you ever considered writing an article for OTR?
Do you need something extra for your Performance Review? Need to add to your Resume being published in a professional journal? Sharing your exper-tise and knowledge can help elevate your visibility in your profession.
OTR is looking for narrowly focused articles of 1000 words or articles with a broader focus up to 2500 words.
Do you have an interest in Financial Underwriting, Technology, Avocations or Living Benefits? We are currently looking for editors who would be willing to commit to these and other topics.
Visit www.ontherisk.com to review a copy of the Author Guidelines or con-tact an Editor today.
JOURNAL OF THE ACADEMY OF LIFE UNDERWRITINGOTR

ON THE RISK vol.31 n.4 (2015) 59
UNDERSTANDING THE COMPLETE BLOOD COUNT
Executive Summary The blood cells (red cells, white cells, platelets) have unique functions in our body. Some are an essential part of the im-mune system (white blood cells), others transport oxygen to all the cells in the body (red blood cells), and others are part of the blood clotting system, preventing the loss of blood (platelets). A com-plete blood count (CBC) gives important details about the blood cells: number, shape, colour, size. Knowing this information may provide clues for particular medical conditions. Underwriting CBC results that are only slightly abnormal can be daunting. The best way to assess a CBC is to ana-lyze the results in the context of accompanying symptoms or signs obtained from the application or medical examination.
Oana Telfer, MD, FALUAssistant Vice President, Corporate Underwriting and Claims Risk ManagementSun LifeToronto, [email protected]
BackgroundThe process of production, multiplication and spe-cialization of blood cells is called hematopoiesis. It begins with the most basic blood cell, the pluripotent hematopoietic stem cell (HSC). The HSCs have the ability to self-renew or to commit into a “differentia-tion” pathway. These pathways eventually result in the production of one of the types of blood cells below (end products of hematopoiesis):
• Mature white blood cells (WBCs) which provide protection from infection.
• Mature red blood cells (RBCs) which carry oxygen to all the cells in our bodies.
• Platelets (thrombocytes) which help control bleeding.
Most of the blood cells are generated at the site where HSCs reside (in the liver during the fetal period and in the bone marrow after birth) except for T cells, which are formed in the thymus from progenitors derived from these hematopoietic sites. The HSCs lose their pluripotency in a stepwise fashion, ultimately giving rise to unipotent progenitor cells.
Complete Blood Count (CBC) – The TestThis is the most frequently requested test. It consists of a panel of tests that evaluates the three types of cells that circulate in the blood: RBCs, WBCs and platelets.
The panel may include any of the following, though not all the tests described below will always be part of a CBC:
• WBC evaluation:o WBC count - provides the total number of
WBCs in blood.o WBC differential - identifies and counts the
number of the various types of WBCs present in the blood (neutrophils, lymphocytes, mono-cytes, eosinophils and basophils).
• Platelets evaluation:o Platelet count - provides the total number of
platelets in blood.
o Mean platelet volume (MPV) - a calculation of the average size of the platelets.
o Platelet distribution width (PDW) - a measure-ment of the variation of platelet size.
• RBC evaluation:o RBC count - provides the total number of RBCs
in blood.o Hemoglobin - measures the amount of oxygen-
carrying protein in blood.o Hematocrit (HCT) or packed cell volume (PCV)
- provides the percentage of RBCs in blood.o RBC indices (calculations that provide infor-
mation on the physical characteristics of the RBCs):◊ Mean corpuscular volume (MCV) - a mea-surement of the average size of RBCs.◊ Mean corpuscular hemoglobin (MCH) - a calculation of the average amount of oxygen-carrying hemoglobin inside a red blood cell.◊ Mean corpuscular hemoglobin concentration (MCHC) - a calculation of the average percent-age of hemoglobin inside a red cell.◊ Red cell distribution width (RDW) - a calcula-tion of the variation of RBC volumes.
ON THE RISK vol.31 n.4 (2015)60
o Reticulocyte count - provides the absolute count or the percentage of young RBCs in blood.
It is easy to interpret a CBC with marked abnormali-ties, but it becomes more difficult when the results show only subtle abnormalities, or the clinical picture is not clear.
Limitations of reference ranges for the CBCDeriving the blood count reference ranges is difficult, due to numerous factors that may affect blood count parameters. There are ethnic differences in some parameters, differences between males and females, and in pregnancy. Some of these factors are taken into account in published ranges (gender, pregnancy); others are not. Finally, there are differences between hematology analyzers that may affect some blood count parameters.
In view of the above, the established blood count reference ranges do not encompass the usual 2.5th to 97.5th percentiles (meaning 95% of normal indi-viduals), but more than that. Marginal results must therefore be interpreted in context, as a normal blood count does not always preclude the possibility of early disease states. Previous results, along with medical history and current medical examination, should be taken into account. Many significant clini-cal conditions will show progressive worsening CBC abnormalities.
Signs and symptoms relevant to interpreting a CBC include, but are not limited to:
• Pallor, jaundice• Fever, lymphadenopathies• Bleeding, bruising• Hepatomegaly, splenomegaly• Frequency and severity of infections• Fatigue, weight loss
1. WBC evaluation Total WBC count should not be considered in isola-tion, as it may be misleading. The absolute count of each of the cell types is more useful than the total (i.e., an abnormally low neutrophils count with an elevated lymphocyte count may produce a normal total WBC count).
A. NeutrophilsThey account for approximately 70% of all WBCs. The normal range depends on the lab, but usually is around 2.0 - 8.0 x 109 /L.
Neutropenia (low neutrophil count) is associated with a risk for developing life-threatening infections.
Concerning findings would be: • Neutrophil levels less than 1.0 x 109 /L• High rate of change of neutropenia• Lymphadenopathy • Hepatosplenomegaly
The most common causes for neutropenia are: • Viral infection• Autoimmune/idiopathic • Drugs
Neutrophilia (high neutrophil count) is mainly caused by bacterial infection, since the neutrophils are primarily associated with the response to a bacte-rial invasion. Other causes are:
• Stress• Acute inflammation• Chronic myeloid leukemia (CML) • Pregnancy
In order for neutrophilia to develop, an increased production of neutrophils in the bone marrow is nec-essary. As a result of this increased production, the number of young neutrophils in the blood will also be high, as they will be released earlier, before they ma-ture completely. The presence of an increased number of young cells in the blood is called left shift. The left shift is characteristic for neutrophilia of pregnancy.
Persistent moderate neutrophilia with a left shift is suggestive of CML. An increase in basophils and eosinophils may also be present. Chronic mild neu-trophilia without a left shift is very unlikely to be due to CML.
B. LymphocytesLymphocytes normally represent 20 - 40% of the circulating WBCs. The normal range is between 1.0 - 4.0 x 109 /L.
Lymphocytopenia (low lymphocyte count) is usually not significant in underwriting. It may be seen in late HIV infection, or after exposure to large doses of radiation (such as seen in nuclear accidents like Chernobyl).
Lymphocytosis (increase in the absolute lymphocyte count) can be seen in acute infections (e.g., Epstein-Barr virus infection and viral hepatitis).
Lymphocytes can also be increased in the following situations:
• Chronic smokers• After splenectomy• Autoimmune thyroiditis • Lymphoproliferative disorders, e.g., chronic
lymphocytic leukemia (CLL)
ON THE RISK vol.31 n.4 (2015) 61
Of note is that CLL is often discovered as an inci-dental finding on a CBC, though it may be associated with clinical signs as lymphadenopathy and hepato-splenomegaly. When underwriting individuals with persistently elevated lymphocyte count accompanied by lymphadenopathy and hepatosplenomegaly, it may be prudent to postpone the risk until they have been evaluated by a hematologist and a malignancy has been ruled out.
C. MonocytesMonocytes constitute 3 - 8% of the WBCs, and their normal range is between 0 - 1.0 x 109 /L. The mono-cytes which migrate from the bloodstream to other tissues are called macrophages, and have a role in immunity by ingesting the pathogens (phagocytosis).
Monocytopenia, a decrease in the total monocyte count, is rarely isolated. A finding of monocytopenia in the absence of other cell lines abnormalities is usually of no underwriting significance.
Monocytosis, an elevated monocyte count, is also un-commonly found in isolation, but can signal a chronic infection (e.g., tuberculosis) or a chronic inflamma-tion (e.g., Crohn’s disease, ulcerative colitis, rheuma-toid arthritis, SLE). A finding of persistently elevated levels (e.g., more than 1.5 x 109 /L) in underwriting, particularly in association with suspicious symptoms and without a hematology assessment, might warrant a postponement until evaluation is completed.
D. BasophilsBasophils are not very common, representing only about 0.01 - 0.3% of all WBCs.
Since the basophil count is normally very low, baso-penia (decreased basophil count) is very difficult to demonstrate.
Significant basophilia (high basophil count) is very rare, but when present it may indicate a myelopro-liferative disorder.
E. EosinophilsThey make up about 1 - 6% of the circulating WBCs, and their normal blood levels are between 0 - 0.5 x 109 /L.
Eosinopenia (low eosinophil count) is difficult to demonstrate in practice because of the low frequency of eosinophils in most healthy people. As a result, eosinopenia is not a cause of concern in underwriting.
Eosinophilia (high eosinophil count), on the other hand, is mostly due to allergic diseases (in developed
countries) or parasitic infections (worldwide).
A hematology assessment can be considered in indi-viduals with persistent (more than 6 months) moder-ate eosinophilia (up to 1.5 x 109 /L), or with marked (more than 1.5 x 109 /L) or increasing eosinophilia.
2. Platelets evaluationA normal platelet count ranges from 150 - 450 x 109 /L.
Low platelet counts (thrombocytopenia) are rela-tively common, and the results should be interpreted in the clinical context. Severe thrombocytopenia is associated with an increased risk of bleeding, and is particularly significant if accompanied by other CBC changes, or if the platelet count is falling.
The causes of isolated thrombocytopenia include pregnancy, viral infections, idiopathic thrombocy-topenic purpura (ITP), medications, liver disease, autoimmune disease, hypersplenism and HIV infec-tion. Bone marrow pathology should be considered if in addition to low platelet count there are other changes to the CBC.
Elevated platelets (thrombocytosis) may be reactive (in infections, inflammations) and not be associated with an increased thrombotic risk. In rare cases, thrombocytosis may reflect a myeloproliferative disorder such as myelofibrosis. This should be con-sidered with persistent (more than 6 months) eleva-tion in platelet count, or a very high count without an obvious reactive cause.
Other conditions that can cause thrombocytosis are pregnancy, essential thrombocythemia, iron defi-ciency and post-splenectomy (in this case the platelet count will be higher than 600 x 109 /L).
3. RBC evaluation - hemoglobin and red cell indicesLow hemoglobin levels are generally indicative of anemia. The mean cell volume (MCV) indicates the size of RBCs and is the main method to classify anemia:
• Microcytic (MCV < 80 fl)• Normocytic (MCV 80 - 100 fl)• Macrocytic (MCV > 100 fl)
Reticulocytes are immature red blood cells. Their number is increased when a high number of RBCs are lost in a short period of time (acute blood loss or hemolysis), and RBCs need to be released in the blood at a higher rate, even before they mature completely.
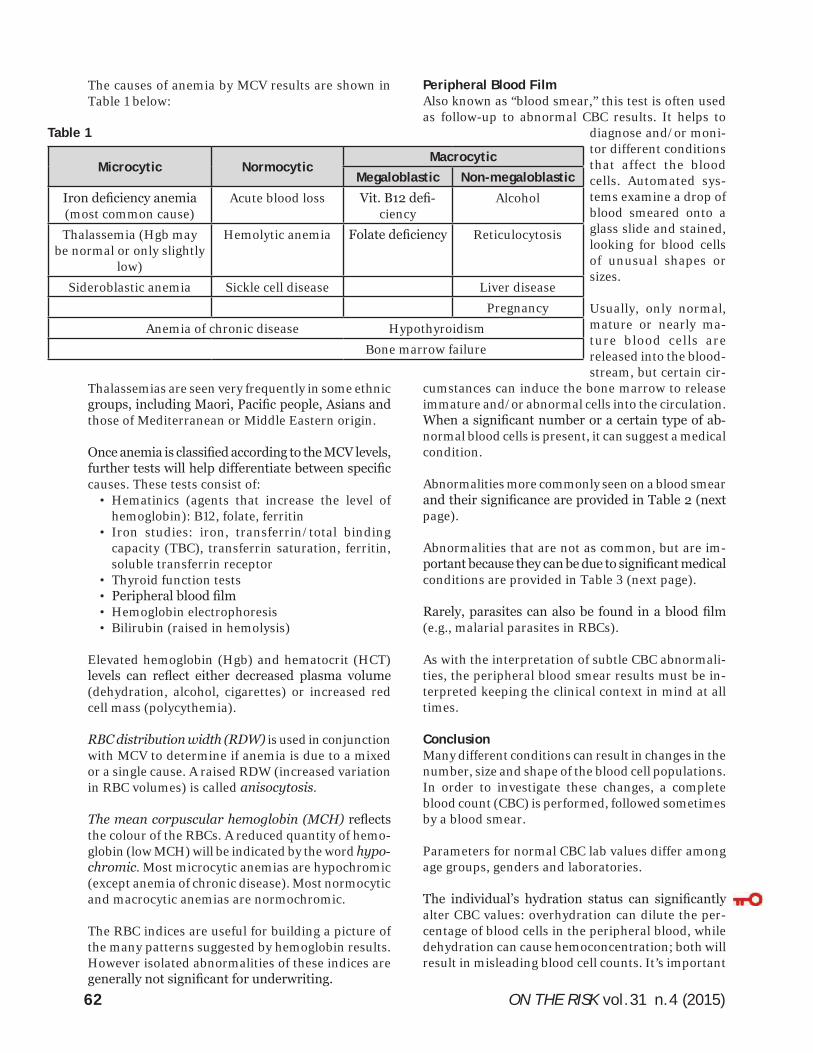
ON THE RISK vol.31 n.4 (2015)62
The causes of anemia by MCV results are shown in Table 1 below:
Thalassemias are seen very frequently in some ethnic groups, including Maori, Pacific people, Asians and those of Mediterranean or Middle Eastern origin.
Once anemia is classified according to the MCV levels, further tests will help differentiate between specific causes. These tests consist of:
• Hematinics (agents that increase the level of hemoglobin): B12, folate, ferritin
• Iron studies: iron, transferrin/total binding capacity (TBC), transferrin saturation, ferritin, soluble transferrin receptor
• Thyroid function tests• Peripheral blood film• Hemoglobin electrophoresis• Bilirubin (raised in hemolysis)
Elevated hemoglobin (Hgb) and hematocrit (HCT) levels can reflect either decreased plasma volume (dehydration, alcohol, cigarettes) or increased red cell mass (polycythemia).
RBC distribution width (RDW) is used in conjunction with MCV to determine if anemia is due to a mixed or a single cause. A raised RDW (increased variation in RBC volumes) is called anisocytosis.
The mean corpuscular hemoglobin (MCH) reflects the colour of the RBCs. A reduced quantity of hemo-globin (low MCH) will be indicated by the word hypo-chromic. Most microcytic anemias are hypochromic (except anemia of chronic disease). Most normocytic and macrocytic anemias are normochromic.
The RBC indices are useful for building a picture of the many patterns suggested by hemoglobin results. However isolated abnormalities of these indices are generally not significant for underwriting.
Peripheral Blood FilmAlso known as “blood smear,” this test is often used as follow-up to abnormal CBC results. It helps to
diagnose and/or moni-tor different conditions that affect the blood cells. Automated sys-tems examine a drop of blood smeared onto a glass slide and stained, looking for blood cells of unusual shapes or sizes.
Usually, only normal, mature or nearly ma-ture blood cells are released into the blood-stream, but certain cir-
cumstances can induce the bone marrow to release immature and/or abnormal cells into the circulation. When a significant number or a certain type of ab-normal blood cells is present, it can suggest a medical condition.
Abnormalities more commonly seen on a blood smear and their significance are provided in Table 2 (next page).
Abnormalities that are not as common, but are im-portant because they can be due to significant medical conditions are provided in Table 3 (next page).
Rarely, parasites can also be found in a blood film (e.g., malarial parasites in RBCs).
As with the interpretation of subtle CBC abnormali-ties, the peripheral blood smear results must be in-terpreted keeping the clinical context in mind at all times.
ConclusionMany different conditions can result in changes in the number, size and shape of the blood cell populations. In order to investigate these changes, a complete blood count (CBC) is performed, followed sometimes by a blood smear.
Parameters for normal CBC lab values differ among age groups, genders and laboratories.
The individual’s hydration status can significantly alter CBC values: overhydration can dilute the per-centage of blood cells in the peripheral blood, while dehydration can cause hemoconcentration; both will result in misleading blood cell counts. It’s important
Microcytic NormocyticMacrocytic
Megaloblastic Non-megaloblasticIron deficiency anemia (most common cause)
Acute blood loss Vit. B12 defi-ciency
Alcohol
Thalassemia (Hgb may be normal or only slightly
low)
Hemolytic anemia Folate deficiency Reticulocytosis
Sideroblastic anemia Sickle cell disease Liver diseasePregnancy
Anemia of chronic disease Hypothyroidism Bone marrow failure
Table 1
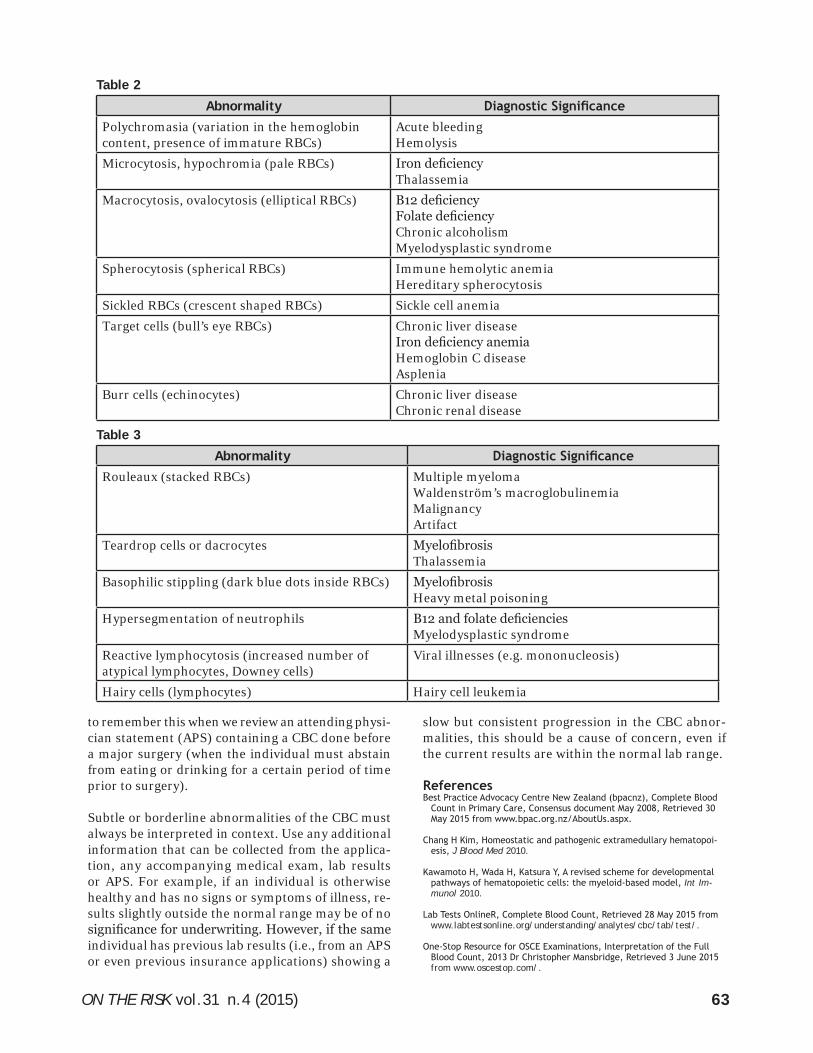
ON THE RISK vol.31 n.4 (2015) 63
to remember this when we review an attending physi-cian statement (APS) containing a CBC done before a major surgery (when the individual must abstain from eating or drinking for a certain period of time prior to surgery).
Subtle or borderline abnormalities of the CBC must always be interpreted in context. Use any additional information that can be collected from the applica-tion, any accompanying medical exam, lab results or APS. For example, if an individual is otherwise healthy and has no signs or symptoms of illness, re-sults slightly outside the normal range may be of no significance for underwriting. However, if the same individual has previous lab results (i.e., from an APS or even previous insurance applications) showing a
Abnormality Diagnostic SignificancePolychromasia (variation in the hemoglobin content, presence of immature RBCs)
Acute bleedingHemolysis
Microcytosis, hypochromia (pale RBCs) Iron deficiencyThalassemia
Macrocytosis, ovalocytosis (elliptical RBCs) B12 deficiencyFolate deficiencyChronic alcoholismMyelodysplastic syndrome
Spherocytosis (spherical RBCs) Immune hemolytic anemiaHereditary spherocytosis
Sickled RBCs (crescent shaped RBCs) Sickle cell anemiaTarget cells (bull’s eye RBCs) Chronic liver disease
Iron deficiency anemiaHemoglobin C diseaseAsplenia
Burr cells (echinocytes) Chronic liver diseaseChronic renal disease
slow but consistent progression in the CBC abnor-malities, this should be a cause of concern, even if the current results are within the normal lab range.
ReferencesBest Practice Advocacy Centre New Zealand (bpacnz), Complete Blood
Count in Primary Care, Consensus document May 2008, Retrieved 30 May 2015 from www.bpac.org.nz/AboutUs.aspx.
Chang H Kim, Homeostatic and pathogenic extramedullary hematopoi-esis, J Blood Med 2010.
Kawamoto H, Wada H, Katsura Y, A revised scheme for developmental pathways of hematopoietic cells: the myeloid-based model, Int Im-munol 2010.
Lab Tests OnlineR, Complete Blood Count, Retrieved 28 May 2015 from www.labtestsonline.org/understanding/analytes/cbc/tab/test/.
One-Stop Resource for OSCE Examinations, Interpretation of the Full Blood Count, 2013 Dr Christopher Mansbridge, Retrieved 3 June 2015 from www.oscestop.com/.
Table 2
Table 3
Abnormality Diagnostic SignificanceRouleaux (stacked RBCs) Multiple myeloma
Waldenström’s macroglobulinemiaMalignancyArtifact
Teardrop cells or dacrocytes MyelofibrosisThalassemia
Basophilic stippling (dark blue dots inside RBCs) MyelofibrosisHeavy metal poisoning
Hypersegmentation of neutrophils B12 and folate deficienciesMyelodysplastic syndrome
Reactive lymphocytosis (increased number of atypical lymphocytes, Downey cells)
Viral illnesses (e.g. mononucleosis)
Hairy cells (lymphocytes) Hairy cell leukemia
ON THE RISK vol.31 n.4 (2015)64
Dr Choladda Vejabhuti Curry, Differential Blood Count, Medscape, up-dated 14 January 2015, Retrieved 30 May 2015 from www.emedicine.medscape.com/article/2085133-overview#aw2aab6b3.
PatientPlus UK, Peripheral Blood Film, Dr Laurence Knott, December 2012, Retrieved 3 June 2015 from www.patient.info/doctor/peripher-al-blood-film.
Lab Tests OnlineR, Blood Smear: Details on RBCs, WBCs, Retrieved 3 June 2015 from www.labtestsonline.org/understanding/analytes/blood-smear/details/start/1.
About the AuthorOana Telfer, MD, FALU, FLMI, ARA, is Assistant Vice President in the Corporate Underwriting and Claims Risk Management Department at Sun Life. She is familiar with both North American and Asian insurance markets, and in her role she provides support and mentoring for Sun Life’s underwriters and claim adjudica-tors on both continents. She is also responsible for maintaining Sun Life’s Worldwide Underwriting manual competitive and up-to-date. Oana holds a medical doctor degree from University Iuliu Hatieganu, Romania. Since coming to Canada in 2003, she has worked as an underwriter in various insurance companies, join-ing Sun Life’s Canadian Individual Insurance team in November 2008. She moved to the corporate team in February 2013, and for the past 2½ years she has been involved in writing ALU examination questions as part of ALU’s Education Committee. This is Oana’s first article for ON THE RISK.
(Left) The ALU embraces generational continu-ity! From the 2015 ALU Annual Meeting (left to right): Past ALU Chair Roland Paradis, AXA, Medical Underwriting Task Force, and his son Brendan Paradis, MetLife, Exam 101 Group (and 2016 OTR Administrative Editor).
(Right) The ALU Marketing Group at the ALU Annual Meeting (left to right): Carla Martin, ExamOne; Di-rector of Marketing Jennifer Dahl, RBC Insurance; William Dumpman, Genworth Financial.

ON THE RISK vol.31 n.4 (2015) 65
LOW CHOLESTEROL AND LOW ALBUMIN LEVELS:ALERTS TO HIDDEN MORTALITY RISK
Executive Summary Total cholesterol (TC) ≤130 mg/dL for women and ≤140 mg/dL for men was present in a small percentage of life insurance applicants and identified substantially increased mortality risk. For albumin, the comparable low values were ≤3.9 g/dL for women and ≤4.1 g/dL for men. Still lower cut-off levels of TC and albumin were also identified where risk remained even if other laboratory studies, BP and build were unremarkable.
Michael Fulks, MD Robert L. Stout, PhD [email protected] [email protected]
Clinical Reference LaboratoryLenexa, KS
IntroductionLow levels of total cholesterol (TC) and albumin may be associated with excess mortality in insur-ance applicants.1,2 Diseases or conditions potentially responsible for both findings include cirrhosis, poor nutrition, inflammatory conditions, advanced malig-nancy and congestive heart failure, all of which may be symptomatically silent or at least unknown to the underwriter. Low TC may also be caused by aggressive lipid therapy for cardiovascular disease. But low TC may also simply be the result of favorable heredity and low albumin the result of 2nd or 3rd trimester pregnancy, neither of which has excess risk. The degree of risk can be better defined by review of de-mographic, medical history, physical measurements and other laboratory results, but some risk may po-tentially remain even if such review is unremarkable.
We conducted a study to determine what low levels of total TC or albumin suggest that further underwrit-ing review is needed, and what low levels suggest increased risk even if no other findings are apparent after review.
How the Study Was DoneApplicants tested at CRL from 1991 to 2007 with both blood chemistry and urine cotinine results were matched to the Social Security Death Master File to obtain vital status in September 2011, and then were de-identified prior to the study. This provided 7,582,518 applicants with 144,725 deaths. We per-formed a survival analysis utilizing Cox regression (IBM SPSS 22) splitting applicants by sex and by age 20-59 and 60-89, with age and smoking status (cotinine ≥200 ng/mL) included as covariates. Rela-tive mortality curves by TC or albumin levels were constructed for all applicants and for only those applicants who had unremarkable values for other
tests, BP and build. “Unremarkable” was defined by an overall lab score (CRL Smart Score) <50, which includes the 71% of applicants with the lowest mortal-ity risk based on lab results, BP and build.
What the Study FoundFigures 1 and 2 (page 66) show relative mortality for men age <60 and 60+ based on TC level, with those having values ≥211 mg/dL comprising the reference band. Relative mortality increased by >25% at TC values ≤140 mg/dL (3.8% of all men in the study). Based on the pool when the composite of other test results, build and BP was unremarkable, relative risk increased >25% when total TC was ≤120 mg/dL (0.5% of all men in the study).
Figures 3 and 4 (page 67) show comparable findings for women based on total TC. Relative mortality is increased by >25% at values ≤130 mg/dL (2.1% of all women in the study). Based on the pool when the composite of other test results, build and BP was unremarkable, risk increased >25% when total TC reached ≤120 mg/dL for age <60 (0.6% of all younger women in the study), but showed little increase in risk at older ages.
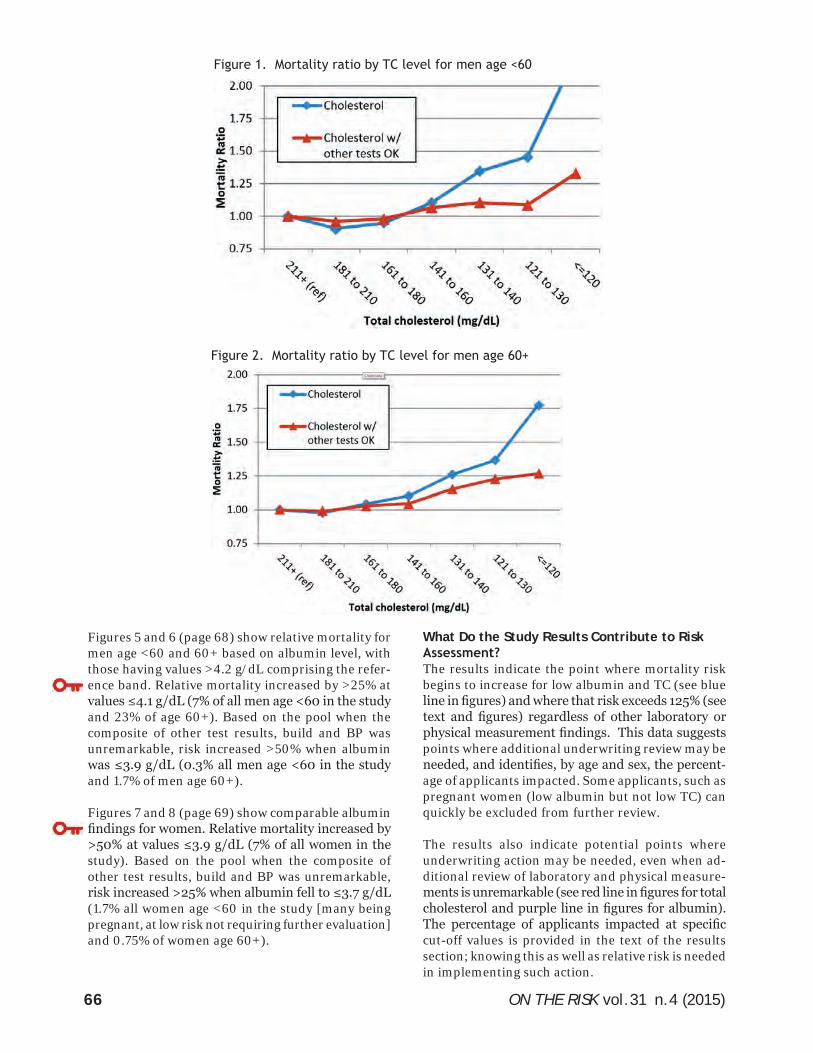
ON THE RISK vol.31 n.4 (2015)66
Figures 5 and 6 (page 68) show relative mortality for men age <60 and 60+ based on albumin level, with those having values >4.2 g/dL comprising the refer-ence band. Relative mortality increased by >25% at values ≤4.1 g/dL (7% of all men age <60 in the study and 23% of age 60+). Based on the pool when the composite of other test results, build and BP was unremarkable, risk increased >50% when albumin was ≤3.9 g/dL (0.3% all men age <60 in the study and 1.7% of men age 60+).
Figures 7 and 8 (page 69) show comparable albumin findings for women. Relative mortality increased by >50% at values ≤3.9 g/dL (7% of all women in the study). Based on the pool when the composite of other test results, build and BP was unremarkable, risk increased >25% when albumin fell to ≤3.7 g/dL (1.7% all women age <60 in the study [many being pregnant, at low risk not requiring further evaluation] and 0.75% of women age 60+).
What Do the Study Results Contribute to Risk Assessment?The results indicate the point where mortality risk begins to increase for low albumin and TC (see blue line in figures) and where that risk exceeds 125% (see text and figures) regardless of other laboratory or physical measurement findings. This data suggests points where additional underwriting review may be needed, and identifies, by age and sex, the percent-age of applicants impacted. Some applicants, such as pregnant women (low albumin but not low TC) can quickly be excluded from further review.
The results also indicate potential points where underwriting action may be needed, even when ad-ditional review of laboratory and physical measure-ments is unremarkable (see red line in figures for total cholesterol and purple line in figures for albumin). The percentage of applicants impacted at specific cut-off values is provided in the text of the results section; knowing this as well as relative risk is needed in implementing such action.
Figure 1. Mortality ratio by TC level for men age <60
Figure 2. Mortality ratio by TC level for men age 60+
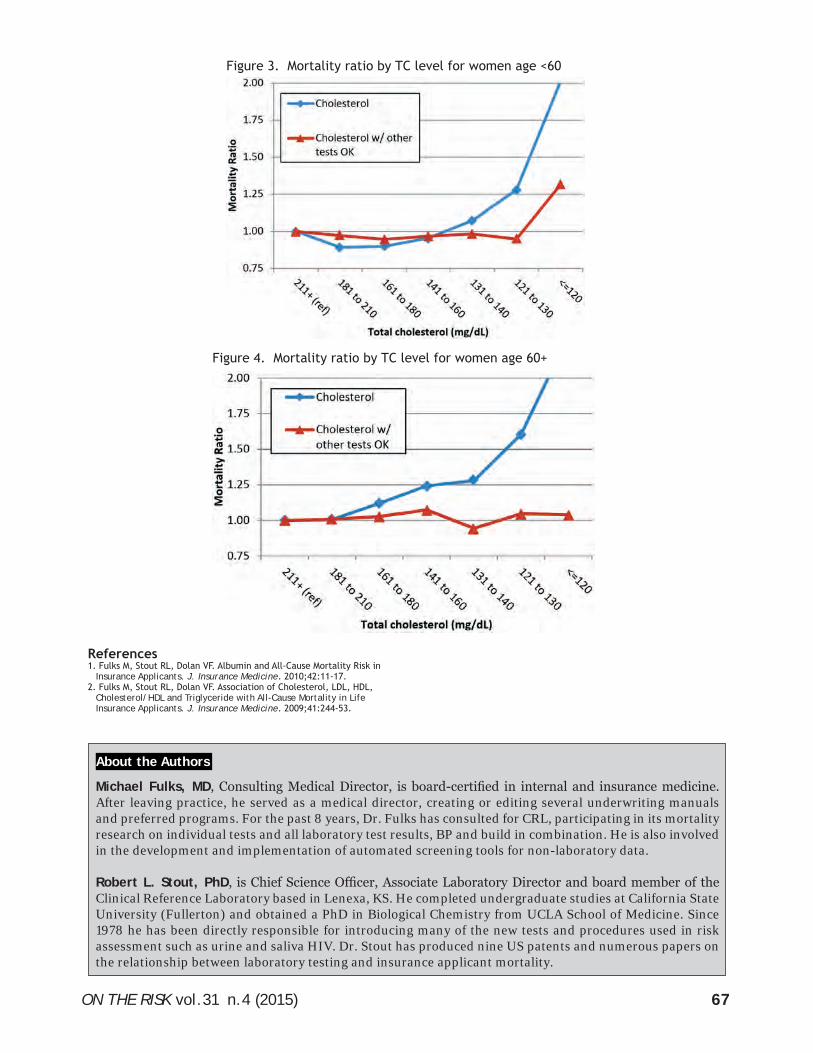
ON THE RISK vol.31 n.4 (2015) 67
Figure 3. Mortality ratio by TC level for women age <60
Figure 4. Mortality ratio by TC level for women age 60+
References1. Fulks M, Stout RL, Dolan VF. Albumin and All-Cause Mortality Risk in
Insurance Applicants. J. Insurance Medicine. 2010;42:11-17.2. Fulks M, Stout RL, Dolan VF. Association of Cholesterol, LDL, HDL,
Cholesterol/HDL and Triglyceride with All-Cause Mortality in Life Insurance Applicants. J. Insurance Medicine. 2009;41:244-53.
Michael Fulks, MD, Consulting Medical Director, is board-certified in internal and insurance medicine. After leaving practice, he served as a medical director, creating or editing several underwriting manuals and preferred programs. For the past 8 years, Dr. Fulks has consulted for CRL, participating in its mortality research on individual tests and all laboratory test results, BP and build in combination. He is also involved in the development and implementation of automated screening tools for non-laboratory data.
Robert L. Stout, PhD, is Chief Science Officer, Associate Laboratory Director and board member of the Clinical Reference Laboratory based in Lenexa, KS. He completed undergraduate studies at California State University (Fullerton) and obtained a PhD in Biological Chemistry from UCLA School of Medicine. Since 1978 he has been directly responsible for introducing many of the new tests and procedures used in risk assessment such as urine and saliva HIV. Dr. Stout has produced nine US patents and numerous papers on the relationship between laboratory testing and insurance applicant mortality.
About the Authors
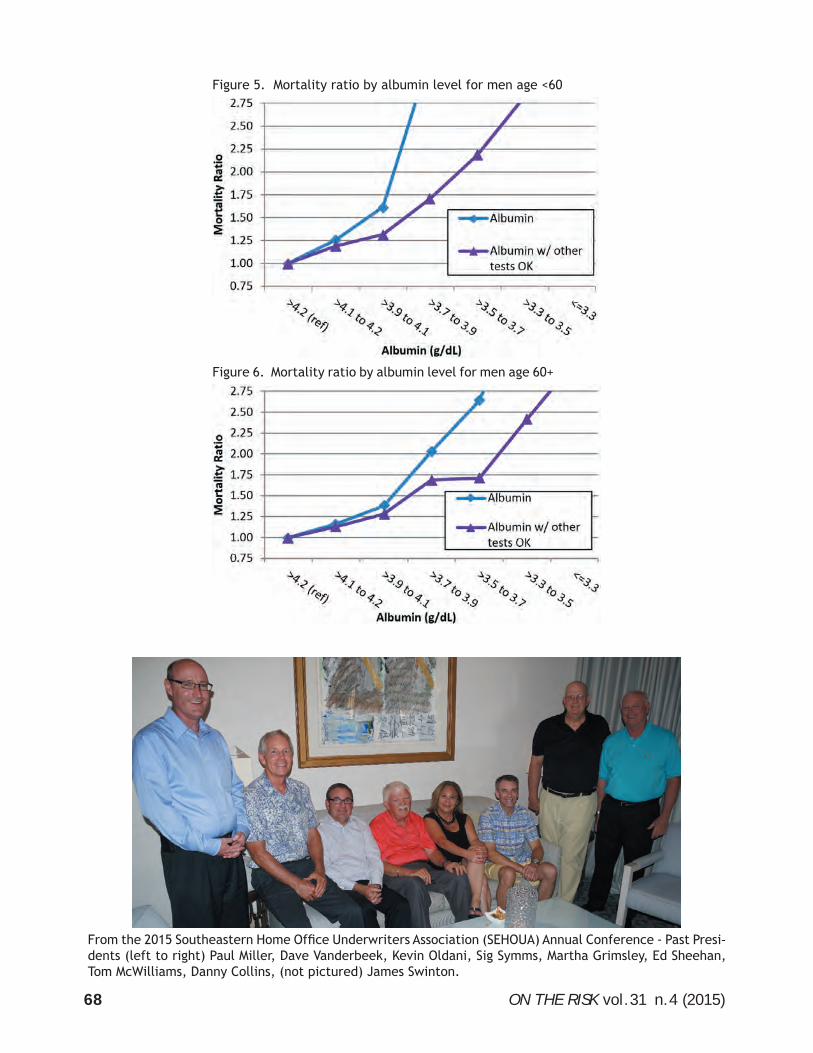
ON THE RISK vol.31 n.4 (2015)68
Figure 5. Mortality ratio by albumin level for men age <60
Figure 6. Mortality ratio by albumin level for men age 60+
From the 2015 Southeastern Home Office Underwriters Association (SEHOUA) Annual Conference - Past Presi-dents (left to right) Paul Miller, Dave Vanderbeek, Kevin Oldani, Sig Symms, Martha Grimsley, Ed Sheehan, Tom McWilliams, Danny Collins, (not pictured) James Swinton.
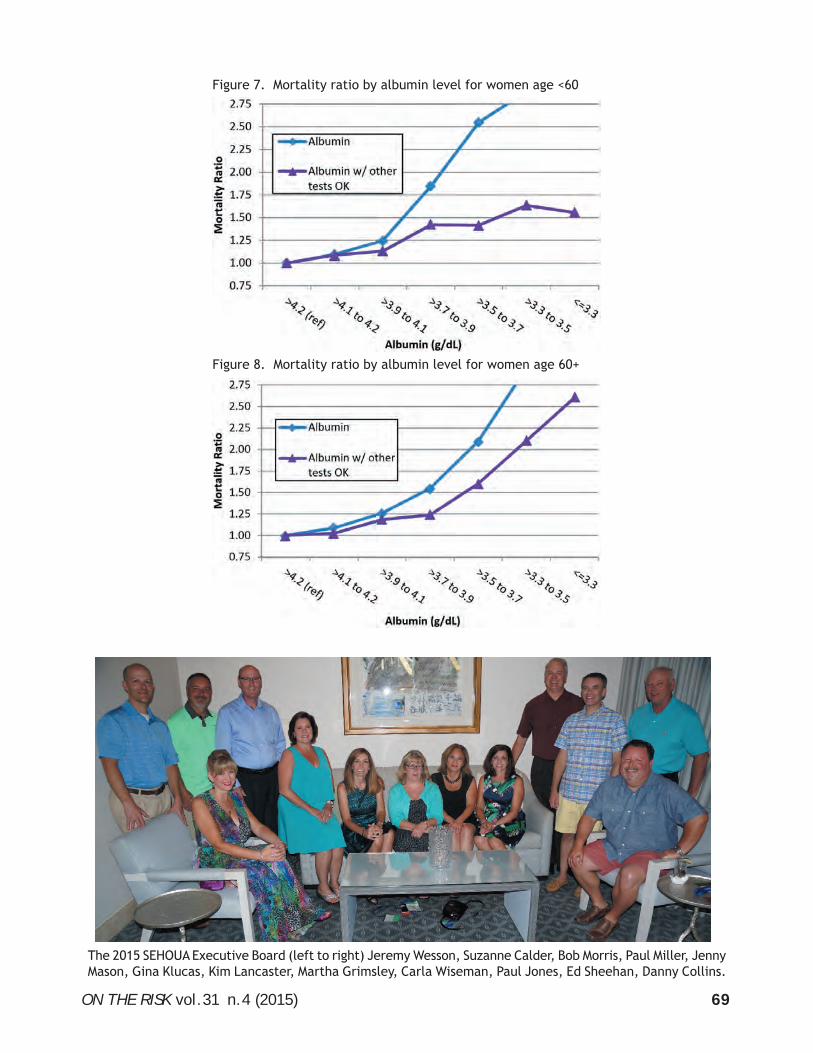
ON THE RISK vol.31 n.4 (2015) 69
Figure 8. Mortality ratio by albumin level for women age 60+
Figure 7. Mortality ratio by albumin level for women age <60
The 2015 SEHOUA Executive Board (left to right) Jeremy Wesson, Suzanne Calder, Bob Morris, Paul Miller, Jenny Mason, Gina Klucas, Kim Lancaster, Martha Grimsley, Carla Wiseman, Paul Jones, Ed Sheehan, Danny Collins.

ON THE RISK vol.31 n.4 (2015)70
MATURE AGE UNDERWRITING
Executive Summary With the increasing number of mature age applicants applying for life insur-ance, are the current requirements appropriate. This article will review the current testing, review how results could impact mortality, and discuss additional testing to be considered. Due to the possible significant impact on mortality, this article will review the assessment of cognition and the tools available for testing.
Dr. Jamie MorrisonAssistant Medical DirectorLondon Life Toronto, [email protected]
In recent decades, there has been an increase in ap-plicants older than age 65 applying for life insurance and it is expected that those numbers will continue to grow. They tend to apply for larger face amounts of insurance, with larger premiums attached. More in-depth and detailed underwriting is required for these applicants, but are our present requirements appropriate and sufficient to assess the whole risk?
This article will review current testing and discuss how the results might impact risk assessment differ-ently in older age applicants. Additional lab testing, as well as testing of cognition and functioning that may be useful in assessing mortality risk in mature ages, will also be discussed. Of course, the cost/benefit ratio of any new testing must be considered, and this must be further reviewed before implementing.
For this discussion, age greater than 65 will be consid-ered ‘mature age,’ but many of the studies referenced use many different age thresholds.
Current testing and the impact in mature agesCommonly, present insurance lab testing includes blood tested for lipids, glucose, liver enzymes, kidney function, total protein, albumin, globulin and HIV, with the urine tested for protein, blood, white blood cells (and other sediment), cotinine and cocaine. In addition to the labs, the blood pressure, pulse and build (height and weight) are also measured.
The question is, do the results from these lab tests and vitals impact older ages differently with respect to mortality? For example, is a total cholesterol of 3.2 as concerning in a 30-year-old as it is in an 80-year-old? Conversely, is a total cholesterol of 8.5 as significant in an 80-year-old as it is in a 30-year-old?
Lipids/cholesterol - There is evidence showing that low cholesterol (not as a result of lipid lowering medications) in older ages has a significant impact on mortality, with cholesterol levels being inversely proportional to total mortality at ages greater than 65. Conversely, in older ages higher levels of cholesterol may actually have a positive impact on survival.(1,2,3,4,5)
Build - Low build is of concern in older ages and is associated with increased mortality, especially with a body mass index (BMI) of less than 25. Some studies have even shown that low build has a more significant impact on mortality than overweight or obese elderly.(6)
Blood sugars (glucose) - Tend to show a slight rise as we age and changes in sugar metablolism are less con-cerning in older ages. That is to say, if a 78-year-old develops diabetes and the blood glucose and HbA1c are borderline, we would be less concerned from an underwriting perspective than if he had developed it at age 50.
Albumin - Decreases approximately 20% during an inflammatory process and is inversely correlated to age, smoking, blood pressure and obesity, and is an independent risk factor for all-cause mortality.(6,7)
Generally, there is less difference in the approach to underwriting abnormalities in liver enzymes and kidney function tests across the ages. Our kidneys lose about 1% of their function every year, so slight increases in creatinine (or reduction in eGFR) in older ages may be expected. However, there is evidence to show that moderate renal insufficiency does adversely affect mortality in older ages and needs to be consid-ered accordingly.(8,9)
Review of lab and functional testing that could assist in our risk assessmentComplete blood count (CBC) -includes the levels of hemoglobin, white blood cells and platelets – Ane-mia (low hemoglobin) is one of the more concerning

ON THE RISK vol.31 n.4 (2015) 71
findings that would be elicited from a CBC and can be caused by blood loss (most concerning would be undetected neoplasms such as colon cancer), nutri-tional deficits and chronic diseases, all of which tend to be more prevalent in older ages. From a mortality perspective, detecting anemia is quite important as evidence shows that there is up to a two-fold increased risk of death associated with it.(10,11,12) However, clients who have more benign forms of anemia such as the hemoglobinopathies (certain thalassemias) should be ruled out as they have minimal effect on mortality. Certainly, anemia that is new and/or undiagnosed should be fully worked up by the applicant’s physician to establish the cause.
Adding a CBC would likely require only minimal changes at the lab and paramedical level, and the cost of performing the CBC itself is approximately $4 to $5.
Functional assessment - In addition to the labs and vitals, important information can be obtained by testing functional status through examination of gait and lung function. A lot can be learned observing a person walk a few meters or blow into a small tube!
Peak expiratory flow (PEF) can be tested fairly easily by blowing into a handheld PEF meter, the results given as liters/min of airflow. The equipment is relatively inexpensive (cost is about $15 to $20 for a basic meter), it would take minimal training by paramedical staff, and is generally not a difficult test to perform for the client. Despite this, there still could be issues with the client effort and ability to follow the instructions properly, which could possibly give inaccurate results. However, it is a good predictor of 5-year mortality with an increase in mortality every 100 L/min drop in PEF.(13,14)
Gait speed is not only reflective of health and func-tional status but a significant predictor of survival in older ages(15) and can be assessed by the Timed Up and Go test (TUG). This involves a client rising from sitting in a chair, walking 3 meters, turning around, walking back and sitting down. This activity is timed from the word “go” when getting up from the chair and, if needed, the client may use his usual walking aid. Generally, completing this exercise in greater than 15 seconds is concerning, and studies have shown significant increases in mortality with every drop of 0.1 m/sec of gait speed.(15)
The TUG would likely require less cost overall as the equipment needed (chair, comfortable clothes) would be found in the person’s home or office.
Assessment of cognition – mild cognitive impair-ment (mci) and dementiaAccording to the Alzheimer’s Society of Canada, ap-proximately 747, 000 people, or 14.9% of Canadians over age 65, were living with cognitive impairment (including dementia) in 2011. That number is ex-pected to almost double by 2031. In addition to the staggering numbers, dementia has a significant impact on mortality, with the median survival from diagnosis of 5.7 years for women and only 4.2 years for men(16) with some studies even showing a median survival of only 3.3 years overall.(17) The age at diag-nosis matters as well, with a median survival of 8.3 years when diagnosed at age 65, dropping to 3.4 years when diagnosed at age 90.(18)
Noting this significant impact on survival, most insur-ance companies are unlikely to insure clients who are diagnosed with dementia. So, is there a way to find applicants who are at an earlier stage of cognitive decline and are they insurable?
An interim stage between normal cognition and dementia: MCIMild cognitive impairment (MCI) is a relatively novel term, introduced in 1991, and becoming a clinically recognized syndrome in the late 1990s. It is recognized as an intermediate stage between normal cognition and dementia, representing a cognitive decline greater than expected for age and education level that does not interfere with activities of daily living (unlike dementia, which does affect ADLs). As a heterogeneous entity, the diagnosis of MCI relies on clinical judgement, corroborators of the history (fam-ily members, etc.) as well as which criteria are used.
The prevalence of MCI is noted between 14-18% after the age of 70(19,20,21,22,23,24) with an annual conversion rate to dementia of 4 to 15%.(25,26,27,28) We would therefore expect about 100% conversion to dementia by 10 years. However, studies show that the 10-year cumulative risk is only 30-50%(25,26,29) suggesting that not all people diagnosed with MCI will progress to full dementia.
Mortality and MCINoting the conversion rates of MCI to dementia and the effect of dementia on mortality, one might infer that the mortality impact of MCI would also be signifi-cant. Somewhat surprisingly, however, studies show the overall risk of death from MCI is only between 1.2 and 1.7 times normal(30,31,32,33,34) with some studies showing that the largest mortality risk is in the first 2 years after diagnosis and falls off after 9 years.(34) It raises the possibility that applicants with MCI may

ON THE RISK vol.31 n.4 (2015)72
be insurable, but also the concern that it may not be worth screening for.
ScreeningIf the choice is made to screen for cognitive impair-ment, there are many issues to address, and optimally a test used by an insurance company should be: a) succinct, b) easy to train the paramedical examiner to administer, c) acceptable to the applicants and easy to take, d) unbiased by language and education level, e) better at detecting MCI (than dementia).
With the novelty of MCI, there is minimal data to support an effective screening test specifically for MCI, or even to compare the effectiveness of a screen-ing test to differentiate between MCI and dementia. However, as we are becoming increasingly aware of patients with MCI, more information is emerging on which tests will perform the best.
There are multiple screening tests for cognitive im-pairment available to clinicians and they can be cat-egorized by the time it takes to administer: very short (<2 minutes), short (2 to 5 minutes) and standard (7 to 10 minutes). The commonly used Mini-mental status examination (MMSE) has a relatively low sen-sitivity for MCI(35,36) and is an example of a “standard” test that doesn’t fit well into the parameters of an optimal test for an insurance company, having many components and taking some time to complete. There is also evidence to show that using subcomponents of the MMSE may offer greater power and discrimi-nation(37) which has led to the development of more succinct screening tests. A good example of a test that may be more appropriate for screening by an insur-ance company is the use of a three-word recall and a clock-drawing test (e.g., Mini-Cog) which is easy and quick to administer and relatively unaffected by language and education level.(38) It is at least as effec-tive as the MMSE or longer neuropsychiatric testing in detecting dementia(39,40) and detected almost 60% of patients with MCI.(41) As well, it tests for many aspects of cognition including memory, comprehen-sion, perception, gross motor function, visual spatial organization, concentration, numerical knowledge, concept of time and inhibition of distracting stimuli.
We must also consider that screening does not confer a specific diagnosis (of either MCI or dementia) and any abnormal results should be further assessed by the applicant’s physician. Of course, from an insur-ance company’s perspective, a proportion of these could be false-positive results and likely would have been declined insurance as such, resulting in lost business.
SummaryIt seems prudent that we should re-examine our ap-proach to many of our lab results and how they impact mortality in the mature age applicant. There is good evidence to consider adding additional screening tests, which include additional labs, assessment of functional status and cognitive function.
With the available mortality data and the information about screening tests, the next steps should include further discussions with the medical board, chief underwriters, actuarial and pricing departments to review the cost/benefits of adding any of the afore-mentioned assessments or screening tests to our risk assessment of the “mature age” applicants.
References(1) Päivi Tuikkala, Sirpa Hartikainen, Maarit J. Korhonen, Piia Lavi-
kainen, Raimo Kettunen, Raimo Sulkava & Hannes Enlund. Serum total cholesterol levels and all-cause mortality in a home-dwelling elderly population: a six-year follow-up. Scandinavian Journal of Primary Health Care, 2010; 28: 121–127.
(2) Newson RS, Felix JF, Heeringa J, Hofman A, Witteman JC, Tiemeier H. Association between serum cholesterol and non cardiovascular mortality in older age. J Am Geriatr Soc. 2011 Oct;59(10):1779-85.
(3) Annelies WE Weverling-Rijnsburger MD, Gerard J Blauw MD, A Margot Lagaay MD, Dick L Knock PhD, A Edo Meinders MD, Rudi GJ Westendorp MD. Total cholesterol and risk of mortality in the oldest old. The Lan-cet, Volume 350, Issue 9085, Pages 1119 - 1123, 18 October 1997.
(4) R.S. Spada, G. Toscano, F.I.I. Cosentino, I. Iero, B. Lanuzza, M. Tripodi, R. Ferri. Low total cholesterol predicts mortality in the non-demented oldest old. Archives of Gerontology and Geriatrics Volume 44, Supplement, Pages 381-384, 2007.
(5) Schupf N, Costa R, Luchsinger J, Tang MX, Lee JH, Mayeux R. Rela-tionship between plasma lipids and all-cause mortality in nondement-ed elderly. J Am Geriatr Soc. 2005 Feb;53(2):219-26.
(6) Mara A. Schonberg, MD, MPH, Roger B. Davis, ScD, Ellen P. McCarthy, PhD, MPH, and Edward R. Marcantonio, MD, SM. Index to Predict 5-Year Mortality of Community-Dwelling Adults Aged 65 and Older Us-ing Data from the National Health Interview Survey. J Gen Intern Med. 2009 October; 24(10): 1115–1122.
(6) Corti MC, Guralnik JM, Salive ME, Sorkin JD. Serum albumin level and physical disability as predictors of mortality in older persons. JAMA. 1994 Oct 5;272(13):1036-42.
(7) Weijenberg MP, Feskens EJ, Souverijn JH, Kromhout D. Serum albu-min, coronary heart disease risk, and mortality in an elderly cohort. Epidemiology. 1997 Jan;8(1):87-92.
(8) Marcello Tonelli, Natasha Wiebe,Bruce Culleton, Andrew House, Chris Rabbat, Mei Fok, Finlay McAlister, and Amit X. Garg. Chronic Kid-ney Disease and Mortality Risk: A Systematic Review. J Am Soc Nephrol 17: 2034–2047, 2006.
(9) Maaravi Y, Bursztyn M, Hammerman-Rozenberg R, Cohen A, Stessman J. Moderate renal insufficiency at 70 years predicts mortality. QJM. 2006 Feb;99(2):97-102. Epub 2006 Jan 11.
(10) Shavelle RM, MacKenzie R, Paculdo DR. Anemia and mortality in older persons: does the type of anemia affect survival? Int J Hematol. 2012 Mar;95(3):248-56. Epub 2012 Feb 21.
(11) Endres HG, Wedding U, Pittrow D, Thiem U, Trampisch HJ, Diehm C. Prevalence of anemia in elderly patients in primary care: impact on 5-year mortality risk and differences between men and women. Curr Med Res Opin. 2009 May;25(5):1143-58.
(12) Woodman R, Ferrucci L, Guralnik J. Anemia in older adults. Curr Opin Hematol. 2005 Mar;12(2):123-8.
(13) Cook NR, Evans DA, Scherr PA, Speizer FE, Taylor JO, Hennekens CH. Peak expiratory flow rate and 5-year mortality in an elderly popu-lation. Am J Epidemiol. 1991 Apr 15;133(8):784-94.
(14) Carlos A. Vaz Fragoso, MD,1,2 Evelyne A. Gahbauer, MD, MPH,1 Peter H. Van Ness, PhD, MPH,1 John Concato, MD, MS, MPH,1,2 and Thomas M. Gill, MD1. Peak expiratory flow as a predictor of subse-quent disability and death in community-living older persons. J Am Geriatr Soc. 2008 June; 56(6): 1014–1020.
(15) Dr. Stephanie Studenski, MD, MPH, Dr. Subashan Perera, PhD, Dr. Kushang Patel, PhD, Dr. Caterina Rosano, MD, PhD, Dr. Kimberly Faulkner, PhD, Dr. Marco Inzitari, MD, PhD, Dr. Jennifer Brach, PhD, Dr. Julie Chandler, PhD, Dr. Peggy Cawthon, PhD, Dr. Elizabeth Barrett Connor, MD, Dr. Michael Nevitt, PhD, Dr. Marjolein Visser, PhD, Dr. Ste-

ON THE RISK vol.31 n.4 (2015) 73
phen Kritchevsky, PhD, Dr. Stefania Badinelli, MD, Dr. Tamara Harris, MD, Dr. Anne B. Newman, MD, Dr. Jane Cauley, PhD, Dr. Luigi Ferrucci, MD, PhD, and Dr. Jack Guralnik, MD, PhD. Gait Speed and Survival in Older Adults. JAMA. 2011 January 5; 305(1): 50–58.
(16) Survival after initial diagnosis of Alzheimer disease. Larson EB, Shadlen MF, Wang L, McCormick WC, Bowen JD, Teri L, Kukull WA. Ann Intern Med. 2004 Apr 6;140(7):501-9.
(17) A reevaluation of the duration of survival after the onset of dementia. Wolfson C, Wolfson DB, Asgharian M, M'Lan CE, Ostbye T, Rockwood K, Hogan DB; Clinical Progression of Dementia Study Group. N Engl J Med. 2001 Apr 12;344(15):1111-6.
(18) Survival following a diagnosis of Alzheimer disease. Brook-meyer R, Corrada MM, Curriero FC, Kawas C. Arch Neurol. 2002 Nov;59(11):1764-7.
(19) Mild cognitive impairment: clinical characterization and outcome. Petersen RC, Smith GE, Waring SC, Ivnik RJ, Tangalos EG, Kokmen E. Arch Neurol. 1999;56(3):303.
(20) Mild cognitive impairment, amnestic type: an epidemiologic study. Ganguli M, Dodge HH, Shen C, DeKosky ST. Neurology. 2004;63(1):115.
(21) Classification criteria for mild cognitive impairment: a population-based validation study. Ritchie K, Artero S, Touchon J. Neurology. 2001;56(1):37.
(22) Incidence and outcome of mild cognitive impairment in a popula-tion-based prospective cohort. Larrieu S, Letenneur L, Orgogozo JM, Fabrigoule C, Amieva H, Le Carret N, Barberger-Gateau P, Dartigues JF. Neurology. 2002;59(10):1594.
(23) Conversion to dementia from mild cognitive disorder: the Cache County Study. Tschanz JT, Welsh-Bohmer KA, Lyketsos CG, Corcoran C, Green RC, Hayden K, Norton MC, Zandi PP, Toone L, West NA, Breitner JC, Cache County Investigators. Neurology. 2006;67(2):229.
(24) Mild cognitive impairment: prevalence and predictive validity according to current approaches. Busse A, Bischkopf J, Riedel-Heller SG, Angermeyer MC, Leipzig Longitudinal Study of the Aged LEILA75+. Acta Neurol Scand. 2003;108(2):71.
(25) Rate of progression of mild cognitive impairment to dementia--meta-analysis of 41 robust inception cohort studies. Mitchell AJ, Shiri-Feshki M. Acta Psychiatr Scand. 2009 Apr;119(4):252-65.
(26) Progression of Mild Cognitive Impairment to Dementia in Clinic- vs Community-Based Cohorts. Sarah Tomaszewski Farias, PhD; Dan Mungas, PhD; Bruce R. Reed, PhD; Danielle Harvey, PhD; Charles DeCarli, MD. Arch Neurol. 2009;66(9):1151-1157. doi:10.1001/arch-neurol.2009.106.
(27) Aging, memory, and mild cognitive impairment. Petersen RC, Smith GE, Waring SC, Ivnik RJ, Kokmen E, Tangelos EG. Department of Neu-rology, Mayo Clinic, Rochester, MN 55905, USA.
(28) Mild cognitive impairment: clinical characterization and outcome. Petersen RC, Smith GE, Waring SC, Ivnik RJ, Tangalos EG, Kokmen E. Department of Neurology, Mayo Clinic, Rochester, Minn 55905, USA.
(29) Ten-year risk of dementia in subjects with mild cognitive impairment. Visser PJ, Kester A, Jolles J, Verhey F. Neurology. 2006;67(7):1201.
(30) Natural history of mild cognitive impairment in older persons. D. A. Bennett, MD, R. S. Wilson, PhD, J. A. Schneider, MD, D. A. Evans, MD, L. A. Beckett, PhD, N. T. Aggarwal, MD, L. L. Barnes, PhD, J. H. Fox, MD and J. Bach, MSW. Neurology July 23, 2002 vol. 59 no. 2 198-205.
(31) Cognitive Impairment: An Independent Predictor of Excess Mortal-ity. A Cohort Study. Greg A. Sachs, MD; Ravan Carter, MA; Laura R. Holtz, BS, CCRP; Faye Smith, MA; Timothy E. Stump, MA; Wanzhu Tu, PhD; and Christopher M. Callahan, MD. Annals of Internal Medicine. 2011:155(5): 300-308.
(32) Mortality in amnestic mild cognitive impairment. A prospective community study. A. L. Hunderfund, MD, R. O. Roberts, MD, MS, T. C. Slusser, BS, C. L. Leibson, PhD, Y. E. Geda, MD, R. J. Ivnik, PhD, E. G. Tangalos, MD and R. C. Petersen, PhD, MD. Neurology November 28, 2006 vol. 67 no. 10 1764-1768.
(33). Level of Cognitive Impairment Predicts Mortality in High-Risk Community Samples: The Memory and Medical Care Study. Hochang B. Lee; Judy D. Kasper; Andrew D. Shore; Jessica L. Yokley; Betty S. Black; Peter V. Rabins. The Journal of Neuropsychiatry and Clinical Neurosciences 2006;18:543-546.
(34). Cognitive impairment and mortality in the community-dwelling elderly. Bassuk SS, Wypij D, Berkman LF. Am J Epidemiol. 2000 Apr 1;151(7):676-88.
(35) Sensitivity and specificity of the mmse and moca in screening for mild and severe cognitive impairment related to dementia Katie Mc-Culloch, M.A.1, 2 & Robert L. Collins, Ph.D. ABPP-CN1, 3.
(36) Methods to improve the detection of mild cognitive impairment. William R. Shankle, A. Kimball Romney, Junko Hara, Dennis Fortier, Malcolm B. Dick, James M. Chen, Timothy Chan, and Xijiang Sun. Departments of Cognitive Science and Anthropology and Brain Aging Research Unit, University of California, Irvine, CA 92612; and Medical Care Corporation, Irvine, CA 92612.
(37) Screening for memory disorders, dementia and Alzheimer’s disease. J Wesson Ashford
(38) The mini-cog: a cognitive 'vital signs' measure for dementia screen-ing in multi-lingual elderly. Borson S, Scanlan J, Brush M, Vitaliano P, Dokmak A. Int J Geriatr Psychiatry. 2000 Nov;15(11):1021-7.
(39) The Mini-Cog as a screen for dementia: validation in a population-based sample. Borson S, Scanlan JM, Chen P, Ganguli M. J Am Geriatr Soc. 2003 Oct;51(10):1451-4.
(40) Improving identification of cognitive impairment in primary care. Soo Borson, James M. Scanlan, Jill Watanabe, Shin, Ping Tu, Mary Lessig.
(41) Improving identification of cognitive impairment in primary care. Soo Borson, James M. Scanlan, Jill Watanabe, Shin, Ping Tu, Mary Lessig.
About the AuthorDr. Jamie Morrison was born and raised in London, ON, and is married with two children. He attended Uni-versity of Western Ontario for his undergraduate years, graduated Medical School in 1992 from University of Toronto and finished a rotating internship in 1993. Dr. Morrison began a family practice in 1993 in London where he practiced until 2007. As well, from 2004 to 2007 he was part owner and practicing physician in a clinic offering non-surgical cosmetic procedures. Dr. Morrison is board-certified in Insurance Medicine and a member of the Canadian Life Insurance Medical Officers Association (CLIMOA) and the American Academy of Insurance Medicine (AAIM). In 2007 he began working as an Assistant Medical Director for London Life, Canada Life and Great West Life, where he continues to work full time and enjoys being a part of the team.
From the 2015 ALU Meeting (left to right): ALU Medical Con-sultants Cathy Percival, RN, BSN, American General Life, and Sue Sokoloski, MD, AXA.

ON THE RISK vol.31 n.4 (2015)74
CHIKUNGUNYA – A NEW TROPICAL DISEASE IN LATIN AMERICA
Executive Summary This article presents infor-mation from recent publications by the World Health Organization (WHO), Centers for Disease Control (CDC), Panamerican Health Organiza-tion (PHO), as well as other health news sources. The focus of this article is on the incidence of chikungunya in Latin America and includes some highlights of the recent outbreak in Central and South America. It also provides a brief definition of the condition and addresses its causes, risk fac-tors, signs and symptoms, diagnosis, treatment, control, prevention and underwriting concerns, particularly relating to life, disability and medi-cal insurance.
Freddy Velasco-A., AALUOTR Latin America EditorL&H Underwriting ConsultantMiami, [email protected]
Epidemiology The Americas have been impacted in recent years by the chikungunya virus that is causing health issues to a significant number of people, particularly in the tropical and subtropical areas of South and Central America as well as the Antilles. This is resulting in the loss of productive work days due to severe discomfort and in some cases temporary disability, which in turn affects the socioeconomic systems in the region. As more and more people are getting infected through-out the continent, it is becoming a big concern to the international community due to the epidemic proportion it is reaching.
Although the recent Ebola outbreak coming from Africa has overshadowed the seriousness of the chi-kungunya situation in Latin America, it is not less important and it deserves much needed attention in order to help control, mitigate and, hopefully, eradicate the aggressive spread of the disease. Entire countries and their governments are being impacted by this disease, and they have already appealed to the international community for support and assistance.
Chikungunya Key Facts• Chikungunya has been identified in over 60 coun-
tries in Asia, Africa, Europe and in most countries in the Americas.
• The virus was first identified in 1952 in Tanzania where it was given its name.
• The name chikungunya derives from a word in the Kimakonde language, meaning “to become contorted” and describes the stooped appearance of sufferers with joint pain (arthralgia).
• It is a mosquito-borne viral, painful and, in some cases, debilitating disease that affects humans who come in contact with the virus.
Transmission Vectors• Chikungunya is an RNA virus that belongs to the
alphavirus genus of the family Togaviridae.
• Transmission to humans occurs by infected vectors or mosquitoes - most commonly Aedes aegypti and Aedes albopictus - carrying the virus, which also transmit dengue.
• The species Aedes albopictus thrives in a wider range of water-filled breeding sites than Aedes aegypti, including coconut husks, cocoa pods, bamboo stumps, tree holes and rock pools, in addition to artificial containers such as vehicle tires and saucers beneath plant pots. This diver-sity of habitats explains the abundance of Aedes albopictus in rural as well as peri-urban areas and shady city parks.
• Aedes aegypti is more closely associated with human habitation and uses indoor breeding sites, including flower vases, water storage vessels and concrete water tanks in bathrooms, as well as the same artificial outdoor habitats as Aedes albopictus.
• Mosquitoes can be found biting throughout day-light hours, though there may be peaks of activity in the early morning and late afternoon. Both species are found biting outdoors.
• Once a human is infected, the virus is transmitted to other humans by the bites of infected female mosquitoes.
ON THE RISK vol.31 n.4 (2015) 75
Risk FactorsPeople traveling to or living in infected areas in Latin America where mosquitoes that transmit the virus live are exposed to and may have higher propensity for becoming infected.
The proximity of mosquito vector breeding sites to human habitation is a significant risk factor for be-ing infected with the chikungunya virus as well as for other diseases that these species transmit.
In addition, several other factors are likely to exac-erbate the situation. The rainy season starts in June and ends in November in the tropics. Heavy rains, humidity and heat are particularly favorable con-ditions for proliferation of the main vector (Aedes aegypti mosquito) which is the primary carrier of the chikungunya virus, whose eggs hatch on the surface of ponds.
Signs and SymptomsAfter the bite of an infected mosquito, onset of the illness occurs usually between 4 and 8 days, but it can range from 2 to 12 days.
The chikungunya disease shares some clinical signs with dengue fever, and can be misdiagnosed in ar-eas where that disease is common. This disease is typically characterized by an abrupt onset of fever frequently accompanied by joint pain. Muscle pain, headache, nausea, fatigue and rash are typically also present.
The joint pain is often quite debilitating, but usually lasts for a few days or may be prolonged to weeks. Most patients recover fully, but in some cases joint pain may persist for several months, or even years – i.e., arthritic pain. Hence, the virus can cause acute, sub-acute or chronic disease.
Occasional cases of eye, neurological and heart complications have been reported, as well as gas-trointestinal complaints. Serious complications are not common, but in older people the disease can contribute to the cause of death. Often symptoms in infected individuals are mild and the infection may go unrecognized, or be misdiagnosed in areas where dengue occurs.
Diagnosis: Exams and TestsMedical professionals can use various methods to determine with certainty whether the virus is in fact chikungunya. The most commonly used methods are serological and virological, which complement each other to confirm presence of infection.
Samples collected during the first week after the onset of symptoms should be tested by both serological and
virological methods to confirm findings.
Serological Tests Enzyme-linked immunosorbent assays (ELISA) which may confirm the presence of IgM and IgG anti-chikungunya antibodies are commonly used. Typically, high levels of IgM antibody are present and are usually the highest 3 to 5 weeks after the onset of illness and persist for about 2 months.
Virological TestsReverse transcriptase–polymerase chain reaction (RT–PCR) methods help isolate the virus from the blood during the first few days of infection. However, these are of variable sensitivity. Some are suited to clinical diagnosis. RT–PCR products from clinical samples may also be used for genotyping of the virus, allowing comparisons with virus samples from vari-ous geographical sources.
TreatmentThere is no vaccine nor specific antiviral drug treat-ment for chikungunya. For this reason, treatment is directed primarily at relieving the symptoms, which, if they go untreated, can result in further complica-tions, exposing patients to high risk of health dete-rioration that can lead even to death, particularly in children and the elderly. Therefore, it is critical to closely monitor and effectively control high fever through the use of analgesics and fluids, as well as anti-pyretics – aspirin, paracetamol, ibuprofen – which also help relieve the joint pain.1
Prevention and ControlHeavy reliance is placed on reducing the number of natural and artificial water-filled container habitats that support breeding of the mosquitoes. During outbreaks, insecticides may be sprayed to kill fly-ing mosquitoes, applied to surfaces in and around containers where the mosquitoes land, and used to treat water in containers to kill the immature larvae.
For protection during outbreaks of chikungunya, following are some recommendations:
• Wearing clothing (i.e., long sleeve shirts and pants) which minimizes skin exposure to the day-biting vectors is advised.
• Repellents can be applied to exposed skin or to clothing in strict accordance with product label instructions.
• For those who sleep during the daytime, par-ticularly young children, sick or older people, insecticide-treated mosquito nets afford good protection.
• Mosquito coils or other insecticide vaporizers may also reduce indoor biting.
• Eliminate mosquitoes found indoors, and use air-conditioning if available.
ON THE RISK vol.31 n.4 (2015)76
Basic precautions should be taken by people traveling to risk areas as the ones stated above.2
Current SituationChikungunya is widely distributed in tropical and subtropical areas of the world. In December 2013, France reported two laboratory-confirmed autoch-thonous cases of the virus in the French part of the Caribbean island of St. Martin. Since then, local trans-mission has been confirmed in over 43 countries and territories in the Americas region, including Canada and the United States. This was the first documented outbreak of chikungunya with autochthonous trans-mission in this part of the world.
This disease did not previously exist in the region; for this reason, 100% of the Latin American and Antillean population is susceptible to it. This being the case, there is no record of antibodies to chikungunya and no natural resistance to the disease. Consequently, risk of infection via mosquito is extremely high.3,4
As of January 2015, over 1,135,000 suspected cases of chikungunya have been recorded in the Latin American countries, the Antilles and North America; 176 deaths have also been attributed to this disease.
In South America, although the virus is still confined to localized outbreaks, numbers continue to grow. As of February 2015, countries such as Bolivia, Brazil, Colombia, Ecuador, Paraguay and Venezuela have reported cases.5
In Colombia, only 15 cases were initially attested in September 2014, but the figure exceeded 600 within 3 days. In January of 2015, the National Institute of Health (INS) confirmed 70,300 cases across the coun-try, although the suspected figure is now estimated to be around 150,000 nationwide. By December 2014, seven deaths had been reported, but three of the cases have since been attributed to other causes. The remaining four are being studied by the INS.
In Central America, El Salvador had over 75,000 re-ported cases by October of 2014. According to the lat-est figures, there are over 160,000 cases of the virus.
In neighboring Honduras, the number of cases rose from 100 to 5,000 in the last quarter of 2014. In Feb-ruary 2015, the figure rose to 9,000, claiming its first fatality in the country. And in Nicaragua as of March 2015, 4110 cases have been reported since July of the previous year.6,7
Underwriting ConcernsThe concerning situation is that since this condition is rapidly spreading, as it has occurred in recent months
in some countries, unless proper mitigating controls are effectively implemented, potentially entire com-munities can become infected. This means that the risk not only of morbidity but also of mortality is present and it represents a serious health threat.
Since the chikungunya outbreak is recent in the Americas region, perhaps few underwriters are aware of the situation on this side of the world, as we (medical and insurance professionals) are learning about the acute, sub-acute and chronic impact of this emerging tropical disease on the health of individuals. Therefore, underwriters working with foreign risks in Latin American countries should apply their best judgement when reviewing cases of insureds either living in or traveling to that part of the continent, as it appears that the chikungunya virus infection is dramatically increasing in Latin America.
Health institutions such as local - public and private - hospitals and clinics are becoming overburdened with infected patients daily as the volume of cases they are currently receiving is on the rise. Although the impact may not be quite palpable yet from an insurance and/or reinsurance perspective, the increasing number of infected patients is indeed a concern as some of them can turn out to be insurance claims of various types, such as emergency room visits, hospitalizations, disability (lost workdays) and even death in more severe cases. The larger the volume of infected cases, the larger the number of potential claims insurance carriers could receive, particularly those writing ac-cident and sickness (i.e., travel) medical business, as well as life policies (either individual or group) with short-term disability riders.
ConclusionThis new disease on the block, although it shares symptomatic similarities with dengue, is in fact a different condition with different challenges in many locations throughout Latin America. Therefore, it is worth it to take a closer look at those countries that have already experienced this viral disease and learn from them to try to mitigate as much as possible the effects of the condition.
Government health institutions, the International Red Cross and other medical institutions are aggres-sively engaged in taking care of infected patients.8 However, only a handful of institutions – i.e., WHO, PHO – may be engaged in prevention efforts. As the saying goes, “An ounce of prevention is worth far more than a pound of cure.” Perhaps it may be impor-tant for some insurers – local and foreign alike – to consider the idea of partnering with health agencies in order to engage in publicity campaigns to raise awareness of this viral condition among their clients
ON THE RISK vol.31 n.4 (2015) 77
and smart ways to prevent it.
Latin America is in a path of growth both demo-graphically and financially and opportunities abound. Nevertheless, insurance carriers working in Latin America can certainly promote and encourage pre-vention of chikungunya, as well as other viral diseases in hopes to have healthier communities, as they make the best clients! References1 World Health Organization, “Chikungunya," Retrieved 3/17/15, www.
who.int/mediacentre/factsheets/fs327/en/.
2 U.S. Environmental Protection Agency. Insect Repellents: Use and Effectiveness. Retrieved 3/21/2015, http://cfpub.epa.gov/oppref/insect/.
3 The World Bank. Latin America Has No Antibodies to Fight Chikun-gunya Fever. Retrieved 3/21/2015, www.worldbank.org/en/news/feature/2014/08/14/chikungunya-en-america-latina.
4 World Health Organization, “Chikungunya,” Retrieved 3/17/15, www.who.int/mediacentre/factsheets/fs327/en/.
5 Centers for Disease Control and Prevention. Traveler’s Health, Re-trieved 3/17/15, www.nc.cdc.gov/travel/destinations/list.
6 Panampost, “Chikungunya Continues March across Latin America,” Re-trieved 3/17/15, http://panampost.com/rebeca-morla/2015/03/02/chikungunya-continues-march-across-latin-america/.
7 OPS llama a unir esfuerzos contra el chikungunya en Nicara-gua. Retrieved 4/25/15. www.laprensa.com.ni/2015/03/16/nacionales/1799806-ops-llama-a-unir-esfuerzos-contra-el-chikungun-ya-en-nicaragua.
8 International Federation of Red Cross and Red Crescent Society. Nicaraguan Red Cross unites in a fight against Chikungunya – Retrieved 4/19/15. www.ifrc.org/en/news-and-media/news-stories/americas/nicaragua/nicaraguan-red-cross-unites-in-a-fight-against-chikungunya-/#sthash.gqg30QYd.dpuf.
FALU Quiz Crossword Answers
If you want to see True
Excellence again...
contact us. T
ILF
OR
D C
ON
SU
LTIN
G
ww
w.ti
lford
cons
ultin
g.co
m
ON THE RISK vol.31 n.4 (2015)78
.
From time to time, ON THE RISK makes its subscriber list available to advertisers. If any subscriber prefers to have his or her name removed from such lists, please submit your written request in writing via letter, fax or e-mail to OTR Publishing Services, 6 Hartley Road, Binghamton, NY 13901; fax: (607) 724-0041; e-mail: [email protected].
ADVERTISE IN For information contact:
Deb Wesenberg, Advertising ManagerPhone (309) 278-2520
E-mail: [email protected]
Add Web advertising to your marketing strategy.Visit the OTR web pages for online advertising rates and information.
www.ontherisk.com
OTR
INDEX TO ADVERTISERS
PLEASE TELL THESE ADVERTISERS HOW MUCH YOU APPRECIATE THEIR SUPPORT OF ON THE RISK!
APPS....................................................................................................................................................80Clinical Reference Laboratory.........................................................................................................40EMSI....................................................................................................................................................13ExamOne..........................................................................................................................................41First Financial Underwriting Services.............................................................................................35Hannover Re ....................................................................................................................................7HOVIN Underwriting Partners, Inc................................................................................................79IBU*.....................................................................................................................................................17Innovative Underwriting Solutions....................................................................................................25IUSolutions..........................................................................................................................................29Lexis Nexis..........................................................................................................................................9MIB, Inc............................................................................................................................................15Parameds.com............................................................................................................................... 2,3RGA .................................................................................................................................................27RGA AURA............................................................................................................................................11Tilford Consulting............................................................................................................................77
CHECK OUT THEIR ADS AND CALL THEM TODAY!
* These companies are also ON THE RISK website advertisers. Visit www.ontherisk.com (OTR Online) and link directly to their sites.
fit your business
QUICK QUOTES – INFORMALS/FORMALS – APS SUMMARIES - AUDITS
Jerry Holmes and Jan Vincent, Principals [email protected] and [email protected]
Visit our website for full service information www.hovinpartners.com. Email [email protected] or Toll free 866-454-6846
Begin with Quality Service. End with a Satisfied Customer.
Strategic Partner of MIB
Professional Life Underwriting Solutions
One Jericho Plaza, Jericho, NY 11753516.822.6230
appslive.com
It’s like comparing . . .
well, you know.
How does the largest paramedical company in America,
with the most coverage,
industry leading technology,
and unparalleled customer
support stack up?























![FALU VÁROS RÉGIÓ 2006_3[1]](https://img.pdfslide.net/doc/110x75/5571f8e449795991698e51d0/falu-varos-regio-200631.jpg)




