Embed Size (px)
Citation preview
SECTION BExperiential Learning Programs
Experiential Learning• Simulation Workshop
Program
• Facilitated Discussion Program
• Independent Learner Program
SECTION BExperiential Learning Programs
Experiential Learning• Simulation Workshop
Program
• Facilitated Discussion Program
• Independent Learner Program
Simulation Workshop Program
Facilitator Guide

Table of Contents
Facilitator Welcome . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
About Simulation Techniques . . . . . . . . . . . . . . . . . . . . . . . . .1
Simulation Workshop Overview . . . . . . . . . . . . . . . . . . . 3
Purpose . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3
Description . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3
Simulation Workshop Planning . . . . . . . . . . . . . . . . . . . . . . . .4
Equipment, Resources & Planning . . . . . . . . . . . . . . . . . . 8
Equipment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8
SP Scenario Resources & Equipment . . . . . . . . . . . . . . . . . . . . .8
Facilitator Resources . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9
Facilitator Instructions . . . . . . . . . . . . . . . . . . . . . . . . .10
Sample Workshop Agenda . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Workshop Overview . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
1© 2010, Mount Sinai Hospital, Toronto, Canada
Facilitator Welcome
Welcome to the Facilitator Guide for the Simulation Workshop Program. This guide has been prepared to assist you in the delivery of this workshop. It outlines the purpose of the workshop, and provides a description and the learning objectives for participants. The guide outlines detailed steps on how to organize the workshop.
This guide should be used in partnership with the Introduction Guide . All of the facilitator resources and participant handouts can be found in the Resources section of the manual.
About Simulation TechniquesSimulation is a technique that replaces or amplifies real patient experiences with guided, artificially contrived experiences that evoke or replicate substantial aspects of the real world in a fully interactive manner(16)*. Simulation training is an established teaching technique in medicine, surgery, nursing and allied health(17).
Standardized patient (SP) simulations have proven successful in teaching general communication skills, behaviour management, symptom assessment, and technical and procedural skills to healthcare professionals(18-22).
Evidence suggests that simulations facilitate learning because they:
f foster opportunities to provide immediate performance feedback;
f offer repetitive practice;
f provide a range of difficulty;
f offer opportunities for integrating multiple learning strategies;
f capture clinical variation;
f provide individualized learning; and,
f allow for the measurement of specific performance outcomes(23).
* ReferencesarefoundattheendoftheResourcesSection.
Introduction Guide
Simulation Workshop Program
iCAMIRA Facilitator’s Resource Manual
2 © 2010, Mount Sinai Hospital, Toronto, Canada
As part of the iCAMIRA education intervention, the University of Toronto’s Standardized Patient Program facilitated the development of generic medical/surgical patient scenarios for the Simulation Workshop. The scenarios were informed by clinical experts and members from Mount Sinai Hospital’s Patient Advisors Group.
Standardized Patients (SPs) were used to play the patient roles in the scenarios. SPs are professional actors who work with the University of Toronto Standardized Patient Program to play a variety of roles that facilitate experiential learning of healthcare professionals.
There are fees associated with the development of scenarios, training SPs for the role and SP time during the actual workshop. If you plan to use SPs from the University of Toronto program, connect with them 3-4 months in advance of your start date to discuss your program needs. Their contact information can be found at: http://www.spp.utoronto.ca.
IMPORTANT !
If you do not have access to standardized patients, the
workshop can be developed using role-playing
techniques with staff.
3© 2010, Mount Sinai Hospital, Toronto, Canada
Simulation Workshop Overview
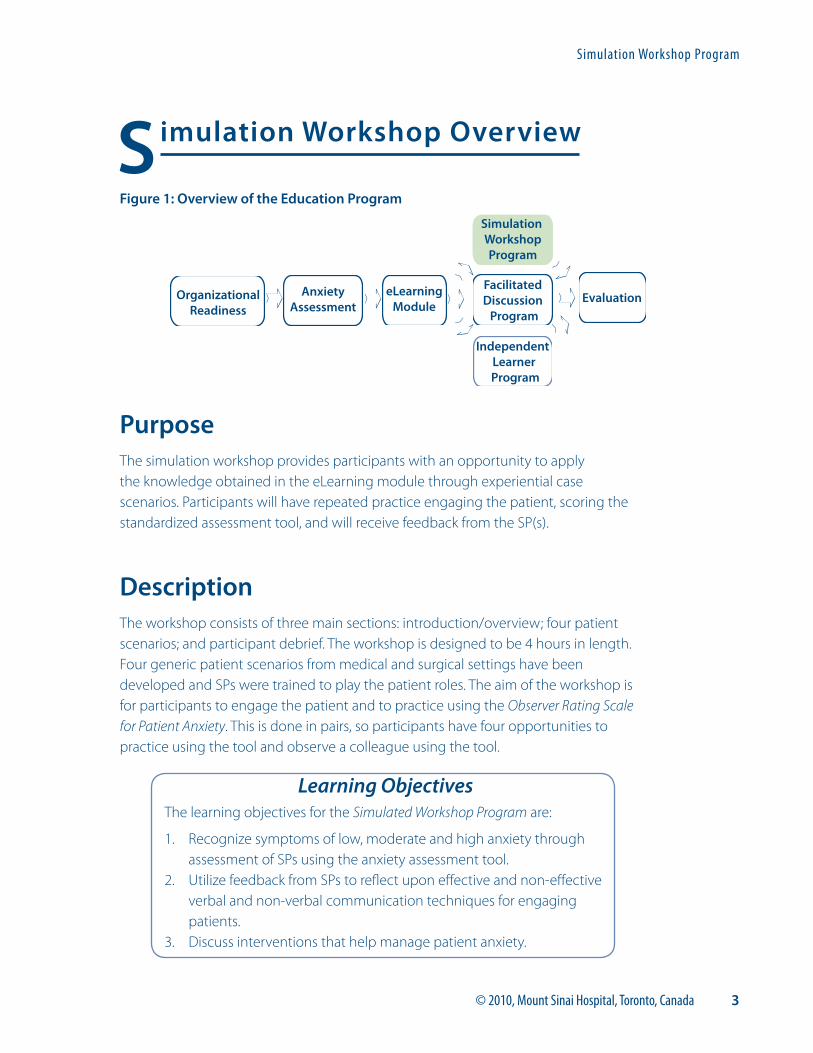
Figure 1: Overview of the Education Program
PurposeThe simulation workshop provides participants with an opportunity to apply the knowledge obtained in the eLearning module through experiential case scenarios. Participants will have repeated practice engaging the patient, scoring the standardized assessment tool, and will receive feedback from the SP(s).
DescriptionThe workshop consists of three main sections: introduction/overview; four patient scenarios; and participant debrief. The workshop is designed to be 4 hours in length. Four generic patient scenarios from medical and surgical settings have been developed and SPs were trained to play the patient roles. The aim of the workshop is for participants to engage the patient and to practice using the Observer Rating Scale for Patient Anxiety. This is done in pairs, so participants have four opportunities to practice using the tool and observe a colleague using the tool.
Simulation WorkshopProgram
FacilitatedDiscussion Program
EvaluationAnxietyAssessment
Independent Learner
Program
OrganizationalReadiness
eLearningModule
Learning ObjectivesThe learning objectives for the Simulated Workshop Program are:
1. Recognize symptoms of low, moderate and high anxiety through assessment of SPs using the anxiety assessment tool.
2. Utilize feedback from SPs to reflect upon effective and non-effective verbal and non-verbal communication techniques for engaging patients.
3. Discuss interventions that help manage patient anxiety.
Simulation Workshop Program
iCAMIRA Facilitator’s Resource Manual
4 © 2010, Mount Sinai Hospital, Toronto, Canada
Simulation Workshop PlanningThe iCAMIRA educational intervention was an organizational initiative targeted to approximately 400 participants. The workshops required a minimum of 8 participants with a maximum of 20. The same four scenarios ran on two separate tracks, with a total of 8 SPs per workshop. The following sections in this guide, which details the simulation workshop, are based on the planning and implementation experience of the iCAMIRA project. The workshop does not require the use of SPs and can be implemented using role-playing techniques. The timelines, materials and resources will vary depending on the magnitude of your planned program.
8 Weeks prior to the workshop
� Determine the date, time and location for the workshop
� Book rooms based on your maximum registration number
� Book SPs
� Prepare promotional materials and registration process
� Promote the workshop
� Provide eLearning module instructions to registered participants
4 Weeks prior to the workshop
� If you develop your own scenarios and use SPs, meet with the SP coordinator to draft scenarios
� Send promotional reminders about the workshop
� Send reminders about the eLearning module to registered participants
� Gather/book equipment that is required for scenarios
� Order linens: each SP requires 2 gowns, a top and bottom sheet, and a pillow case
2 Weeks prior to the workshop
� Print facilitator workshop resources, including:
– Checklist for Simulation Workshop
– Case Scenarios with Scoring Legend
– Simulation Workshop Facilitator Tool
1 - Case Scenarios with Scoring Legend
8 - Simulation Workshop Facilitator Tool
1 - Checklist for Simulation Workshop
5© 2010, Mount Sinai Hospital, Toronto, Canada
� Print Scenario Stems or laminate them if you are providing more than one workshop
� Print participant materials:
– iCAMIRA Participant Evaluation Form
– Observer Rating Scale for Patient Anxiety ( 4 copies per participant )
� Confirm eLearning module completion by participants and send a reminder email to those who have not yet completed the module
� Order catering for the workshop (optional); consider dietary needs of participants and SPs
3 Days to 1 week prior to the workshop
� Send an email reminder to participants, providing workshop instructions and directions to the workshop location
� If registration does not meet minimum numbers, cancel room bookings, catering, SPs and send a cancellation email to registered participants and managers
1 Day prior to the workshop
� Confirm the catering order (retain info for catering order, contact for inquiries)
� Confirm the equipment and room bookings (retain info for contact in case of problems)
� Print signs for directions to the workshop location
� Review the facilitator guide, and facilitator and participant materials
� Print the registration roster
Facilitator TipsIn your communications with participants, be sure to include a note about the workshop being “scent free”. Participants are mindful of this in the workplace and not necessarily for workshops. Remind them that the SPs are essentially patients, some of whom may have perfume allergies.
2 - iCAMIRA Participant Evaluation Form
5 - Observer Rating Scale for Patient Anxiety
7 - Scenario Stems for Simulation Workshop
Simulation Workshop Program
iCAMIRA Facilitator’s Resource Manual
6 © 2010, Mount Sinai Hospital, Toronto, Canada
Day of the workshop
Before the workshop (arrive at least an hour early)
� Post signs for directions to the workshop
� Set up chairs in the main room in a manner that will facilitate discussion
� Set up the equipment and linens in the SP exam rooms
� Tape each scenario stem to the appropriate room door
� Set up the registration/sign in area
� Receive catering
End of the workshop
� Hand out the participant certificates (if required)
� Remind the participants to gather all of their belongings
� Clean up any remaining materials
� Strip linens in the scenario rooms and gather/put away equipment
� Check all rooms for participant belongings
� Take down the signs for directions to the workshop
Facilitator TipsA Checklist for Simulation Workshop is provided for you. It is a helpful tool to use to ensure that you have made all the necessary arrangements and have all of your resources and handouts for the workshop.
Facilitator TipsIf you are using SPs, ensure that the scenario rooms are prepared with linens, gowns and any medical equipment necessary to make the scenario realistic.
Be prepared for participants who show up without having completed their eLearning module. The iCAMIRA project made no exceptions for participants who did not complete the eLearning module, as its completion is critical to participants being fully able to take part in the workshop.
Decide on a cut-off time for late arrivals. Consider turning away participants who arrive after the start of the first scenario rotation. It is challenging to integrate them and may be disruptive to the other participants and SPs.
7© 2010, Mount Sinai Hospital, Toronto, Canada
Post workshop
� Email the group of participants to notify them if any belongings were left behind
� Update your participant tracking system, confirming the names of participants who attended the workshop and those who did not
� Provide an electronic copy of the confirmed participants to the managers (if required)
� Send out ‘thank yous’ as required
� Write the workshop summary report (if required); summarize how the workshop went and note any tips or suggestions for running future workshops (this is an opportunity to refine the process of planning, implementing and evaluating the workshop)
Simulation Workshop Program
iCAMIRA Facilitator’s Resource Manual
8 © 2010, Mount Sinai Hospital, Toronto, Canada
Equipment, Resources & Planning
Equipment � Presentation room large enough
to accommodate all participants for the group discussion
� Chairs (1 per participant, facilitator and SP)
� Box of pens
� Name tags
� Masking tape
� Catering (optional)
SP Scenario Resources & Equipment The following resources and equipment are recommended if you are using the scenarios included in this guide:
� 4-8 Exam/hospital ward type rooms with bed and chair for scenarios
� 4 IV poles
� 4 saline solutions
� 2 newspapers
� 2 rolls of kling
� Paper surgical tape
� 2 NG tubes
� 2 stopwatches
� 2 sets of scenario stems
Facilitator TipsIf you are using SPs, provide a separate room for them to meet and debrief. They prefer not to mingle with the participants until after the scenario rotations are completed.
If you are using SPs, they require beverages, and if it is an early morning workshop, a continental breakfast is appreciated.
9© 2010, Mount Sinai Hospital, Toronto, Canada
Facilitator Resources A copy of the following resources can be found in the Resources section of this manual.
� Planning Resources
– Checklist for Simulation Workshop
– iCAMIRA Poster
– iCAMIRA Registration (sample email/poster)
– Incomplete eLearning Module (sample email)
– Preparing for Simulation Workshop (sample email)
� Implementation Resources
– Case Scenarios with Scoring Legend
– iCAMIRA Participant Evaluation Form
– Observer Rating Scale for Patient Anxiety (4 per participant)
– Simulation Workshop Facilitator Tool
– Scenario Stems for Simulation Workshop
1 - Checklist for Simulation Workshop
2 - iCAMIRA Poster3 - iCAMIRA Registration4 - Incomplete eLearning
Module5 - Preparing for
Simulation Workshop
1 - Case Scenarios with Scoring Legend
2 - iCAMIRA Participant Evaluation Form
5 - Observer Rating Scale for Patient Anxiety
7 - Scenario Stems for Simulation Workshop
8 - Simulation Workshop Facilitator Tool
Simulation Workshop Program
iCAMIRA Facilitator’s Resource Manual
10 © 2010, Mount Sinai Hospital, Toronto, Canada
Facilitator Instructions
Sample Workshop Agenda
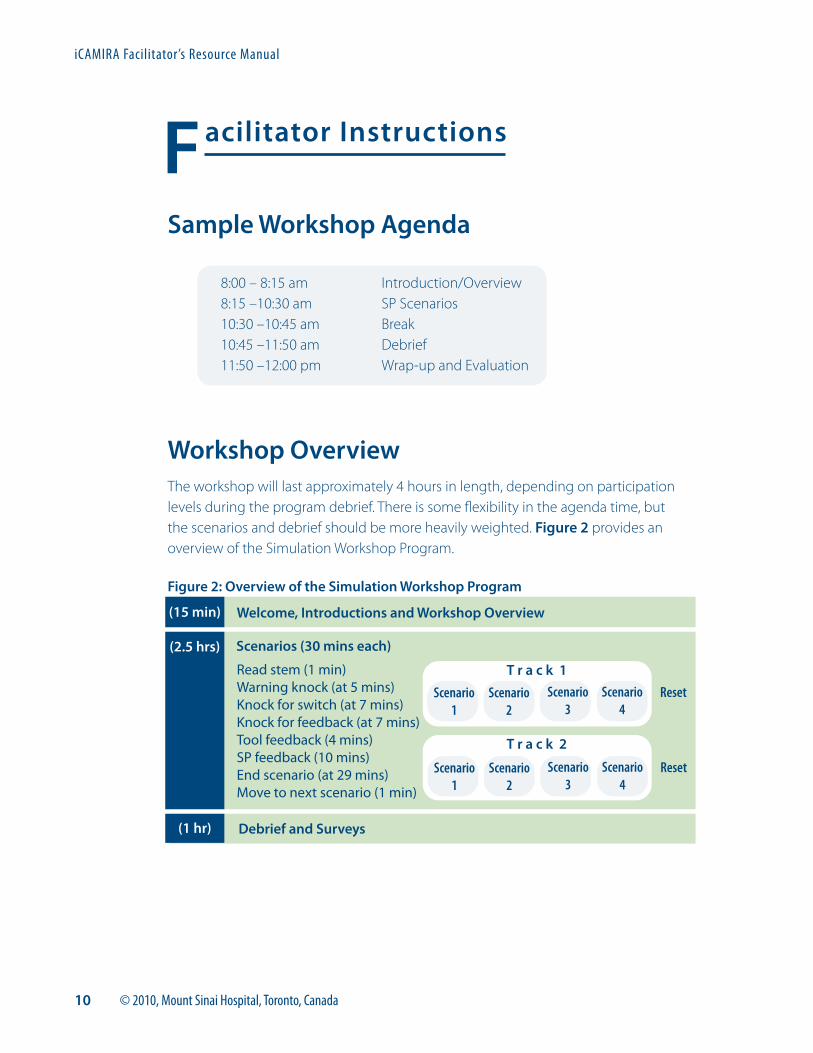
8:00 – 8:15 am8:15 –10:30 am10:30 –10:45 am10:45 –11:50 am 11:50 –12:00 pm
Introduction/OverviewSP ScenariosBreakDebrief Wrap-up and Evaluation
Workshop OverviewThe workshop will last approximately 4 hours in length, depending on participation levels during the program debrief. There is some flexibility in the agenda time, but the scenarios and debrief should be more heavily weighted. Figure 2 provides an overview of the Simulation Workshop Program.
Figure 2: Overview of the Simulation Workshop Program
Welcome, Introductions and Workshop Overview
Scenarios (30 mins each)
Debrief and Surveys
(15 min)
(2.5 hrs)
(1 hr)
Read stem (1 min)Warning knock (at 5 mins)Knock for switch (at 7 mins)Knock for feedback (at 7 mins)Tool feedback (4 mins)SP feedback (10 mins)End scenario (at 29 mins)Move to next scenario (1 min)
T r a c k 1
Scenario1
Scenario2
Scenario3
Scenario4
Reset
T r a c k 2
Scenario1
Scenario2
Scenario3
Scenario4
Reset
11© 2010, Mount Sinai Hospital, Toronto, Canada
Introduction/Overview (15 minutes)
� Use the Simulation Workshop Facilitator Tool.
� Participants who have little or no experience with role-playing may be anxious about the process. Check-in with the group and help to normalize their experience. Emphasize that the workshop is not evaluative and that participants should have fun and enjoy the process.
� It helps to keep the introduction/orientation brief. Because of the participants’ anxiety, they often don’t take in a lot of the explanation regarding the scenario rotations. The facilitator usually needs to go over the scenario rotations again once participants are at the scenario room doors.
� Ensure that each participant has four anxiety assessment tools and a pen/pencil for scoring the SPs anxiety in each scenario. It’s helpful if participants write the name of the SP on each assessment tool, as it reminds them ‘who is who’ during the debrief. They can also use the back of these sheets to jot notes during the discussion.
� Point out the location(s) of the washrooms.
� Ask participant to bring their valuables with them when leaving the main room.
� Let participants know that they will have a 15 minute break between the scenarios and debrief.
Scenarios (120-140 minutes)
Participants rotate through the four scenario stations where they interact with the SP, practice their anxiety assessment skills using the tool, and receive feedback from the SPs. The feedback is around how the SP felt about the experience “in the moment” regarding the healthcare professional’s engagement and communication process. The time allocation for the scenario rotations is broken down in the following steps:
f Each station lasts 30 minutes in total. The estimated 30 minutes for each scenario is based on a group of up to 16 participants. If there are 17 to 20 participants, build in a rest station and shorten each scenario to 25 minutes. Additional time may also need to be built in for travel between stations if the rooms are not close to each other.
f Participants have 1 minute to read the stem on the door, and are then asked by the facilitator to enter the room.
f The facilitator will knock on the door at 5 minute mark of the interview (‘warning’ knock). The facilitator will then knock on the door at the 7 minute mark to have participants switch roles.
Simulation Workshop Program
8 - Simulation Workshop Facilitator Tool
iCAMIRA Facilitator’s Resource Manual
12 © 2010, Mount Sinai Hospital, Toronto, Canada
f Restarting the timer, the facilitator will knock at the 5 minute mark. At 7 minute mark, he/she will knock again, open the door and say “feedback”. Participants will have 4 minutes to discuss the scoring and items of the tool with each other, and then move into feedback from the SPs for 10 minutes.
f At the 29 minute mark, the facilitator will open the door again and give participants 1 minute to wrap up. At 30 minutes, the facilitator opens the door and encourages participants to move on.
Break (15 minutes)
Debrief (60-65 minutes)
Scoring the Scenarios (15 minutes)
Begin the debrief with the scoring of the four scenarios using the Observer Rating Scale for Patient Anxiety. This provides an opportunity to:
� address any discrepancies in the use of and scoring of the tool;
� provide messages about the advantages of using an anxiety assessment tool; and
� allow for the discussion of any challenges of implementing the tool in the clinical context.
Facilitator TipsIf you are running two tracks of scenarios, each track requires a facilitator. Each facilitator requires a stopwatch in order to keep the rotations on time.
Facilitator TipsThe anxiety assessment scoring tools are based on the scenarios that were created for the iCAMIRA project. If you choose to use the scenarios included with this guide, the scoring of the tool may vary depending on your interpretation and implementation of each scenario.
It may be helpful to view the scenarios on the DVD and their associated anxiety tool scoring (this can be found in the Facilitated Discussion Program: Facilitator Guide. The DVD clips were based on the same scenarios as those for
the Simulation Workshop Program. Notice that the anxiety tool scoring is slightly different for the scenarios in the DVD as compared to the Simulation Workshop Program. This is a result of slightly different interpretations for the same scenario.
Facilitated Discussion Program
13© 2010, Mount Sinai Hospital, Toronto, Canada
Participant Debrief & Discussion ( 45-50 minutes)
Ask participants to discuss their experiences with each of the scenarios. If using SPs, ask a SP from each scenario to participate in the discussion and provide feedback about his/her experience.
Sample discussion points for each scenario are provided at the end of the four scenarios.
Sample discussion questions:
f What went well?
f What were some of the challenges?
f What feedback did participants receive from the SP that might be helpful in their practice?
f What strategies did participants use to engage the SP? (e.g., information seeking, open or closed ended questions, touch, humour, use of personal space, or non-verbal communication)
f What strategies were effective in decreasing the patient’s anxiety?
f What strategies were ineffective in decreasing the patient’s anxiety?
f How did participants handle not being able to provide the SP with all the information he/she wanted? What was the SPs experience of this?
Simulation Workshop Program
iCAMIRA Facilitator’s Resource Manual
14 © 2010, Mount Sinai Hospital, Toronto, Canada
Scenario 1: Rose Hatfield
Rose has a low level of anxiety. She has fears about the potential results of the MRI and is not displaying a great deal of anxiety. Her concentration is good and there is not a lot of overt tension, except for some tearfulness when talking about her mother. The difficulty sleeping appears to be because of the tubes. However, it would be important to ask Rose if there is anything else keeping her awake, and whether her sleep has only been disturbed since coming into the hospital. Obtaining this information will help to clarify whether the sleep problems are related to fears and worries, or just a result of the hospital environment.
Rose responds well to open-ended questions. She is the “nice-pleasant” patient who won’t necessarily volunteer a lot of information, but if you take the time to engage her and keep asking open-ended questions, she will divulge more information about herself. On the surface, her main concern is the MRI result. By picking up on cues from Rose, the healthcare professional (HCP) can
probe with more open-ended questions and get to the real source of Rose’s worry. Some HCPs are concerned about probing too much, or asking too many questions. Take your cues from the patient. He/she will let you know if the questions are too intrusive or if he/she doesn’t want to talk.
Like Rose, many of our patients want answers to questions about their diagnosis, treatment, results, etc. There are many times when we don’t have the information or can’t convey the information because of the scope of our role. It’s perfectly okay to say that you don’t have the results. As a HCP, you’re not expected to have all the answers. Though you may not have the answer the patient is looking for, there is a lot of information you do have about how long things take, the process for procedures and results, etc. We sometimes take these things for granted because we live and breathe them every day. Remember however, that for the patient, hospital procedures and routines are unfamiliar, and this often gives rise to fears, anxieties and worries.
15© 2010, Mount Sinai Hospital, Toronto, Canada
Scenario 2: Phil Archer
Phil is a gentleman who doesn’t open up easily. He’s not a big conversationalist! Because of this, there may be a tendency for HCPs to “write Phil off” and forget about him, thinking that he doesn’t want to engage. In fact, he does have a moderate level of anxiety and fears about losing his foot.
Moving from open-ended questions to more close-ended or directive questions allows Phil to engage. For patient’s like Phil, there are two important points to remember:
1. They need more time to open up and engage which means that as a HCP you will need to return several times to engage with Phil in order to develop some rapport
2. Closed or directive type questions will be more effective
Patients like Phil have a lot bottled up and going on in their head. It’s often very hard for them to answer global, open-ended questions. They have difficulties focusing on any one problem or concern.
So as HCPs, we need to help focus, or direct their thinking. This becomes even more pertinent when the patient is anxious or worried. It may seem counter-intuitive because as HCPs we’re taught to ask open-ended questions. It’s generally a good rule of thumb to start with open-ended questions, and to also have other communication strategies in our toolbox when the open-ended approach doesn’t work.
It can also be helpful to Phil, if the HCP reflects back to Phil what he/she is observing (e.g., the lack of eye contact and fidgeting). When patients are anxious or worried, they are often not aware of their behaviour. Reflecting on a patient’s behaviour also acknowledges for the patient that you are paying attention.
So the next time you encounter a Phil-type patient, don’t “write them off” because of their apparent lack of engagement. There’s often a lot going on for these patients. It just takes a little more time and patience on our part to find it out.
Simulation Workshop Program
iCAMIRA Facilitator’s Resource Manual
16 © 2010, Mount Sinai Hospital, Toronto, Canada
Scenario 3: Amanda Cooper
With Amanda, it is important for staff to recognize the signs of high anxiety and to actually manage, rather than assess the anxiety. This includes using techniques like supportive listening and providing reassurance (e.g., that the team is not hiding anything and trying to figure out what is wrong with her). Conveying a non-verbal stance that you are going to stay and not run out the room is important to building trust with Amanda.
Amanda provides all the answers to the anxiety assessment without the HCP needing to ask a lot of questions. Her level of anxiety is clearly high, as are her fears of a brain tumor and dying. She tells the HCP that she isn’t sleeping. Though she isn’t crying, pacing or restless, there is a certain tension in her body posture. Assessing concentration with Amanda is a bit more difficult as it is easy to mistake her constant focus on the brain tumor
and dying as an inability to remember information given to her. Given a supportive and calm approach, Amanda is able to concentrate on the information and understand the difference between a stroke and a TIA.
The challenge for HCPs is to find a way to tolerate Amanda’s affect. If the HCP just keeps leaving the room, Amanda’s anxiety will not be addressed and in fact will continue to increase which leads to her constantly ringing the call bell.
It’s tempting to label patients like Amanda as histrionic or “over-the-top” and to view them as “difficult or needy”. HCPs need to recognize the patient’s distress and find ways to manage their own discomfort with the patient’s affect. Use your colleagues for support, have a care plan for consistency and be aware of your own triggers.
17© 2010, Mount Sinai Hospital, Toronto, Canada
Scenario 4: Derek Lewis
Try to put yourself in Derek’s position for a moment. Most 20 something’s are leading very active lives and don’t have too many worries. Derek is facing his mortality. He is a 22 year old male, so don’t expect that he’s going to come right out and say he’s scared…but he is. All of his questions around the surgery, the pain and what happens afterwards, are an invitation for the HCP to engage with Derek. Engaging with Derek around his questions will help to build rapport and trust. He is overwhelmed and alone in the city. He is desperately wanting to talk with someone, but remember, he is a 22 year old male! As HCPs, we need to recognize that he’s not going to be the one to initiate the conversation.
Derek’s reference to his condition being like Terry Fox’s is silently asking that question that he’s afraid to ask. “Does that mean I’m going to die too?” As the HCP, the reference to Terry Fox provides an opportunity to ask Derek directly if he is afraid of dying which then gives Derek the space to have the conversation if he so chooses. It also allows for a conversation about how medicine has advanced since Terry Fox’s time and to ask Derek is he would like more information from his doctor regarding prognosis. The combination of caring and
taking the time to discuss death as well as providing factual information will help to manage Derek’s anxiety.
The other key point for this scenario is around providing Derek with reassurance regarding the healthcare team. He is angry and feels his family doctor may have missed something. It’s important to not get caught up in that discussion. You weren’t there and so don’t really know what happened. Provide support to Derek and focus on the present by conveying confidence in your colleagues and reassuring him that he has a great team. Genuineness is very important when engaging with Derek. If you are in a position where you don’t have confidence in your colleagues, then don’t say so. You could simply say to Derek that you’ll pass his concerns about “something being missed” on to his doctor.
Derek is a young man facing a possible leg amputation and maybe even death. The reaction of HCPs to Derek’s situation is often one of sadness and feeling badly for the situation he is facing. Sometimes, there is also fear and discomfort on the part of the HCP regarding conversations around death and dying. In order to be an effective care provider, it’s important that HCPs manage their emotions and use their colleagues for support.
Simulation Workshop Program
iCAMIRA Facilitator’s Resource Manual
18 © 2010, Mount Sinai Hospital, Toronto, Canada
Summary of Key Discussion Points for Scenarios
� Engaging your patients and developing rapport helps them feel cared for and will help decrease their anxiety.
� Engaging your patients and developing rapport improves the patient care experience and gives you more job satisfaction.
� Recall from the scenarios that it really didn’t take a lot more time to engage and do a good job of assessing the patient’s anxiety. Remember that an extra minute can make a big difference in decreasing your patient’s anxiety and actually save you a lot of “responding to call-bell” time in the end.
� Be aware of “cues” from the patient and don’t be afraid to ask questions, rather than trying to guess what the cues mean. The cues may be verbal or non-verbal.
� Each patient is different. Use the different communication techniques you’ve learned to connect with your patient.
� The anxiety assessment tool provides you and your colleagues with a common language with which to communicate about patient anxiety. It’s a subjective tool, so not everyone will have exactly the same score. What’s important are the low, moderate and high categories. It’s these categories that determine the appropriate interventions.
Evaluation (5-10 minutes)
f Have participants complete the iCAMIRA Participant Evaluation Form.
2 - iCAMIRA Participant Evaluation Form
Facilitated Discussion Program
Facilitator Guide
Table of Contents
Facilitator Welcome . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Program Overview . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Purpose . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2
Description . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2
Learning Objectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3
Program Planning . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3
Equipment, Resources & Planning . . . . . . . . . . . . . . . . . . 6
Equipment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6
Facilitator Resources . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6
Facilitator Instructions . . . . . . . . . . . . . . . . . . . . . . . . . 7
Program Agenda . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7
Program Overview . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7
DVD Scenarios . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Scenario 1: Rose Hatfield . . . . . . . . . . . . . . . . . . . . . . 10
Rose Clip 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .10
Rose Clip 2. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .12
Scenario 2: Phil Archer . . . . . . . . . . . . . . . . . . . . . . . . 15
Phil Clip 1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .16
Phil Clip 2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .18
Scenario 3: Amanda Cooper . . . . . . . . . . . . . . . . . . . . 20
Amanda Clip 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .21
Amanda Clip 2. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .22
Scenario Summary Points . . . . . . . . . . . . . . . . . . . . . . 24
1© 2010, Mount Sinai Hospital, Toronto, Canada
Facilitator Welcome
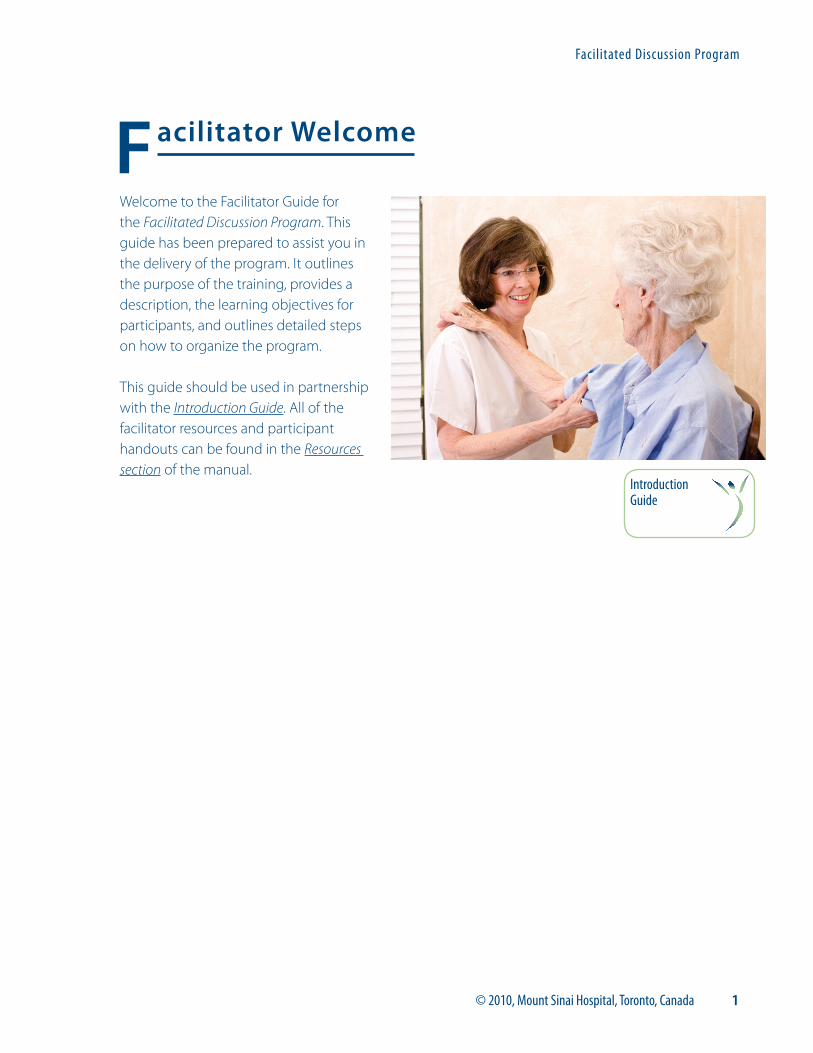
Welcome to the Facilitator Guide for the Facilitated Discussion Program. This guide has been prepared to assist you in the delivery of the program. It outlines the purpose of the training, provides a description, the learning objectives for participants, and outlines detailed steps on how to organize the program.
This guide should be used in partnership with the Introduction Guide. All of the facilitator resources and participant handouts can be found in the Resources section of the manual.
Facilitated Discussion Program
Introduction Guide
iCAMIRA Facilitator’s Resource Manual
2 © 2010, Mount Sinai Hospital, Toronto, Canada
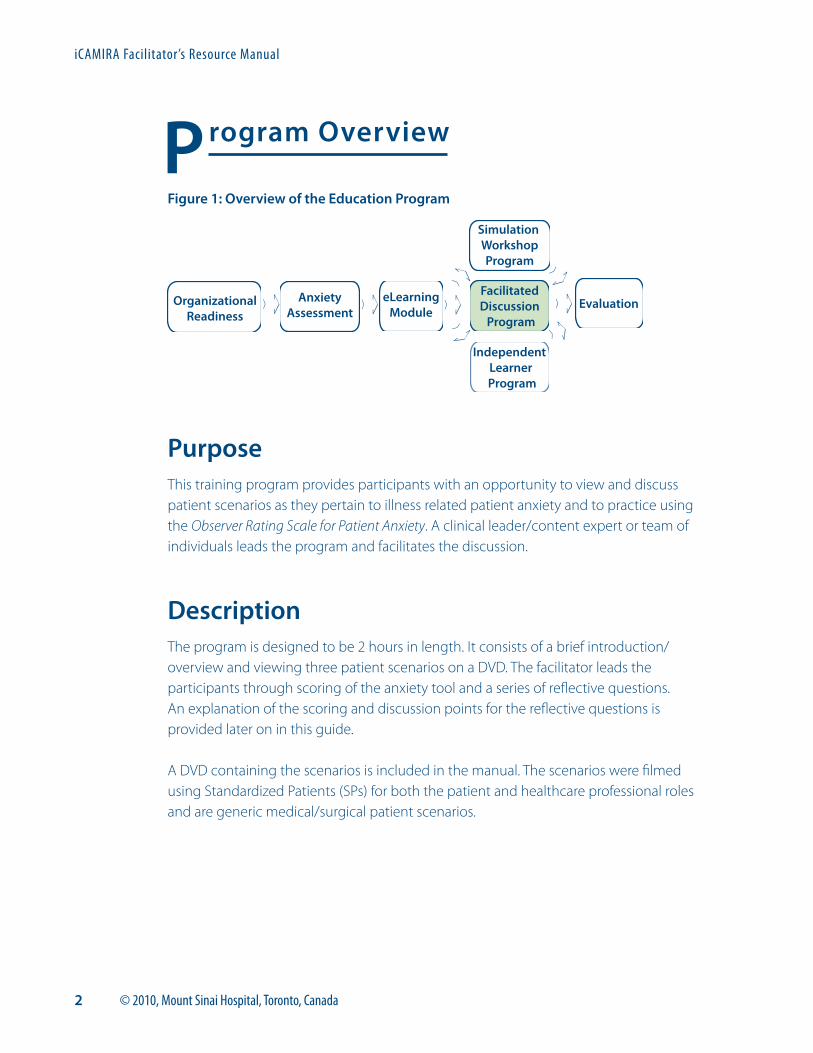
Program Overview
Figure 1: Overview of the Education Program
PurposeThis training program provides participants with an opportunity to view and discuss patient scenarios as they pertain to illness related patient anxiety and to practice using the Observer Rating Scale for Patient Anxiety. A clinical leader/content expert or team of individuals leads the program and facilitates the discussion.
DescriptionThe program is designed to be 2 hours in length. It consists of a brief introduction/overview and viewing three patient scenarios on a DVD. The facilitator leads the participants through scoring of the anxiety tool and a series of reflective questions. An explanation of the scoring and discussion points for the reflective questions is provided later on in this guide.
A DVD containing the scenarios is included in the manual. The scenarios were filmed using Standardized Patients (SPs) for both the patient and healthcare professional roles and are generic medical/surgical patient scenarios.
Simulation WorkshopProgram
FacilitatedDiscussion Program
EvaluationAnxietyAssessment
Independent Learner
Program
OrganizationalReadiness
eLearningModule
3© 2010, Mount Sinai Hospital, Toronto, Canada
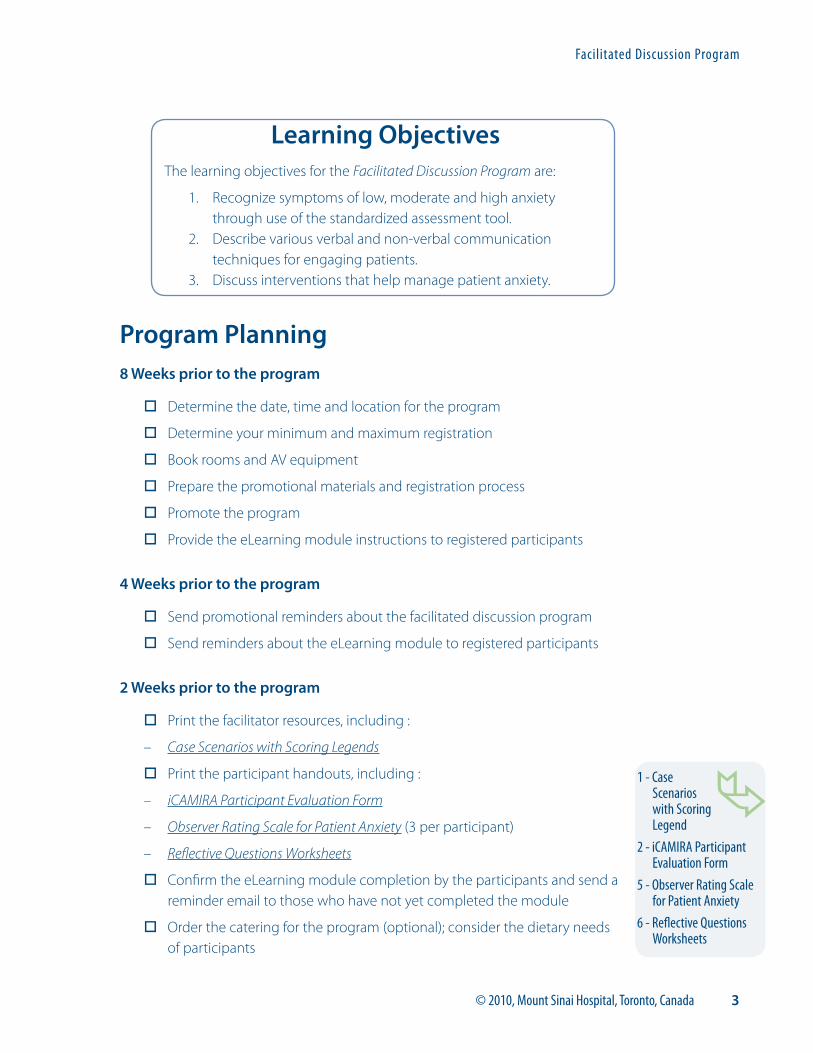
Program Planning8 Weeks prior to the program
� Determine the date, time and location for the program
� Determine your minimum and maximum registration
� Book rooms and AV equipment
� Prepare the promotional materials and registration process
� Promote the program
� Provide the eLearning module instructions to registered participants
4 Weeks prior to the program
� Send promotional reminders about the facilitated discussion program
� Send reminders about the eLearning module to registered participants
2 Weeks prior to the program
� Print the facilitator resources, including :
– Case Scenarios with Scoring Legends
� Print the participant handouts, including :
– iCAMIRA Participant Evaluation Form
– Observer Rating Scale for Patient Anxiety (3 per participant)
– Reflective Questions Worksheets
� Confirm the eLearning module completion by the participants and send a reminder email to those who have not yet completed the module
� Order the catering for the program (optional); consider the dietary needs of participants
Learning ObjectivesThe learning objectives for the Facilitated Discussion Program are:
1. Recognize symptoms of low, moderate and high anxiety through use of the standardized assessment tool.
2. Describe various verbal and non-verbal communication techniques for engaging patients.
3. Discuss interventions that help manage patient anxiety.
Facilitated Discussion Program
1 - Case Scenarios with Scoring Legend
2 - iCAMIRA Participant Evaluation Form
5 - Observer Rating Scale for Patient Anxiety
6 - Reflective Questions Worksheets
iCAMIRA Facilitator’s Resource Manual
4 © 2010, Mount Sinai Hospital, Toronto, Canada
3 Days to 1 week prior to the program
� Send an email reminder to participants and provide instructions and directions to the program location
� If registration does not meet minimum numbers, cancel room bookings, catering, SPs and send a cancellation email to registered participants and managers
1 Day prior to the program
� Confirm the catering order (retain contact information and a copy of the catering order in case of additional inquiries)
� Confirm the equipment and room bookings (retain contact information in case of additional needs)
� Print signs for directions to the program location
� Review the facilitator guide and resources
� Print registration roster
Day of the program
Before the program
� Post the signs for directions to the program
� Set up chairs in the main room in a manner that will support the discussion among participants
� Load the DVD
� Set up the registration/sign in area
� Receive catering
End of the program
� Hand out certificates (if required)
� Remind participants to gather all of their belongings
� Clean up any remaining materials
� Take down signs for directions to the program
5© 2010, Mount Sinai Hospital, Toronto, Canada
Post program
� Email the group of participants if any of their belongings were left behind
� Update your participant tracking system, confirming participants who attended the facilitated discussion and those who did not
� Provide an electronic copy of the confirmed participants to the managers (if required)
� Send out ‘thank yous’ as required
� Write the program summary report (if required); summarize how it went and note any tips or suggestions for running future programs (this is an opportunity to refine the process of planning, implementing and evaluating the facilitated discussion program)
Facilitated Discussion Program
iCAMIRA Facilitator’s Resource Manual
6 © 2010, Mount Sinai Hospital, Toronto, Canada
Equipment, Resources & Planning
Equipment � DVD Player
� TV
� Screen
� Presentation room large enough to accommodate all of the participants for the group discussion
� Chairs (1 per participant and facilitator)
� Tables (consider whether your space will allow for a set-up where participants can face each other)
� Box of pens
� Name tags
� Masking tape
� Catering and tables to place the food/beverages (optional)
Facilitator ResourcesA copy of the following resources can be found in the Resources section of this manual.
Planning Resources
f The following resources were developed for the Simulation Workshop Program and can be modified for the Facilitated Discussion Program:
– Checklist for Simulation Workshop
– iCAMIRA Poster
– iCAMIRA Registration (sample email/poster)
– Incomplete eLearning Module (sample email)
– Preparing for the Simulation Workshop (sample email)
Implementation Resources
– Case Scenarios with Scoring Legend
– DVD of Patient Scenarios
– iCAMIRA Participant Evaluation Form
1 - Case Scenarios with Scoring Legend
2 - iCAMIRA Participant Evaluation Form
1 - Checklist for Simulation Workshop
2 - iCAMIRA Poster3 - iCAMIRA Registration4 - Incomplete eLearning
Module5 - Preparing for
Simulation Workshop
7© 2010, Mount Sinai Hospital, Toronto, Canada
– Observer Rating Scale for Patient Anxiety (3 per participant)
– Reflective Questions Worksheet
– Registration/sign in form
Facilitator Instructions
Program Agenda
8:00 – 8:15 am8:15 – 9:50 am9:50 –10:00 am
Introduction/OverviewDVD Scenarios and DiscussionWrap-up and Evaluation
Program Overview Introduction/Overview (15 minutes)
During the introduction and overview, cover the following key points:
� Welcome
� Have the facilitator and participants introduce themselves
� Housekeeping: note the location of the washrooms; ask participants to turn off all personal communication devices
� Ensure that each participant has 3 observer rating scales and the reflective questions worksheets so they can jot notes
� Overview of the workshop:
– The workshop is Part 2 of the illness related patient anxiety course
– The goal is to apply knowledge from eLearning module using generic scenarios that occur in the clinical areas on a regular basis
– The session provides an opportunity for interprofessional discussion and learning
– The session also provides an opportunity to practice using the anxiety tool
– The workshop is experiential and not evaluative
5 - Observer Rating Scale for Patient Anxiety
6 - Reflective Questions Worksheet
Facilitated Discussion Program
iCAMIRA Facilitator’s Resource Manual
8 © 2010, Mount Sinai Hospital, Toronto, Canada
Scenarios (90 minutes)
The DVD contains three scenarios. There is one scenario demonstrating low anxiety, one demonstrating moderate anxiety, and one demonstrating high anxiety. Each scenario is divided into two separate video clips: one where the nurse engages effectively with the patient, which facilitates decreased patient anxiety; and one where the nurse does not engage effectively with the patient, which does not decrease patient anxiety.
After each clip, it is recommended that you pause the DVD. This provides an opportunity to review the scoring of the anxiety tool with the participants and reflect on a series of questions that relate to the scenario that has just been viewed.
Detailed points of what you will see and hear once you load the DVD are outlined in the DVD Scenarios section of this guide. Also included is the scoring for the anxiety tool and discussion points for the reflective questions in each scenario.
Wrap-up and Evaluation (10 minutes)
� Have the participants complete the workshop evaluation
� Hand out the certificates for participation (if required)
� Remind the participants to gather all their belongings
9© 2010, Mount Sinai Hospital, Toronto, Canada
DVD Scenarios
Note: The SPs in these scenarios are depicting the role of an RN. The focus of the scenarios is not about healthcare professional’s roles and skills. The predominant focus is about communication and therapeutic engagement with the patient, which is applicable and can be generalized to all members of the interprofessional team.
When you load the DVD, you will hear the host narrator say:
“On screen there are two links: Facilitated Discussion and Independent Learner . If you are a facilitator leading a group through the scenarios and discussion, click Facilitated Discussion . If you are working through the scenarios on your own, click Independent Learner .”
Once you have clicked on the Facilitated Discussion link, you will hear the host narrator say:
“Welcome to the Facilitated Discussion version of the iCAMIRA scenarios . Please refer to the Facilitated Discussion section of your facilitator manual .
Press play when you are ready to watch the first scenario .
You can pause the DVD as necessary and you can go back and watch the scenarios as often as you wish .”
There are three patient scenarios included on the DVD:
Scenario 1: Rose HatfieldScenario 2: Phil ArcherScenario 3: Amanda Cooper
Note: Please refer to page 7 of the Independent Learner Program Participant Guide for more detail about how to operate the DVD.
Facilitated Discussion Program
Independent Learner Program
iCAMIRA Facilitator’s Resource Manual
10 © 2010, Mount Sinai Hospital, Toronto, Canada
Scenario 1: Rose Hatfield
A reminder that there are 2 video clips per scenario. It is recommended that you pause for scoring of the tool and discussion after each clip. The clip where the nurse engages less effectively is always played first.
You can read the following stem (introduction) to the scenario and/or have the participants read along from the Reflective Questions Worksheets for Facilitated Discussion.
Rose Hatfield is a married woman in her 50s with three daughters. She came to the emergency department 2 days ago with severe abdominal cramping.
Rose is aware of her bowel obstruction, which is being treated. She is on intravenous fluids, has a naso-gastric tube, and is receiving Tylenol extra strength every 4 hours as needed for pain. The team has done an X-ray, an ultrasound and some blood work. The Resident she saw this morning told her that they detect an obstruction in the large intestine, but they are awaiting results of the MRI before they can proceed.
Jill is meeting Rose Hatfield for the first time. As you watch the scenario, observe not only what Jill and Rose are saying, but also observe the non-verbal communication. As you watch, have a copy of the anxiety scale with you and score each of the categories: anxious mood, fears, trouble thinking, tension, and sleep problems. There may be some categories that Jill does not assess. Think of the questions you might ask Rose to obtain all the necessary information.
Rose Clip 1
Facilitator Questions and Points for DiscussionQUESTION:
Based on your scoring of the anxiety assessment tool, is Rose’s anxiety low, moderate or high?
DISCUSSION:
Rose’s anxiety would be assessed as low.
f Rose appears very minimally anxious, so that would score a 0.
11© 2010, Mount Sinai Hospital, Toronto, Canada
f She expresses a slight fear with regards to being ill and perhaps losing her job, so this would be scored as a 1.
f Trouble thinking wasn’t directly assessed, but Rose does not appear to be having any difficulties with this, so would score a 0.
f There is some tension in her face so depending on interpretation would be a 0 or 1.
f She clearly indicates difficulty with sleep so this would score a 2.
f Total score is 3 or 4, which suggests low anxiety.
QUESTIONS:
What strategies does Jill use to engage Rose? Does she... seek information? ... ask open-ended or directive questions? ... use touch and appropriate
personal space?
What do you notice about Jill’s non-verbal communication?
DISCUSSION:
f Jill clearly obtains the information for her assessment by asking questions such as: “How are you sleeping”? “How’s the abdominal pain”? These are considered open-ended questions. This gives Rose the opportunity to respond with a simple yes or no or, if she chooses, go on to elaborate. Although Jill’s focus is clearly on the patient, her facial expression and overall disposition was one of being rushed. As if to say “…I’m here to get the info I need for my assessment, I’ll answer some questions and then I’m moving on.”
QUESTIONS:
How would you describe Rose’s body language? - Is it relaxed or tense? - Does she look worried, anxious, upset?
DISCUSSION:
f Rose’s expression is somewhat strained. She is clearly tense, but not overly anxious.
Facilitated Discussion Program
iCAMIRA Facilitator’s Resource Manual
12 © 2010, Mount Sinai Hospital, Toronto, Canada
QUESTION:
What appears to be Rose’s main concern/fear/worry?
DISCUSSION:
f Rose appears to be quite focused on her MRI result and she also has some concern about being in the hospital too long and the implications for her job.
QUESTIONS:
Do you think Jill adequately addressed Rose’s anxiety? Explain why you think so.
Would you have done anything differently to address Rose’s concerns?
DISCUSSION:
f These are subjective questions and meant to stimulate discussion before launching into the second clip.
Rose Clip 2
Facilitator Questions and Points for DiscussionQUESTION:
Based on your scoring of the anxiety assessment tool in this second clip, is Rose’s anxiety low, moderate or high?
DISCUSSION:
Rose’s anxiety would be assessed as low.
f Rose appears very minimally anxious so that would score a 0.
f In this interaction Rose does express a fear of an outcome of cancer so this would be scored as a 2.
f Trouble thinking wasn’t directly assessed. Rose does not appear to be having any difficulties with thinking so would score a 0.
f There is some tension in her face so depending on interpretation would be a 0 or 1.
f She clearly indicates difficulty with sleep so this would score a 2.
f Total score is 4 or 5, which suggests low anxiety.
13© 2010, Mount Sinai Hospital, Toronto, Canada
A few words about the assessment tool. The scoring is subjective which is why some categories are scored within a range. It’s very likely that your total score will vary with that of your colleagues. It’s okay if everyone doesn’t end up with exactly the same number. What’s important are the low, moderate and high categories. These categories determine the appropriate interventions for decreasing anxiety.
For this particular interaction, you may be wondering why the fears category is a 2 instead of a 3. Looking at the scoring scale, a 2 indicates the symptom is obvious, but does not interfere with function. A score of 3 indicates that the symptom is severe enough to be interfering with the patient’s function. In this interaction, it is clear that Rose’s function is not impaired by her fear.
QUESTIONS:
What strategies did Jill use to engage Rose? Does she... seek information? ... ask open-ended or directive questions?
Compared to the first clip how is her use of touch and personal space?
Is Jill’s non-verbal communication different from the first clip and if so, how?
What did this interaction reveal as Rose’s greatest concern or fear or worry?
What did Jill do differently in this interaction to get that information?
DISCUSSION:
f Jill engages the patient by asking more open-ended questions like, “How are you doing today”? “Is there something else worrying you”? Jill probes a little to get more information about Rose’s focus on the MRI result. She also stands closer to Rose and her tone is a little warmer.
f The other thing Jill does in this clip is communicate a lot of information to Rose. You may be thinking, “what”?!! Jill couldn’t tell Rose anything about her MRI result. It’s true that Jill did not have the actual test result, and even if she did would not be able to convey the result. That’s not part of her scope of practice. It’s okay to say that you don’t know or you don’t have the results. But don’t stop there. Think about all the information that Jill did tell Rose. She told her how long the result might take and that the doctor would be the one to come in and tell her the result, and that once the result was back, a treatment plan would be developed. We sometimes take these things for granted because we live and breathe these routines everyday. Remember however, that for the patient, hospital procedures and routines are unfamiliar, and this often gives rise to fears, anxieties and worries.
Facilitated Discussion Program
iCAMIRA Facilitator’s Resource Manual
14 © 2010, Mount Sinai Hospital, Toronto, Canada
f At this point, you may think, “The anxiety tool scoring for the two clips is the same. What’s the difference between the two clips?”
f Rose is the type of patient that healthcare professionals (HCPs) often describe as the “nice or pleasant” patient. She doesn’t want to disturb anyone or rock the boat. On the surface, her main concern is the MRI result.
f Jill’s interaction with Rose in the first clip is, reasonable. In the second clip however, Jill’s tone of voice is noticeably warmer. She provides Rose with a lot of useful information about the test result process and the availability of services that might be helpful. She observes Rose’s pre-occupation with the MRI result. Jill takes this as a cue to ask even more open-ended questions. She probes with the question, “Is there something else worrying you?” Sometimes HCPs are wary of asking such pointed questions. Don’t worry; if the patient finds your question too intrusive or doesn’t want to talk, he or she will let you know…and that in itself is a piece of information!
f All of these things help Jill to build trust and rapport with Rose. That trust provides the opportunity for Rose to divulge more about herself. This gives Jill a much clearer picture of why Rose is so worried about the MRI result.
f Our role as HCPs is not just about assessing anxiety and getting a score to document. Our role is to recognize our patients’ anxiety and to try and manage it. Everything Jill did in the second clip to build trust and rapport helped to decrease Rose’s anxiety. Not convinced…go back and watch Rose’s body language at the end of each of the clips…what do you notice? One more thing…Jill’s interaction in the second clip didn’t take much more time than the first clip and overall provided Rose with a better patient experience.
15© 2010, Mount Sinai Hospital, Toronto, Canada
Scenario 2: Phil Archer
A reminder that there are 2 video clips per scenario. It is recommended that you pause for scoring of the tool and discussion after each clip. The clip where the nurse engages only minimally is always played first.
You can read the following stem (introduction) to the scenario and/or have the participants read along from the Reflective Questions Worksheets for Facilitated Discussion.
Phil Archer is a widowed man of 75 who lives alone in a walk up apartment. He has Type I diabetes, which he does not manage very consistently. He uses the emergency department as his main location for care. He has been a frequent visitor to the hospital for various reasons related to his health over the years.
Phil presented to the emergency department with concerns about his foot 3 days ago. It didn’t hurt so much but it was red and swollen and starting to ooze. His blood glucose levels were very high. He was admitted for tests. His insulin is being titrated and he is receiving intravenous antibiotics. He is eating and can move around but isn’t getting out of bed except to go to the bathroom. The surgical consult team have assessed his foot.
Mary is meeting Phil Archer for the first time. As you watch the scenario, observe not only what Mary and Phil are saying, but also observe the non-verbal communication. As you watch the scenario, have a copy of the anxiety scale with you and score each of the categories: anxious mood, fears, trouble thinking, tension, and sleep problems. There may be some categories that Mary does not assess. Think of the questions you might ask Phil to obtain all the necessary information.
Facilitated Discussion Program
iCAMIRA Facilitator’s Resource Manual
16 © 2010, Mount Sinai Hospital, Toronto, Canada
Phil Clip 1
Facilitator Questions and Points for Discussion QUESTION:
Based on your scoring of the anxiety assessment tool, is Phil’s anxiety low, moderate or high?
DISCUSSION:
Using the anxiety assessment tool Phil’s anxiety would be assessed as moderate.
f It’s not clear from this interaction if he has an anxious mood, fears or trouble thinking, so all those components would be scored as 0.
f Phil’s hand ringing and lack of eye contact indicate he is experiencing tension and would be scored as a 2.
f Phil has clearly stated that he has not slept well in hospital. It’s unclear whether this is interfering with Phil’s function and therefore would score a 2.
f Phil’s total score is 4 and therefore a low level of anxiety. Since the assessment has given us no information on the first three categories, we really can’t consider this an accurate reflection of Phil’s level of anxiety.
QUESTIONS:
What strategies does Mary use to engage Phil? Does she... seek information? ... ask open-ended or directive questions?
Describe Mary’s non-verbal communication.
Describe Phil’s non-verbal communication.
DISCUSSION:
f Mary’s tone and facial expression are pleasant. Phil is not making eye contact with Mary and his facial expression appears somewhat put-off or disinterested. Mary seeks information for her assessment by asking questions such as: “How was your sleep last night?” “How’s your foot?” “How are you feeling this morning?” These are open-ended questions.
17© 2010, Mount Sinai Hospital, Toronto, Canada
QUESTION:
Do you have a sense of Phil’s main concern or fear or worry?
DISCUSSION:
f Based on this interaction, it’s very hard to know what Phil’s main worry is.
QUESTION:
Would you have done anything differently in your interaction with Phil?
DISCUSSION:
f Phil is a gentleman who doesn’t open up easily. He’s not a big conversationalist! Because of this, there may be a tendency for HCPs to “write Phil off” and forget about him, thinking that he doesn’t want to engage. The fact that Phil is asking for nurses Margaret or Jackie indicates that he has engaged with staff in the past. This is a cue for Mary.
f Because Phil isn’t a big communicator, he has a lot bottled up and going on in his head. It’s often very hard for this type of patient to answer open-ended questions. They have difficulties focusing on any one problem or concern. So, as HCPs, we need to help focus their thinking. Rather than asking, “How was your sleep last night?”, Mary could ask, “Did you sleep well last night?” Based on Phil’s responses, she could continue to ask more directive questions. This would allow Phil to focus his thinking while at the same time allow for some rapport to develop between Phil and Mary. Another approach would have been for Mary to pick up on Phil’s cue when he responded that he hadn’t been sleeping well in hospital. To ask Phil why he was “having difficulty sleeping”, or “what was interfering with his sleep”, would have helped Mary gain a better understanding of Phil.
Facilitated Discussion Program
iCAMIRA Facilitator’s Resource Manual
18 © 2010, Mount Sinai Hospital, Toronto, Canada
Phil Clip 2
Facilitator Questions and Points for Discussion QUESTION:
Based on this interaction, what is your scoring of the anxiety assessment tool for Phil?
DISCUSSION:
f Phil’s anxious mood would score a 1.
f He has a fear of losing his foot and fears the implications for his independence, so the fears category would score a 2.
f The trouble thinking category would be scored a 3 because it is interfering with his function: he can’t remember information given to him by the surgeon and he can’t read the newspaper.
f The ringing of his hands and lack of eye contact indicate a score of 2 for the tension category and sleep would score a 1 or 2.
f Total score is 9 or 10 which indicates a moderate level of anxiety.
Notice in this second clip that Phil is not engaged and he may be upset that familiar nurses are not looking after him. Mary is not put off by this. She attempts to connect with Phil by saying, “I’d like to get to know you better.” Mary also tries to find out more about why Phil hasn’t been sleeping by asking, “What’s up?” This conveys to Phil that Mary is interested and helps to develop rapport.
QUESTION:
What do you think Mary accomplishes by moving to the other side of the bed and gently tugging at the bedsheets?
DISCUSSION:
f In moving to the other side of the bed, Mary placed herself directly in Phil’s line of site, tugged at the bedsheet and asked, “Is there something you’re upset or worried about?” When patients are anxious or worried, they are often not aware of their behaviour. Fidgeting and wringing of hands can indicate anxiety. By picking up on that cue, Mary is making Phil aware of his fidgeting and it also conveys to Phil that Mary is paying attention which further develops rapport.
19© 2010, Mount Sinai Hospital, Toronto, Canada
QUESTION:
How does Mary get to Phil’s main fear or worry?
DISCUSSION:
f Mary realizes that she is not getting any information from Phil with open-ended questions and so switches to a more direct line of questioning. “Are you worried about your foot, Phil?” There is a possibility that Phil would have answered, “no” and Mary would then need to ask another question. In this case, Phil’s main fear is about his foot and what that might mean for his independence.
f Mary’s interaction in the first clip was reasonable, but incomplete. Recall that three of the five categories on the anxiety tool were not assessed. Based on the interaction in the second clip, it is clear that spending a bit more time to engage with Phil is very beneficial in getting not only a complete assessment of his level of anxiety, but also a better grasp of Phil’s situation overall. If you can’t recall, view the two clips again and pay attention to Phil visibly relaxing in the second clip as compared to the first clip.
f For patients like Phil, there are two important points to remember: 1. They need more time to open up and engage which means that as a HCP
you may need to return several times to engage in order to develop some rapport
2. Closed or directive type questions will be more effective
f This becomes even more pertinent when the patient is anxious or worried. It may seem counter-intuitive to ask closed or directive type questions because as HCPs we are taught to ask open-ended questions. It’s generally a good rule of thumb to start with open-ended questions, and be prepared to move to directive or more close-ended type questions when the open-ended approach doesn’t work.
f So the next time you encounter a Phil-type patient, don’t dismiss them because of their apparent lack of engagement. There’s often a lot going on for these patients. It just takes a little more time and patience as HCPs to find it out.
Facilitated Discussion Program
iCAMIRA Facilitator’s Resource Manual
20 © 2010, Mount Sinai Hospital, Toronto, Canada
Scenario 3: Amanda Cooper
A reminder that there are 2 video clips per scenario. It is recommended that you pause for scoring of the tool and discussion after each clip. The clip where the nurse engages only minimally is always played first.
You can read the following stem (introduction) to the scenario and/or have the participants read along from the Reflective Questions Worksheets for Facilitated Discussion.
Amanda Cooper is a married woman in her 40s. She is the mother of five. Yesterday Amanda was shopping when she began to feel weak and her vision went black. She was then brought to the ER where they did a neurological workup and determined that she had a Transient Ischemic Attack (TIA) “mini stroke”.
Amanda has been sick her whole life and is a seasoned consumer of healthcare services. She had rheumatic fever as a child and has been diagnosed with mitral valve stenosis. She is on Coumadin because they told her she has thick blood and she needed it for her heart. The medical team is doing a diagnostic workup including blood work, electrocardiogram and MRI of the head. There is nothing conclusive at this point and the working diagnosis is still a TIA.
Mike is meeting Amanda Cooper for the first time. As you watch the scenario, observe not only what Mike and Amanda are saying, but also observe the non-verbal communication. As you watch the scenario, have a copy of the anxiety scale with you and score each of the categories: anxious mood, fears, trouble thinking, tension, sleep problems. There may be some categories that Mike does not assess. Think of the questions you might ask Amanda to obtain all the necessary information.
21© 2010, Mount Sinai Hospital, Toronto, Canada
Amanda Clip 1
Facilitator Questions and Points for Discussion QUESTION: Based on your scoring of the anxiety assessment tool, is Amanda’s anxiety low, moderate or high?
DISCUSSION:
f Amanda’s anxiety and fears each score a 4. She is completely focused on having a brain tumor and dying.
f Trouble thinking was not clearly assessed, however she is using her laptop which would indicate an ability to concentrate.
f She is not crying or restless, but there is a certain tension in her body so tension could score a 1.
f She does indicate an inability to sleep and so would score at least a 2. It would require a little more probing to get a sense of how much the lack of sleep is contributing to Amanda’s overall anxiety and whether it is interfering with her ability to function.
f Total score is 11 which indicates a high level of anxiety.
QUESTIONS: Amanda is anxious as soon as Mike walks in. What are the signs of her anxiety?What do you observe in Mike’s non-verbal communication?
Mike tells Amanda to calm down. What impact does that have on her anxiety?Does Mike do anything to decrease Amanda’s anxiety?
DISCUSSION:
f With Amanda, it is important to recognize the signs of high anxiety and to try and manage, rather than assess the anxiety. Her level of anxiety is clearly high, as are her fears of a brain tumor and dying.
f Mike’s body language is one of retreating from Amanda and trying to leave the room as quickly as possible. Telling Amanda to “calm down” just inflames the situation, as she does not feel heard or supported. At times, it appears as if Mike is trying to control a bit of a smirk as if to say, “Lady…are you for real?” None of these things help to build rapport with Amanda, nor do they help to decrease her anxiety.
Facilitated Discussion Program
iCAMIRA Facilitator’s Resource Manual
22 © 2010, Mount Sinai Hospital, Toronto, Canada
Amanda Clip 2
Facilitator Questions and Points for Discussion QUESTION: Based on your scoring of the anxiety assessment tool, is Amanda’s anxiety low, moderate or high?
DISCUSSION:
Scoring is the same as clip 1.
QUESTIONS: What does Mike say and do to help decrease Amanda’s anxiety?Is the deep-breathing exercise effective with Amanda?
DISCUSSION:
f In this clip, Mike’s body language is conveying that he is going to stay and not run out of the room. He listens and is supportive. He provides reassurance that the team is trying to figure out what is wrong with her and not keeping anything from her in the process. Note Amanda’s response and visible change in presentation when Mike says, “Anyone in your position would be worried.” She is relieved by his normalizing statement, which conveys acknowledgement and support. Similar to the Rose scenario, Amanda has questions that Mike can’t completely answer, yet he provides what information is available. Amanda’s anxiety visibly decreases some more when Mike says, “Now I heard you mention a stroke and a TIA. These are not the same thing…” Listening, understanding and providing some information all build trust with Amanda and help to decrease her anxiety.
f In this instance, the deep-breathing exercise is not very effective. It’s always worth a try as some patients find it very effective. Remember that you can also print out the Information Sheet: Breathing Exercises and Information Sheet: Relaxation Techniques and leave it with your patient. Even a patient as anxious as Amanda might do the exercise on their own after the healthcare professional has left the room.
f Similar to the Rose scenario, you may be saying to yourself, “The anxiety tool scoring for the two clips is the same.” “What’s the difference between the two clips?”
3 - Information Sheet: Breathing Exercises
4 - Information Sheet: Relaxation Techniques
23© 2010, Mount Sinai Hospital, Toronto, Canada
f In the first clip, Mike is challenged by Amanda’s high affect and anxiety. His body language and tone of voice convey to Amanda that she is not being taken seriously and that Mike can’t wait to leave the room. For Amanda, –who is looking for answers and some re-assurance that she’s not dying,- Mike’s interaction does nothing to decrease her anxiety.
f In the second clip, Mike is fully present; not retreating. This is very important in building an initial connection with Amanda. Mike listens and conveys understanding for Amanda’s situation. He provides re-assurance that the team is not avoiding her and provides as much information as he can to allay her fears. As you saw in the second clip, all of these things decreased Amanda’s anxiety.
f The challenge for HCPs is to find a way to tolerate Amanda’s affect. If the HCP just keeps leaving the room (as in the first clip), Amanda’s anxiety will not be addressed and in fact will continue to increase, which will probably lead to her constantly ringing the call bell.
f It’s tempting to label patients like Amanda as histrionic or “over-the-top”. They are often viewed as “difficult or needy”. HCPs need to recognize the patient’s distress and find ways to manage their own discomfort with this high affect. Start by recognizing the patient’s distress. Use your colleagues for support, have a care plan for consistency and be aware of your own triggers.
f Our role as HCPs goes beyond assessing for anxiety and getting a score to document. Our role is to recognize our patient’s anxiety and to try and manage it. Everything Mike did in the second clip to build trust and rapport helped to decrease Amanda’s anxiety. One more thing that bares repeating…Mike’s interaction in the second clip didn’t take a lot more time than the first clip, and overall, provided Amanda with a better patient experience!
Facilitated Discussion Program
iCAMIRA Facilitator’s Resource Manual
24 © 2010, Mount Sinai Hospital, Toronto, Canada
Scenario Summary Points
Now that you have seen and reflected upon all three scenarios, let’s summarize the key points.
1. Engaging your patients and developing rapport helps them feel cared for and will help decrease their anxiety.
2. Engaging your patients and developing rapport improves the patient care experience and gives you more job satisfaction.
3. Recall from the scenarios that it really didn’t take a lot more time to engage and do a good assessment of the patient’s anxiety. Remember that an extra minute can make a big difference in decreasing your patient’s anxiety and actually save you a lot of “responding to call-bell” time in the end.
4. Be aware of “cues” from the patient and don’t be afraid to ask questions rather than trying to guess what the cues mean. The cues may be verbal or non-verbal.
5. Each patient is different. Use the different communication techniques you’ve learned to connect with your patient.
6. The anxiety assessment tool provides you and your colleagues with a common language with which to communicate about patient anxiety. It is a subjective tool, so not everyone will have exactly the same score. What are important are the categories of low, moderate and high. It is these categories that determine the appropriate interventions.
Independent Learner Program
Participant Guide
Table of Contents
Participant Welcome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1Purpose . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1Learning Objectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2Description . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2
eLearning Module . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3Instructions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3Purpose . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3Description . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3Learning Objectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4Topics. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4
Experiential Module . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Purpose . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5Description . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5Learning Objectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6
Preparing To View the DVD Scenarios . . . . . . . . . . . . . . . . . . . 7DVD Scenarios. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7
Rose Hatfield Scenario . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Rose Video Clip 1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9Rose Video Clip 2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Phil Archer Scenario . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Phil Video Clip 1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Phil Video Clip 2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Amanda Cooper Scenario . . . . . . . . . . . . . . . . . . . . . . . . . . 13Amanda Video Clip 1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Amanda Video Clip 2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Narrator Script for Rose Hatfield . . . . . . . . . . . . . . . . . . . . . . 15Rose Video Clip 1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Rose Video Clip 2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
Narrator Script for Phil Archer . . . . . . . . . . . . . . . . . . . . . . . 19Phil Video Clip 1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19Phil Video Clip 2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Narrator Script for Amanda Cooper . . . . . . . . . . . . . . . . . . . . 23Amanda Video Clip 1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23Amanda Video Clip 2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Scenario Summary Points . . . . . . . . . . . . . . . . . . . . . . . . . . 26Observer Rating Scale for Patient Anxiety . . . . . . . . . . . . . . . . 27Information Sheet: Breathing Exercises . . . . . . . . . . . . . . . . . 28Information Sheet: Relaxation Techniques . . . . . . . . . . . . . . . 29
1© 2010, Mount Sinai Hospital, Toronto, Canada
Participant Welcome
Welcome to the Participant Guide for the Independent Learner Program. This guide outlines the purpose of the education, provides a description, and the learning objectives. The guide outlines detailed steps on how to complete the modules and contains all the necessary information and resources you will require.
Figure 1: Overview of the Education Program
PurposeThe experience of illness and hospitalization is stressful and anxiety is a very typical occurrence among hospital inpatients. Teaching healthcare professionals proven methods to assess and manage patient anxiety is a step towards improving the quality of care experienced by patients.
This educational program aims to deliver the necessary skills to healthcare professionals so that they can assess and manage illness related patient anxiety. This is the normal type of anxiety that patients and their families experience from being ill and in the hospital. The focus of this training is not on the psychiatric diagnosed type of anxiety.
Simulation WorkshopProgram
FacilitatedDiscussion Program
EvaluationAnxietyAssessment
Independent Learner
Program
OrganizationalReadiness
eLearningModule
Independent Learner Program
iCAMIRA Facilitator’s Resource Manual
2 © 2010, Mount Sinai Hospital, Toronto, Canada
Description The program has two parts. The first is an eLearning module that includes content about illness related patient anxiety and instructions about how to use and interpret an anxiety assessment tool. Following completion of the eLearning module, you will complete an experiential module by watching patient scenarios on a DVD and applying your knowledge from the eLearning module.
Learning ObjectivesThe learning objectives for the Independent Learner Program are:
1. Recognize symptoms of low, moderate and high anxiety through use of the standardized assessment tool.
2. List various verbal and non-verbal communication techniques for engaging patients.
3. List interventions that help manage patient anxiety.
3© 2010, Mount Sinai Hospital, Toronto, Canada
Independent Learner Program
ELearning Module
Instructions You are required to complete the eLearning module prior to starting the experiential module.
You will have received an email or flyer providing the following details:
� How and where to access the eLearning module.
� Passing quiz score for successful completion of the eLearning module.
� Whether or not you are required to print your quiz score and completion of the module. If you are using the eLearning Module CD, it has an option for you to print your quiz score and completion of the module. This is done by clicking “print screen” and then “Ctrl V” (paste) in a Word document in a Windows PC environment.
PurposeThe eLearning module provides information on illness related patient anxiety and will teach you how to assess and manage illness related patient anxiety using the Observer Rating Scale for Patient Anxiety.
DescriptionThe module includes general information on illness related patient anxiety along with an overview and purpose of the Observer Rating Scale for Patient Anxiety. Detailed explanations of each of the five items (anxious mood, fears, trouble thinking, tension, sleep) on the Observer Rating Scale for Patient Anxiety are provided as well as an explanation of the scoring system for the tool. This is done using screen shots of the actual tool. Scoring examples are provided for each of the levels of low, moderate and high anxiety.
5 - Observer Rating Scale for Patient Anxiety
IMPORTANT !
If you have not received this
information, contact your manager or
educator.
iCAMIRA Facilitator’s Resource Manual
4 © 2010, Mount Sinai Hospital, Toronto, Canada
You will then practice using the tool through three vignettes; one each for low, moderate and high anxiety. Based on your responses, you will be provided with feedback and rationale as to whether their response is correct or incorrect. For each of the vignettes, you will be given potential strategies for managing low, moderate and high anxiety.
Throughout the module there are non-evaluative checkpoints for you to assess your knowledge. There is also a quiz at the end of the module. The eLearning module takes approximately 1.5-2 hours to complete.
Learning Objectives
The learning objectives for the eLearning module are:
1. Recognize and assess illness related patient anxiety.
2. Understand the principles of patient and family centered care and interprofessional education as it relates to assessing and managing illness related patient anxiety.
3. Use a standardized tool to assess for illness related patient anxiety.
4. Implement interventions to manage illness related patient anxiety.
TopicsThe module covers the following topics:
1. Interprofessional Education 2. Patient and Family Centered Care3. Definitions are provided for:
a. Anxiety disorderb. Illness related patient anxietyc. Stressd. Distresse. Emotion
4. Effective Communication and the Therapeutic Relationship
5. Assessing Illness Related Patient Anxiety
6. Screening Tool 7. Interventions for Managing Illness
Related Patient Anxiety
5© 2010, Mount Sinai Hospital, Toronto, Canada
Experiential Module
You are required to complete the eLearning module prior to starting this experiential module.
You will have received an email or flyer providing the following details:
f How and where to access the DVD.
f Instructions on whether or not you are required to complete a reflective exercise or writing assignment in order to receive credit for completing this module.
PurposeThis learning experience will give you the opportunity to apply your knowledge from the eLearning module through viewing and reflecting upon patient scenarios as they pertain to illness related anxiety.
DescriptionYou will watch a DVD that contains patient scenarios. The scenarios were filmed using Standardized Patients from the University of Toronto Standardized Patient Program for both the patient and healthcare professional roles.
There are three scenarios and they are generic medical/surgical patient scenarios. There is one scenario demonstrating low anxiety, one demonstrating moderate anxiety and one demonstrating high anxiety. Each scenario is divided into two separate video clips: one where the nurse engages effectively with the patient; and one where the nurse engages less effectively with the patient.
After each clip, the host narrator will review the scoring of the anxiety tool and you will be provided with an explanation of the scoring. The narrator will then lead you through a series of reflective questions related to each scenario.
Independent Learner Program
IMPORTANT !
If you have not received this
information, contact your manager or
educator.
iCAMIRA Facilitator’s Resource Manual
6 © 2010, Mount Sinai Hospital, Toronto, Canada
Learning ObjectivesThe learning objectives for the Experiential Module are:
1. Recognize symptoms of low, moderate and high anxiety through use of the standardized assessment tool.
2. List various verbal and non-verbal communication techniques for engaging patients.
3. List interventions that help manage patient anxiety.
7© 2010, Mount Sinai Hospital, Toronto, Canada
You should allow yourself 1 to 1.5 hours to watch the DVD scenarios. If you are in a room with other people, you will need to wear headphones. Included in this guide is the Observer Rating Tool for Patient Anxiety. This is the tool you will use to score your assessment of the patient’s anxiety in each of the scenarios. You will need three copies of the tool, one for each scenario.
After each video clip, the narrator will guide you through the scoring for the anxiety tool and a series of reflective questions for the video clip you have just watched. There will be a ‘pause’ after each question during which time you can jot down your responses. The reflective questions are provided in a subsequent section in this guide.
You don’t need to take copious notes of the narrator’s discussion points. The complete narrator scripts are provided at the end of this guide.
General Note: You will be viewing the material in DVD form, not DVD ROM.This means you will be navigating using menus which are more like a commercial movie DVD rather than that of a ROM disc or website. To view this disc you will need the type of DVD player that will play DVD movies.This can be either a set top style or in a computer. If your computer cannot play movies (such as the type you might rent or buy) then it will not play this disc. Take a moment to familiarize yourself with the controls of your DVD player so that you can easily Pause, Stop and Play the video. On occasion the narrator will suggest you pause the video manually in order to reflect on the questions. You will want to know whether the remote control or the mouse will give you the control. If you wish to stop and reflect on a question or jot down some notes, press Pause and resume by pressing Play.
Another useful control is the Menu or Title button that takes you back to a menu if you need to make a new selection.
Menus will offer you multiple options. Learn to use the UP / DOWN arrows on your remote control or on you computer keyboard to highlight your selection. Then press Enter or Return to view what you have highlighted.
Preparing To View the DVD Scenarios
Independent Learner Program
5 - Observer Rating Scale for Patient Anxiety
iCAMIRA Facilitator’s Resource Manual
8 © 2010, Mount Sinai Hospital, Toronto, Canada
DVD Scenarios Note: The SPs in these scenarios are depicting the role of an RN. The focus of the scenarios is not about healthcare professional’s roles and skills. The predominant focus is about communication and therapeutic engagement with the patient, which is applicable and can be generalized to all members of the interprofessional team.
When you load the DVD, you will hear the host narrator say:
“On screen there are two links: Facilitated Discussion and Independent Learner . If you are a facilitator leading a group through the scenarios and discussion, click Facilitated Discussion . If you are working through the scenarios on your own, click Independent Learner .”
Once you have clicked on the Independent Learner link, you will hear the host narrator say:
“Welcome to the Independent Learner version of the iCAMIRA scenarios . Please refer to your Independent Learner Guide for more detail .
I will guide you through this DVD . You will be watching three generic medical/surgical patient scenarios .
Each scenario is divided into two separate video clips: one where the nurse engages effectively with the patient which facilitates decreased patient anxiety; and one where the nurse does not engage effectively with the patient which does not decrease patient anxiety .
After each clip, you will review the scoring of the anxiety tool and be provided with an explanation of the scoring . You will then be asked to reflect on a series of questions that relate to the scenario you have just viewed .
Press play when you are ready to watch the first scenario . You can pause the DVD as necessary and you can go back and watch the scenarios as often as you wish .”
9© 2010, Mount Sinai Hospital, Toronto, Canada
Rose Hatfield Scenario
Rose Hatfield is a married woman in her 50s with three daughters. She came to the emergency department 2 days ago with severe abdominal cramping.
Rose is aware of her bowel obstruction, which is being treated. She is on intravenous fluids, has a naso-gastric tube, and is receiving Tylenol extra strength every 4 hours as needed for pain. The team has done an X-ray, an ultrasound and some blood work. The Resident she saw this morning told her that they detect an obstruction in the large intestine, but they are awaiting results of the MRI before they can proceed.
Jill is meeting Rose Hatfield for the first time. As you watch the scenario, observe not only what Jill and Rose are saying, but also observe the non-verbal communication. As you watch, have a copy of the anxiety scale with you and score each of the categories: anxious mood, fears, trouble thinking, tension, and sleep problems. There may be some categories that Jill does not assess. Think of the questions you might ask Rose to obtain all the necessary information.
Rose Video Clip 1The narrator will now guide you through the scoring of the anxiety tool and a series of reflective questions based on the video clip you just watched. There will be a pause after each question during which time you can jot down your responses.
QUESTIONS:
1. Based on your scoring of the anxiety assessment tool, is Rose’s anxiety low, moderate or high?
2. What is the rationale for your scoring on the anxiety tool?
3. What strategies does Jill use to engage Rose? Does she... seek information? ... ask open-ended or directive questions? ... use touch and appropriate personal space?
4. What do you notice about Jill’s non-verbal communication?
NOTES:
Independent Learner Program

iCAMIRA Facilitator’s Resource Manual
10 © 2010, Mount Sinai Hospital, Toronto, Canada
5. How would you describe Rose’s body language? - Is it relaxed or tense?- Does she look worried, anxious, upset?
6. What did you observe to be Rose’s main concern or fear or worry?
7. Do you think Jill adequately addressed Rose’s anxiety? Write down why you think so.
8. Write down if you would you have done anything differently to address Rose’s concerns.
Rose Video Clip 2The narrator will now guide you through the scoring of the anxiety tool and a series of reflective questions based on the video clip you just watched. There will be a pause after each question during which time you can jot down your responses.
QUESTIONS:
1. Based on your scoring of the anxiety assessment tool, is Rose’s anxiety low, moderate or high?
2. What is the rationale for your scoring on the anxiety tool?
3. What strategies does Jill use to engage Rose? Does she... seek information?... ask open or closed ended questions?
4. Compared to the first clip, how is her use of touch and personal space?
5. Is Jill’s non-verbal communication different from the first clip and if so, how?
6. What does this interaction reveal as Rose’s greatest concern or fear or worry?
7. What does Jill do differently in this interaction to get at that information?
NOTES:
NOTES:
11© 2010, Mount Sinai Hospital, Toronto, Canada
Phil Archer Scenario
Phil Archer is a widowed man of 75 who lives alone in a walk up apartment. He has Type I diabetes, which he does not manage very consistently. He uses the emergency department as his main location for care. He has been a frequent visitor to the hospital for various reasons related to his health over the years.
Phil presented to the emergency department with concerns about his foot 3 days ago. It didn’t hurt so much but it was red and swollen and starting to ooze. His blood glucose levels were very high. He was admitted for tests. His insulin is being titrated and he is receiving intravenous antibiotics. He is eating and can move around, but isn’t getting out of bed, except to go to the bathroom. The surgical consult team have assessed his foot.
Mary is meeting Phil Archer for the first time. As you watch the scenario, observe not only what Mary and Phil are saying, but also observe the non-verbal communication. As you watch the scenario, have a copy of the anxiety scale with you and score each of the categories: anxious mood, fears, trouble thinking, tension, and sleep problems. There may be some categories that Mary does not assess. Think of the questions you might ask Phil to obtain all the necessary information.
Phil Video Clip 1The narrator will now guide you through the scoring of the anxiety tool and a series of reflective questions based on the video clip you just watched. There will be a pause after each question during which time you can jot down your responses.
QUESTIONS:
1. Based on your scoring of the anxiety assessment tool, is Phil’s anxiety low, moderate or high?
2. What is the rationale for your scoring on the anxiety tool?
3. What strategies does Mary use to engage Phil? Does she... seek information? ... ask open-ended or directive questions?
NOTES:
Independent Learner Program
iCAMIRA Facilitator’s Resource Manual
12 © 2010, Mount Sinai Hospital, Toronto, Canada
4. Describe Mary’s non-verbal communication?
5. Describe Phil’s non-verbal communication?
6. Do you have a sense of Phil’s main concern or fear or worry?
7. Would you have done anything differently in this interaction with Phil?
Phil Video Clip 2 The narrator will now guide you through the scoring of the anxiety tool and a series of reflective questions based on the video clip you just watched. There will be a pause after each question during which time you can jot down your responses.Based on this interaction, what is your scoring of the anxiety assessment tool for Phil?
QUESTIONS:
1. What is the rationale for your scoring on the anxiety tool?
2. What do you think Mary accomplishes by moving to the other side of the bed and gently tugging at the bed sheets?
3. How does Mary get to Phil’s main fear or worry?
NOTES:
NOTES:
13© 2010, Mount Sinai Hospital, Toronto, Canada
Amanda Cooper ScenarioAmanda Cooper is a married woman in her 40s. She is the mother of five.
Yesterday, Amanda was shopping when she began to feel weak and her vision went black. She was then brought to the ER where they did a neurological workup and determined that she had a Transient Ischemic Attack (TIA) –“mini stroke”.
Amanda has been sick her whole life and is a seasoned consumer of healthcare services. She had rheumatic fever as a child and has been diagnosed with mitral valve stenosis. She is on Coumadin because they told her she has thick blood and she needed it for her heart. The medical team is doing a diagnostic workup including blood work, electrocardiogram and MRI of the head. There is nothing conclusive at this point and the working diagnosis is still a TIA.
Mike is meeting Amanda Cooper for the first time. As you watch the scenario, observe not only what Mike and Amanda are saying, but also observe the non-verbal communication. As you watch the scenario, have a copy of the anxiety scale with you and score each of the categories: anxious mood, fears, trouble thinking, tension, sleep problems. There may be some categories that Mike does not assess. Think of the questions you might ask Amanda to obtain all the necessary information.
Amanda Video Clip 1The narrator will now guide you through the scoring of the anxiety tool and a series of reflective questions based on the video clip you just watched. There will be a pause after each question during which time you can jot down your responses.
QUESTIONS:
1. Based on your scoring of the anxiety assessment tool, is Amanda’s anxiety low, moderate or high?
2. What is the rationale for your scoring on the anxiety tool?
3. Amanda is anxious as soon as Mike walks in? What are the signs of her anxiety?
4. What do you observe in Mike’s non-verbal communication?
NOTES:
Independent Learner Program
iCAMIRA Facilitator’s Resource Manual
14 © 2010, Mount Sinai Hospital, Toronto, Canada
5. Mike tells Amanda to calm down. What impact does that have on her anxiety?
6. Does Mike do anything to decrease Amanda’s anxiety?
Amanda Video Clip 2The narrator will now guide you through the scoring of the anxiety tool and a series of reflective questions based on the video clip you just watched. There will be a pause after each question during which time you can jot down your responses.
QUESTIONS:
1. Based on your scoring of the anxiety assessment tool, is Amanda’s anxiety low, moderate or high?
2. What is the rationale for your scoring on the anxiety tool?
3. What does Mike say and do to help decrease Amanda’s anxiety?
4. Is the deep-breathing exercise effective with Amanda?
NOTES:
NOTES:
3 - Information Sheet: Breathing Exercises
4 - Information Sheet: Relaxation Techniques
15© 2010, Mount Sinai Hospital, Toronto, Canada
Narrator Script for Rose Hatfield
Rose Video Clip 1QUESTION:
Based on your scoring of the anxiety assessment tool, is Rose’s anxiety low, moderate or high?
DISCUSSION:
Rose’s anxiety would be assessed as low.
f Rose appears very minimally anxious, so that would score a 0.
f She expresses a slight fear with regards to being ill and perhaps losing her job, so this would be scored as a 1.
f Trouble thinking wasn’t directly assessed, but Rose does not appear to be having any difficulties with this, so would score a 0.
f There is some tension in her face so depending on interpretation would be a 0 or 1.
f She clearly indicates difficulty with sleep so this would score a 2.
f Total score is 3 or 4, which suggests low anxiety.
QUESTIONS:
What strategies does Jill use to engage Rose? Does she... seek information? ... ask open-ended or directive questions? ... use touch and appropriate
personal space? What do you notice about Jill’s non-verbal communication?
DISCUSSION:
f Jill clearly obtains the information for her assessment by asking questions such as: “How are you sleeping”? “How’s the abdominal pain”? These are considered open-ended questions. This gives Rose the opportunity to respond with a simple yes or no or, if she chooses, go on to elaborate. Although Jill’s focus is clearly on the patient, her facial expression and overall disposition was one of being rushed. As if to say “…I’m here to get the info I need for my assessment, I’ll answer some questions and then I’m moving on.”
Independent Learner Program
iCAMIRA Facilitator’s Resource Manual
16 © 2010, Mount Sinai Hospital, Toronto, Canada
QUESTIONS:How would you describe Rose’s body language? - Is it relaxed or tense? - Does she look worried, anxious, upset?
DISCUSSION:
f Rose’s expression is somewhat strained. She is clearly tense, but not overly anxious.
QUESTION:
What appears to be Rose’s main concern/fear/worry?
DISCUSSION:
f Rose appears to be quite focused on her MRI result and she also has some concern about being in the hospital too long and the implications for her job.
QUESTIONS:
Do you think Jill adequately addressed Rose’s anxiety? Write down why you think so.
Write down if you would have done anything differently to address Rose’s concerns?
DISCUSSION:
f These are subjective questions and meant to stimulate discussion before launching into the second clip.
17© 2010, Mount Sinai Hospital, Toronto, Canada
Rose Video Clip 2QUESTION:
Based on your scoring of the anxiety assessment tool in this second clip, is Rose’s anxiety low, moderate or high?
DISCUSSION:
Rose’s anxiety would be assessed as low.
f Rose appears very minimally anxious so that would score a 0.
f In this interaction Rose does express a fear of an outcome of cancer so this would be scored as a 2.
f Trouble thinking wasn’t directly assessed, but Rose does not appear to be having any difficulties with thinking so would score 0.
f There is some tension in her face so depending on interpretation would be a 0 or 1.
f She clearly indicates difficulty with sleep so this would score a 2.
f Total score is 4 or 5, which suggests low anxiety.
A few words about the assessment tool. The scoring is subjective which is why some categories are scored within a range. It’s very likely that your total score will vary with that of your colleagues. It’s okay if everyone doesn’t end up with exactly the same number. What’s important are the low, moderate and high categories. These categories determine the appropriate interventions for decreasing anxiety.
For this particular interaction, you may be wondering why the fears category is a 2 instead of a 3. Look at the scoring scale. A score of 2 indicates the symptom is obvious, but does not interfere with function. A score of 3 indicates that the symptom is severe enough to be interfering with the patient’s function. In this interaction, it is clear that Rose’s function is not impaired by her fear.
QUESTIONS:
What strategies did Jill use to engage Rose? Does she... seek information? ... ask open-ended or directive questions?
Compared to the first clip how is her use of touch and personal space?
Is Jill’s non-verbal communication different from the first clip and if so, how?
What did this interaction reveal as Rose’s greatest concern or fear or worry?
What did Jill do differently in this interaction to get that information?
Independent Learner Program
iCAMIRA Facilitator’s Resource Manual
18 © 2010, Mount Sinai Hospital, Toronto, Canada
DISCUSSION:
f Jill engages the patient by asking more open-ended questions like, “How are you doing today”? “Is there something else worrying you”? Jill probes a little to get more information about Rose’s focus on the MRI result. She also stands closer to Rose and her tone is a little warmer.
f The other thing Jill does in this clip is communicate a lot of information to Rose. You may be thinking, “what”?!! Jill couldn’t tell Rose anything about her MRI result. It’s true that Jill did not have the actual test result, and even if she did, would not be able to convey the result. That’s not part of her scope of practice. It’s okay to say that you don’t know or you don’t have the results. But don’t stop there. Think about all the information that Jill did tell Rose. She told her how long the result might take and that the doctor would be the one to come in and tell her the result, and that once the result was back, a treatment plan would be developed. We sometimes take these things for granted because we live and breathe these routines everyday. Remember however, that for the patient, hospital procedures and routines, are unfamiliar, and this often gives rise to fears, anxieties and worries.
f At this point, you may think, “The anxiety tool scoring for the two clips is the same.” “What’s the difference between the two clips?”
f Rose is the type of patient that healthcare professionals (HCPs) often describe as the “nice or pleasant” patient. She doesn’t want to disturb anyone or rock the boat. On the surface, her main concern is the MRI result.
f Jill’s interaction with Rose in the first clip is, reasonable. In the second clip however, Jill’s tone of voice is noticeably warmer. She provides Rose with a lot of useful information about the test result process and the availability of services that might be helpful. She observes Rose’s pre-occupation with the MRI result. Jill appropriately takes this as a cue to ask even more open-ended questions. She probes with the question, “Is there something else worrying you”? Sometimes HCPs are wary of asking such pointed questions. Don’t worry; if the patient finds your question too intrusive or doesn’t want to talk, he or she will let you know…and that in itself is a piece of information!
f All of these things help Jill to build trust and rapport with Rose. That trust provides the opportunity for Rose to divulge more about herself. This gives Jill a much clearer picture of why Rose is so worried about the MRI result.
f Our role as HCPs is not just about assessing anxiety and getting a score to document. Our role is to recognize our patients’ anxiety and to try and manage it. Everything Jill did in the second clip to build trust and rapport helped to decrease Rose’s anxiety. Not convinced…go back and watch Rose’s body language at the end of each of the clips…what do you notice? One more thing…Jill’s interaction in the second clip didn’t take much more time than the first clip and overall provided Rose with a better patient experience.
19© 2010, Mount Sinai Hospital, Toronto, Canada
Narrator Script for Phil Archer
Phil Video Clip 1QUESTION:
Based on your scoring of the anxiety assessment tool, is Phil’s anxiety low, moderate or high?
DISCUSSION:
f Using the anxiety assessment tool Phil’s anxiety would be assessed as moderate.
f It’s not clear from this interaction if he has an anxious mood, fears or trouble thinking so all those components would be scored as 0.
f Phil’s hand ringing and lack of eye contact indicate that he is experiencing tension and would be scored as a 2.
f Phil has clearly stated that he has not slept well in hospital. It’s unclear whether this is interfering with Phil’s function and therefore would score a 2.
f Phil’s total score is 4 and therefore a low level of anxiety. Since the assessment has given us no information on the first three categories, we really can’t consider this an accurate reflection of Phil’s level of anxiety.
QUESTIONS:
What strategies does Mary use to engage Phil? Does she... seek information? ... ask open-ended or directive questions?
Describe Mary’s non-verbal communication.
Describe Phil’s non-verbal communication.
DISCUSSION:
f Mary’s tone and facial expression are pleasant. Phil is not making eye contact with Mary and his facial expression appears somewhat put-off or disinterested. Mary seeks information for her assessment by asking questions such as: “How was your sleep last night”? “How’s your foot”? “How are you feeling this morning?” These are open-ended questions.
Independent Learner Program
iCAMIRA Facilitator’s Resource Manual
20 © 2010, Mount Sinai Hospital, Toronto, Canada
QUESTION:
Do you have a sense of Phil’s main concern or fear or worry?
DISCUSSION:
f Based on this interaction, it’s very hard to know what Phil’s main worry is.
QUESTION:
Would you have done anything differently in your interaction with Phil?
DISCUSSION:
f Phil is a gentleman who doesn’t open up easily. He’s not a big conversationalist! Because of this, there may be a tendency for HCPs to “write Phil off” and forget about him, thinking that he doesn’t want to engage. The fact that Phil is asking for Margaret or Jackie indicates that he has engaged with staff in the past. This is cue for Mary.
f Because Phil isn’t a big communicator, he has a lot bottled up and going on in his head. It’s often very hard for this type of patient to answer open-ended questions. They have difficulties focusing on any one problem or concern. So, as HCPs, we need to help focus their thinking. Rather than asking, “How was your sleep last night?”, Mary could ask, “Did you sleep well last night?” Based on Phil’s responses, she could continue to ask more directive questions. This would allow Phil to focus his thinking while at the same time allow for some rapport to develop between Phil and Mary. Another approach would have been for Mary to pick up on Phil’s cue when he responded that he hadn’t been sleeping well in hospital. To ask Phil why he was “having difficulty sleeping”, or “what was interfering with his sleep” would have helped Mary gain a better understanding of Phil.
21© 2010, Mount Sinai Hospital, Toronto, Canada
Phil Video Clip 2 QUESTION:
Based on this interaction, what is your scoring of the anxiety assessment tool for Phil?
DISCUSSION:
f Phil’s anxious mood would score a 1.
f He has a fear of losing his foot and fears the implications for his independence, so the fears category would score a 2.
f The trouble thinking category would be scored a 3 because it is interfering with his function. He can’t remember information given to him by the surgeon and he can’t read the newspaper.
f The ringing of his hands and lack of eye contact indicate a score of 2 for the tension category and sleep would score a 1 or 2.
f Total score is 9 or 10 which indicates a moderate level of anxiety.
Notice in this second clip that Phil is not engaged and he may be upset that familiar nurses are not looking after him. Mary is not put off by this. She attempts to connect with Phil by saying, “I’d like to get to know you better.” Mary also tries to find out more about why Phil hasn’t been sleeping by asking, “What’s up?” This conveys to Phil that Mary is interested and helps to develop rapport.
QUESTION:
What do you think Mary accomplishes by moving to the other side of the bed and gently tugging at the bedsheets?
DISCUSSION:
f In moving to the other side of the bed, Mary placed herself directly in Phil’s line of site, tugged at the bedsheet and asked, “Is there something you’re upset or worried about?” When patients are anxious or worried, they are often not aware of their behaviour. Fidgeting and wringing of hands can indicate anxiety. By picking up on that cue, Mary is making Phil aware of his fidgeting and it also conveys to Phil that Mary is paying attention which further develops rapport.
Independent Learner Program
iCAMIRA Facilitator’s Resource Manual
22 © 2010, Mount Sinai Hospital, Toronto, Canada
QUESTION:
How does Mary get to Phil’s main fear or worry?
DISCUSSION:
f Mary realizes that she is not getting any information from Phil with open-ended questions and so switches to a more direct line of questioning. “Are you worried about your foot, Phil?” There is a possibility that Phil would have answered, “no” and Mary would then need to ask another question. In this case, Phil’s main fear is about his foot and what that might mean for his independence.
f Mary’s interaction in the first clip was reasonable, but incomplete. Recall that 3 of the 5 categories on the anxiety tool were not assessed. Based on the interaction in the second clip, it is clear that spending a bit more time to engage with Phil is very beneficial in getting not only a complete assessment of his level of anxiety, but also a better grasp of Phil’s situation overall. If you can’t recall, view the two clips again and pay attention to Phil’s visibly relaxing in the second clip as compared to the first clip.
f For patient’s like Phil, there are two important points to remember:
1. They need more time to open up and engage which means that as a HCP you may need to return several times to engage in order to develop some rapport
2. Closed or directive type questions will be more effective
f This becomes even more pertinent when the patient is anxious or worried. It may seem counter-intuitive to ask closed or directive type questions because as HCPs, we’re taught to ask open-ended questions. It’s generally a good rule of thumb to start with open-ended questions, and be prepared to move to directive or more close-ended type questions when the open-ended approach doesn’t work.
f So the next time you encounter a Phil-type patient, don’t dismiss them because of their apparent lack of engagement. There’s often a lot going on for these patients. It just takes a little more time and patience as HCPs to find it out.
23© 2010, Mount Sinai Hospital, Toronto, Canada
Narrator Script for Amanda Cooper
Amanda Video Clip 1QUESTION: Based on your scoring of the anxiety assessment tool, is Amanda’s anxiety low, moderate or high?
DISCUSSION:
f Amanda’s anxiety and fears each score a 4. She is completely focused on having a brain tumor and dying.
f Trouble thinking was not clearly assessed, however she is using her laptop which would indicate an ability to concentrate.
f She is not crying or restless, but there is a certain tension in her body so tension could score a 1.
f She does indicate an inability to sleep and so would score at least a 2. It would require a little more probing to get a sense of how much the lack of sleep is contributing to Amanda’s overall anxiety and whether it is interfering with her ability to function.
f Total score is 11 which indicates a high level of anxiety.
QUESTIONS: Amanda is anxious as soon as Mike walks in. What are the signs of her anxiety?What do you observe in Mike’s non-verbal communication?
Mike tells Amanda to calm down. What impact does that have on her anxiety?Does Mike do anything to decrease Amanda’s anxiety?
DISCUSSION:
f With Amanda, it is important to recognize the signs of high anxiety and to try and manage, rather than assess the anxiety. Her level of anxiety is clearly high, as are her fears of a brain tumor and dying.
Independent Learner Program
iCAMIRA Facilitator’s Resource Manual
24 © 2010, Mount Sinai Hospital, Toronto, Canada
f Mike’s body language is one of retreating from Amanda and trying to leave the room as quickly as possible. Telling Amanda to “calm down” just inflames the situation as she does not feel heard or supported. At times, it appears as if Mike is trying to control a bit of a smirk as if to say, “Lady…are you for real?” None of these things help to build rapport with Amanda, nor do they help to decrease her anxiety.
Amanda Video Clip 2QUESTION: Based on your scoring of the anxiety assessment tool, is Amanda’s anxiety low, moderate or high?
DISCUSSION:
f Scoring is the same as clip 1.
QUESTIONS: What does Mike say and do to help decrease Amanda’s anxiety?Is the deep-breathing exercise effective with Amanda?
DISCUSSION:
f In this clip, Mike’s body language is conveying that he is going to stay and not run out of the room. He listens and is supportive. He provides reassurance that the team is trying to figure out what is wrong with her and not keep anything from her in the process. Note Amanda’s response and visible change in presentation when Mike says, “Anyone in your position would be worried.” She is relieved by his normalizing statement, which conveys acknowledgement and support. Similar to the Rose scenario, Amanda has questions that Mike can’t completely answer, yet he provides what information is available. Amanda’s anxiety visibly decreases some more when Mike says, “Now I heard you mention a stroke and a TIA. These are not the same thing…” Listening, understanding and providing some information all build trust with Amanda, and help to decrease her anxiety.
3 - Information Sheet: Breathing Exercises
4 - Information Sheet: Relaxation Techniques
25© 2010, Mount Sinai Hospital, Toronto, Canada
f In this instance, the deep-breathing exercise is not very effective. It’s always worth a try, as some patients find it very effective. Remember that you can also print out the instruction sheet and leave it with your patient. Even a patient as anxious as Amanda might do the exercise on their own after the healthcare professional has left the room.
f Similar to the Rose scenario, you may be saying to yourself, “The anxiety tool scoring for the two clips is the same.” “What’s the difference between the two clips?”
f In the first clip, Mike is challenged by Amanda’s high affect and anxiety. His body language and tone of voice convey to Amanda that she is not being taken seriously and that Mike can’t wait to leave the room. For Amanda, who is looking for answers and some re-assurance that she’s not dying, Mike’s interaction does nothing to decrease her anxiety.
f In the second clip, Mike is fully present; not retreating. This is very important in building an initial connection with Amanda. Mike listens and conveys understanding for Amanda’s situation. He provides re-assurance that the team is not avoiding her and provides as much information as he can to allay her fears. As you saw in the second clip, all of these things decreased Amanda’s anxiety.
f The challenge for HCPs is to find a way to tolerate Amanda’s affect. If the HCP just keeps leaving the room (as in the first clip), Amanda’s anxiety will not be addressed and in fact will continue to increase, which will probably lead to her constantly ringing the call bell.
f It’s tempting to label patients like Amanda as histrionic or “over-the-top”. They are often viewed as “difficult or needy”. HCPs need to manage their own discomfort with this high affect. Start by recognizing the patient distress. Use your colleagues for support, have a care plan for consistency and be aware of your own triggers.
f Our role as HCPs goes beyond assessing for anxiety and getting a score to document. Our role is to recognize our patients’ anxiety and to try and manage it. Everything Mike did in the second clip to build trust and rapport helped to decrease Amanda’s anxiety. One more thing that bares repeating…Mike’s interaction in the second clip didn’t take a lot more time than the first clip and overall provided Amanda with a better patient experience!
Independent Learner Program
iCAMIRA Facilitator’s Resource Manual
26 © 2010, Mount Sinai Hospital, Toronto, Canada
Scenario Summary Points
Now that you have seen and reflected upon all three scenarios, let’s summarize the key points.
1. Engaging your patients and developing rapport helps them feel cared for and will help decrease their anxiety.
2. Engaging your patients and developing rapport improves the patient care experience and gives you more job satisfaction.
3. Recall from the scenarios that it really didn’t take a lot more time to engage and do a good assessment of the patient’s anxiety. Remember that an extra minute can make a big difference in decreasing your patient’s anxiety and actually save you a lot of “responding to call-bell” time in the end.
4. Be aware of “cues” from the patient and don’t be afraid to ask questions rather than trying to guess what the cues mean. The cues may be verbal or non-verbal.
5. Each patient is different. Use the different communication techniques you’ve learned to connect with your patient.
6. The anxiety assessment tool provides you and your colleagues with a common language with which to communicate about patient anxiety. It is a subjective tool, so not everyone will have exactly the same score. What are important are the categories of low, moderate and high. It is these categories that determine the appropriate interventions.
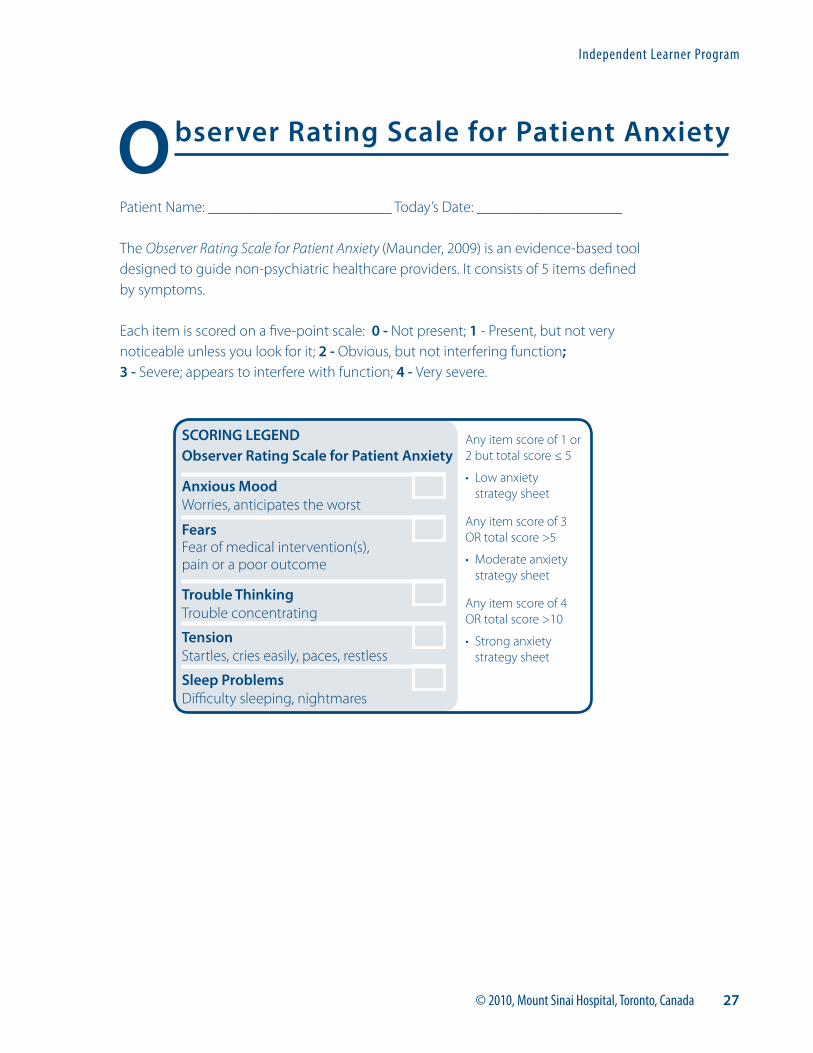
27© 2010, Mount Sinai Hospital, Toronto, Canada
Patient Name: ________________________ Today’s Date: ___________________
The Observer Rating Scale for Patient Anxiety (Maunder, 2009) is an evidence-based tool designed to guide non-psychiatric healthcare providers. It consists of 5 items defined by symptoms.
Each item is scored on a five-point scale: 0 - Not present; 1 - Present, but not very noticeable unless you look for it; 2 - Obvious, but not interfering function; 3 - Severe; appears to interfere with function; 4 - Very severe.
Observer Rating Scale for Patient Anxiety
Anxious Mood Worries, anticipates the worst
Fears Fear of medical intervention(s), pain or a poor outcome
Trouble Thinking Trouble concentrating
Tension Startles, cries easily, paces, restless
Sleep Problems Difficulty sleeping, nightmares
SCORING LEGENDObserver Rating Scale for Patient Anxiety
Any item score of 1 or 2 but total score ≤ 5
• Low anxiety strategy sheet
Any item score of 3 OR total score >5
• Moderate anxiety strategy sheet
Any item score of 4 OR total score >10
• Strong anxiety strategy sheet
Independent Learner Program
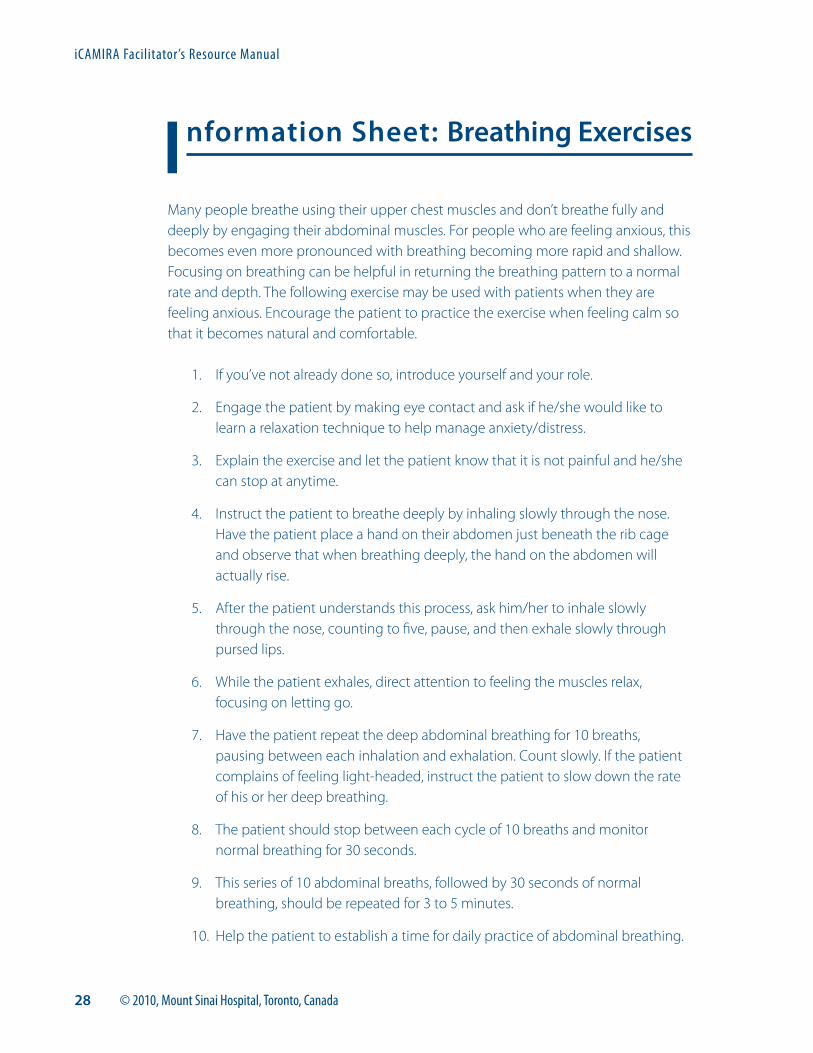
iCAMIRA Facilitator’s Resource Manual
28 © 2010, Mount Sinai Hospital, Toronto, Canada
Many people breathe using their upper chest muscles and don’t breathe fully and deeply by engaging their abdominal muscles. For people who are feeling anxious, this becomes even more pronounced with breathing becoming more rapid and shallow. Focusing on breathing can be helpful in returning the breathing pattern to a normal rate and depth. The following exercise may be used with patients when they are feeling anxious. Encourage the patient to practice the exercise when feeling calm so that it becomes natural and comfortable.
1. If you’ve not already done so, introduce yourself and your role.
2. Engage the patient by making eye contact and ask if he/she would like to learn a relaxation technique to help manage anxiety/distress.
3. Explain the exercise and let the patient know that it is not painful and he/she can stop at anytime.
4. Instruct the patient to breathe deeply by inhaling slowly through the nose. Have the patient place a hand on their abdomen just beneath the rib cage and observe that when breathing deeply, the hand on the abdomen will actually rise.
5. After the patient understands this process, ask him/her to inhale slowly through the nose, counting to five, pause, and then exhale slowly through pursed lips.
6. While the patient exhales, direct attention to feeling the muscles relax, focusing on letting go.
7. Have the patient repeat the deep abdominal breathing for 10 breaths, pausing between each inhalation and exhalation. Count slowly. If the patient complains of feeling light-headed, instruct the patient to slow down the rate of his or her deep breathing.
8. The patient should stop between each cycle of 10 breaths and monitor normal breathing for 30 seconds.
9. This series of 10 abdominal breaths, followed by 30 seconds of normal breathing, should be repeated for 3 to 5 minutes.
10. Help the patient to establish a time for daily practice of abdominal breathing.
Information Sheet: Breathing Exercises
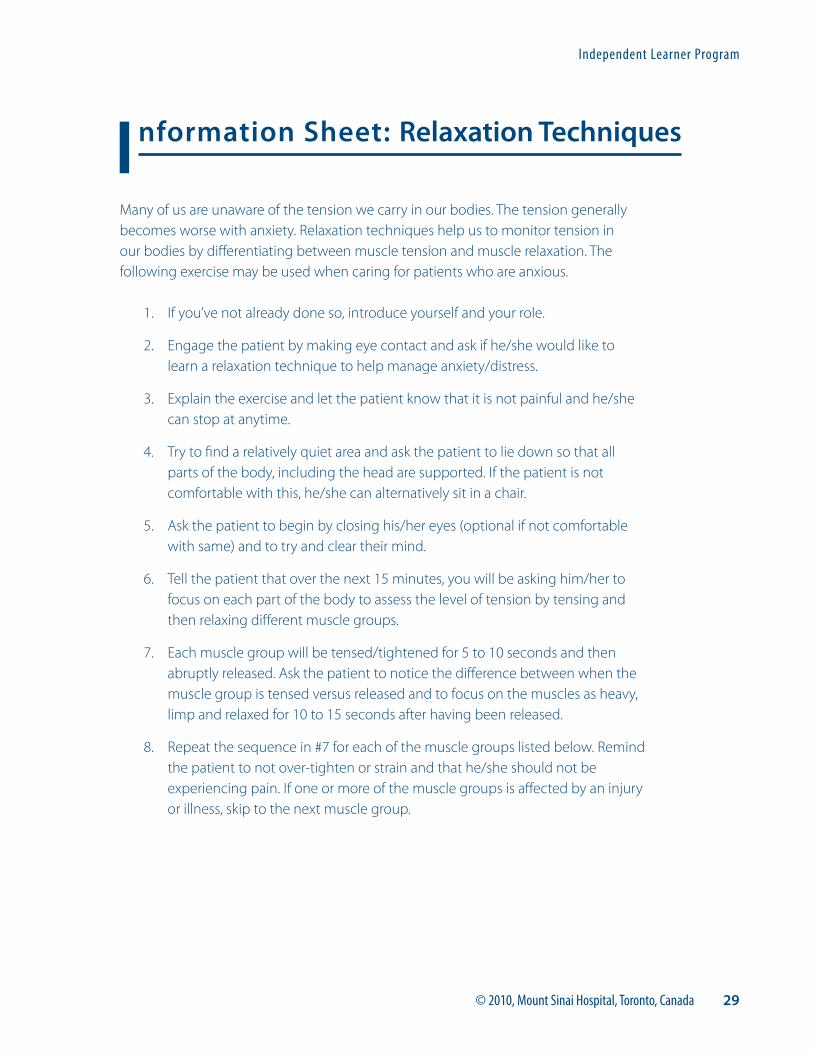
29© 2010, Mount Sinai Hospital, Toronto, Canada
Many of us are unaware of the tension we carry in our bodies. The tension generally becomes worse with anxiety. Relaxation techniques help us to monitor tension in our bodies by differentiating between muscle tension and muscle relaxation. The following exercise may be used when caring for patients who are anxious.
1. If you’ve not already done so, introduce yourself and your role.
2. Engage the patient by making eye contact and ask if he/she would like to learn a relaxation technique to help manage anxiety/distress.
3. Explain the exercise and let the patient know that it is not painful and he/she can stop at anytime.
4. Try to find a relatively quiet area and ask the patient to lie down so that all parts of the body, including the head are supported. If the patient is not comfortable with this, he/she can alternatively sit in a chair.
5. Ask the patient to begin by closing his/her eyes (optional if not comfortable with same) and to try and clear their mind.
6. Tell the patient that over the next 15 minutes, you will be asking him/her to focus on each part of the body to assess the level of tension by tensing and then relaxing different muscle groups.
7. Each muscle group will be tensed/tightened for 5 to 10 seconds and then abruptly released. Ask the patient to notice the difference between when the muscle group is tensed versus released and to focus on the muscles as heavy, limp and relaxed for 10 to 15 seconds after having been released.
8. Repeat the sequence in #7 for each of the muscle groups listed below. Remind the patient to not over-tighten or strain and that he/she should not be experiencing pain. If one or more of the muscle groups is affected by an injury or illness, skip to the next muscle group.
Information Sheet: Relaxation Techniques
Independent Learner Program
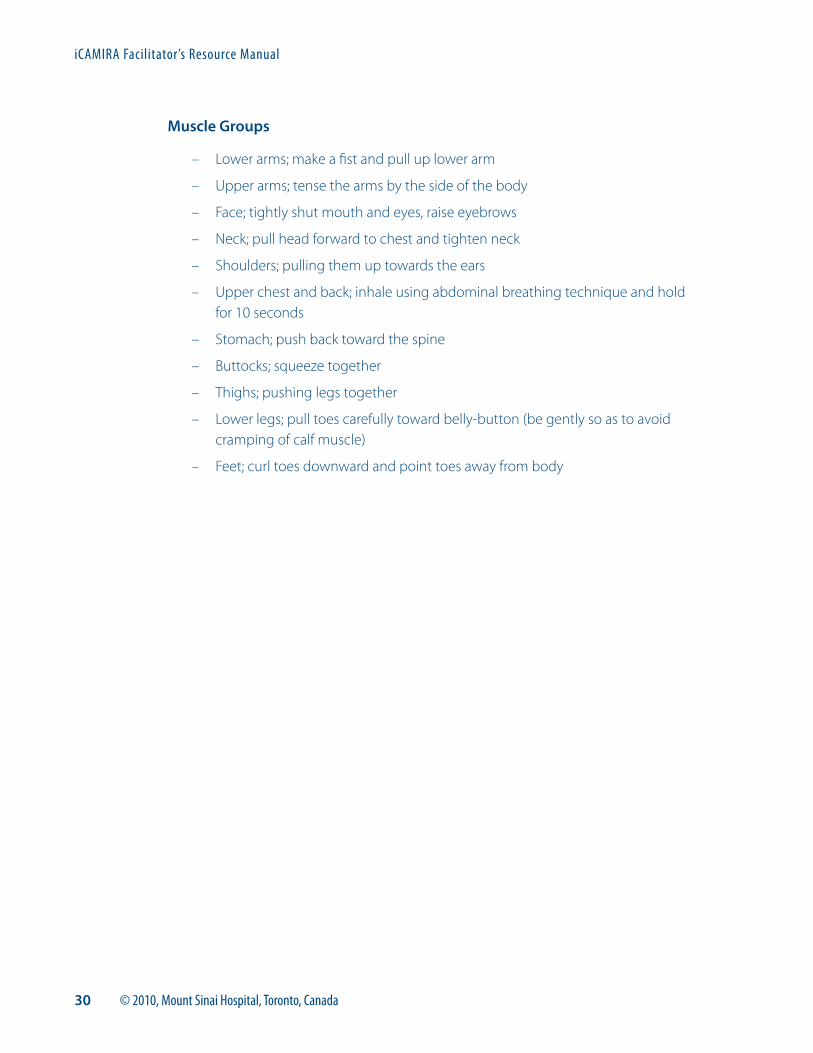
iCAMIRA Facilitator’s Resource Manual
30 © 2010, Mount Sinai Hospital, Toronto, Canada
Muscle Groups
– Lower arms; make a fist and pull up lower arm
– Upper arms; tense the arms by the side of the body
– Face; tightly shut mouth and eyes, raise eyebrows
– Neck; pull head forward to chest and tighten neck
– Shoulders; pulling them up towards the ears
– Upper chest and back; inhale using abdominal breathing technique and hold for 10 seconds
– Stomach; push back toward the spine
– Buttocks; squeeze together
– Thighs; pushing legs together
– Lower legs; pull toes carefully toward belly-button (be gently so as to avoid cramping of calf muscle)
– Feet; curl toes downward and point toes away from body
37© 2010, Mount Sinai Hospital, Toronto, Canada
References
1. Sherbourne, C.D., et al. (1994). Prevalence of comorbid anxiety disorders in primary care outpatients. Archives of Family Medicine, 5(1), 27-34.
2. Stoudemire, A. (1996). Psychiatry in medical practice. Implications for the education of primary care physicians in the era of managed care: Part 1. Psychosomatics, 37(6), 502-508.
3. Bohachick, P. (1984). Progressive relaxation training in cardiac rehabilitation: Effect on perceptions of challenges, control, competition and collaboration in Ontario’s evolving healthcare system. Healthc Q., 8(3), 36-47.
4. Lawlis, G.F., et al. ( 1985). Reduction of postoperative pain parameters by pre-surgical relaxation instructions for spinal pain patients. Spine, 10(7), 649-651.
5. Frazier, S.K., et al. (2002). Management of anxiety after acute myocardial infarction. Heart and Lung: The Journal of Acute and Critical Care, 31(6), 411-420.
6. Saravay, S., et al. (1996). Four-year follow-up of the influence of psychological comorbidity on medical rehospitalisation. American Journal of Psychiatry, 153(3), 397-403.
7. Walker, F.B., et al. (1987). Anxiety and depression among medical and surgical patients nearing hospital discharge. Journal of General Internal Medicine, 2(2):99-101.
8. Simon, E.P., et al. (1995). Delivery of home care services after discharge: what really happens. Health and Social Work, 20(1):5-14.
9. Creed, F., et al. (2002). Depression and anxiety impair health-related quality of life and are associated with increased costs in general medical inpatients. Psychosomatics, 43(4):302-309.
10.Moser, D.K. (2002). Psychosocial factors and their association with clinical outcomes in patients with heart failure: Why clinicians do not seem to care. European Journal of Cardiovascular Nursing, 1(3):183-8.
11. Burman, M.E., et al. (2005). Treatment practices and barriers for depression and anxiety by primary care advanced practice nurses in Wyoming. Journal of the American Academy of Nurse Practitioners, 17(9):370-80.
References
iCAMIRA Facilitator’s Resource Manual
38 © 2010, Mount Sinai Hospital, Toronto, Canada
12.Sheldon, L.K., et al. (2008). Putting evidence into practice: evidence-based interventions for anxiety. Clinical Journal of Oncology Nursing, 12(5):789-97.
13.Brown, A.D., et al. (2008). Comparing patient reports about hospital care across a Canadian-US border. International Journal of Quality in Healthcare, 20(2), 95-104.
14.Maunder, R.G. (2009). [Observer Rating Scale for Patient Anxiety]. Unpublished raw data.
15.Hamilton, M. (1959). The measurement of anxiety states by rating. British Journal of Medical Psychology, 32, 50-55.
16.Gaba, D.M. (2004). The future vision of simulation in healthcare. Quality Safe Healthcare, 13 (Suppl 1);i2-i10.
17.Nishisaki, A., et al. (2007). Does patient simulation improve patient safety, self-efficacy, operational performance and patient safety. Anesthesiology Clinics, 25:225-236.
18. Johnson, J.A., et al. (1996). Effectiveness of standardized patient instruction. Journal of Dentistry Education, 60(3):262-66.
19.Estrada, C.A., et al. (1997). Positive affect facilitates integration of information and decreases anchoring in reasoning among physicians, Organizational Behaviour and Human Performance, 72:117–135.
20.Blue, A.V., et al. (1998). The effectiveness of the structured clinical instruction module. American Journal of Surgery, 176(1):67-70.
21.Madan, A.K., et al. (1998). Comparison of simulated patient and didactic methods of teaching HIV risk assessment to medical residents. American Journal of Prevention Medicine, 15(2):114-9.
22.Aspegren, K. (1999). How to get the best physicians? Admission procedure and education must cooperate. Lakartidningen, 96(36):3742-3.
23. Isenberg, S.B., et al. (2005). Features and uses of high-fidelity medical simulations that lead to effective learning: A BEME systematic review. Medical Teacher, 27:10-28.