Embed Size (px)
Citation preview

Expert Behavior Change in Response to Best Practice Changes:
Evidence from Obstetrics∗
Emily Oster, Brown University and NBER
December, 2018
Abstract
Guidelines for best practices in medicine change frequently. In this paper, I analyze to whatextent such changes alter practice patterns and whether adoption of best practices differentiallyaffects some patient groups. I consider these questions in the context of changes in practiceguidelines in obstetrics. I find, first, that practice patterns do respond to new information, mostnotably to new research. Such response are slow, however, and do not seem to be sped up bychanges in official organizational guidelines. I suggest that media coverage is an important part ofcatalyzing behavior change, even in this setting where the changes come from experts. Changesin practice are faster for more advantaged groups of patients. Related to this, I find evidencethat changes occur more quickly for infants who are otherwise healthier, even conditional onobservable features. I connect this last point to challenges in learning about the impacts of thesepractices. The results overall suggest practice changes would be faster if they were more widelypromoted, and this might especially benefit infants who are otherwise disadvantaged.
1 Introduction
To what extent do doctors respond to changes in treatment guidelines by changing their practice
patterns? Do some change their behavior more quickly than others, implying that some patients
benefit first from improved treatment?
Practice guidelines in medicine change frequently (see, for example, changes in treatment thresh-
olds for high blood pressure (Kristensen et al”
2014; Jackson et al, 2008; Gu et al, 2012) or changes
∗James Okun, Jason Goettisheim and Cathy Yue Bai provided outstanding and crucial research assistance. I amalso grateful to Valeria Zurla and Lauren To.
1

in antibiotic prescribing guidelines for children (Arroll and Kenealy, 2005; Sakulchit and Goldman,
2017), making these important questions for understanding treatment quality.
Changes in guidelines have some parallels to changes in technology, a topic in which economists
have long been interested, beginning with the classic Griliches (1957) work on hybrid corn, and
with many examples in the area of health (e.g. Skinner and Staiger, 2005; Freedman, Lin and
Simon, 2015; Gold et al, 2014; Chandra, Cutler and Song, 2011). A key difference between practice
changes and technology changes is the potential speed. In the case of new technology, adoption
often requires learning about an unfamiliar procedure or practice, and possibly investing in new
capital equipment. In contrast, many of the best practice changes simply change the recommended
balance of procedures, or the threshold for some prescription or treatment. As a result, the only
significant barriers to adoption are learning the information and reacting to it. In principle, changes
could be immediate.
In this paper I address the question of how medical practitioners respond to different types of
information in changing treatment patterns, focusing on obstetrics. Accepted best practices around
childbirth have evolved considerably even in the past two decades, and there may be considerable
welfare gains to improved practices, given that US outcomes for mothers and babies lag the rest of
the world (National Research Council, 2013; Chen, Oster and Williams, 2016).
I analyze the patterns of behavior around four medical decisions which are common during
childbirth: (1) whether to attempt a vaginal birth after cesarean section (VBAC); (2) whether to
deliver a breech baby by planned cesarean section; (3) use of vacuum extraction for vaginal birth;
and; (4) whether to discourage elective labor induction at 37 or 38 weeks of gestation.
The paper has two primary goals. The first is to analyze how these practices have changed
over time, and connect changes to new information or other events. The second is to explore
heterogeneity in the speed of response across groups of patients. Both analyses make use of the
Natality Detail Files, which contain detailed microdata on all births in the United States over time.
Focusing on the first question, I find that there are significant changes in all four behaviors
over time, and they do seem to reflect responses to changes in best practices. These responses are,
however, slow. During this period there are two major research findings - on VBAC and breech
delivery - which do change practice, but over a period of years, not months. I find limited evidence
that changes in official guidelines increase this speed of change.
Notably, there is one example of a sharp and sustained decline in behavior - a large drop in the
use of vacuum extraction over a one month period in 1999. This appears to be a result not, however,
2

of important changes in knowledge but instead a reaction to an episode of the show 20/20.
The slow change has welfare consequences. If new practices achieve (as we expect) better
outcomes, then faster change would benefit more patients. The slow change also opens the related
question of whether some patients systematically benefit from new information first.
The technology adoption literature has been quite interested in variation across space in adop-
tion (e.g. Skinner and Staiger, 2005), so I also begin with this question. In practice in this case I
see very little evidence of variation across space. Although the levels of the behaviors differ across
space, the trends are the same.
Turning to demographics, however, there is evidence that changes in behavior are experienced
differentially by different patients. More specifically, it appears that the changes in behavior initially
benefit more positively selected patients. The changes occur more slowly for groups who have,
on average, worse birth outcomes - in particular, African-American mothers and those with less
education. To give one example of this, prior to the change in VBAC recommendations in 1996
those with less than a high school education were slightly less likely to have a VBAC than those
with more education. By 2005 they were 3 percentage points more likely.
I use regression evidence to show that the selection gradient with respect to race and education
moves systematically along with the level of the behavior. Further, I show similar conclusions when
I focus on predicted mortality - predicted based on demographics - rather than race or education
as the selection variable. In summary, the benefits of new information seem to accrue to mothers
and infants in groups who are initially more advantaged.
I extend this point to show that selective behavior change favors better-off infants even condi-
tional on demographics. Specifically, I explore whether the relationship between infant outcomes
and the treatment varies with recommendations; I find that it does. To continue the VBAC exam-
ple: after the change in recommendation, those infants born by VBAC have a lower APGAR score,
relative to the difference before, even conditional on their observables. This suggests that there is
also negative selection of behavior change on unobservables. This is true for all four behaviors, and
when I consider infant mortality as the outcome rather than APGAR score.
Aggregating these facts paints a consistent overall picture. Despite the fact that these changes
could be made quickly and universally, I see patterns similar to technology adoption: slow diffusion
of change, with the earlier changes benefiting the better off patients. This suggests that it might
be possible to do more to encourage faster changes, and doing so would benefit more vulnerable
patients. Although it seems surprising since the actors here are experts, the evidence suggests that
3

media attention may be a way to prompt more significant and faster changes.
As a final note, the last piece of evidence on the changes in relationship with infant outcomes
over time relates to the general issue of dynamic selection which I explore elsewhere. Oster (2018)
focuses on consumer health recommendations and shows that changes in these recommendations
can generate dynamic selection, with otherwise healthier consumers adopting newly recommended
behaviors first, changing the apparent relationship between the behavior and health. The results
here show a similar dynamic occurs even with expert decision-makers. Similar to the central point
in that paper, these dynamic changes have the potential to make it more difficult to learn about
relationships in the data.
This paper relates closely to the literature on health technology adoption. I focus in particular
on the role of different types of information in driving changes in behavior. A large literature looks at
other drivers, including (among others) peer effects, hospital structure and insurance policy (Burke,
Fournier and Prasad, 2007; Bradley et al, 2006; Gold et al, 2014; Bokhari et al, 2008; Freedman,
Lin and Simon, 2015; Sacarny, 2014; Domino, 2012; Agha and Molitor, 2018; Smieliauskas, 2011;
Yu, 2015).
The analysis also relates to a smaller literature, primarily in medicine, on how doctors respond
to changes in practice guidelines. Notable here are a number of papers on response to changes in
hypertension and statin prescribing guidelines (Kristensen et al”
2014; Jackson et al, 2008; Gu et
al, 2012; Ma et al, 2006; Pauff et al, 2015). These papers tend to find doctors do respond to changes
in prescribing guidelines, although they do not focus on heterogeneity across patient types.
Finally, I relate to a large literature on understanding use of interventions in obstetrics, perhaps
most notably papers on differential use of cesarean sections across patient types (i.e. Johnson and
Rehavi, forthcoming).
The rest of the paper is organized as follows. Section 2 describes the background on the changes
in practice guidelines, and the data I use. Section 3 shows results on changes in practice patterns
over time. Section 4 shows the evidence on heterogeneity and Section 5 concludes.
2 Background and Data
This section begins by describing the context for each of the procedures I consider, and briefly
reviewing the changes in recommendations. In the second subsection I describe the data used in
the analysis.
4

2.1 Background on Contexts Considered
There are four practices considered here: (1) vaginal birth after cesarean section; (2) delivery
method for breech births; (3) use of vacuum extraction for vaginal birth and; (4) elective labor
induction at 37 or 38 weeks of gestation (“early term”).
Vaginal Birth after Cesarean (VBAC)
Vaginal birth after cesarean (VBAC) refers to the case in which a woman who has previously
delivered a child by cesarean section delivers vaginally a subsequent birth. In 1988, the American
College of Obstetricians and Gynecologists (ACOG) recommended VBAC as an option for prior
cesarean patients. In 1996, however, a large study (McMahon et al, 1996) suggested outcomes were
better with planned cesarean section in the case of a prior cesarean. Following this, in 1998 an
ACOG bulletin cautioned that VBAC should only be attempted at hospitals readily equipped to
provide emergency care in the case of uterine rupture. ACOG bulletins after 1998 continued to
focus on the risks of VBAC and the necessity of immediately available emergency cesarean sections.
Breech Delivery
Most infants are head down in the uterus at the time of labor and delivery, a position referred to
as “vertex presentation.” Breech presentation, in contrast, refers to a case where the infant is in
another position, typically either feet down or butt down. Some breech babies can be delivered
vaginally, but it is a more complex birth procedure. In 2000, results of a large trial (TERM-
BREECH) suggested that outcomes for breech infants were better with a planned cesarean section
than a trial of vaginal birth (Hannah et al, 2000). In 2001, ACOG followed this with a bulletin
which recommends cesarean sections for breech births. They note that most physicians are not
experienced in vaginal breech births and that vaginal birth is generally not appropriate for this
position of the fetus.
Vacuum Extraction
Vacuum extraction is a method to assist in the delivery of a baby using a vacuum device which
attaches to the child’s head. It is used in the second stage of labor if the infant appears to be
stuck. Vacuum extraction has been variously recommended and rejected over time. In 1994,
ACOG released a bulletin that detailed the qualifications for vacuum extraction and encouraged it
5

under appropriate circumstances. However, in 1998, the FDA released a report on the dangers of
vacuum extraction, citing reports of deaths, which was followed by significant negative press. Back
in the other direction, subsequent ACOG opinions and bulletins reaffirmed the safety of vacuum
extraction and noted that complications are rare. The widely used alternative to vacuum extraction
is cesarean section.
Redefinition of “Full Term Pregnancy”
On average, a pregnancy lasts 40 weeks, and a full-term pregnancy has generally been considered
to be any delivery that falls between 37 and 42 weeks. A baby born before 37 weeks is considered
premature. However, in 2013, ACOG redefined full-term to be between 39 and 40 weeks, and
divided full term pregnancies into four categories: early-term (37 to 38 weeks), full-term (39 to 40
weeks), late-term (41 to 42 weeks), and post-term (more than 42 weeks). This had implications for
induced labor, as part of the change was to discourage elective induction in the “early term” period.
2.2 Data
The primary data source in this paper is the US Natality Detail Files, from the National Center
for Health Statistics (NCHS). The analysis uses both linked birth-death files and, where those are
not available, birth files only. For most treatments I focus on the period from 1995 through 2005,
where we have consistently coded information on treatments and demographics and during which
time most of the major changes occur. For the redefinition of term pregnancy I extend the data
through 2015.
The NCHS files are a Census of births in the United States based on birth and death certificates
filed in vital statistics offices in all States and the District of Columbia. The data provides infor-
mation on infant death within a year of birth (through 2009), various demographic characteristics
such as race, age and level of education, the health of both mother and child post-partum, and
physician practices carried out during labor.
In most cases it is necessary to recode variables to capture the outcomes of interest. The VBAC
variable takes the value 1 if the infant is delivered vaginally when the mother had delivered another
infant by cesarean and 0 if the infant was delivered by other means and the mother previously
had a cesarean delivery. The breech delivery variable is 1 if the infant is breech presenting and is
delivered by cesarean section and 0 if the infant is breech presenting and delivered vaginally. For
vacuum extraction, the indicator variable is 1 if a vacuum delivery is performed and 0 otherwise.6

Lastly, the early term birth variable takes the value 1 if the infant is delivered between 37 and 38
weeks, inclusive, and 0 if the birth occurs after 38 weeks. Births before 37 weeks are excluded from
this analysis. Table 1 presents summary statistics on treatments, demographics and outcomes.
3 Evidence on Changes Over Time
This section reports the initial results on changes in practice patterns over time.
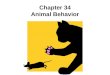
Figure 1 shows the evolution of each procedure over time. There are four sub-figures, each
corresponding to one of the outcomes and showing the monthly means of behavior. Vertical lines
in the figures indicate major research studies, ACOG bulletins or opinions and other events. Table
2 lists the changes in recommendations indicated by the vertical lines.
Below, I discuss these figures in turn.
Vaginal Birth after Cesarean
The trends over time for vaginal birth after cesarean (VBAC) are shown in Figure 1a.
Broadly, this outcome is trending down over time. In the first year of the data - 1995 - the series
shows little trend and the mean is around 27%. To interpret, this implies that of women who had
a prior cesarean section, 27% of them went on to deliver a second pregnancy vaginally. By 2005,
however, only about 7% of women with a prior cesarean section are delivering vaginally.
The change appears to be precipitated by McMahon et al (1996), which indicated that major
maternal complications were almost twice as common for trial of labor after cesarean than for a
repeat cesarean.
The overall changes in this behavior are large. It is notable, however, that they are slow to
diffuse, despite the fact that practitioners were clearly familiar with the procedures required at the
time the change was made. Notable also is that the two official statements from the American
College of Obstetricians and Gynecologists (ACOG) - in 1998 and 1999 - seem to have had little
effect, changing neither the level nor the trend. Both statements echoed the 1996 paper and urged
repeat cesarean sections rather than VBAC in most cases. To the extent that the goal of these
guidelines was to increase the speed with which changes were made, the data does not show strong
evidence of that.
7

Breech Delivery Method
Figure 1b shows the share of breech births delivered by cesarean section.
This series is initially flat, or trending slightly down, and then begins trending up over time in
the 2000s. There is one sharp spike downwards, but overall the trend is towards universal use of
cesarean section for breech deliveries. The changes over time seem, again, to be related to the timing
of research findings. In 2000, researchers published the first results from the TERM-BREECH trial,
a large randomized trial of delivery methods for breech births (Hannah et al, 2000). The authors
concluded that short-term outcomes for breech infants were better after a planned cesarean section
than after a planned vaginal birth.
Similar to the case of VBAC, these findings do seem to prompt an upward trend in the use of
cesarean delivery although, again, the change is not sudden. Later changes in ACOG guidelines,
published in 2001, reinforced the preference for cesarean section for breech delivery. Again, similar
to VBAC, these do not seem to cause a change in level or trend.
In 2003, an abstract (Hannah et al, 2003) was released with follow-up data from the TERM-
BREECH trial. This later follow-up was somewhat more reassuring about the outcomes for the
planned vaginal birth group, showing no differences in outcomes after two years. This seems to
cause a short term revision in the use of cesarean section for breech deliveries, although this is very
short lived.
Vacuum Extraction
Figure 1c shows the share of births in which vacuum extraction is used, over time.
This figure has a sharp decline in the middle - over a one month period in 1999 there is a one
percentage point drop in the use of vacuum extraction in births, from a base of about 6%. This
continues, and is continued by, a downward trend.
The downward trend in use of this procedure seems to begin with a 1998 FDA report suggesting
there were significant dangers to using vacuum extraction, including the possibility of infant injury
or death. This alert was sent to all practitioners. The report begins a period of decline for this
procedure, which had until then been trending upwards. The report does not, however, cause an
immediate spike down. Indeed, the spike down does not coincide with any specific official events.
The timing is, however, consistent with the drop resulting from a sensationalist episode of the
TV news program “20/20” which focused on the risks of vacuum extraction for babies, and featured
8

graphic images of injured or deceased infants. The news program was motivated by some of the
earlier findings from the FDA, but the timing is clearly later. This program aired at the very end
of January, 1999. While it is difficult to prove the two events are linked, we do not see any other
events which line up in terms of timing.
It is notable that there are a number of information shocks which supported the use and safety
of vacuum extraction. These include an ACOG bulletin in 1998 (the second dotted line) and a
significant review study release in 1999 (Towner et al, 1999). Both argued for the safety of vacuum
extraction. Towner et al (1999), for example, showed similar rates of infant injury for use of vacuum,
forceps or cesarean section.
These releases do not seem to have any impact on stemming the reduction in use of vacuum.
The downward trend continues through these releases.
Early Term Birth
Finally, I consider Figure 1d, which shows changes in the rate of early term delivery over time. This
graph is limited to the universe of infants who were born at or after 37 weeks of pregnancy, and
it shows the share of these births which were at 37 or 38 weeks. This share is increasing until the
mid to late 2000s and then declines. This slow decline is hard to trace to any particular event; it
seems, rather, to reflect a growing consensus over this period that early term births result in worse
outcomes than later term births (Reddy, Ko and Willinger, 2006; Engle and Kominiarek, 2008;
Fleischman, Oinuma and Clark, 2010).
In 2013, ACOG issued concrete guidelines around these issues - specifically, classifying 37 or 38
weeks as “early term” rather than “full term” as an approach to making clear that deliveries should
wait for 39 weeks. The timing of this release is shown in the figure. Again, we see no evidence of
an acceleration of change. If anything, the decline in early term births which had been continuous
up to that point is arrested, and the trend flattens, after the change in guidelines.
Discussion
Visually, Figure 1 makes clear that these practices do change over time and the discussion above
shows that, at least to some extent, these changes appear to be a response to changes in best
practice.
Notably and unsurprisingly, we find that major research studies - in particular, those on VBAC
and breech delivery - do play a significant role in catalyzing change. However, this information9

does not seem to result in immediate changes. It takes years for the decline in the VBAC rate to
taper off. If the appropriate level of this treatment is (say) 7% – where it stabilizes – there is a full
decade in which a faster decline would have been feasible.
One natural approach to speeding up adoption is to change official guidelines to reinforce study
findings. However, the evidence here suggests that is not an effective approach.
It is finally worth noting that changes which recommend more conservative behavior seem to
have greater take-up. This is notable in the case of vacuum extraction, where there are large
responses to both the FDA and, seemingly, the media, when they indicate that this procedure may
be dangerous. There is, however, no corresponding recovery in response to either official guidelines
or a major research study promoting safety.
This suggests, overall, that it may be more challenging to change some behaviors than others,
and there is clearly space for trying to better publicize new findings about best practices. The fact
that the behaviors change slowly leaves open the question of who benefits first, which I turn to
now.
4 Heterogeneity in Behavior Change
I focus now on heterogeneity, beginning with geography and demographics. There is significant focus
in the health economics literature on variation in practice patterns across space and demographic
groups; this practice variation has implications for varying health outcomes across these groups.
Here, I ask whether the changes in response to changes in best practice seem to differ across groups.
4.1 Geography and Demographics
A large literature has focused on variation across areas in the US in health outcomes in general
(Skinner, 2011) or in changes in health technology (e.g. Skinner and Staiger, 2005). In contrast
to this literature - which generally finds significant variation across space in health - I do not see
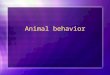
much variation in behavior change across regions of the US. This is visualized in Figure 2, which
replicates Figure 1 but includes separate lines for each region of the country. Note that due to
limited information on region (namely, it is not available after 2004) the early birth graph covers a
shorter time period here.
There are differences in levels of the behaviors - for example, vacuum extraction is used more
commonly in the West than elsewhere - but the changes over time are remarkably consistent. There
10

is neither a coming together nor a fanning out over time across space. The one notable feature is
that the short-lived drop in the use of C-section for breech deliveries in 2003 seems to be entirely
due to the South. It is not clear why this is.
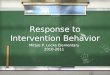
In contrast, I do see evidence that changes in behavior occur faster for some patient demographic
groups. To visualize this, consider Figure 3. This, again, replicates Figure 1 but adds a second series
in each figure. This second series shows the relationship between a dummy for low education and
the procedure over time - effectively, it shows the difference in the level of the procedure between
those with less than a high school degree and those with a high school degree or more.1
If we consider the VBAC example (Figure 3a) we see the series clearly moving in opposite
directions. As the procedure becomes less frequent, it becomes relatively more common among
those with less than a high school degree. Stated conversely, the change over time - the adoption of
VBAC - is faster among those with more education. We see similar patterns elsewhere. Appendix
Figure A1 shows the same graphs with a dummy for the mother reporting African-American race
rather than education. Finally, Appendix Figure A2 uses the predicted death rate - predicted based
on demographics - as the demographic measure. This provides a way to summarize the relative
speed of changes for better or worse off groups ex ante.
In many of these figures and sub-figures we see the same patterns – that is, changes which
suggest the change in practices occur earlier for more advantaged demographic groups. To get a
sense of whether these patterns are systematic, the first three columns of Table 3 show regression
evidence on the relationship. Specifically, in each case I regress the gradient (the coefficient from
a regression of the treatment on the demographic measure) on the level of treatment. A negative
coefficient here implies that as the level of the treatment goes up, the gradient goes down.
In the case of education, for example, the outcome in this regression is the excess procedure rate
for those with less education relative to more and the independent variable is the level of procedure.
A negative coefficient indicates that as the procedure becomes more common, it becomes relatively
less common among those with less education.
Column (1) of Table 3 shows these regression results for education, Column (2) for an indicator
for African-American and Column (3) for the predicted mortality measure. In all three cases, the
gradient is negative. Since each of these gradients are defined such that they take as the baseline the
less advantaged group, this implies that more advantaged women systematically see faster changes.
1These figures are computed at the quarterly, rather than the monthly level, to limit noise.
11

4.2 Outcomes
Changes accrue first to those who are already more advantaged, at least along observable dimen-
sions. To explore the evolving relationship with infant outcomes, Figure 4 echoes Figure 3, but
here the coefficient relationship is between treatment and whether the infant has a low APGAR
score. To create these coefficients, I regress the low APGAR indicator on procedure measures, and
include in the regression a full set of demographic controls.
Figure 4 looks very similar to Figure 3, As procedures become (for example) less common they
become relatively more associated with low APGAR scores. Appendix Figure A3 shows the same
graph for neonatal mortality (deaths in the first month of life) and Columns (4) and (5) of Table 3
shows the corresponding regressions. As in the observables, the regressions show significant negative
coefficients.
This suggests that as the procedures become less common they are more commonly experienced
by infants who have poor outcomes. This can be seen as an extension of the observable selection
seen above, although since these gradient regressions are conditional on observables, the selection
here must be on unobserved characteristics. It should be noted that there is another possible
interpretation - namely, that there are heterogeneous treatment effects in these cases, and when the
behavior becomes less common the infants who are still treated are those with the most negative
treatment effects. This seems possible, but unlikely, as it would suggest that doctors are targeting
these treatments to the mothers and infants who benefit least. More plausible is the interpretation
that infants who are otherwise disadvantaged also get these practice improvements later.
5 Discussion and Conclusion
This paper opens by asking whether doctors respond to changes in best practices, and whether
these changes exacerbate or ameliorate health inequality. The results above suggest that some
types of information do prompt response, although even in these cases where in principle behavior
change could be very fast, actually change is generally slow. The slow pace of change appears to
favor positively selected patients, both based on observable demographics and on examining the
outcomes associated with the procedures over time.
This analysis provides added motivation for improving compliance with changing best prac-
tices. Universal adoption of improved procedures would disproportionately benefit ex ante worse
off mothers and infants. Given the poor record of the US overall in maternal and infant health
12

(National Research Council, 2013) and the particular inequality in outcomes (Chen, Oster and
Williams, 2016) these issue are of policy concern.
These results provide less guidance in terms of how to speed up adoption. Official guidelines
seem to play little or no role, at least over and above the research studies they are based on.
Relying on the example of vacuum extraction, it would seem that alarmist publicity might increase
adoption speeds, but this is unlikely to be a widely acceptable policy response. It is also worth
saying that the approach here is unable to separate slow behavior change resulting from doctors
not learning about new evidence from slow behavior change due to resistance to change even in
the face of evidence. Understanding this distinction better empirically could allow development of
more effective approaches.
As a final point, the dynamics in Section 4.2 are notable because they highlight (as in Oster,
2018) that these changes in recommendations may increase the challenge of further research on the
impacts of these treatments. For research which relies on observational data, there may be biases
introduced by endogenous behavioral response. In the case of VBAC, for example, using these data
to estimate the risks in 2005 would yield a different estimate than in 1995, with the later data
suggesting a more negative outlook on VBAC.Given that much of our scientific knowledge relies on
observational data, these dynamics are worth considering when evaluating research results.
13

References
Agha, Leila and David Molitor, “The local influence of pioneer investigators on technologyadoption: evidence from new cancer drugs,” Review of Economics and Statistics, 2018, 100(1), 29–44.
Arroll, Bruce and Tim Kenealy, “Antibiotics for the common cold and acute purulent rhinitis,”Cochrane Database of Systematic Reviews, 2005, (3).
Bokhari, Farasat AS, “Managed care competition and the adoption of hospital technology: Thecase of cardiac catheterization,” International Journal of Industrial Organization, 2009, 27 (2),223–237.
Bradley, Elizabeth H, Tashonna R Webster, Mark Schlesinger, Dorothy Baker, andSharon K Inouye, “Patterns of diffusion of evidence-based clinical programmes: a case studyof the Hospital Elder Life Program,” BMJ Quality & Safety, 2006, 15 (5), 334–338.
Burke, Mary A, Gary M Fournier, and Kislaya Prasad, “The diffusion of a medical inno-vation: is success in the stars?,” Southern Economic Journal, 2007, pp. 588–603.
Chandra, Amitabh, David Cutler, and Zirui Song, “Who ordered that? The economics oftreatment choices in medical care,” in “Handbook of health economics,” Vol. 2, Elsevier, 2011,pp. 397–432.
Chen, Alice, Emily Oster, and Heidi Williams, “Why is infant mortality higher in the UnitedStates than in Europe?,” American Economic Journal: Economic Policy, 2016, 8 (2), 89–124.
Council”, ”National Research, Committee on Population et al., US health in internationalperspective: Shorter lives, poorer health, National Academies Press, 2013.
Domino, Marisa E, “Does managed care affect the diffusion of psychotropic medications?,”Healtheconomics, 2012, 21 (4), 428–443.
Engle, William A and Michelle A Kominiarek, “Late preterm infants, early term infants,and timing of elective deliveries,” Clinics in perinatology, 2008, 35 (2), 325–341.
Fleischman, Alan R, Motoko Oinuma, and Steven L Clark, “Rethinking the definition of”term pregnancy”,” Obstetrics & Gynecology, 2010, 116 (1), 136–139.
Foster, Andrew D and Mark R Rosenzweig, “Microeconomics of technology adoption,”Annu.Rev. Econ., 2010, 2 (1), 395–424.
Freedman, Seth, Haizhen Lin, and Kosali Simon, “Public health insurance expansions andhospital technology adoption,” Journal of Public Economics, 2015, 121, 117–131.
Gold, Heather T, Huibo Shao, Mary K Hayes, and Eleni Tousimis, “Diffusion of ac-celerated partial breast radiotherapy in the United States: physician-level and patient-levelanalyses,” Medical care, 2014, 52 (11), 969–974.
Griliches, Zvi, “Hybrid corn: An exploration in the economics of technological change,” Econo-metrica, Journal of the Econometric Society, 1957, pp. 501–522.
14

Gu, Qiuping, Vicki L Burt, Charles F Dillon, and Sarah Yoon, “Trends in AntihypertensiveMedication Use and Blood Pressure Control Among United States Adults With Hypertension-Clinical Perspective: The National Health and Nutrition Examination Survey, 2001 to 2010,”Circulation, 2012, 126 (17), 2105–2114.
Hannah, Mary E, Walter J Hannah, Sheila A Hewson, Ellen D Hodnett, Saroj Saigal,Andrew R Willan, and Term Breech Trial Collaborative, “Planned caesarean sectionversus planned vaginal birth for breech presentation at term: a randomised multicentre trial,”The Lancet, 2000, 356 (9239), 1375–1383.
Hannah, Mary, Hilary Whyte, and Walter Hannah, “Maternal outcomes at 2 years postpartum in the term breech trial,”American Journal of Obstetrics & Gynecology, 2003, 189 (6),S136.
Jackson, James H, John Sobolski, Russ Krienke, Ken S Wong, Feride Frech-Tamas, andBrian Nightengale, “Blood pressure control and pharmacotherapy patterns in the UnitedStates before and after the release of the Joint National Committee on the Prevention, Detec-tion, Evaluation, and Treatment of High Blood Pressure (JNC 7) guidelines,” The Journal ofthe American Board of Family Medicine, 2008, 21 (6), 512–521.
Johnson, Erin M and M Marit Rehavi, “Physicians treating physicians: Information andincentives in childbirth,” American Economic Journal: Economic Policy, 2016, 8 (1), 115–41.
Kristensen, Steen Dalby, Juhani Knuuti, Antti Saraste, Stefan Anker, Hans ErikBøtker, Stefan De Hert, Ian Ford, Jose Ramon Gonzalez-Juanatey, BulentGorenek et al., “2014 ESC/ESA Guidelines on non-cardiac surgery: cardiovascular assess-ment and management: The Joint Task Force on non-cardiac surgery: cardiovascular assess-ment and management of the European Society of Cardiology (ESC) and the European Societyof Anaesthesiology (ESA),” European heart journal, 2014, 35 (35), 2383–2431.
Ma, Jun, Ky-Van Lee, and Randall S Stafford, “Changes in antihypertensive prescribingduring US outpatient visits for uncomplicated hypertension between 1993 and 2004,” Hyper-tension, 2006, 48 (5), 846–852.
McMahon, Michael J, Edwin R Luther, Watson A Bowes Jr, and Andrew F Olshan,“Comparison of a trial of labor with an elective second cesarean section,”New England journalof medicine, 1996, 335 (10), 689–695.
Oster, Emily, “Behavioral Feedback: Do Individual Choices Influence Scientific Results?,” Work-ing Paper 25225, National Bureau of Economic Research 2018.
Pauff, Brandy R, Michael R Jiroutek, Melissa A Holland, and Beth S Sutton, “Statinprescribing patterns: an analysis of data from patients with diabetes in the national hospitalambulatory medical care survey outpatient department and national ambulatory medical caresurvey databases, 2005–2010,” Clinical therapeutics, 2015, 37 (6), 1329–1339.
Reddy, Uma, Chia-Wen Ko, and Marian Willinger, “”Early” term births (37-38 weeks) areassociated with increased mortality,”American Journal of Obstetrics & Gynecology, 2006, 195(6), S202.
Sacarny, Adam, “Technological diffusion across hospitals: The case of a revenue-generating prac-tice,” Job market paper, Massachusetts Institute of Technology, 2014.
15

Sakulchit, Teeranai and Ran D Goldman, “Antibiotic therapy for children with acute otitismedia,” Canadian Family Physician, 2017, 63 (9), 685–687.
Skinner, Jonathan, “Causes and consequences of regional variations in health care,” in“Handbookof health economics,” Vol. 2, Elsevier, 2011, pp. 45–93.
, Amitabh Chandra, Douglas Staiger, Julie Lee, and Mark McClellan, “Mortalityafter acute myocardial infarction in hospitals that disproportionately treat black patients,”Circulation, 2005, 112 (17), 2634–2641.
and Douglas Staiger, “Technology adoption from hybrid corn to beta blockers,” TechnicalReport, National Bureau of Economic Research 2005.
Smieliauskas, Fabrice, “Peer effects and service differentiation in technology adoption: evidencefrom physician markets,” 2011.
Towner, Dena, Mary Ames Castro, Elaine Eby-Wilkens, and William M Gilbert, “Effectof mode of delivery in nulliparous women on neonatal intracranial injury,”New England journalof medicine, 1999, 341 (23), 1709–1714.
Whelton, Paul K., Robert M. Carey, Wilbert S. Aronow, Donald E. Casey, Karen J.Collins, Cheryl Dennison Himmelfarb, Sondra M. DePalma, Samuel Gidding, Ken-neth A. Jamerson, Daniel W. Jones, Eric J. MacLaughlin, Paul Muntner, BruceOvbiagele, Sidney C. Smith, Crystal C. Spencer, Randall S. Stafford, Sandra J.Taler, Randal J. Thomas, Kim A. Williams, Jeff D. Williamson, and Jackson T.Wright, “2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNAGuideline for the Prevention, Detection, Evaluation, and Management of High Blood Pres-sure in Adults,” Journal of the American College of Cardiology, 2018, 71 (19), e127–e248.
Yu, Yang, “The Effect of Competition on Technology Diffusion and Treatment Choices in Health-care Market,” 2015.
16

Fig
ure
1:C
han
ges
inP
rocedure
sO
ver
Tim
e
Pan
elA
:V
BA
CC
han
ges
and
Eve
nts
Pan
elB
:B
reec
hSec
tion
Chan
ges
and
Eve
nts
.1.15.2.25.3VBAC Share
1995
m1
2000
m1
2005
m1
Rat
e of
VB
AC
Am
ong
Prio
r C
esar
ean
.84.86.88C-Section Share
1995
m1
2000
m1
2005
m1
Rat
e of
C-S
ectio
n A
mon
g B
reec
h B
irths
Pan
elC
:V
acu
um
Ch
ange
san
dE
vents
Pan
elD
:E
arly
Bir
thC
han
ges
and
Even
ts
.04.045.05.055.06.065Vacuum Share
1995
m1
2000
m1
2005
m1
Rat
e of
Vac
uum
.2.25.3.35Early Term Share
1995
m1
2000
m1
2005
m1
2010
m1
2015
m1
Rat
e of
Ear
ly T
erm
Birt
hs
Note
s:T
hes
efigure
ssh
owch
anges
inobst
etri
cpro
cedure
sov
erti
me
wit
hea
chdot
repre
senti
ng
am
onth
.V
BA
Cis
defi
ned
only
for
wom
enw
ith
apre
vio
us
cesa
rean
sect
ion.
Earl
yte
rmbir
ths
are
bir
ths
at
37
or
38
wee
ks,
as
ash
are
of
all
bir
ths
37
wee
ks
or
late
r.D
ott
edver
tica
llines
repre
sent
the
rele
ase
of
rese
arc
hst
udie
sre
late
dto
the
pro
cedure
s.Solid
ver
tica
llines
repre
sent
AC
OG
com
mit
tee
opin
ions
and
pra
ctic
ebullet
ins.
Det
ails
of
thes
eev
ents
app
ear
inT
able
2.
17

Fig
ure
2:C
han
ges
by
Geogra
phic
Are
a
Pan
elA
:V
BA
Cby
Reg
ion
Pan
elB
:B
reec
hC
-Sec
tion
by
Reg
ion
0.1.2.3.4VBAC Share
1995
m1
2000
m1
2005
m1
Nor
th E
ast
Mid
Wes
tS
outh
Wes
t
Rat
e of
VB
AC
Am
ong
Prio
r C
esar
ean
.8.85.9C-Section Share
1995
m1
2000
m1
2005
m1
Nor
th E
ast
Mid
Wes
tS
outh
Wes
t
Rat
e of
C-S
ectio
n A
mon
g B
reec
h B
irths
Pan
elC
:V
acu
um
by
Reg
ion
Pan
elD
:E
arly
Bir
thby
Reg
ion
.03.04.05.06.07.08Vacuum Share
1995
m1
2000
m1
2005
m1
Nor
th E
ast
Mid
Wes
tS
outh
Wes
t
Rat
e of
Vac
uum
.2.25.3.35Early Term Share
1995
m1
2000
m1
2005
m1
Nor
th E
ast
Mid
Wes
tS
outh
Wes
t
Rat
e of
Ear
ly T
erm
Birt
hs
Note
s:T
hes
efigure
ssh
owth
eth
ele
vel
of
beh
avio
rov
erti
me
by
regio
n.
The
four
are
as
corr
esp
ond
tost
andard
censu
sre
gio
ns:
Nort
hE
ast
,South
,W
est
and
Mid
-Wes
t.D
ott
edver
tica
llines
repre
sent
the
rele
ase
of
rese
arc
hst
udie
sre
late
dto
the
pro
cedure
s.Solid
ver
tica
llines
repre
sent
AC
OG
com
mit
tee
opin
ions
and
pra
ctic
ebullet
ins.
Det
ails
of
thes
eev
ents
app
ear
inT
able
2.
18

Fig
ure
3:V
ari
ati
on
inP
rocedure
Use
by
Educati
on
Over
Tim
e
Pan
elA
:L
owE
du
cati
onan
dV
BA
CP
anel
B:
Low
Edu
can
dB
reec
hC
-Sec
tion
-.02-.010.01.02.03VBAC Coefficients
.1.15.2.25.3VBAC Rate
1995
m1
2000
m1
2005
m1
date
VB
AC
Rat
eC
oeffi
cien
ts
Cov
aria
nce
betw
een
VB
AC
and
Low
Edu
c.
-.08-.06-.04-.020Breech x C-Section Coefficients
.84.86.88Breech x C-Section Rate 19
95m
120
00m
120
05m
1da
te
Bre
ech
x C
-Sec
tion
Rat
eC
oeffi
cien
ts
Cov
aria
nce
betw
een
Bre
ech
x C
-Sec
tion
and
Low
Edu
c.
Pan
elC
:L
owE
du
c.an
dV
acuum
Pan
elD
:L
owE
duc
and
Ear
lyB
irth
-.015-.01-.005Vacuum Coefficients
.04.045.05.055.06.065Vacuum Rate
1995
m1
2000
m1
2005
m1
date
Vac
uum
Rat
eC
oeffi
cien
ts
Cov
aria
nce
betw
een
Vac
uum
and
Low
Edu
c.
-.04-.020.02.04Early Birth Coefficients
.2.25.3.35Early Birth Rate
1995
m1
2000
m1
2005
m1
2010
m1
2015
m1
date
Ear
ly B
irth
Rat
eC
oeffi
cien
ts
Cov
aria
nce
betw
een
Ear
ly B
irth
and
Low
Edu
c.
Note
s:T
hes
efigure
ssh
owth
eth
ele
vel
of
beh
avio
rand
its
rela
tionsh
ipw
ith
educa
tion
over
tim
e.T
he
level
sre
plica
teF
igure
1.
To
crea
teth
eed
uca
tion
seri
esI
esti
mate
the
diff
eren
cein
trea
tmen
tle
vel
sb
etw
een
those
wit
hle
ssed
uca
tion
(defi
ned
as
less
than
hig
hsc
hool)
and
those
wit
hm
ore
educa
tion
than
that.
To
lim
itnois
eI
do
thes
eca
lcula
tions
the
quart
erly
level
.V
erti
cal
lines
indic
ate
even
tsas
inF
igure
1,
wit
hdet
ails
inT
able
2.
19

Fig
ure
4:
Vari
ati
on
inP
rocedure
Eff
ects
on
Outc
om
es:
AP
GA
R
Pan
elA
:E
ffec
tof
VB
AC
onlo
wA
PG
AR
Pan
elB
:E
ffec
tof
Bre
ech
onlo
wA
PG
AR
-.0020.002.004.006.008vbac Coefficients
.1.15.2.25.3VBAC Rate
1995
m1
2000
m1
2005
m1
date
VB
AC
Rat
eC
oeffi
cien
ts
Reg
ress
ion
of L
ow A
PG
AR
on
VB
AC
+ C
ontr
ols
-.095-.09-.085-.08-.075-.07breech Coefficients
.84.86.88Breech x C-Section Rate 19
95m
120
00m
120
05m
1da
te
Bre
ech
x C
-Sec
tion
Rat
eC
oeffi
cien
ts
Reg
ress
ion
of L
ow A
PG
AR
on
Bre
ech
x C
-Sec
tion
+ C
ontr
ols
Pan
elC
:E
ffec
tof
Vacu
um
onlo
wA
PG
AR
Pan
elD
:E
ffec
tof
Ear
lyB
irth
onlo
wA
PG
AR
.001.002.003.004.005vacuum Coefficients
.04.045.05.055.06.065Vacuum Rate
1995
m1
2000
m1
2005
m1
date
Vac
uum
Rat
eC
oeffi
cien
ts
Reg
ress
ion
of L
ow A
PG
AR
on
Vac
uum
+ C
ontr
ols
-.00050.0005.001.0015.002early_birth Coefficients
.2.25.3.35Early Birth Rate
1995
m1
2000
m1
2005
m1
2010
m1
2015
m1
date
Ear
ly B
irth
Rat
eC
oeffi
cien
ts
Reg
ress
ion
of L
ow A
PG
AR
on
Ear
ly B
irth
+ C
ontr
ols
Note
s:T
hes
efigure
ssh
owth
ele
vel
of
beh
avio
rand
its
rela
tionsh
ipw
ith
AP
GA
Rsc
ore
over
tim
e.T
he
level
sre
plica
teF
igure
1.
To
crea
teth
eA
PG
AR
seri
esI
regre
ss,
at
the
quart
erly
level
,an
indic
ato
rfo
rlo
wA
PG
AR
score
(<7)
on
the
trea
tmen
tand
dem
ogra
phic
contr
ols
.T
he
gra
phs
show
evolu
tion
of
this
coeffi
cien
tov
erti
me.
Ver
tica
llines
indic
ate
even
tsas
inF
igure
1,
wit
hdet
ails
inT
able
2.
20

Table 1: Summary Statistics
Mean Standard Deviation Sample Size Time Period
VBAC 0.19 0.39 4,768,286 1995-2005
Vacuum Extraction 0.05 0.22 43,771,430 1995-2005
Breech Delivered by Cesarean 0.86 0.34 1,694,848 1995-2005
Early Term 0.29 0.45 74,898,956 1995-2015
White 0.57 0.49 65,072,301 1995-2015
Black 0.15 0.35 65,072,301 1995-2015
Hispanic 0.22 0.41 65,072,301 1995-2015
Other Race 0.06 0.24 65,072,301 1995-2015
Unknown Education 0.01 0.12 65,072,301 1995-2015
Less than High School 0.10 0.29 65,072,301 1995-2015
High School 0.46 0.50 65,072,301 1995-2015
College 0.43 0.50 65,072,301 1995-2015
Age < 20 0.11 0.31 65,072,301 1995-2015
19 < Age < 30 0.52 0.50 65,072,301 1995-2015
29 < Age < 40 0.34 0.47 65,072,301 1995-2015
Age > 39 0.03 0.16 65,072,301 1995-2015
North East 0.17 0.38 39,929,013 1995-2004
South 0.36 0.48 39,929,013 1995-2004
Midwest 0.22 0.41 39,929,013 1995-2004
West 0.24 0.43 39,929,013 1995-2004
Notes: This table shows summary statistics on the data used from the NHCS. All variables are binary. VBAC shareis the share of women with at least one prior cesarean who have a vaginal birth. Breech delivery by cesarean is limitedto breech births. Early term delivery is defined as delivery at 37 or 38 weeks, among all births at or after 37 weeks.
21

Table 2: Information Events
Treatment Event 1 Event 2 Event 3 Event 4
VBAC 1996, Negative: A
research study from
McMahon is the first to
show that major
complications, including
uterine rupture, were more
likely for patients who
attempted VBAC than
those who had a repeat
cesarean. This study
influences the more
restrictive ACOG
guidelines later.
1998, Negative: ACOG
publishes Practice Bulletin
2 citing the risk of uterine
rupture. There is
subsequent media coverage
on the risks of VBAC.
1999, Negative: ACOG
publishes Practice Bulletin
5, which suggests that
physicians should be
“immediately” available to
provide emergency care to
women attempting VBAC.
This was seen as very
restrictive, and many
commented that there is
no such thing as an
immediate cesarean.
Breech
Delivery
2000, Guideline : A
research study, Hannah,
et. al. (2000), conducts a
trial of term breech births.
It concludes that planned
cesarean sections are
better than vaginal births
for term breech babies.
2001, Guideline :
ACOG publishes a
committee opinion
encouraging c-sections for
breech births.
2003, Guideline : A
follow-up research study
from Hannah, et. al
(2003) finds that there
were no substantial
differences between breech
presenting babies delivered
by planned c-section and
planned vaginal birth at
term 2 years post partum.
Vacuum
Extraction
1998/1999, Negative:
The FDA releases a report
about the dangers of
vacuum extraction. Also
media coverage of a
NJEM article in which
doctors protest a goal of
lowering c-section rates.
1998, Positive: ACOG
publishes a committee
opinion in response to the
FDA report to reassure
physicians that
complications from
vacuum extraction are
rare.
1999, Positive: Towner,
et. al (1999) publish a
study, widely cited in the
media, demonstrating that
the rates of intracranial
hemorrhage were similar
for vacuum extraction,
forceps delivery, and
cesarean delivery, refuting
prior claims about the
relative safety of vacuum
extraction.
2000, Positive: ACOG
published Practice
Bulletin 17, which remarks
that there is no difference
in mortality between
births achieved by forceps
and vacuum.
Redefinition of
Full Term
Pregnancy
2013, Guideline: ACOG
changes the definition of
full-term pregnancy,
creating four categories.
Notes: This table shows the information events identified for each outcome.
22

Table 3: Selection of Behaviors
(1) (2) (3) (4) (5)
Outcome: Low Educ Gradient Black Grad. Pred. Death Grad Low APGAR Grad. Mortality Grad.
Level of Behavior -0.073∗∗∗ -0.047∗∗∗ -0.00017∗∗ -0.025∗∗∗ -0.034∗∗∗
(0.012) (0.008) (0.00008) (0.005) (0.004)
Treatment FE YES YES YES YES YES
Year FE YES YES YES YES YES
Number of Obs. 600 600 600 600 552
Notes: This table shows statistical evidence on the co-movements between levels of treatment and the gradient withrespect to demographics (education and race), the predicted death rate based on demographics and two outcomes(low APGAR score and infant mortality). Each cell represents a different regression of gradients on the level oftreatment. An observation is a treatment-month. All regressions include fixed effects for each treatment and year.∗indicates significance at the 10% level, ∗∗indicates significance at the 5% level, ∗ ∗ ∗ indicates significance at the 1%level.
23

Appendix A: Appendix Figures and Tables
Figure A1: Variation in Procedure Use by Race Over Time
Panel A: Black Race and VBAC Panel B: Black Race and Breech C-Section
-.02
-.01
0.0
1V
BA
C C
oeffi
cien
ts
.1.1
5.2
.25
.3V
BA
C R
ate
1995m1 2000m1 2005m1date
VBAC Rate Coefficients
Covariance between VBAC and Race
-.07
-.06
-.05
-.04
-.03
Bre
ech
x C
-Sec
tion
Coe
ffici
ents
.84
.86
.88
Bre
ech
x C
-Sec
tion
Rat
e
1995m1 2000m1 2005m1date
Breech x C-Section Rate Coefficients
Covariance between Breech x C-Section and Race
Panel C: Black Race and Vacuum Panel D: Black Race and Early Birth
-.03
-.02
5-.
02-.
015
-.01
Vac
uum
Coe
ffici
ents
.04
.045
.05
.055
.06
.065
Vac
uum
Rat
e
1995m1 2000m1 2005m1date
Vacuum Rate Coefficients
Covariance between Vacuum and Race
.03
.04
.05
.06
Ear
ly B
irth
Coe
ffici
ents
.2.2
5.3
.35
Ear
ly B
irth
Rat
e
1995m1 2000m1 2005m1 2010m1 2015m1date
Early Birth Rate Coefficients
Covariance between Early Birth and Race
Notes: These figures show the level of behavior and its relationship with neonatal mortality (deaths in the firstmonth of life) over time. The levels replicate Figure 1. To create the mortality series I regress, at the quarterlylevel, an indicator for infant mortality on the treatment and demographic controls. The graphs show evolution of thiscoefficient over time. Vertical lines indicate events as in Figure 1, with details in Table 2.
24

Figure A2: Variation in Procedure Use by Predicted Death Over Time
Panel A: Predicted Death and VBAC Panel B: Predicted Death and Breech C-Section
-.00
005
0.0
0005
.000
1.0
0015
VB
AC
Coe
ffici
ents
.1.1
5.2
.25
.3V
BA
C R
ate
1995m1 2000m1 2005m1date
VBAC Rate Coefficients
Covariance between VBAC and Predicted Death
-.00
4-.
0035
-.00
3-.
0025
-.00
2B
reec
h x
C-S
ectio
n C
oeffi
cien
ts
.84
.86
.88
Bre
ech
x C
-Sec
tion
Rat
e
1995m1 2000m1 2005m1date
Breech x C-Section Rate Coefficients
Covariance between Breech x C-Section and Predicted Death
Panel C: Predicted Death and Vacuum Panel D: Predicted Death and Early Birth
-.00
03-.
0002
5-.
0002
-.00
015
-.00
01V
acuu
m C
oeffi
cien
ts
.04
.045
.05
.055
.06
.065
Vac
uum
Rat
e
1995m1 2000m1 2005m1date
Vacuum Rate Coefficients
Covariance between Vacuum and Predicted Death
0.0
0001
.000
02.0
0003
.000
04E
arly
Birt
h C
oeffi
cien
ts
.2.2
5.3
.35
Ear
ly B
irth
Rat
e
1995m1 2000m1 2005m1 2010m1 2015m1date
Early Birth Rate Coefficients
Covariance between Early Birth and Predicted Death
Notes: These figures show the level of behavior and its relationship with neonatal mortality (deaths in the firstmonth of life) over time. The levels replicate Figure 1. To create the mortality series I regress, at the quarterlylevel, an indicator for infant mortality on the treatment and demographic controls. The graphs show evolution of thiscoefficient over time. Vertical lines indicate events as in Figure 1, with details in Table 2.
25

Figure A3: Variation in Procedure Effects on Outcomes: Mortality
Panel A: Effect of VBAC on Mortality Panel B: Effect of Breech on Mortality
0.0
01.0
02.0
03.0
04.0
05V
BA
C C
oeffi
cien
ts
.1.1
5.2
.25
.3V
BA
C R
ate
1995m1 2000m1 2005m1date
VBAC Rate Coefficients
Regression of Infant Death on VBAC + Controls
-.08
-.07
5-.
07-.
065
-.06
Bre
ech
x C
-Sec
tion
Coe
ffici
ents
.84
.86
.88
Bre
ech
x C
-Sec
tion
Rat
e
1995m1 2000m1 2005m1date
Breech x C-Section Rate Coefficients
Regression of Infant Death on Breech x C-Section + Controls
Panel C: Effect of Vacuum on Mortality Panel D: Effect of Early Birth on Mortality
-.00
32-.
003
-.00
28-.
0026
Vac
uum
Coe
ffici
ents
.04
.045
.05
.055
.06
.065
Vac
uum
Rat
e
1995m1 2000m1 2005m1date
Vacuum Rate Coefficients
Regression of Infant Death on Vacuum + Controls
.000
1.0
002
.000
3.0
004
.000
5E
arly
Birt
h C
oeffi
cien
ts
.2.2
5.3
.35
Ear
ly B
irth
Rat
e
1995m1 2000m1 2005m1 2010m1 2015m1date
Early Birth Rate Coefficients
Regression of Infant Death on Early Birth + Controls
Notes: These figures show the level of behavior and its relationship with neonatal mortality (deaths in the firstmonth of life) over time. The levels replicate Figure 1. To create the mortality series I regress, at the quarterlylevel, an indicator for infant mortality on the treatment and demographic controls. The graphs show evolution of thiscoefficient over time. Vertical lines indicate events as in Figure 1, with details in Table 2.
26