Embed Size (px)
Citation preview

Jeong Bae Park, MD,PhDDept of Med/Cardiology, Cheil General Hospital,
Kwandong University College of Medicine
Explore the Rationale for the Dual Mechanism CCB/ARB Approach
in Hypertension Management
Apr 23 2008 Angioplasty Summit

Global Mortality 2000: Impact of Hypertension and Other Health Risk Factors
Adapted from The Lancet, 360, Ezzati et al. pp. 1347–60. Copyright © 2002, with permission from Elsevier
Attributable mortality in millions (total: 55,861,000)
Developing regionDeveloped region
0 87654321
High BP
Tobacco
High cholesterol
Unsafe sex
High BMI
Physical inactivity
Alcohol
Underweight

Stroke and Ischemic Heart Disease (IHD) Mortality Rate in Each Decade of Age, Versus Usual Systolic BP at the Start of that Decade
Mor
talit
y*
Usual SBP (mmHg)
50–59 y
60–69 y
70–79 y
80–89 y
StrokeAge at risk
256
128
64
32
16
8
4
2
1
0 120 140 160 180
IHD
Usual SBP (mmHg)
50–59 y
60–69 y
70–79 y
80–89 yAge at risk
40–49 y
256
128
64
32
16
8
4
2
1
0 120 140 160 180
*Floating absolute risk and 95% CIReproduced from The Lancet, 360, Lewington et al. pp. 1903–13
Copyright © 2002, with permission from Elsevier
2 mmHg decrease in mean
SBP10% stroke mortality
7% ischaemicheart disease mortality
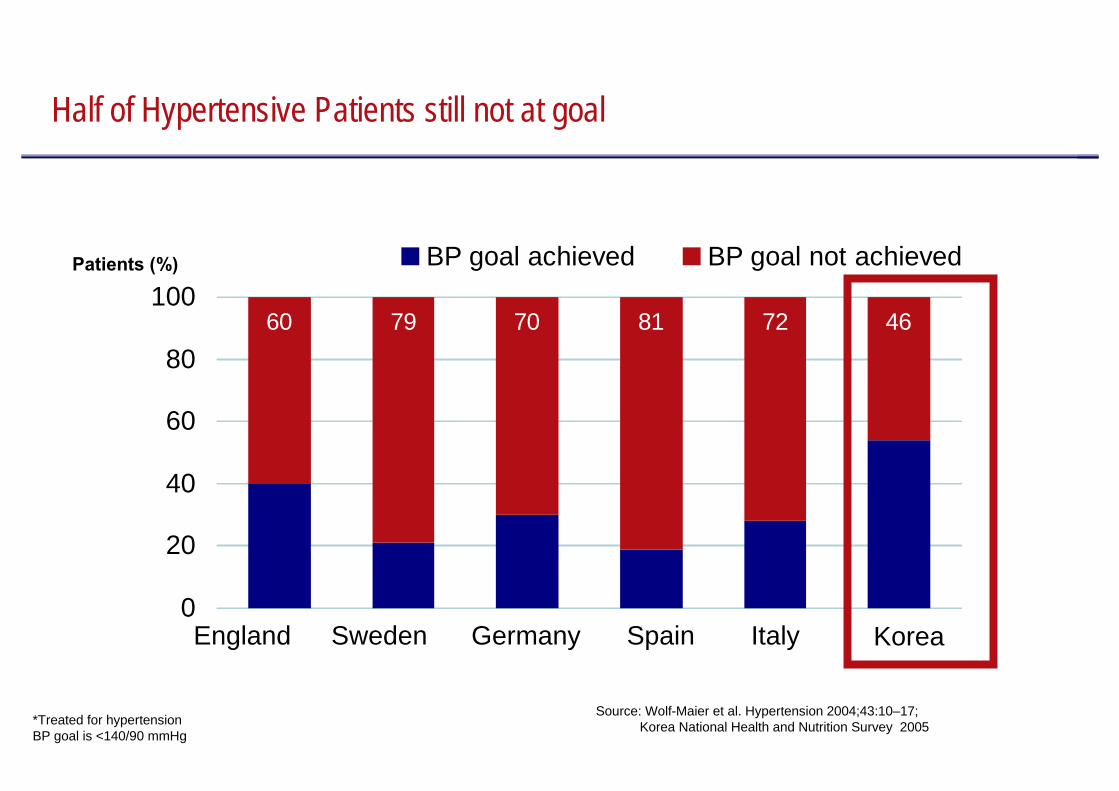
60 79 70 81 72 46
0
20
40
60
80
100BP goal achieved BP goal not achievedPatients (%)
England Sweden Germany Spain Italy Korea
*Treated for hypertensionBP goal is <140/90 mmHg
Source: Wolf-Maier et al. Hypertension 2004;43:10–17; Korea National Health and Nutrition Survey 2005
Half of Hypertensive Patients still not at goal

Multiple Antihypertensive Drugs Required to Achieve Target BP
00
11
22
33
44
UKPDSUKPDSDBP <85DBP <85
MDRDMDRDMAP <92MAP <92
AASKAASKMAP <92MAP <92
ALLHATALLHAT<140/90<140/90
Num
ber o
f Dru
gs*
Num
ber o
f Dru
gs*
ABCDABCDDBP <75DBP <75
HOTHOTDBP <80DBP <80
IDNTIDNT135/85135/85
**UKPDS, ABCD, MDRD, HOT, AASK, IDNT, ASCOT=average; ALLHAT=mean.UKPDS, ABCD, MDRD, HOT, AASK, IDNT, ASCOT=average; ALLHAT=mean.
Adapted from Bakris GL et al. Am J Kidney Dis. 2000;36:646–661. Lewis EJ et al. N Engl J Med. 2001;345:851–860. Cushman WC et al. J Clin Hypertens. 2002:4;393–404. Dahlöf B et al. Lancet. 2005;366:895–906.
ASCOTASCOT<140/90<140/90

Endo(n=30)
Nephro(n=30)
Clinic(n=60)
26
40
23
11
+4 drug combi
3 drug combi
2 drug combi
Mono Tx
(Unit: mean %)
Cardio(n=50)
35
41
18
6
28
36
24
12
38
40
18
4
>60-70% patients need 2 or more anti-hypertensive agents in Korea Practice.
* FDC is considered as 2 drug combination.[Base: HTN patients on medication]
* 2007 CV portfolio optimization study
2 drug combination Rx takes the largest portion across all the specialties.

Sympathetic nervous systemRenin-angiotensin systemTotal body sodium
Patient 1 Patient 2 Patient 3
B. Waeber, March 2007, with permission
Blood Pressure has Multiple Regulatory Pathways

Understand burden of Hypertension- Poor Treatment and control rates
Rationale for Multiple-mechanism Therapy in Hypertension- Inadequacy of agents with a single mechanism of action
Inadequacy of Single MOA approach
Advantages of Multiple-mechanism Therapy
Contemporary Hypertension and its Therapeutic Strategy

Diuretics
Angiotensinreceptor blockers(ARBs)
Calcium channelblockers (CCBs)
Angiotensin-converting enzyme (ACE) inhibitors
β-blockers
α-blockers
Available as a fixed-dose combination
Less frequently used/combination used as necessary
Adapted from Task Force of ESH–ESC. J Hypertens 2007;25:1105–87
ESH−ESC Recommendations for 6 Combining BP-loweringDrugs and Availability as Fixed-dose Combinations
?
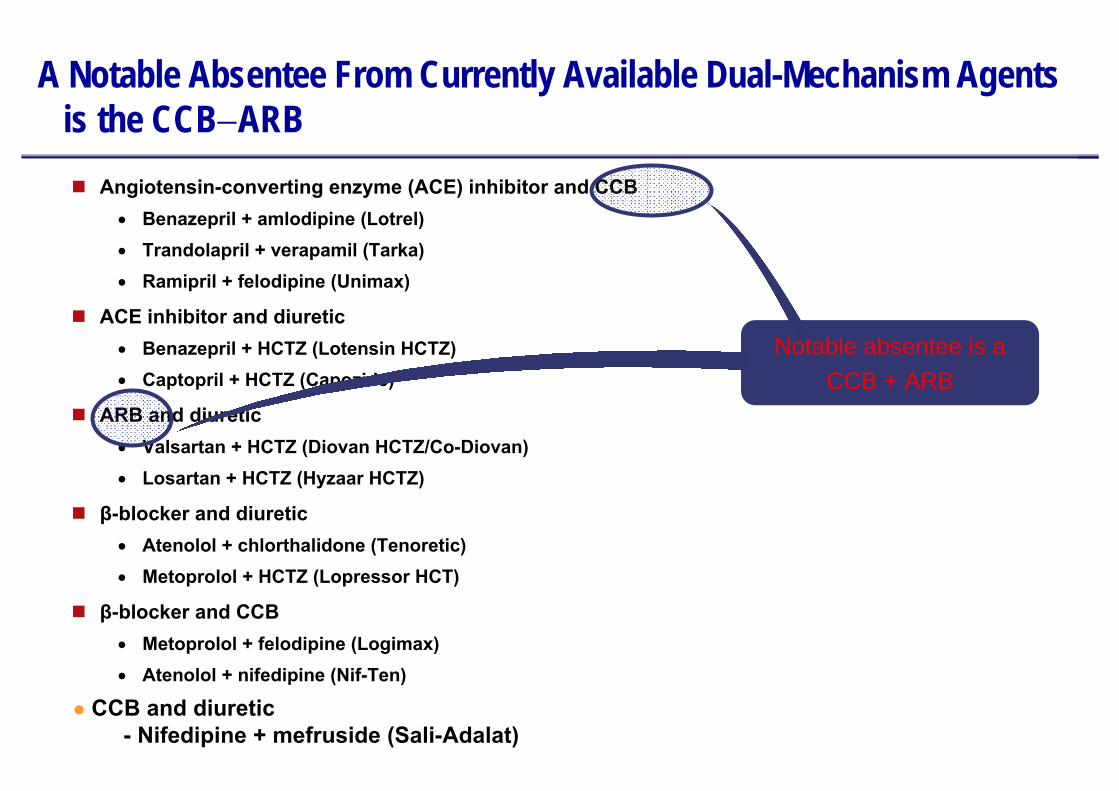
A Notable Absentee From Currently Available Dual-Mechanism Agents is the CCB−ARB
Angiotensin-converting enzyme (ACE) inhibitor and CCB• Benazepril + amlodipine (Lotrel)• Trandolapril + verapamil (Tarka)• Ramipril + felodipine (Unimax)
ACE inhibitor and diuretic• Benazepril + HCTZ (Lotensin HCTZ)• Captopril + HCTZ (Capozide)
ARB and diuretic• Valsartan + HCTZ (Diovan HCTZ/Co-Diovan)• Losartan + HCTZ (Hyzaar HCTZ)
β-blocker and diuretic• Atenolol + chlorthalidone (Tenoretic)• Metoprolol + HCTZ (Lopressor HCT)
β-blocker and CCB• Metoprolol + felodipine (Logimax)• Atenolol + nifedipine (Nif-Ten)
Notable absentee is aCCB + ARB
CCB and diuretic- Nifedipine + mefruside (Sali-Adalat)

Interaction of CCBs and ARBs on Vascular and Renal Function, SNS and RAS Activity
CCBCCB ARBARB
VasodilationVasodilation
NatriuresisNatriuresis
ArterialArterial ArterialArterial ++VenousVenous
RAS RAS ↓↓
SNS SNS ↓↓
↑↑ RASRAS
↑↑ SNSSNS
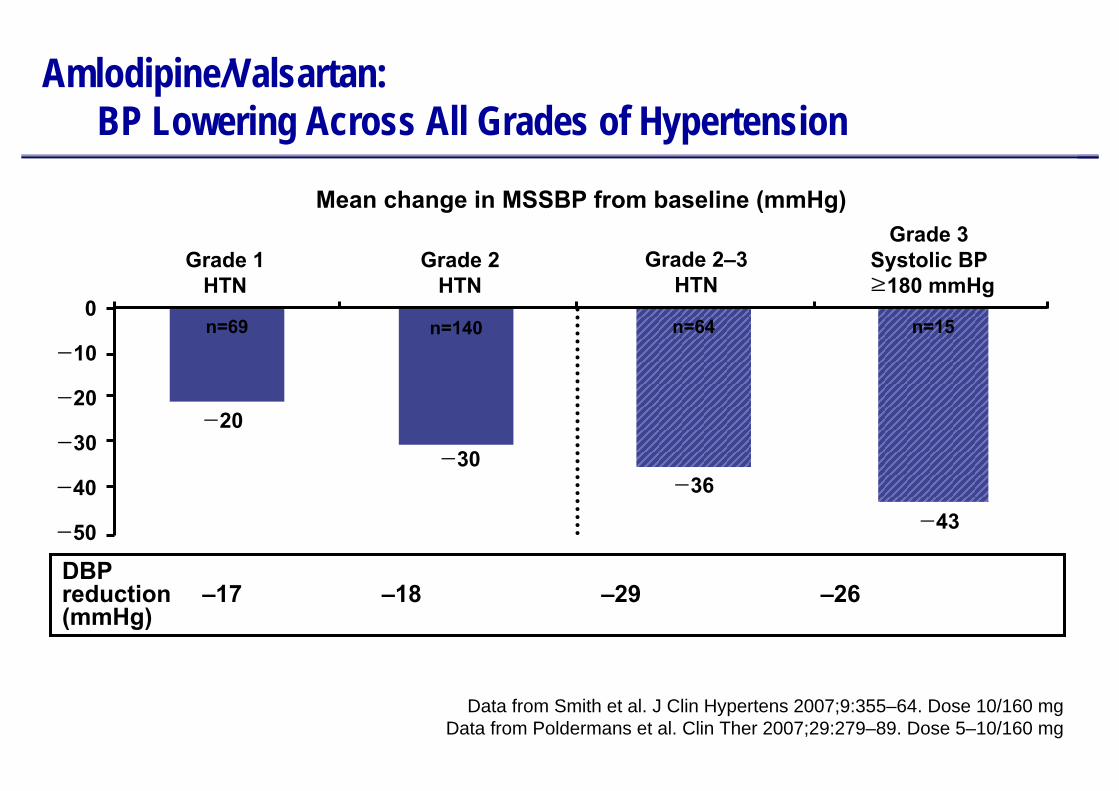
n=69 n=140 n=64 n=15
Amlodipine/Valsartan: BP Lowering Across All Grades of Hypertension
−50
0
−10
−20
−30
Mean change in MSSBP from baseline (mmHg)
−40
−20
Grade 1HTN
Grade 2–3HTN
Grade 3Systolic BP≥180 mmHg
Grade 2HTN
−30−36
−43
DBP reduction –17 –18 –29 –26(mmHg)
Data from Smith et al. J Clin Hypertens 2007;9:355–64. Dose 10/160 mgData from Poldermans et al. Clin Ther 2007;29:279–89. Dose 5–10/160 mg
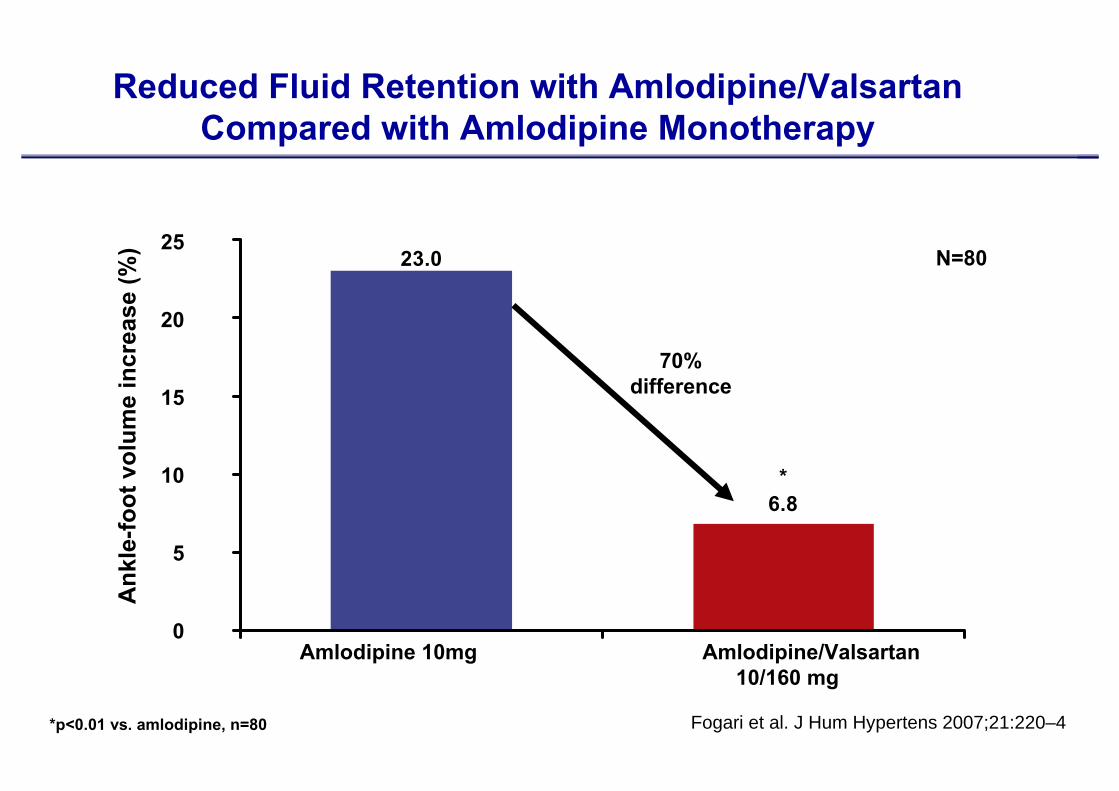
*p<0.01 vs. amlodipine, n=80 Fogari et al. J Hum Hypertens 2007;21:220–4
Reduced Fluid Retention with Amlodipine/ValsartanCompared with Amlodipine Monotherapy
*6.8
23.025
20
15
10
5
0
Ank
le-fo
ot v
olum
e in
crea
se (%
)
Amlodipine 10mg Amlodipine/Valsartan10/160 mg
N=80
70%difference

Complementary Effects of a CCB/RAS Inhibitor: Reduction of CCB-associated Edema
I.
II.
III.
Edema
Arterial hypertension
Constricted blood vessels, high resistance
CCBsBP reduction due to arterial vasodilationTendency towards edema due to absent venodilationBP reduction stimulates RAS and increases angiotensin II level
CCBs + RAS inhibitors*Blockade of RAS inhibits effects of angiotensin II, giving rise to additional BP reductionAdditional venodilation by RAS inhibitors reduces edema
Edema
*Angiotensin receptor blockers or angiotensin-converting enzyme inhibitors Messerli. Am J Hypertens 2001;14:978–9

CCB• Arteriodilation• Peripheral edema• Effective in low-renin patients• Proven efficacy in elderly
CCB• RAS activation• No renal or CHF benefits• No DM benefits
CCB/ARB: Synergy of Counter-regulation
ARB• Arterio-Venodilation• Attenuates peripheral edema• Effective in high-renin patients• Better in younger
ARB• RAS blockade• CHF and renal benefits• DM benefits

ACCOMPLISH [ RAAS+CCB vs. RAAS+HCTZ ]
Avoiding Cardiovascular Events through COMbination Therapy in Patients LIvingwith Systolic Hypertension
A prospective, double-blind, randomized, trial
to compare the effects of
amlodipine / benazepril vs. benazepril / thiazide
on the reduction of CV morbidity and mortality
in patients with high risk hypertension

ACCOMPLISH: Design
Jamerson KA et al. Am J Hypertens. 2004;17:793–801.*Beta blockers; alpha blockers; clonidine; loop diuretics.
14 Days Day 1 Month 1 Month 2 Year 5
ScreeningScreening
Amlodipine 5 mg/benazepril /20 mg
Ran
dom
izat
ion
Benazepril 40 mg +HCTZ 12.5 mg
Benazepril 40 mg + HCTZ 25 mg
Free add-on antihypertensive agents*
Month 3
Free add-on antihypertensive agents*
Amlodipine 5 mg/benazepril /40 mg
Amlodipine 10 mg/benazepril /40 mg
Benazepril 20 mg + HCTZ 12.5 mg
Titrated to achieve BP <140/90 mmHg; <130/80 mmHg in patients with diabetes or renal insufficiency

Systolic Blood Pressure over TIme
2008 ACC

Baseline Control Rates37.2 37.9
ACCOMPLISH: Exceptional Control Rates with Initial Combination Therapy
ACEI / HCTZN=5733
Con
trol
rate
(%)
CCB / ACEIN=5713
10
20
30
40
50
60
70
80
9078.5
81.7
P<0.001 at 30 months follow-up Control defined as <140/90 mmHg 2008 ACC

Kaplan Meier for Primary EndpointC
umul
ativ
e ev
ent r
ate
HR (95% CI): 0.80 (0.72, 0.90)
Time to 1st CV morbidity/mortality (days)
INTERIM RESULTS Mar 08
CCB / ACEI
ACEI / HCTZ
P=0.002
20% Risk Reduction
0 200 400 600 800 1000 1200 1400
0.16
0.14
0.12
0.10
0.08
0.06
0.04
0.02
0
2008 ACC
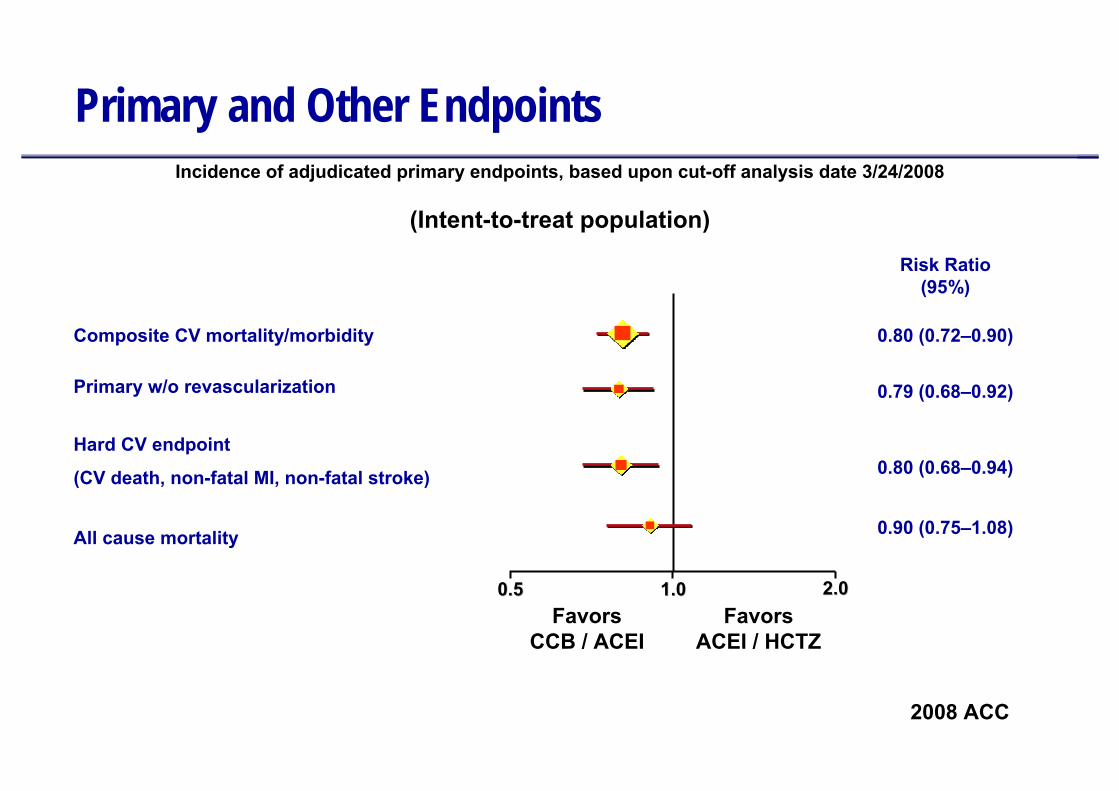
Primary and Other Endpoints
Composite CV mortality/morbidity
Primary w/o revascularization
Hard CV endpoint
(CV death, non-fatal MI, non-fatal stroke)
All cause mortality
Incidence of adjudicated primary endpoints, based upon cut-off analysis date 3/24/2008
(Intent-to-treat population)
Risk Ratio(95%)
0.80 (0.72–0.90)
0.79 (0.68–0.92)
0.80 (0.68–0.94)
0.90 (0.75–1.08)
0.50.5 1.01.0 2.02.0Favors
CCB / ACEIFavors
ACEI / HCTZ
2008 ACC

EXPRESS-C Study DesignNon-responders to Combination Therapy (Ramipril/Felodipine)
133 patients in 16 centers
Open, sequential, non-responder study including patients with moderate hypertension (160 mmHg < SBP < 180 mmHg)
Initial treatment: ramipril 5 mg + felodipine 5 mg (highest permitted dosage in fixed-dosecombination)
Uncontrolled patients (n=105) (SBP >140 mmHg) were treated with Amlodipine/Valsartan 10/160 mg for another 5 weeks
Wash-outphase
1–2 weeks
Studystart
Week 1 Week 10
Ramipril 5 mg + Felodipine 5 mg
Amlodipine/Valsartan10/160 mg
Ramipril5 mg
Week 5
Trenkwalder et al. DMW 2006;131:S164

96.6
89.3
82.380
90
100
Mea
n di
asto
lic B
P (m
mH
g)
136
151.4
166.7
120
140
160
180
Mea
n sy
stol
ic B
P (m
mH
g)Additional Reduction in BP with Amlodipine/Valsartan inNon-responders to Ramipril/Felodipine
–30.7 mmHg–14.3 mmHg
–15.4 mmHgp<0.0001 –7.0 mmHg
p<0.0001
Week 0 5 10
N=133
AfterAmlo/Val 10/160
After Ram 5 + Fel 5
Open, sequential, non-responder, 10-week study Trenkwalder et al. DMW 2006;131:S164
AfterAmlo/Val 10/160
After Ram 5 + Fel 5
Week 0 5 10

VALUE Suggests Immediate BP Control Reduce Cardiac M&M
Fatal/Non-fatal cardiac events
Fatal/Non-fatal stroke
All-cause death
Myocardial infarction
Heart failure hospitalizations
0.4 0.6 0.8 1.0 1.2 1.4Immediate responders*
(n = 9336)Non-immediate responders
(n = 5663)
Odds Ratio 95% CI
*Those not on previous treatment: SBP ↓ ≥10 mmHg at one month; those on previous treatement: SBP ≤ baseline at one month.**P < 0.05; †P < 0.01.
Pooled Treatment Groups
**
†
**
0.88 (0.79–0.97)
0.83 (0.71–0.98)
0.90 (0.81–0.99)
0.89 (0.76–1.04)
0.87 (0.75–1.01)
Odds Ratio
Weber MA et al. Lancet. 2004;363:2047–49.

SHIFT : The Art of Combination Therapy
Adapted from European Society for Hypertension-European Society of Cardiology Guidelines Committee.JHypertens. 2003;21:1011–1053.
Thiazide Diuretics
ACEIs
β-blockers ARBs
α-blockersCCBs
ACEI or
ARB
Diuretic Thiazide
CCB
β-B
ACCOMPLISHESH-ESC
Park JB 2008 Apr
young
old
RecommendPermissiblelittle recommend
20082007

Many Advantages of Combinations “ARB + CCB”Over Monotherapy for Hypertension
Improved CV outcomes
Increased potential for end-organ protection
Efficacy Safety Compliance+ +Faster achievement
of target BPHigher control rates
Potential for fewer side effects
Improved compliance by simple, convenient
regimen
conclusion



























![> > [ARB Title] [Work Order #] [ARB Date]](https://img.pdfslide.net/doc/110x75/56649d305503460f94a093ec/wwwdpwstatepaus-wwwdhsstatepaus-arb-title-work-order-arb.jpg)

