Embed Size (px)
Citation preview
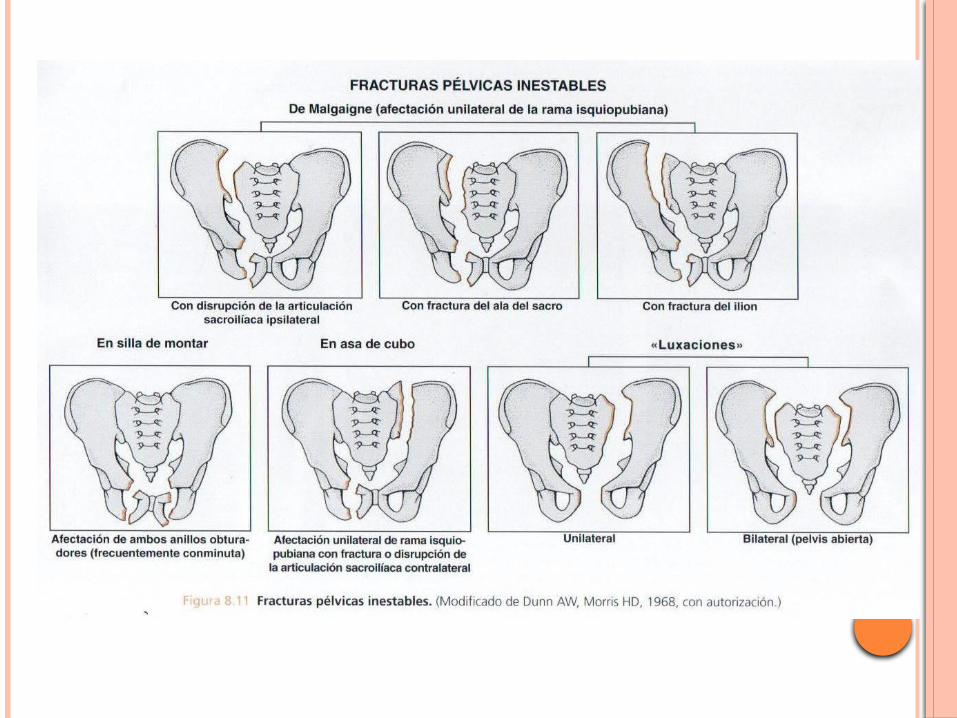
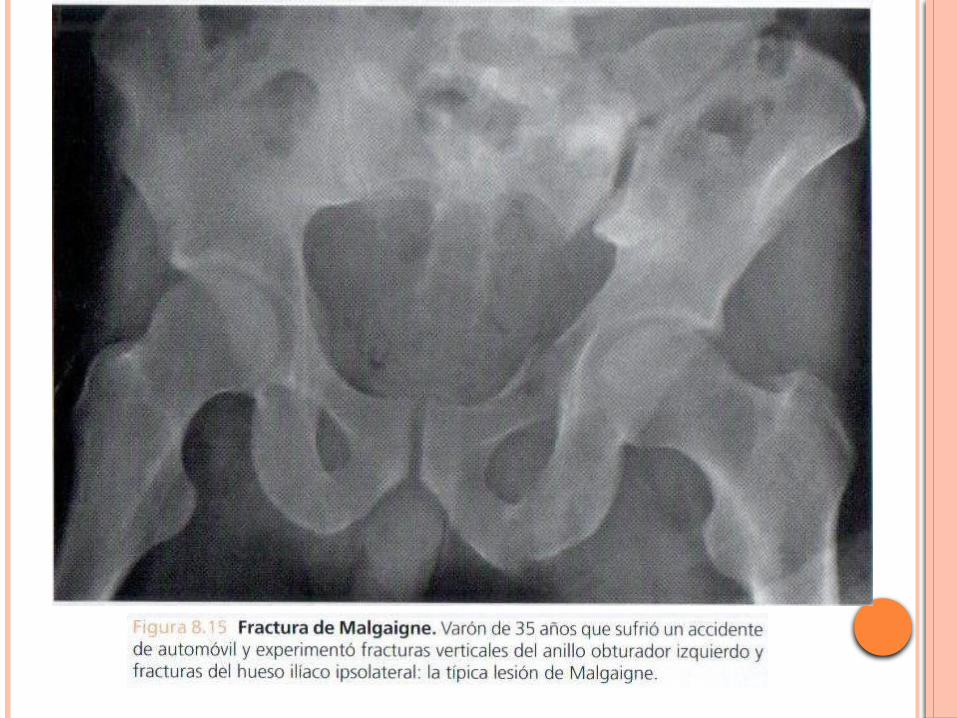
FRACTURAS DE PELVISMR Machicao Justo Jonathan
Traumatología y Ortopedia
Enero 2012
HNERM
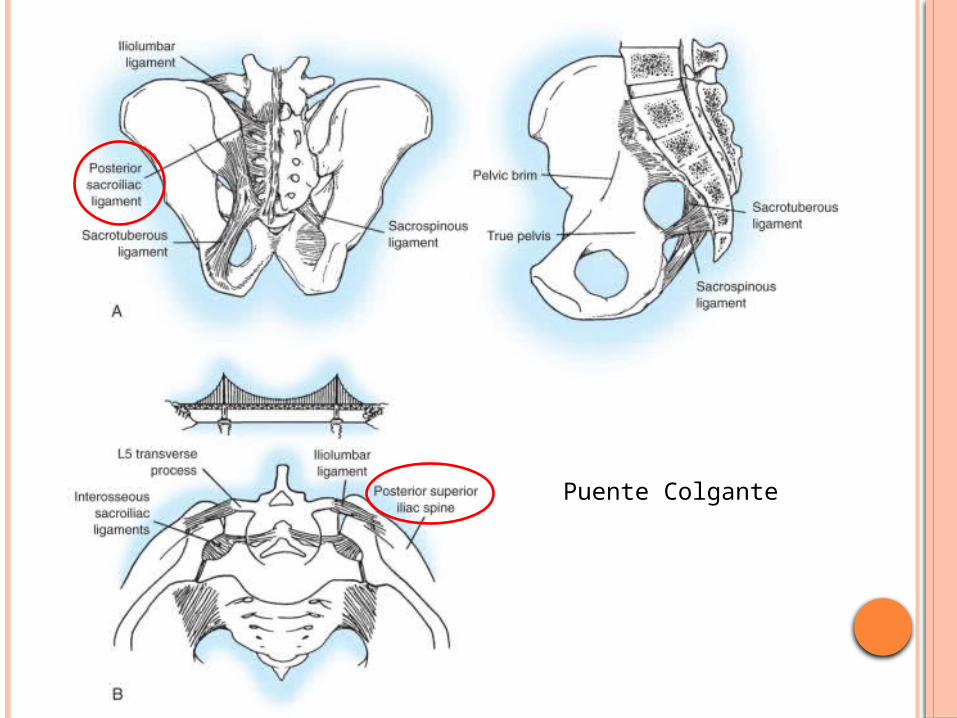
Puente Colgante
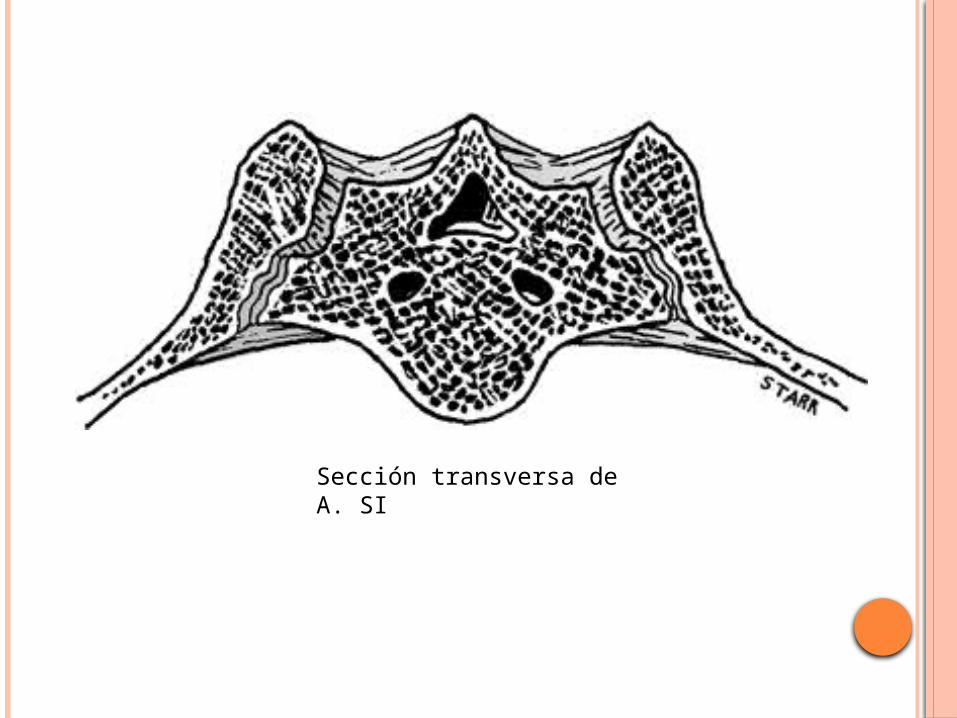
Sección transversa de A. SI
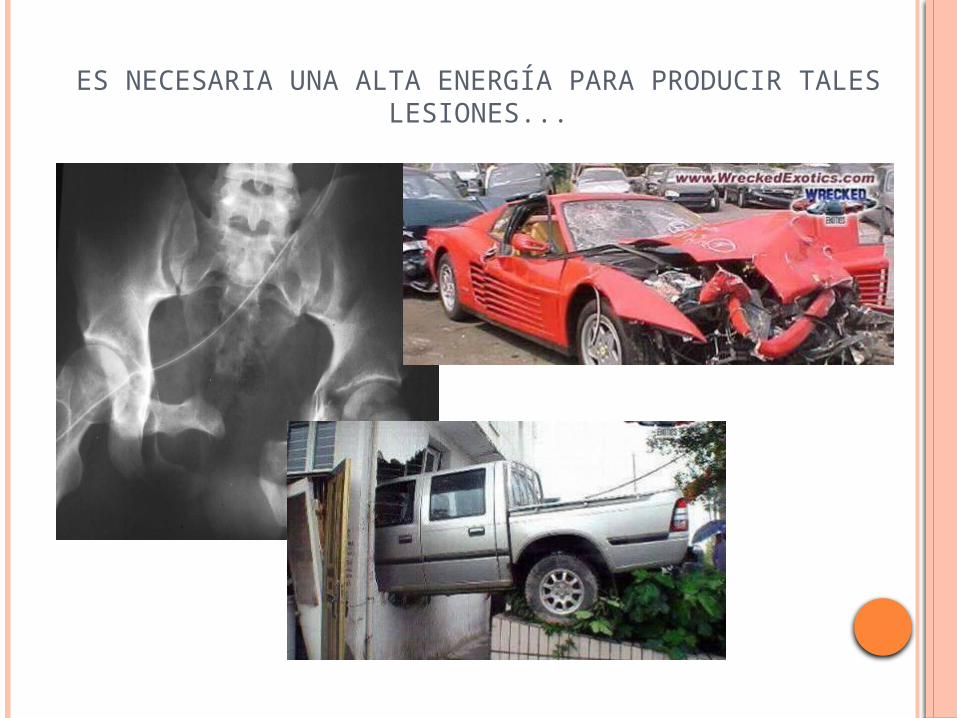
ES NECESARIA UNA ALTA ENERGÍA PARA PRODUCIR TALES LESIONES...

EXAMEN FÍSICO
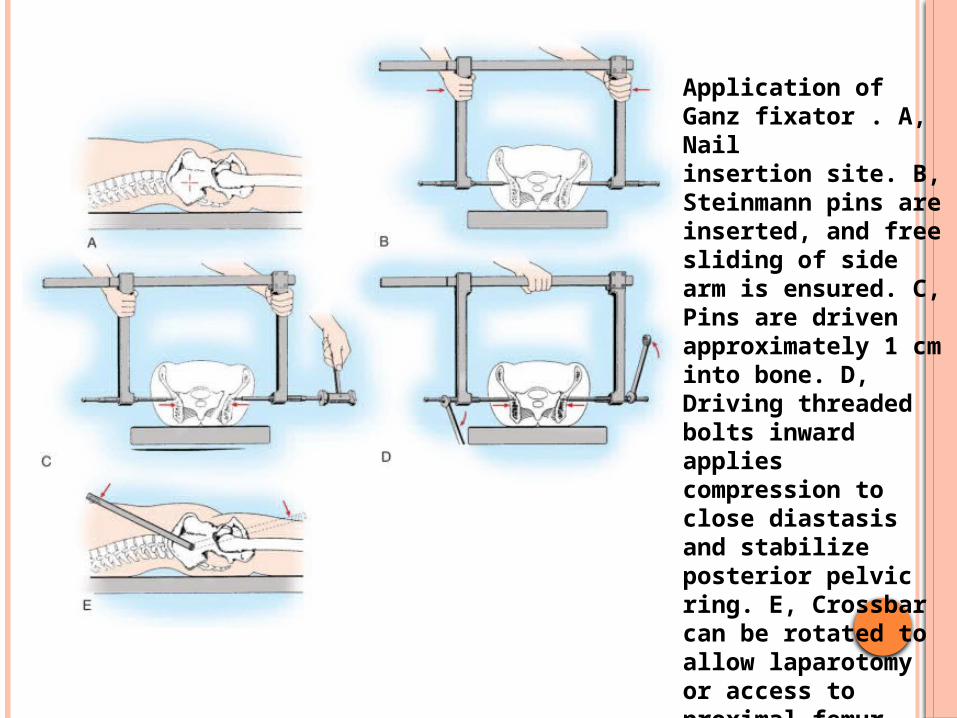
Application of Ganz fixator . A, Nail insertion site. B, Steinmann pins are inserted, and free sliding of side arm is ensured. C, Pins are driven approximately 1 cm into bone. D, Driving threaded bolts inward applies compression to close diastasis and stabilize posterior pelvic ring. E, Crossbar can be rotated to allow laparotomy or access to proximal femur
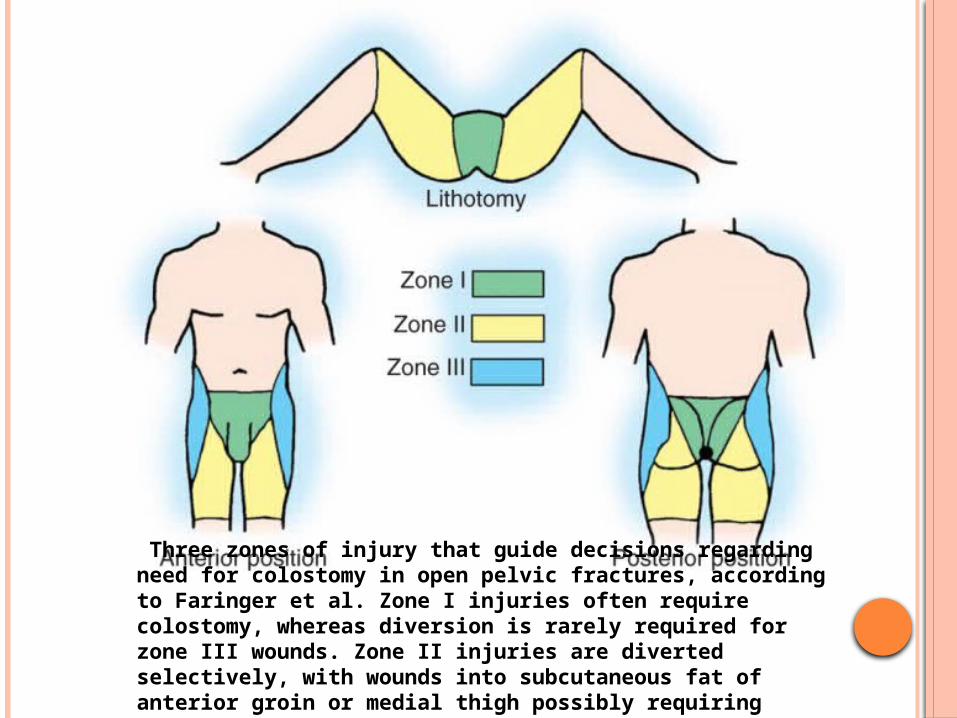
Three zones of injury that guide decisions regarding need for colostomy in open pelvic fractures, according to Faringer et al. Zone I injuries often require colostomy, whereas diversion is rarely required for zone III wounds. Zone II injuries are diverted selectively, with wounds into subcutaneous fat of anterior groin or medial thigh possibly requiring colostomy.
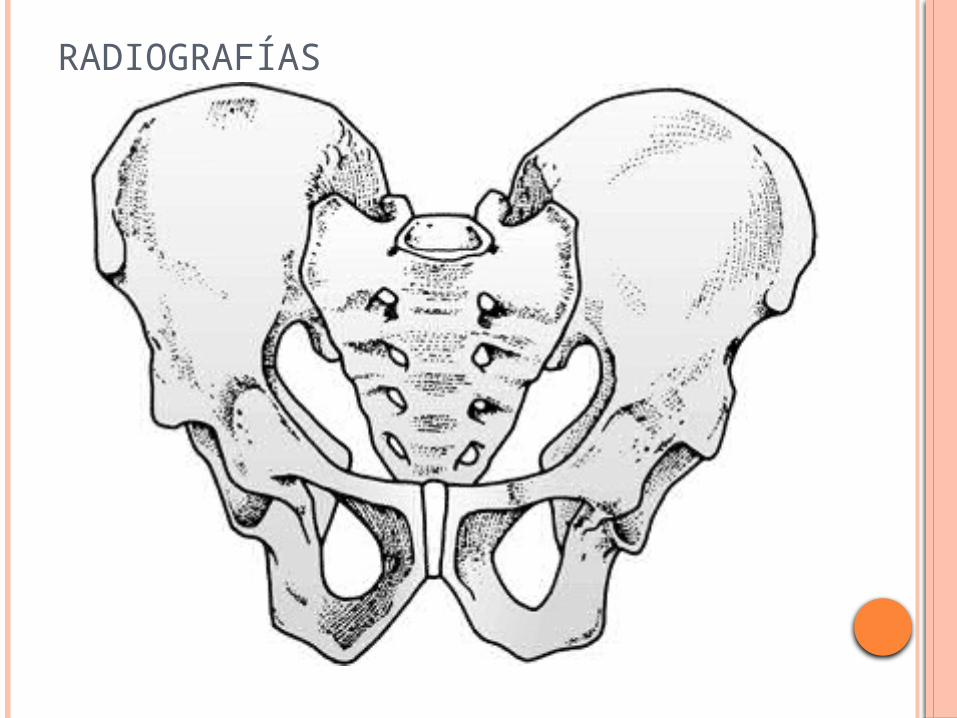
RADIOGRAFÍAS
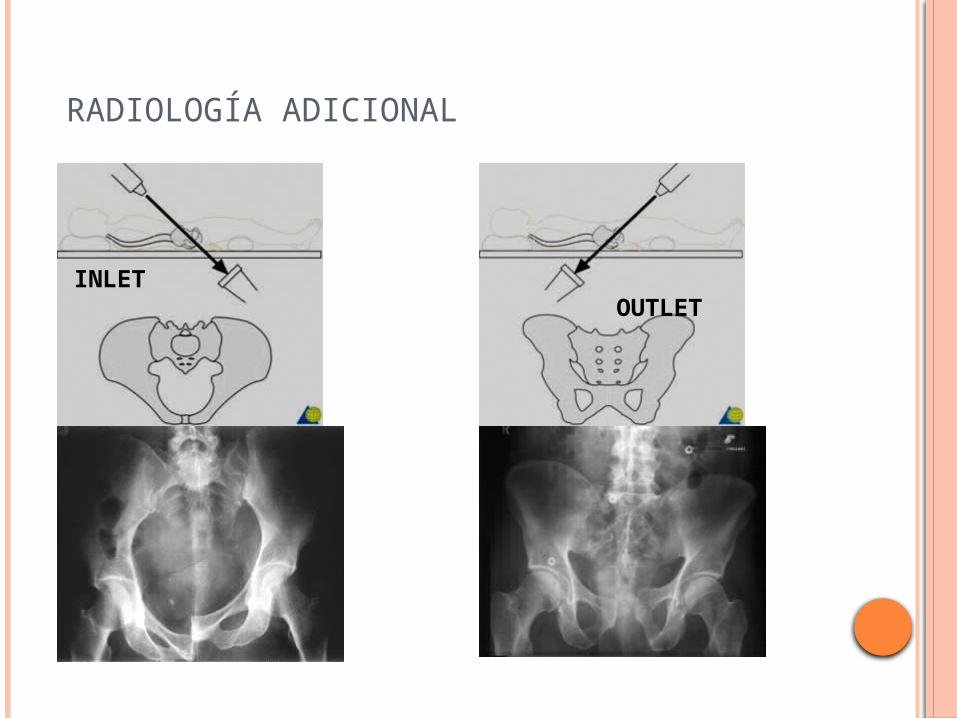
RADIOLOGÍA ADICIONAL
INLET OUTLET
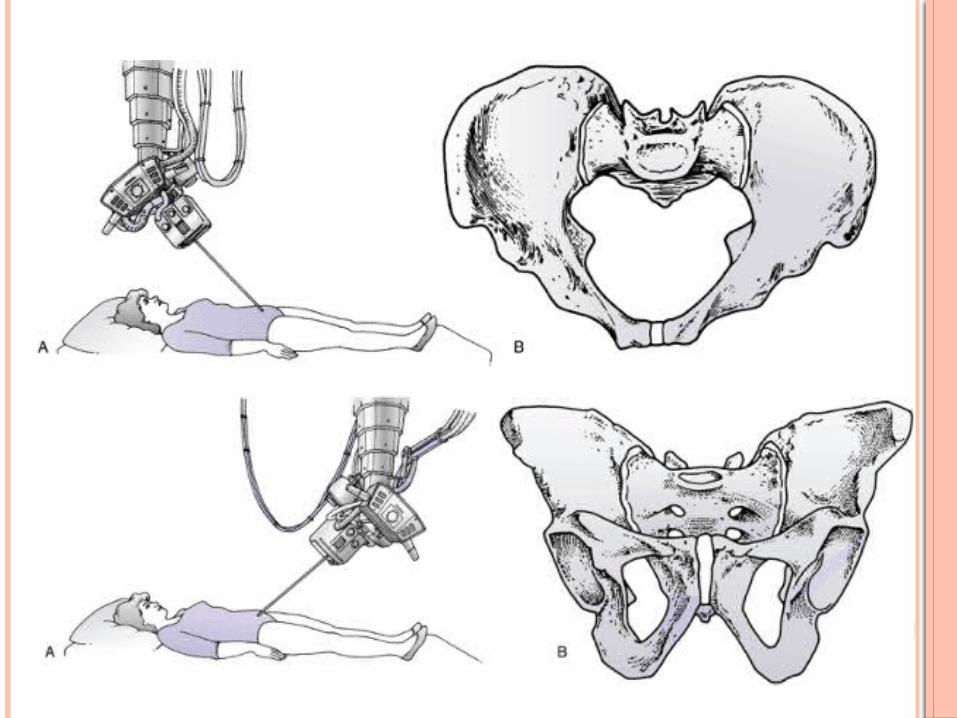
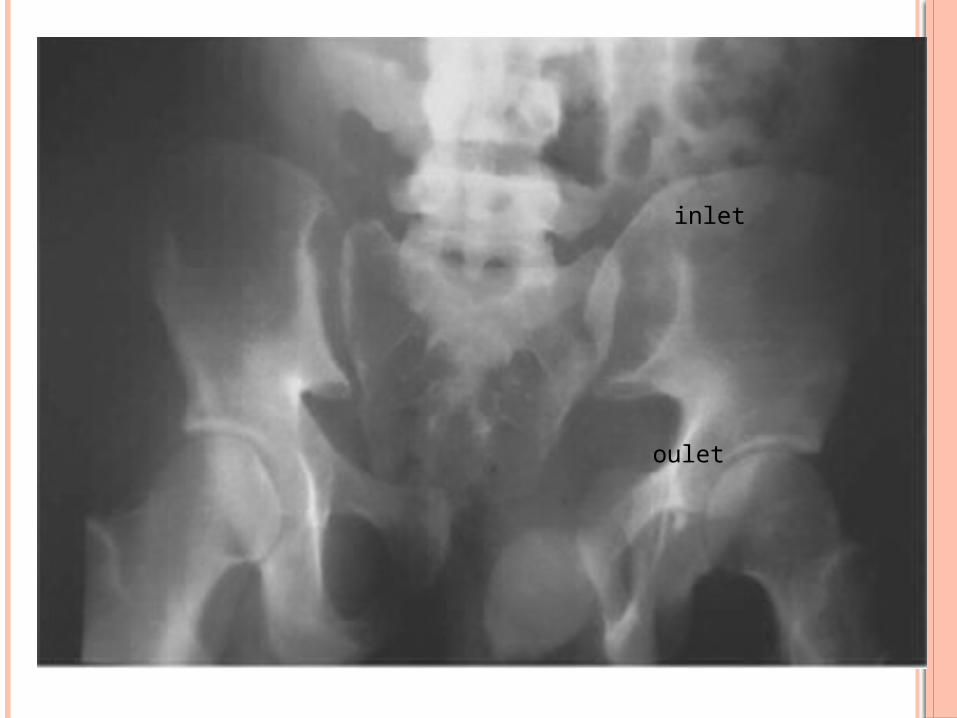
oulet
inlet

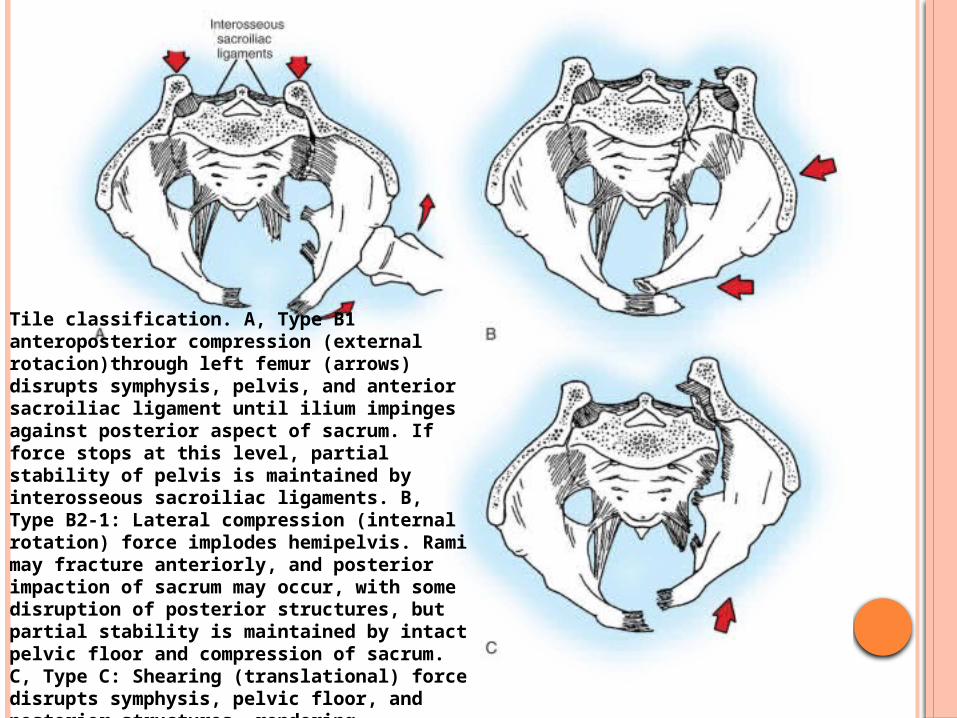
Tile classification. A, Type B1 anteroposterior compression (external rotacion)through left femur (arrows) disrupts symphysis, pelvis, and anterior sacroiliac ligament until ilium impinges against posterior aspect of sacrum. If force stops at this level, partial stability of pelvis is maintained by interosseous sacroiliac ligaments. B, Type B2-1: Lateral compression (internal rotation) force implodes hemipelvis. Rami may fracture anteriorly, and posterior impaction of sacrum may occur, with some disruption of posterior structures, but partial stability is maintained by intact pelvic floor and compression of sacrum. C, Type C: Shearing (translational) force disrupts symphysis, pelvic floor, and posterior structures, rendering hemipelvis completely unstable.
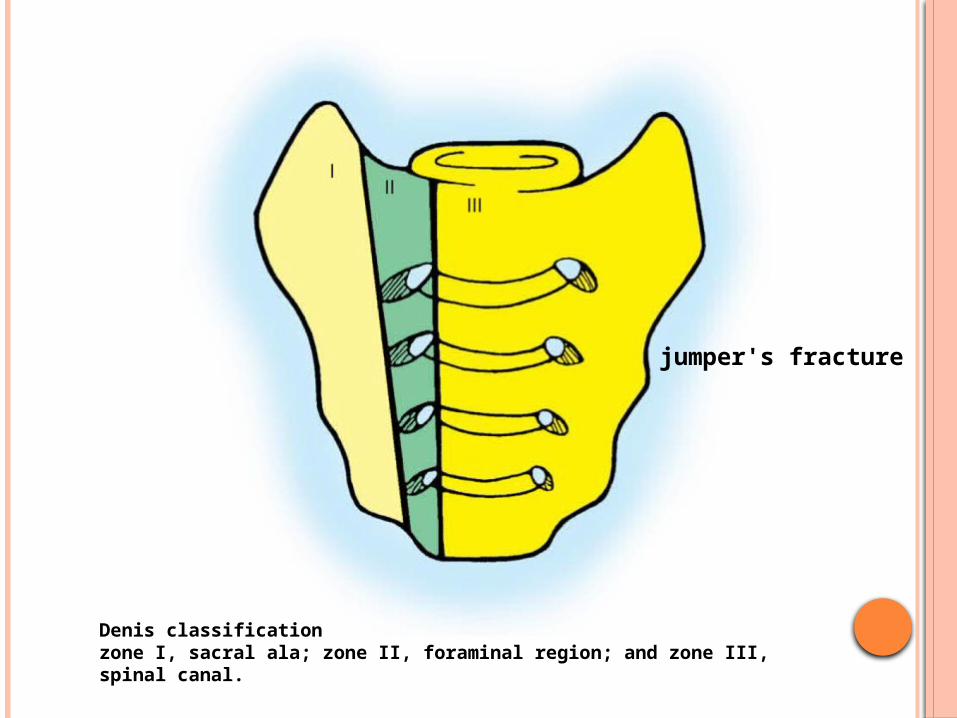
Denis classification zone I, sacral ala; zone II, foraminal region; and zone III, spinal canal.
jumper's fracture

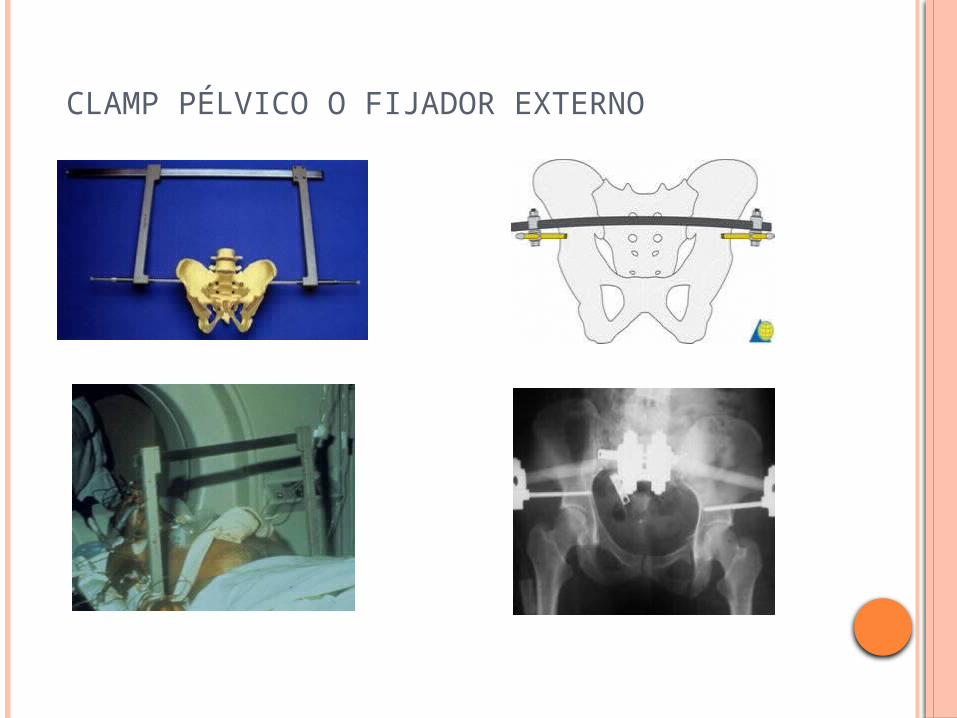
CLAMP PÉLVICO O FIJADOR EXTERNO
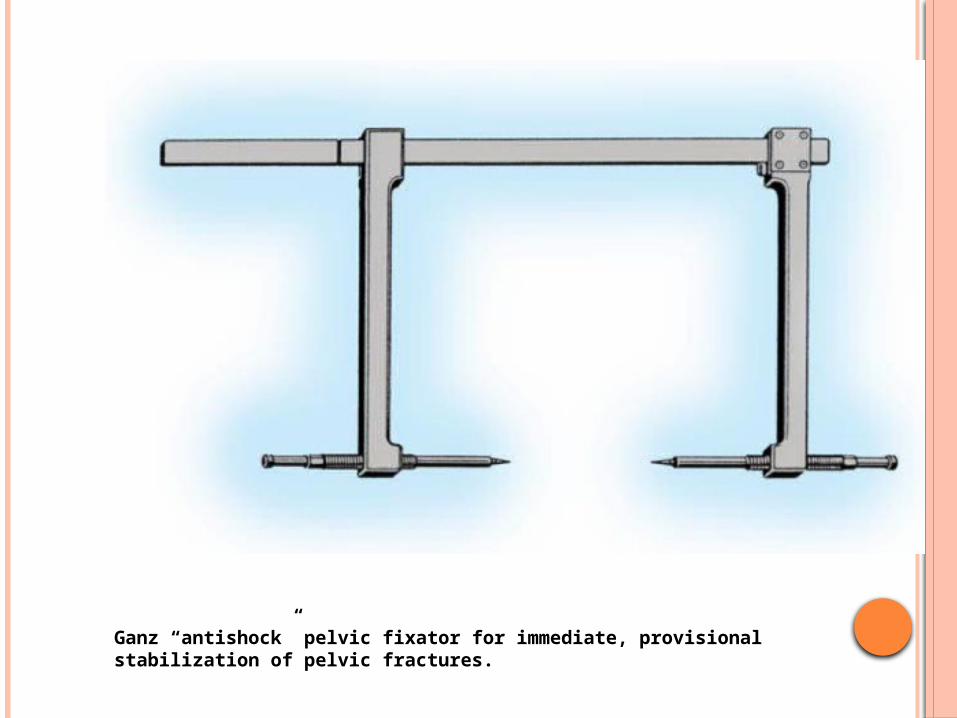
Ganz “antishock” pelvic fixator for immediate, provisional stabilization of pelvic fractures.
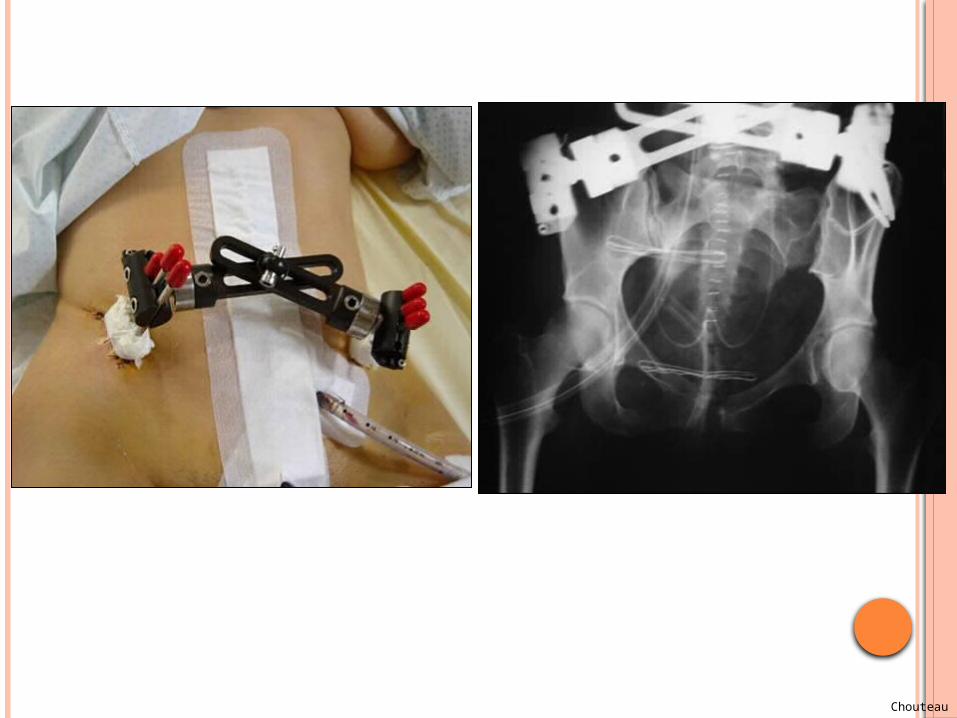
Chouteau

Iliosacral screw fixation for sacroiliac or sacral fracture
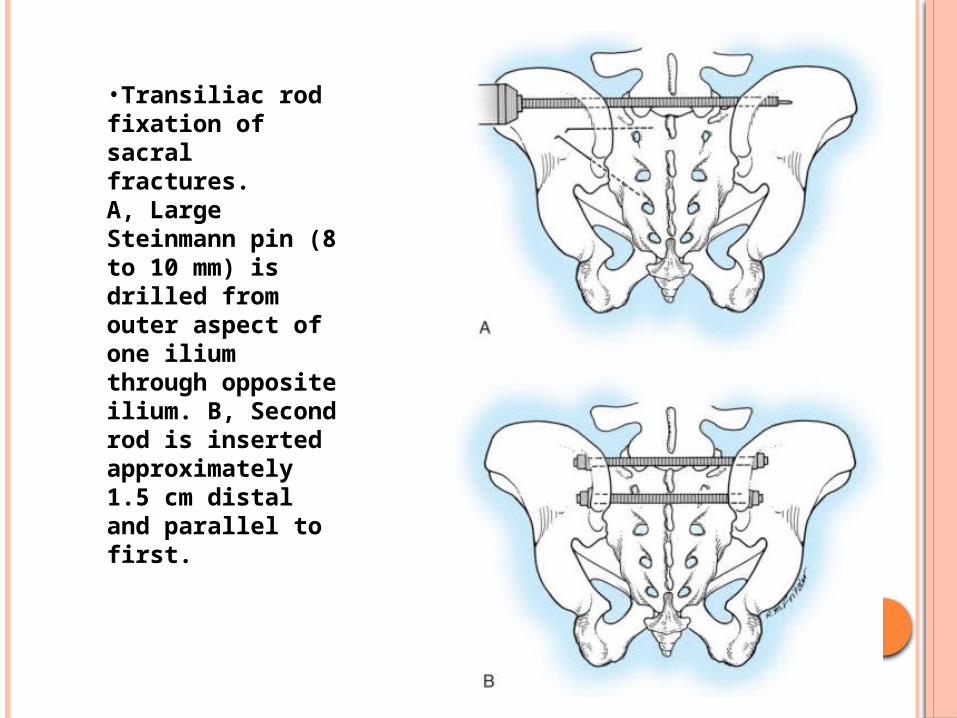
•Transiliac rod fixation of sacral fractures. A, Large Steinmann pin (8 to 10 mm) is drilled from outer aspect of one ilium through opposite ilium. B, Second rod is inserted approximately 1.5 cm distal and parallel to first.
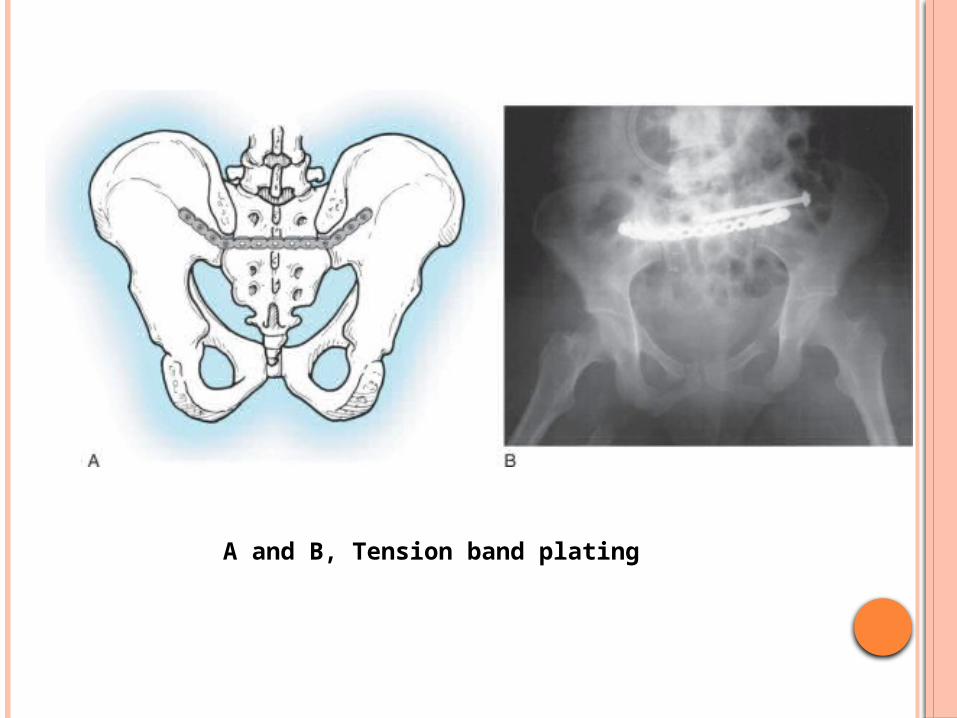
A and B, Tension band plating