Embed Size (px)
Citation preview
, . 182: 311–317 (1997)
EXPRESSION OF CYTOTOXIC MOLECULES ININTESTINAL T-CELL LYMPHOMAS
1, - 2*, 2, 1, 2, 2, - 1, 2
- **1Department of Gastroenterology, Klinikum Benjamin Franklin, Free University of Berlin, Hindenburgdamm 30, 12200 Berlin,
Germany2Konsultations- und Referenzzentrum für Lymphknoten und Hämatopathologie supported by the Deutsche Krebshilfe (grant
M25/89/St1) at the Institute of Pathology, Klinikum Benjamin Franklin, 12200 Berlin, Germany
SUMMARY
Intestinal T-cell lymphoma (ITCL) represents a subgroup of peripheral T-cell lymphomas which is thought to arise from áâintraepithelial T-lymphocytes. Since these lymphocytes may contain cytotoxic molecules, the question of whether this also holds true forITCL arises. Twenty ITCL cases were examined for the presence of granzyme B, perforin, and T-cell-restricted intracellular antigen(TIA-1)/granule membrane protein of 17 kD (GMP-17). Two molecules with restricted expression in cytotoxic cells, granzyme B andperforin, were detected by immunocytochemistry and by in situ hybridization with an isotopically labelled RNA probe, respectively.Immunocytochemistry was also performed with the antibody 2G9, which recognizes two molecules, one expressed by cytotoxic cells(TIA-1) and the other found in granulocytes and cytotoxic cells (GMP-17). Granzyme B, TIA-1/GMP-17, and perforin were found inthe neoplastic cells of 16/19 cases, 19/20 cases, and 16/17 cases, respectively, of ITCL, but not in the tumour cells of the control group,which consisted of intestinal B-cell lymphomas (five cases) and CD8-negative peripheral nodal T-cell lymphomas (six cases). At least oneof these molecules was expressed in the tumour cells of all ITCL cases. 2G9 proved to be the most sensitive immunohistological marker,since reactivity with this antibody was not only observed in the highest number of cases, but also found in high numbers of neoplastic cellsin positive cases. In conclusion, ITCL appears to show cytotoxic differentiation in all cases. In conjunction with immunophenotypicand genotypic data, our results support a uniform derivation of this tumour from intraepithelial áâ cytotoxic T-lymphocytes. ? 1997 byJohn Wiley & Sons, Ltd.
J. Pathol. 182: 311–317, 1997.No. of Figures 1. No of Tables 2. No. of References 31.
KEY WORDS—intestinal T-cell lymphoma
INTRODUCTION
Intestinal T-cell lymphoma (ITCL) is a rare specificsubtype of peripheral T-cell lymphoma, predominantlyarising in the small intestine.1,2 It occurs in adults, oftenin patients with a history of coeliac disease, occasionallyas the initial event in a patient with histological featuresof this disease, or less commonly without evidence ofenteropathy.1,2 Histologically, ITCL is in most cases ahigh-grade lymphoma and demonstrates prominent epi-theliotropism.1 Immunophenotypically, ITCL expressesT-cell antigens (such as CD3 and CD7) in conjunctionwith CD103,3–5 an antigen largely restricted to intra-epithelial T-lymphocytes (IELs) of the intestine.6 Thesecells are thought to represent the normal counterpart ofITCL, as they have a similar immunophenotype.1,2 Most
IELs are probably cytotoxic T-cells, since they displaycytotoxic functions7,8 and may contain cytotoxicmolecules.9,10Among the wealth of cytotoxic molecules, perforin
and granzyme B are two well-characterized pro-teins involved in one major pathway leading toapoptosis.11–14 Perforin allows for the entry of granzymemolecules into the target cells, which then activate theapoptotic protease CPP32.15 The genes for perforin16and granzyme B12 have been cloned and antibodiesdirected against these molecules have been generated.17T-cell-restricted intracellular antigen (TIA)-1, anothermolecule found in cytotoxic cells, is recognized by theantibody 2G9.18 The precise function of TIA-1 has notbeen elucidated. Since it induces DNA fragmentation ofdigitonin-permeabilized thymocytes,19 it may be impli-cated in the killing induced by cytotoxic lymphocytes.More recently, the antibody 2G9 has been demonstratedto react also with another protein, termed GMP-17(granule membrane protein of 17 kD), which is found inthe membrane of the granules of neutrophils and cyto-toxic cells.20 The biological function of this secondmolecule is not well characterized.20 With the exceptionof neutrophils, which are morphologically easily distin-guishable from lymphoid cells, the expression of all ofthe above-mentioned molecules appears to be largely
*Correspondence to: Dr med. H.-D. Foss, Institute of Pathology,Klinikum Benjamin Franklin, Hindenburgdamm 30, 12200 Berlin,Germany.
**The members of the German Study Group on IntestinalNon-Hodgkin Lymphoma are listed in the Appendix.
Severin Daum and Hans-Dieter Foss contributed equally to thiswork.
Contract grant sponsor: Deutsche Forschungsgemeinschaft;Contract grant numbers: Ste 318/5-I and Da 102/2-1.
CCC 0022–3417/97/070311–07 $17.50 Received 19 November 1996? 1997 by John Wiley & Sons, Ltd. Accepted 5 March 1997

restricted to cytotoxic cells.11–13,18,21 Analysis of theexpression of these antigens in conjunction with othermarker molecules can therefore further specify the cel-lular origin of lymphocytes and lymphoid malignancies.Among the above-mentioned molecules, perforin and
TIA-1/GMP-17 have been detected in resting IELs.9,22In contrast, granzyme B is not found in resting IELsof normal small bowel, but only in IELs present indiseased small bowel, such as in gluten-sensitive entero-pathy, an expression pattern most likely reflecting itsrestricted expression in activated cytotoxic T-cells.10 Adetailed analysis of ITCL for the expression of cytotoxicmolecules has not been performed up to now. In onlyone study,23 granzyme B was found to be expressed onlyin a proportion of the cases investigated. However,granzyme B, with its restricted expression in activatedcytotoxic T-cells, may not be the most sensitive moleculefor the detection of cytotoxic potential in lymphomasand this study may have thus underestimated the pro-portion of ITCLs being derived from cytotoxic cells. Toclarify this issue and to characterize ITCL more fully,we examined a large series of these tumours for thepresence of several cytotoxic molecules. This includedthe immunocytochemical detection of granzyme B andTIA-1/GMP-17, as well as in situ hybridization for thedetection of perforin expression.
MATERIALS AND METHODS
MaterialsFormol-fixed/paraffin-embedded material of 25
samples from 20 cases of ITCL, including 24 resection
specimens and one biopsy specimen, were drawnfrom the archives of the Institute of Pathology of theUniversitätsklinikum Benjamin Franklin, Berlin (for theclinical findings and histological findings of the grosslyuninvolved mucosa, see Table I). These included tencases which were collected during the German multi-centre intestinal lymphoma study. In all cases, theprimary localization was small intestine. Five cases ofintestinal B-cell lymphomas served as a control group,including four cases of Burkitt’s or Burkitt’s-likelymphoma and one case of mantle cell lymphoma. Sevennodal cases of peripheral T-cell lymphomas unspecified(large cell type) and one case of angiocentric T-celllymphoma were also included as controls. Granzyme Band perforin expression of the latter was investigated ina earlier study.24 The diagnosis of all the lympho-mas was made according to the criteria of the REALclassification.2
Immunohistology
Four-micrometre sections of paraffin-embedded tissueblocks were stained employing the immunoalkalinephosphate (APAAP) method.25 The primary mono-clonal antibodies were Ber-H2 (CD30), L26 (CD20),âF1 (T-cell antigen receptor â-chain), PGM-1 and KP-1(CD68), C3D1 (CD15), and E29 (epithelial membraneantigen). For the detection of CD3, a polyclonal anti-body was used. With the exception of âF1, which wasfrom T-Cell Sciences, Cambridge, MA, U.S.A., and amonoclonal anti-CD8 antibody (C8-144), which was agift from Dr D. Mason, Oxford, U.K., all antibodies
Table I—Intestinal T-cell lymphomas: clinical data and histological findings in the macroscopically uninvolved mucosa
CaseNo. Sex
Age(years)
Coeliacdisease Enteropathy
Villousatrophy
HighIEL Localization Stage
Clinicalpresentation
1 m 68 " + + + Jejunum EII Malabsorption2 f 61 " " " nk Jejunum EIII Perforation3 m 67 " " " nk Jejunum nk Perforation4 f 52 nk nk + + Small intestine nk nk5 m 52 DH " + + Ileum EIV Perforation6 m 35 + nk + + Small bowel nk Perforation7 f 73 " " " " Jejunum EII Perforation8 f 53 + + + + Duodenum jejunum EIV Malabsorption9 f 72 + + + + Jejunum EI Malabsorption10 m 50 " " " + Jejunum EII Intestinal stenosis11 f 71 + " + + Duodenum jejunum EIII Ileus12 m 56 " " + + Jejunum nk Perforation13 f 69 " " + + Ileum EIII Abdominal pain14 f 71 " + + + Ileum EII Perforation15 m 69 " " + + Ileum EII Perforation16 f 54 " " + + Duodenum jejunum EI Abdominal pain17 f 84 " nk " + Jejunum nk nk18 f 52 nk " " " Duodenum ileum EII Gastrointestinal bleeding19 m 56 + + + + Ileum EIV Malabsorption20 f 48 + + + nk Jejunum EIII Malabsorption
Coeliac disease was defined as proposed previously30 using typical initial histology and clear-cut clinical remission on a strict gluten-free diet ascritica. Enteropathy was defined by positive findings in clinical tests for malabsorption irrespective of histological demonstration of villous atrophy.High IEL denotes increased numbers of intraepithelial lymphocytes. Stage is defined according to the Ann-Arbor classification with themodifications proposed by Musshoff and Schmidt-Vollmer.31
f=female; m=male; nk=not known; DH=dermatitis herpetiformis.
312 S. DAUM ET AL.
? 1997 by John Wiley & Sons, Ltd. , . 182: 311–317 (1997)

were purchased from DAKO, Glostrup, Denmark. Theantibody against granzyme B (GrB7)17,26 waskindly provided by Dr Kummer, Amsterdam, TheNetherlands, and used in a concentration of 1:500.The antibody (2G9) specific for TIA-1 and GMP-17was purchased from Coulter Immunology, CoulterCorporation, Hialeah, FL, U.S.A. All antibodies exceptâF1, which required proteolytic digestion, were appliedafter a high pressure cooking pretreatment for antigenretrieval in a 10 m citrate buffer, pH 6·0. For thedetection of granzyme B, the biotin streptavidin methodwas used.
Plasmids
The cDNA probe was prepared by the subcloning of aperforin cDNA fragment (length 929 bp),16 kindly pro-vided by Dr M. G. Lichtenheld, Department of Micro-biology and Immunology, University of Miami, in therun-off transcription vector pAMP1 (Gibco-BRL, LifeTechnology, Gaithersburg, U.S.A.). This probe com-prises exon 2 and exon 3 sequences. The nucleic acidsequence of the probe was determined on the DNAsequencer 373A (Applied Biosystems, Foster City,U.S.A.) and proved to conform to published data.16
In situ hybridization
After linearization, 35S-labelled run-off anti-sense andsense (control) transcripts were generated using T7 orSP6 RNA polymerases (Promega-Biotech, Madison,WI, U.S.A.). In situ hybridization for the detection ofperforin transcripts was performed as described pre-viously.27 In brief, dewaxed and rehydrated paraffinsections were exposed to 0·2 HCl and 0·125 mg/mlpronase (Boehringer, Mannheim, Germany), followedby acetylation with 0·1 triethanolamine, pH 8·0/0·25 per cent (v/v) acetic anhydride and dehydrationthrough graded ethanols. Slides were hybridised to2–4#105 cpm of labelled probes overnight at 50)C.Washing and autoradiography were carried out asdescribed previously.27
Evaluation
For in situ hybridization, cells containing more than20 grains were scored positive; this corresponded in allcases to more than four times the background signal. Acase was regarded as positive when there was un-equivocal staining of neoplastic cells. This includedeither staining of large atypical lymphoid cells or in thecases with small to medium-sized tumour cells, thepresence of at least focal labelling of the majority ofinfiltrating cells, including atypical cells.
RESULTS
TIA-1/GMP-17Reactivity with the antibody 2G9, which recognizes
both TIA-1 and GMP-17, was observed in the tumourcells of 24/25 samples (19/20 cases) of ITCL and in 2/2 of
CD8-positive non-ITCL peripheral T-cell lymphomacases (Table II and Fig. 1a). The labelling was typicallycytoplasmic and granular. In most cases, the majority oftumour cells were stained and labelling was also foundin a high proportion of the small IELs observed in theadjacent mucosa (Fig. 1b). In B-cell lymphomas andCD8-negative nodal peripheral T-cell lymphomas, 2G9reactivity was observed in only a variable proportion ofreactive lymphoid cells, but not in the neoplastic cells(Fig. 1c). Labelling was also found in the majorityof neutrophil granulocytes, but not in other cell types ofthe intestinal wall.
Granzyme B
This molecule was detected in the tumour cells of16/19 cases (19/22 samples) of ITCL (Table II andFig. 1d). In contradistinction to TIA-1/GMP-17, expres-sion of this molecule was observed in most cases, butonly in a minority of neoplastic cells. In some cases ofgranzyme B-positive tumour cells were only foundbeneath areas of ulceration or adjacent to suppurativeperitonitis related to perforation. The proportion ofIELs in the adjacent mucosa containing granzyme B(Fig. 1e) was substantially lower than IELs containingTIA-1. In B-cell lymphomas, granzyme B was restrictedto reactive cells (Fig. 1f). As reported earlier, amongnon-ITCL peripheral T-cell lymphomas,24 only the neo-plastic cells of two CD8-positive cases were labelled, butnot those of the CD8-negative cases.
Perforin
Transcripts specific for perforin were observed in thetumour cells of 18/20 samples (16/17 cases) of ITCL(Table II and Fig. 1g). Similarly to TIA-1/GMP 17,perforin was often found in the majority of tumour cellsand intraepithelial lymphocytes in the surroundingmucosa (Fig. 1h). As described earlier24 among non-ITCL peripheral T-cell lymphoma cases, only theneoplastic cells of two CD8-positive, but not those ofsix CD8-negative cases, contained perforin transcripts.As for TIA-1/GMP-17 and granzyme B, expression ofthis molecule was observed in reactive cells but notin neoplastic cells in five cases of intestinal B-celllymphomas.
DISCUSSION
IELs of the small intestine are mainly cytotoxic cells28and may express several cytotoxic molecules includingperforin,22 TIA-1/GMP-17,9 and in diseased intestine,granzyme B.10 ITCL is thought to be derived from theseIELs.1,2 Expression of cytotoxic molecules in this lym-phoma entity has not been well characterized; up to thepresent, ITCL cases have been analysed only forgranzyme B expression,23 a serine protease present in thecytotoxic granules of activated cytotoxic T-cells andnatural killer cells.12 The reported data showinggranzyme B expression only in a proportion of ITCLs23are not conclusive, as they imply either a heterogeneous
313EXPRESSION OF CYTOTOXIC MOLECULES IN ITCLs
? 1997 by John Wiley & Sons, Ltd. , . 182: 311–317 (1997)
origin of this lymphoma or a derivation from cytotoxicT-cells of different activation stages.To clarify which of these alternatives applies and to
characterise ITCL more fully, we investigated thesetumours for a broader panel of cytotoxic molecules. Byimmunocytochemistry, granzyme B and TIA-1GMP-17were found in the neoplastic cells of 16/19 cases and19/20 cases, respectively, of ITCL. In situ hybridizationrevealed expression of perforin in 16/17 ITCL cases. Inthe control group consisting of intestinal B-cell lympho-mas and CD8-negative nodal peripheral T-cell lympho-mas, expression of all of these molecules was observedonly in reactive lymphocytes but not in the tumour cells,whereas two cases of CD8-positive peripheral T-celllymphomas other than ITCL contained all three of thesemolecules.Our data concerning the expression of granzyme B in
ITCL, with approximately 84 per cent of cases beingpositive, are not fully in agreement with those obtainedby de Bruin et al.23 They observed this molecule in 43per cent of primary gastrointestinal T-cell lymphomas
and 70 per cent of enteropathy-associated TCLs(EATCL) and EATCL-like TCLs, according to theclassification of Chott et al.3 However, our data andtheirs are not fully comparable, as the lymphoma clas-sifications applied are not identical. Furthermore, differ-ent evaluation criteria and, because granzyme Bexpression may occur in a minority of tumour cells, theamount of tissue investigated may account for thedifferent results. Independently of the precise reason forthe above difference, our data concerning granzyme Bexpression are corroborated by the high frequency ofexpression of other cytotoxic molecules, such as TIA-1/GMP-17 and perforin in ITCL.2G9 reactivity, indicating the presence of TIA-118 or
GMP-1720, was found in all except one of the ITCLcases and was therefore more sensitive in the detectionof cytotoxic differentiation than granzyme B expression.Furthermore, the number of labelled cells was generallyhigher than with the granzyme B antibody. These find-ings may to some extent reflect the expression pattern ofIELs, with constitutive expression of TIA-1/GMP-17,9
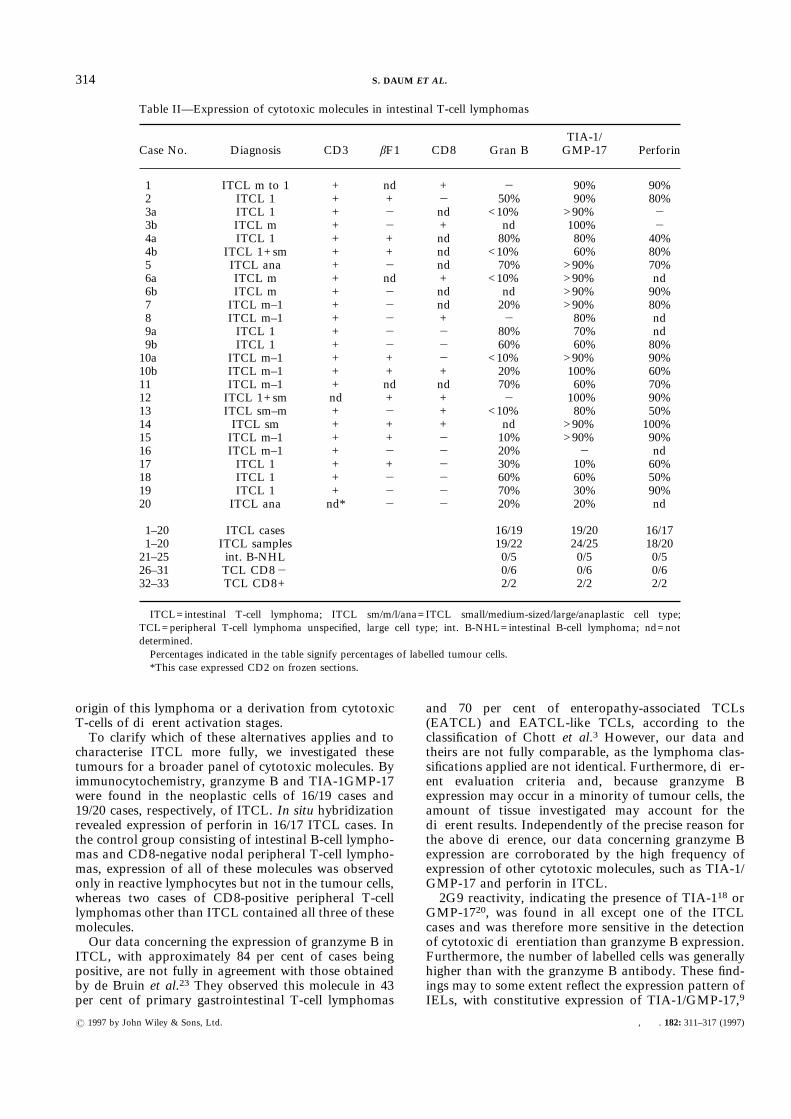
Table II—Expression of cytotoxic molecules in intestinal T-cell lymphomas
Case No. Diagnosis CD3 âF1 CD8 Gran BTIA-1/GMP-17 Perforin
1 ITCL m to 1 + nd + " 90% 90%2 ITCL 1 + + " 50% 90% 80%3a ITCL 1 + " nd <10% >90% "3b ITCL m + " + nd 100% "4a ITCL 1 + + nd 80% 80% 40%4b ITCL 1+sm + + nd <10% 60% 80%5 ITCL ana + " nd 70% >90% 70%6a ITCL m + nd + <10% >90% nd6b ITCL m + " nd nd >90% 90%7 ITCL m–1 + " nd 20% >90% 80%8 ITCL m–1 + " + " 80% nd9a ITCL 1 + " " 80% 70% nd9b ITCL 1 + " " 60% 60% 80%10a ITCL m–1 + + " <10% >90% 90%10b ITCL m–1 + + + 20% 100% 60%11 ITCL m–1 + nd nd 70% 60% 70%12 ITCL 1+sm nd + + " 100% 90%13 ITCL sm–m + " + <10% 80% 50%14 ITCL sm + + + nd >90% 100%15 ITCL m–1 + + " 10% >90% 90%16 ITCL m–1 + " " 20% " nd17 ITCL 1 + + " 30% 10% 60%18 ITCL 1 + " " 60% 60% 50%19 ITCL 1 + " " 70% 30% 90%20 ITCL ana nd* " " 20% 20% nd
1–20 ITCL cases 16/19 19/20 16/171–20 ITCL samples 19/22 24/25 18/2021–25 int. B-NHL 0/5 0/5 0/526–31 TCL CD8" 0/6 0/6 0/632–33 TCL CD8+ 2/2 2/2 2/2
ITCL=intestinal T-cell lymphoma; ITCL sm/m/l/ana=ITCL small/medium-sized/large/anaplastic cell type;TCL=peripheral T-cell lymphoma unspecified, large cell type; int. B-NHL=intestinal B-cell lymphoma; nd=notdetermined.Percentages indicated in the table signify percentages of labelled tumour cells.*This case expressed CD2 on frozen sections.
314 S. DAUM ET AL.
? 1997 by John Wiley & Sons, Ltd. , . 182: 311–317 (1997)
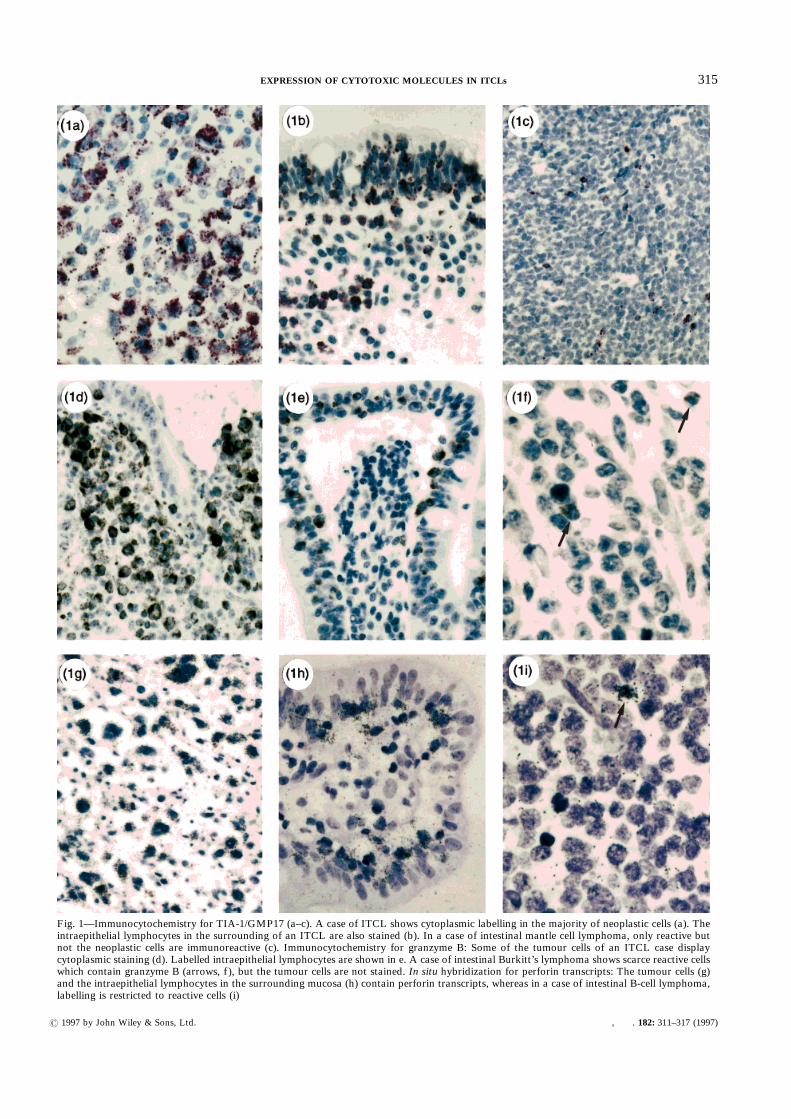
Fig. 1—Immunocytochemistry for TIA-1/GMP17 (a–c). A case of ITCL shows cytoplasmic labelling in the majority of neoplastic cells (a). Theintraepithelial lymphocytes in the surrounding of an ITCL are also stained (b). In a case of intestinal mantle cell lymphoma, only reactive butnot the neoplastic cells are immunoreactive (c). Immunocytochemistry for granzyme B: Some of the tumour cells of an ITCL case displaycytoplasmic staining (d). Labelled intraepithelial lymphocytes are shown in e. A case of intestinal Burkitt’s lymphoma shows scarce reactive cellswhich contain granzyme B (arrows, f), but the tumour cells are not stained. In situ hybridization for perforin transcripts: The tumour cells (g)and the intraepithelial lymphocytes in the surrounding mucosa (h) contain perforin transcripts, whereas in a case of intestinal B-cell lymphoma,labelling is restricted to reactive cells (i)
315EXPRESSION OF CYTOTOXIC MOLECULES IN ITCLs
? 1997 by John Wiley & Sons, Ltd. , . 182: 311–317 (1997)

but restricted expression of granzyme B in activatedstates such as in small bowel from patients with coeliacdisease.10 The frequency of perforin expression in ourITCL cases and the proportion of labelled tumour cellswere similar to those of TIA-1/GMP-17 and may againmirror the situation in normal IELs, which frequentlyexpress perforin.22 Compared with the immuno-cytochemical detection of TIA-1/GMP-17, in situhybridization for perforin is not a suitable diagnostictool, as it requires the use of radioactivity and exposuretimes in the range of several weeks. Non-radioactivein situ hybridization using digoxigenin-labelled probeshas not been feasible for the detection of perforintranscripts in our hands, even in cases of anaplastic largecell lymphoma which express high quantities of thismolecule24 (H. D. Foss and I. Araujò, unpublishedresults).The expression pattern of cytotoxic molecules in the
control group, with absence of expression in B-celllymphomas and CD8-negative peripheral T-cell lympho-mas, underscores the specificity of the investigatedmolecules for lymphomas with cytotoxic potential.In vitro findings have also suggested that with rareexceptions, expression of perforin and granzyme B isrestricted to cytotoxic cells, including natural killer cellsand cytotoxic T-cells.11–13 Natural killer cells areunlikely to be the cellular source of ITCL, since thesecells do not display rearranged T-cell receptor â-chaingenes and are immunophenotypically different fromITCL.29 Since expression of at least one of the abovemolecules was found in all cases of ITCL, our dataindicate that this lymphoma derives from cytotoxicT-cells in all instances and thus suggest that ITCL is ahomogeneous lymphoma entity in terms of cellularderivation. Cytotoxic properties have been found inboth áâ and ãä IELs.22 However, given the rearrange-ment of T-cell receptor â-chain genes4 and theabsence of expression of ãä molecules3–5 in themajority of ITCLs, the CD8-positive áâ intra-epithelial T-lymphocyte is most likely to be the normalcounterpart for ITCL.In summary, we have shown that all cases of ITCL
express cytotoxic molecules and are thus thought to beuniformly derived from cytotoxic T-cells. Consideringthe presence of rearranged T-cell receptor â-chain genesand the absence of ãä molecule expression, the CD8-positive áâ intraepithelial T-lymphocyte is most likely tobe the normal counterpart of ITCL. We have also shownthat in situ hybridization for perforin and immunocyto-chemistry with 2G9 are more sensitive methods for thedetection of cytotoxic potential in these lymphomasthan immunocytochemistry for granzyme B.
ACKNOWLEDGEMENTS
This work contains part of the theses of G. Demeland I. Araujo. We are particularly indebted to ErikaBerg, Heidrun Protz, and Lutz Öhring for excellenttechnical assistance. This work was supported bygrants (Ste 318/5-1 and Da 102/2-1) from the DeutscheForschungsgemeinschaft.
REFERENCES
1. Isaacson PG. Gastrointestinal lymphoma. Hum Pathol 1994; 25: 1020–1029.2. Harris NL, Jaffe ES, Stein H, et al. A revised European–American
classification of lymphoid neoplasms: a proposal from the InternationalLymphoma Study Group. Blood 1994; 84: 1361–1392.
3. Chott A, Dragosics B, Radaszkiewicz T. Peripheral T-cell lymphomas of theintestine. Am J Pathol 1992; 141: 1361–1371.
4. Murray A, Cuevas EC, Jones DB, Wright DH. Study of the immunohisto-chemistry and T cell clonality of enteropathy-associated T cell lymphoma.Am J Pathol 1995; 146: 509–519.
5. Schmitt-Gräff A, Hummel M, Zemlin M, et al. Intestinal T-cell lymphoma:a reassessment of cytomorphological and phenotypic features in relation topatterns of small bowel remodelling. Virchows Arch 1996; 429: 27–36.
6. Cerf-Bensussan N, Jarry A, Brousse N, Lisowska-Grospierre B, Guy-GrandD, Griscelli C. A monoclonal antibody (HML-1) defining a novel mem-brane molecule present on human intestinal lymphocytes. Eur J Immunol1987; 17: 1279–1285.
7. Ruthlein J, Heinze G, Auer IO. Anti-CD2 and anti-CD3 induced T cellcytotoxicity of human intraepithelial and lamina propria lymphocytes. Gut1992; 33: 1626–1632.
8. Taunk J, Roberts AI, Ebert EC. Spontaneous cytotoxicity of humanintraepithelial lymphocytes against epithelial cell tumours. Gastroenterology1992; 102: 69–75.
9. Russell GJ, Nagler-Anderson C, Anderson P, Bhan AK. Cytotoxic poten-tial of intraepithelial lymphocytes (IELs): presence of TIA-1, the cytolyticgranule associated protein, in human IELs in normal and diseased intestine.Am J Pathol 1993; 143: 350–354.
10. Oberhuber G, Vogelsang H, Stolte M, Muthenthaler S, Kummer AJ,Radaszkiewicz T. Evidence that intestinal intraepithelial lymphocytes areactivated cytotoxic T cells in celiac disease but not in giardiasis. Am J Pathol1996; 148: 1351–1357.
11. Liu C-C, Walsh CM, Young JD-E. Perforin: structure and function.Immunol Today 1995; 16: 194–201.
12. Smyth MJ, Trapani JA. Granzymes: exogenous proteinases that inducetarget cell apoptosis. Immunol Today 1995; 16: 202–206.
13. Jenne DE, Tschopp J. Granzymes: a family of serine proteases in granulesof cytotoxic T-lymphocytes. In: Cytotoxic Effector Mechanisms. CurrentTopics in Microbiology and Immunology. Vol 140. Berlin: Springer-Verlag,1989; 33–47.
14. Shresta S, MacIvor DM, Heusel JW, Ley TJ. Natural killer cells andlymphokine-activated killer cells require granzyme B for the rapid inductionof apoptosis in susceptible target cells. Proc Natl Acad Sci USA 1995; 92:5679–5683.
15. Darmon AJ, Nicholson DW, Bleackley RC. Activation of apoptotic pro-tease CPP32 by cytotoxic T-cell-derived granzyme B. Nature 1995; 377:446–448.
16. Lichtenheld MG, Podack ER. Structure of the human perforin gene. Asimple gene organization with interesting potential regulatory sequences.J Immunol 1989; 143: 4267–4274.
17. Kummer JA, Kamp A, van Katwijk M, et al. Production and character-ization of monoclonal antibodies raised against recombinant humangranzymes A and B and showing cross reactions with the natural proteins.J Immunol Methods 1993; 163: 77–83.
18. Anderson P, Nagler-Anderson C, O’Brien C, et al. A monoclonal antibodyreactive with a 15-kDa cytoplasmic granule associated protein defines asubpopulation of CD8+ T lymphocytes. J Immunol 1990; 144: 574–582.
19. Tian Q, Streuli M, Saito H, Schlossman SF, Anderson P. A polyadenylatebinding protein localized to the granules of cytolytic lymphocytes inducedDNA fragmentation in target cells. Cell 1991; 67: 629–639.
20. Medley QG, Kedersha N, O’Brien S, et al. Characterization of GMP-17, agranule membrane protein that moves to the plasma membrane of naturalkiller cells following target cell recognition. Proc Natl Acad Sci USA 1996;93: 685–689.
21. Garcia-Sanz JA, MacDonald HR, Jenne DE, Tschopp J, Nabholz M. Cellspecificity of granzyme gene expression. J Immunol 1990; 145: 3111–3118.
22. Guy-Grand D, Malassis-Seris M, Briottet C, Vassalli P. Cytotoxic differen-tiation of mouse gut thymodependent and independent intraepitheliallymphocytes is induced locally. Correlation between functional assays,presence of perforin and granzyme transcripts, and cytoplasmic granules.J Exp Med 1991; 173: 1549–1552.
23. De Bruin PC, Kummer JA, van der Valk P, et al. Granzyme B-expressingperipheral T-cell lymphomas: neoplastic equivalents of activated cytotoxic Tcells with preference for mucosa-associated lymphoid tissue localization.Blood 1994; 84: 3785–3791.
24. Foss HD, Anagnostopoulos I, Araujo I, et al. Anaplastic large celllymphoma of T-cell and null-cell phenotype express cytotoxic molecules.Blood 1996; 88: 4005–4011.
25. Stein H, Gatter K, Asbahr H, Mason DY. Use of freeze-dried paraffinembedded sections for immunohistological staining with monoclonal anti-bodies. Lab Invest 1985; 52: 676–683.
26. Kummer JA, Kamp AM, Tadema TM, Vos W, Meijer CJ, Hack CE.Localization and identification of granzyme A and B-expressing cells innormal lymphoid tissue and peripheral blood. Clin Exp Immunol 1995; 100:164–172.
316 S. DAUM ET AL.
? 1997 by John Wiley & Sons, Ltd. , . 182: 311–317 (1997)

27. Milani S, Herbst H, Schuppan D, Hahn EG, Stein H. In situ hybridizationfor collagen types I, III and IV mRNA in normal and fibrotic rat liver.Evidence for predominant expression in non-parenchymal liver cells. Hepa-tology 1989; 10: 84–92.
28. Sim G-K. Intraepithelial lymphocytes and the immune system. Adv Immunol1995; 58: 297–343.
29. Spits H, Lanier L, Phillips JH. Development of human T and natural killercells. Blood 1995; 85: 2654.
30. Walker-Smith JA, Guandanilini S, Schmitz J, Shmerling DH, Visakorpi JK.Revised criteria for diagnosis of coeliac disease. Report of Working Groupof European Society of Paediatric Gastroenterology and Nutrition. ArchDis Child 1990; 65: 909–911.
31. Musshoff K, Schmidt-Vollmer H. Prognosis of non-Hodgkin’s lymphomawith special emphasis on the staging procedures. Z Krebsforsch 1975; 83:323–341.
APPENDIXThe following are members of the German Study
Group on Intestinal Non-Hodgkin Lymphoma:
Professor Dr E. Dühmke, Strahlentherapeutische undRadioonkologische Abteilung, UniversitätsklinikumGrosshadern, München; Professor Dr W. Fischbach, II.Medizinische Klinik, Aschaffenburg; Dr W. Heise,Auguste-Viktoria-Krankenhaus, Berlin; Professor DrH.-K. Müller-Hermelink, Institut für Pathologie derUniversität Würzburg, Würzburg; PD Dr C. Ohmann,Chirurgische Klinik der Heinrich-Heine-Universität,Düsseldorf; Professor Dr H. D. Röher, ChirurgischeKlinik der Heinrich-Heine-Universität, Düsseldorf;Professor Dr A. Thiede, Chirurgische Klinik der Univer-sitat Wurzburg, Wurzburg; Professor Dr E. Thiel,Medizinische Klinik des Universitätsklinikum BenjaminFranklin, Berlin; Professor Dr K. Wilms, MedizinischePoliklinik der Universität Würzburg, Würzburg.
317EXPRESSION OF CYTOTOXIC MOLECULES IN ITCLs
? 1997 by John Wiley & Sons, Ltd. , . 182: 311–317 (1997)