Embed Size (px)
Citation preview

Extended FAST Exam
Goal of Trauma Care
Golden Hour of Trauma

eFAST
• Best INITIAL screening modality in trauma

2014 LLSA Article (ACEP Policy Statement)
• Level B Recommendation: In hemodynamically unstable patients (SBP ︎90 mmHg) with blunt abdominal trauma, bedside ultrasound, when available, should be the initial diagnostic modality performed to identify the need for emergent laparotomy
eFAST
Bedside
Non-invasive
Repeatable
Rapid
No Contraindications
Blunt or penetrating trauma to the abdomen or chest
Trauma in pregnancy
Unexplained hypotension
Indications
Thoraco-Abdominal Anatomy - between the ribs

Diaphragm
Liver
Kidneysuperior pole
Morison'spouch Kidney
(inferior pole)
Diaphragm
Need to move probe from diaphragm to lower pole of kidney
Right Upper Quadrant
If Eyes are the Window to the Soul, then Liver is the Window to the Heart
• Start at liver edge and follow the subcostal margin until heart is seen
• Aim beam at chin
• Never cross midline
Sub-Xiphoid Window

SubXiphoid View
Liver
ParaSternal Long
• 15% of the time unable to obtain sub-xiphoid
• Place the sound along the long axis of the heart
ParaSternal Long
• Point indicator towards the patient’s left elbow

ParaSternal Long
LALV
RV
Left Upper Quadrant
Left Upper Quadrant

Suprapubic View - Sagittal
Transducer just superior to the pubic symphysis
Fan side to side looking for anechoic wedges
Suprapubic view - SagittalBladder
Vesico-uterine space
Uterus
Recto-uterine space
Suprapubic Window

Suprapubic view - Transverse
Transducer just superior to pubic symphysis
Mirror Image Artifact• Sound glances off
diaphragm, returning to probe with a longer time of flight
• Machine misinterprets this as more liver tissue further afield
Mirror Image Artifact

Hemothorax
Normal
Pitfalls: Epicardial Fat
Gastric FluidSpleen
Stomach

Hemoperitoneum Fluid in Stomach
Blunt Trauma AlgorithmPositive FAST
Stable Unstable
ORCT
Negative FAST
UnstableStable
CT ??

Case 1: Blunt Traumatic Full Arrest
Case 2: Auto vs Peds
Case 3: Stab Wound to Left Upper Quadrant

Case 4: Fall from Ladder, on Coumadin
Case 5: Stab Wound to Right Upper Quadrant
Case 6: Fell off Motorcycle

Case 7: Auto vs Peds
Pneumothorax?
Pneumothorax?
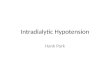
Sensitivity of supine AP CXR is 47-75%

Compare AP chest x-ray with ultrasound for the diagnosis of pneumothorax
Pneumothorax - Methods
• English-language articles on the performance of chest x-ray and ultrasonography in the diagnosis of a pneumothorax were selected
• In eligible studies, data were recalculated, and the forest plots were analyzed
Chest. 2011 Oct;140(4):859-66
Ultrasound 88% Sensitive
Chest Xray 52% sensitive
Chest. 2011 Oct;140(4):859-66
Sensitiv
ity

Ultrasound 99% Specific
Chest Xray 100% Specific
Chest. 2011 Oct;140(4):859-66
Specific
ity
Sonographic Technique
High frequency linear probe
2nd intercostal space
Mid-clavicular line
4-5 respiratory cycles
B-Mode and M-mode
Pneumothorax Technique
Pleural interface
•Air in lung impairs transmission of sound
•Pleural interface is visible
•Visualize visceral & parietal pleura sliding on each other

Pneumothorax Technique
•With pneumothorax, lung falls away from chest wall
•Air separates the pleura
•Pleural interface is no longer “seen” by the probe
Pneumothorax?
Pneumothorax?

Pneumothorax?
Pneumothorax?
Pneumothorax?

Pneumothorax?
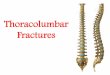
Sky-Ocean-Beach
• Depress M-mode key
• Place cursor line across pleural line
• Depress M-mode key again to generate an M-mode tracing
Sky-Ocean-Beach
SkyOcean
Beach
B-Mode
M-Mode

Sky-Ocean-Beach
SkyOceanNo Beach
B-Mode
M-Mode
Sky-Ocean-Beach
eFAST Summary
• Hepato-Renal • Cardiac • Spleno-Renal • Suprapubic
• 1. Pleural Line • 2. Lung Sliding • 3. M-mode (S-O-B)