Embed Size (px)
Citation preview
Poster Design & Printing by Genigraphics® - 800.790.4001
Mr Simon A McKeanOtolaryngology DepartmentNHS [email protected]/otolaryngology
External Auditory Canal Lesions - Diagnoses and TreatmentSimon A. McKean BSc, MBChB, MRCS (Glasg), DOHNS; Richard D White BSc, MBChB; Thiru Sudarshan MBBS, DMRD, FRCR;
S.S. Musheer Hussain MBBS, MSc Audiology, FRCS (Edin), FRCS (Eng)Ninewells Hospital & Medical School, Dundee, Scotland, United Kingdom
Of 396 patients that had imaging in our department that includedthe external ear, 109 had diagnoses related to the ear canal. We excluded simple chronic otitis externa, cerumen, cholesteatoma that extended from the middle ear and any associated inflammatory polyp and trauma cases. This left 54 patients with 24 different diagnoses. These are detailed in the discussion section.
Most cases (81%), had been investigated using high resolution computed tomography scanning. Other modalities of imaging included magnetic resonance imaging, ultrasound scanning and nuclear medicine scanning. Several cases had had more than one modality used.
Personal case series and radiology databases were examined to identify cases of external ear pathologies between June 2003 and February 2009. The type of imaging and range of diagnoses were noted.
There are many diagnoses to be considered when presented with changes involving the external ear canal. CT imaging can be helpful to plan surgery but often the final diagnosis is not made until the pathologists have examined the specimen. There are other diagnoses described in published case reports which were not seen in our case series. Treatment usually consists of surgical excision +/- canaloplasty. Medical therapy (e.g. antibiotic therapy) is also sometimes needed.
INTRODUCTION
METHODS & MATERIALS
CONCLUSIONS
DISCUSSION
RESULTS
ABSTRACT
CONTACT
Basal cell carcinoma
Benign Necrotizing Otitis Externa
Carcinoma ex-pleomorphic adenoma
Ceruminous adenoma
Histiocytosis X
Intradermal melanonaevus
Keratosis obturans
Lipoma
Neuroma
Paraganglioma
Squamous cell carcinoma
Superficial angiomyxioma
As can be seen from the chart below, there is an extensive differential diagnosis for pathology that affects the external ear. Many are rare entities that will not be recognised purely by clinical examination, even by those doctors with long otological experience. We have excluded simple chronic otitis externa, cerumen, cholesteatoma extending from the middle ear and any associated inflammatory polyp and trauma cases.
References1. Soft tissue abnormalities of the EAC: subject review of CT findings. Chakeres DW et al. Radiology, 1985,156(1);105-92. High resolution CT findings in diseases of the EAC. A review of 31 cases. Vanneste Fet al. J Belge Radiol, 1989, 72(3); 199-2053. An unusual localisation of Kapsoi’s sarcoma: The EAC. Delbrouck C et al. Acta Otorhinolaryngol Belg, 1998, 52(1); 29-364. Ceruminous gland carcinoma of the EAC presenting as chronic otitis media. Selcuk A et al. B-ENT, 2007, 3(4), 195-95. Mucoepidermoid carcinoma of the EAC. Bared A et al. Acta Otolaryngol 2007, 127(3); 280-46. The adenoid cystic carcinoma. Perz Gonzales R et al. An Otorrhinolaryngol Ibero Am, 2005, 32(3), 211-207. Temporal bone CT in the diagnosis of acquired diseases of the EAC. Filippkin MA et al. Vestn Rentgenol Radiol, 2004, (1), 10-4
There are also case reports of diagnoses not mentioned here, including; papilloma, haemangioma, Kaposi’s sarcoma, adenoid cystic carcinoma, and mucoepidermoid carcinoma (see references). We must be aware of this wide range of differential diagnoses, so appropriate investigations can be performed and surgical removal arranged in a timely manner. Excision of the involved tissue, plus widening of the bony canal, meatoplasty and canaloplasty using split skin grafts can reduce post operative recurrence and stenosis.
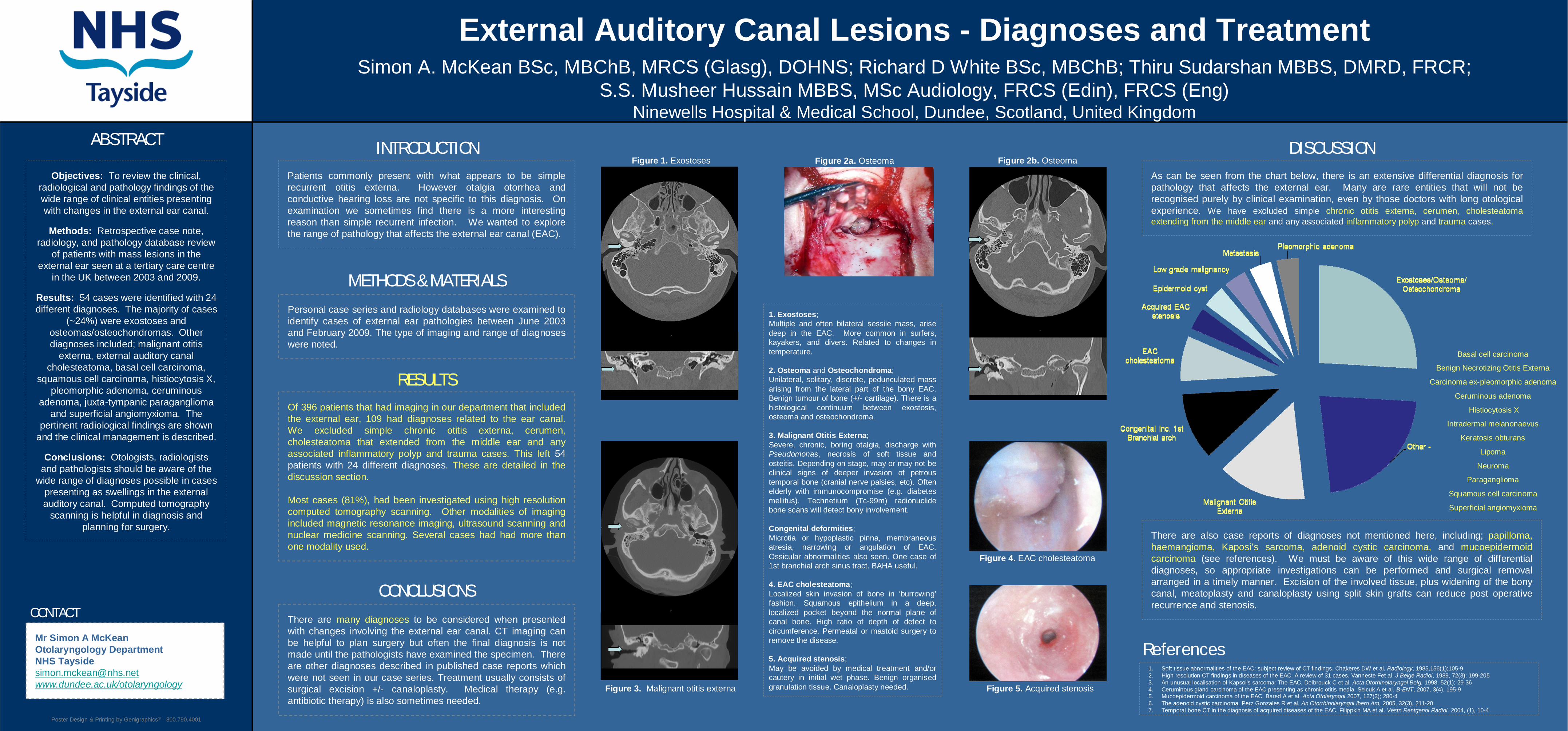
Figure 2a. Osteoma
Patients commonly present with what appears to be simple recurrent otitis externa. However otalgia otorrhea and conductive hearing loss are not specific to this diagnosis. On examination we sometimes find there is a more interesting reason than simple recurrent infection. We wanted to explore the range of pathology that affects the external ear canal (EAC).
1. Exostoses;Multiple and often bilateral sessile mass, arise deep in the EAC. More common in surfers, kayakers, and divers. Related to changes in temperature.
2. Osteoma and Osteochondroma; Unilateral, solitary, discrete, pedunculated mass arising from the lateral part of the bony EAC. Benign tumour of bone (+/- cartilage). There is a histological continuum between exostosis, osteoma and osteochondroma.
3. Malignant Otitis Externa;Severe, chronic, boring otalgia, discharge with Pseudomonas, necrosis of soft tissue and osteitis. Depending on stage, may or may not be clinical signs of deeper invasion of petrous temporal bone (cranial nerve palsies, etc). Often elderly with immunocompromise (e.g. diabetes mellitus). Technetium (Tc-99m) radionuclide bone scans will detect bony involvement.
Congenital deformities;Microtia or hypoplastic pinna, membraneous atresia, narrowing or angulation of EAC. Ossicular abnormalities also seen. One case of 1st branchial arch sinus tract. BAHA useful.
4. EAC cholesteatoma;Localized skin invasion of bone in ‘burrowing’fashion. Squamous epithelium in a deep, localized pocket beyond the normal plane of canal bone. High ratio of depth of defect to circumference. Permeatal or mastoid surgery to remove the disease.
5. Acquired stenosis;May be avoided by medical treatment and/or cautery in initial wet phase. Benign organised granulation tissue. Canaloplasty needed.
Figure 1. Exostoses
Figure 3. Malignant otitis externa
Figure 2b. Osteoma
Figure 5. Acquired stenosis
Figure 4. EAC cholesteatoma
Objectives: To review the clinical, radiological and pathology findings of the wide range of clinical entities presenting with changes in the external ear canal.
Methods: Retrospective case note, radiology, and pathology database review
of patients with mass lesions in the external ear seen at a tertiary care centre
in the UK between 2003 and 2009.
Results: 54 cases were identified with 24 different diagnoses. The majority of cases
(~24%) were exostoses and osteomas/osteochondromas. Other diagnoses included; malignant otitis
externa, external auditory canal cholesteatoma, basal cell carcinoma,
squamous cell carcinoma, histiocytosis X, pleomorphic adenoma, ceruminous
adenoma, juxta-tympanic paraganglioma and superficial angiomyxioma. The
pertinent radiological findings are shown and the clinical management is described.
Conclusions: Otologists, radiologists and pathologists should be aware of the
wide range of diagnoses possible in cases presenting as swellings in the external auditory canal. Computed tomography
scanning is helpful in diagnosis and planning for surgery.





























