Embed Size (px)
Citation preview

1111. J. Radiarion Oncology Rio/. Phys.. Vol. 6, pp. 497-504 0 Pergamon Press Ltd., 1980 Prmted in the U.S.A.
0360.,0,6/80/0497-08102.00/0
0 Brief Communication
EXTRA-HEPATIC BILIARY TRACT METASTASES FROM BREAST CANCER’
GENE KOPELSON, M.D.*, ANN M. CHU, M.D.?, JOANNE A. DOUCETTE, B.A.**, and LEONARD L. GUNDERSON, M.D.$
Department of Radiation Medicine, Massachusetts General Hospital, Boston MA 02 1 14 USA
A retrospective review was conducted of 49 breast cancer patients who were seen at the Massachusetts General Hospital from 1962 to 1978 and who developed biliary tract metastases. Although these findings were incidental at autopsy in 21 patients, clinical evidence of extra-hepatic biliary involvement developed in 28. This was documented radiographically, surgically, and/or confirmed at autopsy. Although most patients had previous or concurrent nonbiliary tract metastases, in 6 patients the initial site of failure was in the extra-hepatic biliary system. Analysis of the 28 patients in the clinical group revealed that initial management with radiation therapy alone produced a response in 3 of 6 patients. However, when radiation was coupled with bypass surgery and/or adjuvant chemothera- py, a response occurred in 3 of 3; the total radiation therapy response rate was 6/9. Chemotherapy given either alone or in combination with surgery produced a response in only one of 7 patients. All 4 irradiated patients who were treated with a time-dose-fractionation (TDF) > 40 had a complete response compared to a complete response in only 2 of 8 with a TDF 5 40. The median survival of the irradiated group was 6 months compared to 3.3 months in the treated-unirradiated patients and 0.7 months in the untreated patients. The onset of jaundice in a breast cancer patient does not necessarily indicate progressive hepatic involvement. Patients with extrahepatic metastatic obstruction are being recognized increasingly and should be treated vigorously, especially since such patients with no liver parenchymal involvement have a greater survival (median 6 months) than those with liver involvement (median 1.8 months).
Radiotherapy, Bile duct neoplasms, Breast neoplasms-complications.
INTRODUCTION The onset of jaundice in a cancer patient is often ascribed to progressive hepatic parenchymal metastases. In the past, extrahepatic metastases causing obstructive jaun- dice have received little attention in the literature. Yet since about 1970, with the increasing use of transhepatic and endoscopic retrograde cholangiography, this phe- nomena has been increasingly recognized (Table 1). We have reviewed the experience of 49 breast cancer patients with extrahepatic biliary tract metastases in an effort to determine more clearly the natural history and proper treatment of these metastases.
MATERIALS AND METHODS A computer search of the hospital charts at the Massa-
chusetts General Hospital, its Tumor Registry, and the Department of Radiation Medicine revealed that of 3961
patients with breast carcinoma who were seen from 1962 through 1978 inclusive, 49 patients were identified who had extra-hepatic biliary tract metastases.
These patients were divided into two groups based upon whether these metastases were found incidentally at autopsy (21 patients) or whether clinical evidence of extra-hepatic biliary metastases had occurred (28 patients). The latter group was defined as follows: 1) Patients with clinical obstructive jaundice (clinical icterus with obstructive liver chemistries) in whom explo- ration (7 patients) or autopsy (16 patients) disclosed metastases in porta hepatis, gall-bladder, and/or peri- pancreatic nodes; 2) in 3 patients documentation of extra-hepatic metastases was only via roentgenographic study and biopsy; 3) extra-hepatic metastases were found in 2 non-jaundiced patients who underwent exploration for suspected biliary tract pathology.
*Resident, and Clinical Fellow in Radiation Therapy, Harvard Medical School.
tlnstructor in Radiation Therapy, Harvard Medical School. **Dosimetrist, Dept. of Radiation Medicine, Massachusetts
General Hospital. SAssistant Professor of Radiation Therapy, Harvard Medical
School. 1 .Presented at the Spring 1979 Meeting, New England
Society for Radiation Oncology, March 23, 1979. Reprint requests to: Dr. Gene Kopelson, Dept. Radiation
Medicine, Massachusetts General Hospital, Boston MA 02 114. Acknowledgemenrs-Mindy Printz-Kopelson, Nikki Priest-
ley, and Joan Horgan helped in the preparation of this manu- script.
Accepted for publication 29 October 1979.
497
498 Radiation Oncology 0 Biology 0 Physics April 1980, Volume 6, Number 4
Table I. Reported patients with clinical extra-hepatic biliary metastases
No. patients (references)
Primary tumor
Reported before 1970
Breast Stomach Colon
Melanoma Lung Miscellaneous
Prior total no. patients 6 Present series 0 Total no. patients 6
Reported 1970 or later
4 (8,24,35,39) 34 (7,24,26,3 I) 12 (16,17,24,25,
28,40) 5 (6,10,30,38) I(121
15 (4*,12’,18, 33?,36**,37t)
71 28 99
*Prostate. + Epiglottis. **Testis. tunspecified. *Uterus.
Clinical presentation Management of the initial breast carcinoma could be
determined in 27 of the 28 patients in the clinical group; 2 of the latter had bilateral breast carcinomas. Initial management consisted of radical or modified radical mastectomy with or without postoperative irradiation for 20 breast carcinomas. Five patients had simple mastec- tomy with or without postoperative irradiation. Two patients were treated primarily with irradiation, and 2 had biopsy only. One patient was treated with modified radical mastectomy plus postoperative radiation therapy and adjuvant cyclophosphamide-methotrexate-5 fluorou- racil. The lymph nodes were positive in 18 of 22 breast carcinomas in 20 patients.
The disease-free interval was calculated from time of initial treatment of the breast carcinoma to the date of onset of the first site of local or distant failures; it ranged from 0 months in 2 patients who presented with metas- tases to 114 months, with a median of 16 months. In six patients the initial site of failure was in the extra-hepatic biliary tract. These latter patients had a disease-free interval ranging from O-79 months from the date of initial treatment (median of I1 months). For the entire clinical group, sites of failure prior to the development of extra-hepatic biliary tract metastases included: local fail- ure, 11 patients; bone, 1 I; pleura, 5; skin, 3; orbit, I; brain, 1; pulmonary hilar nodes, 1; cervical nodes, 1. Three patients had documented liver metastases which were treated prior to the development of biliary tract obstruction because of extra-hepatic metastases.
Eighteen patients developed clinical extra-hepatic biliary metastases while they were on the following systemic therapies: single agent chemotherapy, 1 patient; multi-agent chemotherapy, 4; hormonal manipulation, 8;
and chemotherapy plus hormonal manipulation, 6. The duration of symptoms of extra-hepatic biliary tract metastases was known in 17 patients, and ranged from 1 day to 3 months with a median of 2-3 weeks. Sites of extra-hepatic metastases appear in Table 2.
TREATMENT
Definitions Initial treament of extra-hepatic biliary metastases
was primary surgical decompression and/or radiation therapy and/or chemotherapy while the patient still had obstructive jaundice, or adjuvant (use of one or more modalities after laboratory-documented relief of biliary obstruction had already occurred with one or more of the primary modalities of therapy). A complete response was defined as a fall of bilirubin to normal levels. A partial response was defined as a fall of bilirubin (but not to normal levels), or a decrease in pain, pruritus, or mass shrinkage. No response was defined as no change in icterus, pruritus, mass size, pain, or deterioration. Length of response was analyzed from the date of beginning of therapy. Survival data were calculated from the data of diagnosis of the biliary tract metastases via the actuarial method*.
Surgery In five patients various surgical procedures were
performed for obstructive metastases: cholecystojejunos- tomy with radiation therapy, cholecystectomy with adria- mycin plus prednisone, cholecystojejunostomy with choledochostomy plus adjuvant 5-fluorouracil, and percutaneous transhepatic bile duct intubation (internal stent) with radiation therapy plus adjuvant cyclophos- phamide-methotrexate-5 fluorouracil. The 1 patient who was treated with surgery only had initial cholecystojeju- nostomy and gastrojejunostomy followed by distal pancreatectomy.
Radiation therapy. Radiation therapy was used for initial management in
9 patients (6 radiation therapy alone, 1 with cholecystoje- junostomy, 1 with tube catheter drainage plus adjuvant
Table 2. Sites of extra-hepatic biliary metastases
Incidental autopsy Clinical group group Total
(N = 21) (N = 28) (N = 49)
No. (%) No. (%) No. (%)
Bile duct nodes 9 (43) 26 (93) 35 (71) Peripancreatic nodes 14 (67) 9 (32) 23 (47) Gallbladder 3 (14) 4 (15) 7 (14)
Liver involved I3 (62) 20 (71) 33 (67) Liver not involved 8 (38) 8 (29) I6 (33)
Biliary metastases 0 G. KOPELSON et al. 499
cyclophosphamide-methotrexate-5 fluorouracil, and 1 with adjuvant adriamycin). Modalities included 25MeV or IO-MeV linear accelerator x-rays in 4 patients, 2-MeV Van de Graaff generator x-rays in 2 patients, and 280-kV orthovoltage x-rays in 3 patients. Doses (corrected for Roentgen-to-rad conversion and relative biological effec- tiveness (RBE) differences) ranged from 994 to 4960 rad over 6-42 elapsed days in 5-29 fractions. TDF values ranged from 14 to 86 with a mean of 43.
Radiotherapeutic techniques varied during the 16 years encompassed by this study. In the group that was treated initially with radiation, 5 were treated via
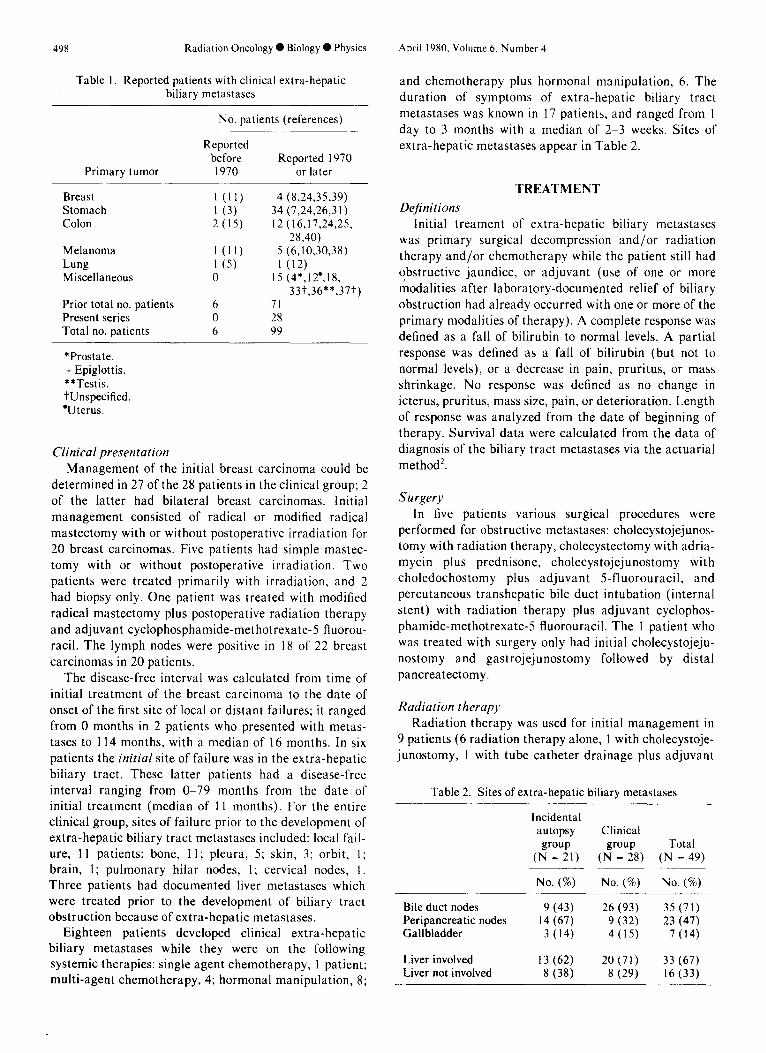
opposed equally weighted anterior-posterior portals, while 2 patients had single anterior fields. Other tech- niques included opposed anterior-posterior fields weighted anteriorly 3:l in I patient, and a 4 field box technique in another (Fig. IA-C). Field sizes ranged from 10 x 10 cm. to 21 x 23 cm. In patients who were treated with larger fields field size often was reduced after 2200-2500 rad. Salvage was attempted with irra- diation in 3 patients who failed initial management with surgery and/or chemotherapy. Doses were lower (TDF- 3, 11, and 16), and the treatment techniques similar to the above.
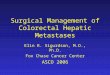
Fig. I. Seventy-two year-old woman whose first failure site was in the extra-hepatic biliary tract 8 months after radical mastec- tomy. Although liver scan was normal, transhepatic cholangio- gram revealed extrinsic compression in the porta hepatis. A transhepatic catheter was inserted through tumor into the duodenum-( Fig. I -A). When bilirubin levels rose again postop- eratively, a dose of 4960 rad was given on a IO-MeV linear accelerator in 29 fractions via shaped anterior-posterior (Fig. 1 -B) and bilateral (Fig. I-C) portals. She is presently alive and well and jaundice-free.
500 Radiation Oncology 0 Biology ??Physics
Chemotherapy 16r 0
Of the 7 patients who were treated initially with chemotherapy, regimens included various combinations including 5-fluorouracil, vincristine, cyclophosphanide, methotrexate, adriamycin and prednisone. The 5 patients who were treated with adjuvant chemotherapy were treated with similar regimens.
14
F
0
Local response RESULTS
The efficacy of surgery for these lesions was difficult to assess since 4 of the 5 patients had other definitive or adjuvant therapies. The 1 patient who was treated with surgery alone died three weeks after distal pancreatec- tomy from a perforated gastric ulcer.
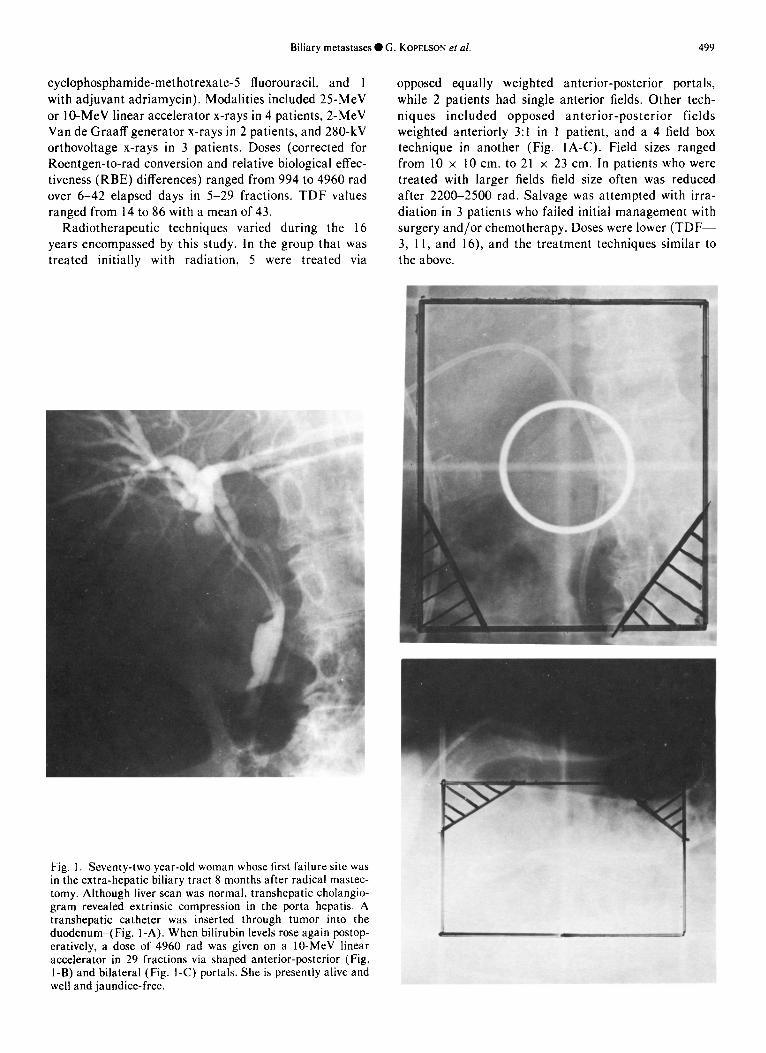
When initial radiation therapy was used alone, it resulted in an overall response in 3 of 6 patients (Table 3); when it was combined with palliative surgery and/or adjuvant chemotherapy, the response occurred in 3 of 3. Overall, radiotherapy produced a response in 6 of 9 patients. The time-course changes in bilirubin levels in patients who responded completely to radiation therapy appear in Fig. 2.
Only one of 7 patients responded to initial chemother- apy (Table 3), and no patients had a complete response. Three patients were given adjuvant chemotherapy after another modality had already resolved the obstruction (Table 4), and 2 others were placed on adjuvant chemo- therapy when as-yet-nonobstructing extra-hepatic metas- tases were found at exploration (Table 4, footnote). Yet of these 5 patients, 4 eventually developed obstruction 2-4 months after they were placed on chemotherapy.
Salvage was attempted after initial management had failed in 6 patients (Table 5); it was successful in 3 of them. In 1 patient who had failed initial chemotherapy a complete response to salvage hormonal manipulation lasted 6 years before recurrence.
Table 3. Results of initial management
Response duration
Complete Partial No response response response
No. (mo.) No. (mo.) No. (mo.)
Radiation therapy only 2 (4,3) 1 (2) 3 (0) Radiation therapy and
other* 3 (9+,8+,5) 0 0
Total Radiation therapy 5 I 3
Chemotherapy only 0 1 (3) 5 (0) Chemotherapy and
other** 0 0 1 (0) Total chemotherapy 0 I 6
*Palliative bypass and/or adjuvant chemotherapy (see text). +Alive and well, no evidence of disease (NED). **Cholecystectomy.
April 1980, Volume 6, Number 4
1 MONTH 2 MONTHS
PRE COMPLETION L POST - RT RT RT
Fig. 2. Time-course fall in bilirubin levels after radiation thera- py. Each patient did not have a level drawn at each time interval; however in all 6 complete responders, levels fell to normal by two months post-irradiation.
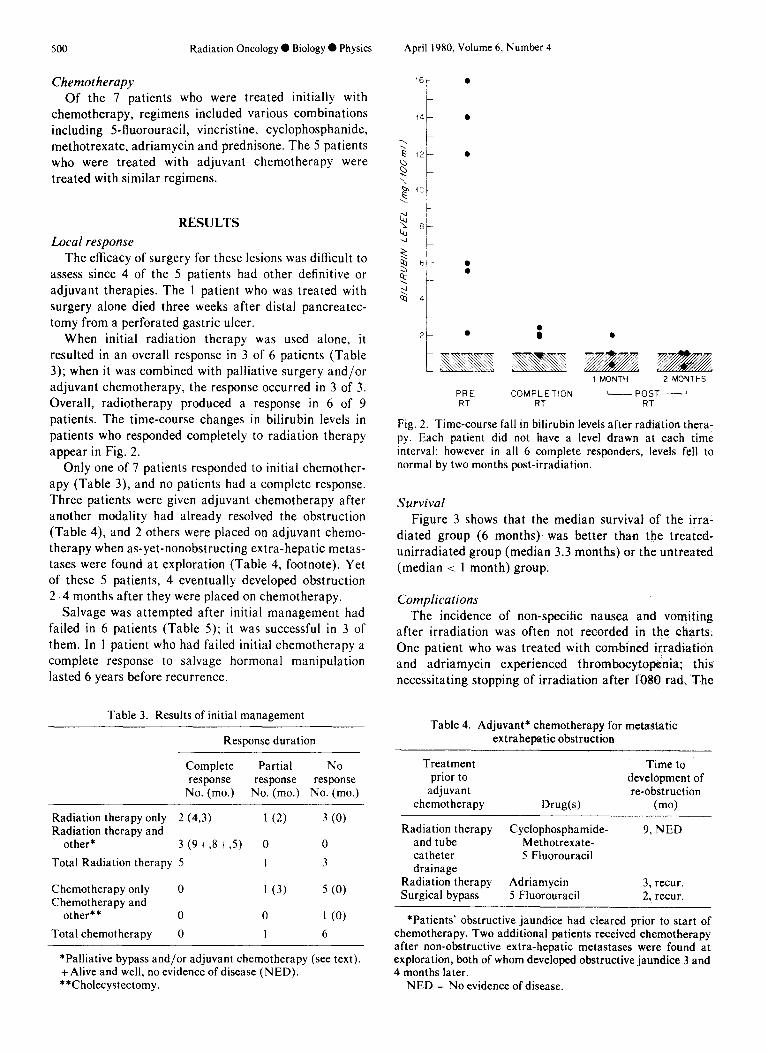
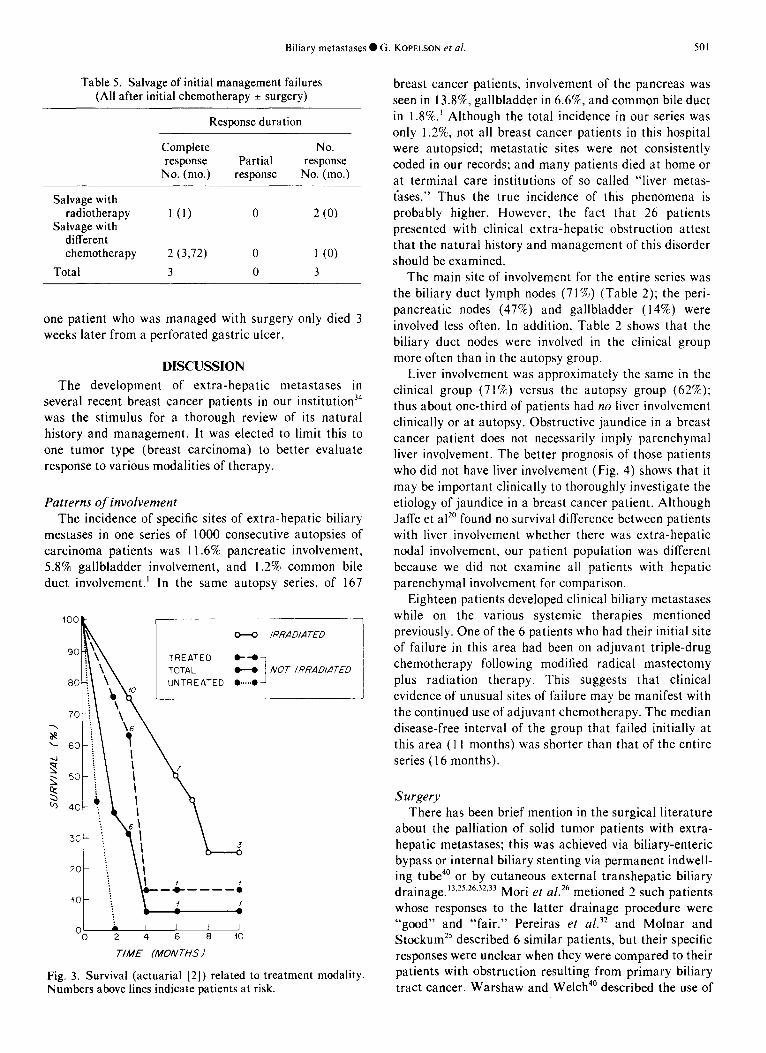
Survival Figure 3 shows that the median survival of the irra-
diated group (6 months) was better than the treated- unirradiated group (median 3.3 months) or the untreated (median < 1 month) group.
Complications The incidence of non-specific nausea and vomiting
after irradiation was often not recorded in the charts. One patient who was treated with combined irradiation and adriamycin experienced thrombocytopenia; this necessitating stopping of irradiation after 1080 rad. The
Table 4. Adjuvant* chemotherapy for metastatic extrahepatic obstruction
Treatment prior to
adjuvant chemotherapy Drug(s)
Time to development of re-obstruction
(mo)
Radiation therapy Cyclophosphamide- 9, NED and tube Methotrexate- catheter 5 Fluorouracil drainage
Radiation therapy Adriamycin 3, recur. Surgical bypass 5 Fluorouracil 2, recur.
*Patients’ obstructive jaundice had cleared prior to start of chemotherapy. Two additional patients received chemotherapy after non-obstructive extra-hepatic metastases were found at exploration, both of whom developed obstructive jaundice 3 and 4 months later.
NED = No evidence of disease.
Biliary metastases 0 G. KOPELSON et al. 501
Table 5. Salvage of initial management failures (Al1 after initial chemotherapy + surgery)
Response duration
Complete No. response Partial response
No. (mo.) response No. (mo.)
Salvage with radiotherapy l(t) 0 2 (0)
Salvage with different chemotherapy 2 (3972) 0 1 (0)
Total 3 0 3
one patient who was managed with surgery only died 3 weeks later from a perforated gastric ulcer.
DISCUSSION
The development of extra-hepatic metastases in several recent breast cancer patients in our institution34 was the stimulus for a thorough review of its natural history and management. It was elected to limit this to one tumor type (breast carcinoma) to better evaluate response to various modalities of therapy.
Patterns of involvement The incidence of specific sites of extra-hepatic biliary
mestases in one series of 1000 consecutive autopsies of carcinoma patients was 11.6% pancreatic involvement, 5.8% gallbladder involvement, and 1.2% common bile duct involvement.’ In the same autopsy series, of 167
100
W IRRADIATED 1 “PA / TREATED e-1
M NOT IRRADIATED . . . . . ..I
01 . I I 1 I 0 2 4 6 8 10
TIME (MONTHS I
Fig. 3. Survival (actuarial [2]) related to treatment modality. Numbers above lines indicate patients at risk.
breast cancer patients, involvement of the pancreas was seen in 13.8%, gallbladder in 6.6%, and common bile duct in 1.8%.’ Although the total incidence in our series was only 1.2%, not all breast cancer patients in this hospital were autopsied; metastatic sites were not consistently coded in our records; and many patients died at home or at terminal care institutions of so called “liver metas- iases.” Thus the true incidence of this phenomena is probably higher. However, the fact that 26 patients presented with clinical extra-hepatic obstruction attest that the natural history and management of this disorder should be examined.
The main site of involvement for the entire series was the biliary duct lymph nodes (71%) (Table 2); the peri- pancreatic nodes (47%) and gallbladder (14%) were involved less often. In addition, Table 2 shows that the biliary duct nodes were involved in the clinical group more often than in the autopsy group.
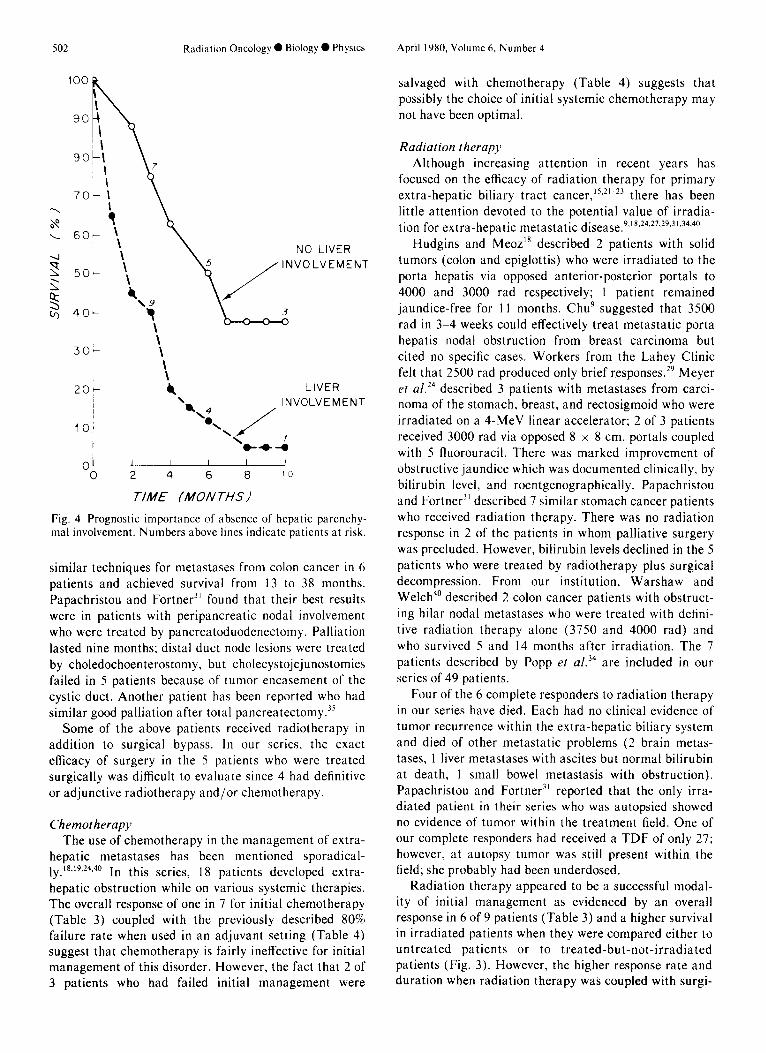
Liver involvement was approximately the same in the clinical group (71%) versus the autopsy group (62%); thus about one-third of patients had no liver involvement clinically or at autopsy. Obstructive jaundice in a breast cancer patient does not necessarily imply parenchymal liver involvement. The better prognosis of those patients who did not have liver involvement (Fig. 4) shows that it may be important clinically to thoroughly investigate the etiology of jaundice in a breast cancer patient. Although Jaffe et aI” found no survival difference between patients with liver involvement whether there was extra-hepatic nodal involvement, our patient population was different because we did not examine all patients with hepatic parenchymal involvement for comparison.
Eighteen patients developed clinical biliary metastases while on the various systemic therapies mentioned previously. One of the 6 patients who had their initial site of failure in this area had been on adjuvant triple-drug chemotherapy following modified radical mastectomy plus radiation therapy. This suggests that clinical evidence of unusual sites of failure may be manifest with the continued use of adjuvant chemotherapy. The median disease-free interval of the group that failed initially at this area (11 months) was shorter than that of the entire series (16 months).
Surgery There has been brief mention in the surgical literature
about the palliation of solid tumor patients with extra- hepatic metastases; this was achieved via biliary-enteric bypass or internal biliary stenting via permanent indwell- ing tube4’ or by cutaneous external transhepatic biliary drainage.13.25.26.32.33 Mori et af.26 metioned 2 such patients whose responses to the latter drainage procedure were “good” and “fair.” Pereiras et al.32 and Molnar and Stockum25 described 6 similar patients, but their specific responses were unclear when they were compared to their patients with obstruction resulting from primary biliary tract cancer. Warshaw and Welch4’ described the use of
502
100
90
90
30
20
10
n
Radiation Oncology 0 Biology 0 Physics
i \
-\
\\
I 7
-:
“0 2 4 6 8 10
TIME (MO/V THS I
Fig. 4 Prognostic importance of absence of hepatic parenchy- mal involvement. Numbers above lines indicate patients at risk.
similar techniques for metastases from colon cancer in 6 patients and achieved survival from 13 to 38 months. Papachristou and Fortner3’ found that their best results were in patients with peripancreatic nodal involvement who were treated by pancreatoduodenectomy. Palliation lasted nine months; distal duct node lesions were treated by choledochoenterostomy, but cholecystojejunostomies failed in 5 patients because of tumor encasement of the cystic duct. Another patient has been reported who had similar good palliation after total pancreatectomy.”
Some of the above patients received radiotherapy in addition to surgical bypass. In our series, the exact efficacy of surgery in the 5 patients who were treated surgically was difficult to evaluate since 4 had definitive or adjunctive radiotherapy and/or chemotherapy.
Chemotherapy The use of chemotherapy in the management of extra-
hepatic metastases has been mentioned sporadical-
LY. ‘8,‘9*24.40 In this series, 18 patients developed extra- hepatic obstruction while on various systemic therapies. The overall response of one in 7 for initial chemotherapy (Table 3) coupled with the previously described 80% failure rate when used in an adjuvant setting (Table 4) suggest that chemotherapy is fairly ineffective for initial management of this disorder. However, the fact that 2 of 3 patients who had failed initial management were
April 1980, Volume 6. Number 4
salvaged with chemotherapy (Table 4) suggests that possibly the choice of initial systemic chemotherapy may not have been optimal.
Radiation therapy Although increasing attention in recent years has
focused on the efficacy of radiation therapy for primary extra-hepatic biliary tract cancer,‘5’2’-23 there has been little attention devoted to the potential value of irradia- tion for extra-hepatic metastatic disease.9~‘x.24,27,29,3’,34.40
Hudgins and Meoz’* described 2 patients with solid tumors (colon and epiglottis) who were irradiated to the porta hepatis via opposed anterior-posterior portals to 4000 and 3000 rad respectively; I patient remained jaundice-free for 11 months. Chug suggested that 3500 rad in 3-4 weeks could effectively treat metastatic porta hepatis nodal obstruction from breast carcinoma but cited no specific cases. Workers from the Lahey Clinic felt that 2500 rad produced only brief responses.29 Meyer et a1.24 described 3 patients with metastases from carci- noma of the stomach, breast, and rectosigmoid who were irradiated on a 4-MeV linear accelerator; 2 of 3 patients received 3000 rad via opposed 8 x 8 cm. portals coupled with 5 fluorouracil. There was marked improvement of obstructive jaundice which was documented clinically, by bilirubin level, and roentgenographically. Papachristou and Fortner3’ described 7 similar stomach cancer patients who received radiation therapy. There was no radiation response in 2 of the patients in whom palliative surgery was precluded. However, bilirubin levels declined in the 5 patients who were treated by radiotherapy plus surgical decompression. From our institution, Warshaw and Welch4’ described 2 colon cancer patients with obstruct- ing hilar nodal metastases who were treated with defini- tive radiation therapy alone (3750 and 4000 rad) and who survived 5 and 14 months after irradiation. The 7 patients described by Popp et a1.34 are included in our series of 49 patients.
Four of the 6 complete responders to radiation therapy in our series have died. Each had no clinical evidence of tumor recurrence within the extra-hepatic biliary system and died of other metastatic problems (2 brain metas- tases, 1 liver metastases with ascites but normal bilirubin at death, 1 small bowel metastasis with obstruction). Papachristou and Fortner3’ reported that the only irra- diated patient in their series who was autopsied showed no evidence of tumor within the treatment field. One of our complete responders had received a TDF of only 27; however, at autopsy tumor was still present within the field; she probably had been underdosed.
Radiation therapy appeared to be a successful modal- ity of initial management as evidenced by an overall response in 6 of 9 patients (Table 3) and a higher survival in irradiated patients when they were compared either to untreated patients or to treated-but-not-irradiated patients (Fig. 3). However, the higher response rate and duration when radiation therapy was coupled with surgi-
Biliary metastases 0 G. KOPELSON et al. 503
cal decompression and/or adjuvant chemotherapy (Table 3) suggest that radiation therapy alone may be insuffi- cient to manage these patients initially. Our series cannot answer whether combined surgical decompression and irradiation might in fact be better than either modality alone because only 1 patient received surgery alone. In addition, therapeutic options may differ depending on whether isolated extra-hepatic metastases develop (with an aggressive combination of surgery, irradiation, and chemotherapy in a vigorous attempt at long term control), or whether extra-hepatic metastases occur in the face of other sites of distant spread (if some form of bypass or stent has already relieved obstruction, the addition of irradiation may not be indicated in the face of limited life-span).
The radiation-only group in Table 3 demonstrated a rather short-lived response duration of 2-4 months (including treatment time). This would also argue for combining irradiation with other modalities and/or for a short course of irradiation. Complete response after irra- diation occurred in 3 of 3 patients who were treated to relatively high dose (TDF > 40)-small field size (< 225 cm.‘) compared to 1 of 2 who were treated to low dose (TDF 5 40)-same field size. For patients who were
treated to large field size (> 225 cm.2), complete response occurred in l/l patient treated to high TDF (> 40) versus l/6 treated to low TDF (-i 40). Although one interpretation of this data would be that high dose-small field irradiation yielded the best results, in fact patients who were treated to the higher volume often were the patients who were treated before 1970 in whom more precise localization techniques (such as endoscopic-retro- grade or transhepatic cholangiography) were not avail- able; thus general right-upper-quadrant fields were used (necessitating lower dose). Other methods to treat the porta hepatis in the absence of specific radiographic localization in a particular patient” were not used in our series.
The lack of fall of bilirubin to normal levels by the completion of radiation therapy need not indicate radio- resistance; as Fig. 2 shows, the bilirubin fell to normal by the end of therapy in only 1 of 6 complete responders to irradiation; but by 2 months all values were normal. Although there have been 3 reported cases of possible extra-heaptic biliary fibrosis after irradiation of pri- mary’4,23 or metastatic3’ extra-hepatic biliary cancer, this was not evident in anyone in our series.
REFERENCES
I.
2.
3.
4.
5.
6.
7.
8.
9.
IO.
Il.
12.
13.
Abrams, H.L., Spiro, R., Goldstein, N.: Metastases in carcinoma. Cancer 3: 74-85, 1950. American Joint Committee for Cancer Staging and End Results Reporting (AJCCS): Manual for Staging of Cancer 1977, American Joint Committee, Chicago, III. 1977, pp. 18-21. Andreassen, M.: Metastasis to the hepatic pedicle in cancer of the stomach. Acta. Chir. Stand. 115: 178-184, 1958. Bentshay, D., Slavin, S., Levi, IS., Eliakim, M.: Obstruc- tive jaundice associated with carcinoma of the prostate. Isr. J. Med. Sci. 11: 838-844, 1977. Berkowitz, D., Gambescia, J., Thompson, C.M.: Jaundice with signs of extra-hepatic obstruction as the presenting symptom of bronchogenic carcinoma. Gastroent. 20: 653- 657, 1952. Bernadino, M.D., Goldstein, H.M.: Gray scale ultraso- nography in the evaluation of metastatic malanoma. Cancer 42: 2529-2533, 1978. Case Records of the Massachusetts General Hospital. N. Eng. J. Med. 285: 1369-1324, 1971. Chang, S.F., Burrell, M.I., Brand, M.H., Garsten, J.J.: The protein gastrointestinal manifestations of metastatic breast carcinoma. Radiology 126: 61 I-617, 1978. Chu, F.C.H.: Radiotherapy for Symptomatic Relief. Breast Cancer Management-Early and Late, Stall, B.A., Ed. Year Book Medical Publishers, Inc., 1977, pp. IOI- 107. Cole, H.S., Freston, J.W.: Recurrent melanoma presenting with obstructive jaundice. Report of 2 cases. Rocky Mount. Med. J. 70: 42-46, 1973. Dodd, G.D.: Percutaneous transhepatic cholangiography. Surg. Clin. N. Amer. 47: 1095-I 106, 1967. Elyaderani, M., Gabriele, O.F.: Percutaneous cholecystos- tomy and cholangiography in patients with obstructive jaundice. Radiology 130: 601-602, 1979. Ferrucci, J.T., Jr., Wittenberg, J.: Refinements in chiba
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24
25
needle transhepatic cholangiography. Am J. Roentgenol. 129: I I-16, 1977. Green, N., Mikkelsen, W.R., Kernen, J.A.: Cancer of the common hepatic bile duct-Palliative radiotherapy. Radi- ology 109: 687-689,1972. Hanna, S.S., Rider, W.D.: Carcinoma of the gallbladder or extra-hepatic bile ducts: The role of radiotherapy. Canad. Med. Assoc. J. 118: 59-61, 1978. Herbut, P.A., Watson, J.S.: Metastatic cancer of the extra-hepatic bile ducts producing jaundice. Amer. J. Clin. Pathol. 61: 365-372, 1974. Hopfan, S., Watson, R.: Porta hepatis irradiation. Int. J. Radiat. Oncol. Biol. Phys. 4: 333-336, 1978. Hudgins, P.R., Meoz, R.T.: Radiation therapy for obstruc- tive jaundice secondary to tumor malignancy. Int. J. Radiat. Oncol. Biol. Phys. 1: 1195-I 198, 1976. Hunt, T.: Malignant jaundice. Br. Med. J. 1: 361-362, 1968. Jaffe, B.M., Donegan, W.L., Watson, F., Spratt, J.S., Jr.: Factors influencing survival in patients with untreated hepatic metastases. Surg. Gynecol. Ohstet. 127: l-l 1, 1968. Kopelson, G.: Common duct cancer and radiotherapy (let- ter). Hosp. Practice 13: 17, 1978. Kopelson, G., Gunderson, L.L.: Radiation for bile-duct tumors (letter). N. Engl. J. Med. 298: 742.-743, 1978. Kopelson, G., Harisiadis, L., Tretter, P.. Chang, C.H.: The role of radiation therapy in cancer of the extra-hepatic biliary system: An analysis of thirteen patients and a review of the literature of the effectiveness of surgery, chemother- apy and radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2: 883-894, 1977. Meyer, J.E., Messer, R.J., Patel, V.C.: Diagnosis and treatment of obstructive jaundice secondary to liver metas- tases. Cancer 41: 773-775, 1978. Molnar, W., Stockum, A.E.: Relief of obstructive jaundice
504 Radiation Oncology 0 Biology 0 Physics April 1980, Volume 6, Number 4
26.
through percutaneous transhepatic catheter-A new thera- peutic method. Am. J. Roentgenol. 122: 356-367, 1974. Mori, K., Misumi, A., Sugiyama, M., Okabe, M., Matsuo- ka, T., Ishii, J., Akagi, M.: Percutaneous transhepatic bile drainage. Ann. Surg. 185: 111-I 15, 1977. Munzenrider, J.E., Tak, W.K., Tchakarova, 1.: Role of radiotherapy in advanced breast cancer, submitted for publication. Nagler, J., Rochwarger, A.M.: Metastatic colon carcinoma simulating primary bile duct carcinoma via endoscopic cholangiography. Gastrointest. Radiol. 2: 75-76, 1977. Oberfield, R.A., Cady, B., Pazianos, A.G., Salzman, F.A.: A multidisciplined approach for the management of meta- static breast cancer. Med. Clin. N.A. 56: 651-664, 1972. Ostick, D.G., Haggani, M.D.: Obstructive cholecystitis due to metastatic malanoma. Postgrad. Med. J. 52: 7 I O-7 12, 1976.
malignant biliary obstruction. Arch. Surg. 114: 148-l 5 I, 1979.
34.
21. 35.
28. 36.
29.
30.
31.
32.
33.
Papachristou, D., Fortner, J.G.: Biliary obstruction after gastrectomy for carcinoma of the stomach. Surg. Gynecol. Obstet. 147: 401-404, 1978. Pereiras, R.V., Jr., Rheingold, O.J., Hutson, D., Mejia, J., Viamonte, M., Chiprut, R.O., Schiff, E.R.: Relief of malig- nant obstructive jaundice by percutaneous insertion of a permanent prosthesis in the biliary tree. Ann. Intern. Med. 89 (Part I): 5899593, 1978. Pollock, T.W., Ring, E.R., Oleaga, J.A., Freiman, D.B., Rosato, E.F.: Percutaneous decompression of benign and
37.
38.
39.
40.
Popp, J.W., Jr., Schapiro, R.H., Warshaw, A.L.: Extra- hepatic biliary obstruction caused by metastatic breast carcinoma. Ann. Inter. Med. 91: 568-57 I, 1979. Rabin, M.S., Richter, I.A.: Metastatic breast carcinoma presently as obstructive jaundice. S. Afr. Med. J. 55: 388-390, 1979. Rentsch, I., Gartner, U., Muller, PL, Kerk, L.: Endoscopic retrograde cholangiopancreatography (ERCP) in obstruc- tive jaundice caused by metastatic testicular teratoma. Endosco~_~9: 101-103, 1977. Rohrmann, C.A., Ansel, J.J.. Protell, R.L., Silverstein, F.E., Silvis, SE., Vennes, J.A.: Significance of the nonopa- cified gallbladder in endoscopic retrograde cholangiogra- phy. Amer. J. Roentgenol. 132: 191-195, 1979. Sample, W.F., Gray, R.K., Poe. N.D., Graham, L.S., Bennett, L.R.: Nuclear imaging, tomographic nuclear imaging, and gray scale ultrasound in the evaluation of the porta hepatis. Radiology 122: 773-779, 1977. Taylor, K.J.W., Carpenter, D.A., McCready, V.R.: Ultra- sound and scintography in the differential diagnosis of obstructive jaundice J. Clin. Ultrasound 2: 105-l 16. 1974. Warshaw, A.L., Welch, J.P.: Extrahepatic biliary obstruc- tion by metastatic colon carcinoma. Ann. Surg. 188: 5933 597, 1978.